
What is Lutein
Lutein is a oxygenated carotenoid found naturally in vegetables and fruits 1. Lutein is synthesized only by plants and like other xanthophylls, is found in high quantities in green leafy vegetables such as spinach, kale and yellow carrots 2. In green plants, xanthophylls act to modulate light energy and serve as non-photochemical quenching agents to deal with triplet chlorophyll (an excited form of chlorophyll), which is overproduced at very high light levels, during photosynthesis 3.
Lutein is also naturally present in a concentrated area of the macula of the human retina, a small area of the retina responsible for central vision, where together with zeaxanthin it forms the macular pigment 4. Zeaxanthin, which is fully conjugated (lutein is not), may offer somewhat better protection than lutein against phototoxic damage caused by blue and near ultraviolet light radiation 3.
Figure 1. Eye Retina and Macula Lutea
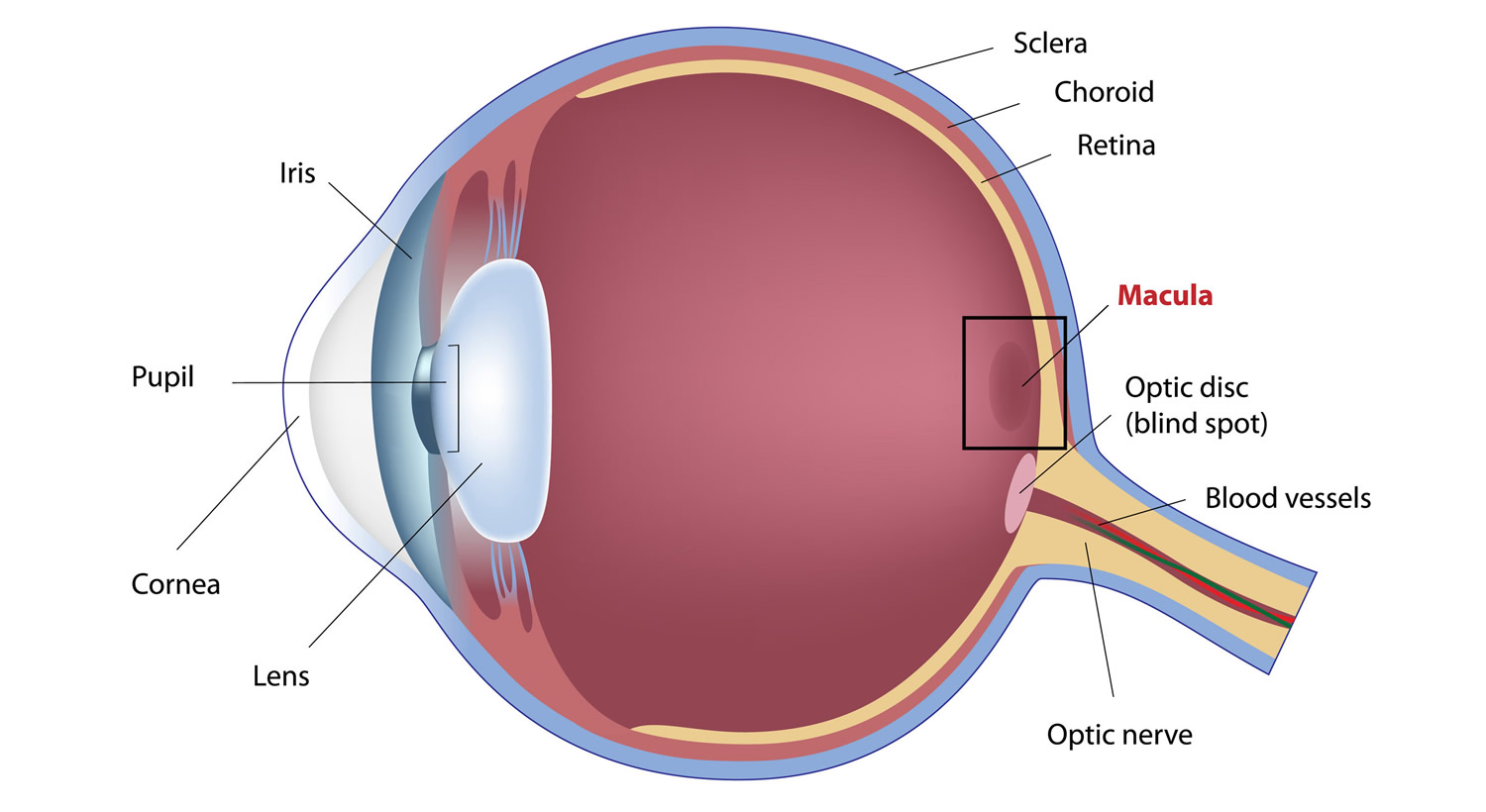
Note: The macula lutea is located in the central and back portion of the retina and possesses the highest concentration of photoreceptors, which are responsible for central vision and high-resolution visual acuity. It is a circular area 5–6 mm in diameter that possesses a characteristic yellow pigment that is made up entirely of lutein and zeaxanthin 5.
Lutein in the retina is believed to act as a yellow filter, filtering out potentially phototoxic blue light and near-ultraviolet radiation from the macula. The protective effect is due in part, to the reactive oxygen species quenching ability of this carotenoid. The hypothesis for the natural concentration is that lutein helps protect from oxidative stress and high-energy light. Several studies show that an increase in macula pigmentation decreases the risk for eye diseases such as Age-related Macular Degeneration (AMD) 6.
Lutein acts as an antioxidant, protecting cells against the damaging effects of free radicals. Lutein like other Xanthophylls also can inhibit peroxidation of membrane phospholipids and reduce lipofuscin formation, both of which contribute to their antioxidant properties.
Lutein is more stable to decomposition by pro-oxidants than are other carotenoids such as beta-carotene and lycopene.
Lutein is one of only two carotenoids that have been identified in the human lens, may be protective against age-related increases in lens density and cataract formation 3. This study showed dietary lutein and zeaxanthin intake is associated with a reduced risk of age-related cataract, especially nuclear cataract in a dose-response manner, indicating a beneficial effect of lutein and zeaxanthin in age-related cataract prevention 7. Again, the possible protection afforded by lutein may be accounted for, in part, by its reactive oxygen species scavenging abilities. Carotenoids also provide protection from cancer 8, 9. One of the mechanisms of this is by increasing the expression of the protein connexin-43, thereby stimulating gap junctional communication and preventing unrestrained cell proliferation 3.
What are Carotenoids
The major carotenoids of current medical research interest, found in colored fruit and vegetables, include carotenes (that animals, including humans, can convert to vitamin A), lycopene, lutein, and zeaxanthin 10. In part because of the beneficial effects of carotenoids are thought to be due to their role as antioxidants. beta-Carotene may have added benefits due its ability to be converted to vitamin A. Furthermore, lutein and zeaxanthin may be protective in eye disease because they absorb damaging blue light that enters the eye. Carotenoids occur widely throughout the vegetable kingdom and are readily accumulated by vegetable-consuming animals, including humans 10. Food sources of these compounds include a variety of fruits and vegetables, although the primary sources of lycopene are tomato and tomato products. Additionally, egg yolk is a highly bioavailable source of lutein and zeaxanthin. These carotenoids are available in supplement form also. However, intervention trials with large doses of beta-carotene found an adverse effect on the incidence of lung cancer in smokers and workers exposed to asbestos 11, 12. Until the efficacy and safety of taking supplements containing these nutrients can be determined, current dietary recommendations of diets high in fruits and vegetables are advised.
The ultimate source of all carotenoids in the human diet is plant material, directly, or indirectly from ingesting carotenoids and their metabolites in animal products such as egg yolk, milk, and poultry. Adequate intake of carotenoids is purportedly important for the prevention of all manner of disease. Yet, whereas supplies of vegetables and fruit vary dramatically around the world, there is little clinical evidence that any sizeable population consumes inadequate amounts for normal physiologic function. Only relatively recently was vitamin A deficiency definitively recognized to influence immune competence and increase infectious morbidity and mortality 13, despite previous suspicions that this might be the case. Until such time as true, carotenoid “deficiency”–related clinical entities are discovered, the only natural physiologic role recognized to be important is that of the provitamin A activity of carotenes, especially β-carotene 10.
Unusually large dietary consumption of various carotenoids has been linked to a reduction in the risk of various chronic diseases, particularly cancer of the lung, gastrointestinal tract, and pancreas; cardiovascular disease; and both cataract and age-related macular degeneration 14, 15, 16. Most supportive data arise from observational epidemiologic studies, which compared the risk (prevalence or incidence) of these conditions among individuals consuming few if any vegetables with those consuming the most. Other analyses and observational studies have failed to support these purported relations.
More worrisome still are the outcomes of several large, particularly well-conducted randomized clinical trials. In 2 of these trials, which specifically enrolled participants at high risk of lung cancer (smokers and/or asbestos workers) the active agents appeared to increase the risk of developing lung cancer 17, 18. Subsequent systematic reviews of the literature confirm the potential for increased cancer risks from β-carotene supplementation 18, 19.
Why these apparently conflicting clinical and epidemiologic results ? The most obvious reason is that purely observational studies are prone to suffer from bias. People who eat the most salad are likely to differ in many other ways from those who eat much less. Whereas these studies purportedly “adjust” for other differences in lifestyle and known risks, they cannot “adjust” for them all, nor necessarily for the most important. No study can collect data on every potentially important variable, and the most important variables may not even be known. Even if frequent consumption of salad, by itself, reduces the risk of certain diseases, salads contain an enormous number of different compounds, not just β-carotene or carotenoids in general.
Clearly, new and very different research designs are needed to begin to dissect out which dietary carotenoids (or combinations of carotenoids) are important for promoting health and preventing disease, if indeed there are diseases that increased carotenoid intake can help to prevent. The fact that lutein and zeaxanthin are highly concentrated in the macula strongly suggests that they might play a vital physiologic role 20. In the meantime, until definitive clinical evidence becomes available, we can only conclude that humans accumulate a variety of carotenoids, but their importance and roles remain uncertain. The only well-established pathophysiologic consequence of dietary carotenoid “deficiency” remains the provitamin A activity of carotene, especially β-carotene 10.
Lutein and Zeaxanthin
The human macula uniquely concentrates three carotenoids: lutein, zeaxanthin, and meso-zeaxanthin. Lutein and zeaxanthin must be obtained from dietary sources such as green leafy vegetables and orange and yellow fruits and vegetables, while meso-zeaxanthin is rarely found in diet and is believed to be formed at the macula by metabolic transformations of ingested carotenoids 21. Unlike the provitamin A carotenoids (α- and β-carotene and cryptoxanthin), they cannot be converted to vitamin A. Their presence in tissues is due entirely to ingestion of plant sources; they are not synthesized by animal tissues. However, a variety of metabolites may be found in animal sources, and several exist in human blood and milk 22. Meso-Zeaxanthin is rarely found in the human diet, but it has been detected in shrimp carapace, fish skin, and turtle fat, where all three isomers of zeaxanthin were found 23 and group of researchers have recently confirmed its presence in fish skin using more modern methods 24, 25. A significant amount of meso-zeaxanthin has been detected in commercially produced chicken eggs in Mexico where it is commonly added to the feed to achieve desirable coloration 26.
Approximately 30 to 50 carotenoids may exist in the diet, and about 20 may be measurable in the serum. The fact that only 2 of these, lutein and zeaxanthin, are present in the retina leads us to question why.
Lutein and zeaxanthin are especially concentrated in leafy green vegetables, many fruits, and colored vegetables such as squash, sweet peppers, sweet corn, and peas. Lutein is the dominant xanthophyll in almost all sources. Given the variability in food preferences among individuals and cultures, it is not surprising to have significant differences reported. African Americans on average consume twice as much lutein (about 3 mg/day) as Hispanic Americans and white Americans (1-2 mg/day) 27.
The macular pigment carotenoids, lutein, zeaxanthin, and meso-zeaxanthin are widely recommended as dietary supplements for the prevention of visual loss from age-related macular degeneration (AMD) and other ocular diseases. There is evidence that suggests that lutein and zeaxanthin may reduce risk for developing the two most common eye diseases in older people, i.e., cataract and macular degeneration. There is also the untested possibility that lutein and/or zeaxanthin may slow progression once these conditions are present. In addition, lutein may slow degeneration of vision in patients with retinitis pigmentosa 28, a heterogeneous group of slow retinal degenerations. However, only preliminary data in a very small number of patients have been published in which lutein slowed vision loss associated with retinitis pigmentosa in one but not another study.
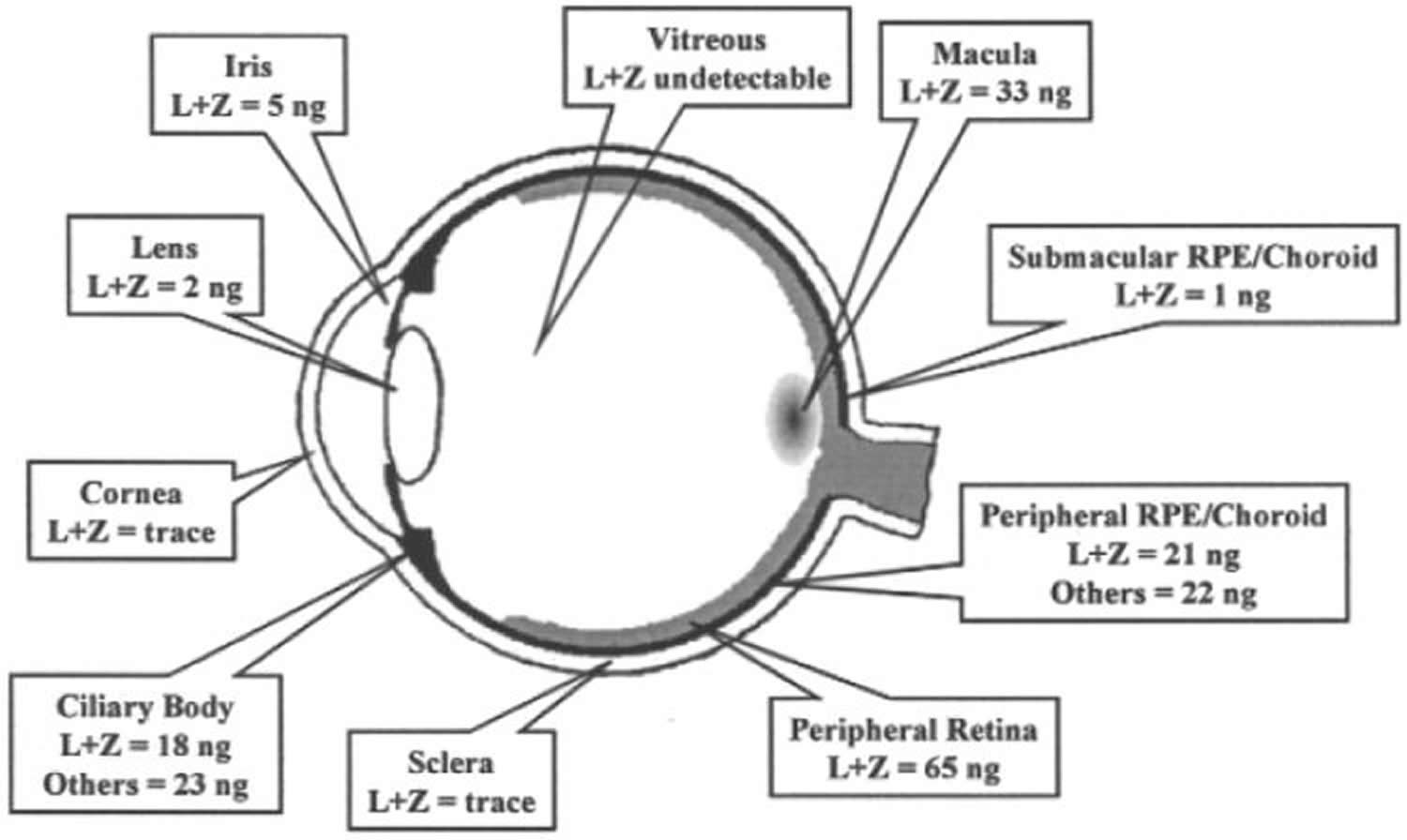
Figure 2. Lutein and Zeaxanthin levels in different parts of the eye
Lutein Health Benefits
A systematic review and meta-analysis of literature published on lutein suggest that higher dietary intake and higher blood concentrations of lutein are generally associated with better cardiometabolic health 2. Currently, there are no dietary recommendations for lutein intake 2. The literature on risk factors of cardiometabolic diseases suggested that lutein might prevent atherosclerosis and reduce inflammatory markers, but there were inconsistent associations with blood pressure, adiposity, insulin resistance, and blood lipids 2. The majority of the studies were observational and performed in adults, and the effects of lutein on cardiometabolic health in children and during pregnancy remains largely unaddressed.
Age-related eye diseases are a burden for the economy and a major cause of moderate to severe visual impairment and blindness 29. Age-related macular degeneration (AMD) is the most common cause of irreversible vision loss and legal blindness among older Americans 30. It is a degenerative condition of the region of the retina that is responsible for central vision (the macula). Age-related macular degeneration (AMD) is a multifactorial disease. Among the important risk factors for AMD are age, genetic susceptibility, sunlight exposure, cigarette smoking, and poor nutritional status 5. This condition, which has been estimated to affect about 0.5 percent of Americans over age 40 years 31, steeply increases in prevalence with age, up to 36% after 85 years of age for early AMD 32. Estimates from one United States community indicate that as many as 7 percent of persons between ages 75 and 84 years have age-related macular degeneration (AMD) 33 and could affect 196 million people by 2020 and 288 million by 2040 34.
Previous studies suggested that a consumption of lutein and zeaxanthin above 6-14 mg daily was considered to reduce the risk of eye diseases such as AMD as well as in alleviating the symptoms if present 35, 36. However, epidemiological studies indicated that the combined daily dietary intake of these carotenoids was only approximately 2 mg per day in western countries 37. Therefore, the additional consumption of these carotenoids supplements should be warranted.
Several risk factors have already been identified, both genetic and environmental 38. Oxidative stress is involved in the pathogenesis of AMD related to the retina’s high consumption of nutrients and oxygen and its exposure to light 39. Previous studies have found that the decrease in macular pigment was related with the functional abnormalities of the macula, which eventually led to some age-related degenerative eye diseases 40, 41.
In this late stage, age-related macular degeneration (AMD) usually cannot be successfully treated, and vision loss cannot be restored 42. Earlier stages of age-related maculopathy (ARM) are much more common, affecting about one quarter of people aged 65 years and older33 and increase the risk of developing late age-related maculopathy (ARM), also referred to as age-related macular degeneration (AMD) 43. Some reports revealed that the donor eyes with AMD showed a drastic decline of macular pigment levels as compared to eyes without AMD 44. According to previous studies, a lower MPOD appeared to be associated with an increased risk of progression to AMD 45, 46.
The functional roles of macular carotenoids, lutein and zeaxanthin, have not been completely characterized. However, some hypothetical functions in the human eye have been extrapolated from their known biological, optical, and photochemical properties. Evolution of the primate eye has ensured that almost all UV-B (320 to 290-nm) and UV-A (320-400-nm) light is absorbed by the cornea and the lens, respectively. Slightly longer-wave (blue) light (400-520 nm) reaching the macula is then largely absorbed by macular pigment, which has a peak absorbance of 460 nm. It has long been hypothesized that the pigment serves to reduce longitudinal chromatic aberration and to improve visual acuity 47. Light-induced retinal damage depends largely on the wavelength, exposure time, and intensity of light. For instance, the blue light (440 nm) requires 100 times less intensity to cause damage than orange light (590 nm). The presence of carotenoids in the macula capable of absorbing light of the blue range wavelength would indicate that they serve a protective function. Specifically lutein appears to play a specific role as a photoprotective agent, effectively screening out the damaging blue light from causing excessive damage on the photoreceptors 5. Glare is a frequent complaint among persons with advanced age, retinal disease, and cataract, as well as at any age in some individuals without obvious reasons for predisposition. A probable explanation may be the less than normal amounts of macular pigment. The extent of glare reduction by preferential absorption of polarized light has not been quantified, but several inferences can be made. Macular pigment is certainly reduced in individuals with age-related macular disease; this may be partly responsible for problems with glare in this population. Macular pigment is absent or severely reduced among those with albinism and advanced retinitis pigmentosa; the photophobia of these patients could be partly explained by their inability to dampen glare with macular pigment. Given the substantial interindividual variability of macular pigment levels, it is plausible that sensitivity to glare is increased in those with low pigment levels 48, 49.
Figure 3. Protective roles of lutein and zeaxanthin, as an absorber of harmful light and as an antioxidant
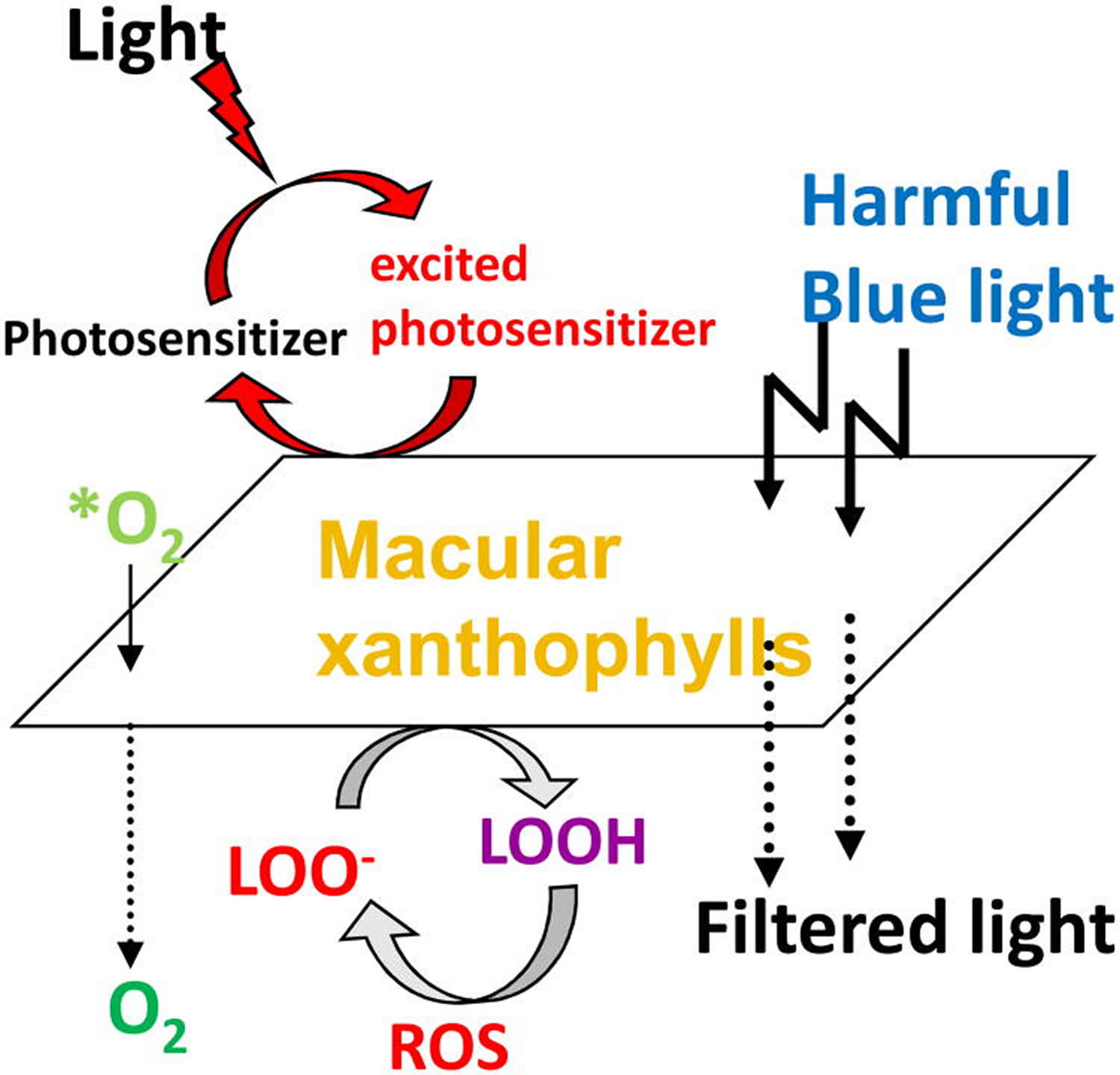
Note: Protective roles of lutein and zeaxanthin, as an absorber of harmful light and as an antioxidant reacting with reactive oxygen species (ROS). *O2, singlet oxygen; LOO-, lipid peroxyl radicals ;LOOH, lipid peroxides.
Another major proposed function of macular pigment, and the one that is pertinent to age-related disease, is neutralization of reactive oxygen species. The antioxidant system in cells and tissues includes enzymes (catalase, glutathione peroxidase, and superoxide dismutase), primary water-soluble antioxidants (such as glutathione and vitamin C), and lipid-soluble antioxidants (xanthophylls, retinoids, and vitamin E). The potential for the creation of reactive oxygen species in the retina is high. Reactive oxygen species are produced by absorption of UV and blue light by a photosensitizing compound or molecule (lipofuscin, protoporphyrin, or cytochrome).These longer-lived molecules can then react with oxygen to produce reactive oxygen species, including superoxide anion, hydroxyl radical, hydrogen peroxide, and singlet oxygen. These in turn can cause lipid peroxidation by attacking polyunsaturated fatty acids, resulting in DNA damage, protein and transmembrane glycoprotein oxidation, and other forms of cellular vandalism 50. To counteract the deleterious effects of free radicals to the retina, macular pigment (MP) made up of three main carotenoids, lutein, zeaxanthin and meso-zeaxanthin, constitutes a barrier to blue-light damage and has antioxidant properties 51. Many epidemiological and interventional studies have assessed carotenoid intake and content through dietary questionnaires or plasma L and Z measurements, finding that the consumption and plasma levels of lutein are inversely correlated with the risk of AMD 52. Carotenoids are potent scavengers of free radicals (eg, superoxide anion and hydroxyl radical) and are particularly efficient at neutralizing singlet oxygen. Because their lipid-soluble nature relegates them to membranes, it is likely that they especially protect the polyunsaturated fatty acid–rich membranes of the outer retina.
Lutein benefits is known mostly for its effect on visual function and its preventive effect against cataracts and macular degeneration 53, potentially through protection against oxidative stress 54. Given its antioxidant properties, it is hypothesized that lutein may also have beneficial effects on metabolic and cardiovascular diseases. Although the larger group of carotenoids has been associated with cardiometabolic protection 55, research has focused mostly on other carotenoids, such as β-carotene 56. Nevertheless, interventional studies with the use of β-carotene supplements have failed to reproduce the beneficial effects that were seen in observational studies. Thus, what the substance is behind the previously published beneficial effects of carotenoids has yet to be determined. The xanthophyll lutein is of particular interest because lutein may be a more active antioxidant than β-carotene 10.
Eliminating lutein from the diet of experimental animals results in early degenerative signs in the retina while patients with an acquired condition of macular pigment loss (Macular Telangiectasia) show serious visual handicap indicating the importance of macular pigment. Whether lutein intake reduces the risk of age related macular degeneration (AMD) or cataract formation is currently a strong matter of debate and abundant research is carried out to unravel the biological properties of the lutein molecule 57. SR-B1 has recently been identified as a lutein binding protein in the retina and this same receptor plays a role in the selective uptake in the gut 57. In the blood lutein is transported via high-density lipoproteins (HDL) 57. Genes controlling SR-B1 and HDL levels predispose to AMD which supports the involvement of cholesterol/lutein transport pathways 57. Apart from beneficial effects of lutein intake on various visual function tests, recent findings show that lutein can affect immune responses and inflammation. Lutein diminishes the expression of various ocular inflammation models including endotoxin induced uveitis, laser induced choroidal neovascularization, streptozotocin induced diabetes and experimental retinal ischemia and reperfusion 57. In vitro studies show that lutein suppresses NF kappa-B activation as well as the expression of iNOS and COX-2. Since AMD has features of a chronic low-grade systemic inflammatory response, attention to the exact role of lutein in this disease has shifted from a local effect in the eye towards a possible systemic anti-inflammatory function 57.
Lutein and zeaxanthin in Cataract
Lutein and zeaxanthin are the only carotenoids present in the crystalline lens 58, 59. Cataract is the opacification of the crystalline lens and is caused by precipitation of lens proteins. The development of cataract is facilitated by oxidative damage and often results in impaired vision or blindness.
Lutein and coronary heart disease
Pooled study results show that the highest intake of lutein was associated with a lower risk of coronary heart disease, compared with the lowest intake 2.
Lutein and stroke
Results of 3 longitudinal studies that reported on the associations between lutein and stroke were pooled 60, 61, 62. The pooled results showed that the highest intake of lutein was associated with a lower risk of stroke compared with the lowest intake 2.
Lutein and mortality from cardiovascular diseases
Five studies reported on lutein in relation to mortality from a combined outcome of any cardiovascular disease 63, 64, 65, 66, 67. Mean follow-up time ranged from 4.25 to 15 years and sample sizes ranged from 216 to 13,293. None of the studies found significant associations, but the effect estimates were mostly in the direction of higher lutein being associated with a lower risk of mortality from cardiovascular disease 63, 65, 66, 67 except for one study 64.
Two studies from a US cohort (one in male subjects and one in female subjects), both studies found no significant associations 68, 69.
Lutein and type 2 diabetes mellitus
The meta-analysis of the results of lutein in relation to type 2 diabetes mellitus included four studies 70, 71, 72, 73, all of which were longitudinal observational studies with follow-up periods between 10 and 23 years, including in total 35,242 participants (including 1661 cases). The pooled results showed no significant association between lutein and risk of diabetes.
Lutein in diabetic retinopathy
The role of lutein in diabetic retinopathy has not been well studied in human subjects. Only one prospective study on patients with non-proliferative diabetic retinopathy by Hu et al. 74 showed that the serum concentration of lutein and zeaxanthin is significantly lower in these patients compared to normal subjects. Their results also suggest that lutein and zeaxanthin supplementation in these patients lead to improvement of visual acuity and decrease in foveal thickness 74. Their study suggests that lutein and zeaxanthin supplementation may potentially be used as therapeutic agents in treating non-proliferative diabetic retinopathy.
Lutein and metabolic syndrome
Of the 6 studies on metabolic syndrome, one was in adolescents 75 and the others were in adults 76, 77, 78, 79, 80. All studies were cross-sectional, with a total of 8133 participants (including 1773 cases). The highest intake of lutein was associated with a lower risk of metabolic syndrome compared with the lowest intake of lutein 2.
Lutein Foods
Lutein and zeaxanthin are the most common xanthophylls in green leafy vegetables (e.g., kale, spinach, broccoli, peas and lettuce) and egg yolks 81 (Table 1). They are also found at relatively high levels in einkorn, Khorasan and durum wheat and corn and their food products (Table 1). The ratio of lutein and zeaxanthin in green vegetables has been reported to range between 12 to 63, highest being in kale, while in yellow-orange fruits and vegetable this ratio ranges between 0.1 and 1.4. Lutein is found in many natural products including broccoli, spinach, kale, corn, orange pepper, kiwi fruit, grapes, orange juice, zucchini, and squash. There is 44 mg of lutein per cup of cooked kale, 26 mg/cup of cooked spinach, and 3 mg/cup of broccoli.
They also quantified small amounts of lutein and zeaxanthin in breads prepared from modern wheat varieties, Pioneer and Catoctin, while breads prepared from green-harvested wheat, Freekeh, an ancient grain, contained considerably large amounts of lutein and zeaxanthin compared to the North American breads. Lutein to zeaxanthin ratio followed the order Pioneer > Catochtin > Freekeh 82. Chicken egg yolk is deemed a better source of lutein and zeaxanthin compared to fruits and vegetables because of its increased bioavailability due to the high fat content in eggs. The concentrations of lutein and zeaxanthin in chicken egg yolk are 292 ± 117 µg/yolk and 213 ± 85 µg/yolk (average weight of yolk is about 17–19 g), respectively and are likely dependent on the type of feed, found mainly in on-esterified form with minute amounts of lycopene and β-carotene 83. It is not surprising that egg noodle had almost 6 times more xanthophyll carotenoids than lasagne. Astaxanthin and fucoxanthin are abundant in green and brown algae, respectively, which are eaten by fish. Capsanthin is found mainly in pepper. β-Cryptoxanthin is a pro-vitamin A and found in many fruits and vegetables, but mainly in corn, oranges, peaches, papaya, watermelon, and egg yolk 84, 85.
In general carotenoids are very minor constituents in cereal grains except for einkorn and durum wheat and corn that contain relatively high levels of carotenoids or yellow pigments. The common carotenoids in cereal grains are α and β-carotene, β-cryptoxanthin, lutein and zeaxanthin with lutein being the dominant carotenoid compound. In common wheat flour (low in carotenoids), the bran/gem fraction had 4-fold more lutein, 12-fold more zeaxanthin, and 2-fold more β-cryptoxanthin than the endosperm fractions 86. Higher amounts of lutein were found in durum, Kamut and Khorasan (5.4–5.8 µg/g) compared with common bread and pastry wheat (2.0–2.1 µg/g). Einkorn, on the other hand, had the highest concentration of all-trans-lutein, which is influenced by environmental growing conditions and processing. Corn also contains exceptionally high levels of non-provitamin A carotenoids primarily lutein and zeaxanthin 87, 88.
Table 1. Commonly consumed foods as high sources of lutein and zeaxanthin (µg/g fresh weight except for corn tortilla and chips µg/g dry matter)
| Food | Lutein | Zeaxanthin |
|---|---|---|
| Vegetables | ||
| Basil a | 70.5 | in |
| Parsley a | 64.0–106.5 | in |
| Spinach a | 59.3–79.0 | in |
| Kale a | 48.0–114.7 | – |
| Leek a | 36.8 | in |
| Pea a | 19.1 | in |
| Lettuce a | 10.0–47.8 | – |
| Green pepper a | 8.8 | – |
| Broccoli a | 7.1–33.0 | in |
| Carrot a | 2.5–5.1 | in |
| Red pepper a | 2.5–85.1 | 5.9–13.5 |
| Eggs | ||
| Egg yolk a | 3.84–13.2 | – |
| Nuts | ||
| Pistachio a | 7.7–49.0 | – |
| Baked foods | ||
| High lutein bread b | 36.7 | 3.3 |
| High lutein cookie b | 21.3 | 2.9 |
| High lutein muffin b | 26.1 | 3.7 |
| Corn tortilla c | 72.5 | 105.3 |
| Corn chips c | 61.1 | 92.5 |
| Grains | ||
| Corn d | 21.9 | 10.3 |
| Einkorn wheat d | 7.4 | 0.9 |
| Khorasan wheat d | 5.5 | 0.7 |
| Durum wheat d | 5.4 | 0.5 |
Note: in = included with lutein.
Lutein supplements
It has been suggested that 6 mg of lutein per day, either through diet or using supplements is likely effective in reducing the risk of cataracts and AMD. Although the optimal dose for lutein supplementation has not been established yet, the most common dose in commercial products is 10 mg/day.
Carotenoids such as lutein and zeaxanthin are generally recognized as safe (GRAS) for human consumption by the FDA, which allows food manufacturers to use them as additives 90, 91. Recently, the European Food Safety Authority (EFSA) Panel on Food Additives and Nutrient Sources added to Food established an acceptable daily intake of 1 mg / kg bodyweight / day for lutein preparations derived from marigold (Tagetes erecta) containing at least 80% carotenoids 92, 93. Based on the available data, EFSA concluded that an intake of 0.75 mg / kg bodyweight / day of synthetic zeaxanthin does not raise any safety concerns 94. These values correspond to a daily intake of 53 mg of zeaxanthin and 70 mg of lutein for a person weighing 70 kg. These numbers are much higher than the earlier claims that 20 mg/day/person was safe in dietary supplements 95, 96. Mutagenic studies have revealed that lutein and zeaxanthin are safe for human consumption 97, 98. The no observed-adverse-effect-level (NOAEL) for lutein/zeaxanthin concentrate was determined to be 400 mg/kg bodyweight/day, the highest dose tested in rats 99. The safety of supplemental meso-zeaxanthin was recently reviewed 100, and the NOAEL of meso-zeaxanthin in rats is 300 mg/kg bodyweight/day when administered orally for 13 consecutive weeks 101.
Lutein Side Effects
Lutein is LIKELY SAFE when taken by mouth appropriately. Consuming 6.9-11.7 mg/day of lutein as part of the diet appears to be safe. Lutein supplements have been used safely in studies in doses up to 15 mg daily for up to 2 years.
Special Precautions & Warnings: Pregnancy and breast-feeding: Lutein is LIKELY SAFE when used in the amounts found in food 102.
Summary
Lutein is a oxygenated carotenoid that is synthesized only by plants and like other xanthophylls, is found naturally in high quantities in green leafy vegetables such as spinach, kale, squash, sweet peppers, sweet corn, peas and yellow carrots. Lutein is also naturally present in a concentrated area of the macula of the human retina, a small area of the retina responsible for central vision, where together with zeaxanthin it forms the macular pigment. Several studies show that lutein, zeaxanthin and meso-zeaxanthin supplementation improved macular pigment optical density both in AMD patients and healthy subjects with a dose-response relationship, whereas the improvement in visual acuity was milder 103, 104. Dietary lutein and zeaxanthin intake is also associated with a reduced risk of age-related cataract, especially nuclear cataract in a dose-response manner, indicating a beneficial effect of lutein and zeaxanthin in age-related cataract prevention.
Studies have also shown that higher dietary intake of lutein and higher blood concentrations are associated with a lower risk of coronary heart disease, stroke, and metabolic syndrome, but not with risk of type 2 diabetes mellitus, possibly through less atherosclerosis and lower inflammatory activity 2.
References- National Center for Biotechnology Information, U.S. National Library of Medicine. Lutein. https://pubchem.ncbi.nlm.nih.gov/compound/Lutein
- Am J Clin Nutr February 2016, vol. 103 no. 2 481-494. The effects of lutein on cardiometabolic health across the life course: a systematic review and meta-analysis. http://ajcn.nutrition.org/content/103/2/481.long
- Canadian Institutes of Health Research. DrugBank. Lutein. https://www.drugbank.ca/drugs/DB00137
- Prog Retin Eye Res. 2012 Jul;31(4):303-15. doi: 10.1016/j.preteyeres.2012.03.002. Epub 2012 Mar 21. Lutein: more than just a filter for blue light. https://www.ncbi.nlm.nih.gov/pubmed/22465791?dopt=Abstract
- Koushan K, Rusovici R, Li W, Ferguson LR, Chalam KV. The Role of Lutein in Eye-Related Disease. Nutrients. 2013;5(5):1823-1839. doi:10.3390/nu5051823. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3708350/
- National Center for Biotechnology Information, U.S. National Library of Medicine. PubChem. Lutein. https://pubchem.ncbi.nlm.nih.gov/compound/Lutein
- Ma L, Hao ZX, Liu RR, Yu RB, Shi Q, Pan JP. Graefes Arch Clin Exp Ophthalmol. 2014 Jan;252(1):63-70. doi: 10.1007/s00417-013-2492-3. Epub 2013 Oct 23. A dose-response meta-analysis of dietary lutein and zeaxanthin intake in relation to risk of age-related cataract. https://www.ncbi.nlm.nih.gov/pubmed/24150707
- Bae J-M. Reinterpretation of the results of a pooled analysis of dietary carotenoid intake and breast cancer risk by using the interval collapsing method. Epidemiology and Health. 2016;38:e2016024. doi:10.4178/epih.e2016024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4974449/
- Chen J, Jiang W, Shao L, Zhong D, Wu Y, Cai J. Int J Food Sci Nutr. 2016 Nov;67(7):744-53. doi: 10.1080/09637486.2016.1197892. Epub 2016 Jun 30. Association between intake of antioxidants and pancreatic cancer risk: a meta-analysis. https://www.ncbi.nlm.nih.gov/pubmed/27356952
- Sommer A, Vyas KS. A global clinical view on vitamin A and carotenoids. Am J Clin Nutr 2012;96:1204S–6S. http://ajcn.nutrition.org/content/96/5/1204S.full
- N Engl J Med. 1996 May 2;334(18):1150-5. Effects of a combination of beta carotene and vitamin A on lung cancer and cardiovascular disease. http://www.nejm.org/doi/full/10.1056/NEJM199605023341802
- Satia JA, Littman A, Slatore CG, Galanko JA, White E. Long-term Use of β-Carotene, Retinol, Lycopene, and Lutein Supplements and Lung Cancer Risk: Results From the VITamins And Lifestyle (VITAL) Study. American Journal of Epidemiology. 2009;169(7):815-828. doi:10.1093/aje/kwn409. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2842198/
- Sommer A, West KP Jr. Vitamin A deficiency: health, survival, and vision. New York, NY: Oxford University Press, 1996.
- Tapiero H, Townsend DM, Tew KD. The role of carotenoids in the prevention of human pathologies. Biomed Pharmacother 2004;58:100–10. https://www.ncbi.nlm.nih.gov/pubmed/14992791?dopt=Abstract
- Ribaya-Mercado JD, Blumberg JB. Lutein and zeaxanthin and their potential roles in disease prevention. J Am Coll Nutr 2004;23:567S–87S. https://www.ncbi.nlm.nih.gov/pubmed/15640510?dopt=Abstract
- Mares-Perlman JA, Millen AE, Ficek TL, Hankinson SE. The body of evidence to support a protective role for lutein and zeaxanthin in delaying chronic disease overview. J Nutr 2002;132(suppl):518S–24S. http://jn.nutrition.org/content/132/3/518S.full
- Omenn GS, Goodman GE, Thornquist MD, Balmes J, Cullen MR, Glass A, Keogh JP, Meyskens FL, Valanis B, Williams JH, et al. Effects of a combination of beta carotene and vitamin A on lung cancer and cardiovascular disease. N Engl J Med 1996;334:1150–5. http://www.nejm.org/doi/full/10.1056/NEJM199605023341802
- Albanes D. β-Carotene and lung cancer: a case study. Am J Clin Nutr 1999;69:1345S–50S. http://ajcn.nutrition.org/content/69/6/1345s.full
- Druesne-Pecollo N, Latino-Martel P, Norat T, Barrandon E, Bertrais S, Galan P, Hercberg S. Beta-carotene supplementation and cancer risk: a systematic review and metaanalysis of randomized controlled trials. Int J Cancer 2010;127:172–84. https://www.ncbi.nlm.nih.gov/pubmed/19876916?dopt=Abstract
- Whitehead AJ, Mares JA, Danis RP. Macular pigment: a review of current knowledge. Arch Ophthalmol 2006;124:1038–45. http://jamanetwork.com/journals/jamaophthalmology/fullarticle/417803
- Bernstein PS, Li B, Vachali PP, et al. Lutein, Zeaxanthin, and meso-Zeaxanthin: The Basic and Clinical Science Underlying Carotenoid-based Nutritional Interventions against Ocular Disease. Progress in retinal and eye research. 2016;50:34-66. doi:10.1016/j.preteyeres.2015.10.003. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4698241/
- Khachik, F., Bernstein, P. & Garland, D. L. (1997) Identification of lutein and zeaxanthin oxidation products in human and monkey retinas. Investig. Ophthamol. Vis. Sci. 38:1802-1811.
- The first isolation of enantiomeric and meso-zeaxanthin in nature. Maoka T, Arai A, Shimizu M, Matsuno T. Comp Biochem Physiol B. 1986; 83(1):121-4. https://www.ncbi.nlm.nih.gov/pubmed/3943294/
- Verification of Meso-Zeaxanthin in Fish. Nolan JM, Beatty S, Meagher KA, Howard AN, Kelly D, Thurnham DI. J Food Process Technol. 2014 Jun 1; 5(6):335. https://www.ncbi.nlm.nih.gov/pubmed/25717420/
- Macular response to supplementation with differing xanthophyll formulations in subjects with and without age-related macular degeneration. Thurnham DI, Nolan JM, Howard AN, Beatty S. Graefes Arch Clin Exp Ophthalmol. 2015 Aug; 253(8):1231-43. https://www.ncbi.nlm.nih.gov/pubmed/25311651/
- The selective retention of lutein, meso-zeaxanthin and zeaxanthin in the retina of chicks fed a xanthophyll-free diet. Wang Y, Connor SL, Wang W, Johnson EJ, Connor WE. Exp Eye Res. 2007 Mar; 84(3):591-8. https://www.ncbi.nlm.nih.gov/pubmed/17227674/
- Mares-Perlman JAFisher AIKlein R et al. Lutein and zeaxanthin in the diet and serum and their relation to age-related maculopathy in the Third National Health and Nutrition Examination Survey. Am J Epidemiol 2001;153424- 432. https://academic.oup.com/aje/article-lookup/doi/10.1093/aje/153.5.424
- Eye (Lond). 2017 Feb;31(2):273-285. doi: 10.1038/eye.2016.286. Epub 2016 Dec 9. Effectiveness and safety of nutritional supplements in the treatment of hereditary retinal dystrophies: a systematic review. https://www.ncbi.nlm.nih.gov/pubmed/27935602
- Bourne RR, Jonas JB, Flaxman SR, et al. Prevalence and causes of vision loss in high-income countries and in Eastern and Central Europe: 1990-2010. Br J Ophthalmol. 2014; 98: 629–638.
- National Advisory Eye Council. Vision research, a national plan, 1999–2003. Bethesda, MD: United States Department of Health and Human Services, National Institutes of Health, National Eye Institute, 1998. (NIH publication no. 98–4120).
- Klein R, Klein BEK, Jensen SC, et al. Age-related maculopathy in a multiracial United States population. The National Health and Nutrition Examination Survey III. Ophthalmology 1999;106:1056–65.
- Seydou Alassane, Christine Binquet, Vanessa Cottet, Olivier Fleck, Niyazi Acar, Sandrine Daniel, Cécile Delcourt, Lionel Bretillon, Alain M. Bron, Catherine Creuzot-Garcher; Relationships of Macular Pigment Optical Density With Plasma Lutein, Zeaxanthin, and Diet in an Elderly Population: The Montrachet Study. Invest. Ophthalmol. Vis. Sci. 2016;57(3):1160-1167. doi: 10.1167/iovs.15-18007. http://iovs.arvojournals.org/article.aspx?articleid=2503589
- Klein R, Klein BEK, Linton KLP. Prevalence of age-related maculopathy. The Beaver Dam Eye Study. Ophthalmology 1992;99:933–43.
- Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014; 2: e106–e116.
- Intake of lutein and zeaxanthin differ with age, sex, and ethnicity.Johnson EJ, Maras JE, Rasmussen HM, Tucker KL. J Am Diet Assoc. 2010 Sep; 110(9):1357-62. https://www.ncbi.nlm.nih.gov/pubmed/20800129/
- Lutein and zeaxanthin intakes and risk of age-related macular degeneration and cataracts: an evaluation using the Food and Drug Administration’s evidence-based review system for health claims. Trumbo PR, Ellwood KC. Am J Clin Nutr. 2006 Nov; 84(5):971-4. https://www.ncbi.nlm.nih.gov/pubmed/17093145/
- Changes in carotenoid intake from fruit and vegetables in the Spanish population over the period 1964-2004. Granado F, Blázquez S, Olmedilla B. Public Health Nutr. 2007 Oct; 10(10):1018-23. https://www.ncbi.nlm.nih.gov/pubmed/17381958/
- Miller JW. Age-related macular degeneration revisited—piecing the puzzle: the LXIX Edward Jackson memorial lecture. Am J Ophthalmol. 2013; 155: 1–35.e13.
- Seydou Alassane, Christine Binquet, Vanessa Cottet, Olivier Fleck, Niyazi Acar, Sandrine Daniel, Cécile Delcourt, Lionel Bretillon, Alain M. Bron, Catherine Creuzot-Garcher; Relationships of Macular Pigment Optical Density With Plasma Lutein, Zeaxanthin, and Diet in an Elderly Population: The Montrachet Study. Invest. Ophthalmol. Vis. Sci. 2016;57(3):1160-1167. doi: 10.1167/iovs.15-18007. http://iovs.arvojournals.org/article.aspx?articleid=2503589
- Macular pigment and risk for age-related macular degeneration in subjects from a Northern European population. Beatty S, Murray IJ, Henson DB, Carden D, Koh H, Boulton ME. Invest Ophthalmol Vis Sci. 2001 Feb; 42(2):439-46. https://www.ncbi.nlm.nih.gov/pubmed/11157880/
- Nutritional manipulation of primate retinas, I: effects of lutein or zeaxanthin supplements on serum and macular pigment in xanthophyll-free rhesus monkeys. Neuringer M, Sandstrom MM, Johnson EJ, Snodderly DM. Invest Ophthalmol Vis Sci. 2004 Sep; 45(9):3234-43. https://www.ncbi.nlm.nih.gov/pubmed/15326146/
- Macular Photocoagulation Study Group. Laser photocoagulation for juxtafoveal choroidal neovascularization. Five-year results for randomized clinical trials. Arch Ophthalmol 1994;112:500–9.
- Klein R, Klein BEK, Jensen SC, et al. The five-year incidence and progression of age-related maculopathy: The Beaver Dam Eye Study. Ophthalmology 1997;104:7–21.
- Bone R.A., Landrum J.T., Mayne S.T., Gomez C.M., Tibor S.E., Twaroska E.E. Macular pigment in donor eyes with and without AMD: A case-control study. Invest. Ophthalmol. Vis. Sci. 2001;42:235–240. https://www.ncbi.nlm.nih.gov/pubmed/11133874
- Biesalski H.K., Aggett P.J., Anton R., Bernstein P.S., Blumberg J., Heaney R.P., Henry J., Nolan J.M., Richardson D.P., van Ommen B., et al. 26th Hohenheim Consensus Conference, September 11, 2010 Scientific substantiation of health claims: Evidence-based nutrition. Nutrition. 2011;27:S1–S20. doi: 10.1016/j.nut.2011.04.002. https://www.ncbi.nlm.nih.gov/pubmed/21700425
- Puell M.C., Palomo-Alvarez C., Barrio A.R., Gómez-Sanz F.J., Pérez-Carrasco M.J. Relationship between macular pigment and visual acuity in eyes with early age-related macular degeneration. Acta. Ophthalmol. 2013;91:e298–e303. doi: 10.1111/aos.12067. https://www.ncbi.nlm.nih.gov/pubmed/23575039
- Howarth PABradley A The longitudinal chromatic aberration of the human eye and its correction. Vis Res 1986;26361- 366. https://www.ncbi.nlm.nih.gov/pubmed/3716229
- Hammond BR JrWooten BRSnodderly DM Preservation of visual sensitivity of older subjects: association with macular pigment density. Invest Ophthalmol Vis Sci 1998;39397- 406. https://www.ncbi.nlm.nih.gov/pubmed/9478000
- Werner JSPeterzell DHScheetz AJ Light, vision, and aging. Optom Vis Sci 1990;67214- 229. https://www.ncbi.nlm.nih.gov/pubmed/2181364
- Winkler BSBoulton MEGottsch JDSternberg P Oxidative damage and age-related macular degeneration. Mol Vis 1999;532 Review. https://www.ncbi.nlm.nih.gov/pubmed/10562656
- Kijlstra A, Tian Y, Kelly ER, Berendschot TT. Lutein: more than just a filter for blue light. Prog Retin Eye Res. 2012; 31: 303–315.
- Delcourt C, Carriere I, Delage M, Barberger-Gateau P, Schalch W. Plasma lutein and zeaxanthin and other carotenoids as modifiable risk factors for age-related maculopathy and cataract: the POLA Study. Invest Ophthalmol Vis Sci. 2006; 47: 2329–2335.
- Kijlstra A, Tian Y, Kelly ER, Berendschot TTJM. Lutein: More than just a filter for blue light. Prog Retin Eye Res 2012;31:303–15. https://www.ncbi.nlm.nih.gov/pubmed/22465791?dopt=Abstract
- Sujak A, Gabrielska J, Grudzinski W, Borc R, Mazurek P, Gruszecki WI. Lutein and zeaxanthin as protectors of lipid membranes against oxidative damage: The structural aspects. Arch Biochem Biophys 1999;371:301–7. https://www.ncbi.nlm.nih.gov/pubmed/10545218?dopt=Abstract
- Voutilainen S, Nurmi T, Mursu J, Rissanen TH. Carotenoids and cardiovascular health. Am J Clin Nutr 2006;83(6):1265–71. http://ajcn.nutrition.org/content/83/6/1265.abstract?ijkey=57ef21c4177b8442f40b357ae0266deeec20c77e
- Karppi J, Laukkanen JA, Makikallio TH, Ronkainen K, Kurl S. Low beta-carotene concentrations increase the risk of cardiovascular disease mortality among Finnish men with risk factors. Nutr Metab Cardiovasc Dis 2012;22:921–8. https://www.ncbi.nlm.nih.gov/pubmed/22494809?dopt=Abstract
- Progress in Retinal and Eye Research Volume 31, Issue 4, July 2012, Pages 303-315. Lutein: More than just a filter for blue light. http://www.sciencedirect.com/science/article/pii/S135094621200016X
- Lutein and zeaxanthin supplementation reduces H2O2-induced oxidative damage in human lens epithelial cells. Gao S, Qin T, Liu Z, Caceres MA, Ronchi CF, Chen CY, Yeum KJ, Taylor A, Blumberg JB, Liu Y, Shang F. Mol Vis. 2011; 17():3180-90. https://www.ncbi.nlm.nih.gov/pubmed/22194644/
- Difference in phototoxicity of cyclodextrin complexed fullerene [(gamma-CyD)2/C60] and its aggregated derivatives toward human lens epithelial cells. Zhao B, He YY, Chignell CF, Yin JJ, Andley U, Roberts JE. Chem Res Toxicol. 2009 Apr; 22(4):660-7. https://www.ncbi.nlm.nih.gov/pubmed/19281132/
- Ascherio A, Rimm EB, Hernan MA, Giovannucci E, Kawachi I, Stampfer MJ, Willett WC. Relation of consumption of vitamin E, vitamin C, and carotenoids to risk for stroke among men in the United States. Ann Intern Med 1999;130:963–70. https://www.ncbi.nlm.nih.gov/pubmed/10383366?dopt=Abstract
- Hak AE, Ma J, Powell CB, Campos H, Gaziano JM, Willett WC, Stampfer MJ. Prospective study of plasma carotenoids and tocopherols in relation to risk of ischemic stroke. Stroke 2004;35:1584–8. http://stroke.ahajournals.org/content/35/7/1584
- Hirvonen T, Virtamo J, Korhonen P, Albanes D, Pietinen P. Intake of flavonoids, carotenoids, vitamins C and E, and risk of stroke in male smokers. Stroke 2000;31:2301–6. http://stroke.ahajournals.org/content/31/10/2301
- Bates CJ, Hamer M, Mishra GD. Redox-modulatory vitamins and minerals that prospectively predict mortality in older British people: the National Diet and Nutrition Survey of people aged 65 years and over. Br J Nutr 2011;105:123–32. https://www.ncbi.nlm.nih.gov/pubmed/20807458?dopt=Abstract
- Buijsse B, Feskens EJM, Kwape L, Kok FJ, Kromhout D. Both (alpha)- and (beta)-carotene, but not tocopherols and vitamin C, are inversely related to 15-year cardiovascular mortality in Dutch elderly men. J Nutr 2008;138:344–50. http://jn.nutrition.org/content/138/2/344.full
- Ito Y, Suzuki K, Ishii J, Hishida H, Tamakoshi A, Hamajima N, Aoki K. A population-based follow-up study on mortality from cancer or cardiovascular disease and serum carotenoids, retinol and tocopherols in Japanese inhabitants. Asian Pac J Cancer Prev 2006;7:533–46. https://www.ncbi.nlm.nih.gov/pubmed/17250424?dopt=Abstract
- Mayne ST, Cartmel B, Lin HQ, Zhang TZ, Goodwin WJ. Low plasma lycopene concentration is associated with increased mortality in a cohort of patients with prior oral, pharynx or larynx cancers. J Am Coll Nutr 2004;23:34–42. https://www.ncbi.nlm.nih.gov/pubmed/14963051?dopt=Abstract
- Shardell MD, Alley DE, Hicks GE, El-Kamary SS, Miller RR, Semba RD, Ferrucci L. Low-serum carotenoid concentrations and carotenoid interactions predict mortality in US adults: the Third National Health and Nutrition Examination Survey. Nutr Res 2011;31:178–89. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3081783/
- Sesso HD, Buring JE, Norkus EP, Gaziano JM. Plasma lycopene, other carotenoids, and retinol and the risk of cardiovascular disease in women. Am J Clin Nutr 2004;79:47–53. http://ajcn.nutrition.org/content/79/1/47.full
- Sesso HD, Buring JE, Norkus EP, Gaziano JM. Plasma lycopene, other carotenoids, and retinol and the risk of cardiovascular disease in men. Am J Clin Nutr 2005;81:990–7. http://ajcn.nutrition.org/content/81/5/990.full
- Hozawa A, Jacobs DR, Steffes MW, Gross MD, Steffen LM, Lee DH. Associations of serum carotenoid concentrations with the development of diabetes and with insulin concentration: interaction with smoking – The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Am J Epidemiol 2006;163:929–37.
- Kataja-Tuomola MK, Kontto JP, Mannisto S, Albanes D, Virtamo J. Intake of antioxidants and risk of type 2 diabetes in a cohort of male smokers. Eur J Clin Nutr 2011;65:590–7. https://www.ncbi.nlm.nih.gov/pubmed/21245884?dopt=Abstract
- Montonen J, Knekt P, Jarvinen R, Reunanen A. Dietary antioxidant intake and risk of type 2 diabetes. Diabetes Care 2004;27:362–6. http://care.diabetesjournals.org/content/27/2/362
- Wang L, Liu SM, Pradhan AD, Manson JE, Buring JE, Gaziano JM, Sesso HD. Plasma lycopene, other carotenoids, and the risk of type 2 diabetes in women. Am J Epidemiol 2006;164:576–85.
- Application of Lutein and Zeaxanthin in nonproliferative diabetic retinopathy. Hu BJ, Hu YN, Lin S, Ma WJ, Li XR. Int J Ophthalmol. 2011; 4(3):303-6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3340817/
- Beydoun MA, Canas JA, Beydoun HA, Chen XL, Shroff MR, Zonderman AB. Serum antioxidant concentrations and metabolic syndrome are associated among US adolescents in recent national surveys. J Nutr 2012;142:1693–704. http://jn.nutrition.org/content/142/9/1693.full
- Beydoun MA, Shroff MR, Chen X, Beydoun HA, Wang Y, Zonderman AB. Serum antioxidant status is associated with metabolic syndrome among U.S. adults in recent national surveys. J Nutr 2011;141:903–13. http://jn.nutrition.org/content/141/5/903.full
- Coyne T, Ibiebele TI, Baade PD, McClintock CS, Shaw JE. Metabolic syndrome and serum carotenoids: findings of a cross-sectional study in Queensland, Australia. Br J Nutr 2009;102:1668–77. https://www.ncbi.nlm.nih.gov/pubmed/19631019?dopt=Abstract
- Sluijs I, Beulens JWJ, Grobbee DE, van der Schouw YT. Dietary carotenoid intake is associated with lower prevalence of metabolic syndrome in middle-aged and elderly men. J Nutr 2009;139:987–92. http://jn.nutrition.org/content/139/5/987.full
- Sugiura M, Nakamura M, Ogawa K, Ikoma Y, Matsumoto H, Ando F, Shimokata H, Yano M. Associations of serum carotenoid concentrations with the metabolic syndrome: interaction with smoking. Br J Nutr 2008;100:1297–306. https://www.ncbi.nlm.nih.gov/pubmed/18445303?dopt=Abstract
- Suzuki K, Ito Y, Inoue T, Hamajima N. Inverse association of serum carotenoids with prevalence of metabolic syndrome among Japanese. Clin Nutr 2011;30:369–75. https://www.ncbi.nlm.nih.gov/pubmed/21216053?dopt=Abstract
- Perry A., Rasmussen H., Johnson E.J. Xanthophyll (lutein, zeaxanthin) content of fruits, vegetables and corn and egg products. J. Food Comp. Anal. 2009;22:9–15. doi: 10.1016/j.jfca.2008.07.006.
- Distribution of lutein, zeaxanthin, and related geometrical isomers in fruit, vegetables, wheat, and pasta products. Humphries JM, Khachik F. J Agric Food Chem. 2003 Feb 26; 51(5):1322-7. https://www.ncbi.nlm.nih.gov/pubmed/12590476/
- Lutein and zeaxanthin concentrations in plasma after dietary supplementation with egg yolk. Handelman GJ, Nightingale ZD, Lichtenstein AH, Schaefer EJ, Blumberg JB. Am J Clin Nutr. 1999 Aug; 70(2):247-51. https://www.ncbi.nlm.nih.gov/pubmed/10426702/
- Chandrika U.G., Jansz E.R., Wickranasinghe S.M.D.N., Warnasuriya N.D. Carotenoids in yellow and red-fleshed papaya (Carcia papaya L) J. Sci. Food Agric. 2003;83:1279–1282. doi: 10.1002/jsfa.1533.
- United States Department of Agriculture. USDA Nutritional database for standard reference release.
- Phytochemicals and antioxidant activity of milled fractions of different wheat varieties. Adom KK, Sorrells ME, Liu RH. J Agric Food Chem. 2005 Mar 23; 53(6):2297-306. https://www.ncbi.nlm.nih.gov/pubmed/15769171/
- Identification and quantification of seed carotenoids in selected wheat species. Abdel-Aal el-SM, Young JC, Rabalski I, Hucl P, Fregeau-Reid J. J Agric Food Chem. 2007 Feb 7; 55(3):787-94. https://www.ncbi.nlm.nih.gov/pubmed/17263475/
- Analysis of xanthophylls in corn by HPLC. Moros EE, Darnoko D, Cheryan M, Perkins EG, Jerrell J. J Agric Food Chem. 2002 Oct 9; 50(21):5787-90. https://www.ncbi.nlm.nih.gov/pubmed/12358439/
- Abdel-Aal E-SM, Akhtar H, Zaheer K, Ali R. Dietary Sources of Lutein and Zeaxanthin Carotenoids and Their Role in Eye Health. Nutrients. 2013;5(4):1169-1185. doi:10.3390/nu5041169. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3705341/
- U.S. Food and Drug Administration. Lutein. https://www.fda.gov/downloads/food/ingredientspackaginglabeling/gras/noticeinventory/ucm439151.pdf
- U.S. Food and Drug Administration. Zeaxanthin. https://www.fda.gov/downloads/food/ingredientspackaginglabeling/gras/noticeinventory/ucm514709.pdf
- EFSA Panel on Food Additives and Nutrient Sources added to Food. Scientific Opinion on the re-evaluation of lutein preparations other than lutein with high concentrations of total saponified carotenoids at levels of at least 80% EFSA Journal. 2011;9:2144.
- Agostoni C, Bresson J, Fairweather-Tait S, Flynn A, Golly I, Korhonen H, Lagiou P, Løvik M, Marchelli R, Martin A. Scientific Opinion on the substantiation of health claims related to lutein and protection of DNA, proteins and lipids from oxidative damage (ID 3427), protection of the skin from UV-induced (including photo-oxidative) damage (ID 1605, 1779) and maintenance of normal vision (ID 1779, 2080) pursuant to Article 13 (1) of Regulation (EC) No 1924/2006. EFSA journal. 2011;9:2030–2030.
- Agostoni C, Bresson J, Fairweather-Tait S, Flynn A, Golly I, Korhonen H, Lagiou P, Løvik M, Marchelli R, Martin A, Moseley B, Neuhäuser-Berthold M, Przyrembel H, Salminen S, Sanz Y, Strain S, Strobel S, Tetens I, Tome D, van Loveren H, Verhagen H. Scientific Opinion on the substantiation of health claims related to lutein and maintenance of normal vision (ID 1603, 1604, further assessment) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA Journal. 2012;10.
- Agostoni C, Bresson J, Fairweather-Tait S, Flynn A, Golly I, Korhonen H, Lagiou P, Løvik M, Marchelli R, Martin A, Moseley B, Neuhäuser-Berthold M, Przyrembel H, Salminen S, Sanz Y, Strain S, Strobel S, Tetens I, Tome D, van Loveren H, Verhagen H. Scientific Opinion on the substantiation of health claims related to lutein and maintenance of normal vision (ID 1603, 1604, further assessment) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA Journal. 2012;10
- European FoodSafetyAuthority. Technical specifications on the harmonised monitoring and reporting of antimicrobial resistance in methicillin-resistant Staphylococcus aureus in food-producing animals and food. EFSA Journal. 2012;10:2897.
- An innovative approach to the determination of safety for a dietary ingredient derived from a new source: case study using a crystalline lutein product. Kruger CL, Murphy M, DeFreitas Z, Pfannkuch F, Heimbach J. Food Chem Toxicol. 2002 Nov; 40(11):1535-49. https://www.ncbi.nlm.nih.gov/pubmed/12176081/
- Effects of lutein and zeaxanthin on aspects of eye health. Ma L, Lin XM. J Sci Food Agric. 2010 Jan 15; 90(1):2-12. https://www.ncbi.nlm.nih.gov/pubmed/20355006/
- Safety assessment of lutein and zeaxanthin (Lutemax 2020): subchronic toxicity and mutagenicity studies. Ravikrishnan R, Rusia S, Ilamurugan G, Salunkhe U, Deshpande J, Shankaranarayanan J, Shankaranarayana ML, Soni MG. Food Chem Toxicol. 2011 Nov; 49(11):2841-8. https://www.ncbi.nlm.nih.gov/pubmed/21872637/
- What is meso-zeaxanthin, and where does it come from? Nolan JM, Meagher K, Kashani S, Beatty S. Eye (Lond). 2013 Aug; 27(8):899-905. https://www.ncbi.nlm.nih.gov/pubmed/23703634/
- Xu X, Zhang L, Shao B, Sun X, Ho CT, Li S. Safety evaluation of meso-zeaxanthin. Food Control. 2013;32:678–686.
- WebMD. LUTEIN. http://www.webmd.com/vitamins-supplements/ingredientmono-754-lutein.aspx?activeIngredientId=754&activeIngredientName=lutein
- Ma L, Liu R, Du JH, Liu T, Wu SS, Liu XH. Lutein, Zeaxanthin and Meso-zeaxanthin Supplementation Associated with Macular Pigment Optical Density. Nutrients. 2016;8(7):426. doi:10.3390/nu8070426. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4963902/
- Wang X, Jiang C, Zhang Y, Gong Y, Chen X, Zhang M, Role of Lutein Supplementation in the Management of Age-Related Macular Degeneration: Meta-Analysis of Randomized Controlled Trials. Ophthalmic Res 2014;52:198-205. https://www.karger.com/Article/Abstract/363327





{kind=link}