What is Glycemic Index?
Carbohydrate is an essential part of our diets, but not all carbohydrate foods are equal. The glycemic index (GI) was first developed by Jenkins and colleagues 1 and the Glycemic Index (GI) is a relative ranking of carbohydrate in foods according to how they affect blood glucose levels 2. Carbohydrates with a low GI value (55 or less) are more slowly digested, absorbed and metabolised and cause a lower and slower rise in blood glucose and, therefore usually, insulin levels.
Research shows that both the amount and the type of carbohydrate in food affect blood glucose levels. Studies also show that the total amount of carbohydrate in food, in general, is a stronger predictor of blood glucose response than the GI.
The glycemic index or GI ranks carbohydrates according to their effect on blood glucose levels. The lower the GI, the slower the rise in blood glucose levels will be when the food is consumed. The effect may differ from person to person.
The GI index runs from 0–100 and usually uses glucose, which has a GI of 100, as the reference. Slowly absorbed carbohydrates have a low GI rating (55 or below), and include most fruits and vegetables, milk, some wholegrain cereals and bread, pulses and basmati rice. GI numbers are to be used as a guide only as individual foods do not have the same response in all people with diabetes.
- Low GI foods are foods with a GI less than 55.
- Intermediate GI foods are foods with a GI between 55 and 70.
- High GI foods are foods with a GI greater than 70.
Below are examples of foods based on their GI.
Low GI Foods (55 or less)
- 100% stone-ground whole wheat or pumpernickel bread
- Oatmeal (rolled or steel-cut), oat bran, muesli
- Pasta, converted rice, barley, bulgar
- Sweet potato, corn, yam, lima/butter beans, peas, legumes and lentils
- Most fruits, non-starchy vegetables and carrots
Not all low-GI foods are healthy choices – chocolate, for example, has a low-GI because of its fat content, which slows down the absorption of carbohydrate.
Medium GI (56-69)
- Whole wheat, rye and pita bread
- Quick oats
- Brown, wild or basmati rice, couscous
High GI (70 or more)
- White bread or bagel
- Corn flakes, puffed rice, bran flakes, instant oatmeal
- Shortgrain white rice, rice pasta, macaroni and cheese from mix
- Russet potato, pumpkin
- Pretzels, rice cakes, popcorn, saltine crackers
- melons and pineapple
Table 1. The average glycemic index (GI) of 62 common foods derived from multiple studies by different laboratories
| High-carbohydrate foods | Glycemic Index (GI) | Breakfast cereals | Glycemic Index (GI) | Fruit and fruit products | Glycemic Index (GI) | Vegetables | Glycemic Index (GI) |
|---|---|---|---|---|---|---|---|
| White wheat bread* | 75 ± 2 | Cornflakes | 81 ± 6 | Apple, raw† | 36 ± 2 | Potato, boiled | 78 ± 4 |
| Whole wheat/whole meal bread | 74 ± 2 | Wheat flake biscuits | 69 ± 2 | Orange, raw† | 43 ± 3 | Potato, instant mash | 87 ± 3 |
| Specialty grain bread | 53 ± 2 | Porridge, rolled oats | 55 ± 2 | Banana, raw† | 51 ± 3 | Potato, french fries | 63 ± 5 |
| Unleavened wheat bread | 70 ± 5 | Instant oat porridge | 79 ± 3 | Pineapple, raw | 59 ± 8 | Carrots, boiled | 39 ± 4 |
| Wheat roti | 62 ± 3 | Rice porridge/congee | 78 ± 9 | Mango, raw† | 51 ± 5 | Sweet potato, boiled | 63 ± 6 |
| Chapatti | 52 ± 4 | Millet porridge | 67 ± 5 | Watermelon, raw | 76 ± 4 | Pumpkin, boiled | 64 ± 7 |
| Corn tortilla | 46 ± 4 | Muesli | 57 ± 2 | Dates, raw | 42 ± 4 | Plantain/green banana | 55 ± 6 |
| White rice, boiled* | 73 ± 4 | Peaches, canned† | 43 ± 5 | Taro, boiled | 53 ± 2 | ||
| Brown rice, boiled | 68 ± 4 | Strawberry jam/jelly | 49 ± 3 | Vegetable soup | 48 ± 5 | ||
| Barley | 28 ± 2 | Apple juice | 41 ± 2 | ||||
| Sweet corn | 52 ± 5 | Orange juice | 50 ± 2 | ||||
| Spaghetti, white | 49 ± 2 | ||||||
| Spaghetti, whole meal | 48 ± 5 | ||||||
| Rice noodles† | 53 ± 7 | ||||||
| Udon noodles | 55 ± 7 | ||||||
| Couscous† | 65 ± 4 |
| Dairy products and alternatives | Glycemic Index (GI) | Legumes | Glycemic Index (GI) | Snack products | Glycemic Index (GI) | Sugars | Glycemic Index (GI) |
|---|---|---|---|---|---|---|---|
| Milk, full fat | 39 ± 3 | Chickpeas | 28 ± 9 | Chocolate | 40 ± 3 | Fructose | 15 ± 4 |
| Milk, skim | 37 ± 4 | Kidney beans | 24 ± 4 | Popcorn | 65 ± 5 | Sucrose | 65 ± 4 |
| Ice cream | 51 ± 3 | Lentils | 32 ± 5 | Potato crisps | 56 ± 3 | Glucose | 103 ± 3 |
| Yogurt, fruit | 41 ± 2 | Soya beans | 16 ± 1 | Soft drink/soda | 59 ± 3 | Honey | 61 ± 3 |
| Soy milk | 34 ± 4 | Rice crackers/crisps | 87 ± 2 | ||||
| Rice milk | 86 ± 7 |
*Low-GI varieties were also identified.
†Average of all available data.
Footnote: The GI should not be used in isolation; the energy density and macronutrient profile of foods should also be considered 3.
[Source 4 ]The amount of carbohydrate you eat has a bigger effect on blood glucose levels than GI alone.
The GI value relates to the food eaten on its own and in practice we usually eat foods in combination as meals. Bread, for example is usually eaten with butter or margarine, and potatoes could be eaten with meat and vegetables. Therefore relying solely on the glycemic index of foods could result in eating unbalanced and un-healthy diets high in fat, salt and saturated fats.
An additional problem is that GI compares the glycaemic effect of an amount of food containing 50g of carbohydrate, but in real life we eat different amounts of food containing different amounts of carbohydrate.
The recommendation is to eat more low and intermediate GI foods, not to exclude high GI foods. By choosing the low glycaemic index foods and thus the minimally processed foods, people can lose more weight, feel fuller longer, and remain healthier.
The GI is only a small part of the healthy eating plan for people with diabetes. For people with diabetes, meal planning with the GI involves choosing foods that have a low or medium GI. If eating a food with a high GI, you can combine it with low GI foods to help balance the meal.
Carbohydrates are an essential nutrient. You need carbs as they break down into glucose in your body providing the:
- main fuel for your brains and nervous systems,
- preferred source of fuel for most organs and your muscles during exercise.
Consuming good quality carbohydrates aka Low GI ones help to facilitate the management of diabetes, weight loss and weight loss management and reducing the risk of developing type 2 diabetes, diabetes complications and other chronic lifestyle diseases. In fact a low GI diet provides health benefits for everybody across all stages of life.

What can affect the Glycemic Index of Foods
Fat and fiber tend to lower the GI of a food. As a general rule, the more cooked or processed a food, the higher the GI; however, this is not always true.
Below are a few specific examples of other factors that can affect the GI of a food:
- Ripeness and storage time — the more ripe a fruit or vegetable is, the higher the GI.
- Processing — juice has a higher GI than whole fruit; mashed potato has a higher GI than a whole baked potato, stone ground whole wheat bread has a lower GI than whole wheat bread.
- Cooking methods — how long a food is cooked (al dente pasta has a lower GI than soft-cooked pasta), frying, boiling and baking.
- Fibre: wholegrains and high-fibre foods act as a physical barrier that slows down the absorption of carbohydrate. This is not the same as ‘wholemeal’, where, even though the whole of the grain is included, it has been ground up instead of left whole. For example, some mixed grain breads that include wholegrains have a lower GI than wholemeal or white bread.
- Fat lowers the GI of a food. For example, chocolate has a medium GI because of it’s fat content, and crisps will actually have a lower GI than potatoes cooked without fat.
- Protein lowers the GI of food. Milk and other diary products have a low GI because they are high in protein and contain fat.
- Variety — converted long-grain white rice has a lower GI than brown rice but short-grain white rice has a higher GI than brown rice.
Starchy foods with a low GI are digested and absorbed more slowly than foods with a high GI. Some factors that influence glycemic properties of foods are listed in Table 2.
Table 2. Food factors influencing glycemic responses
| Nature of the monosaccharide components | |
| Glucose | |
| Fructose | |
| Galactose | |
| Nature of the starch | |
| Amylose | |
| Amylopectin | |
| Starch-nutrient interaction | |
| Resistant starch | |
| Cooking/food processing | |
| Degree of starch gelatinization | |
| Particle size | |
| Food form | |
| Cellular structure | |
| Other food components | |
| Fat and protein | |
| Dietary fibre | |
| Antinutrients | |
| Organic acids | |
What are High in Fiber Foods
Dietary fiber, also known as roughage or bulk, is the part of a plant that the body doesn’t absorb during digestion. Fibre is the part of food that is not digested in the small intestine. Dietary fibre moves largely unchanged into the large intestine or colon where it is fermented by friendly bacteria that live there. The scientific community define dietary fibre as intrinsic plant cell wall polysaccharides of vegetables, fruits and whole-grains, the health benefits of which have been clearly established, rather than synthetic, isolated or purified oligosaccharides and polysaccharides with diverse, and in some cases unique, physiological effects 6. The American Association of Cereal Chemists 7, define “dietary fiber is the edible parts of plants or analogous carbohydrates that are resistant to digestion and absorption in the human small intestine with complete or partial fermentation in the large intestine. Dietary fiber includes polysaccharides, oligosaccharides, lignin, and associated plants substances. Dietary fibers promote beneficial physiological effects including laxation, and/or blood cholesterol attenuation, and/or blood glucose attenuation” 7. The World Health Organization (WHO) and Food and Agriculture Organization (FAO) agree with the American Association of Cereal Chemists International (AACCI) definition but with a slight variation. They state “Dietary fibre means carbohydrate polymers1 with ten or more monomeric units, which are not hydrolysed by the endogenous enzymes in the small intestine of humans and belong to the following categories: that dietary fiber is a polysaccharide with ten or more monomeric units which is not hydrolyzed by endogenous hormones in the small intestine” 8.
Generally speaking, dietary fiber is the edible parts of plants or similar carbohydrates, that are resistant to digestion and absorption in the small intestine. Dietary fiber can be separated into many different fractions. Recent research has begun to isolate these components and determine if increasing their levels in a diet is beneficial to human health. These fractions include arabinoxylan, inulin, pectin, bran, cellulose, β-glucan and resistant starch. The study of these components may give us a better understanding of how and why dietary fiber may decrease the risk for certain diseases 9.
It was considered that the recommended intakes of fruit, vegetables, legumes and regular consumption of whole-grain cereals from Dietary Guidelines for Americans would provide adequate intakes of total dietary fibre 10. Low intakes of dietary fiber are due to low intakes of vegetables, fruits, and whole grains 10.
Dietary fiber and whole grains contain a unique blend of bioactive components including resistant starches, vitamins, minerals, phytochemicals and antioxidants. As a result, research regarding their potential health benefits has received considerable attention in the last several decades. Epidemiological and clinical studies demonstrate that consumption of dietary fiber and whole grain intake is inversely related to obesity 11, type two diabetes 12, cancer 13 and cardiovascular disease 14.
- Eating fibre and wholegrain foods is linked to a lower risk of obesity, type 2 diabetes and heart disease, and may also reduce the risk of bowel cancer.
- Eating high fibre foods can also help prevent constipation – this in turn can help to prevent hemorrhoids.
- Because high fibre foods are filling they may also make it easier to stay at a healthy weight.
- Foods high in fibre are generally good sources of vitamins and minerals, as well as other important nutrients.
The Food and Drug Administration (FDA) has approved two health claims for dietary fiber. The first claim states that, along with a decreased consumption of fats (<30% of calories), an increased consumption of dietary fiber from fruits, vegetables and whole grains may reduce some types of cancer 15. “Increased consumption” is defined as six or more one ounce equivalents, with three ounces derived from whole grains. A one ounce equivalent would be consistent with one slice of bread, ½ cup oatmeal or rice, or five to seven crackers. The second FDA claim supporting health benefits of dietary fiber states that diets low in saturated fat (<10% of calories) and cholesterol and high in fruits, vegetables and whole grain, have a decreased risk of leading to coronary heart disease 16. For most, an increased consumption of dietary fiber is considered to be approximately 25 to 35 g/d, of which 6 g are soluble fiber.
High intake of dietary fiber has been linked to a lower risk of heart disease in a number of large studies that followed people for many years 17. In a Harvard study of over 40,000 male health professionals, researchers found that a high total dietary fiber intake was linked to a 40 percent lower risk of coronary heart disease 18. A related Harvard study of female nurses produced quite similar findings 19.
Higher fiber intake has also been linked to a lower risk of metabolic syndrome, a combination of factors that increases the risk of developing heart disease and diabetes. These factors include high blood pressure, high insulin levels, excess weight (especially around the abdomen), high levels of triglycerides, and low levels of HDL (good) cholesterol. Several studies suggest that higher intake of fiber may offer protective benefits from this syndrome 20, 21.
Diets low in fiber and high in foods that cause sudden increases in blood sugar may increase the risk of developing Type 2 Diabetes. Both Harvard studies—of female nurses and of male health professionals—found that this type of diet more than doubled the risk of type 2 diabetes when compared to a diet high in cereal fiber and low in high-glycemic-index foods 22, 23, 24. A diet high in cereal fiber was linked to a lower risk of type 2 diabetes. Other studies, such as the Black Women’s Health Study 25 and the European Prospective Investigation Into Cancer and Nutrition–Potsdam, have shown similar results.
Recent studies support this inverse relationship between dietary fiber and the development of several types of cancers including colorectal, small intestine, oral, larynx and breast 13, 26, 27. Although most studies agree with these findings, the mechanisms responsible are still unclear. Several modes of actions however have been proposed. First, dietary fiber resists digestion in the small intestine, thereby allowing it to enter the large intestine where it is fermented to produce short chain fatty acids, which have anti-carcinogenic properties 28. Second, since dietary fiber increases fecal bulking and viscosity, there is less contact time between potential carcinogens and mucosal cells. Third, dietary fiber increases the binding between bile acids and carcinogens. Fourth, increased intake of dietary fiber yield increased levels of antioxidants. Fifth, dietary fiber may increase the amount of estrogen excreted in the feces due to an inhibition of estrogen absorption in the intestines 29. Obviously, many studies support the inverse relationship of dietary fiber and the risk for coronary heart disease. However, more recent studies found interesting data illustrating that for every 10 g of additional fiber added to a diet the mortality risk of coronary heart disease decreased by 17–35% 30, 14. Risk factors for CHD include hypercholesterolemia, hypertension, obesity and type two diabetes. It is speculated that the control and treatment of these risk factors underlie the mechanisms behind dietary fiber and coronary heart disease prevention. First, soluble fibers have been shown to increase the rate of bile excretion therefore reducing serum total and LDL “bad” cholesterol 31. Second, short chain fatty acid production, specifically propionate, has been shown to inhibit cholesterol synthesis 32. Third, dietary fiber demonstrates the ability to regulate energy intake thus enhancing weight loss or maintenance of a healthier body weight. Fourth, either through glycemic control or reduced energy intake, dietary fiber has been shown to lower the risk for type two diabetes. Fifth, dietary fiber has been shown to decrease pro-inflammatory cytokines such as interleukin-18 which may have an effect on plaque stability 33. Sixth, increasing dietary fiber intake has been show to decrease circulating levels of C-Reactive protein, a marker of inflammation and a predictor for coronary heart disease 34.
Fiber is found only in plant foods like whole-grain breads and cereals, beans and peas and other vegetables and fruits. Because there are different types of fiber in foods, choose a variety of foods daily. Eating a variety of fiber-containing plant foods is important for proper bowel function, can reduce symptoms of chronic constipation, diverticular disease, and hemorrhoids, and may lower the risk for heart disease and some cancers. However, some of the health benefits associated with a high-fiber diet may come from other components present in these foods, not just from fiber itself. For this reason, fiber is best obtained from foods rather than supplements.
Dietary fiber can be separated into many different fractions. Recent research has begun to isolate these components and determine if increasing their levels in a diet is beneficial to human health. These fractions include arabinoxylan, inulin, pectin, bran, cellulose, β-glucan and resistant starch. The study of these components may give us a better understanding of how and why dietary fiber may decrease the risk for certain diseases 35.
Types of Dietary Fiber
Many people think that if a food is rich in fibre it will automatically be low GI, but that’s not the case at all. To begin with, there’s not just one type of dietary fibre – there are many different kinds and is typically divided into three main categories: soluble fibre, insoluble fibre and resistant starch. In addition, processing makes a big difference to fibre’s digestibility. The American Association of Cereal Chemists 36, define “dietary fiber is the edible parts of plants or analogous carbohydrates that are resistant to digestion and absorption in the human small intestine with complete or partial fermentation in the large intestine. Dietary fiber includes polysaccharides, oligosaccharides, lignin, and associated plants substances. Dietary fibers promote beneficial physiological effects including laxation, and/or blood cholesterol attenuation, and/or blood glucose attenuation” 7. The World Health Organization (WHO) and Food and Agriculture Organization (FAO) agree with the American Association of Cereal Chemists International (AACCI) definition but with a slight variation. They state “Dietary fibre means carbohydrate polymers1 with ten or more monomeric units, which are not hydrolysed by the endogenous enzymes in the small intestine of humans and belong to the following categories: that dietary fiber is a polysaccharide with ten or more monomeric units which is not hydrolyzed by endogenous hormones in the small intestine” 8.
Table 3. Components of dietary fiber according to the American Association of Cereal Chemists
| Non Starch Polysaccharides and Oligosaccharides | |
| Cellulose | |
| Hemicellulose | |
| Arabinoxylans | |
| Arabinogalactans | |
| Polyfructoses | |
| Inulin | |
| Oligofructans | |
| Galacto-oligosaccharides | |
| Gums | |
| Mucilages | |
| Pectins | |
| Analagous carbohydrates | |
| Indigestible dextrins | |
| Resistant maltodextrins | |
| Resistant potato dextrins | |
| Synthesized carbohydrates compounds | |
| Polydextrose | |
| Methyl cellulose | |
| Hydroxypropylmethyl cellulose | |
| Resistant starches | |
| Lignin substances associated with the Non Starch Polysaccharides (NSP) and lignin complex | |
| Waxes | |
| Phytate | |
| Cutin | |
| Saponins | |
| Suberin | |
| Tannin | |
Recent research suggests that fiber should be categorized by its physical characteristics; how well it dissolves (solubility), how thick it is (viscosity) and how well it breaks down (fermentability). Some commonly known terms are described below:
- Soluble fiber including pectins and beta glucans is found in foods like oats, peas, beans, apples, citrus fruits, carrots, barley and psyllium. Soluble fiber dissolves in water to form a gel-like material. It can help lower blood cholesterol and glucose levels. Foods high in soluble fiber can help you feel full. They also help reduce constipation by speeding up the time it takes for feces (poop) to pass through your body. Soluble dietary fiber has been associated with lower postprandial glucose levels and increased insulin sensitivity in diabetic and healthy subjects; these effects were generally attributed to the viscous and/or gelling properties of soluble fiber 37. Soluble dietary fiber exerts physiological effects on the stomach and small intestine that modulate postprandial glycemic responses, including delaying gastric emptying 38, which accounts for ~35% of the variance in peak glucose concentrations following the ingestion of oral glucose 39, modulating gastrointestinal myoelectrical activity and delaying small bowel transit 40, 41, reducing glucose diffusion through the unstirred water layer 42, and reducing the accessibility of α-amylase to its substrates due to the increased viscosity of gut contents 43. Notably, the increased viscosity and gel-forming properties of soluble fiber are predominantly responsible for its glycemic effect, since the hypoglycemic effect can be reversed by the hydrolysis of guar gum or following ultra-high heating and homogenization 38. In addition, the intestinal absorption of carbohydrates was prolonged by soluble dietary fiber, which was partially due to altered incretin levels, including increased glucagon-like peptide 1 levels 43. In experimental clamp studies, soluble dietary fiber also influenced peripheral glucose uptake mechanisms 44, 45, including increasing skeletal muscle expression of the insulin-responsive glucose transporter type 4 (GLUT-4), which enhances skeletal muscle uptake, augments insulin sensitivity and normalizes blood glucose 45. In humans, various fatty acids stimulate the expression of peroxisome proliferator-activated receptor-γ, which increases adipocyte GLUT-4 levels 46. A more recent study to find out the health benefits of soluble fiber on type 2 diabetes 47. A total of 117 patients with type 2 diabetes between the ages of 40 and 70 were assessed. Patients were randomly assigned to one of two groups, and administered extra soluble dietary fiber (10 or 20 g/day), or to a control group (0 g/day) for one month. The 20 g/day soluble dietary fiber group exhibited significantly improved fasting blood glucose and low-density (LDL) lipoprotein “bad cholesterol” levels, as well as a significantly improved insulin resistance index. In addition, 10 and 20 g/day soluble dietary fiber significantly improved the waist and hip circumferences and levels of triglycerides and apolipoprotein A. The results of the present study suggested that increased and regular consumption of soluble dietary fiber led to significant improvements in blood glucose levels, insulin resistance and metabolic profiles 47.
- Insoluble fiber including cellulose is found in wheat bran and nuts. Insoluble fiber is a type of fibre that doesn’t dissolve in water. Because insoluble fiber absorbs water, it helps to soften the contents of your bowel, contributing to keep the bowels regular. Insoluble fiber promotes the movement of material through your digestive system and increases stool bulk, so it can be of benefit to those who struggle with constipation or irregular stools. Whole-wheat flour, wheat bran, nuts, beans and vegetables, such as cauliflower, green beans and potatoes, are good sources of insoluble fiber. Diverticulitis, an inflammation of the intestine, is one of the most common age-related disorders of the colon in Western society. Among male health professionals in a long-term follow-up study, eating dietary fiber, particularly insoluble fiber, was associated with about a 40 percent lower risk of diverticular disease 48.
- Resistant starch is a soluble fiber that is highly fermentable in the gut. While most starch is digested in the upper part of the gut, resistant starch resists digestion in the small intestine and so goes all the way to the large intestine 49. Once in the large intestine, good bacteria ferment resistant starch. This process produces short chain fatty acids (SCFAs) and gasses that help to keep the lining of the bowel healthy. Resistant starch is starch that is not easily absorbed. Different ways of cooking can create different amounts of resistant starch. For example, resistant starch is found in slightly undercooked (‘al dente’) pasta, cooked but cooled potatoes (including potato salad), cooked and cooled grains like rice, quinoa, barley and buckwheat, under-ripe bananas, beans, lentils and a product called Hi-maize used in some breads and breakfast cereals. Freekeh, a Middle Eastern grain available in some supermarkets, is another good source. In general, foods that are less highly processed contain more resistant starch. An important benefit of resistant starch is that it ferments, which produces substances that help to keep the lining of the bowel healthy. Resistant starch has been classified into five basic “types” 50.
- Type 1 (resistant starch 1) is made up of starch granules surrounded by an indigestible plant matrix.
- Type 2 (resistant starch 2) occurs in its natural form such as in an uncooked potato and high amylose maize.
- Type 3 (resistant starch 3) are crystallized starches made by unique cooking and cooling processes.
- Type 4 (resistant starch 4) is a starch chemically modified by esterification, crosslinking, or transglycosylation and is not found in nature.
- Type 5 (resistant starch 5) is a starch consisting of amylose-lipid complex.
- Prebiotics are types of carbohydrate that only our gut bacteria can feed upon. Some examples are onions, garlic, asparagus and banana.
Table 4. Types of resistant starches
| Designation | Description | Example | Reference |
| Type 1 (resistant starch 1) | Physically inaccessible starch | Coarsely ground or whole-kernel grains | 51 |
| Type 2 (resistant starch 2) | Granular starch with the B- or C-polymorph | High-amylose maize starch, raw potato, raw banana starch | 51 |
| Type 3 (resistant starch 3) | Retrograded starch | Cooked and cooled starchy foods | 52 |
| Type 4 (resistant starch 4) | Chemically modified starches | Cross-linked starch and octenyl succinate starch | 53 |
| Type 5 (resistant starch 5) | Amylose-lipid complex | Stearic acid-complexed high-amylose starch | 54 |
Footnote: 1RSI, type I resistant starch; (RS); RSII, type II resistant starch; RSIII, type III resistant starch; RSIV, type IV resistant starch; RSV; type V resistant starch.
[Source 50 ]Arabinoxylan
Arabinoxylan, a constituent of hemicelluloses, is comprised of a xylose backbone with arabinose side chains. Arabinoxylan is a major component of dietary fiber in whole grains having considerable inclusions in both the endosperm and bran. In wheat, Arabinoxylan account for around 64–69% of the structural carbohydrates (complex carbohydrates, non-starch polysaccharide are resistant to digestion in the small intestine and require bacterial fermentation located in the large intestine) in the bran and around 88% in the endosperm 55. During normal wheat flour processing, a majority of the arabinoxylan is removed as a by-product. In the GI tract, arabinoxylan acts much like a soluble fiber being rapidly fermented by the microflora of the colon.
Lu et al. 56, observed an inverse relationship between the intake level of an arabinoxylan rich bread and postprandial glucose response in healthy adult subjects. When compared to the control, postprandial glucose levels were significantly lower with only 6 g of arabinoxylan rich fiber supplementation while 12 g produced the greatest benefit. Breads high in arabinoxylan also appear to control blood glucose and insulin in adults with an already impaired glucose tolerance 57. Fasting blood glucose, postprandial blood glucose and insulin were all significantly lower when adults with type two diabetes were supplemented with 15 g/d of an arabinoxylan rich fiber. The mode of action behind arabinoxylan on improving glucose tolerance is unknown. However, it is thought to be due to the high viscosity of the fiber inside the lumen of the GI tract, thereby slowing the rate of glucose absorption.
The lower glycemic index of arabinoxylan may also play a role. Breads made with a flour rich in arabinoxylan have a relatively low glycemic index of around 59. Whole wheat flour, although high in fiber, has a glycemic index of around 99 56. Arabinoxylan rich bread has a similar glycemic index to that of whole grain bread but offers some distinct advantages such as improved mouth feel and tenderness. There was no significant difference in the sensory analysis between the control and a bread containing 14% arabinoxylan rich fiber 56.
Inulin
Inulin is a polymer of fructose monomers and is present in such foods as onions, garlic, wheat, artichokes and bananas and is used to improve taste and mouthfeel in certain applications. It is also used as a functional food ingredient due to its nutritional properties. Because of this, inulin products can be used as a replacement for fat or soluble carbohydrates without affecting the taste and texture and still contribute to a foods nutritional value.
Enzymatic hydrolyses in the small intestine is minimal (<10%) since inulin consists of beta bonds. Therefore, it enters the large intestine and is almost completely metabolized by the microflora. When fermented, they tend to favor propionate production which, in turn, decreases the acetate to propionate ratio leading to decreased total serum cholesterol and LDL 32, which are important risk factors for coronary heart disease.
Inulin has also demonstrated the ability to contribute to the health of the human large intestine as a prebiotic 58. They demonstrated that inulin stimulated the growth of bifidobacteria while restricting the growth of potential pathogenic bacteria such as E. coli, Salmonella, and Listeria. This could prove to be beneficial in such disorders as ulcerative colitis and C. difficile infections. Rafter et al. 59 agreed with these findings and suggested they were the underlying mechanisms behind the observation that inulin decreased biological compounds associated with colonic cancer, including reduced colorectal cell proliferation and water induced necrosis, decreased exposure to genotoxins, and decreased interleukin-2 release.
Increased mineral absorption may also contribute to the functionality of inulin. Increased calcium absorption, by approximately 20%, was reported in adolescent girls supplemented with inulin 60. Results from Abrams et al. 61, support these findings in a longer (one year) study of pubertal boys and girls consuming an inulin supplement. Subjects in the treatment group also experienced increased bone mineral density when compared to the control. The mechanisms behind these findings are still unclear but may be due to increased calcium absorption from the colon or possibly an increased solubility in the lumen of the GI tract due to short chain fatty acids. Finally, it may increase absorption through an enhancement of vitamin D.
Inulin may also provide a way to prevent and treat obesity. Cani et al. 62 demonstrated that oligofructose, a subgroup of inulin, increased satiety in adults which led to a decrease in total energy intake. This is thought to be due to short chain fatty acids and their ability to increase appetite suppressing hormones such as glucagon-like peptide 1 (GLP-1).
Beta-glucan
Beta-glucan (β-glucan) is a linear polysaccharide of glucose monomers with β(1→4) and β(1→3) linkages and found in the endosperm of cereal grains, primarily barley and oats. β-glucan concentrations in North American oat cultivars range from 3.9% to 6.8% 63. β-glucan is water soluble and highly viscous at low concentrations 63.
The physiological benefits due to β-glucan seem to stem from their effect on lipid metabolism and postprandial glucose metabolism. Many studies agree an inverse relationship exists between consumption levels of β-glucan and cholesterol levels. Several recent studies, in both hypercholesterolemic 64 and healthy 65 subjects, found that the daily consumption of 5 g of β–glucan significantly decreased serum total and LDL cholesterol. Davidson et al. 66 found that only a daily consumption of 3.6 g β-glucan was needed to produce the same significant effects. The same relationship also has been reported to occur between β-glucan and postprandial glucose and insulin responses in both diabetic and healthy subjects. Biorklund et al. 67 found that 5 g of β-glucan from oats significantly decreased postprandial glucose and insulin levels in healthy adults. Tappy et al. 68 reported the same results in adult subjects diagnosed with type two diabetes who consumed 4.0, 6.0 or 8.4 g of β-glucan.
Most authors agree that β-glucan’s viscosity in the GI tract is the most probable mechanism in which it decreases serum cholesterol levels as well as improves post prandial glucose metabolism. This gellation property may decrease bile acid absorption by increasing intestinal viscosity and increase bile acid excretion. This subsequently results in a higher hepatic cholesterol synthesis because of the higher need for bile acid synthesis 69. The same viscosity may also delay glucose absorption into the blood thus lowering post prandial glucose and insulin levels. Nazare et al. 70 observed that 5 g of oat β–glucan added to an oat concentrate cereal significantly delayed, but did not reduce, total glucose absorption.
The production of short chain fatty acids from β-glucan may also be a probable mechanism behind its observed metabolic effects. Fermentation of oat β-glucan has been shown to yield larger amounts of propionate 71, 72. Propionate has been shown to significantly inhibit cholesterol synthesis in humans 32 and is thought to be due to the inhibition of the rate limiting enzyme HMG CoA reductase 73.
Not all research however, agrees that β-glucan can affect lipid and glucose absorption/metabolism. Keogh et al. 74 observed that treatments of 8.1 to 11.9 g/d of barley β-glucan had no effect on total or LDL cholesterol in mildly hyperlipidemic adults. Cugent-Anceau et al. 75 not only observed that 3.5 g of oat β-glucan added to soup did not alter serum lipid profiles, but also produced no change in postprandial glucose levels.
Pectin
Pectin is a linear polymer of galacturonic acid connected with α (1→4) bonds. Regions of this backbone are substituted with α (1→2) rhamnopyranose units from which side chains of neutral sugars such as galactose, mannose, glucose and xylose occur. Pectin is a water soluble polysaccharide that bypasses enzymatic digestion of the small intestine but is easily degraded by the microflora of the colon. Citrus fruit contains anywhere from 0.5% to 3.5% pectin with a large concentration located in the peel. Commercially extracted pectins are also available and are typically used in food applications which require a gelling or a thickening agent.
Inside the GI tract, pectin maintains this ability to form a gel or thicken a solution. This is thought to be the likely mechanism behind its many beneficial effects on health including dumping syndrome, improved cholesterol and lipid metabolism and diabetes prevention and control. However, pectin also contains some unique abilities that may treat or prevent other diseases/disorders such as intestinal infections, atherosclerosis, cancer and obesity.
Several recent clinical studies, demonstrated that oral pectin supplementation to children and infants reduced acute intestinal infections and significantly slowed diarrhea. This is thought to be due to a reduction in pathogenic bacteria such as Shigella, Salmonella, Klebsiella, Enterobacter, Proteus and Citrobacter. This is supported by Olano–Martin et al. 76 who observed that pectin stimulated the growth of certain strains of Bifidobacteria and Lactobacillus in vitro. These bacteria are considered to be directly related to the health of the large intestine and their concentrations depict a healthy microflora population.
The quality of fibrin is thought to be an important risk factor for atherosclerosis, stroke and coronary heart disease. Pectin has been shown to increase fibrin permeability and decrease fibrin tensile strength in hyperlipidaemic men. Although the mechanism behind this is unknown, it is thought to be due in part to acetate production. Pectin yields predominantly acetate in the colon which is thought to enter peripheral circulation and alter fibrin architecture.
Pectin may also have a potential role in the complicated area of cancer prevention. Nangia–Makker et al. 77 found that pectin was able to bind to and decrease tumor growth and cancerous cell migration in rats fed modified citrus pectin. This is thought to be a result of pectin binding to galectin-3 and inhibiting some of its functions.
Bran
Bran is the outer most layer of a cereal grain and consists of the nucellar epidermis, seed coat, pericarp and aleurone. The aleurone consists of heavy walled, cube shaped cells which are composed primarily of cellulose. It is low in starch and high in minerals, protein, and fat. However, due to its thick cellulosic walls, these nutrients are virtually unavailable for digestion in monogastric species. The AACC defines oat bran as “the food which is produced by grinding clean oat groats or rolled oats and separating the resulting oat flour by sieving bolting, and/or other suitable means into fractions such that the oat bran fraction is not more than 50% of the original starting material and has a total betaglucan content of at least 5.5% (dry-weight basis) and a total dietary fiber content of at least 16.0% (dry-weight basis), and such that at least one-third of the total dietary fiber is soluble fiber.”
Bran from a wide array of cereal grains have been shown to have an effect on postprandial glucose levels, serum cholesterol, colon cancer, and body mass. Although the efficacy of bran may change due to its source, the purpose of this section will just evaluate bran’s general effect on the parameters listed above.
In a recent study of healthy adults, 31 g of rye bran decreased peak postprandial glucose levels by 35% when compared to the control 78. This effect may be due to the high arabinoxylan content in rye bran. Arabinoxylan, as discussed previously, may increase intestinal viscosity and slow nutrient absorption. In a more lengthy study, Qureshi et al. 79 found that subjects suffering type one and two diabetes decreased their fasting glucose levels due to the daily consumption of 10 g of stabilized rice bran over two months. The results may arise due to an increased intestinal viscosity, but is more likely a result of a decreased carbohydrate/caloric intake. Koh-Banerjee et al. 80, in a larger clinical study, supports this theory in their finding that for every 20 g/d increase in consumption of bran, body weight decreased by 0.80 lbs. It should be noted that this data remained significant even after adjustment for fat and protein intake, daily activity, caloric intake and baseline weight. In an earlier study, Zhang et al. 81 observed that adults with ileostomies, consuming bread rich in rye bran, significantly increased the ileal excretion of fat, nitrogen and energy. This study suggests bran did not delay nutrient absorption in the small intestine but hindered it.
In addition to a possible effect on carbohydrate absorption and metabolism, bran also seems to have the same effect on lipids. In a long term clinical study, Jensen et al. 82 reported that an increased daily consumption of bran significantly decreased the risk of coronary heart disease in healthy adult men. This is most likely due to the data reported by Qureshi et al. 79 who found that 10 g of rice bran consumed for eight weeks was able to decrease serum total cholesterol, LDL cholesterol and triglycerides. The mechanisms behind these effects may be two fold. The reduction in cholesterol levels is likely due to an increase in bile acid synthesis. Andersson et al. 83 found that oat bran doubled the serum concentration of 7α-hydroxy-4-cholesten-3-one (α-HC), which is a metabolite in the synthesis of bile acids that is oxidized from 7α-hydroxycholesterol. The reduction in serum triglyceride levels may be a result of a decreased absorption of fat from the small intestine.
Cellulose
Cellulose is a linear chain of β(1→4) linked glucose monomers and is the structural component of cell walls in green plants and vegetables. It is water insoluble and inert to digestive enzymes in the small intestine. However, it can go through microbial fermentation to a certain degree in the large intestine in turn producing short chain fatty acid.
Natural cellulose can be divided into two groups: Crystalline and amorphous. The crystalline component, which is made up of intra and intermolecular non covalent hydrogen bonds, make cellulose insoluble in water. However, many modified celluloses such as powdered cellulose, microcrystalline cellulose and hydroxypropylmethyl cellulose have been developed and are used as food ingredients. The difference between natural and modified celluloses is the extent of crystallization and hydrogen bonding. When these hydrogen bonds are disrupted and the crystallinity is lost, the cellulose derivative becomes water soluble 83.
Little research has been conducted evaluating the effects of cellulose in humans. Therefore, studies in other models such as the rat will be discussed. The translation to human relevance is poorly understood and debatable. Cellulose pills have been made available for human consumption with the theory that cellulose may decrease a person’s caloric intake. Although no human studies could be found to support this, several animal studies using cats, dogs and rats have shown that increasing dietary cellulose can reduce daily energy intake. This is most likely a dilution factor since cellulose is virtually undigested in the small intestine and only 51% metabolized by the microflora of the colon.
Many studies have evaluated the effect of cellulose on blood glucose and insulin levels in many different models. However, the data is extremely contradictory and may depend on the subject, type of cellulose and other unknown factors. Using the rat, dog and cat, natural cellulose was shown to decrease postprandial glucose and insulin levels. However, similar studies in pigs and humans 84 demonstrated that natural cellulose had no effect on these parameters. Studies using modified celluloses showed more consistent data. Microcrystalline cellulose has shown the ability to decrease blood glucose levels in the pig and rat. Complimenting this, methylcellulose had demonstrated the same effects in humans. Lightowler and Henry 85 found that adding only 1% high viscosity hydroxypropylmethylcellulose (HV-HPMC) to mashed potatoes decreased postprandial glucose levels by 37% in healthy adults. Also, Maki et al. 86 reported an acute 35% reduction in postprandial blood glucose due to 4 g of HV-HPMC in overweight subjects.
Modified cellulose has also been reported to effect lipid metabolism. Maki et al. 87, 88 both observed a significant reduction in total and LDL cholesterol in hypercholesterolemic adults consuming 5 g/d of HV-HPMC for four weeks. Interestingly, in subjects already receiving statin drugs, HV-HPMC was able to further reduce total and LDL cholesterol.
According to this, modified celluloses may be more beneficial than natural cellulose. These modified celluloses, as described above, act like soluble fiber thus adding to the viscosity of the GI tract. Therefore, it is assumed that increased intestinal viscosity delays nutrient absorption and increases bile acid excretion.
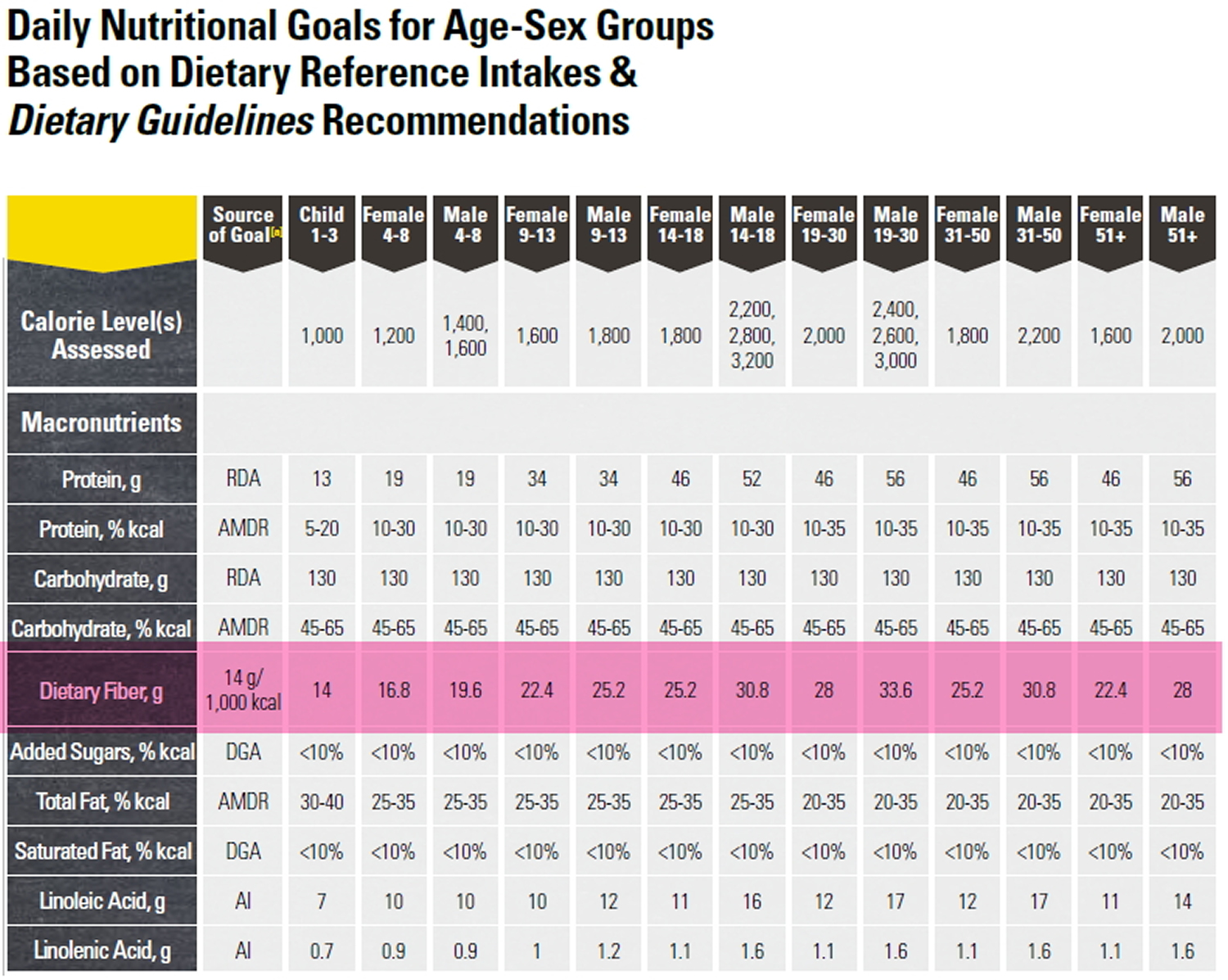
How much fiber do you need?
Depending on your age and sex, adults should get 25 to 31 grams of fiber a day 89. Older adults sometimes don’t get enough fiber because they may lose interest in food.
- Men over the age of 50 should get at least 38 grams of fiber per day.
- Women over the age of 50 should get 25 grams per day.
- Children ages 1 to 3 should get 19 grams of fiber per day.
- Children between 4 and 8 years old should get 25 grams per day.
- Girls between 9 and 18 should get 26 grams of fiber each day. Boys of the same age range should get between 31 and 38 grams of fiber per day.
To get enough fiber every day, the U.S. Department of Health and Human Services 10 recommends that an individual eats:
- at least 4 serves of wholegrain or wholemeal foods every day (or ensure about half of your daily serves of breads and cereals are wholegrain or wholemeal varieties)
- at least 2 serves of fruit daily
- 5 serves of vegetables daily including legumes (also known as ‘pulses’)
- wholefoods rather than dietary fiber supplements as the benefits of fiber from food may be from the combination of nutrients in food working together.
Table 5. Below is an example of how an adult may meet their daily dietary fiber requirements:
| Food | Fiber Content |
| 3/4 cup whole grain breakfast cereal | 4.5g |
| 2 slices wholemeal bread | 4.5g |
| 1 apple (with skin) and 1 orange | 5.5g |
| 2 cups mixed raw vegetables | 10g |
| 1/4 cup legumes eg. baked beans | 3g |
| Total | 27.5g |
Footnote: Daily recommended fiber intake are highlighted in pink. (Source: U.S. Department of Health and Human Services and U.S. Department of Agriculture: Dietary Guidelines for Americans 2015-2020 10 ] [Source 90 ]
Tips for including more fiber in your diet
- Know which packaged foods are high in fibre by reading the nutrient panel on the pack. A food with at least 4g fibre per serve is a good source; food with at least 7g fibre per serve is an excellent source.
- Enjoy wholegrain, wholemeal or mixed grain toast instead of white.
- Use wholegrain pasta instead of white pasta.
- Try brown rice or quinoa instead of white rice with casseroles or curries.
- Use wholemeal flour to thicken sauces, gravies and stews.
- Try wholegrain or wholemeal crisp breads with toppings such as creamed corn or salsa dip.
- For breakfast choose a high-fiber breakfast cereal — 5 or more grams of fiber a serving. Opt for cereals with “whole grain,” “bran” or “fiber” in the name. Or add a few tablespoons of unprocessed wheat bran to your favorite cereal.
- Switch to whole grains. Consume at least half of all grains as whole grains. Look for breads that list whole wheat, whole-wheat flour or another whole grain as the first ingredient on the label and have at least 2 grams of dietary fiber a serving. Experiment with brown rice, wild rice, barley, whole-wheat pasta and bulgur wheat.
- Bulk up baked goods. Substitute whole-grain flour for half or all of the white flour when baking. Try adding crushed bran cereal, unprocessed wheat bran or uncooked oatmeal to muffins, cakes and cookies.
- Lean on legumes. Beans, peas and lentils are excellent sources of fiber. Add kidney beans to canned soup or a green salad. Or make nachos with refried black beans, lots of fresh veggies, whole-wheat tortilla chips and salsa.
- Eat more fruit and vegetables. Fruits and vegetables are rich in fiber, as well as vitamins and minerals. Try to eat five or more servings daily.
- Make snacks count. Fresh fruits, raw vegetables, low-fat popcorn and whole-grain crackers are all good choices. A handful of nuts or dried fruits also is a healthy, high-fiber snack — although be aware that nuts and dried fruits are high in calories.
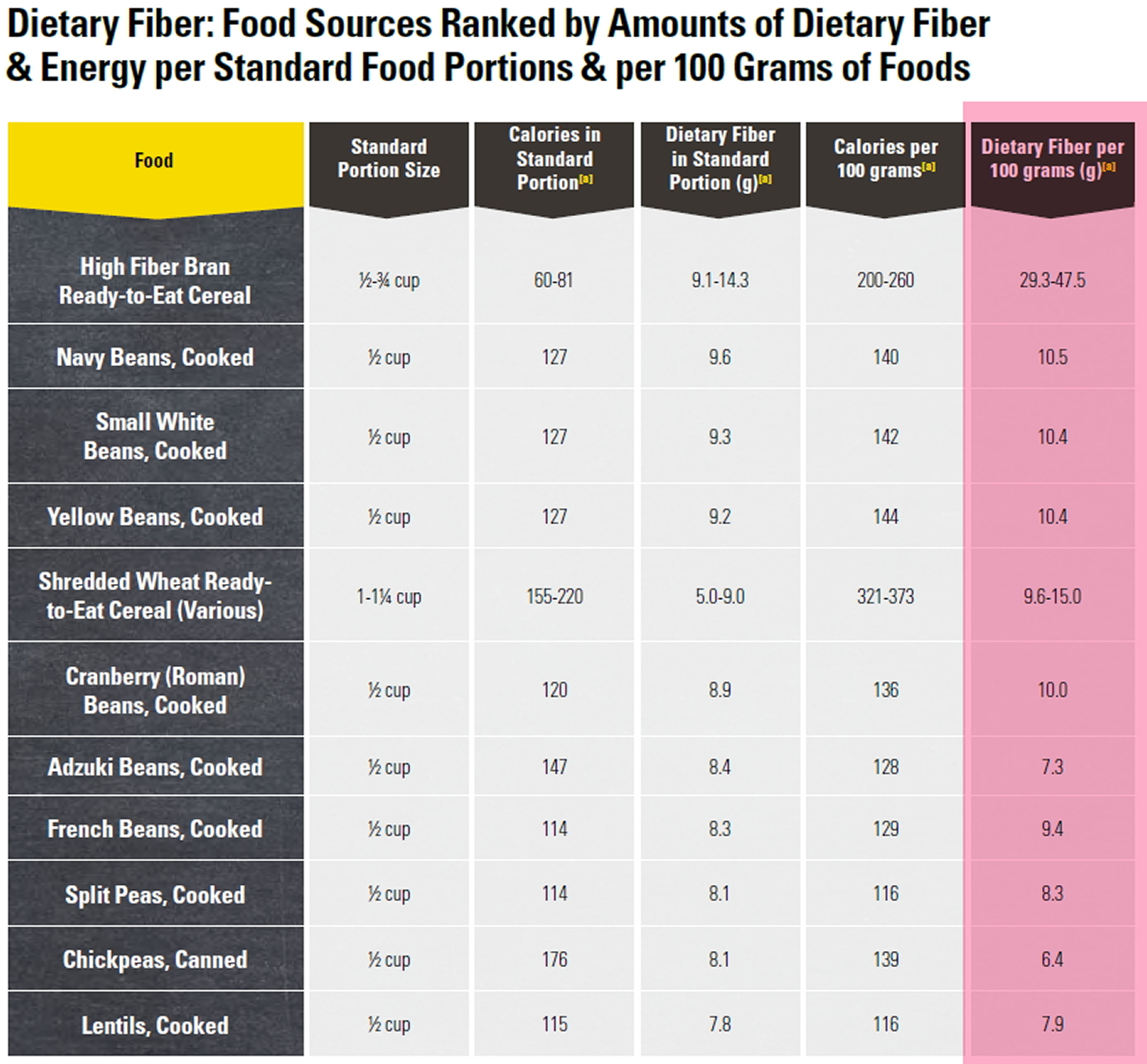
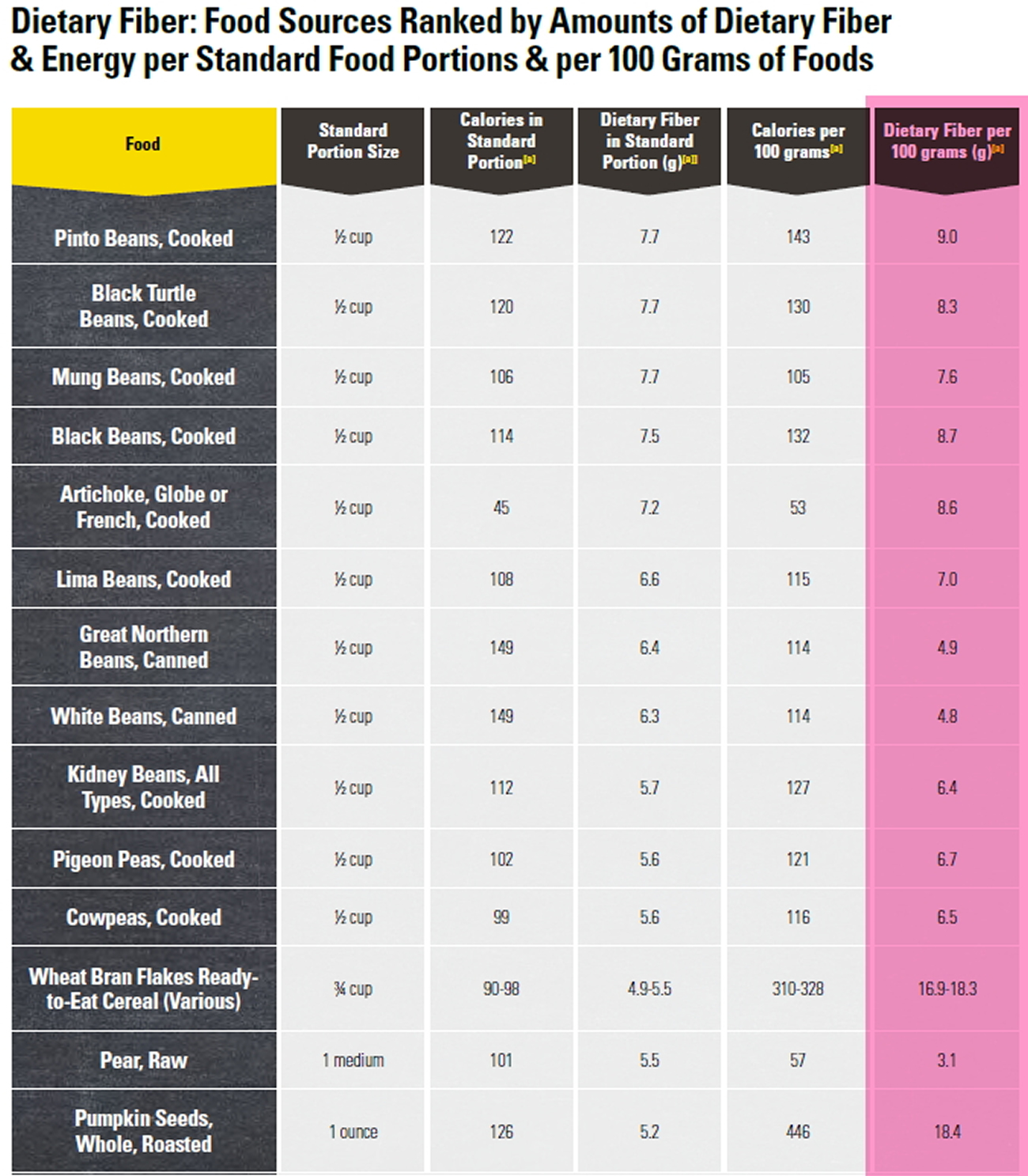
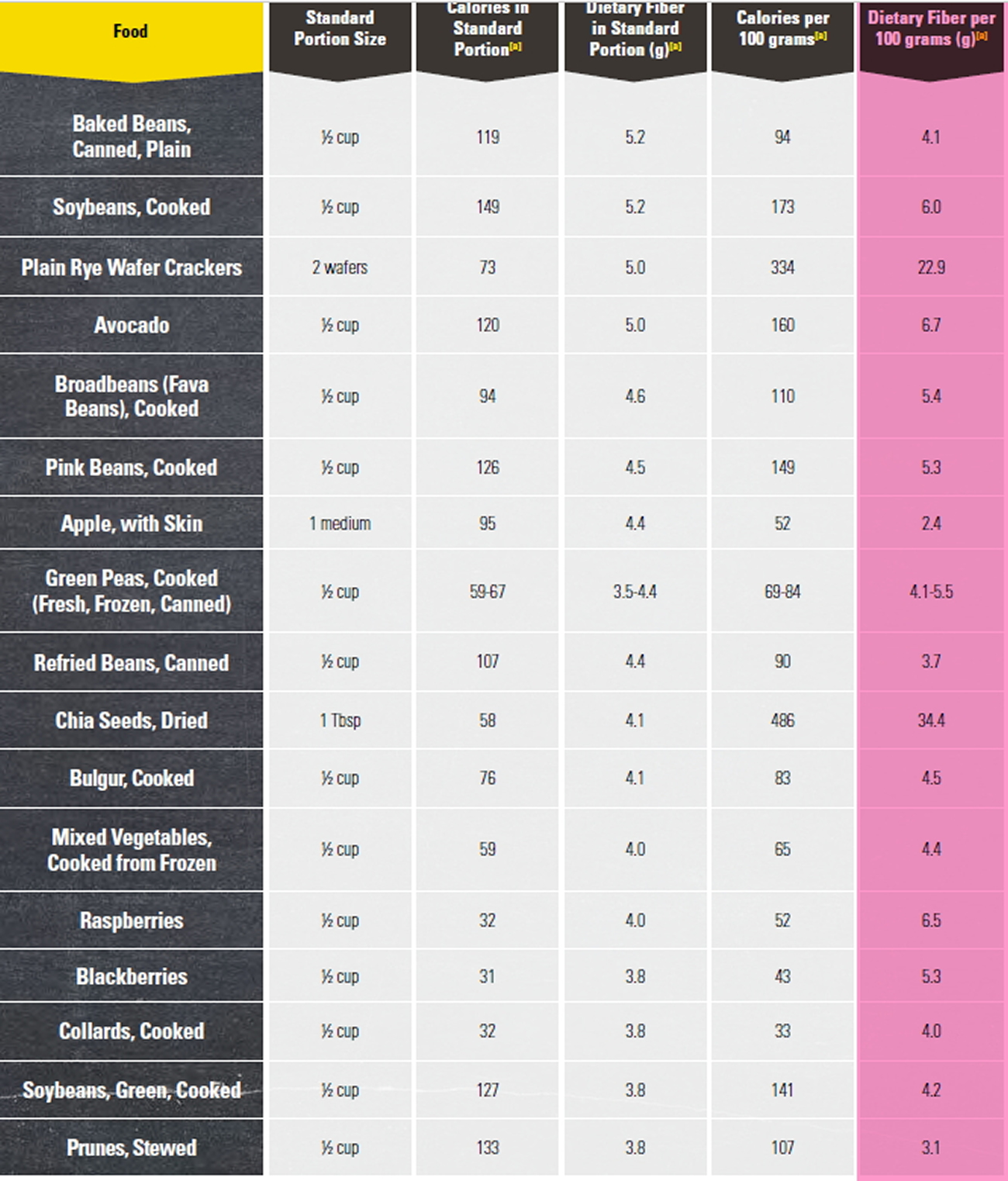
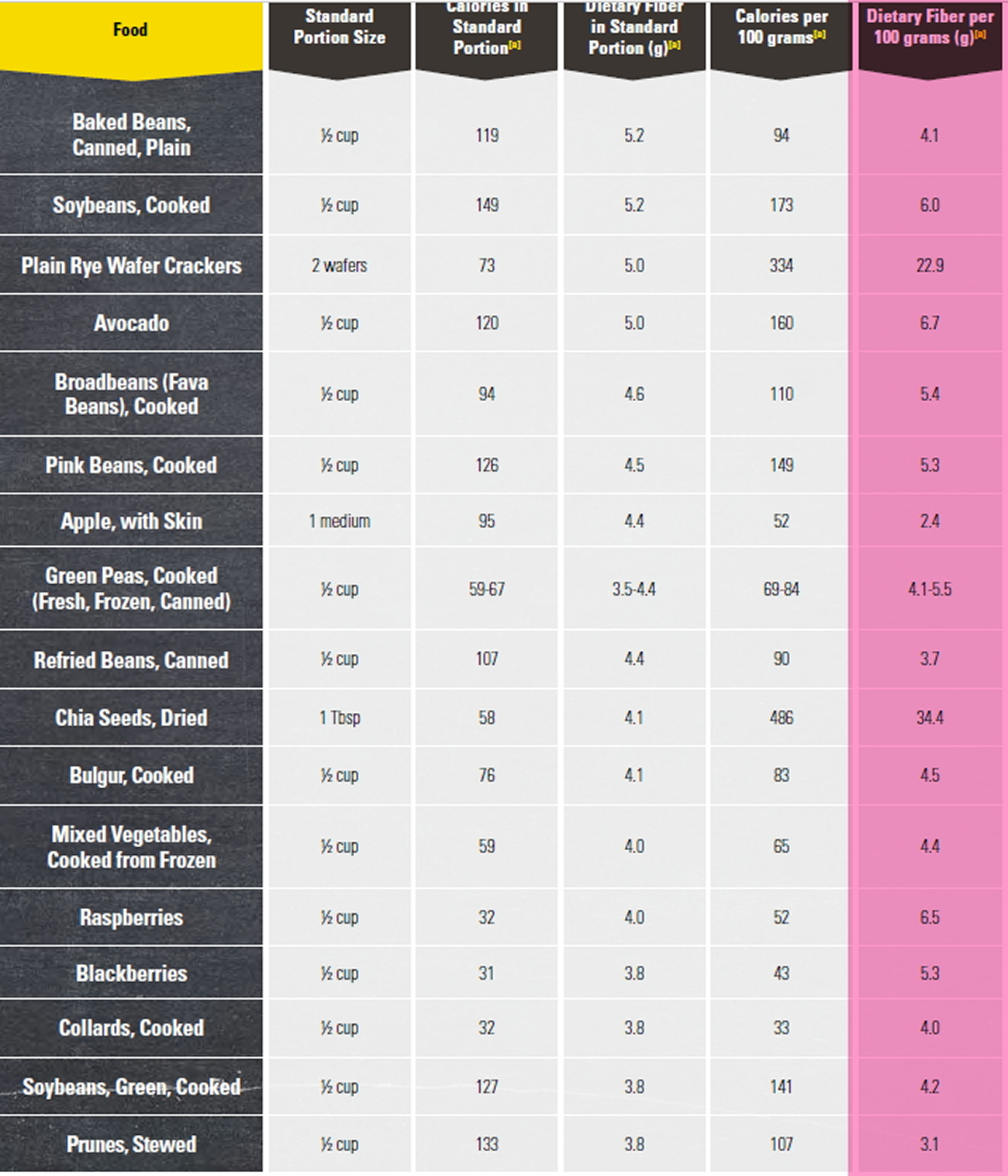
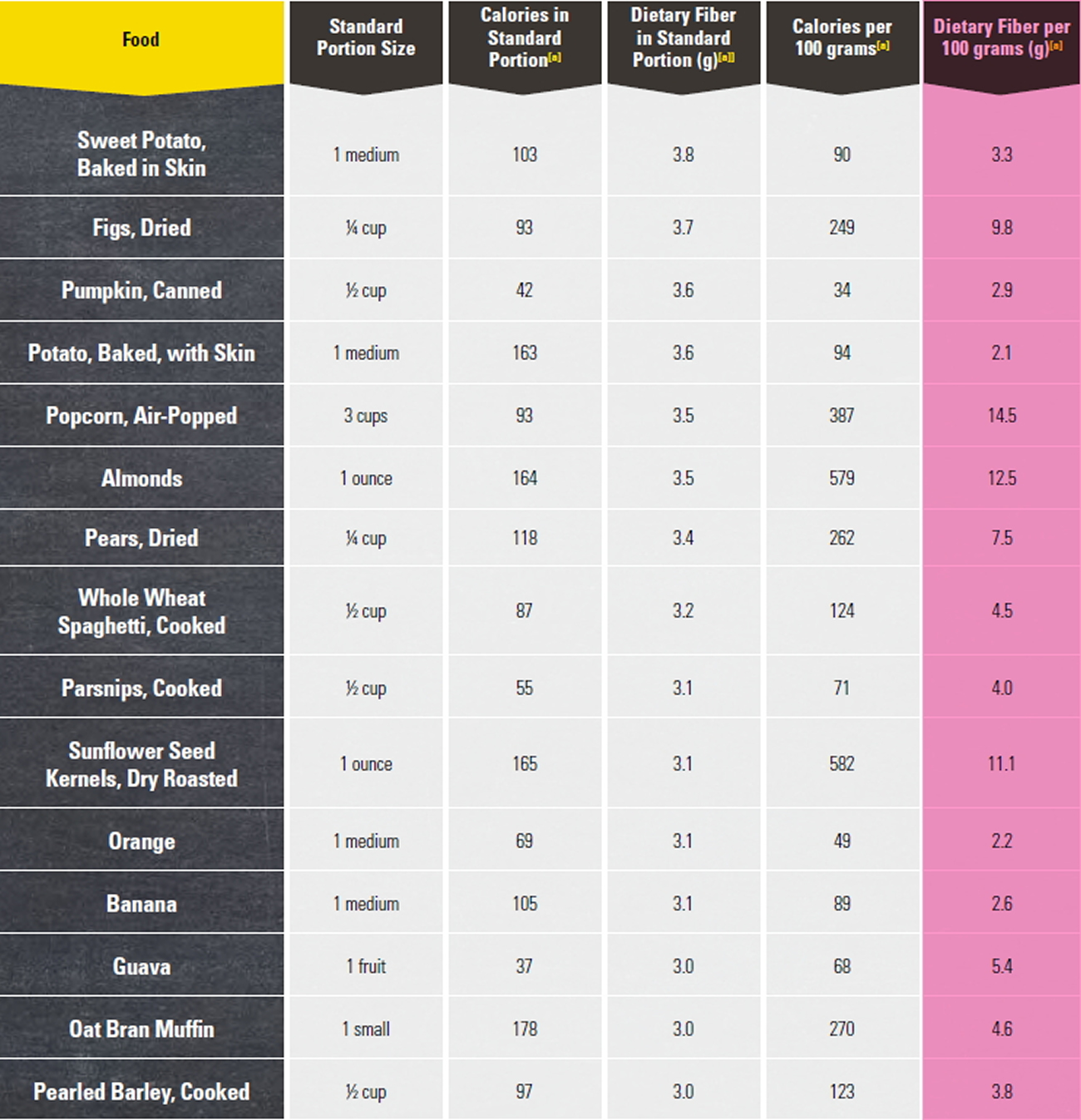
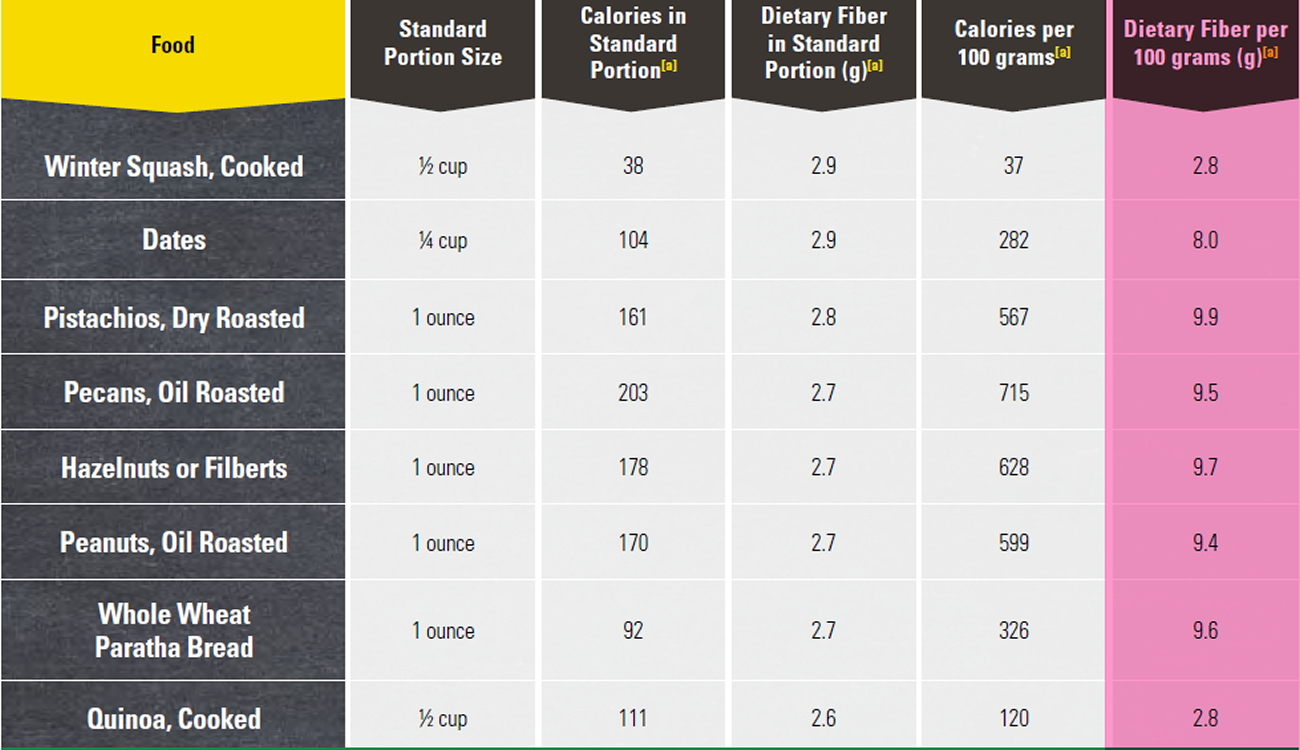
Foods High in Fiber
Good sources of dietary fiber include:
- Pulses (like lentils and peas) and beans and legumes (think navy beans, small white beans, split peas, chickpeas, lentils, pinto beans)
- Fruits and vegetables, vegetables such as carrots, broccoli, green peas, and collard greens; fruits especially those with edible skin (like pears and apples with the skin on) and those with edible seeds (like berries)
- Nuts—try different kinds (pumpkin seeds, almonds, sunflower seeds, pistachios and peanuts are a good source of fiber and healthy fats, but be mindful of portion sizes, because they also contain a lot of calories in a small amount!)
- Whole grains such as:
- Quinoa, barley, bulgur, oats, brown rice and farro
- Whole wheat pasta
- Whole grain cereals, including those made from whole wheat, wheat bran and oats
Choose fiber rich foods from a variety of sources including wholegrains, fruit and vegetable, nuts and seeds, beans and pulses. When you read food labels check for the grams of fiber per serving or per 100g. Foods that are naturally high in fiber and contain at least 3 grams per 100 gram are often labeled as a “good source,” and foods labeled as “excellent source” contain more than 5 grams of fiber per serving.
Keep in mind that if you haven’t been eating a lot of foods high in fiber on a daily basis, it’s important to increase your intake slowly to allow your body to adjust. A sudden increase in eating foods high in fiber (especially foods with added fiber or when using supplements) can cause gas, bloating or constipation. Be sure you are drinking enough water too, because fiber needs water to move through your body, making your stool soft and bulky.
It is now known that diets rich in fiber are generally low in saturated fat and many national authorities including the U.S. Department of Health and Human Services and U.S. Department of Agriculture in their Dietary Guidelines for Americans 10 recommended you eat whole grains, vegetables, and fruits as parts of healthy diet and greater consumption of grain products to control weight 10. Whole grains may have beneficial effects on weight control through promoting satiety 91, 92, 93. Healthy eating patterns include whole grains and limit the intake of refined grains and products made with refined grains, especially those high in saturated fats, added sugars, and/or sodium, such as cookies, cakes, and some snack foods. The grains food group includes grains as single foods (e.g., rice, oatmeal, and popcorn), as well as products that include grains as an ingredient (e.g., breads, cereals,
crackers, and pasta). Grains are either whole or refined. Whole grains (e.g., brown rice, quinoa, and oats) contain the entire kernel, including the endosperm, bran, and germ. Refined grains differ from whole grains in that the grains have been processed to remove the bran and germ, which removes dietary fiber, iron, and other nutrients. The recommended amount of grains in the Healthy U.S.-Style Eating Pattern at the 2,000-calorie level is 6 ounce-equivalents per day. At least half of this amount should be whole grains 10. The intake of whole grains may also slow starch digestion or absorption, which leads to relatively lower insulin and glucose responses that favor the oxidation and lipolysis of fat rather than its storage 91, 92, 93. They are emphasized in the Dietary Guidelines for Americans because they provide vitamins, minerals, complex carbohydrates (starch and dietary fiber), and other substances that are important for good health. They are also generally low in fat, depending on how they are prepared and what is added to them at the table. However, most grain products consumed in the United States are highly refined 93, 94. Refined-grain products have a higher starch content but a lower fiber content (ie, greater energy density) than do whole grains. Concentrations of vitamins, minerals, essential fatty acids, and phytochemicals that are important in carbohydrate metabolism are also lower in refined grains 95.
Indirect evidence from both epidemiologic and short-term experimental studies suggests a beneficial role of a high-fiber diet in weight control 95, 96, 97. Most Americans of all ages eat fewer than the recommended number of servings of grain products, vegetables, and fruits, even though consumption of these foods is associated with a substantially lower risk for many chronic diseases, including certain types of cancer 10.
Dietary fiber is widely prescribed 98, either alone or in combination with lipid-lowering therapies, to reduce cholesterol levels 99. The exact mechanism by which soluble fiber lowers serum levels of low-density lipoprotein (LDL) and cholesterol is not completely understood; however, it has been suggested that soluble fiber may interfere with lipid and/or bile acid metabolism 100. A reasonable increase in dietary fiber intake (20–35 g/day) is recommended by the American Diabetes Association based on the effects of soluble fiber on plasma levels of cholesterol 101. Recent epidemiological findings have suggested that there is an association between high dietary fiber intake and a reduced risk of developing diabetes and coronary heart disease 102, 103. In particular, soluble dietary fiber has been shown to reduce insulin resistance in female non-diabetic patients 104.
A more recent study to find out the health benefits of soluble fiber on type 2 diabetes 47. A total of 117 patients with type 2 diabetes between the ages of 40 and 70 were assessed. Patients were randomly assigned to one of two groups, and administered extra soluble dietary fiber (10 or 20 g/day), or to a control group (0 g/day) for one month. The 20 g/day soluble dietary fiber group exhibited significantly improved fasting blood glucose and low-density (LDL) lipoprotein “bad cholesterol” levels, as well as a significantly improved insulin resistance index. In addition, 10 and 20 g/day soluble dietary fiber significantly improved the waist and hip circumferences and levels of triglycerides and apolipoprotein A. The results of the present study suggested that increased and regular consumption of soluble dietary fiber led to significant improvements in blood glucose levels, insulin resistance and metabolic profiles 47.
Whole grains
Whole grains are an important source of dietary fiber and other nutrients 10. Whole grains are a source of nutrients, such as dietary fiber, iron, zinc, manganese, folate, magnesium, copper, thiamin, niacin, vitamin B6, phosphorus, selenium, riboflavin, and vitamin A 105 10. Healthful diets rich in dietary fiber have been shown to have a number of beneficial effects, including decreasing risk of coronary heart disease and promoting regularity. Some examples of whole-grain products could include whole wheat bread, whole wheat cereal, and brown rice.
Whole grains are just that whole. Nothing has been added or taken away by processing. When whole grains are processed, some of the dietary fiber and other important nutrients are removed. A processed grain is called a refined grain. Most refined grains are enriched, a process that adds back iron and four B vitamins (thiamin, riboflavin, niacin, and folic acid) 10. Because of this process, the term “enriched grains” is often used to describe these refined grains. These are called enriched grains. White rice and white bread are enriched grain products. If you read the packaging for these foods, you will see the word “enriched.” Some enriched grain foods have extra nutrients added. These are called fortified grains. Many ready-to-eat cereals are fortified. At least half of the grains you eat should be whole-grain; other grains should be fortified or enriched 10.
The following are some examples of how whole grains could be listed:
- whole wheat
- wild rice
- quinoa
- brown rice
- whole oats/oatmeal
- buckwheat
- sorghum
- whole rye
- whole-grain corn
- bulgur (cracked wheat)
- popcorn
- whole-grain barley
- millet
- triticale
Note: Foods fiber content are highlighted in pink. (Source: U.S. Department of Health and Human Services and U.S. Department of Agriculture: Dietary Guidelines for Americans 2015-2020 10).
References- Glycemic index of foods: a physiological basis for carbohydrate exchange. Jenkins DJ, Wolever TM, Taylor RH, Barker H, Fielden H, Baldwin JM, Bowling AC, Newman HC, Jenkins AL, Goff DV. Am J Clin Nutr. 1981 Mar; 34(3):362-6. https://www.ncbi.nlm.nih.gov/pubmed/6259925/
- American Diabetes Association. Glycemic Index and Diabetes. http://www.diabetes.org/food-and-fitness/food/what-can-i-eat/understanding-carbohydrates/glycemic-index-and-diabetes.html
- FAO/WHO scientific update on carbohydrates in human nutrition: conclusions. Mann J, Cummings JH, Englyst HN, Key T, Liu S, Riccardi G, Summerbell C, Uauy R, van Dam RM, Venn B, Vorster HH, Wiseman M. Eur J Clin Nutr. 2007 Dec; 61 Suppl 1:S132-7. https://www.ncbi.nlm.nih.gov/pubmed/17992184/
- Atkinson FS, Foster-Powell K, Brand-Miller JC. International Tables of Glycemic Index and Glycemic Load Values: 2008 . Diabetes Care. 2008;31(12):2281-2283. doi:10.2337/dc08-1239. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2584181/
- Food and Agriculture Organization. Chapter 4 – The role of the glycemic index in food choice. http://www.fao.org/docrep/w8079e/w8079e0a.htm#factors%20influencing%20the%20blood%20glucose%20responses%20of%20foods
- European Journal of Clinical Nutrition (2007) 61 (Suppl 1), S132–S137; doi:10.1038/sj.ejcn.1602943. FAO/WHO Scientific Update on carbohydrates in human nutrition: conclusions. http://www.nature.com/ejcn/journal/v61/n1s/full/1602943a.html
- American Association of Cereal Chemists (AACC International). Dietary Fiber. http://www.aaccnet.org/initiatives/definitions/Pages/DietaryFiber.aspx
- Food and Agriculture Organization and World Health Organization. CODEX ALIMENTARIUS COMMISSION. Thirty second Session, Rome, Italy, 29 June – 4 July 2009. http://www.fao.org/input/download/report/710/al32_26e.pdf
- Lattimer JM, Haub MD. Effects of Dietary Fiber and Its Components on Metabolic Health. Nutrients. 2010;2(12):1266-1289. doi:10.3390/nu2121266. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3257631/
- U.S. Department of Health and Human Services and U.S. Department of Agriculture: Dietary Guidelines for Americans 2015-2020. https://health.gov/dietaryguidelines/
- Increasing total fiber intake reduces risk of weight and fat gains in women. Tucker LA, Thomas KS. J Nutr. 2009 Mar; 139(3):576-81. https://www.ncbi.nlm.nih.gov/pubmed/19158230/
- Carbohydrates, dietary fiber, and incident type 2 diabetes in older women. Meyer KA, Kushi LH, Jacobs DR Jr, Slavin J, Sellers TA, Folsom AR. Am J Clin Nutr. 2000 Apr; 71(4):921-30. https://www.ncbi.nlm.nih.gov/pubmed/10731498/
- Dietary fiber intake and risk of breast cancer in postmenopausal women: the National Institutes of Health-AARP Diet and Health Study. Park Y, Brinton LA, Subar AF, Hollenbeck A, Schatzkin A. Am J Clin Nutr. 2009 Sep; 90(3):664-71. https://www.ncbi.nlm.nih.gov/pubmed/19625685/
- Dietary fiber intake in relation to coronary heart disease and all-cause mortality over 40 y: the Zutphen Study. Streppel MT, Ocké MC, Boshuizen HC, Kok FJ, Kromhout D. Am J Clin Nutr. 2008 Oct; 88(4):1119-25. https://www.ncbi.nlm.nih.gov/pubmed/18842802/
- FDA, authors. Code of Federal Regulations. Vol. 2 Food and Drug Administration; Silver Spring, MD, USA: 2008. Health claims: Fiber-contaning grain products, fruits and vegetables and cancer.
- FDA, authors. Code of Federal Regulations. Vol. 2 Food and Drug Administration; Silver Spring, MD, USA: 2008. Health claims: fruits, vegetables, and grain products that contain fiber, particularly soluble fiber, and risk of coronary heart disease.
- Pereira MA, O’Reilly E, Augustsson K, et al. Dietary fiber and risk of coronary heart disease: a pooled analysis of cohort studies. Arch Intern Med. 2004;164:370-6. https://www.ncbi.nlm.nih.gov/pubmed/14980987
- Rimm EB, Ascherio A, Giovannucci E, Spiegelman D, Stampfer MJ, Willett WC. Vegetable, fruit, and cereal fiber intake and risk of coronary heart disease among men. JAMA. 1996;275:447-51. https://www.ncbi.nlm.nih.gov/pubmed/8627965
- Brown L, Rosner B, Willett WW, Sacks FM. Cholesterol-lowering effects of dietary fiber: a meta-analysis. Am J Clin Nutr. 1999;69:30-42. https://www.ncbi.nlm.nih.gov/pubmed/9925120
- McKeown NM, Meigs JB, Liu S, Wilson PW, Jacques PF. Whole-grain intake is favorably associated with metabolic risk factors for type 2 diabetes and cardiovascular disease in the Framingham Offspring Study. Am J Clin Nutr. 2002;76:390-8. https://www.ncbi.nlm.nih.gov/pubmed/12145012
- McKeown NM, Meigs JB, Liu S, Saltzman E, Wilson PW, Jacques PF. Carbohydrate nutrition, insulin resistance, and the prevalence of the metabolic syndrome in the Framingham Offspring Cohort. Diabetes Care. 2004;27:538-46. https://www.ncbi.nlm.nih.gov/pubmed/14747241
- Fung TT, Hu FB, Pereira MA, et al. Whole-grain intake and the risk of type 2 diabetes: a prospective study in men. Am J Clin Nutr. 2002;76:535-40. https://www.ncbi.nlm.nih.gov/pubmed/12197996
- Liu S, Willett WC, Stampfer MJ, et al. A prospective study of dietary glycemic load, carbohydrate intake, and risk of coronary heart disease in US women. Am J Clin Nutr. 2000;71:1455-61. https://www.ncbi.nlm.nih.gov/pubmed/10837285
- Schulze MB, Liu S, Rimm EB, Manson JE, Willett WC, Hu FB. Glycemic index, glycemic load, and dietary fiber intake and incidence of type 2 diabetes in younger and middle-aged women. Am J Clin Nutr. 2004;80:348-56. https://www.ncbi.nlm.nih.gov/pubmed/15277155
- Krishnan S, Rosenberg L, Singer M, et al. Glycemic index, glycemic load, and cereal fiber intake and risk of type 2 diabetes in US black women. Arch Intern Med. 2007;167:2304-9. https://www.ncbi.nlm.nih.gov/pubmed/18039988
- Dietary fiber and colorectal cancer risk: the multiethnic cohort study. Nomura AM, Hankin JH, Henderson BE, Wilkens LR, Murphy SP, Pike MC, Le Marchand L, Stram DO, Monroe KR, Kolonel LN. Cancer Causes Control. 2007 Sep; 18(7):753-64. https://www.ncbi.nlm.nih.gov/pubmed/17557210/
- Prospective study of dietary fiber, whole grain foods, and small intestinal cancer. Schatzkin A, Park Y, Leitzmann MF, Hollenbeck AR, Cross AJ. Gastroenterology. 2008 Oct; 135(4):1163-7. https://www.ncbi.nlm.nih.gov/pubmed/18727930/
- Dietary fibre and colorectal cancer: a model for environment–gene interactions. Young GP, Hu Y, Le Leu RK, Nyskohus L. Mol Nutr Food Res. 2005 Jun; 49(6):571-84. https://www.ncbi.nlm.nih.gov/pubmed/15864783/
- Adlercreutz H., Hamalainen E., Gorbach S.L., Goldin B.R., Woods M.N., Brunson L.S., Dwyer J.T. Association of Diet and Sex-Hormones in Relation to Breast-Cancer. Eur. J. Cancer Clin. Oncol. 1987;23:1725–1726.
- Dietary fiber and risk of coronary heart disease: a pooled analysis of cohort studies. Pereira MA, O’Reilly E, Augustsson K, Fraser GE, Goldbourt U, Heitmann BL, Hallmans G, Knekt P, Liu S, Pietinen P, Spiegelman D, Stevens J, Virtamo J, Willett WC, Ascherio A. Arch Intern Med. 2004 Feb 23; 164(4):370-6. https://www.ncbi.nlm.nih.gov/pubmed/14980987/
- Dietary fiber and bile acid metabolism–an update. Story JA, Furumoto EJ, Buhman KK. Adv Exp Med Biol. 1997; 427():259-66. https://www.ncbi.nlm.nih.gov/pubmed/9361851/
- Amaral L., Morgan D., Stephen A.M., Whiting S. Effect of Propionate on Lipid-Metabolism in Healthy-Human Subjects. FASEB J. 1992;6:A1655.
- Meal modulation of circulating interleukin 18 and adiponectin concentrations in healthy subjects and in patients with type 2 diabetes mellitus. Esposito K, Nappo F, Giugliano F, Di Palo C, Ciotola M, Barbieri M, Paolisso G, Giugliano D. Am J Clin Nutr. 2003 Dec; 78(6):1135-40. https://www.ncbi.nlm.nih.gov/pubmed/14668275/
- Association between dietary fiber and serum C-reactive protein. Ma Y, Griffith JA, Chasan-Taber L, Olendzki BC, Jackson E, Stanek EJ 3rd, Li W, Pagoto SL, Hafner AR, Ockene IS. Am J Clin Nutr. 2006 Apr; 83(4):760-6. https://www.ncbi.nlm.nih.gov/pubmed/16600925/
- Nutrients. 2010 Dec; 2(12): 1266–1289. – Effects of Dietary Fiber and Its Components on Metabolic Health – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3257631/
- American Association of Cereal Chemists (AACC International). Dietary Fiber. http://www.aaccnet.org/initiatives/definitions/Pages/DietaryFiber.aspx
- Therapeutic effects of psyllium in type 2 diabetic patients. Sierra M, García JJ, Fernández N, Diez MJ, Calle AP. Eur J Clin Nutr. 2002 Sep; 56(9):830-42. https://www.ncbi.nlm.nih.gov/pubmed/12209371/
- Dietary fibres, fibre analogues, and glucose tolerance: importance of viscosity. Jenkins DJ, Wolever TM, Leeds AR, Gassull MA, Haisman P, Dilawari J, Goff DV, Metz GL, Alberti KG. Br Med J. 1978 May 27; 1(6124):1392-4. https://www.ncbi.nlm.nih.gov/pubmed/647304/
- Gastric emptying in early noninsulin-dependent diabetes mellitus. Jones KL, Horowitz M, Carney BI, Wishart JM, Guha S, Green L. J Nucl Med. 1996 Oct; 37(10):1643-8. https://www.ncbi.nlm.nih.gov/pubmed/8862300/
- Action of guar gums on the viscosity of digestive contents and on the gastrointestinal motor function in pigs. Cherbut C, Albina E, Champ M, Doublier JL, Lecannu G. Digestion. 1990; 46(4):205-13. https://www.ncbi.nlm.nih.gov/pubmed/2178135/
- Effect of viscous fiber (guar) on postprandial motor activity in human small bowel. Schönfeld J, Evans DF, Wingate DL. Dig Dis Sci. 1997 Aug; 42(8):1613-7. https://www.ncbi.nlm.nih.gov/pubmed/9286225/
- Effect of gel-forming gums on the intestinal unstirred layer and sugar transport in vitro. Johnson IT, Gee JM. Gut. 1981 May; 22(5):398-403. https://www.ncbi.nlm.nih.gov/pubmed/7250752/
- Role of viscous guar gums in lowering the glycemic response after a solid meal. Leclère CJ, Champ M, Boillot J, Guille G, Lecannu G, Molis C, Bornet F, Krempf M, Delort-Laval J, Galmiche JP. Am J Clin Nutr. 1994 Apr; 59(4):914-21. https://www.ncbi.nlm.nih.gov/pubmed/7818627/
- Dietary guar gum improves insulin sensitivity in streptozotocin-induced diabetic rats. Cameron-Smith D, Habito R, Barnett M, Collier GR. J Nutr. 1997 Feb; 127(2):359-64. https://www.ncbi.nlm.nih.gov/pubmed/9039840/
- Soluble dietary fibre improves insulin sensitivity by increasing muscle GLUT-4 content in stroke-prone spontaneously hypertensive rats. Song YJ, Sawamura M, Ikeda K, Igawa S, Yamori Y. Clin Exp Pharmacol Physiol. 2000 Jan-Feb; 27(1-2):41-5. https://www.ncbi.nlm.nih.gov/pubmed/10696527/
- Troglitazone effects on gene expression in human skeletal muscle of type II diabetes involve up-regulation of peroxisome proliferator-activated receptor-gamma. Park KS, Ciaraldi TP, Lindgren K, Abrams-Carter L, Mudaliar S, Nikoulina SE, Tufari SR, Veerkamp JH, Vidal-Puig A, Henry RR. J Clin Endocrinol Metab. 1998 Aug; 83(8):2830-5. https://www.ncbi.nlm.nih.gov/pubmed/9709955/
- Chen C, Zeng Y, Xu J, et al. Therapeutic effects of soluble dietary fiber consumption on type 2 diabetes mellitus. Experimental and Therapeutic Medicine. 2016;12(2):1232-1242. doi:10.3892/etm.2016.3377. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4950069/
- Aldoori WH, Giovannucci EL, Rockett HR, Sampson L, Rimm EB, Willett WC. A prospective study of dietary fiber types and symptomatic diverticular disease in men. J Nutr. 1998;128:714-9. https://www.ncbi.nlm.nih.gov/pubmed/9521633
- Resistant starch: metabolic effects and potential health benefits. Higgins JA. J AOAC Int. 2004 May-Jun; 87(3):761-8. https://www.ncbi.nlm.nih.gov/pubmed/15287677/
- Birt DF, Boylston T, Hendrich S, et al. Resistant Starch: Promise for Improving Human Health. Advances in Nutrition. 2013;4(6):587-601. doi:10.3945/an.113.004325. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3823506/
- Englyst HN, Kingman SM, Cummings JH. Classification and measurement of nutritionally important starch fractions. Eur J Clin Nutr. 1992;46(Supp 2):S33–50. https://www.ncbi.nlm.nih.gov/pubmed/1330528
- Woo KS, Seib PA. Cross-linked resistant starch: preparation and properties. Cereal Chem. 2002;79:819–25.
- Han J-A, BeMiller JN. Preparation and physical characteristics of slowly digesting modified food starches. Carbohydr Polym. 2007;67:366–74.
- Seneviratne HD, Biliaderis CG. Action of α-amylases on amylose-lipid complex superstructures. J Cereal Sci. 1991;13:129–43.
- Ring S.G., Selvendran R.R. Isolation and Analysis of Cell-Wall Material from Beeswing Wheat Bran (Triticum-Aestivum) Phytochemistry. 1980;19:1723–1730.
- Arabinoxylan fiber, a byproduct of wheat flour processing, reduces the postprandial glucose response in normoglycemic subjects. Lu ZX, Walker KZ, Muir JG, Mascara T, O’Dea K. Am J Clin Nutr. 2000 May; 71(5):1123-8. https://www.ncbi.nlm.nih.gov/pubmed/10799374/
- Arabinoxylan fibre improves metabolic control in people with Type II diabetes. Lu ZX, Walker KZ, Muir JG, O’Dea K. Eur J Clin Nutr. 2004 Apr; 58(4):621-8. https://www.ncbi.nlm.nih.gov/pubmed/15042130/
- Selective stimulation of bifidobacteria in the human colon by oligofructose and inulin. Gibson GR, Beatty ER, Wang X, Cummings JH. Gastroenterology. 1995 Apr; 108(4):975-82. https://www.ncbi.nlm.nih.gov/pubmed/7698613/
- Dietary synbiotics reduce cancer risk factors in polypectomized and colon cancer patients. Rafter J, Bennett M, Caderni G, Clune Y, Hughes R, Karlsson PC, Klinder A, O’Riordan M, O’Sullivan GC, Pool-Zobel B, Rechkemmer G, Roller M, Rowland I, Salvadori M, Thijs H, Van Loo J, Watzl B, Collins JK. Am J Clin Nutr. 2007 Feb; 85(2):488-96. https://www.ncbi.nlm.nih.gov/pubmed/17284748/
- Griffin I.J., Hicks P.M.D., Heaney R.P., Abrams S.A. Enriched chicory inulin increases calcium absorption mainly in girls with lower calcium absorption. Nutr. Res. 2003;23:901–909.
- A combination of prebiotic short- and long-chain inulin-type fructans enhances calcium absorption and bone mineralization in young adolescents. Abrams SA, Griffin IJ, Hawthorne KM, Liang L, Gunn SK, Darlington G, Ellis KJ. Am J Clin Nutr. 2005 Aug; 82(2):471-6. https://www.ncbi.nlm.nih.gov/pubmed/16087995/
- Oligofructose promotes satiety in healthy human: a pilot study. Cani PD, Joly E, Horsmans Y, Delzenne NM. Eur J Clin Nutr. 2006 May; 60(5):567-72. https://www.ncbi.nlm.nih.gov/pubmed/16340949/
- Wood P.J., Weisz J., Fedec P. Potential for Beta-Glucan Enrichment in Brans Derived from Oat (Avena sativa L.) Cultivars of Different (1→3),(1→4)-Beta-D-Glucan Concentrations. Cereal Chem. 1991;68:48–51.
- Simultaneous intake of beta-glucan and plant stanol esters affects lipid metabolism in slightly hypercholesterolemic subjects. Theuwissen E, Mensink RP. J Nutr. 2007 Mar; 137(3):583-8. https://www.ncbi.nlm.nih.gov/pubmed/17311944/
- Beta-glucan incorporated into a fruit drink effectively lowers serum LDL-cholesterol concentrations. Naumann E, van Rees AB, Onning G, Oste R, Wydra M, Mensink RP. Am J Clin Nutr. 2006 Mar; 83(3):601-5. https://www.ncbi.nlm.nih.gov/pubmed/16522906/
- Davidson M.H., McDonald A. Fiber: Forms and functions. Nutr. Res. 1998;18:617–624.
- Changes in serum lipids and postprandial glucose and insulin concentrations after consumption of beverages with beta-glucans from oats or barley: a randomised dose-controlled trial. Biörklund M, van Rees A, Mensink RP, Onning G. Eur J Clin Nutr. 2005 Nov; 59(11):1272-81. https://www.ncbi.nlm.nih.gov/pubmed/16015250/
- Regulation of hepatic glucose production in healthy subjects and patients with non-insulin-dependent diabetes mellitus. Tappy L. Diabete Metab. 1995 Oct; 21(4):233-40. https://www.ncbi.nlm.nih.gov/pubmed/8529757/
- Oat beta-glucan increases bile acid excretion and a fiber-rich barley fraction increases cholesterol excretion in ileostomy subjects. Lia A, Hallmans G, Sandberg AS, Sundberg B, Aman P, Andersson H. Am J Clin Nutr. 1995 Dec; 62(6):1245-51. https://www.ncbi.nlm.nih.gov/pubmed/7491888/
- Modulation of the postprandial phase by beta-glucan in overweight subjects: effects on glucose and insulin kinetics. Nazare JA, Normand S, Oste Triantafyllou A, Brac de la Perrière A, Desage M, Laville M. Mol Nutr Food Res. 2009 Mar; 53(3):361-9. https://www.ncbi.nlm.nih.gov/pubmed/18837470/
- In vitro bile-acid binding and fermentation of high, medium, and low molecular weight beta-glucan. Kim HJ, White PJ. J Agric Food Chem. 2010 Jan 13; 58(1):628-34. https://www.ncbi.nlm.nih.gov/pubmed/20020684/
- In vitro fermentation of oat flours from typical and high beta-glucan oat lines. Kim HJ, White PJ. J Agric Food Chem. 2009 Aug 26; 57(16):7529-36. https://www.ncbi.nlm.nih.gov/pubmed/19572543/
- Regulation by dietary fats of 3-hydroxy-3-methylglutaryl-Coenzyme A reductase in rat liver. Ide T, Okamatsu H, Sugano M. J Nutr. 1978 Apr; 108(4):601-12. https://www.ncbi.nlm.nih.gov/pubmed/632948/
- Randomized controlled crossover study of the effect of a highly beta-glucan-enriched barley on cardiovascular disease risk factors in mildly hypercholesterolemic men. Keogh GF, Cooper GJ, Mulvey TB, McArdle BH, Coles GD, Monro JA, Poppitt SD. Am J Clin Nutr. 2003 Oct; 78(4):711-8. https://www.ncbi.nlm.nih.gov/pubmed/14522728/
- A controlled study of consumption of beta-glucan-enriched soups for 2 months by type 2 diabetic free-living subjects. Cugnet-Anceau C, Nazare JA, Biorklund M, Le Coquil E, Sassolas A, Sothier M, Holm J, Landin-Olsson M, Onning G, Laville M, Moulin P. Br J Nutr. 2010 Feb; 103(3):422-8. https://www.ncbi.nlm.nih.gov/pubmed/19781120/
- Olano-Martin E., Gibson G.R., Rastell R.A. Comparison of the in vitro bifidogenic properties of pectins and pectic-oligosaccharides. J. Appl. Microbiol. 2002;93:505–511. doi: 10.1046/j.1365-2672.2002.01719.x. https://www.ncbi.nlm.nih.gov/pubmed/12174051
- Nangia-Makker P., Hogan V., Honjo Y., Baccarini S., Tait L., Bresalier R., Raz A. Inhibition of human cancer cell growth and metastasis in nude mice by oral intake of modified citrus pectin. J. Natl. Cancer Inst. 2002;94:1854–1862. https://www.ncbi.nlm.nih.gov/pubmed/12488479
- Ulmius M., Johansson A., Onning G. The influence of dietary fibre source and gender on the postprandial glucose and lipid response in healthy subjects. Eur. J. Nutr. 2009;48:395–402. https://www.ncbi.nlm.nih.gov/pubmed/19415409
- Qureshi A.A., Sami S.A., Khan F.A. Effects of stabilized rice bran, its soluble and fiber fractions on blood glucose levels and serum lipid parameters in humans with diabetes mellitus Types I and II. J. Nutr. Biochem. 2002;13:175–187. https://www.ncbi.nlm.nih.gov/pubmed/11893482
- Koh-Banerjee P., Franz M.V., Sampson L., Liu S.M., Jacobs D.R., Spiegelman D., Willett W., Rimm E. Changes in whole-grain, bran, and cereal fiber consumption in relation to 8-y weight gain among men. Am. J. Clin. Nutr. 2004;80:1237–1245. https://www.ncbi.nlm.nih.gov/pubmed/15531671
- Zhang J.X., Lundin E., Hallmans G., Adlercreutz H., Andersson H., Bosaeus I., Aman P., Stenling R., Dahlgren S. Effect of Rye Bran on Excretion of Bile-Acids, Cholesterol, Nitrogen, and Fat in Human-Subjects with Ileostomies. Am. J. Clin. Nutr. 1994;59:389–394. https://www.ncbi.nlm.nih.gov/pubmed/8310990
- Jensen M.K., Koh-Banerjee P., Hu F.B., Franz M., Sampson L., Gronbaek M., Rimm E.B. Intakes of whole grains, bran, and germ and the risk of coronary heart disease in men. Am. J. Clin. Nutr. 2004;80:1492–1499. https://www.ncbi.nlm.nih.gov/pubmed/15585760
- Andersson M., Ellegard L., Andersson H. Oat bran stimulates bile acid synthesis within 8 h as measured by 7 alpha-hydroxy-4-cholesten-3-one. Am. J. Clin. Nutr. 2002;76:1111–1116. https://www.ncbi.nlm.nih.gov/pubmed/12399287
- Schwartz S.E., Levine R.A., Singh A., Scheidecker J.R., Track N.S. Sustained pectin ingestion delays gastric emptying. Gastroenterology. 1982;83:812–817. https://www.ncbi.nlm.nih.gov/pubmed/6286402
- Lightowler H.J., Henry C.J. Glycemic response of mashed potato containing high-viscocity hydroxypropylmethylcellulose. Nutr. Res. 2009;29:551–557. https://www.ncbi.nlm.nih.gov/pubmed/19761889
- Maki K.C., Davidson M.H., Witchger M.S., Dicklin M.R., Subbaiah P.V. Effects of high‑fiber oat and wheat cereals on postprandial glucose and lipid responses in healthy men. Int. J. Vitam. Nutr. Res. 2007;77:347–356. https://www.ncbi.nlm.nih.gov/pubmed/18453320
- Maki K.C., Davidson M.H., Torri S., Ingram K.A., O’Mullane J., Daggy B.P., Albrecht H.H. High-molecular-weight hydroxypropylmethylcellulose taken with or between meals is hypocholesterolemic in adult men. J. Nutr. 2000;130:1705–1710. https://www.ncbi.nlm.nih.gov/pubmed/10867040
- Maki K.C., Carson M.L., Anderson W.H.K., Geohas J., Reeves M.S., Farmer M.V., Turowski M., Miller M., Kaden V.N., Dicklin M.R., Rains T.M. Lipid-altering effects of different formulations of hydroxypropylmethylcellulose. J. Clin. Lipidol. 2009;3:159–166. https://www.ncbi.nlm.nih.gov/pubmed/21291811
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2015-2020. https://health.gov/sites/default/files/2019-09/2015-2020_Dietary_Guidelines.pdf
- Dietitians Association of Australia. Dietary fibre: key for a happy, healthy gut. https://daa.asn.au/smart-eating-for-you/smart-eating-fast-facts/nourishing-nutrients/dietary-fibre-a-key-ingredient-in-gut-happiness/
- Jenkins DJ, Jenkins AL, Wolever TM, Collier GR, Rao AV, Thompson LU. Starchy foods and fiber: reduced rate of digestion and improved carbohydrate metabolism. Scand J Gastroenterol Suppl 1987;129:132-41. https://www.ncbi.nlm.nih.gov/pubmed/2820027?dopt=Abstract
- Jenkins DJ, Wesson V, Wolever TM, et al. Wholemeal versus wholegrain breads: proportion of whole or cracked grain and the glycaemic response. BMJ 1988;297:958-60.
- Slavin JL, Martini MC, Jacobs DR Jr, Marquart L. Plausible mechanisms for the protectiveness of whole grains. Am J Clin Nutr 1999;70(suppl):459S-63S. http://ajcn.nutrition.org/content/70/3/459s.full
- Putnam J, Allshouse J, Kantor LS. US per capita food supply trends: more calories, refined carbohydrates, and fats. Food Rev 2002;25:2-15.
- Liu S. Intake of refined carbohydrates and whole grain foods in relation to risk of type 2 diabetes mellitus and coronary heart disease.J Am Coll Nutr 2002;21:298-306. https://www.ncbi.nlm.nih.gov/pubmed/12166526?dopt=Abstract
- Roberts SB, Heyman MB. Dietary composition and obesity: do we need to look beyond dietary fat? J Nutr 2000;130:267S (editorial).
- Ludwig DS, Pereira MA, Kroenke CH, et al. Dietary fiber, weight gain, and cardiovascular disease risk factors in young adults. JAMA1999 ;282:1539-46. https://www.ncbi.nlm.nih.gov/pubmed/10546693?dopt=Abstract
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III): Third report of the national cholesterol education program (ncep) expert panel on detection, evaluation, and treatment of high blood cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143–3421. https://www.ncbi.nlm.nih.gov/pubmed/12485966
- Ortega RM, Palencia A, López-Sobaler AM. Improvement of cholesterol levels and reduction of cardiovascular risk via the consumption of phytosterols. Br J Nutr. 2006;96(Suppl 1):S89–S93. doi: 10.1079/BJN20061708. https://www.ncbi.nlm.nih.gov/pubmed/16923260
- Theuwissen E, Mensink RP. Water-soluble dietary fibers and cardiovascular disease. Physiol Behav. 2008;94:285–292. doi: 10.1016/j.physbeh.2008.01.001. https://www.ncbi.nlm.nih.gov/pubmed/18302966
- American Diabetes Association: Nutrition recommendations and principles for people with diabetes mellitus. Diabetes Care. 2000;23(Suppl 1):S43–S46. https://www.ncbi.nlm.nih.gov/pubmed/12017676
- Bernaud FS, Rodrigues TC. Dietary fiber-adequate intake and effects on metabolism health. Arq Bras Endocrinol Metabol. 2013;57:397–405. doi: 10.1590/S0004-27302013000600001. https://www.ncbi.nlm.nih.gov/pubmed/24030179
- Frankenfeld CL. Cardiometabolic risk factors are associated with high urinary enterolactone concentration, independent of urinary enterodiol concentration and dietary fiber intake in adults. J Nutr. 2014;144:1445–1453. doi: 10.3945/jn.114.190512. https://www.ncbi.nlm.nih.gov/pubmed/24966407
- Breneman CB, Tucker L. Dietary fibre consumption and insulin resistance-the role of body fat and physical activity. Br J Nutr. 2013;110:375–383. doi: 10.1017/S0007114512004953. https://www.ncbi.nlm.nih.gov/pubmed/23218116
- in the form of provitamin A carotenoids





{kind=link}