What are white blood cells
White blood cells, also called leukocytes (or leucocytes), are the cells of the immune system that are involved in protecting the body against both infectious disease and foreign invaders 1. All white blood cells are produced and derived from multipotent cells in the bone marrow known as hematopoietic stem cells. Leukocytes are found throughout the body, including the blood and lymphatic system.
Most blood samples are about 45% red blood cells by volume, with the white blood cells and platelets accounting for less than 1% of blood volume. The remaining blood sample, about 55%, is the plasma, a clear, straw-colored liquid (see Figure 1). Blood transports leukocytes to sites of infection. Leukocytes may then leave the bloodstream.
Like red blood cells, white blood cells (leukocytes) have limited life spans, so they must constantly be replaced. Leukocytes develop from hematopoietic stem cells in the red bone marrow (see Figure 2) in response to hormones, much as red blood cells form from precursors upon stimulation from erythropoietin. The hormones that affect leukocyte development fall into two groups—interleukins and colony-stimulating factors (CSFs). Interleukins are numbered, while most colony stimulating factors are named for the cell population they stimulate.
Types of white blood cells
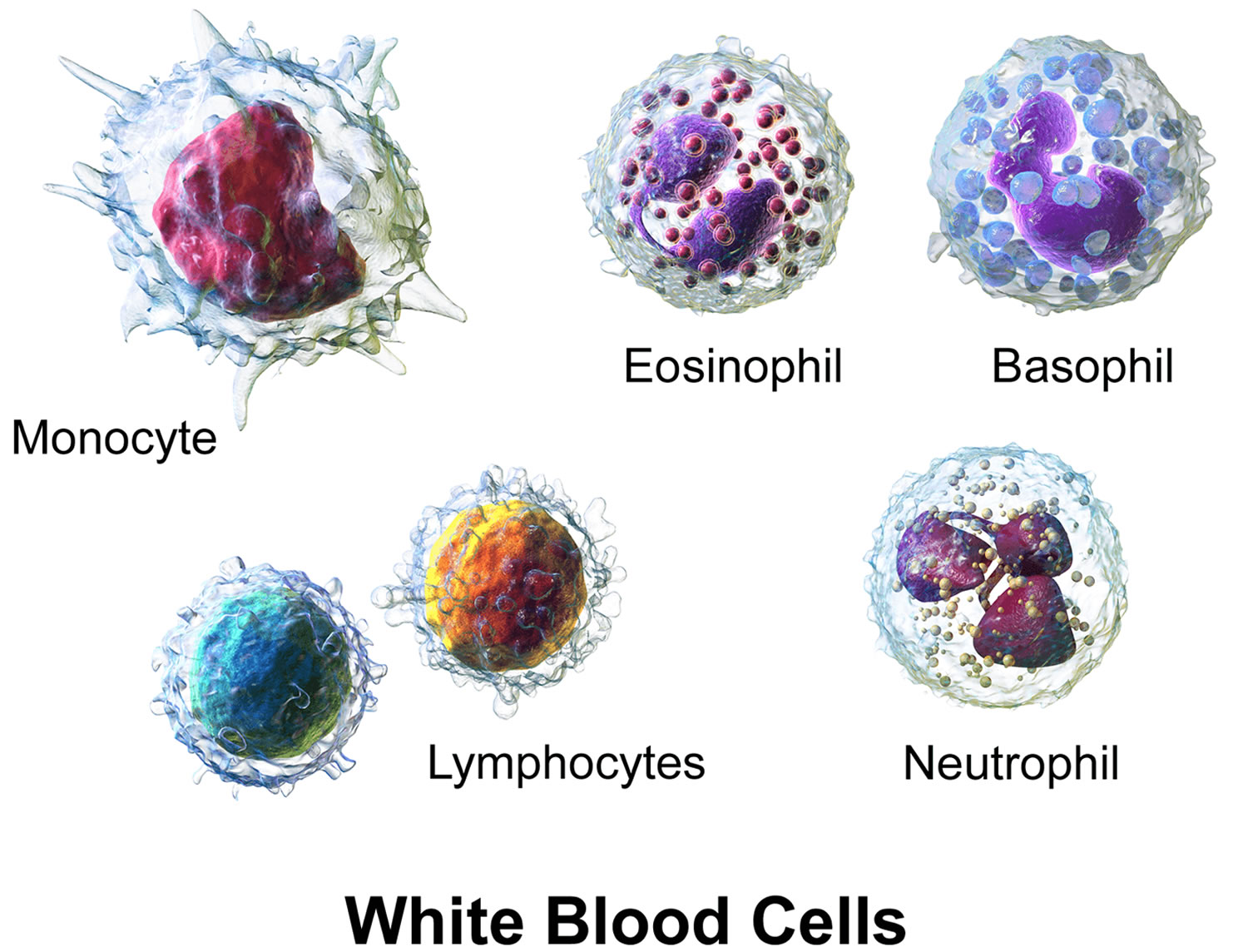
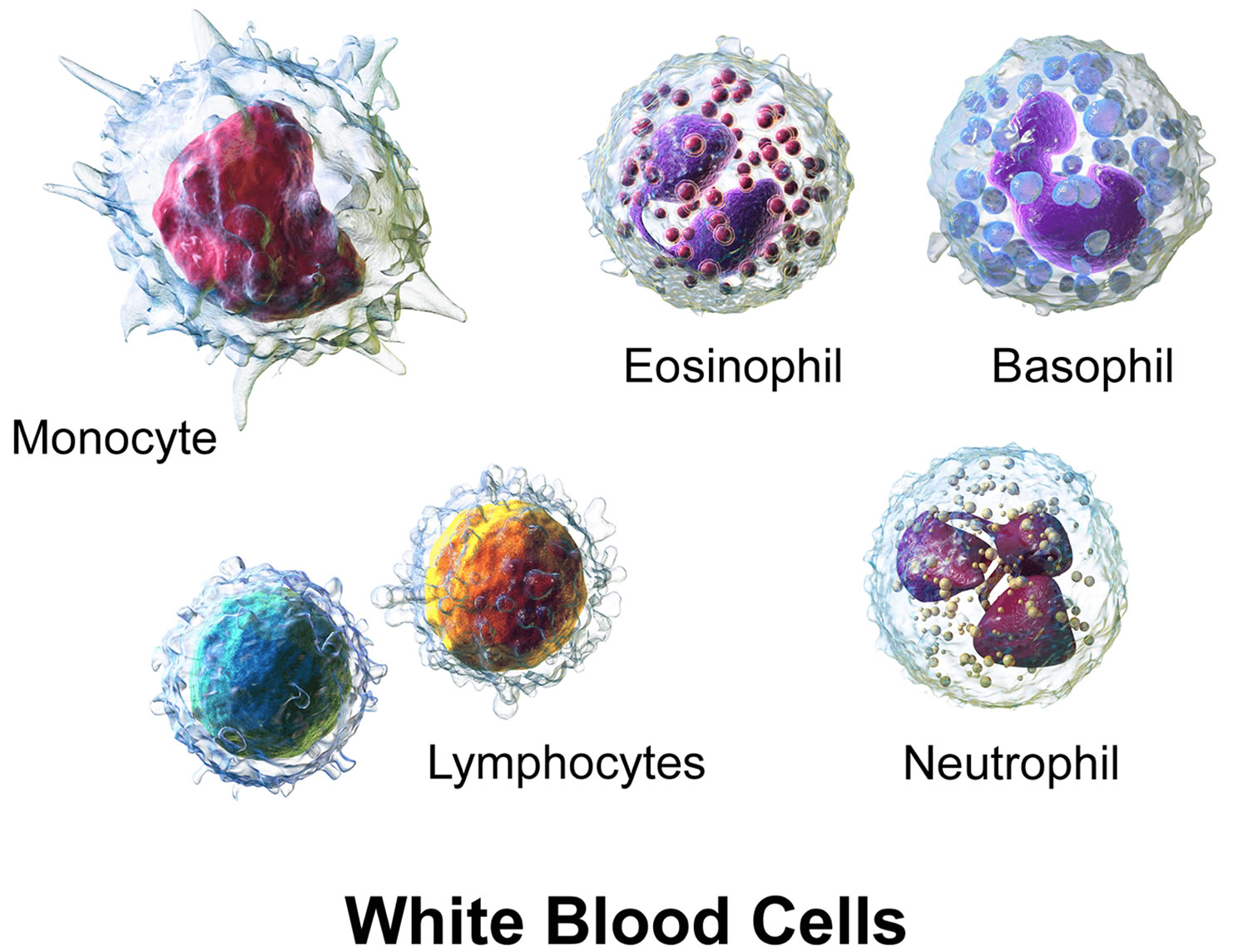
All white blood cells have nuclei, which distinguishes them from the other blood cells, the anucleated red blood cells and platelets. They differ in size, the nature of their cytoplasm, the shape of the nucleus, and their staining characteristics, and they are named for these distinctions. Two pairs of broadest categories classify them either by structure (granulocytes or agranulocytes) or by cell division lineage (myeloid cells or lymphoid cells) (see Figure 3). These broadest categories can be further divided into the five main types: neutrophils, eosinophils, basophils, lymphocytes, and monocytes 2. These types are distinguished by their physical and functional characteristics. Monocytes and neutrophils are phagocytic. Further subtypes can be classified; for example, among lymphocytes, there are B cells, T cells, and NK (natural killer) cells.
Normally, five types of white blood cells are in circulating blood. For example, leukocytes with granular cytoplasm are called granulocytes, whereas those without cytoplasmic granules are called agranulocytes (see Figure. 3).
A typical granulocyte is about twice the size of a red blood cell. Members of this group include neutrophils, eosinophils, and basophils. Granulocytes develop in red bone marrow as do red blood cells, but they have short life spans, averaging about 12 hours.
Neutrophils have fine cytoplasmic granules that appear light purple in neutral stain. The nucleus of an older neutrophil is lobed and consists of two to five sections (segments, so these cells are sometimes called segs) connected by thin strands of chromatin (Figure 4). Younger neutrophils are also called bands because their nuclei are C-shaped. Neutrophils account for 54% to 62% of the leukocytes in a typical blood sample from an adult.
Eosinophils contain coarse, uniformly sized cytoplasmic granules that appear deep red in acid stain (Figure 4). The nucleus usually has only two lobes (termed
bilobed). Eosinophils make up 1% to 3% of the total number of circulating leukocytes.
Basophils are similar to eosinophils in size and in the shape of their nuclei, but they have fewer, more irregularly shaped cytoplasmic granules that appear deep
blue in basic stain (Figure 4). Basophils usually account for less than 1% of the circulating leukocytes.
The leukocytes of the agranulocyte group include monocytes and lymphocytes. Monocytes generally arise from red bone marrow. Lymphocytes are formed in the organs of the lymphatic system, as well as in the red bone marrow.
Monocytes, the largest blood cells, are two to three times greater in diameter than red blood cells. Their nuclei are round, kidney-shaped, oval, or lobed. They usually make up 3% to 9% of the leukocytes in a blood sample and live for several weeks or even months.
Lymphocytes are only slightly larger than red blood cells. A typical lymphocyte has a large, round nucleus surrounded by a thin rim of cytoplasm. These cells account for 25% to 33% of circulating leukocytes. Lymphocytes may live for years.
Figure 1. Blood composition
Note: Blood is a complex mixture of formed elements in a liquid extracellular matrix, called blood plasma. Note that water and proteins account for 99% of the blood plasma.


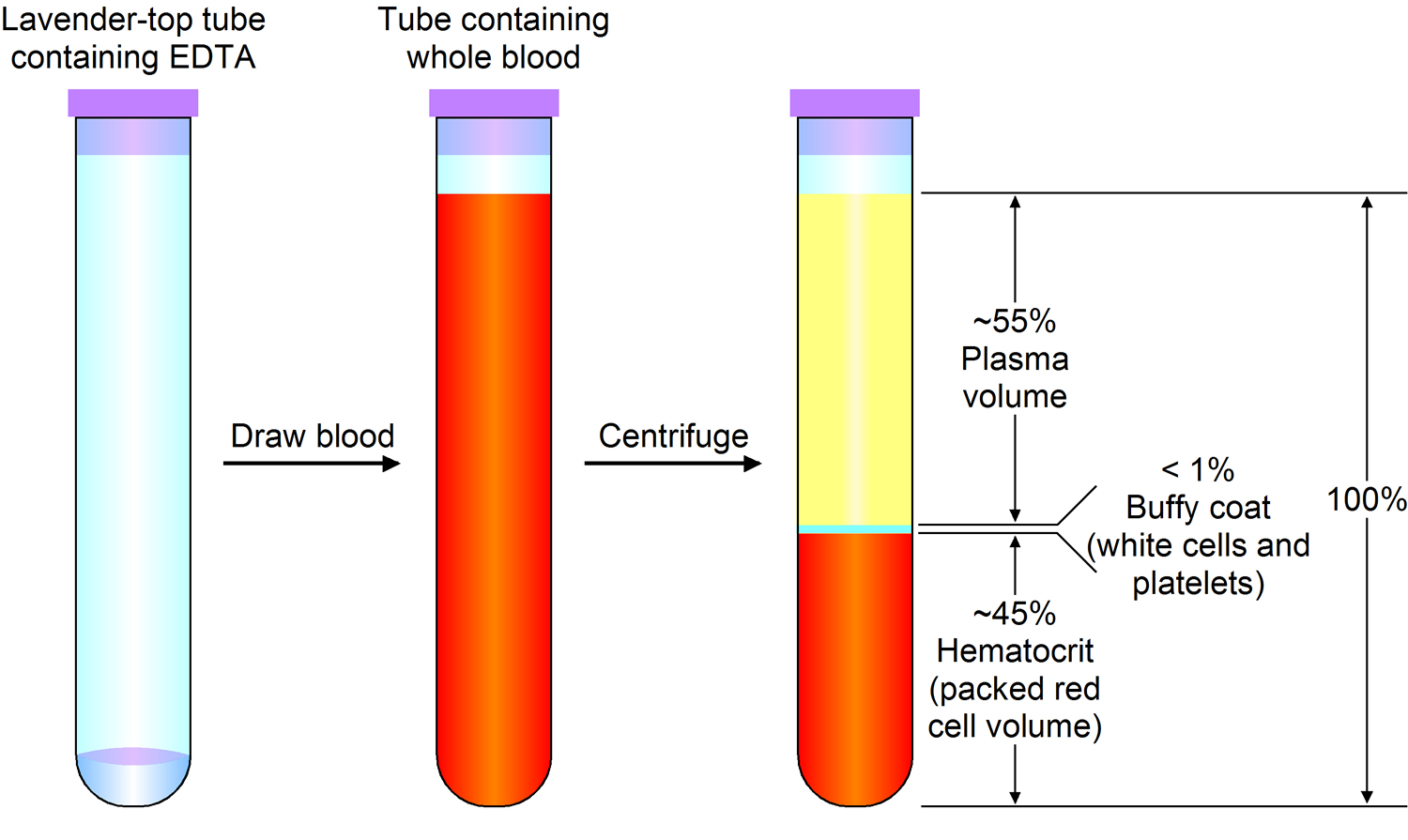
Note: Blood consists of a liquid portion called plasma and a solid portion (the formed elements) that includes red blood cells, white blood cells, and platelets. When blood components are separated by centrifugation, the white blood cells and platelets form a thin layer, called the “buffy coat,” between the plasma and the red blood cells, which accounts for about 1% of the total blood volume. Blood cells and platelets can be seen under a light microscope when a blood sample is smeared onto a glass slide.
Normal Leukocyte Life Cycle and Responses
The life cycle of leukocytes includes development and differentiation, storage in the bone marrow, margination within the vascular spaces, and migration to tissues. Stem cells in the bone marrow produce cell lines of erythroblasts, which become red blood cells; megakaryoblasts, which become platelets; lymphoblasts; and myeloblasts. Lymphoblasts develop into various types of T and B cell lymphocytes. Myeloblasts further differentiate into monocytes and granulocytes, a designation that includes neutrophils, basophils, and eosinophils (Figure 2 and 3). Once white blood cells have matured within the bone marrow, 80% to 90% remain in storage in the bone marrow. This large reserve allows for a rapid increase in the circulating white blood cell count within hours. A relatively small pool (2% to 3%) of leukocytes circulate freely in the peripheral blood 3; the rest stay deposited along the margins of blood vessel walls or in the spleen. Leukocytes spend most of their life span in storage. Once a leukocyte is released into circulation and peripheral tissues, its life span ranges from two to 16 days, depending on the type of cell.
Figure 2. Bone marrow anatomy

Anatomy of the bone. The bone is made up of compact bone, spongy bone, and bone marrow. Compact bone makes up the outer layer of the bone. Spongy bone is found mostly at the ends of bones and contains red marrow. Bone marrow is found in the center of most bones and has many blood vessels. There are two types of bone marrow: red and yellow. Red marrow contains blood stem cells that can become red blood cells, white blood cells, or platelets. Yellow marrow is made mostly of fat.
Figure 3. White blood cells development. A blood stem cell goes through several steps to become a red blood cell, platelet, or white blood cell

Figure 4. White blood cells development
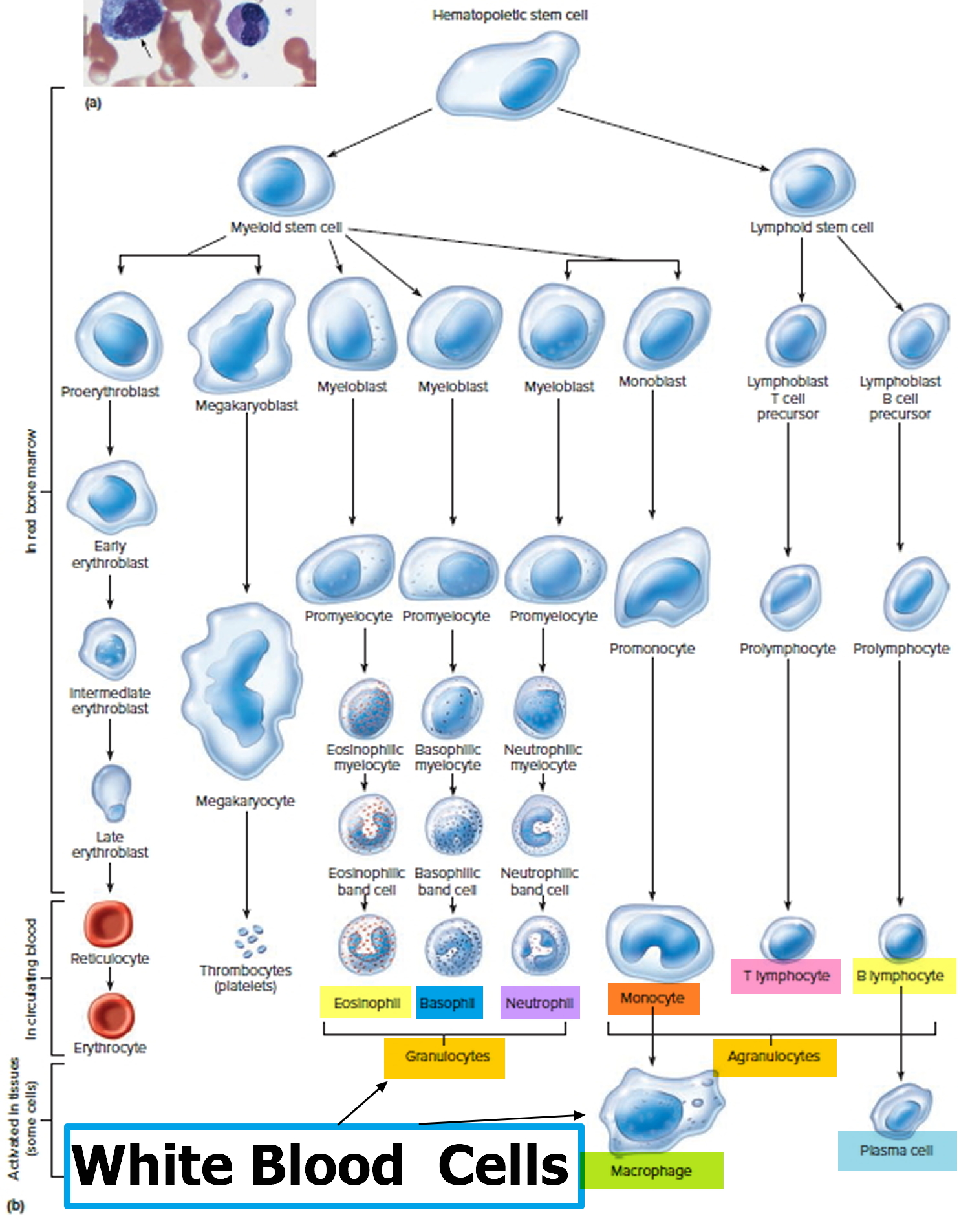
Figure 5. White blood cells
White Blood Cell Counts
The number of leukocytes in a microliter of human blood, called the white blood cell count (WBCC or WCC), normally is 3,500 to 10,500 per mm3 (3.5 to 10.5 × 109 per L). White blood cell counts are of clinical interest because their number may change in response to abnormal conditions. A total number of white blood cells exceeding 10,500 per mm3 (10.5 × 109 per L) of blood constitutes leukocytosis, indicating acute infection, such as appendicitis. The white blood cell count is greatly elevated in leukemia.
A total white blood cell count below 3,500 per mm3 (<3.5 × 109 per L) of blood is called leukopenia. Such a deficiency may accompany typhoid fever, influenza, measles, mumps, chickenpox, AIDS, or poliomyelitis.
Healthy newborn infants may have a white blood cell count from 13,000 to 38,000 per mm3 (13.0 to 38.0 × 109 per L) at 12 hours of life. By two weeks of age, this decreases to approximately 5,000 to 20,000 per mm3 (5.0 to 20.0 × 109 per L), and gradually declines throughout childhood to reach adult levels of 4,500 to 11,000 per mm3 (4.5 to 11.0 × 109 per L) by about 21 years of age 4. There is also a shift from relative lymphocyte to neutrophil predominance from early childhood to the teenage years and adulthood 5. During pregnancy, there is a gradual increase in the normal white blood cell count (third trimester 95% upper limit = 13,200 per mm3 [13.2 × 109 per L] and 99% upper limit = 15,900 per mm3 [15.9 × 109 per L]), and a slight shift toward an increased percentage of neutrophils 6. In one study of afebrile postpartum patients, the mean white blood cell count was 12,620 per mm3 (12.62 × 109 per L) for women after vaginal deliveries and 12,710 per mm3 (12.71 × 109 per L) after cesarean deliveries. Of note, positive bacterial cultures were not associated with leukocytosis or neutrophilia, making leukocytosis an unreliable discriminator in deciding which postpartum patients require antibiotic therapy 7. Patients of black African descent tend to have a lower white blood cell count (by 1,000 per mm3 [1.0 × 109 per L]) and lower absolute neutrophil counts 8.
A differential white blood cell count lists percentages of the various types of leukocytes in a blood sample. This test is useful because the relative proportions of white blood cells may change in particular diseases. The number of neutrophils, for instance, usually increases during bacterial infections. Eosinophils may become more abundant during certain parasitic infections and allergic reactions. In AIDS, the number of a type of lymphocyte called T cells drops sharply.
Table 1. White Blood Cell Count Variation with Age and Pregnancy
| Patient characteristic | Normal total leukocyte count |
|---|---|
Newborn infant | 13,000 to 38,000 per mm3 (13.0 to 38.0 × 109 per L) |
Infant two weeks of age | 5,000 to 20,000 per mm3 (5.0 to 20.0 × 109 per L) |
Adult | 4,500 to 11,000 per mm3 (4.5 to 11.0 × 109 per L) |
Pregnant female (third trimester) | 5,800 to 13,200 per mm3 (5.8 to 13.2 × 109 per L) |
Differentiation by Type of White Blood Cell
Changes in the normal distribution of types of white blood cells can indicate specific causes of leukocytosis 9. Although the differential of the major types of white blood cells is important for evaluating the cause of leukocytosis, it is sometimes helpful to think in terms of absolute, rather than relative, leukopenias and leukocytoses. To calculate the absolute cell count, the total leukocyte count is multiplied by the differential percentage. For example, with a normal white blood cell count of 10,000 per mm3 (10.0 × 109 per L) and an elevated monocyte percentage of 12, the absolute monocyte count is 12% or 0.12 times the white blood cell count of 10,000 per mm3, yielding 1,200 per mm3 (1.2 × 109 per L), which is abnormally elevated.
Table 2. Normal White Blood Cell Distribution
| White blood cell line | Normal percentage of total leukocyte count |
|---|---|
Neutrophils | 40 to 60 |
Lymphocytes | 20 to 40 |
Monocytes | 2 to 8 |
Eosinophils | 1 to 4 |
Basophils | 0.5 to 1 |
Functions of White Blood Cells
White blood cells protect your body against infection in various ways. Some leukocytes phagocytize (engulfing and destroying bacteria and other foreign material) bacterial cells in the body, and others produce proteins (antibodies) that destroy or disable foreign particles.
Leukocytes can squeeze between the cells that form the walls of the smallest blood vessels. This movement, called diapedesis, allows the white blood cells to leave the circulation. Once outside the blood, they move through interstitial spaces using a form of self propulsion called amoeboid motion.
The most mobile and active phagocytic leukocytes are neutrophils and monocytes. Monocytes leave the bloodstream and specialize further to become macrophages that phagocytize bacteria, dead cells, and other debris in the tissues.
Neutrophils cannot ingest particles much larger than bacterial cells, but monocytes can engulf large objects. Both of these phagocytes contain many lysosomes, which are organelles filled with digestive enzymes that break down organic molecules in captured bacteria, nutrients, and wornout organelles. Neutrophils and monocytes may become so engorged with digestive products and bacterial toxins that they die.
Eosinophils are only weakly phagocytic, but they are attracted to and can kill certain parasites. Eosinophils also help control inflammation and allergic reactions by removing biochemicals associated with these reactions.
Basophils migrate to damaged tissues, where they release heparin, which inhibits blood clotting, and histamine, which promotes inflammation. Basophils also play major roles in certain allergic reactions.
Lymphocytes are important in immunity. Lymphocytes called B cells, for example, produce antibodies that attack specific foreign substances that enter the body.
Phagocytosis
Phagocytosis removes foreign particles from the lymph as it moves from the interstitial spaces to the bloodstream. Phagocytes in the blood vessels and in the tissues of the spleen, liver, or bone marrow remove particles that reach the blood. The blood’s most active phagocytic cells are neutrophils and monocytes. Chemicals released from injured tissues attract these cells by chemotaxis. Neutrophils engulf and digest smaller particles; monocytes phagocytize larger ones.
Monocytes that leave the bloodstream by diapedesis become macrophages. These large cells may be free, or fixed in various tissues. The fixed macrophages can divide and produce new macrophages. Neutrophils, monocytes and macrophages constitute the mononuclear phagocytic system (reticuloendothelial system).
Table 3. White blood cells types and functions
| Type | Approx. % in adults | Diameter (μm) | Main targets | Nucleus | Granules | Lifetime |
|---|---|---|---|---|---|---|
| Neutrophil | 62% | 10–12 |
| Multilobed | Fine, faintly pink (H&E stain) | 6 hours–few days (days in spleen and other tissue) |
| Eosinophil | 2.3% | 10–12 |
| Bi-lobed | Full of pink-orange (H&E stain) | 8–12 days (circulate for 4–5 hours) |
| Basophil | 0.4% | 12–15 |
| Bi-lobed or tri-lobed | Large blue | A few hours to a few days |
| Lymphocyte | 30% | Small lymphocytes 7–8 Large lymphocytes 12–15 |
| Deeply staining, eccentric | NK-cells and cytotoxic (CD8+) T-cells | Years for memory cells, weeks for all else. |
| Monocyte | 5.3% | 15–30 | Monocytes migrate from the bloodstream to other tissues and differentiate into tissue resident macrophages, Kupffer cells in the liver. | Kidney shaped | None | Hours to days |
Lymphatic tissue contains lymphocytes, macrophages, and other cells.
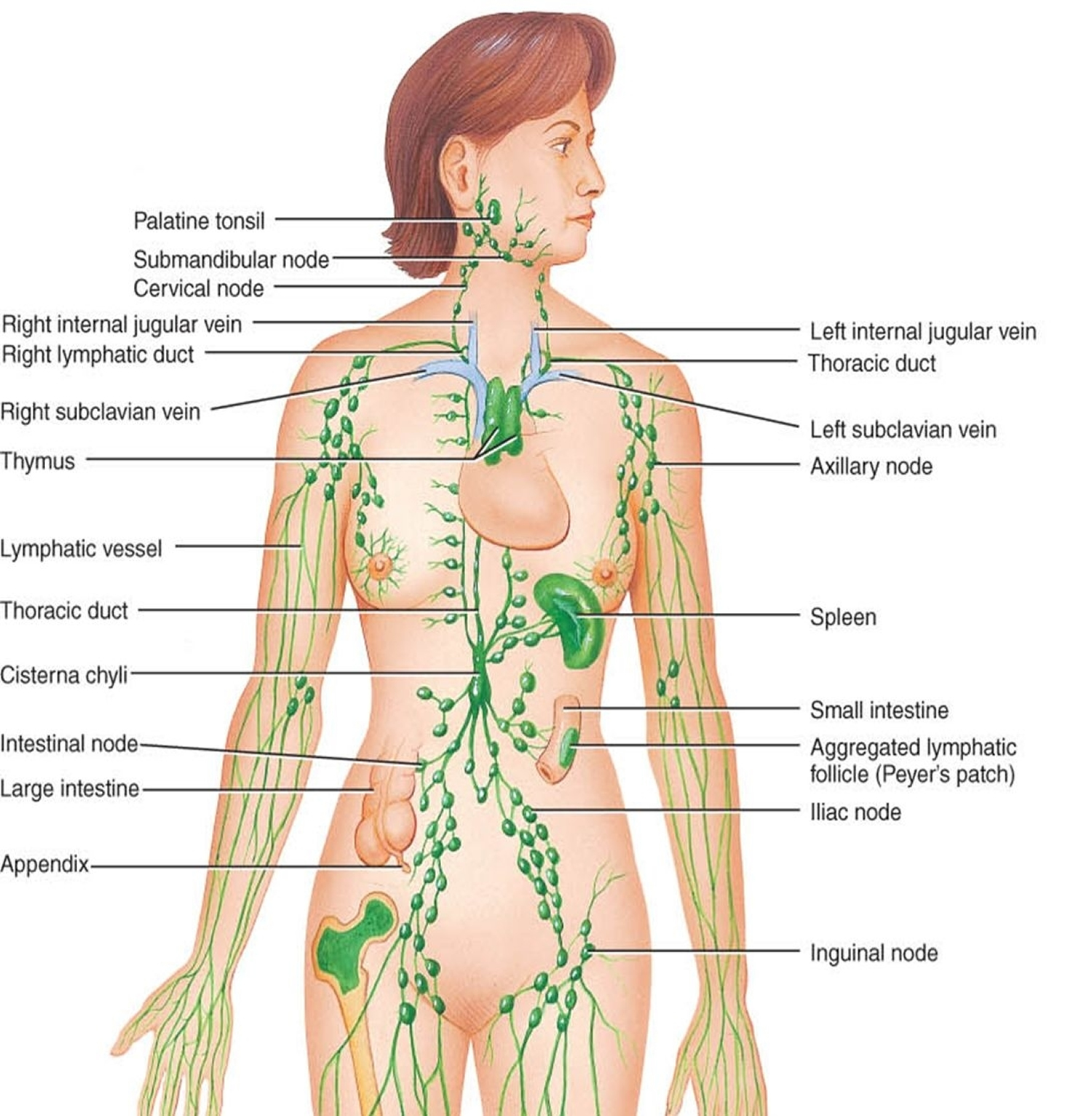
The unencapsulated diffuse lymphatic tissue associated with the digestive, respiratory, urinary, and reproductive tracts is called the mucosa-associated lymphoid tissue (MALT). Compact masses of lymphatic tissue compose the tonsils and appendix. Mucosa-associated lymphoid tissue (MALT) aggregates of lymphatic tissue, called Peyer’s patches, are scattered throughout the mucosal lining of the distal portion of the small intestine. The lymphatic organs, including the lymph nodes, thymus, and spleen, are encapsulated lymphatic tissue. A capsule of connective tissue with many fibers encloses each organ.
Lymph Nodes
Lymph nodes contain large numbers of lymphocytes (B cells and T cells) and macrophages that fight invading microorganisms. Masses of B cells and macrophages in the cortex are contained within lymphatic nodules, also called lymphatic follicles, the functional units of the lymph node. The spaces within a node, called lymphatic sinuses, provide a complex network of chambers and channels through which lymph circulates.
Lymph nodes are generally in groups or chains along the paths of the larger lymphatic vessels throughout the body, but are absent in the central nervous system. Figure 5 shows the major locations of lymph nodes.
Lymph nodes have two primary functions: (1) filtering potentially harmful particles from lymph before returning it to the bloodstream, and (2) monitoring body fluids (immune surveillance), a function performed by lymphocytes and macrophages. Along with red bone marrow, the lymph nodes are centers for lymphocyte production. Lymphocytes attack viruses, bacteria, and other parasitic cells that are brought to the lymph nodes by lymph in the lymphatic vessels. Macrophages in the lymph nodes engulf and destroy foreign substances, damaged cells, and cellular debris.
Superficial lymphatic vessels inflamed by bacterial infection appear as red streaks beneath the skin, a condition called lymphangitis. Inflammation of the lymph nodes, called lymphadenitis, often follows. In lymphadenopathy, affected lymph nodes enlarge and may be quite painful.
Figure 5. Locations of major lymph nodes
Thymus
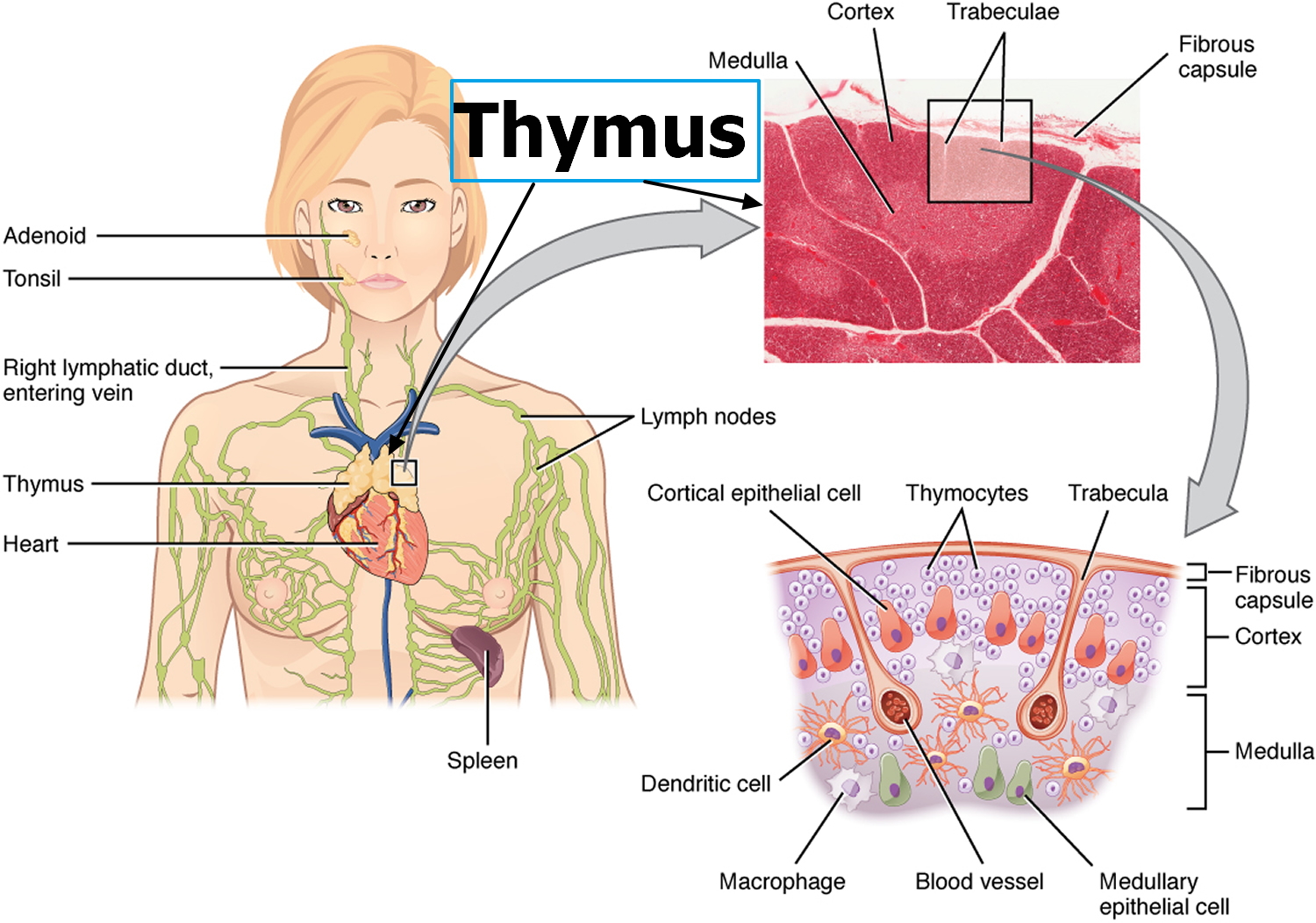
The thymus is a soft, bilobed gland enclosed in a connective tissue capsule and located anterior to the aorta. It is posterior to the upper part of the sternum. The
thymus is usually proportionately larger during infancy and early childhood, but shrinks after puberty and may be quite small in an adult. In elderly people, adipose and connective tissues replace lymphatic tissue in the thymus. In a person aged seventy, the thymus is one-tenth the size it was in that person at the age of ten.
Connective tissues extend inward from the surface of the thymus, subdividing it into lobules. The lobules house many lymphocytes. Most of these cells (thymocytes) are inactive; however, some mature into T lymphocytes (T cells), which leave the thymus and provide immunity. Epithelial cells in the thymus secrete hormones called thymosins, which stimulate maturation of T lymphocytes.
Figure 6. Thymus
Spleen
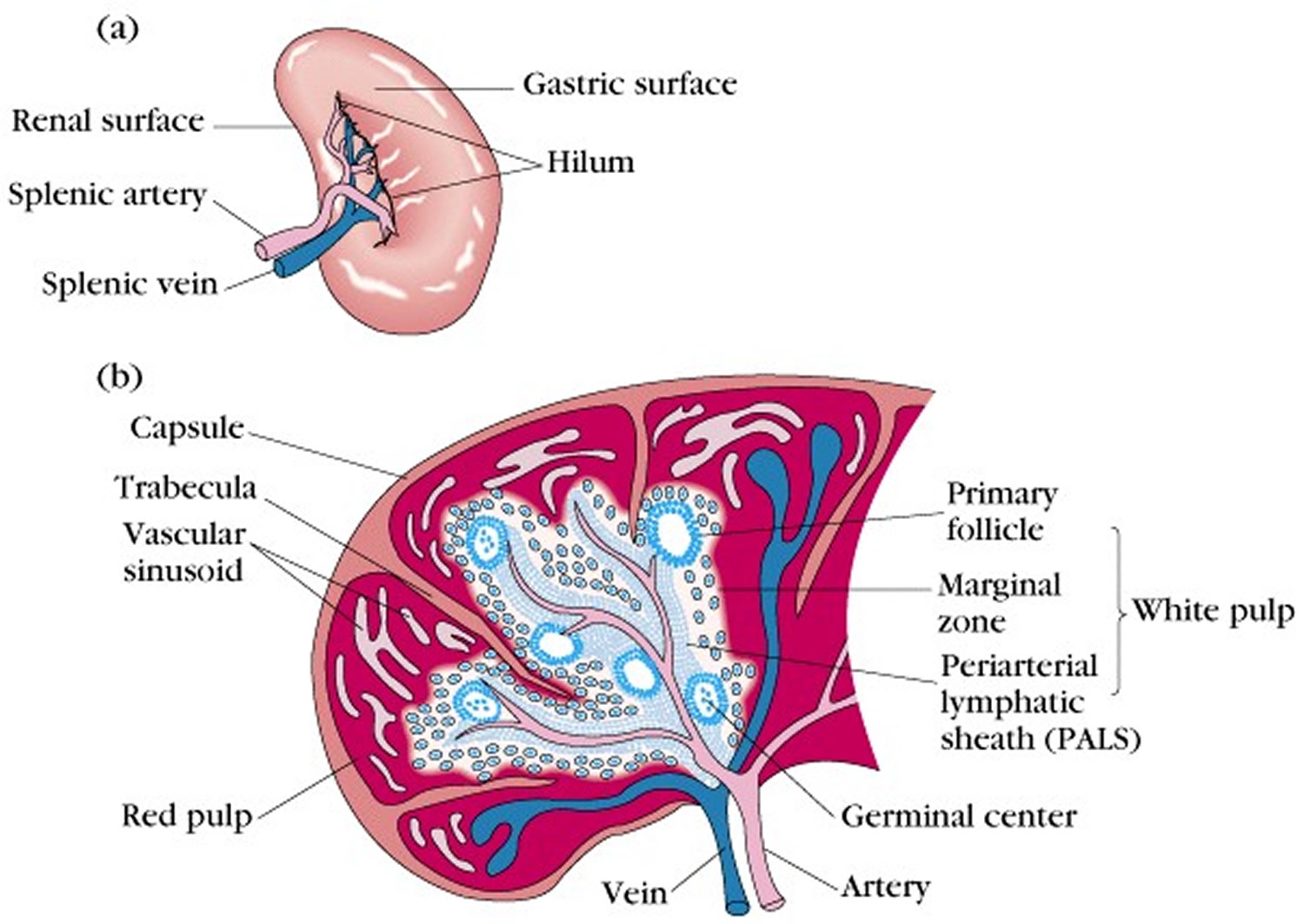
The spleen, the largest lymphatic organ, is in the upper left portion of the abdominal cavity, just inferior to the diaphragm. It is posterior and lateral to the stomach. The spleen resembles a large lymph node and is subdivided into lobules. However, unlike the lymphatic sinuses of a lymph node, the spaces in the spleen, called venous sinuses, are filled with blood instead of lymph.
The tissues within splenic lobules are of two types (Figure 7). The white pulp is distributed throughout the spleen in tiny islands. This tissue is composed of splenic nodules, which are similar to the lymphatic nodules in lymph nodes and are packed with lymphocytes. The red pulp, which fills the remaining spaces of the lobules, surrounds the venous sinuses. This pulp contains numerous red blood cells, which impart its color, plus many lymphocytes and macrophages.
Blood capillaries in the red pulp are quite permeable. Red blood cells can squeeze through the pores in these capillary walls and enter the venous sinuses. The older, more fragile red blood cells may rupture during this passage, and the resulting cellular debris is removed by phagocytic macrophages in the venous sinuses. These macrophages also engulf and destroy foreign particles, such as bacteria, that may be carried in the blood as it flows through the venous sinuses. Thus, the spleen filters blood much as the lymph nodes filter lymph.
Figure 7. The Spleen
Body Defenses Against Infection
The presence and multiplication of a disease-causing agent, or pathogen, which if unchecked may cause an infection. Pathogens include viruses, bacteria, fungi, and protozoans.
The human body can prevent the entry of pathogens or destroy them if they enter. Some mechanisms are general in that they protect against many types of pathogens, providing innate (nonspecific) defense. These mechanisms include species resistance, mechanical barriers, inflammation, chemical barriers (enzyme action, interferon, and complement), natural killer cells, phagocytosis, and fever.
Other defense mechanisms are very precise, targeting specific pathogens and providing adaptive (specific) defense, or immunity. Specialized lymphocytes that recognize foreign molecules (nonself antigens) in the body act against the foreign molecules in several ways, including the production of cytokines and antibodies. Innate and adaptive defense mechanisms work together to protect the body against infection. The innate defenses respond quite rapidly, while adaptive defenses develop more slowly.
Inflammation
Inflammation is a tissue response to injury or infection, producing localized redness, swelling, heat, and pain. The redness is a result of blood vessel dilation that increases blood flow and volume in the affected tissues. This effect, coupled with an increase in the permeability of nearby capillaries and subsequent leakage of protein-rich fluid into tissue spaces, swells tissues (edema). The heat comes as blood enters from deeper body parts, which are warmer than the surface. Pain results from stimulation of nearby pain receptors.
Infected cells release chemicals that attract white blood cells to sites of inflammation. Here the white blood cells phagocytize pathogens. Local heat speeds up phagocytic activity. In bacterial infections, the resulting mass of white blood cells, bacterial cells, and damaged tissue may form a thick fluid called pus.
Fluids that leak out of the capillaries, called exudates, also collect in inflamed tissues. These fluids contain fibrinogen and other blood-clotting factors. Clotting forms a network of fibrin threads in the affected region. Later, fibroblasts may arrive and secrete matrix components until the area is enclosed in a connective tissue sac. This walling off of the infected area helps inhibit the spread of pathogens and toxins to adjacent tissues.
Chemical Barriers
Lymphocytes and fibroblasts produce hormone like peptides called interferons in response to viruses or tumor cells. Once released from the virus-infected cell, interferon binds to receptors on uninfected cells, stimulating them to synthesize proteins that block replication of a variety of viruses. Thus, interferon’s effect is nonspecific. Interferons also stimulate phagocytosis and enhance the activity of other cells that help resist infections and the growth of tumors.
Complement is a group of proteins, in plasma and other body fluids, that interact in an expanding series of reactions or cascade. Activation of complement stimulates inflammation, attracts phagocytes, and enhances phagocytosis.
Natural Killer (NK) Cells
Natural killer (NK) cells are a small population of lymphocytes. They are different from the lymphocytes (T and B cells) that provide adaptive (specific) defense mechanisms. NK cells defend the body against various viruses and cancer cells by secreting cytolytic (“cell-cutting”) substances called perforins that lyse the cell membrane, destroying the infected cell. NK cells also secrete chemicals that enhance inflammation.
Fever
Fever is body temperature elevated above an individual’s normal temperature due to an elevated setpoint. It is part of the innate defense because as a result of the fever the body becomes inhospitable to certain pathogens. Higher body temperature causes the liver and spleen to sequester iron, which reduces the level of iron in the blood. Because bacteria and fungi require iron for normal metabolism, their growth and reproduction in a fever-ridden body slows and may cease. Also, phagocytic cells attack more vigorously when the temperature rises. For these reasons, low-grade fever of short duration may be a natural response to infection, not a treated symptom.
Immunity
The third line of defense, immunity, is resistance to specific pathogens or to their toxins or metabolic by-products. Lymphocytes and macrophages that recognize and remember specific foreign molecules carry out adaptive immune responses, which include the cellular immune response and the humoral immune response.
Antigens
Antigens are proteins, polysaccharides, glycoproteins, or glycolipids that can elicit an immune response. Before birth, cells inventory the antigens in the body, learning to identify these as “self.” The immune response is to “nonself,” or foreign, antigens, but not normally to self antigens. Receptors on lymphocyte surfaces enable these cells to recognize nonself antigens.
The antigens most effective in eliciting an immune response are large and complex, with few repeating parts. A smaller molecule that cannot by itself stimulate an immune response may combine with a larger molecule, which makes it detectable. Such a small molecule is called a hapten. Stimulated lymphocytes react either to the hapten or to the larger molecule of the combination. Hapten molecules are in drugs such as penicillin, in household and industrial chemicals, in dust particles, and in animal dander.
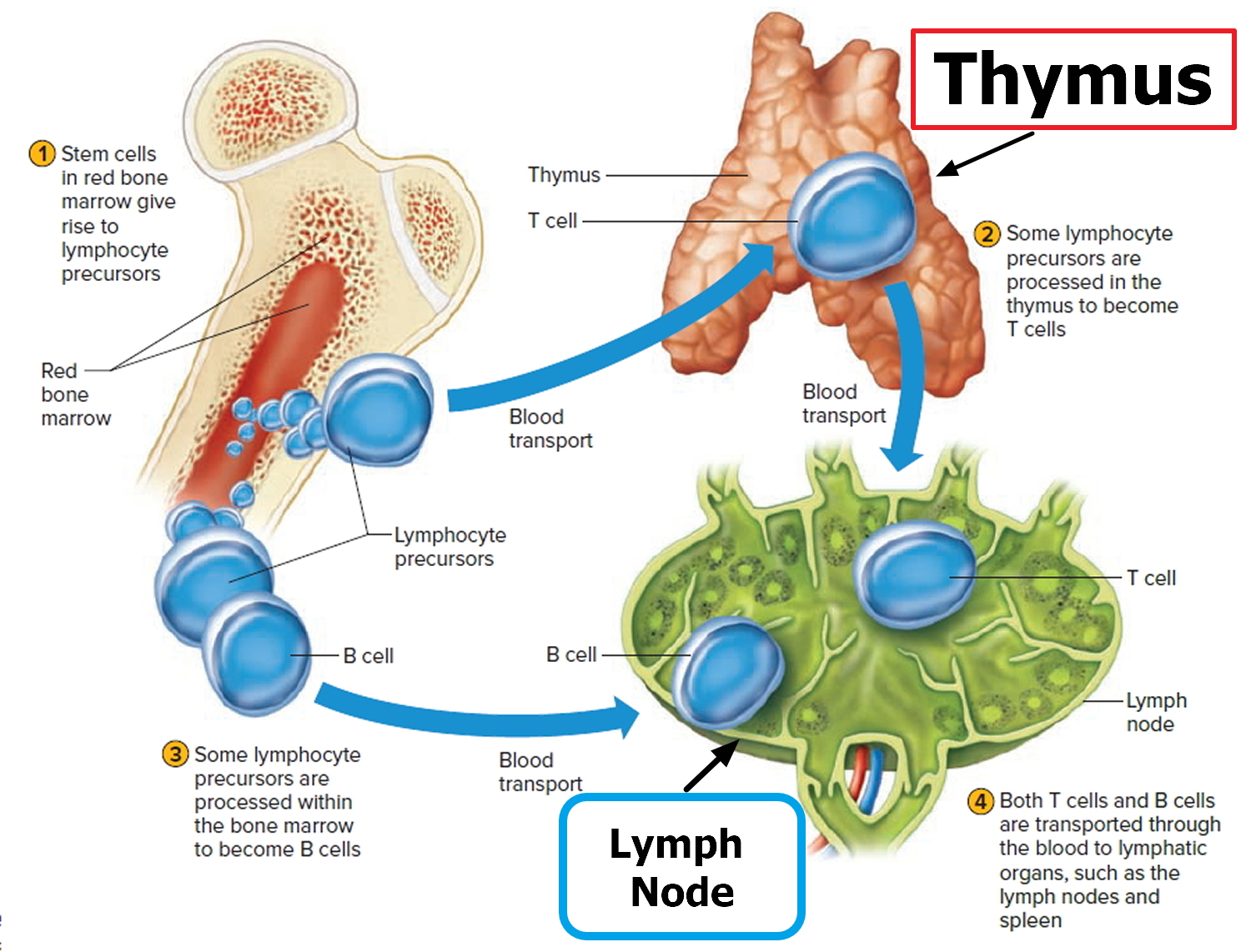
Lymphocyte Origins
Lymphocyte production begins during fetal development and continues throughout life, with red bone marrow releasing unspecialized precursors to lymphocytes into the circulation. About half of these cells reach the thymus, where they specialize into T lymphocytes, or T cells. After leaving the thymus, some of these T cells constitute 70% to 80% of the circulating lymphocytes in blood. Other T cells reside in lymphatic organs and are particularly abundant in the lymph nodes, thoracic duct, and white pulp of the spleen.
Other lymphocytes remain in the red bone marrow until they differentiate into B lymphocytes, or B cells. The blood distributes B cells, which constitute 20% to 30% of circulating lymphocytes. B cells settle in lymphatic organs along with T cells and are abundant in the lymph nodes, spleen, bone marrow, and intestinal lining. Figure 8 illustrates B cell and T cell production. Table 1 compares the characteristics of T cells and B cells.
Figure 8. Lymphocyte production
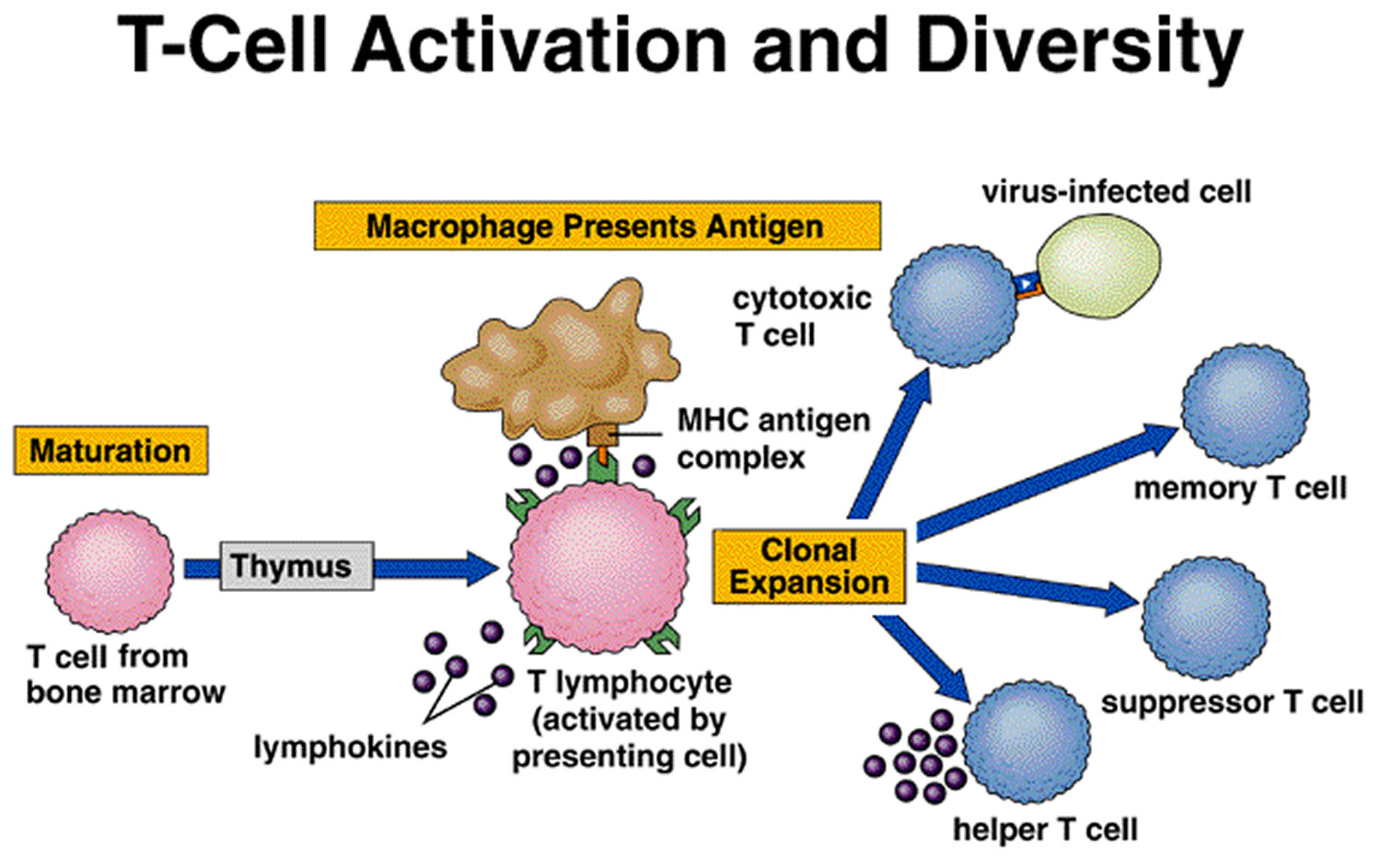
T Cells and the Cellular Immune Response
A lymphocyte must be activated before it can respond to an antigen. T cell activation requires that processed fragments of the antigen be attached to the surface of another type of cell, called an antigen-presenting cell (accessory cell). Macrophages, B cells, and several other cell types can be antigen-presenting cells.
T cell activation may occur when a macrophage phagocytizes a bacterium and digests it within a phagolysosome formed by the fusion of the vesicle containing the bacterium (phagosome) and a lysosome. Some of the resulting bacterial antigens are then displayed on the macrophage’s cell membrane near certain protein molecules that are part of a group of proteins called the major histocompatibility complex (MHC). MHC antigens help T cells recognize that a newly displayed antigen is foreign (nonself).
Activated T cells interact directly with antigen-bearing cells. Such cell-to-cell contact is called the cellular immune response, or cell-mediated immunity. T cells (and some macrophages) also synthesize and secrete polypeptides called cytokines that enhance certain cellular responses to antigens. For example, interleukin-1 and interleukin-2 stimulate the synthesis of several other cytokines from other T cells. Additionally, interleukin-1 helps activate T cells, whereas interleukin-2 causes T cells to proliferate. This proliferation increases the number of T cells in a clone, which is a group of genetically identical cells that descend from a single, original cell. Other cytokines, called colony stimulating factors (CSFs), stimulate leukocyte production in red bone marrow and activate macrophages. T cells may also secrete toxins that kill their antigen-bearing target cells, growth-inhibiting factors that prevent target cell growth, or interferon that inhibits the proliferation of viruses and tumor cells. Several types of T cells have distinct functions.
A specialized type of T cell, called a helper T cell, is activated when its antigen receptor combines with a displayed foreign antigen (Figure 9). Once activated, the
helper T cell proliferates and the resulting cells stimulate B cells to produce antibodies that are specific for the displayed antigen.
Another type of T cell is a cytotoxic T cell, which recognizes and combines with nonself antigens that cancerous cells or virally infected cells display on their surfaces near certain MHC proteins. Cytokines from helper T cells activate the cytotoxic T cell. Next, the cytotoxic T cell proliferates. Cytotoxic T cells then bind to the surfaces of antigen-bearing cells, where they release perforin protein that cuts pore like openings in the cell membrane, destroying these cells. In this way, cytotoxic T cells continually monitor the body’s cells, recognizing and eliminating tumor cells and cells infected with viruses. Cytotoxic T cells provide much of the body’s defense against HIV infection.
Some cytotoxic T cells do not respond to a nonself antigen on first exposure, but remain as memory T cells that provide for future immune protection. Upon subsequent exposure to the same antigen, these memory cells immediately divide to yield more cytotoxic T cells and helper T cells, often before symptoms arise.
Figure 9. T-cell activation
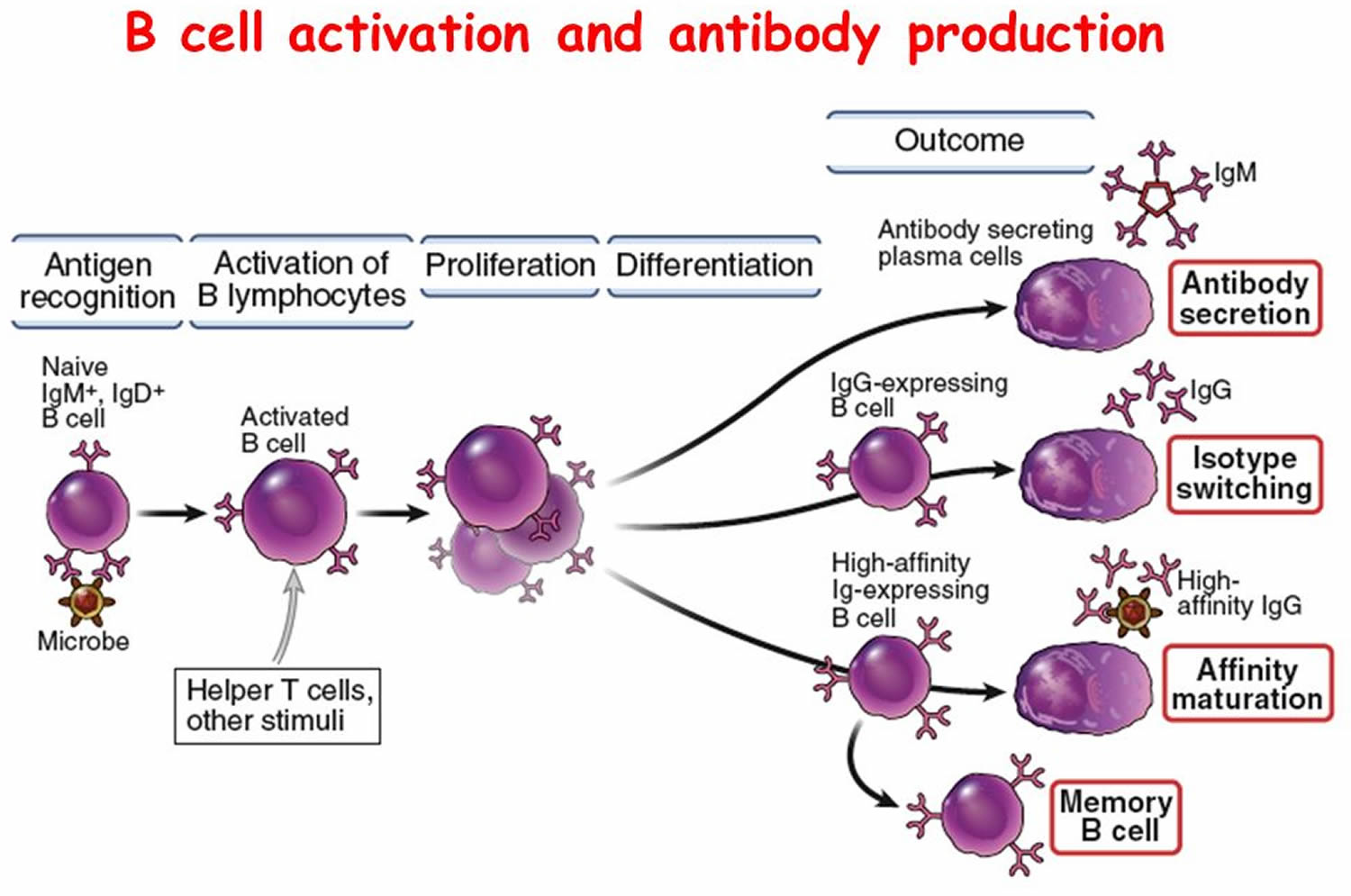
B Cells and the Humoral Immune Response
When a B cell encounters an antigen whose molecular shape fits the shape of the B cell’s antigen receptors, it becomes activated. In response to the receptor-antigen combination, the B cell divides repeatedly, expanding its clone. However, most of the time B cell activation requires T cell “help.” When an activated helper T cell encounters a B cell already combined with a foreign antigen identical to the one that activated the helper T cell, the helper T cell releases certain cytokines. These cytokines stimulate the B cell to proliferate, increasing the number of cells in its clone of antibody-producing cells (Figure 10). The cytokines also attract macrophages and leukocytes into inflamed tissues and help keep them there.
Some members of the activated B cell’s clone differentiate further into plasma cells, which produce and secrete large globular proteins called antibodies, also called immunoglobulins. Antibodies are similar in structure to the antigen-receptor molecules on the original B cell’s surface. Body fluids carry antibodies, which then react in various ways to destroy specific antigens or antigen-bearing particles. This antibody-mediated immune response is called the humoral immune response.
An individual’s B cells can produce more than 1,000,000,000 different antibodies, each reacting against a specific antigen. The enormity and diversity of the antibody response defends against many pathogens.
Other members of the activated B cell’s clone differentiate further into memory B cells. Like memory T cells, these memory B cells respond rapidly to subsequent exposure to a specific antigen.
Table 2 summarizes the steps leading to antibody production as a result of B cell and T cell activities.
Table 2. Steps in Antibody Production
| B Cell Activities |
|
| T Cell Activities |
|
Figure 10. B-cell activation
Types of Antibodies
Antibodies (immunoglobulins) are soluble, globular proteins that constitute the gamma globulin fraction of blood plasma proteins (see Blood Plasma). Of the five major types of immunoglobulins, the most abundant are immunoglobulin G, immunoglobulin A, and immunoglobulin M.
Immunoglobulin G (IgG) is in plasma and tissue fluids and is particularly effective against bacteria, viruses, and toxins. It also activates complement.
Immunoglobulin A (IgA) is commonly found in exocrine gland secretions. It is in breast milk, tears, nasal fluid, gastric juice, intestinal juice, bile, and urine.
Immunoglobulin M (IgM) is a type of antibody present in plasma in response to contact with certain antigens in foods or bacteria. The antibodies anti-A and anti-B, described in Blood Donation – Blood Transfusions, are examples of IgM. IgM also activates complement.
Immunoglobulin D (IgD) is found on the surfaces of most B cells, especially those of infants. IgD is important in activating B cells.
Immunoglobulin E (IgE) is found on the surfaces of basophils and mast cells. It is associated with allergic responses.
A newborn does not yet have its own antibodies, but does retain for a while IgG that passed through the placenta from the mother. These maternal antibodies protect the infant against some illnesses to which the mother is immune. As the maternal antibody supply falls, the infant begins to manufacture its own antibodies. The newborn also receives IgA from colostrum, a substance secreted from the mother’s breasts for the first few days after birth, and then from breast milk. Antibodies in colostrum protect against certain digestive and respiratory infections.
Antibody Actions
In general, antibodies react to antigens in three ways. Antibodies directly attack antigens, activate complement, or stimulate localized changes (inflammation) that help prevent the spread of pathogens or cells bearing foreign antigens.
In a direct attack, antibodies combine with antigens, causing them to clump (agglutination) or to form insoluble substances (precipitation). Such actions make it easier for phagocytic cells to recognize and engulf the antigen-bearing agents and eliminate them. In other instances, antibodies cover the toxic portions of antigen molecules and neutralize their effects (neutralization). However, under normal conditions, direct antibody attack is not as important as complement activation in protecting against infection.
When certain IgG or IgM antibodies combine with antigens, they expose reactive sites on antibody molecules. This triggers a series of reactions, leading to activation of the complement proteins, which in turn produce a variety of effects. These include:
- coating the antigen-antibody complexes (opsonization), making the complexes more susceptible to phagocytosis;
- attracting macrophages and neutrophils into the region (chemotaxis);
- rupturing membranes of foreign cells (lysis); agglutination of antigen-bearing cells; and
- neutralization of viruses by altering their molecular structure, making them harmless.
Other proteins promote inflammation, which helps prevent the spread of infectious agents.
Immune Responses
Activation of B cells or T cells after they first encounter the antigens for which they are specialized to react constitutes a primary immune response. During such a response, plasma cells release antibodies (IgM, followed by IgG) into the lymph. The antibodies are transported to the blood and then throughout the body, where they help destroy antigen bearing agents. Production and release of antibodies continues for several weeks.
Following a primary immune response, some of the B cells produced during proliferation of the clone remain dormant as memory cells. If the same antigen is encountered again, the clones of these memory cells enlarge, and they can respond rapidly by producing IgG to the antigen to which they were previously sensitized. These memory B cells, along with the memory cytotoxic T cells, produce a secondary immune response.
As a result of a primary immune response, detectable concentrations of antibodies usually appear in the blood plasma five to ten days after exposure to antigens. If the same type of antigen is encountered later, a secondary immune response may produce the same antibodies within a day or two. Although newly formed antibodies may persist in the body for only a few months or years, memory cells live much longer.
Naturally acquired active immunity occurs when a person exposed to a pathogen develops a disease. Resistance to that pathogen is the result of a primary immune response.
A vaccine is a preparation that produces artificially acquired active immunity. A vaccine might consist of bacteria or viruses that have been killed or weakened so that they cannot cause a serious infection, or only molecules unique to the pathogens. A vaccine might also be a toxoid, which is a toxin from an infectious organism that has been chemically altered to destroy its dangerous effects. Whatever its composition, a vaccine includes the antigens that stimulate a primary immune response, but does not produce symptoms of disease and the associated infections.
Specific vaccines stimulate active immunity against a variety of diseases, including typhoid fever, cholera, whooping cough, diphtheria, tetanus, polio, chickenpox, measles (rubeola), German measles (rubella), mumps, influenza, hepatitis A, hepatitis B, and bacterial pneumonia. A vaccine has eliminated naturally acquired smallpox from the world.
Autoimmunity
The immune response can turn against the body itself. It may become unable to distinguish a particular self antigen from a nonself antigen, producing autoantibodies and cytotoxic T cells that attack and damage the body’s tissues and organs. This reaction against self is called autoimmunity.
The specific nature of an autoimmune disorder reflects the cell types that are the target of the immune attack. In type 1 (insulin dependent) diabetes mellitus the target is beta cells in the pancreas. The tissues within the joints are targeted in rheumatoid arthritis. In systemic lupus erythematosus the target is DNA and proteins associated with it in the cell nuclei. About 5% of the population has an autoimmune disorder.
Why might the immune response attack body tissues ?
Perhaps a virus, while replicating inside a human cell, takes proteins from the host cell’s surface and incorporates them onto its own surface. When the immune response “learns” the surface of the virus in order to destroy it, it also learns to attack the human cells that normally bear those particular proteins. Another explanation of autoimmunity is that somehow T cells never learn to distinguish self from nonself. A third possible route of autoimmunity is when a nonself antigen coincidentally resembles a self antigen.
What does low white blood cells mean
Low white blood cells or leucopenia is a range of disorders can cause decreases in white blood cells. Leukopenia is characterized by a reduction in the circulating white blood cell count to < 4000/μL 11. The type of white blood cell decreased is usually the neutrophil. In this case the decrease may be called neutropenia or granulocytopenia. Less commonly, a decrease in lymphocytes (called lymphocytopenia or lymphopenia) may be seen.
Neutropenia
Neutropenia is an abnormally low level of neutrophils. Neutrophils are a common type of white blood cell important to fighting off infections — particularly those caused by bacteria and fungal infections 12. When neutropenia is present, the inflammatory response to such infections is ineffective.
Normal lower limit of the neutrophil count (total white blood cell × % neutrophils and bands) is 1500/μL in whites and is somewhat lower in blacks (about 1200/μL) 12. Neutrophil counts are not as stable as other cell counts and may vary considerably over short periods, depending on many factors such as activity status, anxiety, infections, and drugs. Thus, several measurements may be needed when determining the severity of neutropenia 12.
Severity of neutropenia relates to the relative risk of infection and is classified as follows 12:
- Mild (1000 to 1500/μL)
- Moderate (500 to 1000/μL)
- Severe (<500/μL)
When neutrophil counts fall to <500/μL, endogenous microbial flora (eg, in the mouth or gut) can cause infections. If the count falls to < 200/μL, inflammatory response may be muted and the usual inflammatory findings of leukocytosis or white blood cells in the urine or at the site of infection may not occur. Acute, severe neutropenia, particularly if another factor (eg, cancer) is present, significantly impairs the immune system and can lead to rapidly fatal infections. The integrity of the skin and mucous membranes, the vascular supply to tissue, and the nutritional status of the patient also influence the risk of infections.
The most frequently occurring infections in patients with profound neutropenia are:
- Cellulitis (infection of subcutaneous connective tissue)
- Furunculosis (boils on the skin)
- Pneumonia (lung infection)
- Septicemia (bacteria in the blood)
Vascular catheters and other puncture sites confer extra risk of skin infections; the most common bacterial causes are coagulase-negative staphylococci and Staphylococcus aureus, but other gram-positive and gram-negative infections also occur. Stomatitis, gingivitis, perirectal inflammation, colitis, sinusitis, paronychia, and otitis media often occur. Patients with prolonged neutropenia after hematopoietic stem cell transplantation or chemotherapy and patients receiving high doses of corticosteroids are predisposed to fungal infections.
Causes of neutropenia
Cancer chemotherapy is probably the most common cause of neutropenia. People with chemotherapy-related neutropenia are prone to infections while they wait for their cell counts to recover.
Neutrophils are manufactured in bone marrow — the spongy tissue inside some of your larger bones. Anything that disrupts neutrophil production can result in neutropenia.
Acute neutropenia (occurring over hours to a few days) can develop as a result of rapid neutrophil use or destruction or due to impaired production.
Chronic neutropenia (lasting months to years) usually arises as a result of reduced production or excessive splenic sequestration.
Neutropenia also may be classified as primary due to an intrinsic defect in marrow myeloid cells or as secondary (due to factors extrinsic to marrow myeloid cells).
Neutropenia can be acquired or intrinsic 13. A decrease in levels of neutrophils on lab tests is due to either decreased production of neutrophils or increased removal from the blood 14.
The following is a list of neutropenia causes due to intrinsic defects in myeloid cells or their precursors:
- Aplastic anemia
- Chronic idiopathic neutropenia, including benign neutropenia
- Cyclic neutropenia
- Myelodysplasia
- Neutropenia associated with dysgammaglobulinemia
- Paroxysmal nocturnal hemoglobinuria
- Severe congenital neutropenia (Kostmann syndrome)
- Syndrome-associated neutropenias (eg, cartilage-hair hypoplasia syndrome, dyskeratosis congenita, glycogen storage disease type IB, warts, hypogammaglobulinemia, infections, myelokathexis [WHIM] syndrome, Shwachman-Diamond syndrome)
The following is a list of causes of secondary neutropenias:
- Alcoholism
- Autoimmune neutropenia, including chronic secondary neutropenia in AIDS
- Bone marrow replacement (eg, due to cancer, myelofibrosis, granuloma, or Gaucher cells)
- Cytotoxic chemotherapy or radiation therapy
- Drug-induced neutropenia – sulfas or other antibiotics, phenothiazenes, benzodiazepines, antithyroids, anticonvulsants, quinine, quinidine, indomethacin, procainamide, thiazides
- Folate deficiency, vitamin B12 deficiency, or severe undernutrition
- Hypersplenism
- Infection
- T cell large granular lymphocyte disease
Symptoms and Signs of Neutropenia
Neutropenia is asymptomatic until infection develops. Fever is often the only indication of infection. Typical signs of inflammation (erythema, swelling, pain, infiltrates, leukocytic reaction) may be muted or absent. Focal symptoms (eg, oral ulcers) may develop but are often subtle. Patients with drug-induced neutropenia due to hypersensitivity may have a fever, rash, and lymphadenopathy as a result of the hypersensitivity.
Neutropenia is usually found when your doctor orders tests for a condition you’re already experiencing. It’s rare for neutropenia to be discovered unexpectedly or by chance.
Talk to your doctor about what your test results mean. Neutropenia and results from other tests might indicate the cause of your illness. Or, your doctor may suggest other tests to further check your condition.
Because neutropenia makes you vulnerable to bacterial and fungal infections, your doctor will probably advise certain precautions. These often include wearing a face mask, avoiding anyone with a cold, and washing your hands regularly and thoroughly.
Some patients with chronic benign neutropenia and neutrophil counts < 200/μL do not experience many serious infections. Patients with cyclic neutropenia or severe congenital neutropenia tend to have episodes of oral ulcers, stomatitis, or pharyngitis and lymph node enlargement during severe neutropenia. Pneumonias and septicemia often occur.
Treatment of neutropenia
- Treatment of associated conditions (eg, infections, stomatitis)
- Sometimes antibiotic prophylaxis
- Myeloid growth factors
- Discontinuation of suspected etiologic agent (eg, drug)
- Sometimes corticosteroids
Acute neutropenia
Suspected infections are always treated immediately. If fever or hypotension is present, serious infection is assumed, and empiric, high-dose, broad-spectrum antibiotics are given IV. Regimen selection is based on the most likely infecting organisms, the antimicrobial susceptibility of pathogens at that particular institution, and the regimen’s potential toxicity. Because of the risk of creating resistant organisms, vancomycin is used only if gram-positive organisms resistant to other drugs are suspected.
Indwelling vascular catheters can usually remain in place even if bacteremia is suspected or documented, but removal is considered if infections involve S. aureus or Bacillus sp, Corynebacterium sp, or Candida sp or if blood cultures are persistently positive despite appropriate antibiotics. Infections caused by coagulase-negative staphylococci generally resolve with antimicrobial therapy alone. Indwelling Foley catheters can also predispose to infections in these patients, and change or removal of the catheter should be considered for persistent urinary infections.
If cultures are positive, antibiotic therapy is adjusted to the results of sensitivity tests. If a patient defervesces within 72 h, antibiotics are continued for at least 7 days and until the patient has no symptoms or signs of infection. When neutropenia is transient (such as that following myelosuppressive chemotherapy), antibiotic therapy is usually continued until the neutrophil count is >500/μL; however, stopping antimicrobials can be considered in selected patients with persistent neutropenia, especially those in whom symptoms and signs of inflammation have resolved, if cultures remain negative.
Fever that persists > 72 h despite antibiotic therapy suggests a nonbacterial cause, infection with a resistant species, a superinfection with a 2nd bacterial species, inadequate serum or tissue levels of the antibiotics, or localized infection, such as an abscess. Neutropenic patients with persistent fever are reassessed every 2 to 4 days with physical examination, cultures, and chest x-ray. If the patient is well except for the presence of fever, the initial antibiotic regimen can be continued, and drug-induced fever should be considered. If the patient is deteriorating, alteration of the antimicrobial regimen is considered.
Fungal infections are the most likely cause of persistent fevers and deterioration. Antifungal therapy is added empirically if unexplained fever persists after 3 to 4 days of broad-spectrum antibiotic therapy. Selection of the specific antifungal drug (eg, fluconazole, caspofungin, voriconazole, posaconazole) depends on the type of risk (eg, duration and severity of neutropenia, past history of fungal infection, persistent fever despite use of narrower spectrum antifungal drug) and should be guided by an infectious disease specialist. If fever persists after 3 wk of empiric therapy (including 2 wk of antifungal therapy) and the neutropenia has resolved, then stopping all antimicrobials can be considered and the cause of fever reevaluated.
For afebrile patients with neutropenia, antibiotic prophylaxis with fluoroquinolones (levofloxacin, ciprofloxacin) is used in some centers for patients who receive chemotherapy regimens that commonly result in neutrophils ≤ 100/µL for > 7 days.. Prophylaxis is usually started by the treating oncologist. Antibiotics are continued until the neutrophil count increases to > 1500/µL. Also, antifungal therapy can be given for afebrile neutropenic patients at higher risk of fungal infection (eg, after hematopoietic stem cell transplantation, intensive chemotherapy for acute myelogenous leukemia or a myelodysplastic disorder, prior fungal infections). Selection of the specific antifungal drug should be guided by an infectious disease specialist. Antibiotic and antifungal prophylaxis is not routinely recommended for afebrile neutropenic patients without risk factors who are anticipated to remain neutropenic for < 7 days on the basis of their specific chemotherapy regimen.
Myeloid growth factors (ie, granulocyte colony-stimulating factor [G-CSF]) are widely used to increase the neutrophil count and to prevent infections in patients with severe neutropenia (eg, after hematopoietic stem cell transplantation and intensive cancer chemotherapy). They are expensive. However, if the risk of febrile neutropenia is ≥ 30% (as assessed by neutrophil count < 500 μL, presence of infection during a previous cycle of chemotherapy, associated comorbid disease, or age > 75), growth factors are indicated. In general, most clinical benefit occurs when the growth factor is administered beginning about 24 h after completion of chemotherapy. Patients with neutropenia caused by an idiosyncratic drug reaction may also benefit from myeloid growth factors, particularly if a delayed recovery is anticipated. The dose for G-CSF (filgrastim) is 5 to 10 mcg/kg sc once/day, and the dose for pegylated G-CSF (pegfilgrastim) is 6 mg sc once per chemotherapy cycle.
Glucocorticoids, anabolic steroids, and vitamins do not stimulate neutrophil production but can affect distribution and destruction. If acute neutropenia is suspected to be drug- or toxin-induced, all potentially etiologic agents are stopped. If neutropenia develops during treatment with a drug known to induce low counts (eg, chloramphenicol), then switching to an alternative antibiotic may be helpful.
Saline or hydrogen peroxide gargles every few hours, liquid oral rinses (containing viscous lidocaine, diphenhydramine, and liquid antacid), anesthetic lozenges (benzocaine 15 mg q 3 or 4 h), or chlorhexidine mouth rinses (1% solution) bid or tid may relieve the discomfort of stomatitis with oropharyngeal ulcerations. Oral or esophageal candidiasis is treated with nystatin (400,000 to 600,000 units oral rinse qid; swallowed if esophagitis is present), clotrimazole troche (10 mg slowly dissolved in the mouth 5 times a day), or systemic antifungal drugs (eg, fluconazole). A semisolid or liquid diet may be necessary during acute stomatitis or esophagitis, and topical analgesics (eg,viscous lidocaine) may be needed to minimize discomfort.
Chronic neutropenia
Neutrophil production in congenital neutropenia, cyclic neutropenia, and idiopathic neutropenia can be increased with administration of G-CSF 1 to 10 mcg/kg sc once/day. Effectiveness can be maintained with daily or intermittent G-CSF for months or years. Long-term G-CSF has also been used in other patients with chronic neutropenia, including those with myelodysplasia, HIV, and autoimmune disorders. In general, neutrophil counts increase, although clinical benefits are less clear, especially for patients who do not have severe neutropenia. For patients with autoimmune disorders or who have had an organ transplant, cyclosporine can also be beneficial.
In some patients with accelerated neutrophil destruction caused by autoimmune disorders, corticosteroids (generally, prednisone 0.5 to 1.0 mg/kg po once/day) can increase blood neutrophils. This increase often can be maintained with alternate-day G-CSF therapy.
Splenectomy has been used in the past to increase the neutrophil count in some patients with splenomegaly and splenic sequestration of neutrophils (eg, Felty syndrome); however,because growth factors and other newer therapies are often effective, splenectomy should be avoided in most patients. However, splenectomy can be considered for patients with persistent painful splenomegaly or with severe neutropenia (ie, <500/μL) and serious problems with infections in whom other treatments have failed. Patients should be vaccinated against infections caused by Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae before splenectomy because splenectomy predisposes patients to infection by encapsulated organisms.
Lymphocytopenia
The normal lymphocyte count in adults is 1000 to 4800/μL; in children < 2 yr, 3000 to 9500/μL. At age 6 yr, the lower limit of normal is 1500/μL.
Lymphocytopenia is a total lymphocyte count of < 1000/μL in adults or < 3000/μL in children < 2 yr 15.
Both B and T cells are present in the peripheral blood; about 75% of the lymphocytes are T cells and 25% B cells. Because lymphocytes account for only 20 to 40% of the total WBC count, lymphocytopenia may go unnoticed when WBC count is checked without a differential.
Almost 65% of blood T cells are CD4+ T-helper cells. Most patients with lymphocytopenia have a reduced absolute number of T cells, particularly in the number of CD4+ T cells. The average number of CD4+ T-helper cells in adult blood is 1100/μL (range, 300 to 1300/μL), and the average number of cells of the other major T-cell subgroup, CD8+ (suppressor) T cells, is 600/μL (range, 100 to 900/μL).
Lymphocytopenia can be 15:
- Acquired
- Inherited
Causes of Acquired lymphocytopenia:
- AIDS
- Other infectious disorders, including hepatitis, influenza, TB, typhoid fever, and sepsis
- Dietary deficiency in patients with ethanol abuse, protein-energy undernutrition, or zinc deficiency
- Protein losing enteropathy
- Iatrogenic after use of cytotoxic chemotherapy, glucocorticoids, high-dose psoralen and ultraviolet A radiation therapy, lymphocyte antibody therapy, immunosuppressants, radiation therapy, or thoracic duct drainage
- Systemic disorders with autoimmune features (eg, aplastic anemia, Hodgkin lymphoma, myasthenia gravis, protein-losing enteropathy, RA, chronic kidney disease, sarcoidosis, SLE, thermal injury).
Causes of Inherited lymphocytopenia:
- Aplasia of lymphopoietic stem cells
- Ataxia-telangiectasia
- Cartilage-hair hypoplasia syndrome
- Idiopathic CD4+ T lymphocytopenia
- Immunodeficiency with thymoma
- Severe combined immunodeficiency associated with a defect in the IL-2 receptor gamma-chain, deficiency of adenosine deaminase or purine nucleoside phosphorylase, or an unknown defect
- Wiskott-Aldrich syndrome
Acquired lymphocytopenia
Acquired lymphocytopenia can occur with a number of other disorders. The most common causes include:
- Protein-energy undernutrition
- AIDS and certain other viral infections
Protein-energy undernutrition is the most common cause worldwide.
AIDS is the most common infectious disease causing lymphocytopenia, which arises from destruction of CD4+ T cells infected with HIV. Lymphocytopenia may also reflect impaired lymphocyte production arising from destruction of thymic or lymphoid architecture. In acute viremia due to HIV or other viruses, lymphocytes may undergo accelerated destruction from active infections with the virus, may be trapped in the spleen or lymph nodes, or may migrate to the respiratory tract.
Iatrogenic lymphocytopenia is caused by cytotoxic chemotherapy, radiation therapy, or the administration of antilymphocyte globulin (or other lymphocyte antibodies). Long-term treatment for psoriasis using psoralen and ultraviolet A irradiation may destroy T cells. Glucocorticoids can induce lymphocyte destruction.
Lymphocytopenia may occur with lymphomas, autoimmune diseases such as SLE, rheumatoid arthritis, myasthenia gravis, and protein-losing enteropathy.
Inherited lymphocytopenia
Inherited lymphocytopenia (see Table: Causes of Lymphocytopenia) most commonly occurs in:
- Severe combined immunodeficiency disorder
- Wiskott-Aldrich syndrome
It may occur with inherited immunodeficiency disorders and disorders that involve impaired lymphocyte production. Other inherited disorders, such as Wiskott-Aldrich syndrome, adenosine deaminase deficiency, and purine nucleoside phosphorylase deficiency, may involve accelerated T-cell destruction. In many disorders, antibody production is also deficient.
Symptoms and Signs of Lymphocytopenia
Lymphocytopenia per se generally causes no symptoms. However, findings of an associated disorder may include:
- Absent or diminished tonsils or lymph nodes, indicative of cellular immunodeficiency
- Skin abnormalities (eg, alopecia, eczema, pyoderma, telangiectasia)
- Evidence of hematologic disease (eg, pallor, petechiae, jaundice, mouth ulcers)
- Generalized lymphadenopathy and splenomegaly, which may suggest HIV infection or Hodgkin lymphoma
Lymphocytopenic patients experience recurrent infections or develop infections with unusual organisms. Pneumocystis jirovecii, cytomegalovirus, rubeola, and varicella pneumonias often are fatal. Lymphocytopenia is also a risk factor for the development of cancers and for autoimmune disorders.
Diagnosis of Lymphocytopenia
- Clinical suspicion (repeated or unusual infections)
- Complete blood count with differential
- Measurement of lymphocyte subpopulations and immunoglobulin levels
Lymphocytopenia is suspected in patients with recurrent viral, fungal, or parasitic infections but is usually detected incidentally on a complete blood count. P. jirovecii, cytomegalovirus, rubeola, or varicella pneumonias with lymphocytopenia suggest immunodeficiency. Lymphocyte subpopulations are measured in patients with lymphocytopenia. Measurement of immunoglobulin levels should also be done to evaluate antibody production. Patients with a history of recurrent infections undergo complete laboratory evaluation for immunodeficiency, even if initial screening tests are normal.
Treatment of Lymphocytopenia
- Treatment of associated infections
- Treatment of underlying disorder
- Sometimes IV immune globulin
- Possibly hematopoietic stem cell transplantation
In acquired lymphocytopenias, lymphocytopenia usually remits with removal of the underlying factor or successful treatment of the underlying disorder. IV immune globulin is indicated if patients have chronic IgG deficiency, lymphocytopenia, and recurrent infections. Hematopoietic stem cell transplantation can be considered for all patients with congenital immunodeficiencies and may be curative.
What does increase white blood cells mean ?
A high white blood cell count is also called leukocytosis. A high white blood cell count is an increase in disease-fighting cells in your blood.
The exact threshold for a high white blood cell count varies from one laboratory to another. The normal range for white blood cell counts changes with age and pregnancy (Table 1). In general, for nonpregnant adults a count of more than 11,000 per mm3 (11.0 × 109 per L) white blood cells (leukocytes) in a microliter of blood is considered a high white blood cell count 16.
Leukocytosis in the range of approximately 50,000 to 100,000 per mm3 (50.0 to 100.0 × 109 per L) is sometimes referred to as a leukemoid reaction. This level of elevation can occur in some severe infections, such as Clostridium difficile infection, sepsis, organ rejection, or in patients with solid tumors 3. Leukocytosis greater than 100,000 per mm3 is almost always caused by leukemias or myeloproliferative disorders 17.
The most common type of leukocytosis is neutrophilia (an increase in the absolute number of mature neutrophils to greater than 7,000 per mm3 [7.0 × 109 per L]), which can arise from infections, stressful conditions, chronic inflammation, medication use, and other causes (Table 4) 3, 8, 18, 19. Lymphocytosis (when lymphocytes make up more than 40% of the white blood cell count or the absolute count is greater than 4,500 per mm3 [4.5 × 109 per L]) can occur in patients with pertussis, syphilis, viral infections, hypersensitivity reactions, and certain subtypes of leukemia or lymphoma. Lymphocytosis is more likely to be benign in children than in adults 5. Epstein-Barr virus infection, tuberculosis or fungal disease, autoimmune disease, splenectomy, protozoan or rickettsial infections, and malignancy can cause monocytosis (monocytes make up more than 8% of the white blood cell count or the absolute count is greater than 880 per mm3 [0.88 × 109 per L]) 9.
Eosinophilia (eosinophil absolute count greater than 500 per mm3 [0.5 × 109 per L]), although uncommon, may suggest allergic conditions such as asthma, urticaria, atopic dermatitis or eosinophilic esophagitis, drug reactions, dermatologic conditions, malignancies, connective tissue disease, idiopathic hypereosinophilic syndrome, or parasitic infections, including helminths (tissue parasites more than gut-lumen parasites) 20, 21. Isolated basophilia (number of basophils greater than 100 per mm3 [0.1 × 109 per L]) is rare and unlikely to cause leukocytosis in isolation, but it can occur with allergic or inflammatory conditions and chronic myelogenous leukemia 22 (Table 5).
A high white blood cell count is usually found when your doctor orders tests to help diagnose a condition you’re already experiencing. It’s rarely an unexpected finding or simply discovered by chance.
Speak to your doctor about what these results mean. A high white blood cell count, along with results from other tests, might already indicate the cause of your illness. Or your doctor may suggest other tests to further evaluate your condition.
Nonmalignant Causes of of Raised White Blood Cell
A reactive leukocytosis, typically in the range of 11,000 to 30,000 per mm3 (11.0 to 30.0 × 109 per L), can arise from a variety of etiologies. Any source of stress can cause a catecholamine-induced demargination of white blood cells, as well as increased release from the bone marrow storage pool. Examples include surgery, exercise, trauma, burns, and emotional stress.9 One study showed an average increase in white blood cells of 2,770 per mm3 (2.77 × 109 per L) peaking on postoperative day 2 after knee or hip arthroplasty.10 Medications known to increase the white blood cell count include corticosteroids, lithium, colony-stimulating factors, beta agonists, and epinephrine. During the recovery phase after hemorrhage or hemolysis, a rebound leukocytosis can occur.
Leukocytosis is one of the hallmarks of infection. In the acute stage of many bacterial infections, there are primarily mature and immature neutrophils; sometimes, as the infection progresses, there is a shift to lymphocyte predominance. The release of less-mature bands and metamyelocytes into the peripheral circulation results in the so-called “left shift” in the white blood cell differential. Of note, some bacterial infections paradoxically cause neutropenias, such as typhoid fever, rickettsial infections, brucellosis, and dengue 3, 23. Viral infections may cause leukocytosis early in their course, but a sustained leukocytosis is not typical, except for the lymphocytosis in some childhood viral infections.
An elevated white blood cell count is a suggestive, but not definitive, marker of the presence of significant infection. For example, the sensitivity and specificity of an elevated white blood cell count in diagnosing acute appendicitis are 62% and 75%, respectively 24, 25. For diagnosing serious bacterial infections without a source in febrile children, the discriminatory value of leukocytosis is less than that of other biomarkers, such as C-reactive protein or procalcitonin 26. Although a WBC count greater than 12,000 per mm3 (12.0 × 109 per L) is one of the criteria for the systemic inflammatory response syndrome (or sepsis when there is a known infection), leukocytosis alone is a poor predictor of bacteremia and not an indication for obtaining blood cultures 27, 28.
Other acquired causes of leukocytosis include functional asplenia (predominantly lymphocytosis), smoking, and obesity. Patients with a chronic inflammatory condition, such as rheumatoid arthritis, inflammatory bowel disease, or a granulomatous disease, may also exhibit leukocytosis. Genetic causes include hereditary or chronic idiopathic neutrophilia and Down syndrome.
Table 4. Nonmalignant Causes of Neutrophilia
| Cause | Distinguishing features | Evaluation |
|---|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Note: After patient characteristics, causes are listed in approximate order of frequency.
CRP = C-reactive protein; WBC = white blood cell.
Table 5. Selected Conditions Associated with Elevations in Certain White Blood Cell Types
| White blood cell line | Conditions that typically cause elevations |
|---|---|
Basophils | Allergic conditions, leukemias |
Eosinophils | Allergic conditions, dermatologic conditions, eosinophilic esophagitis, idiopathic hypereosinophilic syndrome, malignancies, medication reactions, parasitic infections |
Lymphocytes | Acute or chronic leukemia, hypersensitivity reaction, infections (viral, pertussis) |
Monocytes | Autoimmune disease, infections (Epstein-Barr virus, fungal, protozoan, rickettsial, tuberculosis), splenectomy |
Neutrophils | Bone marrow stimulation, chronic inflammation, congenital, infection, medication induced, reactive, splenectomy |
Causes of high white blood cells
A high white blood cell count usually indicates 16:
- An increased production of white blood cells to fight an infection
- A reaction to a drug that increases white blood cell production
- A disease of bone marrow, causing abnormally high production of white blood cells
- An immune system disorder that increases white blood cell production
Specific causes of a high white blood cell count include 16:
- Acute lymphocytic leukemia
- Acute myelogenous leukemia (AML)
- Allergy, especially severe allergic reactions
- Chronic lymphocytic leukemia
- Chronic myelogenous leukemia
- Drugs, such as corticosteroids and epinephrine
- Infections, bacterial or viral
- Myelofibrosis
- Polycythemia vera
- Rheumatoid arthritis
- Smoking
- Stress, such as severe emotional or physical stress
- Tuberculosis
- Whooping cough.
Malignant Causes of Raised White Blood Cells
Leukocytosis may herald a malignant disorder, such as an acute or chronic leukemia or a myeloproliferative disorder, such as polycythemia vera, myelofibrosis, or essential thrombocytosis 30. Many solid tumors may lead to a leukocytosis in the leukemoid range, either through bone marrow involvement or production of granulocyte colony-stimulating or granulocyte-macrophage colony-stimulating factors 31. Chronic leukemias are most commonly diagnosed after incidental findings of leukocytosis on complete blood counts in asymptomatic patients. Patients with features suggestive of hematologic malignancies require prompt referral to a hematologist/oncologist (Table 6) 32.
Table 6. Findings Suggestive of Blood Cancers in the Setting of Leukocytosis
Symptoms |
Bruising/bleeding tendency |
Fatigue, weakness |
Fever > 100.4°F (38°C) |
Immunosuppression |
Night sweats |
Unintentional weight loss |
Physical examination findings |
Lymphadenopathy |
Petechiae |
Splenomegaly or hepatomegaly |
Laboratory abnormalities |
Decreased red blood cell count or hemoglobin/hematocrit levels |
Increased or decreased platelet count |
Monomorphic lymphocytosis on peripheral smear |
Predominantly immature cells on peripheral smear |
White blood cell count > 30,000 per mm3 (30.0 × 109 per L), or > 20,000 per mm3 (20.0 × 109 per L) after initial management |
- Maton, D., Hopkins, J., McLaughlin, Ch. W., Johnson, S., Warner, M. Q., LaHart, D., & Wright, J. D., Deep V. Kulkarni (1997). Human Biology and Health. Englewood Cliffs, New Jersey, US: Prentice Hall. ISBN 0-13-981176-1.
- LaFleur-Brooks, M. (2008). Exploring Medical Language: A Student-Directed Approach (7th ed.). St. Louis, Missouri, US: Mosby Elsevier. p. 398. ISBN 978-0-323-04950-4.
- Cerny J, Rosmarin AG. Why does my patient have leukocytosis? Hematol Oncol Clin North Am. 2012;26(2):303–319, viii.
- Hoffman R, Benz EJ Jr, Silberstein LE, Heslop H, Weitz J, Anastasi J. Hematology: Basic Principles and Practice. 6th ed. Philadelphia, Pa.: Elsevier/Saunders; 2013:table 164–20.
- Chabot-Richards DS, George TI. Leukocytosis. Int J Lab Hematol. 2014;36(3):279–288.
- Lurie S, Rahamim E, Piper I, Golan A, Sadan O. Total and differential leukocyte counts percentiles in normal pregnancy. Eur J Obstet Gynecol Reprod Biol. 2008;136(1):16–19.
- Dior UP, Kogan L, Elchalal U, et al. Leukocyte blood count during early puerperium and its relation to puerperal infection. J Matern Fetal Neonatal Med. 2014;27(1):18–23.
- Lim EM, Cembrowski G, Cembrowski M, Clarke G. Race-specific WBC and neutrophil count reference intervals. Int J Lab Hematol. 2010;32(6 pt 2):590–597.
- Berliner N. Leukocytosis and leukopenia. In: Goldman L, Schafer AI, eds. Goldman’s Cecil Medicine. 24th ed. Philadelphia, Pa.: Elsevier/Saunders; 2012.
- White blood cell. Wikipedia. https://en.wikipedia.org/wiki/White_blood_cell
- Overview of Leukopenias. Merck Manual. https://www.merckmanuals.com/professional/hematology-and-oncology/leukopenias/overview-of-leukopenias
- Neutropenia. Merck Manual. https://www.merckmanuals.com/professional/hematology-and-oncology/leukopenias/neutropenia
- Richard A. McPherson; Matthew R. Pincus; Naif Z. Abraham Jr.; et al. (eds.). Henry’s clinical diagnosis and management by laboratory methods (22nd ed.). Philadelphia, PA: Elsevier/Saunders. ISBN 1437709745.
- Vinay Kumar; et al. (2010). Robbins and Cotran pathologic basis of disease. (8th ed.). Philadelphia, PA: Saunders/Elsevier. ISBN 1416031219.
- Lymphocytopenia. Merck Manual. https://www.merckmanuals.com/professional/hematology-and-oncology/leukopenias/lymphocytopenia
- High white blood cell count. Mayo Clinic. http://www.mayoclinic.org/symptoms/high-white-blood-cell-count/basics/definition/sym-20050611
- Jain R, Bansal D, Marwaha RK. Hyperleukocytosis: emergency management. Indian J Pediatr. 2013;80(2):144–148.
- Iskandar JW, Griffeth B, Sapra M, Singh K, Giugale JM. Panic-attack-induced transient leukocytosis in a healthy male: a case report. Gen Hosp Psychiatry. 2011;33(3):302.e11–302.e12.
- Deirmengian GK, Zmistowski B, Jacovides C, O’Neil J, Parvizi J. Leukocytosis is common after total hip and knee arthroplasty. Clin Orthop Relat Res. 2011;469(11):3031–3036.
- Ustianowski A, Zumla A. Eosinophilia in the returning traveler. Infect Dis Clin North Am. 2012;26(3):781–789.
- Cormier SA, Taranova AG, Bedient C, et al. Pivotal Advance: eosinophil infiltration of solid tumors is an early and persistent inflammatory host response. J Leukoc Biol. 2006;79(6):1131–1139.
- Munker R. Leukocytosis, leukopenia, and other reactive changes of myelopoiesis. In: Munker R, Hiller E, Glass J, Paquette R, eds. Modern Hematology: Biology and Clinical Management. 2nd ed. Totowa, N.J.; Humana Press; 2007.
- Potts JA, Rothman AL. Clinical and laboratory features that distinguish dengue from other febrile illnesses in endemic populations. Trop Med Int Health. 2008;13(11):1328–1340.
- Yu CW, Juan LI, Wu MH, Shen CJ, Wu JY, Lee CC. Systematic review and meta-analysis of the diagnostic accuracy of procalcitonin, C-reactive protein and white blood cell count for suspected acute appendicitis. Br J Surg. 2013;100(3):322–329.
- Van den Bruel A, Thompson MJ, Haj-Hassan T, et al. Diagnostic value of laboratory tests in identifying serious infections in febrile children: systematic review. BMJ. 2011;342:d3082.
- Yo CH, Hsieh PS, Lee SH, et al. Comparison of the test characteristics of procalcitonin to C-reactive protein and leukocytosis for the detection of serious bacterial infections in children presenting with fever without source: a systematic review and meta-analysis. Ann Emerg Med. 2012;60(5):591–600.
- Dellinger RP, Levy MM, Rhodes A, et al.; Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637.
- Coburn B, Morris AM, Tomlinson G, Detsky AS. Does this adult patient with suspected bacteremia require blood cultures? [published correction appears in JAMA. 2013;309(4):343]. JAMA. 2012;308(5):502–511.
- Evaluation of Patients with Leukocytosis. Am Fam Physician. 2015 Dec 1;92(11):1004-1011. http://www.aafp.org/afp/2015/1201/p1004.html
- Davis AS, Viera AJ, Mead MD. Leukemia: an overview for primary care. Am Fam Physician. 2014;89(9):731–738.
- Granger JM, Kontoyiannis DP. Etiology and outcome of extreme leukocytosis in 758 nonhematologic cancer patients: a retrospective, single-institution study. Cancer. 2009;115(17):3919–3923.
- Racil Z, Buresova L, Brejcha M, et al. Clinical and laboratory features of leukemias at the time of diagnosis: an analysis of 1,004 consecutive patients. Am J Hematol. 2011;86(9):800–803.

{kind=link}