
What is DHA ?
Docosahexaenoic acid (DHA) is an essential fatty acid and a member of the omega-3 fatty acid family. Docosahexaenoic acid (DHA) is an “essential” fatty acid, meaning that people must obtain it from food or supplements because the human body cannot manufacture it 1. Omega-3 fatty acids are important for a number of bodily functions, including muscle activity, blood clotting, digestion, fertility, and cell division and growth. Docosahexaenoic acid (DHA) is also found in all cell membranes, and play an important role as structural membrane lipids, particularly in nerve tissue for brain development and the retina of the eye 2. Various organizations worldwide have made dietary recommendations for eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and fish intake that are primarily for coronary disease risk reduction and triglyceride lowering. Recommendations also have been made for docosahexaenoic acid (DHA) intake for pregnant women, infants, and vegetarians/vegans 3. Over the past decades, evidence has accumulated in support of the hypothesis that DHA (docosahexaenoic acid) may have an important role in pregnancy health and outcome, as well as in the postnatal development of perceptual and cognitive function in infancy.
What are Omega-3 fatty acids
Fats are essential for living organisms. Fatty acid molecules have a variable length carbon chain with a methyl terminus and a carboxylic acid head group 4. They can be categorized based on the degree of saturation of their carbon chains. Saturated fatty acids possess the maximal number of hydrogen atoms, while monounsaturated fatty acids (MUFAs) and polyunsaturated fatty acids (PUFAs) have one, or two or more, double bonds, respectively.
Figure 1. Monounsaturated Fatty Acids Structure
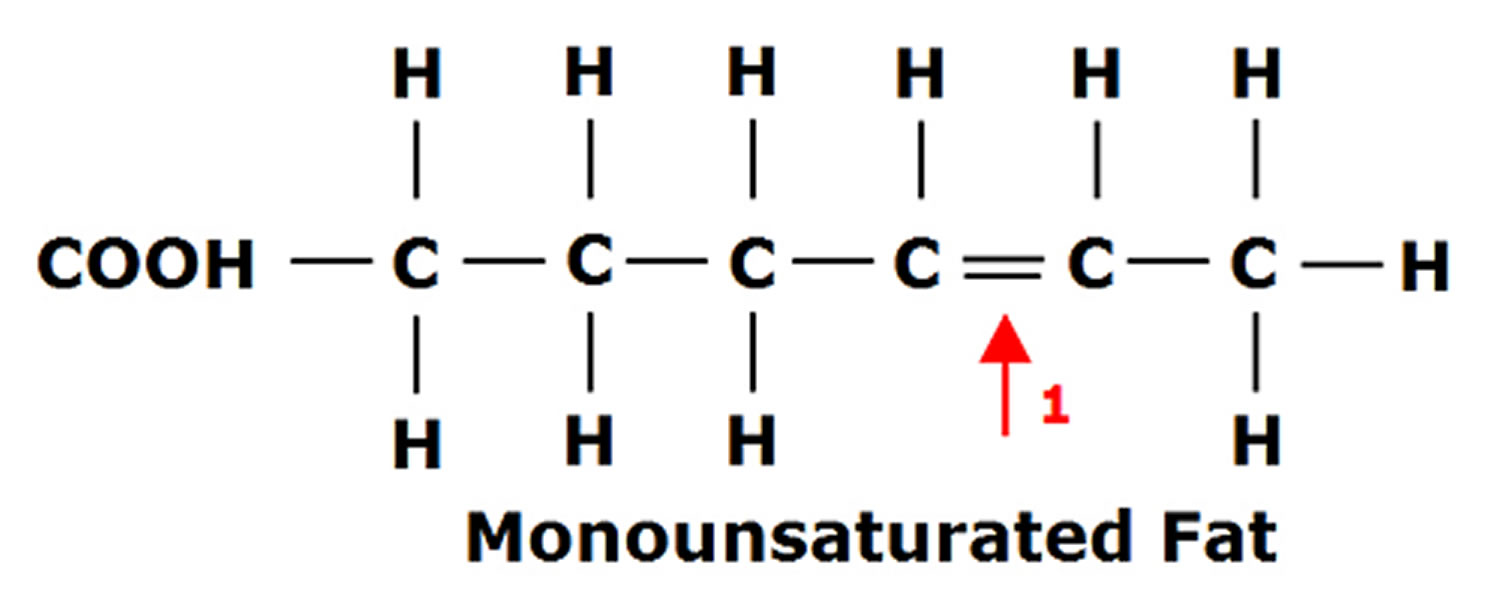
Figure 2. Polyunsaturated Fatty Acids Structure
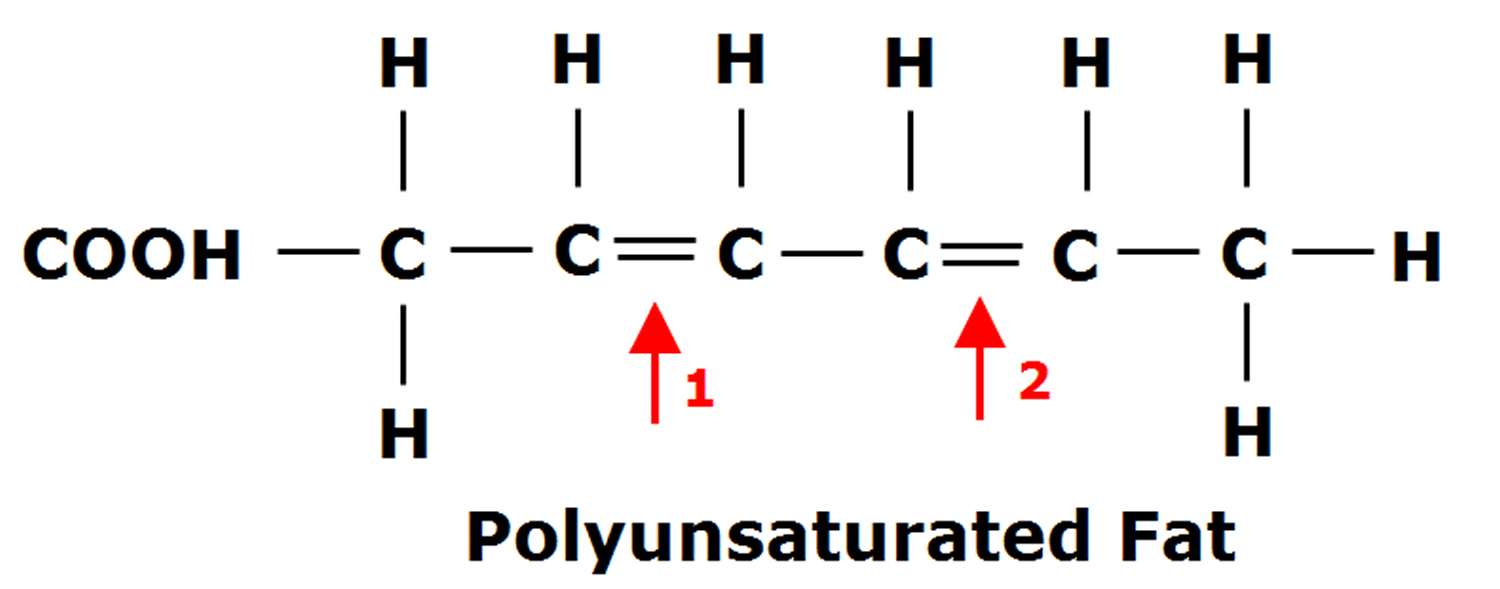
Figure 3. Omega-3 fatty acids and Omega-6 fatty acids structure
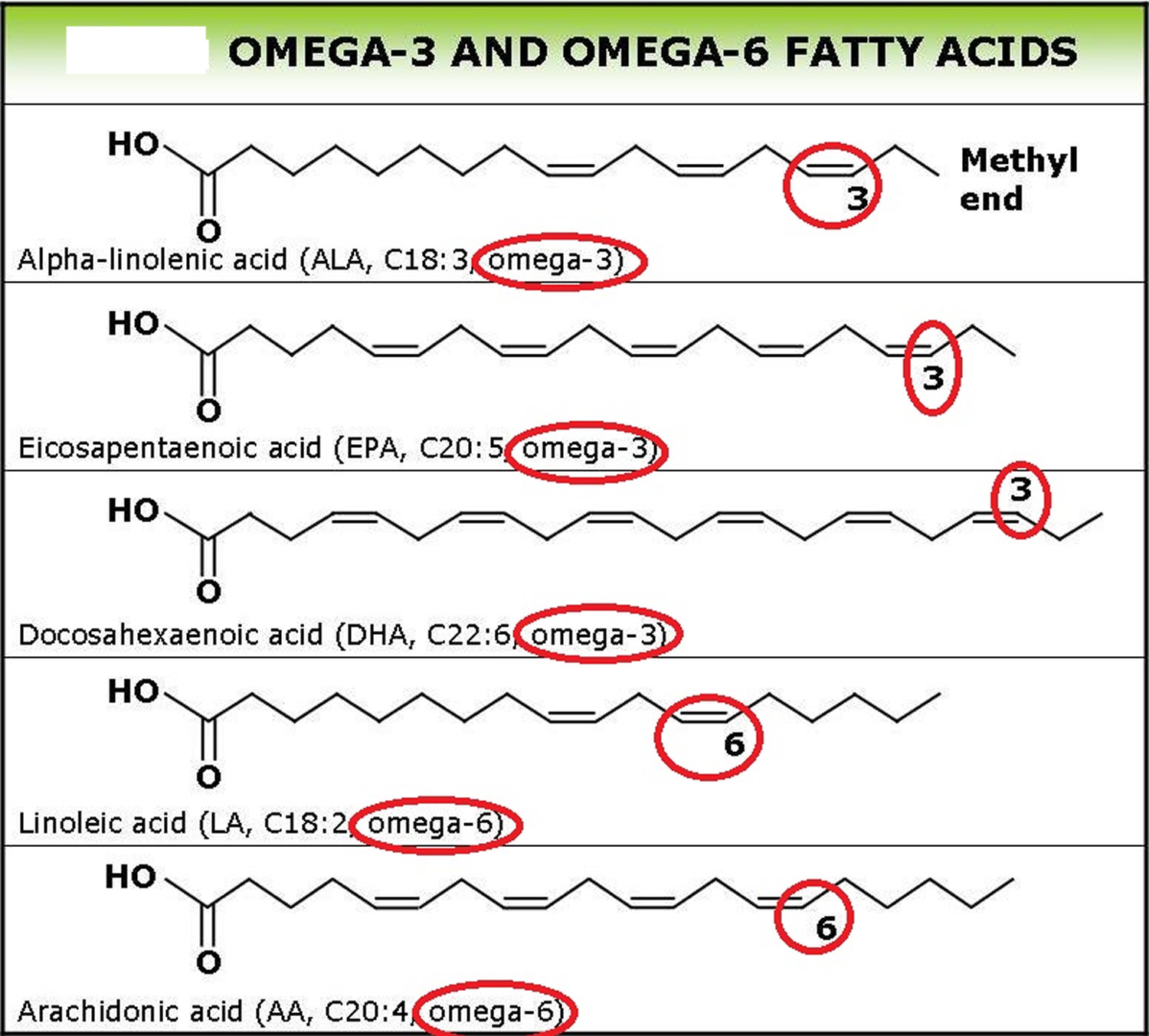
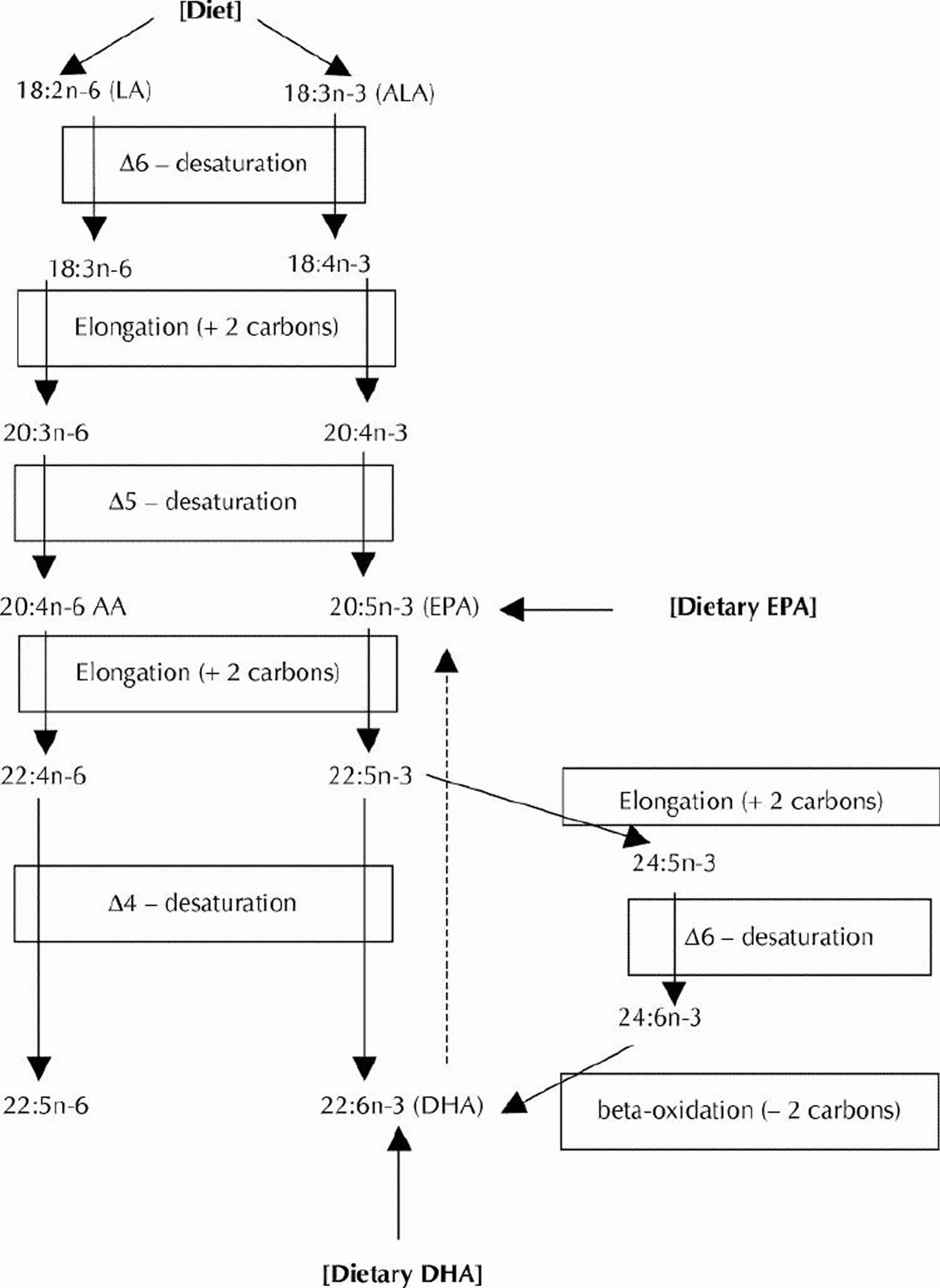
Figure 4. Conversion of dietary ALA to EPA and DHA via Desaturation, elongation and retroconversion of polyunsaturated fatty acids.
Omega-3 fatty acids are long-chain polyunsaturated fatty acids (18–22 carbon atoms in chain length) with the first of many double bonds beginning with the third carbon atom, n-3, when counting from the methyl end of the fatty acid molecule (see Figure 3). The three principal omega-3 fatty acids are:
- Alpha-linolenic acid (ALA) (18:3ω-3),
- Eicosapentaenoic acid (EPA) (20:5ω-3),
- Docosahexaenoic acid (DHA) (22:6ω-3).
The three principal omega-3 fatty acids are alpha-linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA). The main sources of alpha-linolenic acid (ALA) in the U.S. diet are vegetable oils, particularly canola and soybean oils; flaxseed oil is richer in ALA than soybean and canola oils but is not commonly consumed. ALA can be converted, usually in small amounts, into EPA and DHA in the body. EPA and DHA are found in seafood, including fatty fish (e.g., salmon, tuna, and trout) and shellfish (e.g., crab, mussels, and oysters).
Long-chain Omega-3 PUFAs are synthesized from the essential fatty acid linoleic acid (LA) and alpha-linolenic acid (ALA). An essential fatty acid cannot be made by the body and must be obtained through dietary sources. Fatty fish, such as mackerel, herring and salmon, provide an excellent source of the long-chain derivatives of ALA, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) 6. The typical North American diet provides about 1–3 g of n-3 PUFA alpha-linolenic acid (ALA) per day but only 0.10–0.15 g of EPA (Eicosapentaenoic acid) plus DHA (Docosahexaenoic acid) per day 7, 8. The results indicate that the majority of American are failing to meet intake recommendations for long chain Omega-3 PUFA and emphasize the need for strategies, to increase the availability and consumption of Omega-3-containing foods 2.
Of the 20 or so edible fatty acids, only omega-3 and omega-6 fatty acids cannot be synthesized by the body 9. All of the omega-3 and omega-6 fatty acids accumulated by the fetus must ultimately be derived from the mother by placental transfer. The typical American diet is well-supplied with omega-6 fatty acids, particularly linoleic acid (LA), which is readily converted to arachidonic acid (AA). Omega-6 fatty acids can be found in the vegetable oils used in processed foods, fried foods, and condiments like salad dressings 10, 11. One teaspoon of corn oil can satisfy the daily omega-6 requirement, but most individuals eat 10 to 20 times that amount 10, 11.
Table 1. Adequate Intakes for Omega-3s
| Age | Male | Female | Pregnancy | Lactation |
|---|---|---|---|---|
| Birth to 6 months* | 0.5 g | 0.5 g | ||
| 7–12 months* | 0.5 g | 0.5 g | ||
| 1–3 years** | 0.7 g | 0.7 g | ||
| 4–8 years** | 0.9 g | 0.9 g | ||
| 9–13 years** | 1.2 g | 1.0 g | ||
| 14–18 years** | 1.6 g | 1.1 g | 1.4 g | 1.3 g |
| 19-50 years** | 1.6 g | 1.1 g | 1.4 g | 1.3 g |
| 51+ years** | 1.6 g | 1.1 g |
*As total omega-3s
**As ALA
In contrast, the intake of omega-3 fatty acids is suboptimal 9. The richest dietary sources of omega-3 fatty acids are from marine sources, fish oil supplements, and selected vegetable oils like flaxseed (57% omega-3 fatty acids), canola (11% omega-3 fatty acids), and soybean (8% omega-3 fatty acids). Most individuals in the United States do not consume these omega-3-rich foods on a regular basis. The ratio of dietary omega- 6/omega-3 fatty acids in the American diet approximates 10 to 25:1 11.
The omega-3 fatty acid eicosapentaenoic acid (EPA) and the omega-6 fatty acid arachidonic acid (AA) are essential structural components of every cell in the body. Both eicosapentaenoic acid (EPA) and arachidonic acid (AA) serve as precursors for biologically active compounds called eicosanoids. These fatty acids compete for the enzyme systems cyclooxygenase, which makes prostaglandins and thromboxanes, and lipoxygenase, which makes leukotrienes. Diets that are rich in omega-6 fatty acids produce potent eicosanoids, whereas a diet with a more balanced intake of omega-6 and omega-3 fatty acids makes less inflammatory and less immunosuppressive eicosanoids 13.
Specific to pregnancy, although both DHA and arachidonic acid (AA) appear to be essential to fetal CNS development, the relatively poor intake of EPA coupled with the high intake of linoleic acid (which produces AA), may affect pregnancy outcome by altering the balance of the eicosanoids produced 14, 15. A high ratio of arachidonic acid (AA) to eicosapentaenoic acid (EPA) may promote untoward effects such as preterm labor and preeclampsia 16. A linoleic acid-rich diet produces an abundance of arachidonic acid (AA), which serves as a precursor of the potent 2-series prostaglandins (PGs) E2 and PGF2α, and the vasoconstrictor thromboxane (TX) A2. Both PGE2 and PGF2α are closely associated with the initiation of labor and preterm labor, whereas thromboxane A2 has been associated with preeclampsia 17, 18. Whereas the omega-3 fatty acid, DHA, is not usually considered to be involved with eicosanoid formation, EPA is a precursor for the 3-series of PGs and produces PGE3 and PGI3, which promote relaxation of myometrium 19, 20. Also, EPA and DHA competitively displace arachidonic acid (AA) in the membrane phospholipids and thereby reduce production of 2-series eicosanoids 21. Thus, a diet that provides a closer balance of omega-3 to omega-6 fatty acids may be as important to pregnant women as the absolute individual plasma levels of these fatty acids.
Nonetheless, in pregnancy, the real significance of eicosapentaenoic acid (EPA) may be related to its role in mediating DHA and arachidonic acid (AA) concentrations across the placenta rather than its production of the relatively less potent PGI3. Free fatty acids need to be bound for transfer to the fetal circulation. Selective transport across the human placenta for individual fatty acids has been suggested as a mechanism to explain greater concentrations of some PUFAs like DHA and AA in the fetal, rather than maternal, circulation. In this regard, the effect of EPA on mRNA expression of fatty acid transport proteins (FATPs) becomes important 22. EPA, but not DHA, has been positively correlated with mRNA expression of all membrane proteins. Thus, higher maternal EPA concentrations may increase FATP expression (FATP-4 in particular) that, in turn, has been shown to increase cord blood DHA levels 22. In addition, the free fatty acids need to be bound to fatty acid binding proteins (FABPs) in order to gain entry into placental and fetal cells. Because, as noted above, EPA has been positively correlated with mRNA expression of all membrane proteins, higher EPA concentrations also lead to increased expression of FABPs including B-FABP, which is strongly expressed in developing brain cells and has a strong affinity for DHA 23.
Because only about 4% to 11% of DHA is retroconverted to EPA 24, pregnant women who just take DHA supplements, without any dietary EPA, may be unable to produce the right balance of eicosanoids and may limit the transport and uptake of DHA into fetal cells 24.
In the field of perinatal nutrition, polyunsaturated fatty acids (PUFAs) of the omega-3 and omega-6 groups have gained recent attention because of their important functions in fetal and newborn neurodevelopment and because of their roles in inflammation 25, 26, 27.
Two PUFAs, arachidonic acid (AA) and docosahexaenoic acid (DHA), are critical to fetal and infant central nervous system (brain) growth and development 25, 28. Embedded in the cell membrane phospholipid, arachidonic acid (AA) is involved in cell signaling pathways and cell division, and serves as an inflammatory precursor for eicosanoids. The DHA concentration is high in retinal and brain membrane phospholipids, and it is involved in visual and neural function and neurotransmitter metabolism 26. During the last trimester, the fetus accrues about 50 to 70 mg a day of omega-3 fatty acid, DHA 29, 30. Both maternal DHA intake and circulating DHA concentrations are important determinants of fetal blood concentrations of DHA 27. Babies accrue DHA into the brain up until about 18 months of age 31, 32.
Although research into the specific pathways affected by these PUFAs is still in its infancy, there is enough understanding to draw conclusions and make recommendations about their dietary intake during the perinatal period.
Foods with DHA and EPA
The U.S. Department of Agriculture’s (USDA’s) Nutrient Database website 33 lists the nutrient content of many foods with DHA (Docosahexaenoic acid) arranged by DHA nutrient content 34 and by DHA food name 35.
Table 2. Omega-3 Fatty Acid Foods EPA (Eicosapentaenoic acid) and DHA (Docosahexaenoic acid) – Fish and Seafood Sources
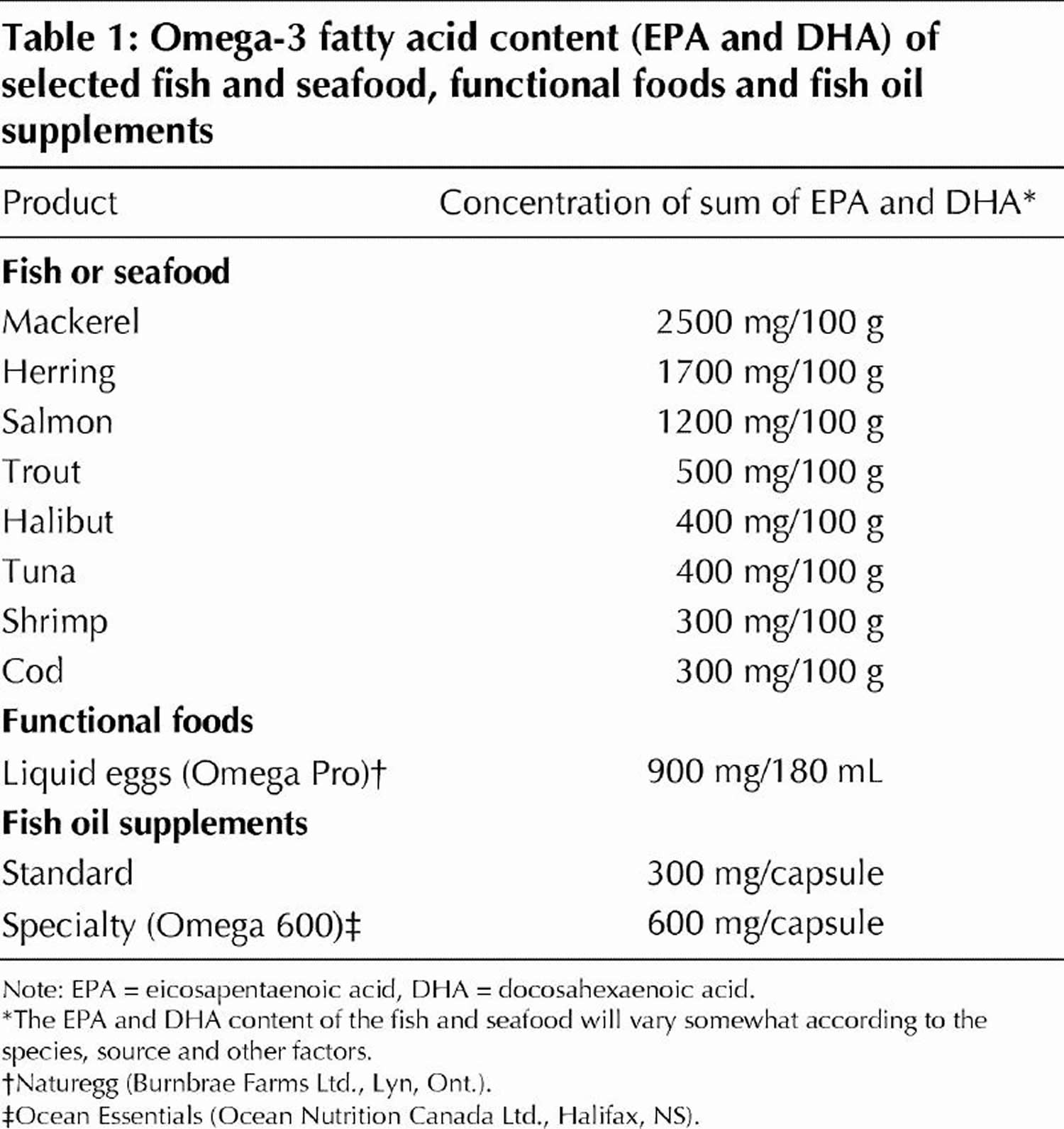
Table 3. Other sources of Omega-3 Alpha-Linolenic Acid (ALA) – Non-Seafood Sources
| Source of ALA | ALA content, g |
|---|---|
| Pumpkin seeds (1 tbsp) | 0.051 |
| Olive oil (1 tbsp) | 0.103 |
| Walnuts, black (1 tbsp) | 0.156 |
| Soybean oil (1 tbsp) | 1.231 |
| Rapeseed oil (1 tbsp) | 1.302 |
| Walnut oil (1 tbsp) | 1.414 |
| Flaxseeds (1 tbsp) | 2.350 |
| Walnuts, English (1 tbsp) | 2.574 |
| Flaxseed oil (1 tbsp) | 7.249 |
| Almonds (100 g) | 0.4 |
| Peanuts (100 g) | 0.003 |
| Beans, navy, sprouted (100 g) | 0.3 |
| Broccoli, raw (100 g) | 0.1 |
| Lettuce, red leaf (100 g) | 0.1 |
| Mustard (100 g) | 0.1 |
| Purslane (100 g) | 0.4 |
| Spinach (100 g) | 0.1 |
| Seaweed, spirulina, dried (100 g) | 0.8 |
| Beans, common, dry (100 g) | 0.6 |
| Chickpeas, dry (100 g) | 0.1 |
| Soybeans, dry (100 g) | 1.6 |
| Oats, germ (100 g) | 1.4 |
| Rice, bran (100 g) | 0.2 |
| Wheat, germ (100 g) | 0.7 |
| Avocados, California, raw (100 g) | 0.1 |
| Raspberries, raw (100 g) | 0.1 |
| Strawberries, raw (100 g) | 0.1 |
| Novel sources of ALA | ALA content, g |
| Breads and pasta (100 g) | 0.1–1.6 |
| Cereals (and granola bars) (55 g) | 1.0–4.9 |
| Eggs (50 g or 1 egg) | 0.1–0.6 |
| Processed meats (100 g) | 0.5 |
| Salad dressing (14 g – 31 g) | 2.0–4.0 |
| Margarine spreads (10 g – 100 g) | 0.3–1.0 |
| Nutrition bars (50 g) | 0.1–2.2 |
Note: 1 tablespoon (tbsp) oil = 13.6 g; 1 tbsp seeds or nuts = 12.35 g.
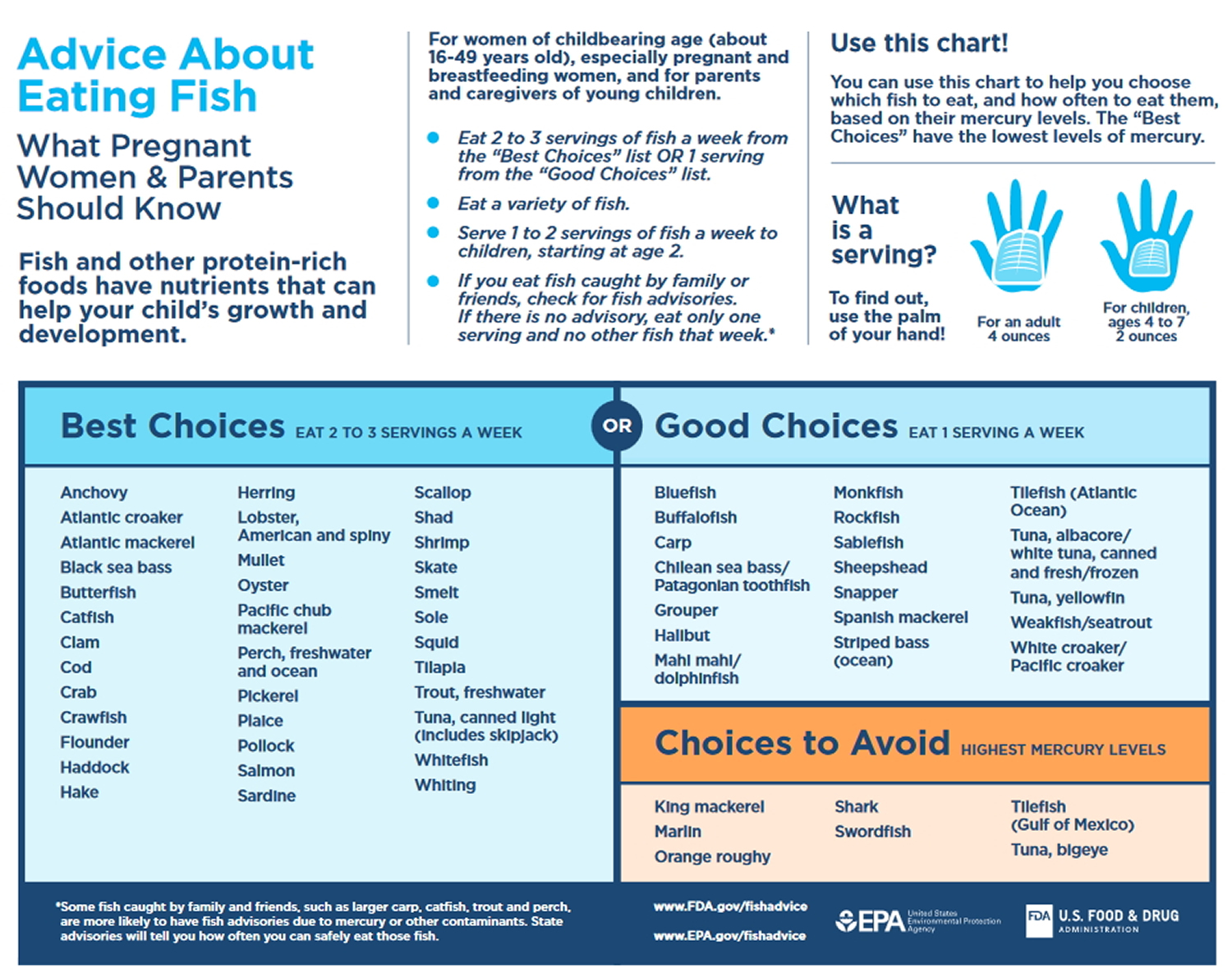
The typical Western diet is deficient in omega-3 PUFAs, in general, and in DHA in particular. Although seafood is a good source of both DHA and EPA, concerns about mercury contamination have led to both fear and confusion about whether to recommend it during pregnancy. Both the Environmental Protection Agency and The American College of Obstetricians and Gynecologists recommend that women consume 12 ounces of seafood per week from low-mercury species:
- Shrimp 880 mg (320 mg DHA) 37
- Salmon 620 mg (260 mg DHA) 37
- Pollock 520 mg (360 mg DHA) 37
- Catfish 340 mg (180 mg DHA) 37
- Scallops 740 mg (360 mg DHA) 37
- Sardines 2.2 g (1.2 g DHA) 38
- Light tuna 380 mg (170 mg DHA) 37
Avoid large predatory fish (e.g. marlin, pike, swordfish and shark), which are more likely to be contaminated with methylmercury.
For those seeking to avoid seafood, there are few nonsupplement options. Plant-based omega-3 fatty acids (ie, α-linolenic acid [ALA]), like flaxseed oil, are poorly converted to the biologically active omega-3 fatty acid EPA, and converts even less to DHA 24, 40. The range of conversion of Alpha-linolenic acid (ALA) to Eicosapentaenoic acid (EPA) is generally between 0.2% and 9%, although some authors have suggested that women of childbearing age may be able to convert up to 21% of their dietary ALA to EPA. Regardless of which conversion factor is correct, trying to obtain all omega-3 fatty acids from plant-based oils requires ingestion of too many fat calories.
Infant health and neurodevelopment
Numerous studies have examined the effects of maternal seafood and omega-3 intakes on infant birth weight, length of gestation, visual and cognitive development, and other infant health outcomes. High concentrations of DHA are present in the cellular membranes of the brain and retina 41, and DHA is important for fetal growth and development. The accumulation of DHA in the retina is complete by birth, whereas accumulation in the brain continues throughout the first 2 years after birth.
In 2016, Agency for Healthcare Research and Quality (AHRQ) published a review on the effects of omega-3 fatty acids on child and maternal health 42. This comprehensive report evaluated the findings from 95 randomized controlled trials and 48 prospective longitudinal studies and nested case-control studies. Most studies examined the effects of fish oil supplements or other DHA and EPA combinations in pregnant or breastfeeding women or of infant formula fortified with DHA plus arachidonic acid, an omega-6. The authors concluded that, except for small beneficial effects on infant birth weight and length of gestation, omega-3 supplementation or fortification has no consistent effects on infant health outcomes.
Recommendations from the Dietary Guidelines for Americans: The 2015–2020 Dietary Guidelines for Americans states that women who are pregnant or breastfeeding should consume 8–12 ounces of seafood per week, choosing from varieties that are higher in EPA and DHA and lower in methyl mercury, such as salmon, herring, sardines, and trout. These women should not consume certain types of fish, such as king mackerel, shark, swordfish, and tilefish that are high in methyl mercury, and they should limit the amount of white (albacore) tuna they consume to 6 ounces a week. The American Academy of Pediatrics has similar advice for breastfeeding women, recommending intakes of 200–300 mg DHA per day by consuming one to two servings of fish per week to guarantee a sufficient amount of DHA in breast milk 43.
Most currently available infant formulas in the United States contain DHA and arachidonic acid. However, the authors of a paper published by the American Academy of Family Physicians and of two Cochrane reviews (one on full-term infants and one on preterm infants) have concluded that the evidence is insufficient to recommend the use of infant formulas that are supplemented with these fatty acids 44, 45, 46.
DHA supplement
Fish oil supplements are commercially available from multiple companies. A typical fish oil supplement provides about 1,000 mg fish oil, the amount of EPA and DHA per capsule varies, but most contain one-third to one-half of these omega-3 fatty acids (eg, in a 1000-mg capsule, 300 or 500 mg would come from EPA and DHA) 1. Although seafood contains varying levels of methyl mercury (a toxic heavy metal) 47, omega-3 supplements have not been found to contain this contaminant because it is removed during processing and purification 48. Cod liver oil is considered a less desirable source of EPA and DHA, because it is also rich in vitamin A, unlike other fish oils 1. Long-term use of vitamin A has been associated with an increased risk of osteoporosis 49.
Meaningful vegetarian sources of DHA are essentially limited to algae-derived DHA from Martek Biosciences (Columbia, MD) 1. Using a strain of algae, Crypthecodinium cohnii, which is a naturally high producer of DHA, DHA oil is produced in US Food and Drug Administration-inspected, environmentally controlled manufacturing facilities. Although free of any environmental contaminants such as mercury, the oils do not contain any EPA and data demonstrating the benefits in pregnancy of DHA alone are lacking 1.
Much of the interest in omega-3 fatty acid intake and pregnancy began in the early 1980s, when Danish investigators determined that women living on the Faroe Islands delivered babies that were 194 g heavier and had gestation lengths 4 days longer than babies born in Denmark 20. The Faroese diet had substantially more omega-3 fatty acids and less omega-6 fatty acids than a Danish diet. Red blood cell fatty acid content (expressed as the ratio of omega-3 to omega-6) was significantly higher in the Faroese pregnant women than in Danish pregnant women 50. From this study, the authors theorized that a Danish woman who adjusted her diet to increase her blood ratio of these fatty acids by 20% would expect to increase gestation 5.7 days 50.
Following up on their earlier epidemiologic work, the same Danish group then randomized pregnant women at week 30 of gestation to either a fish oil supplement (2.7 g omega-3 fatty acids, of which 920 mg were DHA), olive oil, or no supplement 19. Women in the fish oil group had a gestational period 4 days longer than women taking either olive oil or no supplement. The babies born to the women in the fish oil group also weighed 107 g more than babies born to the women in the olive oil group, and 43 g more than those born to those mothers without supplementation. The supplemental amount of dietary omega-3 fatty acids used in this study was larger than a typical Danish diet, which only provided about 10% of this amount (ie, 270 mg of omega-3 fatty acids). Thus, it appeared that rather high amounts of omega-3 fatty acids need to be consumed to affect gestation and fetal weight.
The time of the most rapid neural and retinal development occurs in the second half of pregnancy, mainly during the third trimester. On this basis, supplementation of the maternal diet later in pregnancy with omega-3 fatty acids, especially DHA, was thought to be especially important 10, 14, 51. In a trial focused on the benefits of naturally occurring DHA from food, a sample of pregnant Inuit women living in Arctic Quebec was assessed 21. Maternal DHA blood concentrations were shown to be directly related to cord plasma phospholipid levels, and the correlation of the DHA/AA ratio in maternal and cord plasma was even stronger. In this study, higher DHA cord blood concentration was related to longer gestation, better visual acuity and mental and psychomotor skills at 6 months and 11 months, suggesting that raising DHA concentrations alone may independently yield some benefits 21. It must be noted that the Inuit population has a dietary intake of EPA and DHA that is higher than most other nations because of their regular intake of fish and marine animals. Such foods are also rich in EPA, but it was not measured.
A second study providing large amounts of DHA as a supplement explored its effects during pregnancy and, later, on fetal cognition 27. From week 16 of gestation until delivery, healthy Canadian women (average age, 33 years) who were not taking supplemental fish oil capsules were randomized to 400 mg of algae-derived DHA or a blend of corn and soybean oil. The purpose of the study was to compare red blood cell DHA levels, dietary intakes of DHA and other omega-3 fatty acids, and infant visual acuity at 60 days of age. At week 36, DHA in the supplemented women was 32% higher than the control group, and no differences were found between the groups for EPA and AA, both of which decreased. Infants were 3 times more likely to have low visual acuity scores in the placebo group than the DHA group, indicating that the usual diet may have had insufficient DHA to maximize visual acuity in infants. In fact, omega-3 fatty acid deficiency, as measured by red blood cell DHA, was more prevalent in the control group than in the DHA-supplemented group.
DHA Benefits
Docosahexaenoic acid (DHA), as a fundamental constituent in cell membranes, is essential to the structure, maturation and function of the retina and the brain 52, 53. DHA is mainly contained in aquatic products, especially in seafood. Dietary DHA intake is a major source to meet human body requirements, since humans only synthesize a limited amount of DHA from α-linolenic acid (ALA) 54. It is widely acknowledged that pregnant and lactating women are more susceptible to DHA deficiency because they need to meet their own needs as well as those of the fetuses. Increased intake of DHA during pregnancy and lactation has been documented to benefit fetal and infant development 55, 56, 57.
The availability and consumption of aquatic products plays an important role in DHA status. In a study 58 conducted among women from four Tanzanian tribes differing in lifetime intakes of fish, Luxwolda et al. observed an obvious positive correlation between fish consumption and DHA levels 58. DHA status may also vary across ethnicities. In a study 59 comparing plasma DHA phospholipids between Dutch and ethnic minority pregnant women in Netherlands, van Eijsden et al. 59 reported significant ethnic differences in maternal DHA status despite controlling for fish intake. Besides, in an earlier study 60 involving women from Ecuador and four European countries with different baseline phospholipid DHA status, Otto et al. 60 observed consistent decreases in the DHA weight percentage of total fatty acids as women progress from early pregnancy to delivery.
Babies fed with breast milk are known to have more mature visual skills and a higher IQ (intelligence quotient) than babies fed with formula milk. Unlike breast milk that contains high levels of long chain PUFA (e.g. DHA and AA), most infant formulae are known to only contain minimal amounts of long chain PUFA. The presence of docosahexaenoic acid (DHA) and arachidonic acid (AA) in human milk but not in infant formula, coupled with lower plasma and brain lipid contents of DHA in formula-fed than in breast-fed infants and reports of higher IQ in individuals who were breast-fed versus formula-fed as infants, suggest that exogenous DHA (and AA) may be essential for optimal development 61. Thus, since 1990, several studies have examined the impact of formulas containing DHA or DHA plus AA on visual function and neurodevelopmental outcome. Some of these studies have shown benefits but others have not. These results leave largely unanswered the question of whether these fatty acids are beneficial for either the term or preterm infant. However, evidence that preterm infants might benefit is somewhat more convincing than that for term infants. Despite the limited evidence for efficacy, formulas supplemented with DHA and AA are now available and appear to be safe.
In terms of feeding full-term babies with formula milk enriched with long chain polyunsaturated fatty acids (long chain PUFA e.g. DHA or EPA), this Cochrane review 62 analysed studies that compared outcomes of full-term babies (born at ≥ 37 weeks of pregnancy) who were given formula milk enriched with long chain polyunsaturated fatty acids versus outcomes of full-term babies fed formula milk without enrichment with long chain PUFA. Review authors found that full-term babies fed formula milk supplemented with long chain PUFA did not have better outcomes than were reported for full-term babies fed formula milk without long chain PUFA. Most of the included randomised clinical trials reported no beneficial effects or harms of long chain PUFA supplementation on neurodevelopmental outcomes of formula-fed full-term infants and no consistent beneficial effects on visual acuity. Routine supplementation of full-term infant milk formula with long chain PUFA cannot be recommended at this time 62.
It has been suggested that the relatively high levels of long chain PUFA found in breast milk may contribute to the higher IQ levels and visual skills. Some milk formulae are available with added long chain PUFA, usually as fish oil. In another 2016 Cochrane Review 63 studies that compared the outcomes of premature babies (born at < 37 weeks of pregnancy) who were given formula milk enriched with long chain polyunsaturated fatty acids versus formula milk without enrichment with long chain PUFA were analysed. The researchers found that premature babies fed formula milk supplemented with long chain PUFA do not have better outcomes compared to those fed formula milk without long chain PUFA 63.
Prenatal DHA and Pregnancy
According to this 2007 European Commission on Early Nutrition Programming Project 64 pregnant and lactating women should aim to achieve an average dietary intake of at least 200 mg DHA per day can be reached with the consumption of one to two portions of sea fish per week, including oily fish such as herring, mackerel and salmon 64. The European Food Safety Authority concluded that pregnant women eating up to two portions per week of fish are unlikely to exceed the provisional tolerable weekly intake for dioxin, dioxin-like compounds and contaminants such as methylmercury, polychlorinated biphenyls, brominated flame retardants, camphechlor and organotin 64. However, particularly high levels of contamination are found in herring or wild salmon from the Baltic Sea and women of childbearing age should limit the consumption of Baltic Sea herring or wild salmon to no more than one portion per week 64. Intakes of up to 1 g per day of DHA or 2·7 g/d Omega-3 long-chain PUFA have been used in randomized clinical trials without significant adverse effects; women of childbearing age should aim to consume one to two portions of sea fish per week, including oily fish 64. Intake of the DHA precursor, α-linolenic acid (ALA), is far less effective with regard to DHA deposition in fetal brain than preformed DHA 64. Intake of fish or other sources of long-chain Omega-3 fatty acids results in a slightly longer pregnancy duration; dietary inadequacies should be screened for during pregnancy and individual counselling be offered if needed.
The Omega-3 long chain-PUFA, DHA, must be deposited in appreciable amounts in the central nervous system during the perinatal brain growth spurt, as well as in other membrane-rich tissues. Fetal DHA accretion amounts to about 30–45 mg per day in the last trimester of gestation, while arachidonic acid (AA) accretion mainly occurs postnatally 65, 66. The pathways to form DHA from the precursor essential fatty acid, α-linolenic acid (ALA), exist in man (see Figure 4 above). The fractional conversion of α-linolenic acid (ALA) to Omega-3 long chain-PUFA may be greater in women than in men, which may contribute to meeting the demands of the fetus and the breast-fed neonate for DHA, but most evidence indicates that the overall contribution of α-linolenic acid (ALA) to DHA is limited; therefore, adequate intakes of preformed Omega-3 long chain-PUFA and in particular DHA, appear important for maintaining optimal tissue function 67, 68, 69. In intrauterine growth-restricted pregnancies, indications for reduced placental and/or fetal conversion of precursor essential fatty acids to long chain-PUFA (DHA and EPA) have been reported 70. Moreover, recent data indicate a considerable inter-individual variation in the ability to convert the precursor α-linolenic acid (ALA) to DHA, related to common polymorphisms in the human Δ-5 and Δ-6 desaturase genes FADS1 and FADS29. Preformed DHA is preferentially transferred across the human placenta to the fetus mediated by specific transfer proteins 71. In non-human primates, preformed dietary DHA is about an order of magnitude more efficient as a source for the neonatal brain accumulation of DHA than is α-linolenic acid 72.
The effects of supplementing pregnant women with Omega-3 long chain-PUFA from fish oil or single cell oils on pregnancy outcomes have been evaluated in a number of randomized controlled clinical trials, which provided daily DHA intakes ranging from 150–200 mg up to about 1200 mg/d, or up to 2·7 g total Omega-3 long chain-PUFA per day. Systematic evaluation of these studies in recent meta analyses revealed that Omega-3 long chain-PUFA prolonged gestation by a mean of 1·6 or 2·6 days in two independent analyses, respectively 73, 74, accompanied by a slight increase of birth weight by a mean 47 or 54 g, respectively 73, 74 and reduced the risk of preterm birth before 34 weeks of gestation by 31 % in all pregnancies 74 or by 61 % in high-risk pregnancies 75. Except for some reported discomfort associated with the intake of Omega-3 oil capsules, such as belching and unpleasant taste, no adverse effects were detected up to the highest intake of 2·7 g total Omega-3 long chain-PUFA per day tested in a randomized controlled trial in pregnancy.
Enhanced maternal dietary intakes of DHA increase fetal supply and lead to higher DHA concentrations in cord blood 76. A higher DHA supply to the fetus during pregnancy and to the infant after birth was associated with beneficial effects on the development of visual acuity, cognitive functions and attention, maturity of sleep patterns, spontaneous motor activity, immune phenotypes in cohort studies and in a limited number of randomized clinical trials 77, 78, 79. Based on the information available at this time, it is advisable that pregnant women aim at achieving an average intake of at least 200 mg DHA per day. Supplementation of lactating women with 200 mg DHA/d increased human milk DHA content by about 0·2 % fatty acids to a level considered desirable for infant outcomes 80, 81. Therefore, an average dietary intake of at least 200 mg DHA/d appears to be also adequate during lactation.
Postnatal depression is a common condition that affects women and may impact on their babies. Common symptoms of postnatal depression include fluctuations in mood, mood changes, suicidal ideation and preoccupation with infant well-being ranging from over-concern to frank delusions. There is currently not much evidence regarding interventions that might prevent or treat postnatal depression. A diet lacking in certain vitamins, minerals or other nutrients (e.g. DHA, EPA) may cause postnatal depression in some women. Correcting this deficiency with dietary supplements might therefore prevent postnatal depression. In a large double-blind, multicenter, randomized controlled trial involving DHA and mother infant outcome conducted in 5 Australian maternity hospitals involving 2399 women who were less than 21 weeks’ gestation with singleton pregnancies 82. Women allocated to the DHA group were asked to consume three 500-mg/d capsules of DHA-rich fish oil concentrate, providing 800 mg/d of DHA and 100 mg/d of eicosapentaenoic acid (EPA, 20:5n-3; Incromega 500 TG); and women in the control group were asked to take three 500-mg/d vegetable oil capsules without DHA 82. The dose of 800 mg/d was chosen because this was above the estimated threshold associated with lower risk of depressed maternal mood and higher scores on developmental outcomes of children 83, as well as being consistent with the estimated requirement to cover 97% of the population 84. The vegetable oil capsules contained a blend of 3 nongenetically modified oils (rapeseed, sunflower, and palm) in equal proportions. This blend of oils was designed to match the polyunsaturated, monounsaturated, and saturated fatty acid profile of the average Australian diet 85. Women were asked to take their assigned capsules daily, from study entry until birth of their child. All capsules were similar in size, shape, and color. In addition, 694 children (95.6% of those selected for follow-up) were assessed at 18 months.
The results were the percentage of women reporting high levels of depressive symptoms during the first 6 months postpartum did not differ between the DHA and control groups 82. Depressive symptoms were more common among women with a previous or current diagnosis of depression at trial entry but did not differ between groups 82. The percentage of women with a new medical diagnosis for depression during the trial or a diagnosis requiring treatment also did not differ between groups 82.
Mean cognitive scores of children from women allocated to the DHA group did not differ from mean scores of children of women from the control group, although fewer children from the DHA group had cognitive scores indicating delayed cognitive development compared with controls 82. Overall, mean language scores also did not differ between groups; however, a significant treatment × sex interaction indicated a differential response of boys and girls. Girls from the DHA group had a lower mean language score than girls from the control group, as well as an increased risk of delayed language development, and the response of boys did not differ between groups 82. For the secondary developmental outcomes, motor development, social-emotional behavior, and adaptive behavior did not differ between groups overall, although girls exposed to DHA in utero had poorer mean adaptive behavior scores than girls from the control group 82.
The secondary clinical outcomes of the infants – there were fewer very preterm births (<34 weeks’ gestation) in the DHA group compared with the control group, but there were more postterm births requiring obstetric intervention (inductions or cesarean deliveries) in the DHA group compared with the control group 82. Mean birth weight was 68 g heavier and fewer infants were of low birth weight in the DHA group compared with the control group 82. However, mean birth weight z scores (corrected for gestational age and sex) did not differ between groups, indicating that group differences in birth size were largely a function of gestational age at birth 82.
In summary, the use of DHA-rich fish oil capsules compared with vegetable oil capsules during pregnancy did not result in lower levels of postpartum depression in mothers or improved cognitive and language development in their offspring during early childhood 82.
Furthermore, in a 2013 Cochrane Review 86, the study authors stated there is insufficient evidence to conclude that selenium, DHA or EPA prevent postnatal depression 86. There is currently no evidence to recommend any other dietary supplement for prevention of postnatal depression.
Summary
Women of childbearing age can meet the recommended intake of DHA (at least 200 mg DHA/day) by consuming one to two portions of sea fish per week, including oily fish, which is a good source of Omega-3 long chain-PUFA. This intake of oily fish rarely exceeds the tolerable intake of environmental contaminants. Dietary fish should be selected from a wide range of species without undue preference for large predatory fish (e.g. marlin, pike, swordfish and shark), which are more likely to be contaminated with methylmercury.
Intake of the precursor, α-linolenic acid (ALA), is far less effective with regard to DHA deposition in fetal brain than the intake of preformed DHA.
There is no evidence that women of childbearing age whose dietary intake of linoleic acid (LA) is adequate, need an additional dietary intake of arachidonic acid (AA).
Some studies have shown that maternal intake of fish, fish oils or Omega-3 long chain-PUFA results in a slightly longer duration of gestation 87, a somewhat higher birth weight (greater birth size) and a reduced risk of early preterm delivery 88. The clinical importance of such effects with regard to overall infant health and development of most infants has not been fully elucidated and is subject to further investigation.
The amount of Omega-3 long chain-PUFA supplementation (DHA plus EPA) in the published trials ranges from 100 mg to 3.3 grams per day. Studies did not identify any serious safety concerns related to DHA supplementation for mother or newborn.
There is currently no evidence to recommend any other dietary supplement for prevention of postnatal depression. The use of DHA-rich fish oil capsules during pregnancy did not result in lower levels of postpartum depression in mothers or improved cognitive and language development in their offspring during early childhood. Furthermore, brain development and function is influenced by many variables other than DHA. To add complexity, infant development is a distribution in which an individual’s potential is unknown.
- Greenberg JA, Bell SJ, Ausdal WV. Omega-3 Fatty Acid Supplementation During Pregnancy. Reviews in Obstetrics and Gynecology. 2008;1(4):162-169. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2621042/[↩][↩][↩][↩][↩]
- National Academy of Sciences. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements. https://www.nap.edu/catalog/11537/dietary-reference-intakes-the-essential-guide-to-nutrient-requirements[↩][↩]
- Dietary fat intakes for pregnant and lactating women. British Journal of Nutrition, Volume 98, Issue 5, November 2007 , pp. 873-877. https://www.cambridge.org/core/journals/british-journal-of-nutrition/article/dietary-fat-intakes-for-pregnant-and-lactating-women/0D7D3496EE4A080986B649ED90295464[↩]
- Salem N., Jr Introduction to polyunsaturated fatty acids. Backgrounder. 1999;3:1–8.[↩]
- Holub BJ. Clinical nutrition: 4. Omega-3 fatty acids in cardiovascular care. Hoffer LJ, Jones PJ, eds. CMAJ: Canadian Medical Association Journal. 2002;166(5):608-615. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC99405/[↩][↩]
- Clinical nutrition: 4. Omega-3 fatty acids in cardiovascular care. Holub BJ. CMAJ. 2002 Mar 5; 166(5):608-15. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC99405/[↩]
- Omega-3 fatty acid content of the US food supply. Raper NR, Cronin FJ, Exler J. J Am Coll Nutr. 1992 Jun; 11(3):304-8. https://www.ncbi.nlm.nih.gov/pubmed/1619182/[↩]
- Kris-Etherton PM, Taylor DS, Yu-Poth S, Huth P, Moriarty K, Fishell V, et al. Polyunsaturated fatty acids in the food chain in the United States. Am J Clin Nutr 2000;71(Suppl 1):179-88.[↩]
- Bell SJ, Bradley D, Forse RA, et al. The new dietary fats in health and disease. J Am Diet Assoc. 1997;97:280–286. https://www.ncbi.nlm.nih.gov/pubmed/9060945[↩][↩]
- Burdge G. α-Linolenic acid metabolism in men and women: nutritional and biological implications. Curr Opin Clin Nutr Metab Care. 2004;7:137–144. https://www.ncbi.nlm.nih.gov/pubmed/15075703[↩][↩][↩]
- Kris-Etherton PM, Taylor DS, Yu-Poth S, et al. Polyunsaturated fatty acids in the food chain in the United States. Am J Clin Nutr. 2000;71:179S–188S. http://ajcn.nutrition.org/content/71/1/179S.long[↩][↩][↩]
- Institute of Medicine, Food and Nutrition Board. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids (macronutrients). Washington, DC: National Academy Press; 2005. https://www.nap.edu/read/10490/chapter/1[↩]
- Endres S, Ghorbani R, Kelley VE, et al. The effect of dietary supplementation with n-3 polyunsaturated fatty acids on the synthesis of interleukin-1 and tumor necrosis factor by mononuclear cells. N Engl J Med. 1989;320:265–271. https://www.ncbi.nlm.nih.gov/pubmed/2783477[↩]
- Jensen CL. Effects of n-3 fatty acids during pregnancy and lactation. 2006;83:1452S–1457S. http://ajcn.nutrition.org/content/83/6/S1452.long[↩][↩]
- Allen KGD, Harris MA. The role of n-3 fatty acids in gestation and parturition. Exp Biol Med. 2001;226:498–506. https://www.ncbi.nlm.nih.gov/pubmed/11395920[↩]
- Wang Y, Walsh SW, Kay HH. Placental tissue levels of nonesterified polyunsaturated fatty acids in normal and preeclamptic pregnancies. Hypertens Pregnancy. 2005;24:235–245. https://www.ncbi.nlm.nih.gov/pubmed/16263596[↩]
- Olson DM. The role of prostaglandins in the initiation of parturition. Best Pract Res Clin Obstet Gynaecol. 2003;17:717–730. https://www.ncbi.nlm.nih.gov/pubmed/12972010[↩]
- Malatyalioglu E, Adam B, Yanik FF, et al. Levels of stable metabolites of prostacyclin and thromboxane A2 and their ratio in normotensive and preeclamptic pregnant women during the antepartum and postpartum periods. J Matern Fetal Med. 2000;9:173–177. https://www.ncbi.nlm.nih.gov/pubmed/10914626[↩]
- Olsen SF, Sorensen JD, Secher NJ, et al. Randomised controlled trial of effect of fish-oil supplementation on pregnancy duration. Lancet. 1992;339:1003–1007. https://www.ncbi.nlm.nih.gov/pubmed/1349049[↩][↩]
- Olsen SF, Hansen HS, Sorensen TI, et al. Intake of marine fat, rich in (n-3)-polyunsaturated fatty acids, may increase birthweight by prolonging gestation. Lancet. 1986;2:367–369. https://www.ncbi.nlm.nih.gov/pubmed/2874370[↩][↩]
- Jacobson JL, Jacobson SW, Muckle G, et al. Beneficial effects of a polyunsaturated fatty acid on infant development: evidence from the Inuit of Arctic Quebec. J Pediatr. 2008;152:356–364. https://www.ncbi.nlm.nih.gov/pubmed/18280840[↩][↩][↩]
- Larqué E, Krauss-Etschmann S, Campoy C, et al. Docosahexaenoic acid supply in pregnancy affects placental expression of fatty acid transport proteins. Am J Clin Nutr. 2006;84:853–861. http://ajcn.nutrition.org/content/84/4/853.long[↩][↩]
- Xu LZ, Sanchez R, Sali A, et al. Ligand specificity of brain lipid-binding protein. J Biol Chem. 1996;271:24711–24719. http://www.jbc.org/content/271/40/24711.long[↩]
- Conquer JA, Holub BJ. Supplementation with an algae source of docosahexaenoic acid increases (n-3) fatty acid status and alters selected risk factors for heart disease in vegetarian subjects. J Nutr. 1996;126:3032–3039. https://www.ncbi.nlm.nih.gov/pubmed/9001371[↩][↩][↩]
- Birch EE, Garfield S, Castaneda Y, et al. Visual acuity and cognitive outcomes at 4 years of age in a double-blind, randomized trial of long-chain polyunsaturated fatty acid-supplemented infant formula. Early Hum Dev. 2007;83:279–284. https://www.ncbi.nlm.nih.gov/pubmed/17240089[↩][↩]
- Elias SL, Innis SM. Infant plasma trans, n-6, and n-3 fatty acids and conjugated linoleic acids are related to maternal plasma fatty acids, length of gestation, and birth weight and length. Am J Clin Nutr. 2001;73:807–814. http://ajcn.nutrition.org/content/73/4/807.long[↩][↩]
- Innis SM, Friesen RW. Essential n-3 fatty acids in pregnant women and early visual acuity maturation in term infants. Am J Clin Nutr. 2008;87:548–557. http://ajcn.nutrition.org/content/87/3/548.long[↩][↩][↩]
- Birch EE, Castaneda YS, Wheaton DH, et al. Visual maturation of term infants fed long-chain polyunsaturated fatty acid-supplemented or control formula for 12 mo. Am J Clin Nutr. 2005;81:871–879. http://ajcn.nutrition.org/content/81/4/871.long[↩]
- Clandinin MT, Chappell JE, Heim T, et al. Fatty acid utilization in perinatal de novo synthesis of tissues. Early Hum Dev. 1981;5:355–366. https://www.ncbi.nlm.nih.gov/pubmed/7285840[↩]
- Innis SM. Essential fatty acid transfer and fetal development. Placenta. 2005;26:S70–S75. https://www.ncbi.nlm.nih.gov/pubmed/15837071[↩]
- Denomme J, Stark KD, Holub BJ. Directly quantitated dietary (n-3) fatty acid intakes of pregnant Canadian women are lower than current dietary recommendations. J Nutr. 2005;135:206–211. http://jn.nutrition.org/content/135/2/206.long[↩]
- Szajewska H, Horvath A, Koletzko B. Effect of n-3 long-chain polyunsaturated fatty acid supplementation of women with low-risk pregnancies on pregnancy outcomes and growth measures at birth: a meta-analysis of randomized controlled trials. Am J Clin Nutr. 2006;83:1337–1344. http://ajcn.nutrition.org/content/83/6/1337.long[↩]
- The USDA Food Composition Databases. https://ndb.nal.usda.gov/ndb/[↩]
- The USDA Food Composition Databases. DHA Content of Foods. https://ods.od.nih.gov/pubs/usdandb/DHA-Content.pdf[↩]
- The USDA Food Composition Databases. Foods DHA Content. https://ods.od.nih.gov/pubs/usdandb/DHA-Food.pdf[↩]
- Rodriguez-Leyva D, Bassett CM, McCullough R, Pierce GN. The cardiovascular effects of flaxseed and its omega-3 fatty acid, alpha-linolenic acid. The Canadian Journal of Cardiology. 2010;26(9):489-496. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2989356/[↩]
- Mahaffey KR. Fish and shellfish as dietary sources of methylmercury and the omega-3 fatty acids, eicosahexaenoic acid and docosahexaenoic acid: risks and benefits. Environ Res. 2004;95:414–428. https://www.ncbi.nlm.nih.gov/pubmed/15220075[↩][↩][↩][↩][↩][↩]
- Nettleton JA. Omega-3 fatty acids: comparison of plant and seafood sources in human nutrition. J Am Diet Assoc. 1991;91:331–337. https://www.ncbi.nlm.nih.gov/pubmed/1825498[↩]
- U.S. Food and Drug Administration. Eating Fish: What Pregnant Women and Parents Should Know. https://www.fda.gov/downloads/Food/FoodborneIllnessContaminants/Metals/UCM536321.pdf[↩]
- Pawlosky RJ, Hibbeln JR, Novotny JA, et al. Physiological compartmental analysis of alinolenic acid metabolism in adult humans. J Lipid Res. 2001;42:1257–1265. http://www.jlr.org/content/42/8/1257.long[↩]
- Institute of Medicine, Food and Nutrition Board. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids (macronutrients). Washington, DC: National Academy Press; 2005.[↩]
- Newberry SJ, Chung M, Booth M, Maglione M, Tang AM, C.E. OH, et al. Omega-3 fatty acids and maternal and child health: an updated systematic review. Evidence Report/Technology Assessment No. 224. (Prepared by the RAND Southern California Evidence-based Practice Center under Contract No. 290-2012-00006-I.) AHRQ Publication No. 16-E003-EF. Rockville, MD: Agency for Healthcare Research and Quality; 2016.[↩]
- Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2012;129:2011-3552. https://www.ncbi.nlm.nih.gov/pubmed/22371471?dopt=Abstract[↩]
- O’Connor NR. Infant formula. Am Fam Physician 2009;79:565-70. https://www.ncbi.nlm.nih.gov/pubmed/19378873?dopt=Abstract[↩]
- Simmer K, Patole SK, Rao SC. Long-chain polyunsaturated fatty acid supplementation in infants born at term. Cochrane Database Syst Rev 2011:CD000376. https://www.ncbi.nlm.nih.gov/pubmed/22161363?dopt=Abstract[↩]
- Schulzke SM, Patole SK, Simmer K. Long-chain polyunsaturated fatty acid supplementation in preterm infants. Cochrane Database Syst Rev 2011:CD000375. https://www.ncbi.nlm.nih.gov/pubmed/21328248?dopt=Abstract[↩]
- U.S. Food and Drug Administration. Fish: what pregnant women and parents should know. https://www.fda.gov/Food/ResourcesForYou/Consumers/ucm393070.htm[↩]
- ConsumerLab.com. Product review: fish oil and omega-3 fatty acid supplements review (including krill, algae, calamari, green-lipped mussel oil). https://www.consumerlab.com/reviews/fish_oil_supplements_review/omega3[↩]
- Feskanich D, Singh V, Willett WC, et al. Vitamin A intake and hip fractures among postmenopausal women. JAMA. 2002;287:47–54. https://www.ncbi.nlm.nih.gov/pubmed/11754708[↩]
- Olsen SF, Hansen HS, Sommer S, et al. Gestational age in relation to marine n-3 fatty acids in maternal erythrocytes: a study of women in the Faroe Islands and Denmark. Am J Obstet Gynecol. 1991;164:1203–1209. https://www.ncbi.nlm.nih.gov/pubmed/1827949[↩][↩]
- Koletzko B, Larqué E, Demmelmair H. Placental transfer of long-chain polyunsaturated fatty acids (LC-PUFA) J Perinat Med. 2007;35:S5–S11. https://www.ncbi.nlm.nih.gov/pubmed/17302540[↩]
- Heird W.C., Lapillonne A. The role of essential fatty acids in development. Ann. Rev. Nutr. 2005;25:549–571. doi: 10.1146/annurev.nutr.24.012003.132254. https://www.ncbi.nlm.nih.gov/pubmed/16011478[↩]
- Lauritzen L., Hansen H.S., Jorgensen M.H., Michaelsen K.F. The essentiality of long chain n-3 fatty acids in relation to development and function of the brain and retina. Prog. Lipid Res. 2001;40:1–94. doi: 10.1016/S0163-7827(00)00017-5. https://www.ncbi.nlm.nih.gov/pubmed/11137568[↩]
- FAO . Fats and Fatty Acids in Human Nutrition. Volume 91. Karger; Basel, Switzerland: 2010. pp. 1–166. Report of an Expert Consultation. https://www.ncbi.nlm.nih.gov/pubmed/21812367[↩]
- Carlson S.E., Colombo J., Gajewski B.J., Gustafson K.M., Mundy D., Yeast J., Georgieff M.K., Markley L.A., Kerling E.H., Shaddy D.J., et al. DHA supplementation and pregnancy outcomes. Am. J. Clin. Nutr. 2013;97:808–815. doi: 10.3945/ajcn.112.050021. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3607655/[↩]
- Hibbeln J.R., Davis J.M., Steer C., Emmett P., Rogers I., Williams C., Golding J. Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood (ALSPAC study): An observational cohort study. Lancet. 2007;369:578–585. doi: 10.1016/S0140-6736(07)60277-3. https://www.ncbi.nlm.nih.gov/pubmed/17307104[↩]
- Muthayya S., Dwarkanath P., Thomas T., Ramprakash S., Mehra R., Mhaskar A., Mhaskar R., Thomas A., Bhat S., Vaz M., et al. The effect of fish and omega-3 LCPUFA intake on low birth weight in Indian pregnant women. Eur. J. Clin. Nutr. 2009;63:340–346. doi: 10.1038/sj.ejcn.1602933. https://www.ncbi.nlm.nih.gov/pubmed/17957193[↩]
- Luxwolda M.F., Kuipers R.S., Koops J.H., Muller S., de Graaf D., Dijck-Brouwer D.A., Muskiet F.A. Interrelationships between maternal DHA in erythrocytes, milk and adipose tissue. Is 1 wt % DHA the optimal human milk content? Data from four tanzanian tribes differing in lifetime stable intakes of fish. Br. J. Nutr. 2014;111:854–866. doi: 10.1017/S0007114513003255. https://www.ncbi.nlm.nih.gov/pubmed/24175990[↩][↩]
- Van Eijsden M., Hornstra G., van der Wal M.F., Bonsel G.J. Ethnic differences in early pregnancy maternal n-3 and n-6 fatty acid concentrations: An explorative analysis. Br. J. Nutr. 2009;101:1761–1768. doi: 10.1017/S0007114508123455. https://www.ncbi.nlm.nih.gov/pubmed/18983717[↩][↩]
- Otto S.J., Houwelingen A.C., Antal M., Manninen A., Godfrey K., Lopez-Jaramillo P., Hornstra G. Maternal and neonatal essential fatty acid status in phospholipids: An international comparative study. Eur. J. Clin. Nutr. 1997;51:232–242. doi: 10.1038/sj.ejcn.1600390. https://www.ncbi.nlm.nih.gov/pubmed/9104573[↩][↩]
- Heird WC, Lapillonne A. The role of essential fatty acids in development. Annu Rev Nutr. 2005;25:549-71. https://www.ncbi.nlm.nih.gov/pubmed/16011478/[↩]
- Jasani B, Simmer K, Patole SK, Rao SC. Long chain polyunsaturated fatty acid supplementation in infants born at term. Cochrane Database of Systematic Reviews 2017, Issue 3. Art. No.: CD000376. DOI: 10.1002/14651858.CD000376.pub4. http://www.cochrane.org/CD000376/NEONATAL_long-chain-polyunsaturated-fatty-acid-supplementation-infants-born-term[↩][↩]
- Moon K, Rao SC, Schulzke SM, Patole SK, Simmer K. Longchain polyunsaturated fatty acid supplementation in preterm infants. Cochrane Database of Systematic Reviews 2016, Issue 12. Art. No.: CD000375. DOI: 10.1002/14651858.CD000375.pub5. http://www.cochrane.org/CD000375/NEONATAL_longchain-polyunsaturated-fatty-acid-supplementation-preterm-infants[↩][↩]
- Dietary fat intakes for pregnant and lactating women. British Journal of Nutrition, Volume 98, Issue 5, November 2007 , pp. 873-877. https://www.cambridge.org/core/journals/british-journal-of-nutrition/article/dietary-fat-intakes-for-pregnant-and-lactating-women/0D7D3496EE4A080986B649ED90295464/core-reader[↩][↩][↩][↩][↩][↩]
- M Fleith & MT Clandinin (2005) Dietary PUFA for preterm and term infants: review of clinical studies. Crit Rev Food Sci Nutr 45, 205–229.[↩]
- M Martinez & I Mougan (1998) Fatty acid composition of human brain phospholipids during normal development. J Neurochem 71, 2528–2533.[↩]
- JT Brenna (2002) Efficiency of conversion of alpha-linolenic acid to long chain n-3 fatty acids in man. Curr Opin Clin Nutr Metab Care 5, 127–132.[↩]
- GC Burdge & PC Calder (2005) Conversion of alpha-linolenic acid to longer-chain polyunsaturated fatty acids in human adults. Reprod Nutr Dev 45, 581–597.[↩]
- SM Innis (2005) Essential fatty acid transfer and fetal development. Placenta 26, S70–S75.[↩]
- I Cetin , N Giovannini , G Alvino , et al. (2002) Intrauterine growth restriction is associated with changes in polyunsaturated fatty acid fetal-maternal relationships. Pediatr Res 52, 750–755.[↩]
- E Larque , S Krauss-Etschmann , C Campoy , et al. (2006) Docosahexaenoic acid supply in pregnancy affects placental expression of fatty acid transport proteins. Am J Clin Nutr 84, 853–861.[↩]
- RC Greiner , J Winter , PW Nathanielsz & JT Brenna (1997) Brain docosahexaenoate accretion in fetal baboons: bioequivalence of dietary alpha-linolenic and docosahexaenoic acids. Pediatr Res 42, 826–834.[↩]
- H Szajewska , A Horvath & B Koletzko (2006) Effect of n-3 long-chain polyunsaturated fatty acid supplementation of women with low-risk pregnancies on pregnancy outcomes and growth measures at birth: a meta-analysis of randomized controlled trials. Am J Clin Nutr 83, 1337–1344.[↩][↩]
- M Makrides , L Duley & SF Olsen (2006) Marine oil, and other prostaglandin precursor, supplementation for pregnancy uncomplicated by pre-eclampsia or intrauterine growth restriction. Cochrane Database Syst Rev 3, CD003402.[↩][↩][↩]
- A Horvath , B Koletzko & H Szajewska (In Press) Effect of supplementation of women in high-risk pregnancies with long-chain polyunsaturated fatty acids on pregnancy outcomes and growth measures at birth: a meta-analysis of randomized controlled trials. Br J Nutr. Published online 10 April 2007. doi: 10.1017/S0007114507709078.[↩]
- S Krauss-Etschmann , R Shadid , C Campoy , et al. (In Press) Fish oil and folate supplementation of pregnant women and maternal and fetal DHA and EPA plasma levels – a randomized European multicenter trial. Am J Clin Nutr.[↩]
- SR Cheruku , HE Montgomery-Downs , SL Farkas , EB Thoman & CJ Lammi-Keefe (2002) Higher maternal plasma docosahexaenoic acid during pregnancy is associated with more mature neonatal sleep-state patterning. Am J Clin Nutr 76, 608–613.[↩]
- E Oken , RO Wright , KP Kleinman , et al. (2005) Maternal fish consumption, hair mercury, and infant cognition in a U.S. Cohort. Environ Health Perspect 113, 1376–1380.[↩]
- EE Birch , S Garfield , Y Castaneda , D Hughbanks-Wheaton , R Uauy & D Hoffman (2007) Visual acuity and cognitive outcomes at 4 years of age in a double-blind, randomized trial of long-chain polyunsaturated fatty acid-supplemented infant formula. Early Hum Dev 18 Jan.[↩]
- N Fidler , T Sauerwald , A Pohl , H Demmelmair & B Koletzko (2000) Docosahexaenoic acid transfer into human milk after dietary supplementation: a randomized clinical trial. J Lipid Res 41, 1376–1383.[↩]
- B Koletzko , C Agostoni , SE Carlson , et al. (2001) Long chain polyunsaturated fatty acids (LC-PUFA) and perinatal development. Acta Paediatr 90, 460–464.[↩]
- Makrides M, Gibson RA, McPhee AJ, Yelland L, Quinlivan J, Ryan P, DOMInO Investigative Team AT. Effect of DHA Supplementation During Pregnancy on Maternal Depression and Neurodevelopment of Young Children A Randomized Controlled Trial. JAMA. 2010;304(15):1675–1683. doi:10.1001/jama.2010.1507, http://jamanetwork.com/journals/jama/fullarticle/186750[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Golding J, Steer C, Emmett P, Davis JM, Hibbeln JR. High levels of depressive symptoms in pregnancy with low omega-3 fatty acid intake from fish. Epidemiology. 2009;20(4):598-603. https://www.ncbi.nlm.nih.gov/pubmed/19289957[↩]
- Hibbeln JR, Davis JM. Considerations regarding neuropsychiatric nutritional requirements for intakes of omega-3 highly unsaturated fatty acids. Prostaglandins Leukot Essent Fatty Acids. 2009;81(2-3):179-186. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3182570/[↩]
- Meyer BJ, Mann NJ, Lewis JL, Milligan GC, Sinclair AJ, Howe PR. Dietary intakes and food sources of omega-6 and omega-3 polyunsaturated fatty acids. Lipids. 2003;38(4):391-398. https://www.ncbi.nlm.nih.gov/pubmed/12848284[↩]
- Miller BJ, Murray L, Beckmann MM, Kent T, Macfarlane B. Dietary supplements for preventing postnatal depression. Cochrane Database of Systematic Reviews 2013, Issue 10. Art. No.: CD009104. DOI: 10.1002/14651858.CD009104.pub2. http://www.cochrane.org/CD009104/PREG_dietary-supplements-for-preventing-postnatal-depression[↩][↩]
- A randomized trial of docosahexaenoic acid supplementation during the third trimester of pregnancy. Smuts CM, Huang M, Mundy D, Plasse T, Major S, Carlson SE. Obstet Gynecol. 2003 Mar; 101(3):469-79. https://www.ncbi.nlm.nih.gov/pubmed/12636950/[↩]
- Carlson SE, Colombo J, Gajewski BJ, et al. DHA supplementation and pregnancy outcomes. The American Journal of Clinical Nutrition. 2013;97(4):808-815. doi:10.3945/ajcn.112.050021. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3607655[↩]




{kind=link}