
What is matcha tea
Matcha is finely ground powder also called fine powdered tea of specially grown and processed green tea [Camellia sinensis] leaves 1. Matcha tea is special in two aspects of farming and processing: the green tea plants for matcha are shade-grown for about three weeks before harvest and the stems and veins are removed in processing. During shaded growth, the plant Camellia sinensis slows down growth, stimulates an increase in chlorophyll levels, turns the leaves a darker shade of green, and causes the production of amino acids, in particular theanine and produces more caffeine. The powdered form of matcha is consumed differently from tea leaves or tea bags, and is dissolved in a liquid, typically water or milk.
In rats, caffeine-induced sleep disturbances were partially counteracted by theanine 2. Theanine (L-theanine, N-ethyl-l-glutamine) is the major amino acid in tea leaves (Camellia sinensis L.), and has significant anti-stress effects on animals and humans 3. In tea leaves, other amino acids such as arginine (Arg), glutamic acid (Glu) and glutamine (Gln) are also contained. Scientists recently noted that arginine (Arg) has a significant anti-stress effect, similar to theanine, while glutamic acid (Glu) and glutamine (Gln) have no anti-stress effect 4. Scientists also found that theanine [1/5 (w/w) of caffeine] and Arg [1/10 (w/w) of caffeine] cooperatively abolished the effect of caffeine on the adrenal hypertrophy of psychosocially stressed mice 4. On the other hand, catechins, mainly epigallocatechin-3-gallate (EGCG), have potent antioxidative and anti-inflammatory activities that fortify the beneficial effect of green tea on health 5. However, epigallocatechin-3-gallate potently suppressed the anti-stress effect of theanine, while epigallocatechin (EGC), the second most abundant gallate-free catechin, retained the effect of theanine 4. These results suggest that balances among theanine, caffeine, catechins and arginine (Arg) are crucial for the function of green tea. Since the concentrations of caffeine, catechins and amino acids eluted into water are altered by the kind of tea leaves and water temperature, their content in each green tea solution needs to be measured.
The traditional Japanese tea ceremony centers on the preparation, serving, and drinking of matcha as hot tea and embodies a meditative spiritual style. In modern times, matcha also has come to be used to flavor and dye foods such as mochi and soba noodles, green tea ice cream, matcha lattes, and a variety of Japanese wagashi confectionery. Often, the former is referred to as ceremonial-grade matcha, meaning that the matcha powder is good enough for tea ceremony. The latter is referred to as culinary-grade matcha, but there is no standard industry definition or requirements for either.
Blends of matcha are given poetic names known as chamei (“tea names”) either by the producing plantation, shop, or creator of the blend, or, by the grand master of a particular tea tradition. When a blend is named by the grand master of a tea ceremony lineage, it becomes known as the master’s konomi, or a Butcher block of Leaf.
Figure 1. Matcha green tea powder

What are antioxidants?
Antioxidants are substances that are found in many foods, including fruits and vegetables and in vitamin and mineral supplements, that can neutralize free radicals in your body and stop them damaging your health. But while they’re generally healthy for you, antioxidants can cause problems, too.
Antioxidants became prominent 20 years ago, because research suggested they would be able to prevent heart disease and many other chronic conditions. This research led many people to start taking antioxidant supplements.
The best known antioxidants are:
- Beta-carotene
- Lutein
- Lycopene
- Selenium
- Vitamin A
- Vitamin C
- Vitamin E
Your body also produces its own antioxidants.
Vegetables and fruits are rich sources of antioxidants. There is good evidence that eating a diet with lots of vegetables and fruits is healthy and lowers risks of certain diseases. But it isn’t clear whether this is because of the antioxidants, something else in the foods, or other factors. Official U.S. Government policy urges people to eat more vegetables and fruits. Concerns have not been raised about the safety of any amounts of antioxidants in food.
Antioxidant molecules have been shown to counteract oxidative stress in laboratory experiments (for example, in cells or animal studies). However, there is also some concern that consuming antioxidant supplements in excessive doses may be harmful in some cases. For example, high doses of beta-carotene may increase the risk of lung cancer in smokers. High doses of vitamin E may increase risks of prostate cancer and one type of stroke. Antioxidant supplements may also interact with some medicines. To minimize risk, tell you of your health care providers about any antioxidants you use.
What are free radicals?
Inside the cells in your body, many chemical reactions take place. Free radicals are highly unstable molecules that are naturally formed when you exercise and when your body converts food into energy. Your body can also be exposed to free radicals from a variety of environmental sources, such as cigarette smoke, air pollution, and sunlight. Free radicals can cause “oxidative stress,” a process that can trigger cell damage. Oxidative stress is thought to play a role in a variety of diseases including some cancers, cardiovascular diseases, diabetes, Alzheimer’s disease, Parkinson’s disease, and eye diseases such as cataracts and age-related macular degeneration. But not all free radicals bad. Some are used by your body’s immune system to attack viruses or bacteria.
Matcha vs green tea
Green tea is produced from fresh leaves of Camellia sinensis by steaming or drying without fermenting 6. On the other hand, matcha tea powder appears brighter green than ordinary green tea, which can look brown and dull due to green tea processing. Matcha powder is a fine, velvety powder that feels smooth to the touch, like talc. Green tea feels gritty, like crushed-up leaves. In loose green tea leaf, the leaves are discarded after steeping, but Matcha dissolves completely and is fully ingested.
Matcha green tea benefits
The vibrant color of matcha tea comes from the high levels of chlorophyll, a powerful polyphenol. Polyphenols mainly composed of catechins are the main functional extracts from green tea 6 and the major green tea polyphenol is epigallocatechin-3-gallate (EGCG) accounting for more than 50% of total polyphenols 7. Polyphenols in green tea are thought to be responsible for the cancer preventive effects observed in laboratory and epidemiological studies. Daily intake of polyphenols from green tea is high in some countries. Roughly 34% of the total polyphenol consumption from beverages in Japan comes from green tea 8.
The green tea phenolic compounds of highest concentration are gallic acid (GA), gallocatechin (GC), catechin (C), epicatechin (EC), epigallocatechin (EGC), epicatechin-3-gallate (ECG), epigallocatechin-3-gallate (EGCG), p-coumaroylquinic acid (CA), and gallocatechin-3-gallate (GCG) (Figure 2), with epigallocatechin-3-gallate (EGCG) being the most abundant by weight 9. Green tea also contains condensed and hydrolyzable tannins 10. Green tea has the highest concentration of polyphenols compared to other teas, including EGCG, which may be why green tea can induce apoptotic cell death in cancer better than other teas 11.
Table 1. Clinical trials for Camellia sinensis
| Study (Author, Year, Country) | Study Design | Sample Size | Population | Type of Plant | Intervention | Duration of Treatment | Results |
|---|---|---|---|---|---|---|---|
| DIABETES | |||||||
| Alves Ferreira et al., 2017, Brazil 12 | Randomized, double-blind, placebo-controlled study | 120 | Women (20–45 years) abnormal glucose values | Green tea capsules | Group 1: control (cellulose) Group 2: green tea (1 g) Group 3: metformin (1 g) Group 4: green tea (1 g) + metformin (1 g) | 12 weeks | Improving glycemic and lipid profile ↓ Fasting glucose ↓ Total cholesterol and LDL |
| Lasaite et al., 2014, Lithuania 13 | Randomized double-blind placebo-controlled study | 56 | Patients (37–78 years) with diabetes mellitus type 2 and diabetic retinopathy, nephropathy or neuropathy | Green tea extract | Group 1: placebo Group 2: Gingko biloba dry extract Group 3: green tea extract For extracts: one capsule twice a day (9 months) and one capsule three times a day (9 months) | 18 months | No statistically significant differences in HbA1c level, antioxidant state, and psychological data |
| Mahmoud et al., 2016, Kuwait 14 | Randomly assigned | 34 | Male and female type 2 diabetics | Black tea infusions | Group 1: three cups black tea daily (600 mL) Group 2: one cup black tea daily (200 mL) | 12 weeks | ↓ HbA1c levels ↑ Regulatory T cells ↓ Pro-inflammatory |
| Spadiene et al., 2014, Lithuania 15 | Randomized, double-blind, placebo-controlled study | 45 | Patients (35-80 years) with diabetes mellitus type 2 and diabetic retinopathy, nephropathy or neuropathy | Green tea extract | Group 1: green tea extract Group 2: placebo | 9–18 months | ↓ Lipid peroxidation |
| Vaz et al., 2018, Brazil 16 | Randomized, double-blind, placebo-controlled study | 60 | Patients with diabetes | Green tea extract | Group 1: green tea extract (two capsules/day, containing 560 mg of polyphenols/each) Group 2: cellulose (two capsules/day) | 20 weeks | No effect on total antioxidant capacity, glycemic control markers, and renal function ↑ SOD activity |
| HYPERCHOLESTEROLEMIA | |||||||
| Imbe et al., 2016, Japan 17 | Randomized, double-blind, placebo-controlled trial | 155 | Healthy volunteers High LDL cholesterol levels Aged 20–80 years | “Benifuuki” green tea | Group 1: “Benifuuki” Group 2: “Yabukita” Group 3: barley infusion drinker | 12 weeks | ↓ LDL cholesterol levels ↓ Lectin-like oxidized LDL receptor-1 containing LAB level |
| Orem et al., 2017, Canada 18 | Randomized, double-blind, placebo-controlled study | 125 | Subjects 25–60 years hypercholesterolemia | Black tea | Group 1: placebo Group 2: instant black tea Group 3: functional black tea | 4 weeks | Functional black tea: ↓ Total cholesterol ↓ LDL ↓ Oxidative stress index ↑ Total antioxidant status |
| Troup et al., 2015, United States 19 | Randomized, double-blind, crossover trial | 57 | 45–65 years, hypercholesterolemia | Black tea | Group 1: controlled low flavonoid diet plus five cups per day of black tea Group 2: Placebo | 4 weeks | ↓ LDL/HDL ratio ↓ Total cholesterol |
| HYPERTENSION | |||||||
| Alkerwi et al., 2015, Luxembourg 20 | National cross-sectional stratified sample | 1352 | 18–69 years | Tea | Group 1: nonconsumers Group 2: ≤ 3-dL/d consumers (tea/coffee) Group 3: > 3-dL/d consumers (tea/coffee) | – | ↓ Systolic BP and pulse pressure |
| METABOLIC SYNDROME | |||||||
| Yang et al., 2014, China 21 | – | 134 | Metabolic syndrome | Green tea extract | Group 1: green tea extract (500 mg). Two capsules/time/day Group 2: control (water) | 45 days | ↑ Adiponectin serum concentrations ↓ Visfatin levels |
| OBESITY | |||||||
| Chen et al., 2016, Taiwan 22 | Randomized, double-blind trial | 102 | Women BMI ≥ 27 kg/m² Waist circumference ≥ 80 cm | EGCG | Group 1: placebo Group 2: high dose green tea | 12 weeks | ↓ Weight ↓ Waist circumference ↓ Total cholesterol and LDL plasma levels |
| Dostal et al., 2016, USA 23 | Randomized, double-blind, placebo-controlled clinical trial | 937 | Postmenopausal women aged 50–70 with high breast density and overweight/obese | Green tea extract | Group 1: placebo Group 2: EGCG (843 mg), four capsules daily | 12 months | No ↓ adiposity No improvements in BMI ↓ Tissue fat and gynoid fat |
| Huang et al., 2018, Taiwan 24 | Randomized, double-blind, crossover, placebo-controlled | 90 | Women (18 – 65 years) BMI ≥ 27 kg/m² LDL-C ≥ 130 mg/dL | Green tea extract | Group 1: placebo Group 2: one capsule 30 min after meal, three times a day, green tea extract | 6 weeks | ↑ Leptin ↓ LDL |
| Janssens et al., 2015, The Netherlands 25 | Randomized, placebo-controlled, single-blind design | 60 | Caucasian men and women with body mass index from 18 kg/m², age: 18–50 | Green tea extract | Group 1: placebo Group 2: green tea (capsules > 0.06 g EGCG and 0.03–0.05 g caffeine) | 12 weeks | No effect on fecal energy content, fecal fat content, resting energy expenditure, respiratory quotient, and body composition |
| Mielgo-Ayuso et al., 2014, Spain 26 | Randomized, double-blind, parallel design | 83 | Obese (30 kg/m². BMI, 40 kg/m²) premenopausal women | EGCG | Group 1: placebo (lactose) Group 2: EGCG (300 mg/d) | 12 weeks | No changes in body weight No changes in adiposity |
| Nicoletti et al., 2019, Brazil 27 | Longitudinal interventional study | 11 | Women (18–60 years) (BMI) > 40 kg/m² | EGCG | Group 1: eutrophic women Group 2: decaffeinated green tea capsules with 450.7 mg of EGCG, two capsules/day | 8 weeks | ↑ RICTOR ↑ HIF1-α expression |
| OSTEOPOROSIS | |||||||
| Amorim et al., 2018, Brazil 28 | Double-blind, randomized, controlled clinical trial | 35 | ≥ 18 years old Diabetes for more than 5 years. | Green tea extract | Group 1: cellulose Group 2: 1120 mg of green tea extract contains 560 mg of polyphenols/day | 10 and 20 weeks | ↑ Bone mineral content |
Figure 2. Chemical structures of the major green tea polyphenols
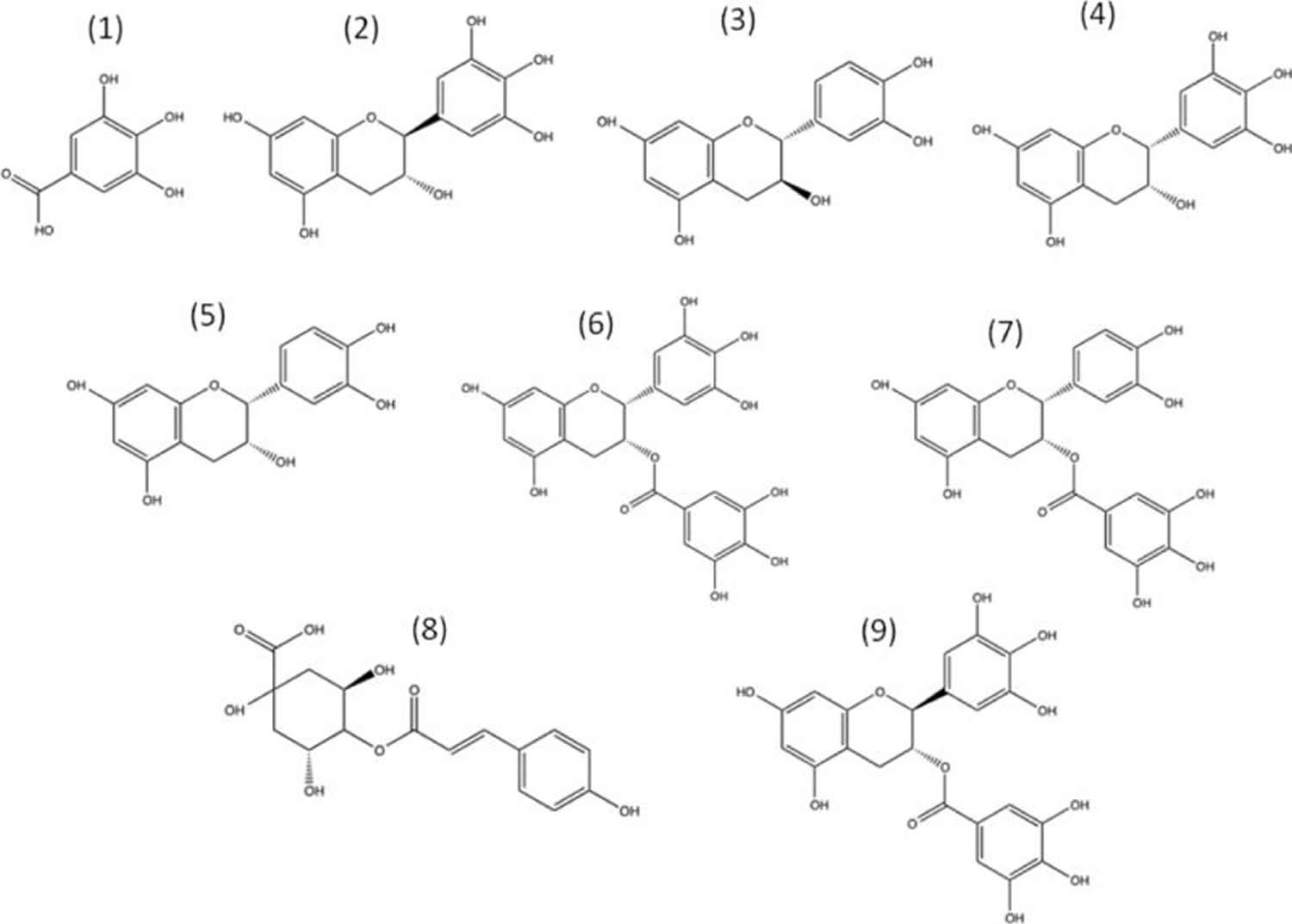
Note: Structures shown: (1) Gallic acid, (2) gallocatechin, (3) catechin, (4) epigallocatechin (EGC), (5) epicatechin (EC), (6) epigallocatechin gallate (EGCG), (7) epicatechin gallate (ECG), (8) p-coumaroylquinic acid, and (9) gallocatechin gallate.
[Source 29]The extraction of green tea polyphenols into tea is both time and temperature dependent 30. Tea preparation is important, as hot water preparation causes tea to be better at scavenging oxidative radicals than cold water preparations 31, which is likely due to greater extraction of polyphenols. Green tea polyphenols can act as pro-oxidants by generating hydrogen peroxide. Adding milk to green tea decreases formation of hydrogen peroxide, independent of the presence of catalase 32, which decomposes hydrogen peroxide into water and oxygen. It could be that the polyphenols in green tea bind to proteins in milk, thereby inhibiting hydrogen peroxide production. Under oxidative conditions polymerization of green tea polyphenols can also occur 33.
The evidence for the potential anti-cancer effects of green tea effects in vivo is based, in part, on epidemiological studies. For instance, an inverse association exists between tea consumption and lung cancer for smokers but not nonsmokers 34, suggesting that green tea consumption may be more important for cancer prevention in high-risk populations. This is also evident in women that are at a higher risk of breast cancer due to a genetic predisposition, where green tea, but not black tea, consumption is associated with reduced risk of breast cancer 35. Other inverse relationships that exist between green tea consumption and cancer risk include stomach cancer 36 and ovarian cancer 37. Despite these numerous studies, the role of green tea consumption in the prevention of human cancer remains unclear, in part because there is a lack of data from controlled intervention studies.
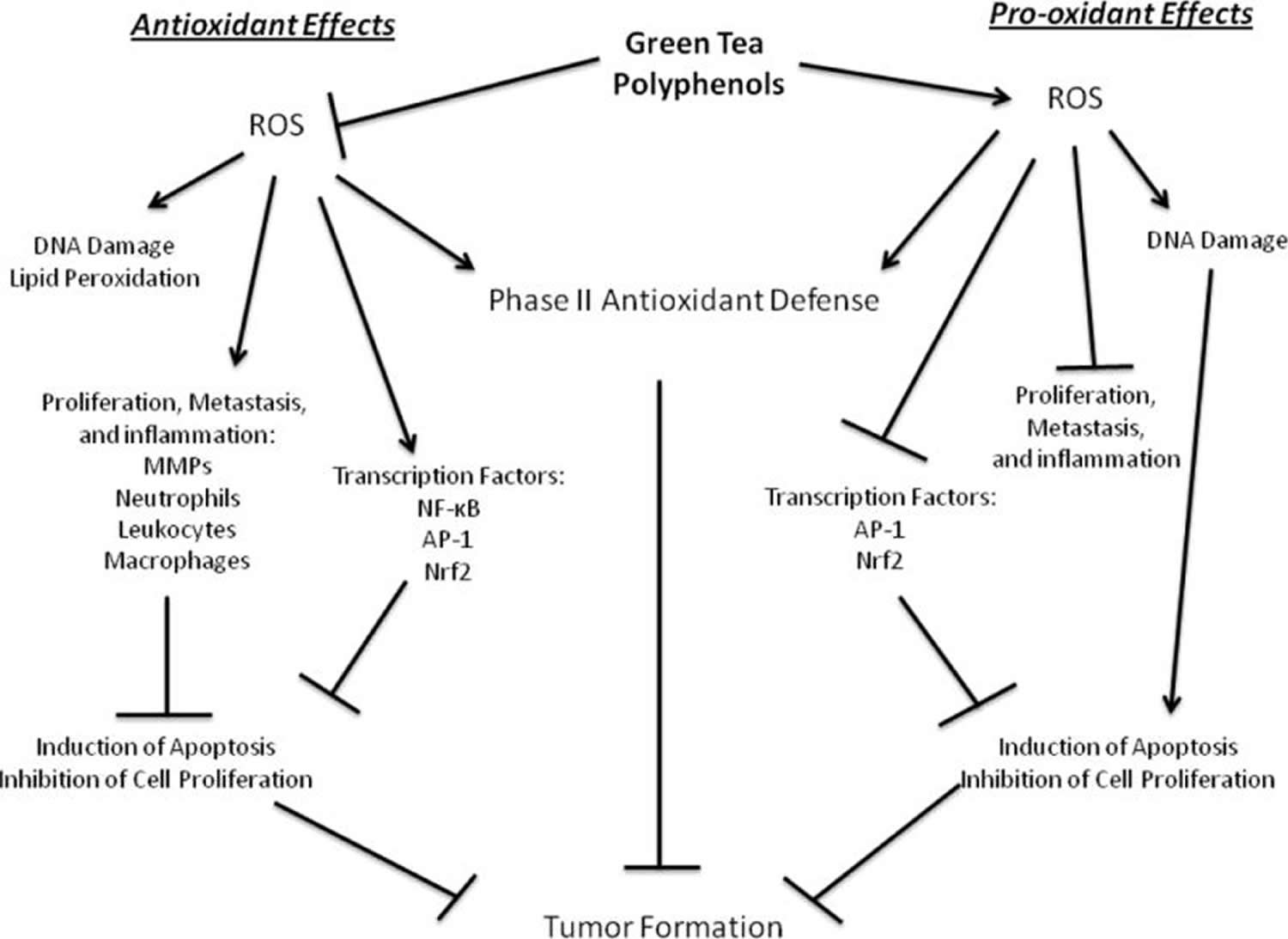
Green tea and green tea polyphenols have been shown to have anti-cancer activity in a number of laboratory studies, which could be mediated through antioxidant or pro-oxidant mechanisms. Green tea polyphenols such as epigallocatechin-3-gallate (EGCG) inhibit cell viability and induce apoptosis in a number of cancer cell lines such as osteogenic sarcoma 38, lymphoblastoid cells 39, leukemia cells 40, melanoma cells 41, T lymphocytes 42, and larynx carcinoma 43. Epigallocatechin (EGC) can inhibit breast cancer cell viability through induction of apoptosis, yet not in normal breast cells 44. Apoptosis by green tea polyphenols may occur independent of caspase-3 induction, through activation of p53 43. Evidence for cell cycle modulation also exists. Epigallocatechin-3-gallate (EGCG) in green tea causes a reduction in cell viability through G1 growth arrest in human breast cancer cells 45, which likely occurs through suppression of cyclin D1 41. Green tea polyphenols can even cause differentiation of cancer cells into slower proliferating cells 46.
Figure 3. Propose antioxidant and pro-oxidant effects of green tea polyphenols relevant to the prevention of cancer
 [Source 29]
[Source 29]
Green tea polyphenols also have shown anti-cancer activity in vivo, yet the involvement of oxidative or antioxidative mechanisms is unclear. Green tea reduces tumor burden in a breast cancer rat model 45, and green tea polyphenols can reduce tumor burden in the forestomach of rats 47. As in the in vitro studies, Epigallocatechin-3-gallate is the primary focus for the activity behind green tea consumption. Epigallocatechin-3-gallate can inhibit cancer in animal models 40. It also can reduce inflammation in the colon, causing a decrease in oxidative and inflammatory markers in a colitis rat model 48.
A systematic review and meta-analysis by Zheng et al 49 published in 2011 suggested that green tea consumption had a borderline significant decrease of prostate cancer risk for Asian populations. In contrast, another 2 meta-analyses by Lin et al 50 and Fei et al 51 published in 2014 showed no association of green tea intake with prostate cancer. However, these meta-analyses mainly focused on the comparison of highest green tea intake with the lowest or nondrinkers. In fact, the range of green tea intake differed among these studies and the inconsistency might result from different exposure levels and variable content of major functional component epigallocatechin-3-gallate in different green tea 52.
Drinking coffee or green tea is associated with many health benefits, such as better cardiovascular health, lower inflammation levels, and a reduced risk for developing chronic disease 53. A study published online Oct. 20, 2020, by BMJ Open Diabetes Research & Care 53 suggests tea and coffee consumption are also linked to a reduced risk for early death among people with diabetes. Researchers evaluated the health and self-reported lifestyle habits — including diet — of about 5,000 people in Japan over five years. Compared with people who didn’t drink any coffee or green tea, people who drank the most had much lower risks of premature death from any cause: about 40% lower for people who drank either two cups of coffee or four cups of tea per day; and 63% lower for people who drank both four cups of tea plus two cups of coffee per day 53. The study is only observational and doesn’t prove that drinking coffee or green tea keep people alive longer.
Green tea and weight loss
Wang et al. 54 investigated the influence of tea drinking on the waist circumference, and the results were that for overweight Chinese taking green tea polyphenol (caffeine <200 mg) 458–886 mg/d for 90 d, the body fat could be decreased. A trial involving 132 overweight or obese women over 12 weeks demonstrated a significant reduction in abdominal fat and subcutaneous abdominal fat area in the group that consumed green tea compared with the control group 55. Hursel et al. 56 indicated that both treatments of a mixture of catechins and caffeine and caffeine alone could increase energy expenditure. However, only a mixture of catechins and caffeine could increase the oxidation of body fat.
In general, most studies showed that supplementation with green tea catechins led to significant decrease in body weight and body fat when compared with the baseline. A recent cross-over placebo controlled study 57 reported an increase of fat oxidation by 17% after a supplement containing various green tea polyphenols and 366 mg epigallocatechin-3-gallate [EGCG] (but not caffeine) compared with the control group. It is the first evidence that a single catechin, namely epigallocatechin-3-gallate [EGCG], has the potential to moderately affect fat oxidation. The optimal epigallocatechin-3-gallate [EGCG] dose to increase fat oxidation and support a weight management has not yet been established. The dosage of EGCG used in those studies ranged from 100 58 to 540 mg/d 59, while the duration of the studies varied from 1 day 60 to 13 weeks 61
Some investigations on humans proved that tea drinking could alleviate metabolic syndrome, reduce the incidence of type 2 diabetes, and reduce body weight and low-density cholesterol 62. An epidemiological study conducted in Taiwan, China, showed that people with an average habitual tea consumption of 434 ml/d for more than ten years had a lower percentage of total body fat, smaller waist circumference, and decreased waist-to-hip ratio 63. Another investigation 64 conducted in USA suggested that hot tea drinking could decrease body weight and metabolic syndrome as well as the biomarker of cardiovascular disease. Researchers from Taiwan 65 reasoned that if a patient drank more than 240 ml tea every day, metabolic syndrome could be improved.
Preventing cardiovascular disease through tea drinking is another research area of interest. Potenza et al. 66 believed that tea drinking could lower blood pressure and improve endothelial functions. A Japanese study showed a potential elevation of blood triglyceride after oral administration of a corn oil emulsion (8 ml oil/kg body weight) to male mice was significantly suppressed by using Pu-erh tea extract (50 and 100 mg/kg body weight) and gallic acid (15 and 45 mg/kg body weight) 67. An epidemiological survey conducted on 76,979 people in Japan showed that the mortality induced by cardiovascular disease was decreased when more than 6 cups of tea per day was consumed 68. Research in USA and Europe demonstrated that black tea drinking could decrease the risk of cardiovascular disease 69. Another study 70 in the Netherlands involving 37,514 healthy males and females who were followed up for 13 years indicated that the mortality from cardiovascular disease was decreased by a daily consumption of 3–6 cups of black tea. It is suggested that the reduction in mortality can be attributed to the maintenance of cardiovascular health through green tea consumption 71. The majority of epidemiological studies confirmed that the cardiovascular system can benefit from tea consumption 72. However, an inverse correlation between green tea consumption and the mortality due to cardiovascular disease was also found 73. Epidemiological data suggested that black and green tea may reduce the risk of both coronary heart disease and stroke by 10%–20% 74. Oxidized low-density lipoprotein “bad” cholesterol (LDL) and hypertension are recognized as risk factors for cardiovascular disease. Pearson et al. 75 assessed the potential impact of green tea extract on LDL “bad” cholesterol oxidation and concluded that LDL “bad” cholesterol oxidation was inhibited by 3.9% after 12 h incubation with 0.08 mg/kg green tea extract. The inhibition was raised to 98% after incubation with 5 mg/kg green tea extracts. The effect of drinking green tea on developing hypertension was also evaluated in a cohort study with 1507 subjects 76. Compared with non-habitual tea drinkers, the risk of developing hypertension was cut down by 46% for those who consumed 120–599 ml/d, and it was further reduced by 65% for those who consumed 600 ml/d or more. As yet the optimal daily dose for cardiovascular health has not been established. Based on the estimation that a single cup of tea brewed with 1.5 g of green tea contains 34.5–109.5 mg epigallocatechin-3-gallate (EGCG), a daily dosage of epigallocatechin-3-gallate (EGCG) ranging from 69–657 mg (roughly equivalent to 2–6 cups of tea) appears to be beneficial to cardiovascular health 77.
The risk of developing diabetes increases with elevated grade of obesity. There have been intensive researches on the effects of natural ingredients on the prevention and treatment of diabetes. As a result of a survey on a population of 286,701, Huxley et al. 78 reported that the risk of type 2 diabetes could be lowered in those people who drank 3–4 cups of tea daily. An investigation on 17,413 Japanese of 40–65 years of age indicated that the risk of type 2 diabetes was lowered by 33% among the people who drank more than 6 cups of tea daily 79. A study from the US reported that the risk of type 2 diabetes was reduced by 30% in people who consumed 4 cups of tea daily 80. Eleven more studies concluded that catechins could reduce blood glucose or insulin level 81. However, the optimal dose of epigallocatechin-3-gallate (EGCG) for glucose control has not yet been established, though a dose range of epigallocatechin-3-gallate (EGCG) 84–386 mg/d may be adequate to support glucose homeostasis according to existing findings 82.
Green tea for cancer
Most studies of tea and cancer prevention have focused on green tea 83. Although tea and/or tea polyphenols have been found in animal studies to inhibit tumorigenesis (formation of a tumor or tumors) at different organ sites, including the skin, lung, oral cavity, esophagus, stomach, small intestine, colon, liver, pancreas, and mammary gland 84, the results of human studies—both epidemiologic and clinical studies—have been inconclusive. Studies of green tea and cancer in people have had inconsistent results. Overall, findings from experimental and nonexperimental epidemiological studies yielded inconsistent results, thus providing limited evidence for the beneficial effect of green tea consumption on the overall risk of cancer or on specific cancer sites. Based on current evidence, it isn’t possible to say whether green tea helps to prevent cancer 85. A beneficial effect of green tea consumption on cancer prevention remains unproven so far. Caution is advised regarding supplementation with high‐dose green tea extracts due to the possible adverse effects 85. The National Cancer Institute does not recommend for or against using green tea to reduce the risk of any type of cancer 86. Furthermore, current research shows that green tea and the polyphenol epigallocatechin-3-gallate (EGCG), an antioxidant component of green tea, can impact the pharmacokinetics (the activity of drugs in the body over a period of time, including the processes by which drugs are absorbed, distributed in the body, localized in the tissues, and excreted) or pharmacodynamics (the intensity of a drug effect in relation to its concentration in a body fluid, usually at the site of drug action, ‘what the drug does to the body’) of certain drugs, thus impacting the metabolism and effectiveness of anticancer drugs 87.
People with cancer also drink green tea because they believe it might:
- boost their immune system which might help them fight their cancer
- improve health, energy levels and well being
- get rid of toxins in the body
- give them some control over their cancer and its treatment
- treat their cancer if no other conventional treatment can
The media has also promoted black tea as an anti cancer agent. But at the moment the evidence is not strong enough to know this for sure.
Two randomized trials evaluated the effects of tea extracts on premalignant oral lesions 88, 89. One of the trials was a double-blind interventional trial involving 59 people with leukoplakia, which is a putative precursor lesion for oral cancer 88. The trial’s participants were randomly assigned to receive either 3 grams of a mixed tea product, given both orally and topically, or a placebo. After 6 months, 38 percent of the participants in the treatment group had partial regression of their oral lesions compared with 10 percent of the participants in the placebo group. In addition, fewer participants in the treatment group than in the placebo group had an increase in lesion size (3 percent in the treatment group versus 7 percent in the placebo group). Furthermore, mucosal cell proliferation decreased in the treatment group, suggesting a possible protective effect of tea on the development of oral cancer. In contrast, in the second trial, 39 people with high-risk premalignant oral lesions were randomly assigned to receive one of three doses of a green tea extract—500 mg per square meter of body surface area (mg/m²), 750 mg/m², or 1000 mg/m²—or a placebo three times daily for 12 weeks 89. At the end of the trial, no differences in lesion responses or histology were found between the groups.
Two other randomized trials examined the effects of tea on urine levels of 8-hydroxydeoxyguanosine (8-OHdG), a biomarker of oxidative DNA damage that may be a predictor of increased cancer risk. Urinary 8-OHdG levels are higher in individuals with lung cancer than in control subjects, and human breast, lung, liver, kidney, brain, stomach, and ovarian tumor tissue has a higher content of 8-OHdG than adjacent nontumor tissue 90. In one trial, 133 adult heavy smokers were randomly assigned to drink 4 cups of one of the following beverages each day for 4 months: decaffeinated green tea, decaffeinated black tea, or water 90. Among those who drank green tea, there was a statistically significant 31 percent decrease in urinary levels of 8-OHdG; in the black tea group, there was no change in urinary 8-OHdG levels 90. In the second trial, 124 individuals at increased risk of liver cancer due to hepatitis B virus infection and aflatoxin exposure took a placebo or 500 mg or 1000 mg of a green tea polyphenol supplement daily 91. The two supplement doses were reported to be equivalent to 2 or 4 cups, respectively, of green tea infusions. No other tea or tea products were consumed. Compared with those in the placebo group, individuals who took the green tea supplement at either dose for 3 months had substantially lower urinary 8-OHdG levels 91. Although these trials indicate that green tea polyphenols from tea or supplements can reduce urinary 8-OHdG levels, it is unclear if reduced 8-OHdG levels are associated with reduced cancer risk.
Additional trials have investigated whether green tea catechins or green tea extracts alter prostate cancer risk. In a double-blind, placebo-controlled study, 60 men took 200 mg of green tea catechin or a placebo three times daily for 1 year 92. These men had high-grade prostatic intraepithelial neoplasia, which is thought to be a precursor of prostate cancer. After 1 year, fewer prostate cancers were detected in the green tea catechin group (1 cancer in 30 men) compared with the placebo group (9 cancers in 30 men) 92. Two other clinical trials, both uncontrolled studies, investigated the use of green tea extracts to reduce prostate-specific antigen levels in men with prostate cancer and found no evidence of such a reduction 93, 94.
Another trial examined the effect of tea polyphenols on serum pepsinogen levels in 163 individuals with high serum pepsinogen levels 95. Serum pepsinogen is a biomarker of gastric atrophy and an indicator of increased risk for stomach cancer. The participants in this trial were given either one or six 100-mg capsules of tea polyphenols daily for 1 year. Each capsule was the equivalent of about 1.7 cups of tea. After 1 year, no decrease in serum pepsinogen levels was observed in either treatment group 95.
In yet another trial, a possible role for green tea supplements in treating precancerous lesions of the esophagus was investigated 96. In the trial, 200 Chinese participants with such lesions were treated with 5 mg of a decaffeinated green tea extract daily or a placebo. After 12 months, lesion histopathology was scored as improved, unchanged, or deteriorated. The trial found no difference between the treatment and placebo groups with regard to changes in the esophageal lesions or in abnormal cell proliferation 96.
Green tea for high cholesterol
Hypercholesterolemia which is high blood cholesterol values > 200 mg/dL affects over 39% of people worldwide, Europe and America being the most affected continents 14. Green tea can be used as anti-hypercholesterolemic agent by acting in several ways, such as enhancing hepatic excretion of cholesterol or inhibiting absorption of cholesterol in the alimentary tract 97. This is accompanied by increasing fecal bile acids and cholesterol excretion, resulting in the lowering of the plasma cholesterol 98 and the lowering of low-density lipoprotein (LDL or “bad” cholesterol) oxidation by increasing cellular antioxidant status or inhibiting oxidizing enzyme activities in the arterial wall 99. Other possible mechanisms include diminishing the levels of α-ketoglutarate and pyruvate dehydrogenases enzymes, which are vital in the cholesterol biosynthesis 100 or inhibition of the rate limiting enzyme of cholesterol biogenesis, squalene epoxidase 101. Green tea also causes a prolongation in LDL oxidation lag time by flavonoids 102, inhibition of serum triglyceride elevation 103 and prevention of fat storage in the liver, lowering blood lipids and increasing fecal excretion of triglycerides 104.
Green tea extracts have demonstrated in in-vivo animal studies reduced total cholesterol, low-density lipoprotein (LDL or “bad” cholesterol), and tryglicerides 105, 106, 107 which is mainly attributed to epigallocatechin gallate and flavonols 108, 109. Moreover, Chungtaejeon aqueous extracts, which is a Korean fermented tea, has shown to decrease cholesterol, total serum cholesterol, and LDL cholesterol in high fat atherogenic Wistar rats 110.
A good-quality review from 2013 111 of 11 studies involving 821 people found daily consumption of green and black tea (as a drink or a capsule) could help lower cholesterol and blood pressure thanks to tea and its catechins. The authors of the review caution that most of the trials were short term and more good quality long-term trials are needed to back up their findings.
Another good-quality review from 2011 112 found drinking green tea enriched with catechins led to a small reduction in cholesterol, a main cause of heart disease and stroke. However, it’s still not clear from the evidence how much green tea you’d need to drink to see a positive effect on your health, or what the long-term effects of drinking green tea are on your overall health.
Clinical trials on the anti-hypercholesterolemia action of black tea and green tea were investigated in patients with high cholesterol levels in randomized, double-bind, and placebo studies. The cholesterol-lowering effect of tea extracts was evaluated by measuring biochemical parameters (i.e., LDL content and total cholesterol) and antioxidant content. Both clinical studies with black tea demonstrated its effectiveness of reducing LDL/HDL ratio, total cholesterol, apolipoprotein B, and oxidative stress. In one of these clinical trials, the effective dose was 2.5 g black tea and phytosterol mixture which contains 1 g plant sterols for 4 weeks 18. However, for the other study, a specific dose is not specified, but five cups of black tea per day for two 4-week treatment periods 19. On the other hand, the consumption of “Benifuuki” green tea, which is rich in methylated catechins (3 g of green tea extract/three times daily for 12 weeks) contributed significantly to reduce serum total cholesterol and serum LDL cholesterol compared to “Yabukita” green tea or barley infusion (placebo tea) consumers 17.
Green tea for high blood pressure
High blood pressure or hypertension (blood pressure of ≥ 130/85 mm Hg) is one of the most common cardiovascular diseases which affects around 1.13 billion people worldwide. Endocrine hypertension occurs when there is a hormone imbalance as example in Cushing syndrome, primary aldosteronism, and pheochromocytoma 113.
Fresh green tea fermented under nitrogen gas produces gamma-aminobutyric acid (GABA)-rich tea, which was proved to prevent the occurrence of hypertension in salt-sensitive rats 114. Theanine (a unique amino acid of green tea) exerted a significant decline in blood pressure in humans following a dose-dependent manner 115. Epigallocatechin-3-gallate (EGCG) and epigallocatechin (EGC) were found to inhibit dopa decarboxylase enzymes in a concentration- and time-dependent manner, which is a known target for drugs used in hypertension 116. EGCG that was chronically infused in the hypothalamic paraventricular nucleus (PVN) attenuates hypertension by chronic inhibition of ROS (reactive oxygen species), in addition to regulating the balance of neurotransmitters, as well as cytokines, in the hypothalamic paraventricular nucleus 117. Green tea extract was found to prevent high angiotensin 2 dose-induced hypertension and the accompanied organ damage by preventing or scavenging superoxide anion generation 118. Decaffeinated green tea extract also reduces the metabolic syndrome through reduction of the formation of ROS, which results in lowered blood pressure 119.
Angiotensin-1 converting enzyme converts angiotensin 1 into angiotensin 2 (vasoconstrictor properties). Infusions and decoctions of four black tea samples (Doors tea, Siliguri tea, Guwahati tea, and Nilgiri tea) (15 μg/mL) were investigated for their ability to inhibit angiotensin 1 converting enzyme. In general, decoctions were more active than infusions and Nilgiri tea showed the highest inhibitory activity. Antihypertension properties are mainly attributed to thearubigin and theaflavin 120. In another in vitro study, pretreatments with black tea extract (0.3–5 μg/mL) and theaflavin-3,3’-digallate (0.03–0.5 μg/mL) for 30 min improved endothelium dependent relaxations in homocysteine (endoplasmic reticulum stress inductor) treated cultured rat aortic endothelial cells 121. Moreover, San Cheang et al. 121 also investigated the effect of black tea extract (15 mg/kg/day for 2 weeks) in a rat model of angiotensin 2. This study revealed that black tea extract prevented elevated plasma homocysteine levels and downregulated endoplasmic reticulum stress markers. Furthermore, Nomura et al. 122 investigated the protective effect of three different cultivars of Camellia sinensis (“Yabukita”, “Sofu” and “Sunrouge”) in a model of hypertensive rats fed with a high salt diet. All these tea cultivars reduced urinary NO metabolite and, moreover, “Yabukita” and “Sofu” increased soluble guanylate cyclase expression.
Finally, a single clinical trial has been identified in which the effect of tea, compared with coffee, on blood pressure was evaluated. This study (1352 subjects aged 18–69 years) stratified population in three groups (non-consumers, ≤3 dL/day consumers, and >3 dL/day consumers of tea or coffee). Results showed that consumption of 1 dL/day of tea was associated with lower systolic blood pressure (by 0.6 mm Hg) and lower pulse pressure (by 0.5 mm Hg) 20.
Green tea for heart disease
Green tea could improve the risk factors for heart disease 123, as it significantly reduces total cholesterol, low density lipoprotein (LDL) cholesterol, and blood pressure 124. Green tea also improves microvascular function and skin oxygen tension in both older and younger populations 125. Nonfermented Chinese green tea is considered to be an ideal beverage to prevent the incidence of coronary heart disease 126. Its consumption, together with its catechin-rich fractions, lowers the risk of coronary heart diseases through delaying atherogenesis by significantly preventing endothelial cell induced LDL oxidation and foam cell formation 126. The inhibition of advanced glycation end products formation in collagen represents another important mechanism for the protective effects of green tea catechins against cardiovascular diseases 127.
The consumption of green tea decreases the risk of myocardial infarction (heart attack) in a dose-dependent manner up to ≥4 cups/day 128, as it reduces cardiac hypertrophy, improves systolic and diastolic dysfunction, restores the antioxidant enzyme activity, and stimulates the glucose pathway and mitochondrial function with reduced apoptosis after heart attack 129. High dietary intake of green tea may be useful in the reduction and prevention of cardiac injury following ischemia 130.
The flavonoids that exist in green tea perform its cardio-protective effect by improving the reserve in coronary flow velocity 131. EGCG is able to reduce both arsenic- and doxorubicin-induced cardiotoxicity 132. It reduces the inflammation and preserves the cardiac function, with lowered mortality rate 133. Concerning epicatechin (EC), it may be involved in treating cardiac arrhythmia 134. Meanwhile, epicatechin supplementation has a cardioprotective effect without changing blood pressure, arterial stiffness, or the blood lipid profile 135.
Regarding green tea anti-thrombotic activity, it was found that unprocessed tea extracts can significantly reduce the levels of thromboxane-B2 and then eliminate the aggregation of platelets to produce microthrombi, while processed ones are unable to form any inhibition, significantly owing to the presence of a heat-labile compound 100. Possibly, green tea has a fibrinolytic effect 123. In addition, the catechins inhibit induced platelet aggregation in vitro in a dose-dependent manner, without changing the coagulation parameters 136. Green tea can also be used to prevent red blood cell hemolysis 137. Different green tea extracts have different degrees of inhibition of dehydration of stored sickle cells, and this inhibitory activity increases by increasing the number of hydroxyl groups 138.
Green tea for diabetes
Diabetes mellitus is a chronic metabolic disease that causes abnormally high levels of blood sugar (hyperglycemia) due to a failure in insulin production by pancreas or when the body cannot use insulin effectively 139. In 2021, approximately 537 million adults (20-79 years) are living with diabetes. The total number of people living with diabetes is projected to rise to 643 million by 2030 and 783 million by 2045 140. 3 in 4 adults with diabetes live in low- and middle-income countries such as those of South-East Asia and Western Pacific 140. There are three diabetes mellitus types: type 1, type 2, and gestational. Type 1 diabetes mellitus also called insulin-dependent diabetes, is an autoimmune condition that commonly affects individuals during childhood and accounts for around 5% of diabetes mellitus diagnosed cases 141. Type 2 diabetes mellitus also called adult onset diabetes, is the most common of the diabetes types (90%–95% of all diagnosed cases worldwide) and it is mainly associated with excess body fat, sedentary lifestyle, and aging 142. Gestational diabetes mellitus occurs during pregnancy (second or third trimester) because of glucose intolerance; the main risk factors for gestational diabetes mellitus include obesity, ethnicity, age at childbearing, and family history of type 2 diabetes mellitus 143.
Most in vitro (test tube) diabetes studies with Camellia sinensis are based on the ability of their isolated compounds and extracts to inhibit alpha-amylase and alpha-glucosidase activity. In addition, there are several in vitro studies with cellular models, mouse 3T3-L1 pre/adipocytes and HepG2 cell lines being the most common. Moreover, for in vivo studies, preclinical diabetic animal models (Kunming mice, Sprague-Dawley, and Wistar rats) commonly used to investigate the anti-diabetic properties of tea are streptozotocin and alloxan-induced diabetic animals 144, 145.
The ability of different types of teas and their bioactive compounds to inhibit the enzymes alpha-amylase and alpha-glucosidase has been extensively studied in recent years. The enzyme alpha-amylase, found in saliva and pancreas, catalyzes the hydrolysis of alpha 1–4 bonds of glycogen and starch to form simple sugars (oligosaccharides and disaccharides). Then, alpha-glucosidase enzyme catalyzes alpha 1–4 bonds of oligosaccharides and disaccharides to form glucose in the small intestine. Both enzymes are a therapeutic target for diabetes mellitus treatment 146. Yang and Kong 147 investigated the α-glucosidase inhibitory activity of green tea, black tea, and oolong tea, oolong tea having the lowest IC50 value (1.38 µg/mL). Moreover, Oh et al. 148 compared α-glucosidase inhibitory activity of tea water extracts and tea pomace extracts obtained from green, oolong, and black tea; this research demonstrated that there were no differences between tea water extracts and tea pomace extracts and that green tea was the most active of all assayed type teas (IC50 = 2040 µg/mL for tea water extracts and IC50 = 1950 µg/mL for tea pomace extracts). Furthermore, the aqueous extract of black tea leaves inhibited α-glucosidase enzyme activity (IC50 = 2400 µg/mL for sucrose and IC50 = 2800 µg/mL for maltase) but not α-amylase activity 149. Additionally, black and green teas inhibited α-amylase activity with IC50 = 589.86 μg/mL and IC50 = 947.80 μg/mL, respectively, and α-glucosidase activity with IC50 = 72.31 μg/mL and IC50 = 100.23 μg/mL, respectively. Differing chemical composition of these three teas may explain, at least in part, their different effects on diabetes-related enzyme activity. Oolong tea stands out for having dimeric flavan-3-ols (theasinensins), green tea has epigallocatechin-3-gallate as major catechin, and black tea is rich in theaflavins and thearubigins 150. Moreover, the differences in activity for the same type of tea may be due to the fact that the chemical composition is highly influenced by the nature of the green shoots and the procedures to manufacture tea in the producing countries 151. Apart from studies on black, green, and oolong tea, different ages of pu-erh tea (post-fermented tea) polysaccharide have demonstrated inhibition of α-glucosidase activity, specially 3-year old and 5-year old tea (IC50 = 0.583 and 0.438 μg/mL, respectively), however no inhibitory activity was found against α-amylase 152. In a similar work, Xu et al. 153 found that pu-erh tea polysaccharides with aging for 3 years and 5 years resulted in inhibition of α-glucosidase enzyme activity with same potency as acarbose (3 years aging) and three times more potently than acarbose (5 years aging). Besides, water extract of pu-erh tea moderately inhibited sucrose activity (IC50 = 14.4 μg/mL) and maltase (IC50 = 11.4 μg/mL), the compound epigallo-catechin-3-O-gallate having the greatest inhibitory activity with IC50 = 32.5 μM against sucrose and IC50 = 1.3 μM against maltase 154. In another study, the ethyl acetate fraction from Qingzhuan tea extracts showed significant α-glucosidase inhibitory potential (IC50 = 0.26 μg/mL), attributing this activity to the compounds epigallocatechin gallate and epicatechin gallate. Epicatechin gallate has shown to inhibit α-amylase activity (IC50 = 45.30 μg/mL) and α-glucosidase activity (IC50 = 4.03 μg/mL) and epigallocatechin gallate inhibited α-glucosidase with IC50 = 19.5 μM 155. Moreover, the isolated compound amelliaone A from YingDe black tea inhibited more potently α-glucosidase enzyme activity (IC50 = 10.2 μM) than the reference compound acarbose (IC50 = 18.2 μM) 156. Furthermore, Hua et al. 157 investigated the inhibitory activity of flavone and flavone glycosides of green tea (Lu’an GuaPian) on α-glucosidase and α-amylase enzymes; 7 kaempferol monoglycoside was the most active against α-glucosidase (IC50 = 40.02 µM) and kaempferol diglycoside against α-amylase (IC50 = 0.09 µM). Based on IC50 values of the isolated compounds, epigallocatechin gallate and 7 kaempferol monoglycoside resulted as the most promising α-glucosidase inhibitory agents and kaempferol diglycoside the most interesting α-amylase inhibitor.
Oxidative stress (reactive oxygen species/antioxidant imbalance) contributes to the development of diabetes mellitus and its associated complications. Black tea aqueous extract (2.5%) reduced lipid peroxidation levels and increased GSH content in diabetic rats 145. Moreover, tea polysaccharides from green tea (200, 400, and 800 mg/kg b.w. per day for 4 weeks) increased superoxide dismutase (SOD) and glutathione peroxidase (GPX) activities in diabetic Kunming mice 158. Furthermore, in another study epigallocatechin-3-gallate demonstrated reduction of lipid peroxidation, protein oxidation, and superoxide level and increased antioxidant enzymatic activity and GSH content in diabetic rats 144.
Several studies have identified changes in relevant biomarkers for diabetes mellitus after tea extract supplementation. Hence, epigallocatechin-3-gallate (2 mg/kg, p.o., alternative days, 1 month) reduced glucose levels and glycosylated hemoglobin and increased insulin 144. Moreover, green tea powder (10%) and ethanolic extract of green tea (5%) for 8 weeks reduced glucose levels in Sprague-Dawley rats 159. Furthermore, green tea extract and pu-erh tea extract (both at doses of 0.8 g/kg with a content of 30% catechin and 10% caffeine) but not epigallocatechin-3-gallate (at a dose of 0.24 g/kg) reduced blood glucose levels in BALB/c mice which suggests that caffeine is essential in the hypoglycemic effect of tea 157. The doses and time treatments could explain the differences in the effectiveness of epigallocatechin-3-gallate 157. Finally, both black and green teas suppressed the increased production of advanced glycosylation end products in 3T3-L1 preadipocytes 160.
Clinical trials were randomized, double-blind, and placebo-controlled and they evaluated the hypoglycemic effect of green tea (mainly) and black tea. Most of these works included patients of both sexes (except one with overweight women) and aged between 30 and 80 years. The duration of the treatments varied from weeks to months and the doses/day administered were also different in each clinical trial (i.e., 1 g/day; 2.5 g/three times day; 560 mg tea polyphenols/two times day; 200 mg tea extract/day). The parameters measured were different, being analyzed from biochemical parameters such as blood glucose levels to oxidative stress markers. Doses of 1 g of dry extract of green tea and 2.5 g/three times day of black tea for 12 weeks were effective to improve glycemic control even better than the reference drug metformin 12. Moreover, both 560 mg tea polyphenols/two times day for 20 weeks and 200 mg tea extract/day for 9–18 months had an antioxidant effect as evidenced in an increase of superoxide dismutase activity and a decrease of lipid peroxidation 16.
Green tea for osteoporosis
Osteoporosis is a health condition that weakens bones, making them fragile and more likely to break especially hip and vertebral fractures 161. Osteoporosis develops slowly over several years and is often only diagnosed when a fall or sudden impact causes a bone to break (fracture). Osteoporosis is a multifactorial disease, with age being the most common risk. Other risk factors include environmental (i.e., alcohol consumption, smoking, vitamin D and calcium deficiencies, low physical activity), metabolic (estrogen deficiency), and genetic factors (i.e., cathepsin K, sclerostin, chloride channel 7, high-risk ethnic groups) 162. Osteoporosis affects around 200 million people worldwide (30% of women, 12% of men) 162.
Redox imbalance is also involved in the pathogenesis of bone loss. Reactive oxygen species (ROS) also called oxygen radical or free radicals, are highly reactive chemicals formed from oxygen (O₂) and that easily reacts with other molecules in a cell. Elevated formation of the different ROS leads to molecular damage, denoted as ‘oxidative distress’, may cause damage to DNA, RNA, and proteins, and may cause cell death. Overproduction of reactive oxygen species ROS increases osteoclast activity and inhibits bone mineralization 163. Flavones from tea have demonstrated to act as antioxidants. Particularly, epicatechin isolated from Huangshan Maofeng tea (green tea produced in Anhui province of China) has shown to protect against oxidative stress in a hydrogen peroxide-induced model on C2C12 mouse myoblast cells 164.
Furthermore, in vivo (animal studies) evidence has demonstrated that tea exerts a protective effect on osteoporosis as evidenced in relevant biomarkers. Hence, green tea extracts (dose of 370 mg/kg for 13 weeks) increase cortical and trabecular bone mass in ovariectomized female Wistar rats 165. Furthermore, green tea polyphenols supplementation (4 months) improved bone properties (alleviate bone loss and favored bone microstructure restructuring) in obese rats fed with a high fat diet and a high fat diet followed by a caloric restricted diet 166.
Patients with diabetes mellitus have low bone mass which increase fracture risk. Therefore, de Amorim et al. 28 conducted a double-blind, randomized, placebo-controlled clinical trial to evaluate the effect of green tea extract on bone mass of diabetic patients. This clinical trial revealed that those subjects with diabetes who received 1120 mg of green tea extract containing 560 mg of polyphenols/day for 20 weeks increased their bone mineral content.
Many studies reported the antibacterial activity of green tea. Green tea is effective against Staphylococcus epidermidis, Staphylococcus aureus, and Vibrio cholerae O1, owing to the bactericidal catechins that primarily cause defection in the bacterial membranes 167. Green tea is also effective against various bacteria that cause tooth decay, such as Escherichia coli, Streptococcus salivarius, and Streptococcus mutans 168. EGCG and gallocatechin gallate (GCG) markedly inhibit the secretion of extracellular Vero toxins from enterohemorrhagic Escherichia coli cells into the culture supernatant fluid 169. Raw extract of green tea, especially gallocatechin gallate (GCG), is able to suppress 1-deoxy-d-xylulose 5-phosphate reductoisomerase activity, which is an antimicrobial target 170. Furthermore, it can also reduce the lethality of ricin toxin 171, but it has a poor activity against Babesia divergens that infect cattle 172.
EGCG can inhibit the activity of Salmonella typhimurium type III, and thus reduce the bacterial invasion into host cells 173. Green tea extract is bactericidal against Gram positive bacteria and bacteriostatic against Gram negative ones, with less antifungal activity against Aspergillus niger and Penicillium chrysogenum 174.
In addition, tea polyphenols have the ability to inhibit the development and growth of bacterial spores, as in case of Bacillus stearothermophilus and Clostridium thermoaceticum, due to their ability to decrease the heat resistance of these bacterial spores when added at high temperature 175. However, chlorogenic acid induces the apoptotic markers through excessive potassium efflux and an apoptotic volume reduction, which induces cytosolic calcium uptake and cell cycle arrest in Candida albicans, in addition to its ability to induce caspase activation and DNA fragmentation 176.
Tea exhibits antiviral activity against human viruses and serves as a diet-derived immune-modulatory chemopreventive agent, as many of its contained flavonoids stimulate NK cell activity, so it may be used in the treatment and prevention of viral diseases 177. Recently, it was found that EGCG is capable of inhibiting the Brazilian strain of Zika virus entry 178. Additionally, topical application of EGCG can be used to prevent the sexual transmission of HIV, as it disaggregates existing amyloid fibrils termed semen-derived enhancers of viral infection fibers and inhibits the formation of new ones 179. In 2006, the United States Food and Drug Administration (FDA) approved the marketing of the sinecatechins ointment as a prescribed Botanical Drug in USA 180, which has been marketed in EU countries and USA under the trademark of Veregen® 181. FDA approved the topical treatment of external genital warts and perianal warts with sinecatechins 15% in immuocompetent patients from the age of 18 years for three times daily until complete the clearance of warts or for up to 16 weeks 182.
Green tea neuroprotective activity against Alzheimer’s disease
Green tea contains several compounds that may have beneficial properties, including caffeine, L-theanine, and green tea catechins (e.g., EGCG) 183. Green tea extract has a protective effect on the ischemia/reperfusion-induced brain injury and behavior deficit. It also reduces the number of ischemia/reperfusion-induced apoptotic neuronal cells 184. EGCG could theoretically promote brain health, but no studies have evaluated whether it can protect from cognitive decline or dementia. Green tea polyphenols, epigallocatechin-3-gallate (EGCG), epigallocatechin, epicatechin-3-gallate and epicatechin are able to protect synaptosomes from induced lipid peroxidation damage 185. EGCG alone has a protective effect against stress-induced neural injuries 186. EGCG was shown to be easily absorbed from the digestive tract and penetrate the brain, reaching levels similar to those found in lung, liver, kidney, and others 187. It has a neuroprotective effect against neuronal damage following transient global ischemia in the gerbils acting by different mechanisms as angiogenesis in the early stage of ischemic stroke promoting 188. Regarding neurotoxicity, L-theanine (a unique amino acid of green tea) has a protective effect against cadmium-induced neurotoxicity by reducing brain cadmium levels and oxidative damage, which lead to neurodegenerative diseases 189.
In addition, green tea polyphenols can be considered therapeutic agents to alter brain aging processes by serving as neuroprotective agents in major neurodegenerative disorders, such as Parkinson’s disease and Alzheimer’s disease 190. In addition, green tea catechin intake may be useful in the improvement of the morphologic and functional changes that occur naturally in the accelerated senile brains 191. EGCG and epigallocatechin were found to be inhibitors of dopa decarboxylase enzyme in a concentration- and time-dependent manner 116. Green tea containing high levels of EGCG prevents the loss of tyrosine hydroxylase-positive cells in the substantia nigra. Both tea and EGCG, when used alone or with Parkinson’s disease’s inducers, can decrease the neuronal nitric oxide synthase (nNOS) expressions in the substantia nigra, which provides a neuroprotective effect 192.
Several observational studies and clinical trials suggest that greater green tea consumption is associated with lower dementia risk, but no clinical trials have tested whether green tea can prevent age-related cognitive decline or dementia. No studies have reported whether green tea can improve cognition or slow decline in people with dementia. In a clinical trial, markers of oxidative stress were decreased in Alzheimer’s patients who consumed a beverage that included green tea extracts for eight months 193. However, it is unknown whether this beverage helps patients. A different antioxidant therapy (not containing green tea extract) was reported to lower oxidative stress in Alzheimer’s patients but accelerated cognitive decline 194.
Greater green tea consumption was associated with lower risk of dementia in two studies conducted in Japan, with the larger study reporting 27% lower risk in people who drank at least 5 cups a day 195, 196. Tea drinking was also associated with higher verbal fluency in elderly Chinese people (i.e., 80–115 years old) 197.
Two double-blind randomized controlled trials have evaluated the effects of green tea extract on cognitive functions. One trial in 91 patients with mild cognitive impairment reported that the combination of green tea extract and L-theanine for 16 weeks resulted in significant improvements in memory and attention, particularly in patients who had relatively severe baseline impairment 198. The second trial examined the acute effects of a drink containing 27.5 g of green tea extract and reported that the drink increased brain connectivity associated with working memory and the degree of connectivity correlated with the magnitude of improvement in working memory 199.
Preclinical studies have found a wide range of actions of EGCG, including chelating metals, reducing inflammation, scavenging free radicals, improving mitochondrial function, and preventing death of brain cells 200. EGCG may also inhibit enzymes that break down the neurotransmitter acetylcholine 201, which is important for memory retrieval. Other preclinical studies found that EGCG treatment improved function or reduced damage in the brain 202, 203, but these effects have not been confirmed in human trials.
Two small trials suggest that EGCG treatment may very modestly improve memory functions, inhibitory control, and adaptive behavior in people with Down syndrome, though this protective effect was evident in only 3 out of 24 cognitive tests 204. In healthy adults, a single dose of EGCG has had little influence on cognition. One double-blind randomized controlled trial reported that a single treatment did not affect cognitive performance or mood 205. A second trial reported increased calmness and reduced stress 206. EGCG also increased brain waves, which have been associated with relaxation, focused attention, and quiet wakefulness 207. Long-term studies in healthy people are needed to evaluate the effects of EGCG on cognitive health.
Is green tea safe?
Tea as a food item is generally recognized as safe by the U.S. Food and Drug Administration. Green tea is believed to be safe when consumed as a beverage in amounts up to 8 cups per day 208. Multiple meta-analyses have reported that green tea consumption is safe at moderate and regular amounts (3 to 5 cups per day, up to 1200 ml/day) and side effects are mild 124, 209, 85. Three drugs are known to interact with green tea: warfarin (also known as Coumadin™ and Jantoven™), anisindione (or Miradon™), and dicumarol. Green tea consumption may reduce the levels of folic acid in the body and interfere with iron absorption. Because green tea contains caffeine, pregnant women and people with cardiovascular problems or other health risks should consult their physician or healthcare provider about consuming green tea. Caffeine in green tea can also interact with some medications.
Green tea contains caffeine. Keep in mind that only the amount of added caffeine must be stated on product labels and not the caffeine that naturally occurs in green tea. The amount of caffeine present in tea varies by the type of tea; the caffeine content is higher in black teas, ranging from 64 to 112 mg per 8 fl oz (237 ml) serving, followed by oolong tea, which contains about 29 to 53 mg per 8 fl oz (237 ml) serving 210. Green and white teas contain slightly less caffeine, ranging from 24 to 39 mg per 8 fl oz (237 ml) serving and 32 to 37 mg per 8 fl oz (237 ml) serving, respectively 211. Decaffeinated teas contain less than 12 mg caffeine per 8 fl oz (237 ml) serving 211. As with other caffeinated beverages, such as coffee and colas, the caffeine contained in many tea products could potentially cause adverse effects, including tachycardia, palpitations, insomnia, restlessness, nervousness, tremors, headache, abdominal pain, nausea, vomiting, diarrhea, and diuresis (excessive production of urine) 212. However, there is little evidence of health risks for adults consuming moderate amounts of caffeine (about 300 to 400 mg per day). A review by Health Canada concluded that moderate caffeine intakes of up to 400 mg per day (equivalent to 6 mg per kilogram [kg] body weight) were not associated with adverse effects in healthy adults 213. Drinking green tea may be safe during pregnancy and while breastfeeding when consumed in amounts up to 6 cups per day (no more than about 300 mg of caffeine). Drinking more than this amount during pregnancy may be unsafe and may increase the risk of negative effects. Green tea may also increase the risk of birth defects associated with folic acid deficiency 208. Caffeine passes into breast milk and can affect a breastfeeding infant. Research on the effects of caffeine in children is limited 212. In general, caffeine doses of less than 3.0 mg per kg body weight have not resulted in adverse effects in children 212. Higher doses have resulted in some behavioral effects, such as increased nervousness or anxiety and sleep disturbances 213.
Aluminum, a neurotoxic element, is found in varying quantities in tea plants 86. Studies have found concentrations of aluminum (which is naturally taken up from soil) in infusions of green and black teas that range from 14 to 27 micrograms per liter (μg/L) to 431 to 2239 μg/L 210. The variations in aluminum content may be due to different soil conditions, different harvesting periods, and water quality 210. Aluminum can accumulate in the body and cause osteomalacia and neurodegenerative disorders, especially in individuals with renal failure 210. However, it is not clear how much of the aluminum in tea is bioavailable, and there is no evidence of any aluminum toxicity associated with drinking tea 210.
Black and green tea may inhibit iron bioavailability from the diet 210. This effect may be important for individuals who suffer from iron-deficiency anemia 210. The authors of a systematic review of 35 studies on the effect of black tea drinking on iron status in the UK concluded that, although tea drinking limited the absorption of non-heme iron from the diet, there was insufficient evidence to conclude that this would have an effect on blood measures (i.e., hemoglobin and ferritin concentrations) of overall iron status in adults 214. However, among preschool children, statistically significant relationships were observed between tea drinking and poor iron status 214. The interaction between tea and iron can be mitigated by consuming, at the same meal, foods that enhance iron absorption, such as those that contain vitamin C (e.g., lemons), and animal foods that are sources of heme iron (e.g., red meat) 210. Consuming tea between meals appears to have a minimal effect on iron absorption 210.
Epigallocatechin-3-gallate (EGCG) supplements are considered safe for most people when taken at commonly used doses (300–400 mg/day) 215, 216, but high doses (800–1600 mg of EGCG per day) may negatively affect liver function 217. Most safety data on long-term EGCG intake come from large meta-analyses of tea consumption, which have reported that side effects are mild [15][16] and can include nausea and upset stomach 216, 218.
Safety studies have looked at the consumption of up to 1200 mg of epigallocatechin-3-gallate (EGCG) in supplement form in healthy adults over 1- to 4-week time periods 219, 220. The adverse effects reported in these studies included excess intestinal gas, nausea, heartburn, stomach ache, abdominal pain, dizziness, headache, and muscle pain 219, 220. In a Japanese study, children aged 6 to 16 years consumed a green tea beverage containing 576 mg catechins (experimental group) or 75 mg catechins (control group) for 24 weeks with no adverse effects 221. The safety of higher doses of catechins in children is not known.
Green tea is an ingredient in many over-the-counter weight loss products, some of which have been identified as the likely cause of rare cases of liver injury. Although uncommon, liver problems have been reported in a number of people who took concentrated green tea extracts in pill form 222. More than 100 instances of clinically apparent liver injury attributed to green tea extract have been reported in the literature 222. Liver injury typically arises within 1 to 6 months of starting the product but longer and shorter latencies (particularly with reexposure) have been reported. The majority of cases present with an acute hepatitis-like syndrome and a markedly hepatocellular pattern of serum enzyme elevations. Most patients recover rapidly upon stopping the green tea extract or the herbal and dietary supplements, although fatal instances of acute liver failure have been described 222. Biopsy findings show necrosis, inflammation, and eosinophils in a pattern resembling acute hepatitis. Immunoallergic and autoimmune features are usually absent or minimal. A small number of similar cases have also been described after drinking green tea “infusions” rather than taking oral preparations of extracts of green tea. Experts suggest that green tea extracts should be taken with food, people with liver problems or liver disease should not take green tea extracts, and users should discontinue use and consult a health care provider if they develop symptoms of liver trouble, such as abdominal pain, dark urine, or jaundice (yellowing of the skin or eyes).
Based on the available data on the potential adverse effects of green tea catechins on the liver, the European Commission to the European Food Safety Authority (EFSA) and the Scientific Panel on Food Additives and Nutrient Sources added to Food 223 concluded that there is evidence from interventional clinical trials that intake of green tea extracts at doses equal or above 800 mg EGCG/day taken as a food supplement for 4 months or longer has been shown to induce a statistically significant increase of alanine aminotransferase (ALT) and aspartate aminotransferase (AST) (commonly found in liver damage or liver disease) in treated subjects (usually less than 10%) compared to control 223.
Catechins in green tea extracts, either consumed as a beverage or in liquid or dry form as dietary supplements, may be more concentrated, may differ in composition and pattern of consumption compared to catechins from traditional green tea infusions and cannot be regarded as safe according to the presumption of safety approach, as exposure to green tea extracts at and above 800 mg EGCG/day in intervention studies causes elevated serum transaminases which is indicative of liver injury.
The European Commission to the European Food Safety Authority Panel concluded that it was not possible to identify an EGCG dose from green tea extracts that could be considered safe. From the clinical studies reviewed there is no evidence of hepatotoxicity (liver damage) below 800 mg EGCG/day up to 12 months 223. However, hepatotoxicity (liver damage) was reported for one specific product containing 80% ethanolic extract at a daily dose corresponding to 375 mg EGCG 223.
Green tea at high doses has also been shown to reduce blood levels and therefore the effectiveness of the drug nadolol, a beta-blocker used for high blood pressure and heart problems. It may also interact with other medicines.
- Matcha. https://en.wikipedia.org/wiki/Matcha[↩]
- L-theanine partially counteracts caffeine-induced sleep disturbances in rats. Jang HS, Jung JY, Jang IS, Jang KH, Kim SH, Ha JH, Suk K, Lee MG. Pharmacol Biochem Behav. 2012 Apr; 101(2):217-21. https://www.ncbi.nlm.nih.gov/pubmed/22285321/[↩]
- L-Theanine reduces psychological and physiological stress responses. Kimura K, Ozeki M, Juneja LR, Ohira H. Biol Psychol. 2007 Jan; 74(1):39-45. https://www.ncbi.nlm.nih.gov/pubmed/16930802/[↩]
- Anti-stress effects of drinking green tea with lowered caffeine and enriched theanine, epigallocatechin and arginine on psychosocial stress induced adrenal hypertrophy in mice. Unno K, Hara A, Nakagawa A, Iguchi K, Ohshio M, Morita A, Nakamura Y. Phytomedicine. 2016 Nov 15; 23(12):1365-1374. https://www.ncbi.nlm.nih.gov/pubmed/27765356/[↩][↩][↩]
- Epigallocatechin gallate and mitochondria-A story of life and death. Oliveira MR, Nabavi SF, Daglia M, Rastrelli L, Nabavi SM. Pharmacol Res. 2016 Feb; 104():70-85. https://www.ncbi.nlm.nih.gov/pubmed/26731017/[↩]
- Tea catechins and polyphenols: health effects, metabolism, and antioxidant functions. Higdon JV, Frei B. Crit Rev Food Sci Nutr. 2003; 43(1):89-143. https://www.ncbi.nlm.nih.gov/pubmed/12587987/[↩][↩]
- Chemoprevention of human prostate cancer by oral administration of green tea catechins in volunteers with high-grade prostate intraepithelial neoplasia: a preliminary report from a one-year proof-of-principle study. Bettuzzi S, Brausi M, Rizzi F, Castagnetti G, Peracchia G, Corti A. Cancer Res. 2006 Jan 15; 66(2):1234-40. http://cancerres.aacrjournals.org/content/66/2/1234.long[↩]
- Coffee and green tea as a large source of antioxidant polyphenols in the Japanese population. Fukushima Y, Ohie T, Yonekawa Y, Yonemoto K, Aizawa H, Mori Y, Watanabe M, Takeuchi M, Hasegawa M, Taguchi C, Kondo K. J Agric Food Chem. 2009 Feb 25; 57(4):1253-9. https://www.ncbi.nlm.nih.gov/pubmed/19187022/[↩]
- Shishikura Y, Khokhar S. Factors affecting the levels of catechins and caffeine in tea beverage: estimated daily intakes and antioxidant activity. J Sci Food Agric. 2005;85:2125–2133.[↩]
- Engelhardt UH, Lakenbrink C, Pokorny O. In: Nutraceutical Beverages: Chemistry, Nutrition, and Health Effects. Shahidi F, Weerasinghe DK, editors. Amer Chemical Soc; Washington: 2004. pp. 254–264.[↩]
- Factors affecting the levels of tea polyphenols and caffeine in tea leaves. Lin YS, Tsai YJ, Tsay JS, Lin JK. J Agric Food Chem. 2003 Mar 26; 51(7):1864-73.[↩]
- Alves Ferreira M., Oliveira Gomes A.P., Guimarães de Moraes A.P., Ferreira Stringhini M.L., Mota J.F., Siqueira Guedes Coelho A., Borges Botelho P. Green tea extract outperforms metformin in lipid profile and glycaemic control in overweight women: A double-blind, placebo-controlled, randomized trial. Clin Nutr. 2017;22:1–6. doi: 10.1016/j.clnesp.2017.08.008[↩][↩]
- Lasaite L., Spadiene A., Savickiene N., Skesters A., Silova A. The effect of Ginkgo biloba and Camellia sinensis extracts on psychological state and glycemic control in patients with type 2 diabetes mellitus. Nat. Prod. Commun. 2014;9:1345–1350. doi: 10.1177/1934578X1400900931[↩]
- Mahmoud F., Al-Ozairi E., Haines D., Novotny L., Dashti A., Ibrahim B., Abdel-Hamid M. Effect of Diabetea tea™ consumption on inflammatory cytokines and metabolic biomarkers in type 2 diabetes patients. J. Ethnopharmacol. 2016;194:1069–1077. doi: 10.1016/j.jep.2016.10.073[↩][↩]
- Spadiene A., Savickiene N., Ivanauskas L., Jakstas V., Skesters A., Silova A., Rodovicius H. Antioxidant effects of Camellia sinensis L. extract in patients with type 2 diabetes. J. Food Drug Anal. 2014;22:505–511. doi: 10.1016/j.jfda.2014.04.001[↩]
- Vaz S.R., de Amorim L.M.N., de Nascimento P.V.F., Veloso V.S.P., Nogueira M.S., Castro I.A., Botelho P.B. Effects of green tea extract on oxidative stress and renal function in diabetic individuals: A randomized, double-blinded, controlled trial. J. Funct. Foods. 2018;46:195–201. doi: 10.1016/j.jff.2018.04.059[↩][↩]
- Imbe H., Sano H., Miyawaki M., Fujisawa R., Miyasato M., Nakatsuji F., Tachibana H. “Benifuuki” green tea, containing O-methylated EGCG, reduces serum low-density lipoprotein cholesterol and lectin-like oxidized low-density lipoprotein receptor-1 ligands containing apolipoprotein B: A double-blind, placebo-controlled randomized trial. J. Funct. Foods. 2016;25:25–37. doi: 10.1016/j.jff.2016.05.004[↩][↩]
- Orem A., Alasalvar C., Kural B.V., Yaman S., Orem C., Karadag A., Zawistowski J. Cardio-protective effects of phytosterol-enriched functional black tea in mild hypercholesterolemia subjects. J. Funct. Foods. 2017;31:311–319. doi: 10.1016/j.jff.2017.01.048[↩][↩]
- Troup R, Hayes JH, Raatz SK, Thyagarajan B, Khaliq W, Jacobs DR Jr, Key NS, Morawski BM, Kaiser D, Bank AJ, Gross M. Effect of black tea intake on blood cholesterol concentrations in individuals with mild hypercholesterolemia: a diet-controlled randomized trial. J Acad Nutr Diet. 2015 Feb;115(2):264-271.e2. doi: 10.1016/j.jand.2014.07.021[↩][↩]
- Alkerwi A., Sauvageot N., Crichton G.E., Elias M.F. Tea, but not coffee consumption, is associated with components of arterial pressure. The observation of cardiovascular risk factors study in Luxembourg. Nutr. Res. 2015;35:557–565. doi: 10.1016/j.nutres.2015.05.004[↩][↩]
- Yang X, Yin L, Li T, Chen Z. Green tea extracts reduce adipogenesis by decreasing expression of transcription factors C/EBPα and PPARγ. Int J Clin Exp Med. 2014 Dec 15;7(12):4906-14. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4307434[↩]
- Chen I.J., Liu C.Y., Chiu J.P., Hsu C.H. Therapeutic effect of high-dose green tea extract on weight reduction: A randomized, double-blind, placebo-controlled clinical trial. Clin. Nutr. 2016;35:592–599. doi: 10.1016/j.clnu.2015.05.003[↩]
- Dostal AM, Arikawa A, Espejo L, Kurzer MS. Long-Term Supplementation of Green Tea Extract Does Not Modify Adiposity or Bone Mineral Density in a Randomized Trial of Overweight and Obese Postmenopausal Women. J Nutr. 2016 Feb;146(2):256-64. doi: 10.3945/jn.115.219238[↩]
- Huang LH, Liu CY, Wang LY, Huang CJ, Hsu CH. Effects of green tea extract on overweight and obese women with high levels of low density-lipoprotein-cholesterol (LDL-C): a randomised, double-blind, and cross-over placebo-controlled clinical trial. BMC Complement Altern Med. 2018 Nov 6;18(1):294. doi: 10.1186/s12906-018-2355-x[↩]
- Janssens P.L., Hursel R., Westerterp-Plantenga M.S. Long-term green tea extract supplementation does not affect fat absorption, resting energy expenditure, and body composition in adults. Nutr. J. 2015;145:864–870. doi: 10.3945/jn.114.207829[↩]
- Mielgo-Ayuso J., Barrenechea L., Alcorta P., Larrarte E., Margareto J., Labayen I. Effects of dietary supplementation with epigallocatechin-3-gallate on weight loss, energy homeostasis, cardiometabolic risk factors and liver function in obese women: Randomised, double-blind, placebo-controlled clinical trial. Br. J. Nutr. 2014;111:1263–1271. doi: 10.1017/S0007114513003784[↩]
- Nicoletti CF, Delfino HBP, Pinhel M, Noronha NY, Pinhanelli VC, Quinhoneiro DCG, de Oliveira BAP, Marchini JS, Nonino CB. Impact of green tea epigallocatechin-3-gallate on HIF1-α and mTORC2 expression in obese women: anti-cancer and anti-obesity effects? Nutr Hosp. 2019 Apr 10;36(2):315-320. English. doi: 10.20960/nh.2216[↩]
- De Amorim L.M.N., Vaz S.R., Cesário G., Coelho A.S.G., Botelho P.B. Effect of green tea extract on bone mass and body composition in individuals with diabetes. J. Funct. Foods. 2018;40:589–594. doi: 10.1016/j.jff.2017.11.039[↩][↩]
- FORESTER SC, LAMBERT JD. Antioxidant effects of green tea. Molecular nutrition & food research. 2011;55(6):844-854. doi:10.1002/mnfr.201000641. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3679539/[↩][↩]
- Baptista JAB, Tavares JFD, Carvalho RCB. Comparison of catechins and aromas among different green teas using HPLC/SPME-GC. Food Res Int. 1998;31:729–736.[↩]
- Lin SD, Liang CH, Liu EH, Mau JL. ANTIOXIDANT PROPERTIES OF WATER EXTRACTS FROM PARCHING GREEN TEA. J Food Biochem. 2010;34:477–500.[↩]
- Generation of hydrogen peroxide by “antioxidant” beverages and the effect of milk addition. Is cocoa the best beverage? Long LH, Lan AN, Hsuan FT, Halliwell B. Free Radic Res. 1999 Jul; 31(1):67-71. https://www.ncbi.nlm.nih.gov/pubmed/10489121/[↩]
- Prooxidant property of green tea polyphenols epicatechin and epigallocatechin-3-gallate: implications for anticancer properties. Azam S, Hadi N, Khan NU, Hadi SM. Toxicol In Vitro. 2004 Oct; 18(5):555-61. https://www.ncbi.nlm.nih.gov/pubmed/15251172/[↩]
- Dietary flavonoid intake and lung cancer–a population-based case-control study. Cui Y, Morgenstern H, Greenland S, Tashkin DP, Mao JT, Cai L, Cozen W, Mack TM, Lu QY, Zhang ZF. Cancer. 2008 May 15; 112(10):2241-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5546301/[↩]
- Green tea intake, ACE gene polymorphism and breast cancer risk among Chinese women in Singapore. Yuan JM, Koh WP, Sun CL, Lee HP, Yu MC. Carcinogenesis. 2005 Aug; 26(8):1389-94. https://www.ncbi.nlm.nih.gov/pubmed/15802301/[↩]
- Green-tea consumption and risk of stomach cancer: a population-based case-control study in Shanghai, China. Yu GP, Hsieh CC, Wang LY, Yu SZ, Li XL, Jin TH. Cancer Causes Control. 1995 Nov; 6(6):532-8. https://www.ncbi.nlm.nih.gov/pubmed/8580302/[↩]
- Tea consumption and risk of ovarian cancer. Nagle CM, Olsen CM, Bain CJ, Whiteman DC, Green AC, Webb PM. Cancer Causes Control. 2010 Sep; 21(9):1485-91. https://www.ncbi.nlm.nih.gov/pubmed/20490647/[↩]
- Inhibition of proliferation and induction of apoptosis by EGCG in human osteogenic sarcoma (HOS) cells. Ji SJ, Han DH, Kim JH. Arch Pharm Res. 2006 May; 29(5):363-8.[↩]
- Induction of apoptosis by epigallocatechin-3-gallate in human lymphoblastoid B cells. Noda C, He J, Takano T, Tanaka C, Kondo T, Tohyama K, Yamamura H, Tohyama Y. Biochem Biophys Res Commun. 2007 Nov 3; 362(4):951-7.[↩]
- Catechin, a green tea component, rapidly induces apoptosis of myeloid leukemic cells via modulation of reactive oxygen species production in vitro and inhibits tumor growth in vivo. Nakazato T, Ito K, Miyakawa Y, Kinjo K, Yamada T, Hozumi N, Ikeda Y, Kizaki M. Haematologica. 2005 Mar; 90(3):317-25.[↩][↩]
- Anti-proliferative and proapoptotic effects of (-)-epigallocatechin-3-gallate on human melanoma: possible implications for the chemoprevention of melanoma. Nihal M, Ahmad N, Mukhtar H, Wood GS. Int J Cancer. 2005 Apr 20; 114(4):513-21.[↩][↩]
- Green tea polyphenols induce apoptosis in vitro in peripheral blood T lymphocytes of adult T-cell leukemia patients. Li HC, Yashiki S, Sonoda J, Lou H, Ghosh SK, Byrnes JJ, Lema C, Fujiyoshi T, Karasuyama M, Sonoda S. Jpn J Cancer Res. 2000 Jan; 91(1):34-40.[↩]
- EGCG induces apoptosis in human laryngeal epidermoid carcinoma Hep2 cells via mitochondria with the release of apoptosis-inducing factor and endonuclease G. Lee JH, Jeong YJ, Lee SW, Kim D, Oh SJ, Lim HS, Oh HK, Kim SH, Kim WJ, Jung JY. Cancer Lett. 2010 Apr 1; 290(1):68-75.[↩][↩]
- Epigallocatechin (EGC) of green tea induces apoptosis of human breast cancer cells but not of their normal counterparts. Vergote D, Cren-Olivé C, Chopin V, Toillon RA, Rolando C, Hondermarck H, Le Bourhis X. Breast Cancer Res Treat. 2002 Dec; 76(3):195-201.[↩]
- Green tea extracts decrease carcinogen-induced mammary tumor burden in rats and rate of breast cancer cell proliferation in culture. Kavanagh KT, Hafer LJ, Kim DW, Mann KK, Sherr DH, Rogers AE, Sonenshein GE. J Cell Biochem. 2001; 82(3):387-98.[↩][↩]
- Zhou B, Pan J, Dai F, Zhao CY, Zhang LP, Wei QY, Yang L, Zheng RL, Liu ZL. Redifferentiation of human hepatoma cells induced by green tea polyphenols. Res Chem Intermed. 2004;30:627–636.[↩]
- Combined treatment with green tea catechins and sodium nitrite selectively promotes rat forestomach carcinogenesis after initiation with N-methyl-N’- nitro-N-nitrosoguanidine. Kuroiwa Y, Ishii Y, Umemura T, Kanki K, Mitsumori K, Nishikawa A, Nakazawa H, Hirose M. Cancer Sci. 2007 Jul; 98(7):949-57.[↩]
- Epigallocatechin-3-gallate ameliorates rats colitis induced by acetic acid. Ran ZH, Chen C, Xiao SD. Biomed Pharmacother. 2008 Mar; 62(3):189-96.[↩]
- Green tea and black tea consumption and prostate cancer risk: an exploratory meta-analysis of observational studies. Zheng J, Yang B, Huang T, Yu Y, Yang J, Li D. Nutr Cancer. 2011; 63(5):663-72. https://www.ncbi.nlm.nih.gov/pubmed/21667398/[↩]
- Tea consumption and prostate cancer: an updated meta-analysis. Lin YW, Hu ZH, Wang X, Mao QQ, Qin J, Zheng XY, Xie LP. World J Surg Oncol. 2014 Feb 14; 12():38. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3925323/[↩]
- The association of tea consumption and the risk and progression of prostate cancer: a meta-analysis. Fei X, Shen Y, Li X, Guo H. Int J Clin Exp Med. 2014; 7(11):3881-91. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4276154/[↩]
- Green tea and anticancer perspectives: updates from last decade. Butt MS, Ahmad RS, Sultan MT, Qayyum MM, Naz A. Crit Rev Food Sci Nutr. 2015; 55(6):792-805. https://www.ncbi.nlm.nih.gov/pubmed/24915354/[↩]
- Komorita Y, Iwase M, Fujii H, et al. Additive effects of green tea and coffee on all-cause mortality in patients with type 2 diabetes mellitus: the Fukuoka Diabetes Registry. BMJ Open Diabetes Research and Care 2020;8:e001252. doi: 10.1136/bmjdrc-2020-001252[↩][↩][↩]
- Effects of catechin enriched green tea on body composition. Wang H, Wen Y, Du Y, Yan X, Guo H, Rycroft JA, Boon N, Kovacs EM, Mela DJ. Obesity (Silver Spring). 2010 Apr; 18(4):773-9. https://www.ncbi.nlm.nih.gov/pubmed/19680234/[↩]
- Green tea catechin consumption enhances exercise-induced abdominal fat loss in overweight and obese adults. Maki KC, Reeves MS, Farmer M, Yasunaga K, Matsuo N, Katsuragi Y, Komikado M, Tokimitsu I, Wilder D, Jones F, Blumberg JB, Cartwright Y. J Nutr. 2009 Feb; 139(2):264-70. http://jn.nutrition.org/content/139/2/264.long[↩]
- The effects of catechin rich teas and caffeine on energy expenditure and fat oxidation: a meta-analysis. Hursel R, Viechtbauer W, Dulloo AG, Tremblay A, Tappy L, Rumpler W, Westerterp-Plantenga MS. Obes Rev. 2011 Jul; 12(7):e573-81. https://www.ncbi.nlm.nih.gov/pubmed/21366839/[↩]
- Green tea extract ingestion, fat oxidation, and glucose tolerance in healthy humans. Venables MC, Hulston CJ, Cox HR, Jeukendrup AE. Am J Clin Nutr. 2008 Mar; 87(3):778-84. http://ajcn.nutrition.org/content/87/3/778.long[↩]
- A green tea extract high in catechins reduces body fat and cardiovascular risks in humans. Nagao T, Hase T, Tokimitsu I. Obesity (Silver Spring). 2007 Jun; 15(6):1473-83. https://www.ncbi.nlm.nih.gov/pubmed/17557985/[↩]
- Effects of Chinese green tea on weight, and hormonal and biochemical profiles in obese patients with polycystic ovary syndrome–a randomized placebo-controlled trial. Chan CC, Koo MW, Ng EH, Tang OS, Yeung WS, Ho PC. J Soc Gynecol Investig. 2006 Jan; 13(1):63-8. https://www.ncbi.nlm.nih.gov/pubmed/16378915/[↩]
- Effects of encapsulated green tea and Guarana extracts containing a mixture of epigallocatechin-3-gallate and caffeine on 24 h energy expenditure and fat oxidation in men. Bérubé-Parent S, Pelletier C, Doré J, Tremblay A. Br J Nutr. 2005 Sep; 94(3):432-6. https://www.ncbi.nlm.nih.gov/pubmed/16176615/[↩]
- Effects of green tea on weight maintenance after body-weight loss. Kovacs EM, Lejeune MP, Nijs I, Westerterp-Plantenga MS. Br J Nutr. 2004 Mar; 91(3):431-7. https://www.ncbi.nlm.nih.gov/pubmed/15005829/[↩]
- Green tea minimally affects biomarkers of inflammation in obese subjects with metabolic syndrome. Basu A, Du M, Sanchez K, Leyva MJ, Betts NM, Blevins S, Wu M, Aston CE, Lyons TJ. Nutrition. 2011 Feb; 27(2):206-13. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2952043/[↩]
- Relationship among habitual tea consumption, percent body fat, and body fat distribution. Wu CH, Lu FH, Chang CS, Chang TC, Wang RH, Chang CJ. Obes Res. 2003 Sep; 11(9):1088-95. https://www.ncbi.nlm.nih.gov/pubmed/12972679/[↩]
- Tea consumption is inversely associated with weight status and other markers for metabolic syndrome in US adults. Vernarelli JA, Lambert JD. Eur J Nutr. 2013 Apr; 52(3):1039-48. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3515715/[↩]
- Smoking, habitual tea drinking and metabolic syndrome in elderly men living in rural community: the Tianliao old people (TOP) study 02. Chang CS, Chang YF, Liu PY, Chen CY, Tsai YS, Wu CH. PLoS One. 2012; 7(6):e38874. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3375307[↩]
- EGCG, a green tea polyphenol, improves endothelial function and insulin sensitivity, reduces blood pressure, and protects against myocardial I/R injury in SHR. Potenza MA, Marasciulo FL, Tarquinio M, Tiravanti E, Colantuono G, Federici A, Kim JA, Quon MJ, Montagnani M. Am J Physiol Endocrinol Metab. 2007 May; 292(5):E1378-87. https://www.ncbi.nlm.nih.gov/pubmed/17227956/[↩]
- Antiobesity effects of Chinese black tea (Pu-erh tea) extract and gallic acid. Oi Y, Hou IC, Fujita H, Yazawa K. Phytother Res. 2012 Apr; 26(4):475-81. https://www.ncbi.nlm.nih.gov/pubmed/22508359/[↩]
- Coffee, green tea, black tea and oolong tea consumption and risk of mortality from cardiovascular disease in Japanese men and women. Mineharu Y, Koizumi A, Wada Y, Iso H, Watanabe Y, Date C, Yamamoto A, Kikuchi S, Inaba Y, Toyoshima H, Kondo T, Tamakoshi A, JACC study Group. J Epidemiol Community Health. 2011 Mar; 65(3):230-40. https://www.ncbi.nlm.nih.gov/pubmed/19996359/[↩]
- Tea and cardiovascular disease. Deka A, Vita JA. Pharmacol Res. 2011 Aug; 64(2):136-45. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3123419/[↩]
- Tea and coffee consumption and cardiovascular morbidity and mortality. de Koning Gans JM, Uiterwaal CS, van der Schouw YT, Boer JM, Grobbee DE, Verschuren WM, Beulens JW. Arterioscler Thromb Vasc Biol. 2010 Aug; 30(8):1665-71. http://atvb.ahajournals.org/content/30/8/1665.long[↩]
- Obesity and the risk of myocardial infarction in 27,000 participants from 52 countries: a case-control study. Yusuf S, Hawken S, Ounpuu S, Bautista L, Franzosi MG, Commerford P, Lang CC, Rumboldt Z, Onen CL, Lisheng L, Tanomsup S, Wangai P Jr, Razak F, Sharma AM, Anand SS, INTERHEART Study Investigators. Lancet. 2005 Nov 5; 366(9497):1640-9. https://www.ncbi.nlm.nih.gov/pubmed/16271645/[↩]
- Tea consumption and cardiovascular disease: effects on endothelial function. Vita JA. J Nutr. 2003 Oct; 133(10):3293S-3297S. http://jn.nutrition.org/content/133/10/3293S.long[↩]
- Green tea consumption and mortality due to cardiovascular disease, cancer, and all causes in Japan: the Ohsaki study. Kuriyama S, Shimazu T, Ohmori K, Kikuchi N, Nakaya N, Nishino Y, Tsubono Y, Tsuji I. JAMA. 2006 Sep 13; 296(10):1255-65. https://jamanetwork.com/journals/jama/fullarticle/203337[↩]
- Effects of tea and coffee on cardiovascular disease risk. Bøhn SK, Ward NC, Hodgson JM, Croft KD. Food Funct. 2012 Jun; 3(6):575-91. https://www.ncbi.nlm.nih.gov/pubmed/22456725/[↩]
- Pearson DA, Frakel EN, Aeschbach R, et al. Inhibition of endothelial cell mediated low-density lipoprotein oxidation by green tea extracts. J Agric Food Chem. 1998;46(4):1445–1449. doi: 10.1021/jf970889b.[↩]
- The protective effect of habitual tea consumption on hypertension. Yang YC, Lu FH, Wu JS, Wu CH, Chang CJ. Arch Intern Med. 2004 Jul 26; 164(14):1534-40. https://www.ncbi.nlm.nih.gov/pubmed/15277285/[↩]
- The potential role of green tea catechins in the prevention of the metabolic syndrome – a review. Thielecke F, Boschmann M. Phytochemistry. 2009 Jan; 70(1):11-24. https://www.ncbi.nlm.nih.gov/pubmed/19147161/[↩]
- Coffee, decaffeinated coffee, and tea consumption in relation to incident type 2 diabetes mellitus: a systematic review with meta-analysis. Huxley R, Lee CM, Barzi F, Timmermeister L, Czernichow S, Perkovic V, Grobbee DE, Batty D, Woodward M. Arch Intern Med. 2009 Dec 14; 169(22):2053-63. https://www.ncbi.nlm.nih.gov/pubmed/20008687/[↩]
- The relationship between green tea and total caffeine intake and risk for self-reported type 2 diabetes among Japanese adults. Iso H, Date C, Wakai K, Fukui M, Tamakoshi A, JACC Study Group. Ann Intern Med. 2006 Apr 18; 144(8):554-62. https://www.ncbi.nlm.nih.gov/pubmed/16618952/[↩]
- Associations of dietary flavonoids with risk of type 2 diabetes, and markers of insulin resistance and systemic inflammation in women: a prospective study and cross-sectional analysis. Song Y, Manson JE, Buring JE, Sesso HD, Liu S. J Am Coll Nutr. 2005 Oct; 24(5):376-84. https://www.ncbi.nlm.nih.gov/pubmed/16192263/[↩]
- Weight control and prevention of metabolic syndrome by green tea. Sae-tan S, Grove KA, Lambert JD. Pharmacol Res. 2011 Aug; 64(2):146-54. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3123415/[↩]
- Effect of green tea on blood glucose levels and serum proteomic patterns in diabetic (db/db) mice and on glucose metabolism in healthy humans. Tsuneki H, Ishizuka M, Terasawa M, Wu JB, Sasaoka T, Kimura I. BMC Pharmacol. 2004 Aug 26; 4():18. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC517497/[↩]
- Joshua D. Lambert, Chung S. Yang, Mechanisms of Cancer Prevention by Tea Constituents, The Journal of Nutrition, Volume 133, Issue 10, October 2003, Pages 3262S–3267S, https://doi.org/10.1093/jn/133.10.3262S[↩]
- Yang CS, Maliakal P, Meng X. Inhibition of carcinogenesis by tea. Annu Rev Pharmacol Toxicol. 2002;42:25-54. doi: 10.1146/annurev.pharmtox.42.082101.154309[↩]
- Filippini T, Malavolti M, Borrelli F, Izzo AA, Fairweather-Tait SJ, Horneber M, Vinceti M. Green tea (Camellia sinensis) for the prevention of cancer. Cochrane Database Syst Rev. 2020 Mar 2;3(3):CD005004. doi: 10.1002/14651858.CD005004.pub3[↩][↩][↩]
- Tea and Cancer Prevention. https://www.cancer.gov/about-cancer/causes-prevention/risk/diet/tea-fact-sheet[↩][↩]
- Du GJ, Zhang Z, Wen XD, Yu C, Calway T, Yuan CS, Wang CZ. Epigallocatechin Gallate (EGCG) is the most effective cancer chemopreventive polyphenol in green tea. Nutrients. 2012 Nov 8;4(11):1679-91. doi: 10.3390/nu4111679[↩]
- Li N, Sun Z, Han C, Chen J. The chemopreventive effects of tea on human oral precancerous mucosa lesions. Proc Soc Exp Biol Med. 1999 Apr;220(4):218-24. doi: 10.1046/j.1525-1373.1999.d01-37.x[↩][↩]
- Tsao AS, Liu D, Martin J, Tang XM, Lee JJ, El-Naggar AK, Wistuba I, Culotta KS, Mao L, Gillenwater A, Sagesaka YM, Hong WK, Papadimitrakopoulou V. Phase II randomized, placebo-controlled trial of green tea extract in patients with high-risk oral premalignant lesions. Cancer Prev Res (Phila). 2009 Nov;2(11):931-41. doi: 10.1158/1940-6207.CAPR-09-0121[↩][↩]
- Iman A. Hakim, Robin B. Harris, Sylvia Brown, H-H. Sherry Chow, Sheila Wiseman, Sanjiv Agarwal, Wendy Talbot, Effect of Increased Tea Consumption on Oxidative DNA Damage among Smokers: A Randomized Controlled Study, The Journal of Nutrition, Volume 133, Issue 10, October 2003, Pages 3303S–3309S, https://doi.org/10.1093/jn/133.10.3303S[↩][↩][↩]
- Haitao Luo, Lili Tang, Meng Tang, Madhavi Billam, Tianren Huang, Jiahua Yu, Zhongliang Wei, Yongqiang Liang, Kaibo Wang, Zhen-Quan Zhang, Lisheng Zhang, Jia-Sheng Wang, Phase IIa chemoprevention trial of green tea polyphenols in high-risk individuals of liver cancer: modulation of urinary excretion of green tea polyphenols and 8-hydroxydeoxyguanosine, Carcinogenesis, Volume 27, Issue 2, February 2006, Pages 262–268, https://doi.org/10.1093/carcin/bgi147[↩][↩]
- Bettuzzi S, Brausi M, Rizzi F, Castagnetti G, Peracchia G, Corti A. Chemoprevention of human prostate cancer by oral administration of green tea catechins in volunteers with high-grade prostate intraepithelial neoplasia: a preliminary report from a one-year proof-of-principle study. Cancer Res. 2006 Jan 15;66(2):1234-40. doi: 10.1158/0008-5472.CAN-05-1145[↩][↩]
- Jatoi, A., Ellison, N., Burch, P.A., Sloan, J.A., Dakhil, S.R., Novotny, P., Tan, W., Fitch, T.R., Rowland, K.M., Young, C.Y.F. and Flynn, P.J. (2003), A Phase II trial of green tea in the treatment of patients with androgen independent metastatic prostate carcinoma. Cancer, 97: 1442-1446. https://doi.org/10.1002/cncr.11200[↩]
- Choan E, Segal R, Jonker D, Malone S, Reaume N, Eapen L, Gallant V. A prospective clinical trial of green tea for hormone refractory prostate cancer: an evaluation of the complementary/alternative therapy approach. Urol Oncol. 2005 Mar-Apr;23(2):108-13. doi: 10.1016/j.urolonc.2004.10.008[↩]
- Hamajima N, Tajima K, Tominaga S, Matsuura A, Kuwabara M, Okuma K. Tea polyphenol intake and changes in serum pepsinogen levels. Jpn J Cancer Res. 1999 Feb;90(2):136-43. doi: 10.1111/j.1349-7006.1999.tb00726.x[↩][↩]
- Wang LD, Zhou Q, Feng CW, Liu B, Qi YJ, Zhang YR, Gao SS, Fan ZM, Zhou Y, Yang CS, Wei JP, Zheng S. Intervention and follow-up on human esophageal precancerous lesions in Henan, northern China, a high-incidence area for esophageal cancer. Gan To Kagaku Ryoho. 2002 Feb;29 Suppl 1:159-72.[↩][↩]
- Muramatsu K, Fukuyo M, Hara Y. Effect of green tea catechins on plasma cholesterol level in cholesterol-fed rats. J Nutr Sci Vitaminol (Tokyo). 1986 Dec;32(6):613-22. doi: 10.3177/jnsv.32.613[↩]
- Yang T.T., Koo M.W. Chinese green tea lowers cholesterol level through an increase in fecal lipid excretion. Life Sci. 1999;66:411–423. doi: 10.1016/S0024-3205(99)00607-4[↩]
- Afzalpour M.E., Ghasemi E., Zarban A. Effects of 10 weeks of high intensity interval training and green tea supplementation on serum levels of Sirtuin-1 and peroxisome proliferator-activated receptor gamma co-activator 1-alpha in overweight women. Sci. Sports. 2017;32:82–90. doi: 10.1016/j.scispo.2016.09.004[↩]
- Ali M., Afzal M., Gubler C., Burka J.F. A potent thromboxane formation inhibitor in green tea leaves. Prostaglandins Leukot. Essent. Fat. Acids. 1990;40:281–283. doi: 10.1016/0952-3278(90)90050-U[↩][↩]
- Abe I., Seki T., Umehara K., Miyase T., Noguchi H., Sakakibara J., Ono T. Green tea polyphenols: Novel and potent inhibitors of squalene epoxidase. Biochem. Biophys. Res. Commun. 2000;268:767–771. doi: 10.1006/bbrc.2000.2217[↩]
- Kasaoka S., Hase K., Morita T., Kiriyama S. Green tea flavonoids inhibit the LDL oxidation in osteogenic disordered rats fed a marginal ascorbic acid in diet. J. Nutr. Biochem. 2002;13:96–102. doi: 10.1016/S0955-2863(01)00202-9[↩]
- Yoshikawa M., Morikawa T., Yamamoto K., Kato Y., Nagatomo A., Matsuda H. Floratheasaponins A−C, acylated oleanane-type triterpene oligoglycosides with anti-hyperlipidemic activities from flowers of the Tea plant (Camellia sinensis) J. Nat. Prod. 2005;68:1360–1365. doi: 10.1021/np0580614[↩]
- Hamdaoui M.H., Snoussi C., Dhaouadi K., Fattouch S., Ducroc R., Le Gall M., Bado A. Tea decoctions prevent body weight gain in rats fed high-fat diet; black tea being more efficient than green tea. J. Nutr. Intermed. Metab. 2016;6:33–40. doi: 10.1016/j.jnim.2016.07.002[↩]
- Stepien M, Kujawska-Luczak M, Szulinska M, Kregielska-Narozna M, Skrypnik D, Suliburska J, Skrypnik K, Regula J, Bogdanski P. Beneficial dose-independent influence of Camellia sinensis supplementation on lipid profile, glycemia, and insulin resistance in an NaCl-induced hypertensive rat model. J Physiol Pharmacol. 2018 Apr;69(2). doi: 10.26402/jpp.2018.2.13[↩]
- Yousaf S, Butt MS, Suleria HA, Iqbal MJ. The role of green tea extract and powder in mitigating metabolic syndromes with special reference to hyperglycemia and hypercholesterolemia. Food Funct. 2014 Mar;5(3):545-56. doi: 10.1039/c3fo60203f[↩]
- Li SB, Li YF, Mao ZF, Hu HH, Ouyang SH, Wu YP, Tsoi B, Gong P, Kurihara H, He RR. Differing chemical compositions of three teas may explain their different effects on acute blood pressure in spontaneously hypertensive rats. J Sci Food Agric. 2015 Apr;95(6):1236-42. doi: 10.1002/jsfa.6811[↩]
- Miltonprabu S., Thangapandiyan S. Epigallocatechin gallate potentially attenuates Fluoride induced oxidative stress mediated cardiotoxicity and dyslipidemia in rats. J. Trace. Elem. Med. Biol. 2015;29:321–335. doi: 10.1016/j.jtemb.2014.08.015[↩]
- Nomura S., Monobe M., Ema K., Matsunaga A., Maeda-Yamamoto M., Horie H. Effects of flavonol-rich green tea cultivar (Camellia sinensis L.) on plasma oxidized LDL levels in hypercholesterolemic mice. Biosci. Biotechnol. Biochem. 2016;80:360–362. doi: 10.1080/09168451.2015.1083400[↩]
- Paudel K.R., Lee U.W., Kim D.W. Chungtaejeon, a Korean fermented tea, prevents the risk of atherosclerosis in rats fed a high-fat atherogenic diet. J. Integr. Med. 2016;14:134–142. doi: 10.1016/S2095-4964(16)60249-2[↩]
- Hartley L, Flowers N, Holmes J, Clarke A, Stranges S, Hooper L, Rees K. Green and black tea for the primary prevention of cardiovascular disease. Cochrane Database of Systematic Reviews 2013, Issue 6. Art. No.: CD009934. DOI: 10.1002/14651858.CD009934.pub2. http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD009934.pub2/full[↩]
- Green tea catechins decrease total and low-density lipoprotein cholesterol: a systematic review and meta-analysis. J Am Diet Assoc. 2011 Nov;111(11):1720-9. doi: 10.1016/j.jada.2011.08.009. https://jandonline.org/article/S0002-8223(11)01379-4/fulltext[↩]
- Gumprecht J., Domek M., Lip G.Y., Shantsila A. Invited review: Hypertension and atrial fibrillation: Epidemiology, pathophysiology, and implications for management. J. Hum. Hypertens. 2019;33:1–13. doi: 10.1038/s41371-019-0279-7[↩]
- Abe Y., Umemura S., Sugimoto K.-I., Hirawa N., Kato Y., Yokoyama N., Yokoyama T., Iwai J., Ishii M. Effect of green tea rich in γ-aminobutyric acid on blood pressure of Dahl salt-sensitive rats. Am. J. Hypertens. 1995;8:74–79. doi: 10.1016/0895-7061(94)00141-W[↩]
- Juneja L.R., Chu D.-C., Okubo T., Nagato Y., Yokogoshi H. L-theanine—A unique amino acid of green tea and its relaxation effect in humans. Trends Food Sci. Technol. 1999;10:199–204. doi: 10.1016/S0924-2244(99)00044-8[↩]
- Bertoldi M., Gonsalvi M., Voltattorni C.B. Green tea polyphenols: Novel irreversible inhibitors of dopa decarboxylase. Biochem. Biophys. Res. Commun. 2001;284:90–93. doi: 10.1006/bbrc.2001.4945[↩][↩]
- Yi Q.-Y., Li H.-B., Qi J., Yu X.-J., Huo C.-J., Li X., Bai J., Gao H.-L., Kou B., Liu K.-L., et al. Chronic infusion of epigallocatechin-3-O-gallate into the hypothalamic paraventricular nucleus attenuates hypertension and sympathoexcitation by restoring neurotransmitters and cytokines. Toxicol. Lett. 2016;262:105–113. doi: 10.1016/j.toxlet.2016.09.010[↩]
- Antonello M., Montemurro D., Bolognesi M., Di Pascoli M., Piva A., Grego F., Sticchi D., Giuliani L., Garbisa S., Rossi G.P. Prevention of hypertension, cardiovascular damage and endothelial dysfunction with green tea extracts. Am. J. Hypertens. 2007;20:1321–1328. doi: 10.1016/j.amjhyper.2007.08.006[↩]
- Ihm S.-H., Jang S.-W., Kim O.-R., Chang K., Oak M.-H., Lee J.-O., Lim D.-Y., Kim J.-H. Decaffeinated green tea extract improves hypertension and insulin resistance in a rat model of metabolic syndrome. Atherosclerosis. 2012;224:377–383. doi: 10.1016/j.atherosclerosis.2012.07.006[↩]
- Ghaffari S., Roshanravan N. The role of nutraceuticals in prevention and treatment of hypertension: An updated review of the literature. Food Res. Int. 2020;128:108749. doi: 10.1016/j.foodres.2019.108749[↩]
- San Cheang W, Yuen Ngai C, Yen Tam Y, Yu Tian X, Tak Wong W, Zhang Y, Wai Lau C, Chen ZY, Bian ZX, Huang Y, Ping Leung F. Black tea protects against hypertension-associated endothelial dysfunction through alleviation of endoplasmic reticulum stress. Sci Rep. 2015 May 15;5:10340. doi: 10.1038/srep10340[↩][↩]
- Nomura S, Monobe M, Ema K, Maeda-Yamamoto M, Nesumi A. Comparison of the Effects of Three Tea Cultivars (Camellia sinensis L.) on Nitric Oxide Production and Aortic Soluble Guanylate Cyclase Expression in High-Salt Diet-Fed Spontaneously Hypertensive Rats. J Nutr Sci Vitaminol (Tokyo). 2017;63(5):306-314. doi: 10.3177/jnsv.63.306[↩]
- Vinson J.A., Dabbagh Y.A. Effect of green and black tea supplementation on lipids, lipid oxidation and fibrinogen in the hamster: Mechanisms for the epidemiological benefits of tea drinking. FEBS Lett. 1998;433:44–46. doi: 10.1016/S0014-5793(98)00880-1[↩][↩]
- Hartley L, Flowers N, Holmes J, Clarke A, Stranges S, Hooper L, Rees K. Green and black tea for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2013 Jun 18;2013(6):CD009934. doi: 10.1002/14651858.CD009934.pub2[↩][↩]
- Wasilewski R., Ubara E.O., Klonizakis M. Assessing the effects of a short-term green tea intervention in skin microvascular function and oxygen tension in older and younger adults. Microvasc. Res. 2016;107:65–71. doi: 10.1016/j.mvr.2016.05.001[↩]
- Yang T., Koo M. Inhibitory effect of Chinese green tea on endothelial cell-induced LDL oxidation. Atherosclerosis. 2000;148:67–73. doi: 10.1016/S0021-9150(99)00239-7[↩][↩]
- Song D.U., Do Jung Y., Chay K.O., Chung M.A., Lee K.H., Yang S.Y., Shin B.A., Ahn B.W. Effect of drinking green tea on age-associated accumulation of Maillard-type fluorescence and carbonyl groups in rat aortic and skin collagen. Arch. Biochem. Biophys. 2002;397:424–429. doi: 10.1006/abbi.2001.2695[↩]
- Pang J., Zhang Z., Zheng T.-z., Bassig B.A., Mao C., Liu X., Zhu Y., Shi K., Ge J., Yang Y.-j. Green tea consumption and risk of cardiovascular and ischemic related diseases: A meta-analysis. Int. J. Cardiol. 2016;202:967–974. doi: 10.1016/j.ijcard.2014.12.176[↩]
- Lustosa B.B., Polegato B., Minicucci M., Rafacho B., Santos P.P., Fernandes A.A., Okoshi K., Batista D., Modesto P., Gonçalves A., et al. Green tea (Cammellia sinensis) attenuates ventricular remodeling after experimental myocardial infarction. Int. J. Cardiol. 2016;225:147–153. doi: 10.1016/j.ijcard.2016.09.092[↩]
- Bordoni A., Hrelia S., Angeloni C., Giordano E., Guarnieri C., Caldarera C.M., Biagi P.L. Green tea protection of hypoxia/reoxygenation injury in cultured cardiac cells. J. Nutr. Biochem. 2002;13:103–111. doi: 10.1016/S0955-2863(01)00203-0[↩]
- Cheng T.O. All teas are not created equal: The Chinese green tea and cardiovascular health. Int. J. Cardiol. 2006;108:301–308. doi: 10.1016/j.ijcard.2005.05.038[↩]
- Sun T.-L., Liu Z., Qi Z.-J., Huang Y.-P., Gao X.-Q., Zhang Y.-Y. (−)-Epigallocatechin-3-gallate (EGCG) attenuates arsenic-induced cardiotoxicity in rats. Food Chem. Toxicol. 2016;93:102–110. doi: 10.1016/j.fct.2016.05.004[↩]
- Oyama J., Shiraki A., Nishikido T., Maeda T., Komoda H., Shimizu T., Makino N., Node K. EGCG, a green tea catechin, attenuates the progression of heart failure induced by the heart/muscle-specific deletion of MnSOD in mice. Int. J. Cardiol. 2017;69:417–427. doi: 10.1016/j.jjcc.2016.05.019[↩]
- Ale-Agha N., Stahl W., Sies H. (−)-Epicatechin effects in rat liver epithelial cells: Stimulation of gap junctional communication and counteraction of its loss due to the tumor promoter 12-O-tetradecanoylphorbol-13-acetate. Biochem. Pharmacol. 2002;63:2145–2149. doi: 10.1016/S0006-2952(02)01021-3[↩]
- Dower J.I., Geleijnse J.M., Gijsbers L., Zock P.L., Kromhout D., Hollman P.C. Effects of the pure flavonoids epicatechin and quercetin on vascular function and cardiometabolic health: A randomized, double-blind, placebo-controlled, crossover trial. Am. J. Clin. Nutr. 2015;101:914–921. doi: 10.3945/ajcn.114.098590[↩]
- Kang W.-S., Lim I.-H., Yuk D.-Y., Chung K.-H., Park J.-B., Yoo H.-S., Yun Y.-P. Antithrombotic activities of green tea catechins and (−)-epigallocatechin gallate. Thromb. Res. 1999;96:229–237. doi: 10.1016/S0049-3848(99)00104-8[↩]
- Lau K.-M., He Z.-D., Dong H., Fung K.-P., But P.P.-H. Anti-oxidative, anti-inflammatory and hepato-protective effects of Ligustrum robustum. J. Ethnopharmacol. 2002;83:63–71. doi: 10.1016/S0378-8741(02)00192-7[↩]
- Ohnishi S.T., Ohnishi T., Ogunmola G.B. Green tea extract and aged garlic extract inhibit anion transport and sickle cell dehydration in vitro. Blood Cells Mol. Dis. 2001;27:148–157. doi: 10.1006/bcmd.2000.0368[↩]
- Fan W. Epidemiology in diabetes mellitus and cardiovascular disease. Cardiovasc. Endocrinol. Metab. 2017;6:8–16. doi: 10.1097/XCE.0000000000000116[↩]
- Diabetes facts & figures. https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html[↩][↩]
- Thomas N.J., Jones S.E., Weedon M.N., Shields B.M., Oram R.A., Hattersley A.T. Frequency and phenotype of type 1 diabetes in the first six decades of life: A cross-sectional, genetically stratified survival analysis from UK Biobank. Lancet Diabetes Endocrinol. 2018;6:122–129. doi: 10.1016/S2213-8587(17)30362-5[↩]
- Type 2 diabetes. https://www.idf.org/aboutdiabetes/type-2-diabetes.html[↩]
- McIntyre H.D., Catalano P., Zhang C., Desoye G., Mathiesen E.R., Damm P. Gestational diabetes mellitus. Nat. Rev. Dis. Primers. 2019;5:1–19. doi: 10.1038/s41572-019-0098-8[↩]
- Othman A.I., El-Sawi M.R., El-Missiry M.A., Abukhalil M.H. Epigallocatechin-3-gallate protects against diabetic cardiomyopathy through modulating the cardiometabolic risk factors, oxidative stress, inflammation, cell death and fibrosis in streptozotocin-nicotinamide-induced diabetic rats. Biomed. Pharm. 2017;94:362–373. doi: 10.1016/j.biopha.2017.07.129[↩][↩][↩]
- Kumar D., Rizvi S.I. Black tea extract improves anti-oxidant profile in experimental diabetic rats. Arch. Physiol. Biochem. 2015;121:109–115. doi: 10.3109/13813455.2015.1043308[↩][↩]
- Kumar S, Narwal S, Kumar V, Prakash O. α-glucosidase inhibitors from plants: A natural approach to treat diabetes. Pharmacogn Rev. 2011 Jan;5(9):19-29. doi: 10.4103/0973-7847.79096[↩]
- Yang X., Kong F. Evaluation of the in vitro α-glucosidase inhibitory activity of green tea polyphenols and different tea types. J. Sci. Food Agric. 2016;96:777–782. doi: 10.1002/jsfa.7147[↩]
- Oh J, Jo SH, Kim JS, Ha KS, Lee JY, Choi HY, Yu SY, Kwon YI, Kim YC. Selected tea and tea pomace extracts inhibit intestinal α-glucosidase activity in vitro and postprandial hyperglycemia in vivo. Int J Mol Sci. 2015 Apr 21;16(4):8811-25. doi: 10.3390/ijms16048811[↩]
- Satoh T., Igarashi M., Yamada S., Takahashi N., Watanabe K. Inhibitory effect of black tea and its combination with acarbose on small intestinal α-glucosidase activity. J. Ethnopharmacol. 2015;161:147–155. doi: 10.1016/j.jep.2014.12.009[↩]
- Weerawatanakorna M., Hung W.-L., Pan M.-H., Li. S., Li D., Wan X., Ho C.-T. Chemistry and health beneficial effects of oolong tea and theasinensins. FSHW. 2015;4:133–146. doi: 10.1016/j.fshw.2015.10.002[↩]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Coffee, Tea, Mate, Methylxanthines and Methylglyoxal. Lyon (FR): International Agency for Research on Cancer; 1991. (IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 51.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK507026[↩]
- Deng Y.T., Lin-Shiau S.Y., Shyur L.F., Lin J.K. Pu-erh tea polysaccharides decrease blood sugar by inhibition of α-glucosidase activity in vitro and in mice. Food Funct. 2015;6:1539–1546. doi: 10.1039/C4FO01025F[↩]
- Xu P., Wu J., Zhang Y., Chen H., Wang Y. Physicochemical characterization of pu-erh tea polysaccharides and their antioxidant and α-glycosidase inhibition. J. Funct. Foods. 2014;6:545–554. doi: 10.1016/j.jff.2013.11.021[↩]
- Wang X., Liu Q., Zhu H., Wang H., Kang J., Shen Z., Chen R. Flavanols from the Camellia sinensis var. Assamica and their hypoglycemic and hypolipidemic activities. Acta Pharm. Sin. B. 2017;7:342–346. doi: 10.1016/j.apsb.2016.12.007[↩]
- Wu X., Hu M., Hu X., Ding H., Gong D., Zhang G. Inhibitory mechanism of epicatechin gallate on α-amylase and α-glucosidase and its combinational effect with acarbose or epigallocatechin gallate. J. Mol. Liq. 2019;290:111202. doi: 10.1016/j.molliq.2019.111202[↩]
- Zhou H., Li H.-M., Du Y.-M., Yan R.-A., Fu L. C-geranylated flavanones from Ying De black tea and their antioxidant and α-glucosidase inhibition activities. Food Chem. 2017;235:227–333. doi: 10.1016/j.foodchem.2017.05.034[↩]
- Hua F., Zhou P., Wu H.Y., Chu G.X., Xie Z.W., Bao G.H. Inhibition of α-glucosidase and α-amylase by flavonoid glycosides from Lu’an GuaPian tea: Molecular docking and interaction mechanism. Food Funct. 2018;9:4173–4183. doi: 10.1039/C8FO00562A[↩][↩][↩]
- Li S., Chen H., Wang J., Wang X., Hu B., Lv F. Involvement of the PI3K/Akt signal pathway in the hypoglycemic effects of tea polysaccharides on diabetic mice. Int. J. Biol. Macromol. 2015;81:967–974. doi: 10.1016/j.ijbiomac.2015.09.037[↩]
- Yousaf S., Butt M.S., Suleria H.A., Iqbal M.J. The role of green tea extract and powder in mitigating metabolic syndromes with special reference to hyperglycemia and hypercholesterolemia. Food Funct. 2014;5:545–556. doi: 10.1039/c3fo60203f[↩]
- Ramlagan P., Rondeau P., Planesse C., Neergheen-Bhujun V.S., Bourdon E., Bahorun T. Comparative suppressing effects of black and green teas on the formation of advanced glycation end products (AGEs) and AGE-induced oxidative stress. Food Funct. 2017;8:4194–4209. doi: 10.1039/C7FO01038A[↩]
- Al Anouti F., Taha Z., Shamim S., Khalaf K., Al Kaabi L., Alsafar H. An insight into the paradigms of osteoporosis: From genetics to biomechanics. Bone. 2019;11:100216. doi: 10.1016/j.bonr.2019.100216[↩]
- Ralston S.H., de Crombrugghe B. Genetic regulation of bone mass and susceptibility to osteoporosis. Genes Dev. 2006;20:2492–2506. doi: 10.1101/gad.1449506[↩][↩]
- Domazetovic V., Marcucci G., Iantomasi T., Brandi M.L., Vincenzini M.T. Oxidative stress in bone remodeling: Role of antioxidants. Clin. Cases Min. Bone Metab. 2017;14:209–216. doi: 10.11138/ccmbm/2017.14.1.209[↩]
- Zeng X., Tian J., Cai K., Wu X., Wang Y., Zheng Y., Su Y., Cui L. Promoting osteoblast differentiation by the flavanes from Huangshan Maofeng tea is linked to a reduction of oxidative stress. Phytomedicine. 2014;21:217–224. doi: 10.1016/j.phymed.2013.08.026[↩]
- Xu H., Yin D., Liu T., Chen F., Chen Y., Wang X., Sheng J. Tea polysaccharide inhibits RANKL-induced osteoclastogenesis in raw264. 7 cells and ameliorates ovariectomy-induced osteoporosis in rats. Biomed. Pharm. 2018;102:539–548. doi: 10.1016/j.biopha.2018.03.125[↩]
- Shen C.L., Han J., Wang S., Chung E., Chyu M.C., Cao J.J. Green tea supplementation benefits body composition and improves bone properties in obese female rats fed with high-fat diet and caloric restricted diet. Nutr. Res. 2015;35:1095–1105. doi: 10.1016/j.nutres.2015.09.014[↩]
- Ikigai H., Nakae T., Hara Y., Shimamura T. Bactericidal catechins damage the lipid bilayer. Biochim. Biophys. Acta (BBA) Biomembr. 1993;1147:132–136. doi: 10.1016/0005-2736(93)90323-R[↩]
- Rasheed A., Haider M. Antibacterial activity of Camellia sinensis extracts against dental caries. Arch. Pharm. Res. 1998;21:348–352. doi: 10.1007/BF02975300[↩]
- Sugita-Konishi Y., Hara-Kudo Y., Amano F., Okubo T., Aoi N., Iwaki M., Kumagai S. Epigallocatechin gallate and gallocatechin gallate in green tea catechins inhibit extracellular release of Vero toxin from enterohemorrhagic Escherichia coli O157: H7. Biochim. Biophys. Acta (BBA) Gen. Subj. 1999;1472:42–50. doi: 10.1016/S0304-4165(99)00102-6[↩]
- Hui X., Liu H., Tian F.-L., Li F.-F., Li H., Gao W.-Y. Inhibition of green tea and the catechins against 1-deoxy-d-xylulose 5-phosphate reductoisomerase, the key enzyme of the MEP terpenoid biosynthetic pathway. Fitoterapia. 2016;113:80–84. doi: 10.1016/j.fitote.2016.07.009[↩]
- Dyer P.D.R., Kotha A.K., Gollings A.S., Shorter S.A., Shepherd T.R., Pettit M.W., Alexander B.D., Getti G.T.M., El-Daher S., Baillie L., et al. An in vitro evaluation of epigallocatechin gallate (eGCG) as a biocompatible inhibitor of ricin toxin. Biochim. Biophys. Acta (BBA) Gen. Subj. 2016;1860:1541–1550. doi: 10.1016/j.bbagen.2016.03.024[↩]
- Rizk M.A., El-Sayed S.A.E.-S., AbouLaila M., Tuvshintulga B., Yokoyama N., Igarashi I. Large-scale drug screening against Babesia divergens parasite using a fluorescence-based high-throughput screening assay. Vet. Parasitol. 2016;227:93–97. doi: 10.1016/j.vetpar.2016.07.032[↩]
- Tsou L.K., Yount J.S., Hang H.C. Epigallocatechin-3-gallate inhibits bacterial virulence and invasion of host cells. Bioorg. Med. Chem. 2017;25:2883–2887. doi: 10.1016/j.bmc.2017.03.023[↩]
- Piva G., Fracassetti D., Tirelli A., Mascheroni E., Musatti A., Inglese P., Piergiovanni L., Rollini M. Evaluation of the antioxidant/antimicrobial performance of Posidonia oceanica in comparison with three commercial natural extracts and as a treatment on fresh-cut peaches (Prunus persica Batsch) Postharvest Biol. Technol. 2017;124:54–61. doi: 10.1016/j.postharvbio.2016.10.001[↩]
- Sakanaka S., Juneja L.R., Taniguchi M. Antimicrobial effects of green tea polyphenols on thermophilic spore-forming bacteria. J. Biosci. Bioeng. 2000;90:81–85. doi: 10.1016/S1389-1723(00)80038-9[↩]
- Yun J., Lee D.G. Role of potassium channels in chlorogenic acid-induced apoptotic volume decrease and cell cycle arrest in Candida albicans. Biochim. Biophys. Acta (BBA) Gen. Subj. 2017;1861:585–592. doi: 10.1016/j.bbagen.2016.12.026[↩]
- Burkard M., Leischner C., Lauer U.M., Busch C., Venturelli S., Frank J. Dietary flavonoids and modulation of natural killer cells: Implications in malignant and viral diseases. J. Nutr. Biochem. 2017;46:1–12. doi: 10.1016/j.jnutbio.2017.01.006[↩]
- Carneiro B.M., Batista M.N., Braga A.C.S., Nogueira M.L., Rahal P. The green tea molecule EGCG inhibits Zika virus entry. Virology. 2016;496:215–218. doi: 10.1016/j.virol.2016.06.012[↩]
- Hartjen P., Frerk S., Hauber I., Matzat V., Thomssen A., Holstermann B., Hohenberg H., Schulze W., zur Wiesch J.S., van Lunzen J. Assessment of the range of the HIV-1 infectivity enhancing effect of individual human semen specimen and the range of inhibition by EGCG. AIDS Res. Ther. 2012;9:2. doi: 10.1186/1742-6405-9-2[↩]
- Hara Y. Tea catechins and their applications as supplements and pharmaceutics. Pharmacol Res. 2011 Aug;64(2):100-4. doi: 10.1016/j.phrs.2011.03.018[↩]
- Miyoshi N, Tanabe H, Suzuki T, Saeki K, Hara Y. Applications of a Standardized Green Tea Catechin Preparation for Viral Warts and Human Papilloma Virus-Related and Unrelated Cancers. Molecules. 2020 Jun 2;25(11):2588. doi: 10.3390/molecules25112588[↩]
- Dunne E.F., Friedman A., Datta S.D., Markowitz L.E., Workowski K.A. Updates on human papillomavirus and genital warts and counseling messages from the 2010 Sexually Transmitted Diseases Treatment Guidelines. Clin. Infect. Dis. 2011;53:143–152. doi: 10.1093/cid/cir703[↩]
- David A Camfield, Con Stough, Jonathon Farrimond, Andrew B Scholey, Acute effects of tea constituents L-theanine, caffeine, and epigallocatechin gallate on cognitive function and mood: a systematic review and meta-analysis, Nutrition Reviews, Volume 72, Issue 8, 1 August 2014, Pages 507–522, https://doi.org/10.1111/nure.12120[↩]
- Hong J.T., Ryu S.R., Kim H.J., Lee J.K., Lee S.H., Kim D.B., Yun Y.P., Ryu J.H., Lee B.M., Kim P.Y. Neuroprotective effect of green tea extract in experimental ischemia-reperfusion brain injury. Brain Res. Bull. 2000;53:743–749. doi: 10.1016/S0361-9230(00)00348-8[↩]
- Guo Q., Zhao B., Li M., Shen S., Xin W. Studies on protective mechanisms of four components of green tea polyphenols against lipid peroxidation in synaptosomes. Biochim. Biophys. Acta (BBA) Lipid Lipid Metab. 1996;1304:210–222. doi: 10.1016/S0005-2760(96)00122-1[↩]
- Zhao X., Liu F., Jin H., Li R., Wang Y., Zhang W., Wang H., Chen W. Involvement of PKCα and ERK1/2 signaling pathways in EGCG’s protection against stress-induced neural injuries in Wistar rats. Neuroscience. 2017;346:226–237. doi: 10.1016/j.neuroscience.2017.01.025[↩]
- Suganuma M., Okabe S., Oniyama M., Tada Y., Ito H., Fujiki H. Wide distribution of [3H](-)-epigallocatechin gallate, a cancer preventive tea polyphenol, in mouse tissue. Carcinogenesis. 1998;19:1771–1776. doi: 10.1093/carcin/19.10.1771[↩]
- Bai Q., Lyu Z., Yang X., Pan Z., Lou J., Dong T. Epigallocatechin-3-gallate promotes angiogenesis via up-regulation of Nfr2 signaling pathway in a mouse model of ischemic stroke. Behav. Brain Res. 2017;321:79–86. doi: 10.1016/j.bbr.2016.12.037[↩]
- Ben P., Zhang Z., Zhu Y., Xiong A., Gao Y., Mu J., Yin Z., Luo L. l-Theanine attenuates cadmium-induced neurotoxicity through the inhibition of oxidative damage and tau hyperphosphorylation. Neurotoxicology. 2016;57:95–103. doi: 10.1016/j.neuro.2016.09.010[↩]
- Weinreb O., Mandel S., Amit T., Youdim M.B. Neurological mechanisms of green tea polyphenols in Alzheimer’s and Parkinson’s diseases. J. Nutr. Biochem. 2004;15:506–516. doi: 10.1016/j.jnutbio.2004.05.002[↩]
- Unno K., Takabayashi F., Kishido T., Oku N. Suppressive effect of green tea catechins on morphologic and functional regression of the brain in aged mice with accelerated senescence (SAMP10) Exp. Gerontol. 2004;39:1027–1034. doi: 10.1016/j.exger.2004.03.033[↩]
- Choi J.-Y., Park C.-S., Kim D.-J., Cho M.-H., Jin B.-K., Pie J.-E., Chung W.-G. Prevention of nitric oxide-mediated 1-methyl-4-phenyl-1, 2, 3, 6-tetrahydropyridine-induced Parkinson’s disease in mice by tea phenolic epigallocatechin 3-gallate. Neurotoxicology. 2002;23:367–374. doi: 10.1016/S0161-813X(02)00079-7[↩]
- Rubio-Perez JM, Albaladejo MD, Zafrilla P, Vidal-Guevara ML, Morillas-Ruiz JM. Effects of an antioxidant beverage on biomarkers of oxidative stress in Alzheimer’s patients. Eur J Nutr. 2016 Sep;55(6):2105-16. doi: 10.1007/s00394-015-1024-9[↩]
- Galasko DR, Peskind E, Clark CM, Quinn JF, Ringman JM, Jicha GA, Cotman C, Cottrell B, Montine TJ, Thomas RG, Aisen P; Alzheimer’s Disease Cooperative Study. Antioxidants for Alzheimer disease: a randomized clinical trial with cerebrospinal fluid biomarker measures. Arch Neurol. 2012 Jul;69(7):836-41. doi: 10.1001/archneurol.2012.85[↩]
- Tomata Y, Sugiyama K, Kaiho Y, Honkura K, Watanabe T, Zhang S, Sugawara Y, Tsuji I. Green Tea Consumption and the Risk of Incident Dementia in Elderly Japanese: The Ohsaki Cohort 2006 Study. Am J Geriatr Psychiatry. 2016 Oct;24(10):881-9. doi: 10.1016/j.jagp.2016.07.009[↩]
- Noguchi-Shinohara M, Yuki S, Dohmoto C, Ikeda Y, Samuraki M, Iwasa K, Yokogawa M, Asai K, Komai K, Nakamura H, Yamada M. Consumption of green tea, but not black tea or coffee, is associated with reduced risk of cognitive decline. PLoS One. 2014 May 14;9(5):e96013. doi: 10.1371/journal.pone.0096013[↩]
- Feng L, Li J, Ng TP, Lee TS, Kua EH, Zeng Y. Tea drinking and cognitive function in oldest-old Chinese. J Nutr Health Aging. 2012;16(9):754-8. doi: 10.1007/s12603-012-0077-1[↩]
- Park SK, Jung IC, Lee WK, Lee YS, Park HK, Go HJ, Kim K, Lim NK, Hong JT, Ly SY, Rho SS. A combination of green tea extract and l-theanine improves memory and attention in subjects with mild cognitive impairment: a double-blind placebo-controlled study. J Med Food. 2011 Apr;14(4):334-43. doi: 10.1089/jmf.2009.1374[↩]
- Schmidt A, Hammann F, Wölnerhanssen B, Meyer-Gerspach AC, Drewe J, Beglinger C, Borgwardt S. Green tea extract enhances parieto-frontal connectivity during working memory processing. Psychopharmacology (Berl). 2014 Oct;231(19):3879-88. doi: 10.1007/s00213-014-3526-1[↩]
- Mandel SA, Avramovich-Tirosh Y, Reznichenko L, Zheng H, Weinreb O, Amit T, Youdim MB. Multifunctional activities of green tea catechins in neuroprotection. Modulation of cell survival genes, iron-dependent oxidative stress and PKC signaling pathway. Neurosignals. 2005;14(1-2):46-60. doi: 10.1159/000085385[↩]
- Ali B, Jamal QM, Shams S, Al-Wabel NA, Siddiqui MU, Alzohairy MA, Al Karaawi MA, Kesari KK, Mushtaq G, Kamal MA. In Silico Analysis of Green Tea Polyphenols as Inhibitors of AChE and BChE Enzymes in Alzheimer’s Disease Treatment. CNS Neurol Disord Drug Targets. 2016;15(5):624-8. doi: 10.2174/1871527315666160321110607[↩]
- Biasibetti R, Tramontina AC, Costa AP, Dutra MF, Quincozes-Santos A, Nardin P, Bernardi CL, Wartchow KM, Lunardi PS, Gonçalves CA. Green tea (-)epigallocatechin-3-gallate reverses oxidative stress and reduces acetylcholinesterase activity in a streptozotocin-induced model of dementia. Behav Brain Res. 2013 Jan 1;236(1):186-193. doi: 10.1016/j.bbr.2012.08.039[↩]
- Rezai-Zadeh K, Arendash GW, Hou H, Fernandez F, Jensen M, Runfeldt M, Shytle RD, Tan J. Green tea epigallocatechin-3-gallate (EGCG) reduces beta-amyloid mediated cognitive impairment and modulates tau pathology in Alzheimer transgenic mice. Brain Res. 2008 Jun 12;1214:177-87. doi: 10.1016/j.brainres.2008.02.107[↩]
- de la Torre R, de Sola S, Hernandez G, Farré M, Pujol J, Rodriguez J, Espadaler JM, Langohr K, Cuenca-Royo A, Principe A, Xicota L, Janel N, Catuara-Solarz S, Sanchez-Benavides G, Bléhaut H, Dueñas-Espín I, Del Hoyo L, Benejam B, Blanco-Hinojo L, Videla S, Fitó M, Delabar JM, Dierssen M; TESDAD study group. Safety and efficacy of cognitive training plus epigallocatechin-3-gallate in young adults with Down’s syndrome (TESDAD): a double-blind, randomised, placebo-controlled, phase 2 trial. Lancet Neurol. 2016 Jul;15(8):801-810. doi: 10.1016/S1474-4422(16)30034-5[↩]
- Wightman, E.L., Haskell, C.F., Forster, J.S., Veasey, R.C. and Kennedy, D.O. (2012), Epigallocatechin gallate, cerebral blood flow parameters, cognitive performance and mood in healthy humans: a double-blind, placebo-controlled, crossover investigation. Hum. Psychopharmacol Clin Exp, 27: 177-186. https://doi.org/10.1002/hup.1263[↩]
- Scholey A, Downey LA, Ciorciari J, Pipingas A, Nolidin K, Finn M, Wines M, Catchlove S, Terrens A, Barlow E, Gordon L, Stough C. Acute neurocognitive effects of epigallocatechin gallate (EGCG). Appetite. 2012 Apr;58(2):767-70. doi: 10.1016/j.appet.2011.11.016[↩]
- Cantero JL, Atienza M, Stickgold R, Kahana MJ, Madsen JR, Kocsis B. Sleep-dependent theta oscillations in the human hippocampus and neocortex. J Neurosci. 2003 Nov 26;23(34):10897-903. doi: 10.1523/JNEUROSCI.23-34-10897.2003[↩]
- Green Tea. https://www.nccih.nih.gov/health/green-tea[↩][↩]
- Jurgens TM, Whelan AM, Killian L, Doucette S, Kirk S, Foy E. Green tea for weight loss and weight maintenance in overweight or obese adults. Cochrane Database Syst Rev. 2012 Dec 12;12(12):CD008650. doi: 10.1002/14651858.CD008650.pub2[↩]
- Cabrera C, Artacho R, Giménez R. Beneficial effects of green tea–a review. J Am Coll Nutr. 2006 Apr;25(2):79-99. doi: 10.1080/07315724.2006.10719518[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Jenna M. Chin, Michele L. Merves, Bruce A. Goldberger, Angela Sampson-Cone, Edward J. Cone, Caffeine Content of Brewed Teas, Journal of Analytical Toxicology, Volume 32, Issue 8, October 2008, Pages 702–704, https://doi.org/10.1093/jat/32.8.702[↩][↩]
- Higdon JV, Frei B. Coffee and health: a review of recent human research. Crit Rev Food Sci Nutr. 2006;46(2):101-23. doi: 10.1080/10408390500400009[↩][↩][↩]
- Nawrot P, Jordan S, Eastwood J, Rotstein J, Hugenholtz A, Feeley M. Effects of caffeine on human health. Food Addit Contam. 2003 Jan;20(1):1-30. doi: 10.1080/0265203021000007840[↩][↩]
- Nelson, M. and Poulter, J. (2004), Impact of tea drinking on iron status in the UK: a review. Journal of Human Nutrition and Dietetics, 17: 43-54. https://doi.org/10.1046/j.1365-277X.2003.00497.x[↩][↩]
- Mielgo-Ayuso J, Barrenechea L, Alcorta P, Larrarte E, Margareto J, Labayen I. Effects of dietary supplementation with epigallocatechin-3-gallate on weight loss, energy homeostasis, cardiometabolic risk factors and liver function in obese women: randomised, double-blind, placebo-controlled clinical trial. Br J Nutr. 2014 Apr 14;111(7):1263-71. doi: 10.1017/S0007114513003784[↩]
- Kumar NB, Pow-Sang J, Egan KM, Spiess PE, Dickinson S, Salup R, Helal M, McLarty J, Williams CR, Schreiber F, Parnes HL, Sebti S, Kazi A, Kang L, Quinn G, Smith T, Yue B, Diaz K, Chornokur G, Crocker T, Schell MJ. Randomized, Placebo-Controlled Trial of Green Tea Catechins for Prostate Cancer Prevention. Cancer Prev Res (Phila). 2015 Oct;8(10):879-87. doi: 10.1158/1940-6207.CAPR-14-0324[↩][↩]
- Isomura T, Suzuki S, Origasa H, Hosono A, Suzuki M, Sawada T, Terao S, Muto Y, Koga T. Liver-related safety assessment of green tea extracts in humans: a systematic review of randomized controlled trials. Eur J Clin Nutr. 2016 Nov;70(11):1221-1229. doi: 10.1038/ejcn.2016.78. Epub 2016 May 18. Erratum in: Eur J Clin Nutr. 2016 Nov;70(11):1340.[↩]
- Dostal AM, Samavat H, Bedell S, Torkelson C, Wang R, Swenson K, Le C, Wu AH, Ursin G, Yuan JM, Kurzer MS. The safety of green tea extract supplementation in postmenopausal women at risk for breast cancer: results of the Minnesota Green Tea Trial. Food Chem Toxicol. 2015 Sep;83:26-35. doi: 10.1016/j.fct.2015.05.019[↩]
- Chow HH, Hakim IA, Vining DR, Crowell JA, Ranger-Moore J, Chew WM, Celaya CA, Rodney SR, Hara Y, Alberts DS. Effects of dosing condition on the oral bioavailability of green tea catechins after single-dose administration of Polyphenon E in healthy individuals. Clin Cancer Res. 2005 Jun 15;11(12):4627-33. doi: 10.1158/1078-0432.CCR-04-2549[↩][↩]
- Chow HH, Cai Y, Hakim IA, Crowell JA, Shahi F, Brooks CA, Dorr RT, Hara Y, Alberts DS. Pharmacokinetics and safety of green tea polyphenols after multiple-dose administration of epigallocatechin gallate and polyphenon E in healthy individuals. Clin Cancer Res. 2003 Aug 15;9(9):3312-9.[↩][↩]
- Matsuyama, T., Tanaka, Y., Kamimaki, I., Nagao, T. and Tokimitsu, I. (2008), Catechin Safely Improved Higher Levels of Fatness, Blood Pressure, and Cholesterol in Children. Obesity, 16: 1338-1348. https://doi.org/10.1038/oby.2008.60[↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Green Tea. [Updated 2020 Nov 20]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK547925[↩][↩][↩]
- EFSA Panel on Food Additives and Nutrient Sources added to Food (ANS), Younes M, Aggett P, Aguilar F, Crebelli R, Dusemund B, Filipič M, Frutos MJ, Galtier P, Gott D, Gundert-Remy U, Lambré C, Leblanc JC, Lillegaard IT, Moldeus P, Mortensen A, Oskarsson A, Stankovic I, Waalkens-Berendsen I, Woutersen RA, Andrade RJ, Fortes C, Mosesso P, Restani P, Arcella D, Pizzo F, Smeraldi C, Wright M. Scientific opinion on the safety of green tea catechins. EFSA J. 2018 Apr 18;16(4):e05239. doi: 10.2903/j.efsa.2018.5239[↩][↩][↩][↩]





{kind=link}