
What is Vibrio vulnificus
Vibrio vulnificus is an opportunistic human pathogen that is highly lethal and is responsible for the overwhelming majority of reported seafood-related deaths in the United States 1. Vibrio vulnificus is a Gram-negative bacterium that is a part of the natural flora of coastal marine environments worldwide and has been isolated from water, sediments, and a variety of seafood, including shrimp, fish, oysters, and clams 2. Consumption of seafood (primarily raw oysters) containing Vibrio vulnificus can result in a severe, fulminant systemic infection.
Vibrio vulnificus is responsible for two major syndromes: primary septicemia and wound infection. Vibrio vulnificus can cause skin infections after wound exposure to contaminated seawater, as well as primary septicemia through the consumption of contaminated raw or undercooked seafood.
Vibrio vulnificus causes an estimated 207 cases of illness each year, with 202 hospitalizations and 77 deaths 3.
Vibrio vulnificus is one of about a dozen species of Vibrio bacteria that can cause human illness, called vibriosis 4. Vibrio vulnificus naturally live in certain coastal waters and are present in higher concentrations between May and October when water temperatures are warmer. Those months overlap with the time when hurricanes and tropical storms are more likely to affect the U.S. mainland and many U.S. territories.
Vibrio vulnificus infection is characterized by fever, chills, nausea, hypotensive septic shock, and the formation of secondary lesions on the extremities of patients 5. Vibrio vulnificus septicemia (blood infection) is the most lethal infection caused by Vibrio vulnificus, with an average mortality rate exceeding 50% 1. A review of 459 U.S. cases reported by the U.S. Food and Drug Administration (FDA) between 1992 and 2007 revealed that 51.6% of the patients died 6. Interestingly, 85.6% of the cases were male. Of 180 cases in 2002 to 2007 for which FDA data were available, 92.8% of patients had consumed raw oysters prior to the onset of symptoms and 95.3% had some preexisting disease(s). The latter are clearly associated with Vibrio vulnificus infection, with liver diseases, such as cirrhosis or hepatitis, being the most common 7.
In addition to septicemia (sepsis), Vibrio vulnificus can produce serious wound infections that typically result from exposure of open wounds to water harboring the bacterium 8. Wound infections are frequently contracted as a result of recreational swimming, fishing injuries, or seafood handling 9. Like systemic disease, Vibrio vulnificus wound infections progress rapidly to cellulitis, ecchymoses, and bullae, which can progress to necrotizing fasciitis at the site of infection; however, the mortality rate for wound infections (approx. 25%) is lower than that for systemic disease 10. Vibrio vulnificu bacterium possesses a wide array of virulence factors, including acid neutralization, capsular polysaccharide expression, iron acquisition, cytotoxicity, motility, and expression of proteins involved in attachment and adhesion 6. These factors likely require concerted expression for pathogenesis to take place and appear to be under the control of global regulators. Overall, Vibrio vulnificus is a complex microorganism with physiological characteristics that contribute to its survival in the marine environment and in the human host.
Exposure of open wounds to seawater
Skin infection can result when open wounds are exposed to warm seawater. Wounds may be pre-existing or obtained in the water, e.g., from crabs, coral, or fishhooks. These infections may lead to cellulitis, necrosis (tissue death), hemorrhagic bullae, and infection of the bloodstream, particularly in people with impaired immunity.
Antibiotic therapy with doxycycline and a third-generation cephalosporin (eg, ceftazidime) is generally recommended for Vibrio vulnificus infection. Children can be treated with trimethoprim-sulfamethoxazole plus an aminoglycoside.
Necrotic tissue should be surgically removed. In contaminated wounds involving the limbs, amputation is sometimes necessary.
Ingestion of contaminated seafood
Raw oysters are most commonly implicated in transmission of Vibrio vulnificus. In healthy people, ingestion of contaminated seafood can cause vomiting, diarrhoea, and abdominal pain. In people with impaired immunity, particularly those with chronic liver disease or diabetes mellitus, Vibrio vulnificus can infect the bloodstream (septicaemia). This results in widespread hemorrhagic bullae (large blood-filled blisters) with fever and chills, and decreased blood pressure (septic shock). This condition is fatal in about 50% of patients.
Figure 1. Vibrio vulnificus bacteria
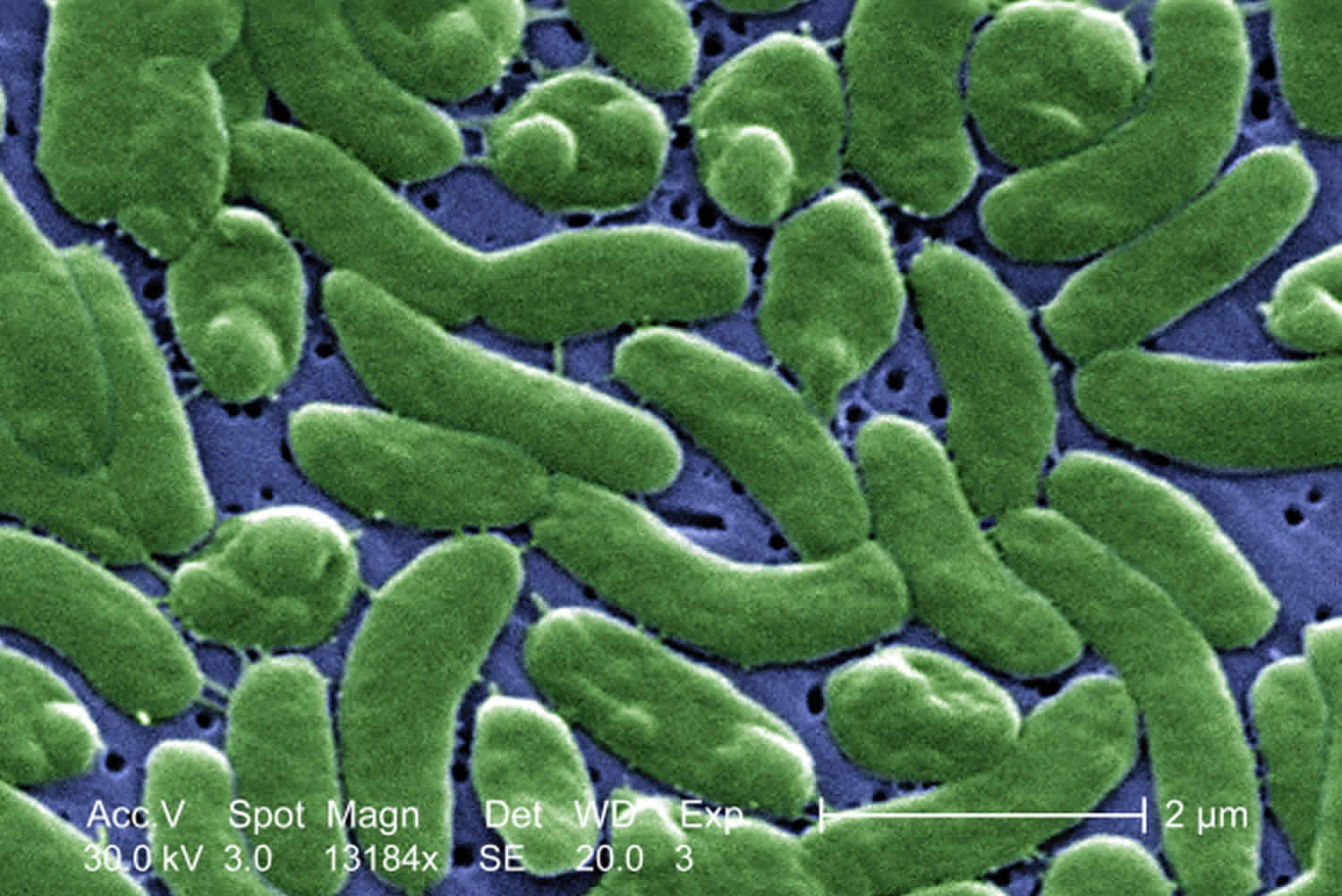
Figure 2. Vibrio vulnificus infection
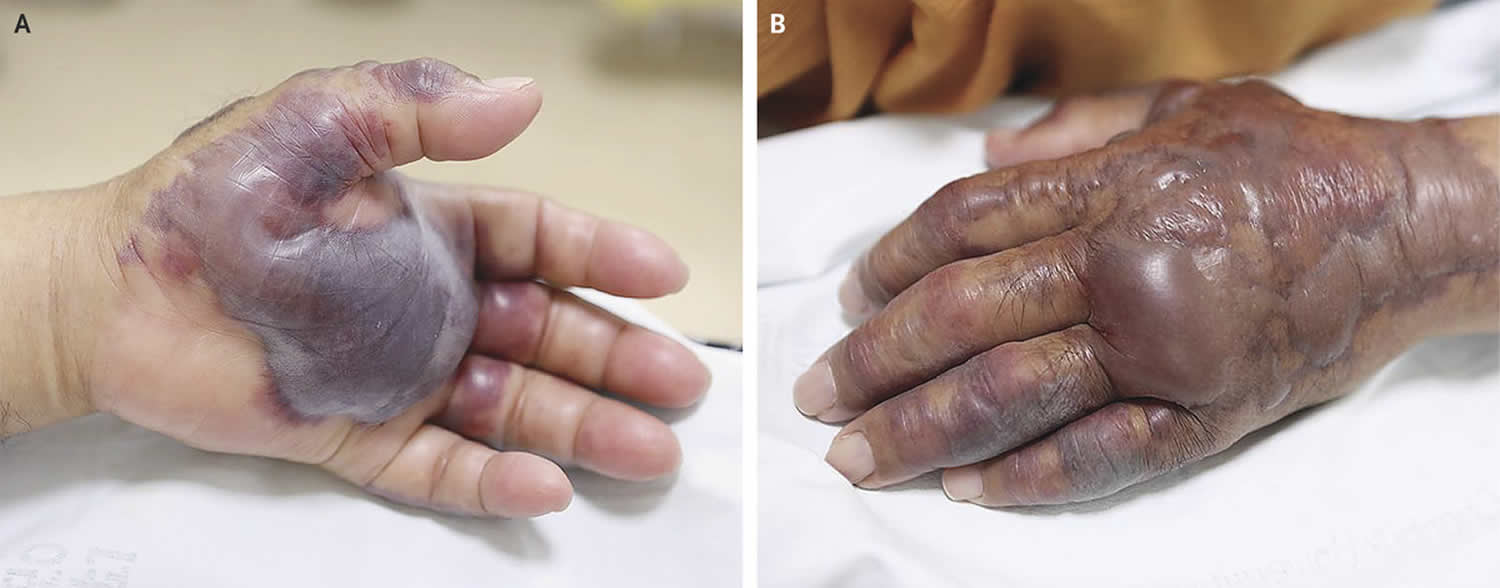
Footnote: A 71-year-old man presented to the emergency department with a 2-day history of fever and excruciating pain in his left hand that had developed 12 hours after eating raw seafood. He had a history of type 2 diabetes mellitus and hypertension and was undergoing hemodialysis for end-stage renal disease. At the time of presentation, hemorrhagic bullae measuring 3.5 by 4.5 cm had developed on the palm of his left hand (Panel A), and erythematous swelling with confluent tense bullae and ecchymoses had developed on the dorsum of the hand and forearm (Panel B). Surgical intervention was performed urgently, and Vibrio vulnificus was isolated from the bullae. Postoperatively, the patient received intravenous ceftazidime and ciprofloxacin. Despite treatment, the skin lesions progressed to deep necrotic ulcers, and amputation of the left forearm was performed 25 days after presentation. The patient did well after the surgery and was discharged home.
[Source 11]Are Vibrio vulnificus infections serious?
Yes. People with a Vibrio vulnificus infection can get seriously ill and need intensive care or limb amputation. About 1 in 7 people with a Vibrio vulnificus wound infection dies.
Who is more likely to get a Vibrio vulnificus infection?
Anyone can get a Vibrio vulnificus infection. People with a compromised immune system or liver disease are more likely to get an infection and severe complications.
The Centers for Disease Control and Prevention (CDC) estimates 80,000 people become sick with vibriosis, and 100 people die from their infection, in the United States every year.
Some Vibrio species, such as Vibrio vulnificus, can cause particularly severe and life-threatening infections. Many people with Vibrio vulnificus infections require intensive care or limb amputations, and about a quarter of people with this infection die, sometimes within a day or two of becoming ill.
Anyone can get sick from Vibrio vulnificus, but you may be more likely to get an infection or severe life-threatening illness if you:
- Have liver disease, cancer, diabetes, HIV/AIDS, or thalassemia
- Alcoholism
- Receive immune-suppressing therapy for the treatment of disease
- Take medicine to decrease stomach acid levels
- Have had recent stomach surgery
- Hemochromatosis/hemolytic anemia
- Chronic renal failure
- Other conditions that result in immunosuppression
How do people get a Vibrio vulnificus infection?
In the United States, people most often become infected with Vibrio vulnificus and other species of Vibrio by eating raw or undercooked shellfish, particularly oysters. Certain Vibrio species, including Vibrio vulnificus, can also cause a skin infection when an open wound is exposed to brackish or salt water. Brackish water is a mixture of fresh and sea water that is often found where rivers meet the sea.
When a hurricane or storm surge causes flooding, you may be exposed to coastal water. If you are in a group more likely to get a Vibrio vulnificus infection, it is especially important to take steps to reduce your risk of infection.
Vibrio vulnificus symptoms
Vibrio vulnificus is a bacterium that is a rare cause of illness in the United States. Infection with Vibrio vulnificus is a serious health threat that predominantly affects people with a compromised immune system or an underlying illness, especially liver disease. People who develop wound infections generally do so following contamination of a pre-existing wound or through an injury acquired while exposed to brackish or salt water. Vibrio vulnificus infection is very rare among children.
Vibrio vulnificus can cause two types of illnesses:
- Vibrio vulnificus wound infections, which may start as redness and swelling at the site of the wound that can spread to affect much of the body, and
- Vibrio vulnificus septicemia, a bloodstream infection is characterized by the abrupt onset of chills, fever, headache, myalgias, vomiting, and diarrhea 24 to 48 hours after ingestion of raw oysters, and sometimes followed by hypotension. Cutaneous lesions develop within the first 36 hours of onset.
The two most common clinical syndromes caused by Vibrio vulnificus are foodborne disease and wound infections; foodborne disease results from the ingestion of raw seafood, particularly oysters, and wound infections occur after skin lesions are exposed to contaminated seawater 12. According to U.S. surveillance data, patients with foodborne illness have higher rates of septicemia (87% versus 55%) and death (61% versus 17%) than those with wound infections 12. Since Vibrio vulnificus disseminates from the gastrointestinal tract to the bloodstream, patients with foodborne infections can progress rapidly to septicemia, disseminated intravascular coagulation (DIC), and multiorgan failure within days of consuming seafood 13. Of concern, recent epidemiological studies have reported an increase in the incidence of Vibrio vulnificus infections worldwide. According to FoodNet, an active surveillance network of foodborne diseases in the United States, the annual incidence of Vibrio vulnificus per 100,000 population increased from 0.01 to 0.05 between 1996 and 2010 14. Furthermore, warming ocean patterns have coincided with the emergence of Vibrio vulnificus infections along the northern U.S. Atlantic coast and Baltic Sea 15.
Symptoms of a Vibrio vulnificus infection include:
- Serious illness, with a rapid decline in health;
- Watery diarrhea, often accompanied by stomach cramping, nausea, vomiting, and fever;
- Skin infection after an open wound is exposed to brackish or salt water;
- Bloodstream infection, with fever, chills, dangerously low blood pressure, blistering skin lesion, and sometimes death.
Vibrio vulnificus prevention
Prompt first aid can help heal small wounds and prevent infection.
You can reduce your risk of Vibrio vulnificus wound infection by following these tips regarding wounds:
- Stay out of brackish or salt water if possible if you have a wound. Cover your wound with a waterproof bandage if there’s a possibility it could come into contact with brackish or salt water, raw seafood, or raw seafood juices.
- Wash wounds and cuts thoroughly with soap and water if they have been exposed to brackish or salt water, or raw seafood or its juices.
- If you develop a skin infection, tell your medical provider if your skin has come into contact with brackish or salt water, raw seafood, or raw seafood juices.
- Cover clean, open wounds with a waterproof bandage to reduce chance of infection.
- Seek immediate medical care if a wound develops redness, swelling, or oozing or other signs of working infection such as fever, increasing pain, shortness of breath, fast heart rate, or confusion or disorientation, high heart rate.
Take Care of Wounds
- Wash your hands thoroughly with soap and clean water, if possible.
- Avoid touching the wound with your fingers while treating it (if possible, use disposable, latex gloves).
- Remove obstructive jewelry and clothing from the injured body part.
- Apply direct pressure to any bleeding wound to control bleeding.
- Clean the wound after bleeding has stopped.
- Examine wounds for dirt and foreign objects.
- Gently flood the wound with bottled water or clean running water (if available, saline solution is preferred).
- Gently clean around the wound with soap and clean water.
- Pat dry and apply an adhesive bandage or dry clean cloth.
- Leave unclean wounds, bites, and punctures open. Wounds that are not cleaned correctly can trap bacteria and result in infection.
- Provide pain relievers when possible.
- Review the wound every 24 hours.
Seek medical attention as soon as possible if:
- There is a foreign object (soil, wood, metal, or other objects) embedded in the wound;
- A wound is a result of an animal bite;
- A wound is a result of a puncture by a dirty object;
- The wound is infected (pain and soreness, swelling, redness, draining, or you develop a fever);
- You have signs of sepsis such as confusion or disorientation, shortness of breath, high heart rate, fever or shivering, extreme pain or discomfort or clammy or sweaty skin.
If you have wounds, you should be evaluated for a tetanus immunization. If you receive a puncture wound or a wound contaminated with feces, soil, or saliva, have a health care professional determine whether a tetanus booster is necessary based on individual records.
Tips for cooking shellfish
Before cooking, discard any shellfish with open shells.
For shellfish in the shell, either:
- Boil until the shells open and continue boiling 5 more minutes, or
- Steam until the shells open and continue steaming for 9 more minutes.
Only eat shellfish that open during cooking. Discard shellfish that do not open fully after cooking.
For shucked oysters, either:
- Boil for at least 3 minutes,
- Fry in oil for at least 3 minutes at 375° F (191 °C),
- Broil 3 inches from heat for 3 minutes, or
- Bake at 450° F (232 °C) for 10 minutes.
Vibrio vulnificus diagnosis
Vibrio vulnificus infection is diagnosed when Vibrio bacteria are found in the wound, blood, or stool (poop) of an ill person. Vibrio vulnificus infection is treated with antibiotics. Limb amputation is sometimes necessary to remove dead or infected tissue.
Vibrio vulnificus treatment
Given the severity of foodborne Vibrio vulnificus infections, effective empirical treatments and timely diagnosis are essential for halting the progression of disease and improving clinical outcomes 16. Based on test tube and animal studies, the Centers for Disease Control and Prevention (CDC) recommend a fluoroquinolone or a third-generation cephalosporin in combination with a tetracycline for the treatment of Vibrio vulnificus infections 16. A time-kill study found that cefotaxime and minocycline were synergistic in test tube, since subinhibitory concentrations of cefotaxime with minocycline reduced Vibrio vulnificus growth by 6 orders of magnitude from that with either antibiotic alone 17. These results translated in animal: cefotaxime-and-minocycline combination therapy resulted in survival rates significantly higher than those with minocycline monotherapy in a wound infection model in mice 18. Synergy was attributed to the fact that the antibiotics target different processes essential for Vibrio vulnificus growth: cefotaxime targets cell wall growth, while minocycline inhibits protein synthesis 18. Fluoroquinolones were found to be equivalent in efficacy to combination therapy with cefotaxime and minocycline in wound infection models 19. The activity of fluoroquinolones against Vibrio vulnificus may be related to their ability to decrease the production of the Vibrio vulnificus multifunctional autoprocessing repeats-in-toxin toxin, the primary virulence factor associated with mortality in mice 20. Because all prior antibiotic efficacy studies were performed in wound infection models, there is a significant gap in our knowledge about the optimal antimicrobial therapy for foodborne Vibrio vulnificus infections. Since foodborne infections are associated with worse clinical outcomes than wound infections, studies are needed to assess the efficacy of antibiotics in an intestinal Vibrio vulnificus infection model.
While CDC treatment guidelines are applicable once a Vibrio vulnificus diagnosis is confirmed, fluoroquinolones, third-generation cephalosporins, and tetracyclines are rarely administered in the initial management of sepsis pending a microbiological diagnosis. For initial treatment, the Surviving Sepsis Campaign recommends the initiation of extended-spectrum β-lactam antibiotics, including cefepime and piperacillin-tazobactam, for coverage of resistant Gram-negative organisms 21. Although sepsis is the most common initial presentation of patients with foodborne Vibrio vulnificus infections, there are no studies on the efficacy of extended-spectrum β-lactam antibiotics for Vibrio vulnificus foodborne septicemia. While one is awaiting a microbiological diagnosis for a septic patient with a recent history of raw seafood consumption, it is essential for the initial empirical antibiotic regimen to provide effective treatment for a possible foodborne Vibrio vulnificus infection, since the illness can progress to death within days.
Vibrio vulnificus skin infection
Vibrio vulnificus infection should be considered for infected wounds that were exposed to coastal waters. Treatment should be initiated immediately because antibiotics improve survival. Aggressive attention should be given to the wound site; amputation of the infected limb is sometimes necessary.
- Culture of wound or hemorrhagic bullae is recommended, and all Vibrio vulnificus isolates should be forwarded to a public health laboratory
- Blood cultures are recommended if the patient is febrile, has hemorrhagic bullae, or has any sign of sepsis
- Necrotic tissue should be debrided; severe cases may require fasciotomy or limb amputation
- Antibiotic therapy: Doxycycline (100mg PO/IV twice a day for 7–14 days) and a third-generation cephalosporin (e.g., ceftazidime 1–2g IV/IM every eight hours) is generally recommended
- A single agent regimen with a fluoroquinolone such as levofloxacin, ciprofloxacin, or gatifloxacin, has been reported to be at least as effective in an animal model as a regimens with doxycycline and a cephalosporin
- Children, in whom doxycycline and fluoroquinolones are sometimes contradicted, can be treated with trimethoprim-sulfamethoxazole plus an aminoglycoside.
- Feldhusen, F. 2000. The role of seafood in bacterial foodbourne diseases. Microbes Infect. 21651-1660.
- Baffone, W., R. Tarsi, L. Pane, R. Campana, B. Repetto, G. L. Mariottini, and C. Pruzzo. 2006. Detection of free-living and plankton-bound vibrios in coastal waters of the Adriatic Sea (Italy) and study of their pathogenicity associated properties. Environ. Microbiol. 81299-1305.
- 217 – Other Pathogenic Vibrios. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases (Eighth Edition). Volume 2, 2015, Pages 2480-2484.e1
- Vibrio vulnificus Infections and Disasters. https://www.cdc.gov/disasters/vibriovulnificus.html
- Bowdre, J. H., J. H. Hull, and D. M. Cocchetto. 1983. Antibiotic efficacy against Vibrio vulnificus in the mouse: superiority of tetracycline. J. Pharmacol. Exp. Ther. 22595-598.
- Jones MK, Oliver JD. Vibrio vulnificus: Disease and Pathogenesis. Infection and Immunity. 2009;77(5):1723-1733. doi:10.1128/IAI.01046-08. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2681776/
- Oliver, J. D. 2006. Vibrio vulnificus, p. 253-276. In S. Belkin and R. R. Colwell (ed.), Oceans and health: pathogens in the marine environment. Springer Science, New York, NY.
- Oliver, J. D. 2005. Wound infections caused by Vibrio vulnificus and other marine bacteria. Epidemiol. Infect. 133383-391. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2870261/
- Bisharat, N., V. Agmon, R. Finkelstein, R. Raz, G. Ben-Dror, L. Lemer, S. Soboh, R. Colodner, D. N. Cameron, D. L. Wykstra, D. L. Swerdlow, and J. J. Farmer III. 1999. Clinical, epidemiological, and microbiological features of Vibrio vulnificus biogroup 3 causing outbreaks of wound infection and bacteraemia in Israel. Lancet 3541421-1424
- Bowdre, J. H., M. D. Poole, and J. D. Oliver. 1981. Edema and hemoconcentration in mice experimentally infected with Vibrio vulnificus. Infect. Immun. 321193-1199.
- Vibrio vulnificus Infection. New England Journal of Medicine July 26, 2018 379(4):375 https://www.nejm.org/doi/full/10.1056/NEJMicm1716464
- Menon MP, Yu PA, Iwamoto M, Painter J. 2014. Pre-existing medical conditions associated with Vibrio vulnificus septicaemia. Epidemiol Infect 142:878–881. doi:10.1017/S0950268813001593
- Zhao H, Xu L, Dong H, Hu J, Gao H, Yang M, Zhang X, Chen X, Fan J, Ma W. 2015. Correlations between clinical features and mortality in patients with Vibrio vulnificus infection. PLoS One 10:e0136019. doi:10.1371/journal.pone.0136019 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4537211/
- Newton A, Kendall M, Vugia DJ, Henao OL, Mahon BE. 2012. Increasing rates of vibriosis in the United States, 1996–2010: review of surveillance data from 2 systems. Clin Infect Dis 54(Suppl 5):S391–S395. doi:10.1093/cid/cis243
- Vezzulli L, Grande C, Reid PC, Helaouet P, Edwards M, Hofle MG, Brettar I, Colwell RR, Pruzzo C. 2016. Climate influence on Vibrio and associated human diseases during the past half-century in the coastal North Atlantic. Proc Natl Acad Sci U S A 113:E5062–E5071. doi:10.1073/pnas.1609157113
- Wong KC, Brown AM, Luscombe GM, Wong SJ, Mendis K. 2015. Antibiotic use for Vibrio infections: important insights from surveillance data. BMC Infect Dis 15:226. doi:10.1186/s12879-015-0959-z
- Chuang YC, Liu JW, Ko WC, Lin KY, Wu JJ, Huang KY. 1997. In vitro synergism between cefotaxime and minocycline against Vibrio vulnificus. Antimicrob Agents Chemother 41:2214–2217
- Chuang YC, Ko WC, Wang ST, Liu JW, Kuo CF, Wu JJ, Huang KY. 1998. Minocycline and cefotaxime in the treatment of experimental murine Vibrio vulnificus infection. Antimicrob Agents Chemother 42:1319–1322
- Tang HJ, Chang MC, Ko WC, Huang KY, Lee CL, Chuang YC. 2002. In vitro and in vivo activities of newer fluoroquinolones against Vibrio vulnificus. Antimicrob Agents Chemother 46:3580–3584. doi:10.1128/AAC.46.11.3580-3584.2002
- Jang HC, Choi SM, Kim HK, Kim SE, Kang SJ, Park KH, Ryu PY, Lee TH, Kim YR, Rhee JH, Jung SI, Choy HE. 2014. In vivo efficacy of the combination of ciprofloxacin and cefotaxime against Vibrio vulnificus sepsis. PLoS One 9:e101118. doi:10.1371/journal.pone.0101118
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb SA, Beale RJ, Vincent JL, Moreno R., Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup. 2013. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med 41:580–637. doi:10.1097/CCM.0b013e31827e83af





{kind=link}