What is the sphenoid bone
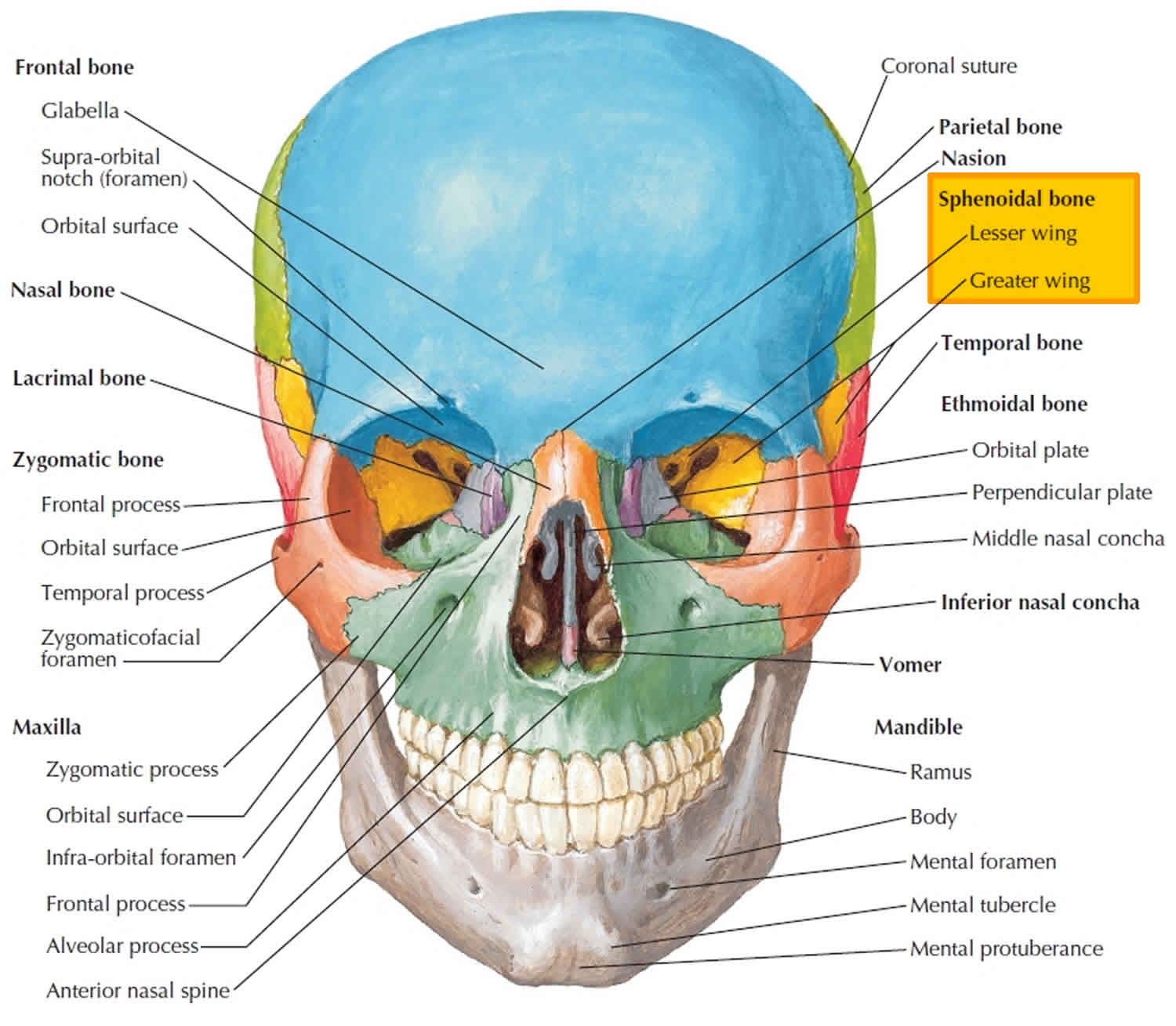
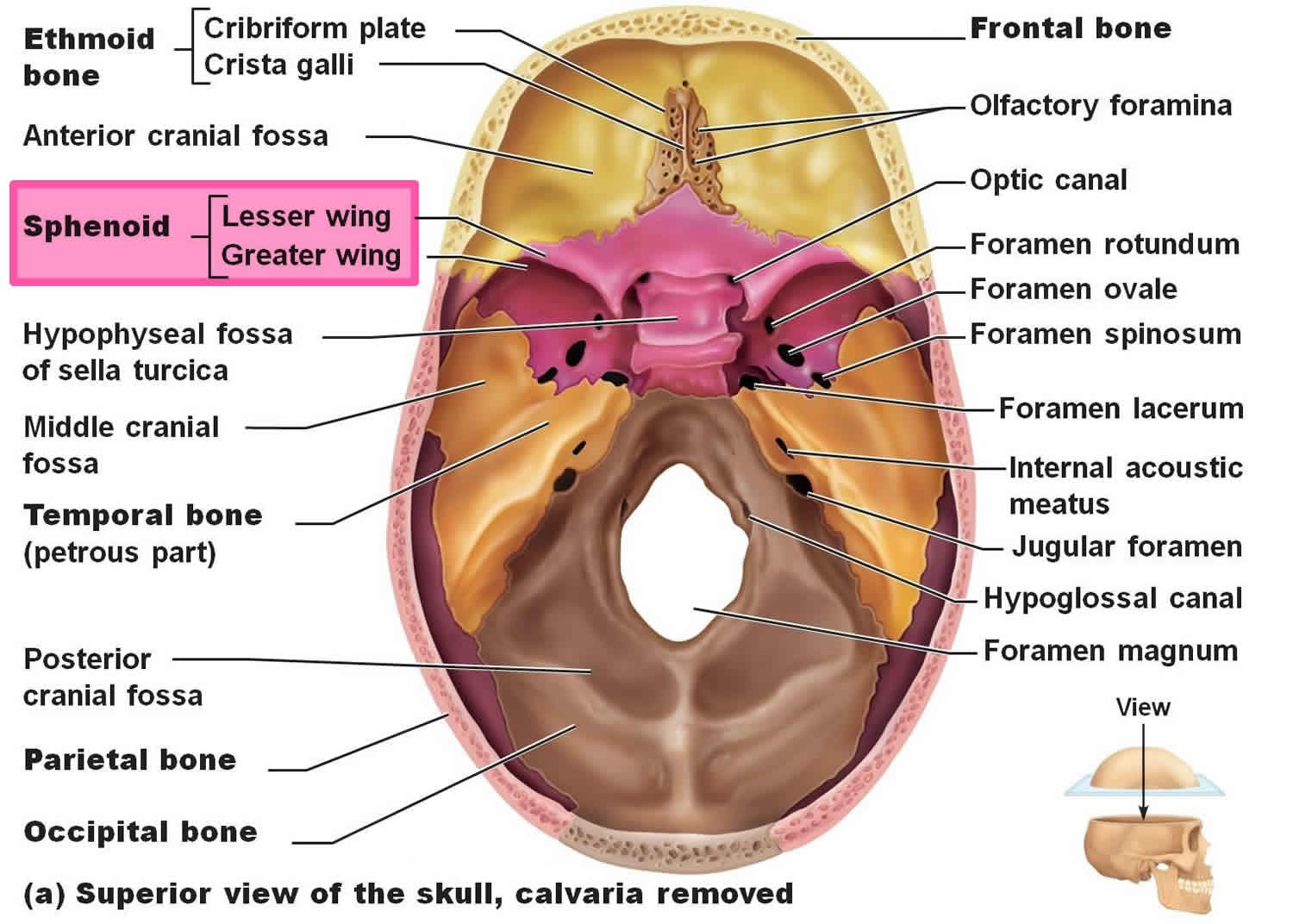
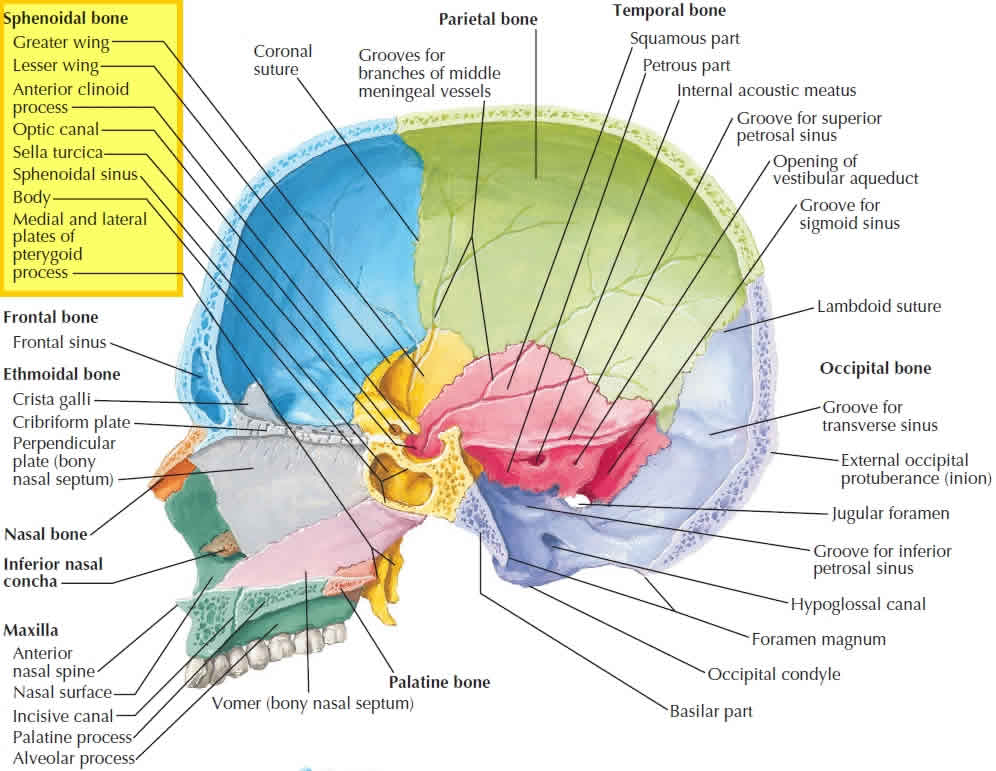
The sphenoid bone called wedge-shaped bone, lies at the middle part of the base of the skull. Sphenoid bone is called the keystone of the cranial floor because it articulates with all the other cranial bones, holding them together. View the floor of the cranium superiorly (Figure 1) and note the sphenoid articulations. The sphenoid bone joins anteriorly with the frontal and ethmoid bones, laterally with the temporal bones, and posteriorly with the occipital bone. The sphenoid lies posterior and slightly superior to the nasal cavity and forms part of the floor, side walls, and rear wall of the orbit (Figure 1).
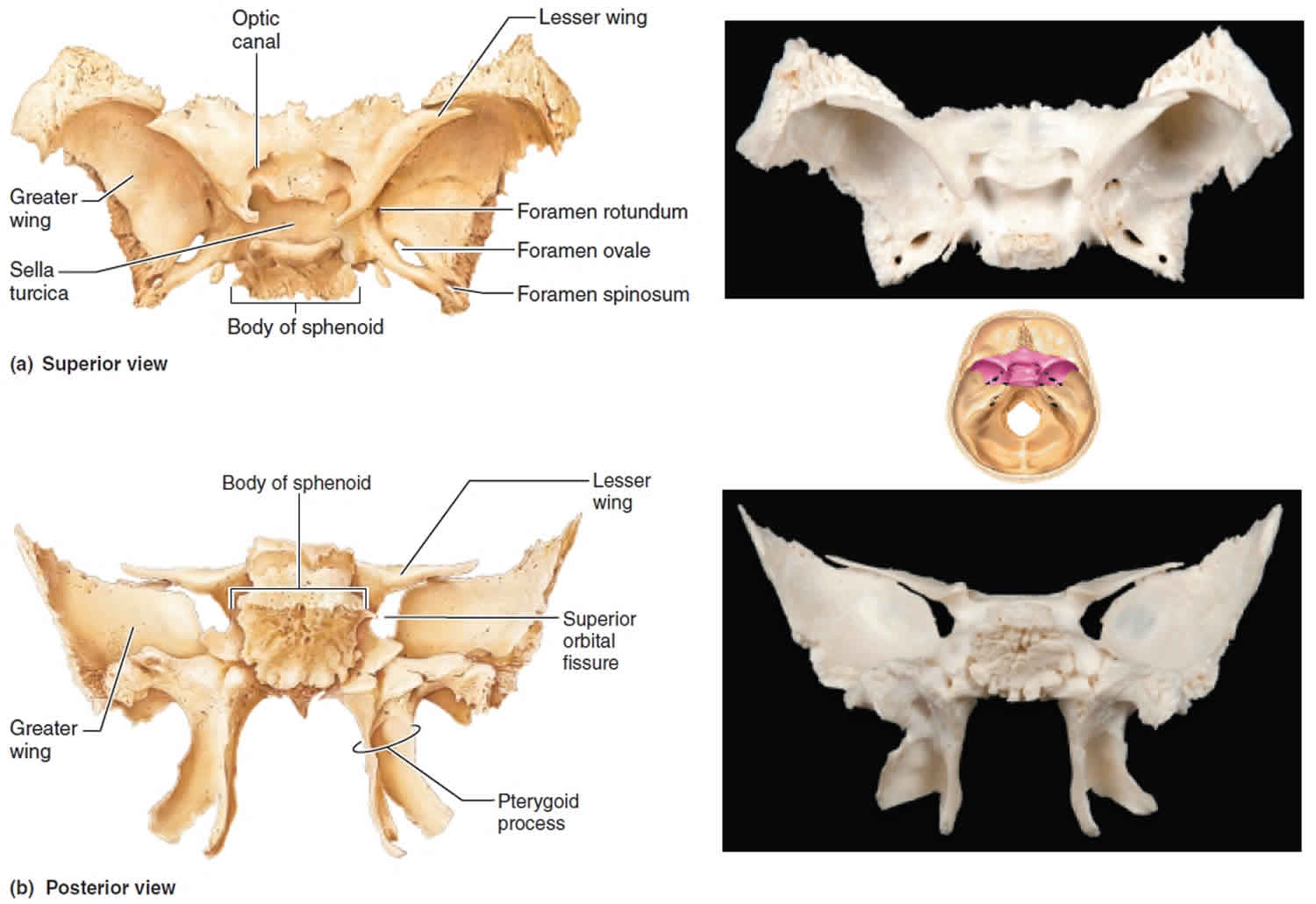
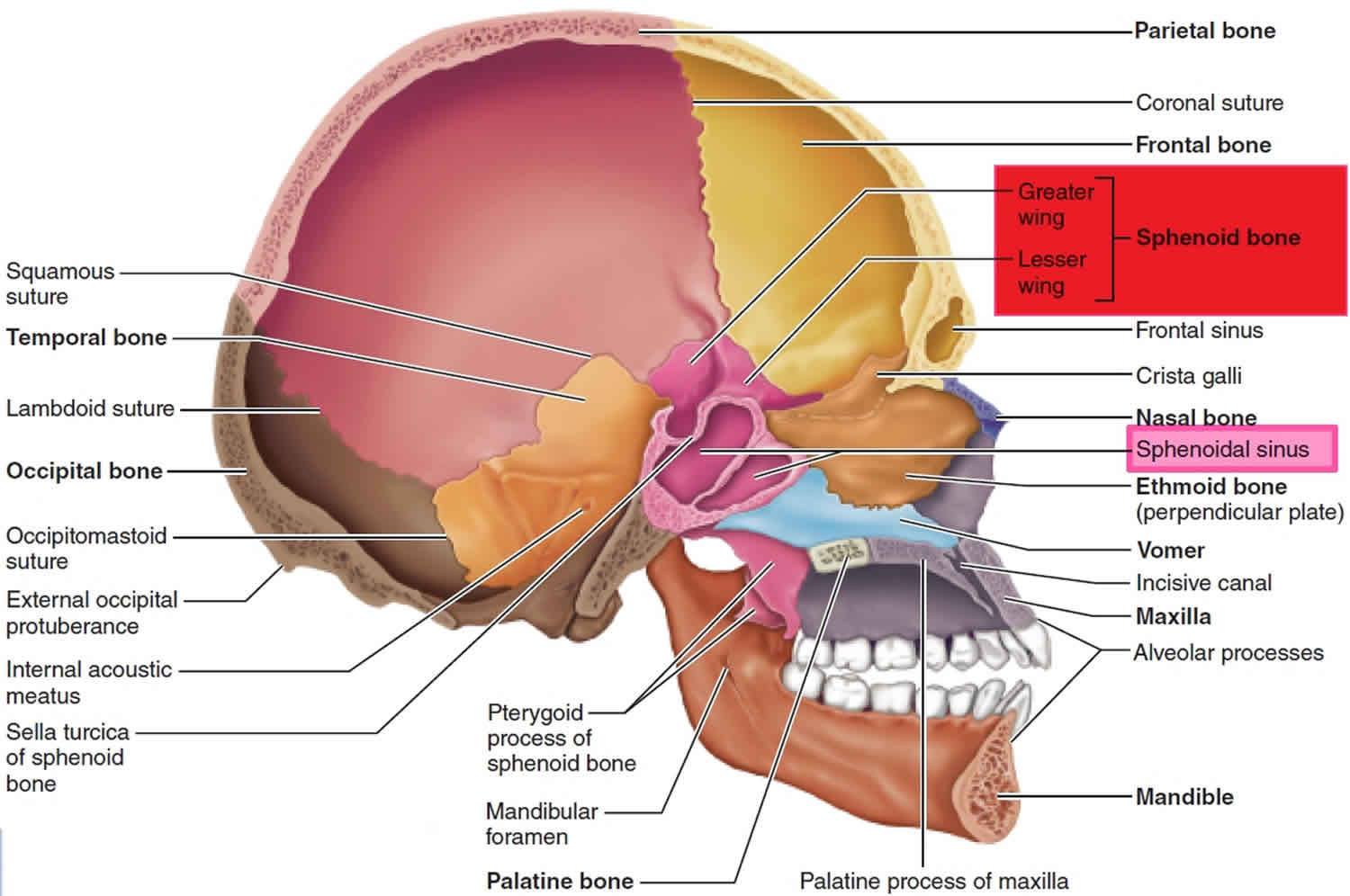
The shape of the sphenoid resembles a butterfly with outstretched wings (Figures 1 and 2). The body of the sphenoid is the hollowed cubelike medial portion between the ethmoid and occipital bones. The space inside the body is the sphenoidal sinus, which drains into the nasal cavity (see Figure 3). The sella turcica (sella = saddle; turcica = Turkish) is a bony saddle-shaped structure on the superior surface of the body of the sphenoid (Figure 1). The anterior part of the sella turcica, which forms the horn of the saddle, is a ridge called the tuberculum sellae. The seat of the saddle is a depression, the hypophyseal fossa, which contains the pituitary gland. The posterior part of the sella turcica, which forms the back of the saddle, is another ridge called the dorsum sellae.
The greater wings of the sphenoid project laterally from the body and form the anterolateral floor of the cranium. The greater wings also form part of the lateral wall of the skull just anterior to the temporal bone and can be viewed externally. The lesser wings, which are smaller, form a ridge of bone anterior and superior to the greater wings. They form part of the floor of the cranium and the posterior part of the orbit of the eye.
Between the body and lesser wing just anterior to the sella turcica is the optic foramen or canal (optic = eye), through which the optic (II) nerve and ophthalmic artery pass into the orbit. Lateral to the body between the greater and lesser wings is a triangular slit called the superior orbital fissure. This fissure may also be seen in the anterior view of the orbit in Figure 1. Blood vessels and cranial nerves pass through this fissure.
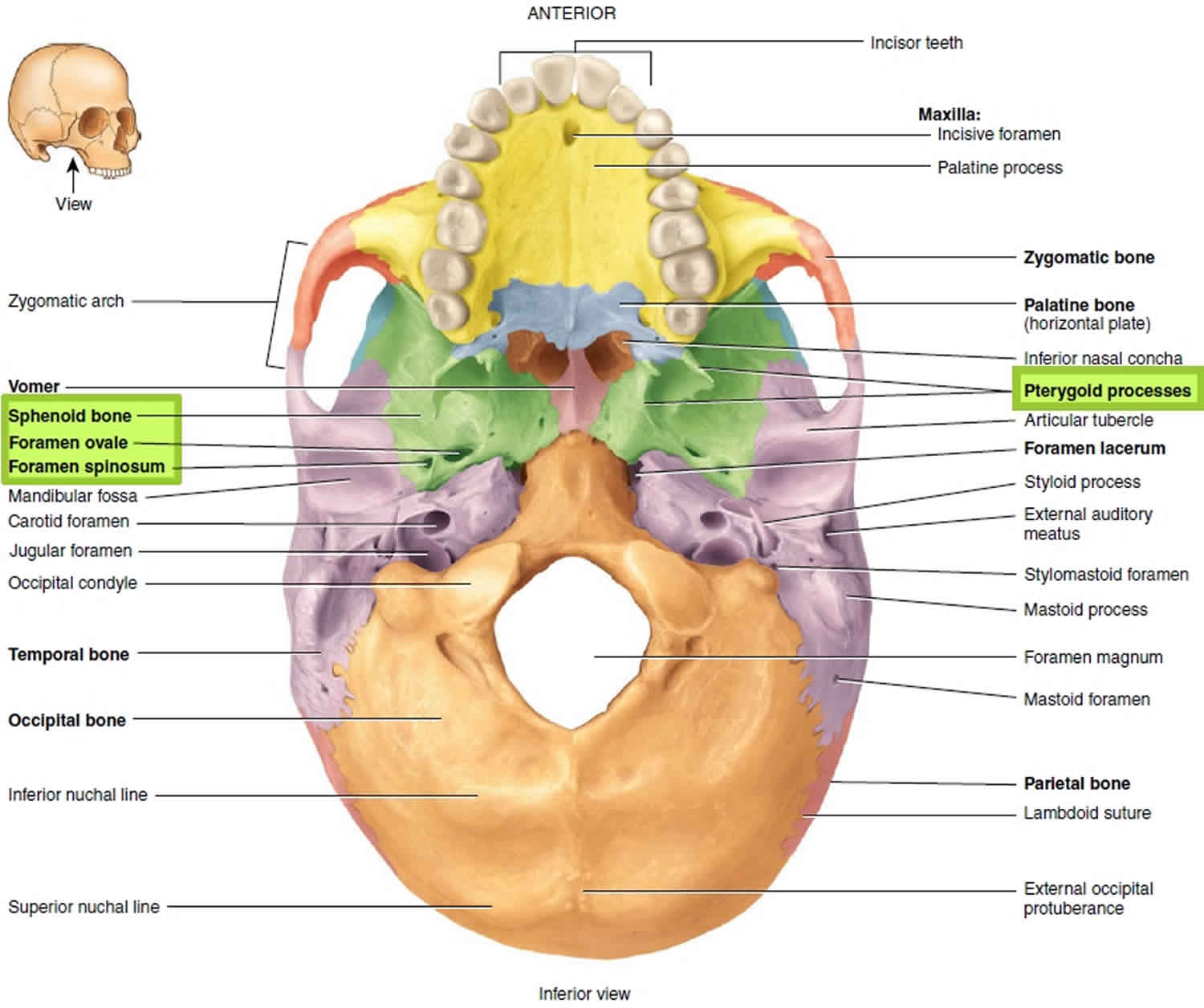
The pterygoid processes (winglike) project inferiorly from the points where the body and greater wings of the sphenoid bone unite; they form the lateral posterior region of the nasal cavity (see Figures 1 and 2). Some of the muscles that move the mandible attach to the pterygoid processes. At the base of the lateral pterygoid process in the greater wing is the foramen ovale (= oval hole). The foramen lacerum (= lacerated), covered in part by a layer of fibrocartilage in living subjects, is bounded anteriorly by the sphenoid bone and medially by the sphenoid and occipital bones. It transmits a branch of the ascending pharyngeal artery. Another foramen associated with the sphenoid bone is the foramen rotundum (= round hole) located at the junction of the anterior and medial parts of the sphenoid bone. The maxillary branch of the trigeminal (V) nerve passes through the foramen rotundum.
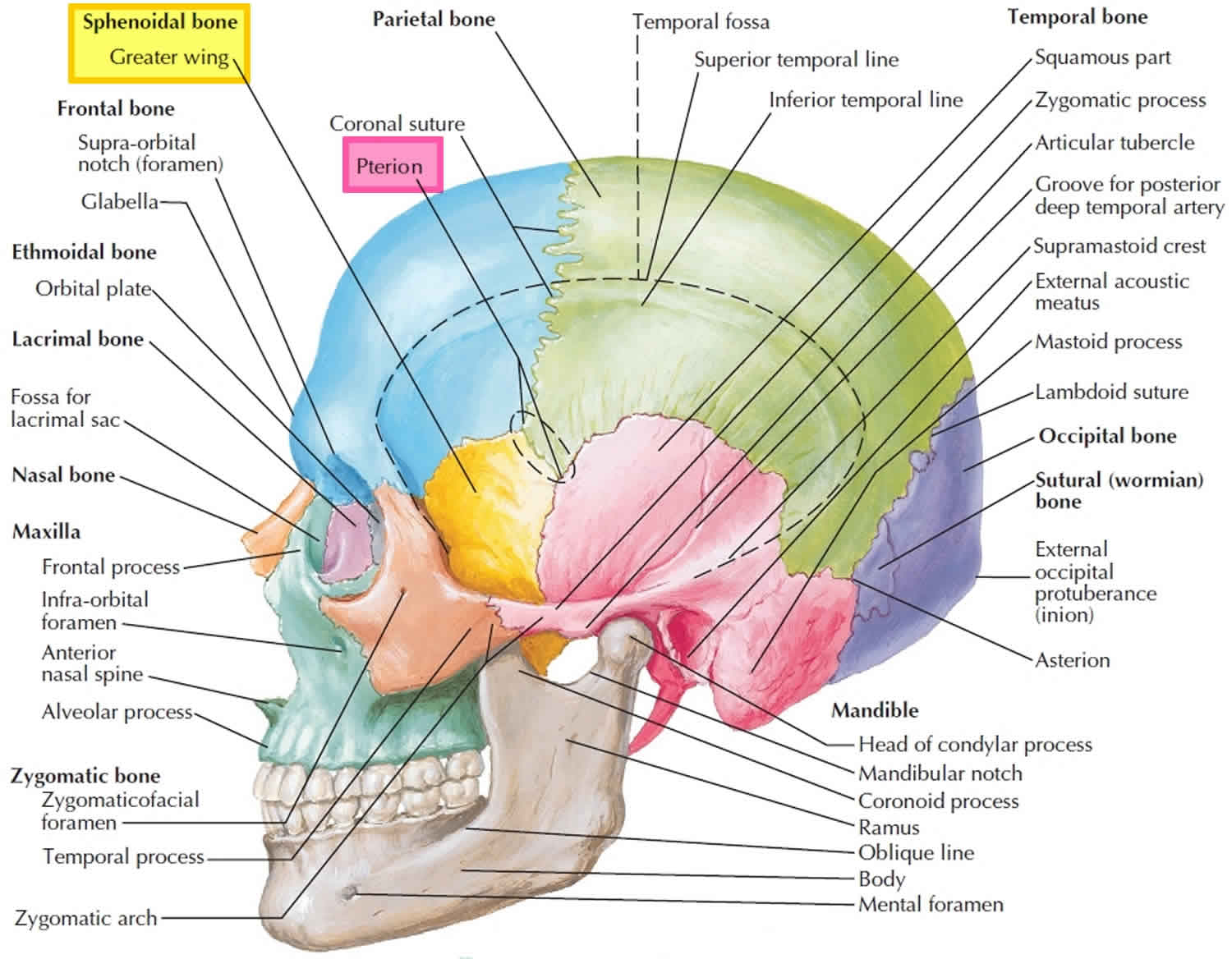
The pterion is an area on the lateral aspect of the frontal bone. This area is a joining of four cranial bones: frontal, temporal, sphenoid, and parietal. It is clinically significant because it overlies the middle meningeal artery, a large artery supplying the dura. A fracture or trauma to this area should receive a thorough assessment to determine any damage to this structure.
Sphenoid bone anatomy
The sphenoid bone spans the width of the cranial floor and has been said to resemble a bat with its wings spread. The sphenoid bone is considered the keystone of the cranium because it forms a central wedge that articulates with every other cranial bone. It is a challenging bone to study because of its complex shape and orientation: Portions of the sphenoid are viewable from most aspects of the skull. It also has a number of foramina for the passage of cranial nerves and vessels.
Parts of the sphenoid bone include:
- body
- greater wing
- lesser wing
- process and plates
Articulations
The sphenoid bone articulates with twelve bones. Unpaired bones include: frontal, ethmoid, vomer, and occipital. Paired bones include: zygomatic, parietal, temporal, and palatine.
Fissures, foramina, grooves and canals
The sphenoid bone includes:
- optic canal
- superior orbital fissure
- foramen rotundum
- pterygoid canal
- foramen ovale
- foramen spinosum
- carotid groove
The sphenoid bone consists of a central body and three pairs of processes: the greater wings, lesser wings, and pterygoid processes (Figures 1 to 3). The superior surface of the sphenoid body bears a saddle-shaped prominence, the sella turcica (“Turkish saddle”). The seat of this saddle, called the hypophyseal fossa, holds the pituitary gland, or hypophysis. Within the sphenoid body are the paired sphenoidal sinuses (Figure 3). The greater wings project laterally from the sphenoid body, forming parts of the middle cranial fossa (Figure 1) and the orbit. Externally, the greater wings form the lateral wall of the skull anterior to the squamous part of the temporal bones (Figure 1). The horn-shaped lesser wings form part of the floor of the anterior cranial fossa (Figures 1 and 2) and a part of the orbit. The trough-shaped pterygoid (“winglike”) processes project inferiorly from the greater wings. These processes, which have both medial and lateral plates, are attachment sites for the pterygoid muscles that help close the jaw in chewing.
The sphenoid bone has five important openings (Figure 1) on each side. The optic canal lies just anterior to the sella turcica. Cranial nerve 2, the optic nerve, passes through this hole from the orbit into the cranial cavity. The other four openings lie in a crescent-shaped row just lateral to the sphenoid body on each side. The most anterior of these openings, the superior orbital fissure, is a long slit between the greater and lesser wings (Figure 1). It transmits several structures to and from the orbit, such as the cranial nerves that control eye movements (III, IV, and VI). This fissure is best seen in an anterior view of the orbit (Figure 1). The foramen rotundum lies in the medial part of the greater wing. It is usually oval, despite its name, which means “round opening.” The foramen ovale is an oval hole posterolateral to the foramen rotundum. The foramen rotundum and foramen ovale are passageways through which two large branches of cranial nerve V (the maxillary and mandibular nerves) exit the cranium. Posterior and lateral to the foramen ovale lies the small foramen spinosum (spi-nosum), named for a short spine that projects from its margin on the inferior aspect of the skull. Through this foramen passes the middle meningeal artery, which supplies blood to the broad inner surfaces of the parietal bones and the squamous part of the temporal bones.
Figure 1. Sphenoid bone anatomy
Parts of sphenoid bone
Body of sphenoid
The body of the sphenoid bone is the midline cubical portion of the sphenoid bone, hollowed by the sphenoid air sinuses.
The body has superior, inferior, anterior, posterior, and lateral surfaces.
The superior surface features:
- ethmoidal spine: prominent spine that articulates with the cribriform plate and grooved on either side by olfactory lobes of brain
- chiasmatic groove (a.k.a. optic groove): optic chiasm lies above and behind
- optic canal: transmits optic nerve and ophthalmic artery
- tuberculum sellae: elevation anterior to sella turcica
- sella turcica: deep depression, pituitary fossa is deepest part
- middle clinoid processes: small prominences on anterior part of sella turcica
- dorsum sellae: plate of bone forming posterior boundary of sella turcica
- posterior clinoid processes: tubercles on superior angle of dorsum sellae
- petrosal process: articulates with petrous apex of the temporal bone
- clivus: shallow depression posterior to dorsum sellae
The inferior surface features:
- sphenoidal rostrum: continuous with sphenoidal crest
- vaginal process: projecting lamina on either side of rostrum, directed medially
The anterior surface features:
- sphenoidal crest: middle, vertical crest that articulates with perpendicular plate of ethmoid that contributes to nasal septum
- sphenoidal air sinus opening
- sphenoidal conchae
Articulations
The posterior surface joins the basilar part of the occipital bone.
The lateral surface unites with the greater wing and medial pterygoid plate. It features:
- carotid groove: broad groove that lodges internal carotid artery and cavernous sinus
- lingula: ridge of bone between body and greater wing
Figure 2. Parts of sphenoid bone
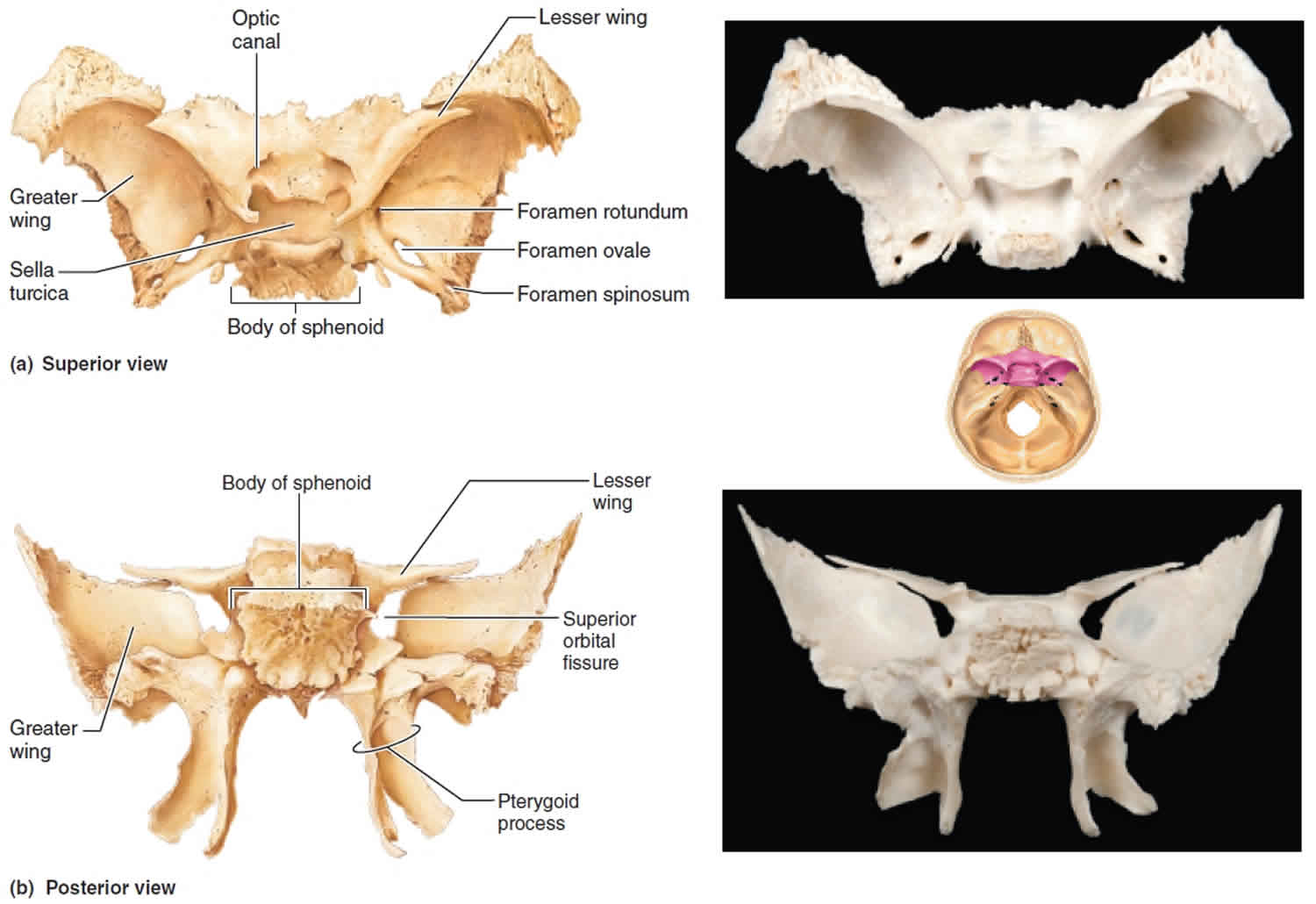
Figure 3. Sphenoid sinus
Greater wing of sphenoid
The greater wing or ali-sphenoid of the sphenoid bone is a process which projects from either side of the lower part of the sphenoid body, at a common junction with the pterygoid process. It is a paired structure, which curves upward, backward and laterally from each side of the sphenoid body, which can be likened to the extended wings of a bat. Both wings also have a triangular process projecting inferiorly which are known as the spine(s) of the sphenoid bone.
The greater wing of the sphenoid features superior, lateral and orbital surfaces.
The superior surface features:
- foramen rotundum: transmits the maxillary branch of the trigeminal nerve
- foramen ovale: transmits the mandibular division of the trigeminal nerve, accessory meningeal artery and (occasionally) the lesser petrosal nerve
- foramen spinosum: transmits the middle meningeal artery and meningeal branch of the mandibular nerve
- foramen Vesalii: variable presence, transmits small vein of cavernous sinus
The lateral surface features:
- infratemporal crest: a transverse ridge dividing the lateral surface in two parts
- temporal: forms part of the temporal fossa and provides attachment for the temporalis
- infratemporal: forms part of the infratemporal fossa and provides attachment for the pterygoideus externus
- spina angularis: serves as attachment for sphenomandibular ligament and the tensor veli palatini. Grooved by the chorda tympani.
The orbital surface features:
- inferior margin: forms postero-lateral boundary of the inferior orbital fissure
- medial margin:forms lower boundary of the superior orbital fissure.
- a tubercle at its centers serves as an attachment to the inferior head of the lateral rectus muscle.
- upper part of the margin is notched by the transmission of a recurrent branch of the lacrimal artery.
- lateral margin – articulates with the zygomatic bone
Articulations
The lateral margin of the greater wing articulates with petrous temporal bone.
The posterior most part of the greater wing projects as a triangular process, sitting within the angle of the junction between the squamous and petrous portions of the temporal bone.
The tip of the great wing articulates with the parietal bone at the pterion.
Variant anatomy
- sphenoidal emissary foramen (occasionally present) it is a small aperture medial to the foramen ovale, opposite the root of the pterygoid process; it opens below near the scaphoid fossa and transmits a small vein from the cavernous sinus
- foramen petrosum (occasionally present), a small opening between the foramen spinosum and foramen ovale, for transmission of the lesser petrosal nerve
- common variant of foramen spinosum where the meningeal artery passes through foramen ovale instead of foramen spinosum
Osseous development
The greater wings of the sphenoid are the only bony structures of the skull which undergo both intramembranous and endochondral ossification.
Surgical relevance
- lateral orbital decompression surgery for exophthalmos
- lateral orbital wall fracture repair 1
- emergent surgical relief of optic nerve compression
Lesser wing of sphenoid
The lesser wing of the sphenoid bone, or orbito-sphenoid, is a sharp, pointed triangular plate arising laterally from the upper anterior portion of the sphenoid body.
The lesser wing features both superior and inferior surfaces:
- the superior surface is flattened and is in contact with the frontal lobe of the brain
- the inferior surface forms the upper border of the superior orbital fissure
The lesser wing also features an anterior and posterior border:
- A serrated anterior border
- A posterior border which projects in to the sylvian fissure. Its medial end forms the anterior clinoid process which acts as an attachment for tentorium cerebelli
The optic foramen perforates the base of the lesser wing at its attachment to the body of the sphenoid. This transmits the optic nerve and ophthalmic artery, which traverse the lesser wing through the optic canal.
Articulations
The anterior border of the lesser wing articulates with the frontal bone.
Pterygoid processes
The pterygoid processes or pterygoid plates are paired posteroinferior projections of the sphenoid bone.
Each pterygoid process projects inferiorly from the junction of the body and greater wing of the sphenoid bone and bifurcates into a medial pterygoid plate and a lateral pterygoid plate. At the inferior tip of the medial pterygoid plate is the small hook-shaped process, the pterygoid hamulus.
Relations
The spaces separated the medial and lateral plate are pterygoid fissure inferiorly and pterygoid fossa posterosuperiorly. The lateral aspect of the lateral pterygoid plate forms the medial wall of the infratemporal fossa. The root of the pterygoid process forms the posterior wall of the pterygopalatine fossa. The anterior opening of the pterygoid canal also sits on the anterior aspect of the root of the pterygoid process.
The pterygoid hamulus has two important relations, related to its function:
- tensor veli palatini tendon passes immediately behind it
- superior attachment of the pterygomandibular raphe
Attachments
Musculotendinous
- lateral pterygoid muscle: the lower part of the lateral pterygoid is attached to the lateral aspect of the lateral pterygoid plate
- medial pterygoid muscle: medial aspect of the lateral pterygoid plate
- superior pharyngeal constrictor: inferior end of the medial pterygoid plate
Related pathology
Pterygoid plates are important in diagnosing midface fractures. In Le Fort classification of midface fracture, the involvement of pterygoid plates is necessary to confirm the diagnosis.
Sphenoid bone function
Sphenoid bone is called the keystone of the cranial floor because it articulates with all the other cranial bones, holding them together. The function of the skull is both structurally supportive and protective 2. It protects its inner contents: the cerebrum, cerebellum, brainstem, and orbits. Structurally, it supports the muscles of the face and scalp, providing an anchor for muscular and tendinous attachments. It also protects complexes of nerves and vessels that feed and innervate the brain, facial muscles, and skin 3.
Sphenoid bone location
The sphenoid bone called wedge-shaped bone, lies at the middle part of the base of the skull. Sphenoid bone is called the keystone of the cranial floor because it articulates with all the other cranial bones, holding them together. View the floor of the cranium superiorly (Figure 1) and note the sphenoid articulations. The sphenoid bone joins anteriorly with the frontal and ethmoid bones, laterally with the temporal bones, and posteriorly with the occipital bone. The sphenoid lies posterior and slightly superior to the nasal cavity and forms part of the floor, side walls, and rear wall of the orbit (Figure 1).
Sphenoid bone fracture
The skull can be divided into the calvarium and the skull base. The calvarium is made up of the frontal, parietal, occipital, and temporal bones. The skull base is composed of the sphenoid, palatine, and maxillary bones along with portions of the temporal and occipital bones.
Injuries most commonly associated with fractures of the sphenoid are orbital fractures and mid-face fractures which usually occur following high energy trauma 4. Fractures of the greater wing of the sphenoid are relatively uncommon and mostly associated with lateral orbital wall fractures along the broad spheno-zygomatic suture 5.
Basal skull fracture
Basal fractures involve any of the bones of the base of the skull. Basal fractures are more complicated due to underlying structures such as cranial nerves and sinuses which can lead to hearing loss, facial paralysis, or decreased sense of smell. They also can pose a risk for meningitis.
Basal skull fractures are usually managed conservatively unless there is persistent CSF (cerebrospinal fluid) leakage. A patient with a basal skull fracture should not have a nasogastric tube or nasal cannula. There is no evidence to support the role of prophylactic antibiotics in preventing meningitis, although, persistent CSF leak may increase the risk of meningitis.
Fractures of the skull base should be considered, especially in high impact motor vehicle accidents. The type of fracture and the impact that it has on the contents of the skull are determined by the location of the fracture and the mechanism of injury. However, the treatment management of the fracture is determined by the injury to the inner contents of the skull and their complications. Thin sliced CT has become an integral part of the diagnosis of subtle skull base fractures.
Examination should include:
- A trauma protocol with primary, secondary, and tertiary survey if major trauma suspected.
- Glasgow coma scale (GCS) to assess the level of alertness. GCS may be less accurate in younger age groups, and a modified score should be used.
- Examination of the head to palpate for a boggy swelling (may indicate an underlying fracture), a palpable fracture line, or lacerations. Head circumference should be measured if the fontanelle is open as an increasing head circumference can indicate intracranial bleeding or swelling.
- Ear, nose, and throat examination to look for signs of basal skull fracture including haemotympanum, cerebrospinal fluid (CSF) or bloody otorrhoea or rhinorrhoea, Battle sign (ecchymosis on the mastoid process), or raccoon eyes (periorbital ecchymosis). Ring sign can be used to assess for CSF rhinorrhoea/otorrhoea that is mixed with blood. When the fluid is dropped onto filter paper, the CSF separates as a ring around the blood (central blood with a clear ring around it). However, ring sign is not specific to CSF as blood mixed with water, saline, and other mucous also will produce a ring sign.
- Neurological and cranial nerve examination for signs of raised intracranial pressure including fundoscopy. Cranial nerve abnormalities such as visual defect, anosmia, hearing defect, facial numbness, or paralysis also can indicate a skull base fracture.
- Head to toe examination assessing for bruising or other injuries in case of other traumatic injuries, or if suspicious, of non-accidental injury.
Le Fort fractures
Le Fort fractures are fractures of the midface, which collectively involve separation of all or a portion of the midface from the skull base. In order to be separated from the skull base, the pterygoid plates of the sphenoid bone need to be involved as these connect the midface to the sphenoid bone dorsally. The Le Fort classification system attempts to distinguish according to the plane of injury.
Practical points
- fracture of the pterygoid plates is mandatory to diagnose Le Fort fractures
- if the anterolateral margins of the nasal fossa are intact it excludes a type I fracture
- if the zygomatic arch is intact it excludes a type III fracture
- if the infraorbital rims are intact it excludes a type III fracture
- if the nasofrontal suture is involved, then it is either a type II or III fracture
Le Fort fractures classification
The commonly used classification is as follows:
Le Fort type I
- horizontal maxillary fracture, separating the teeth from the upper face
- fracture line passes through the alveolar ridge, lateral nose and inferior wall of the maxillary sinus
Le Fort type II
- pyramidal fracture, with the teeth at the pyramid base, and nasofrontal suture at its apex
- fracture arch passes through the posterior alveolar ridge, lateral walls of maxillary sinuses, inferior orbital rim and nasal bones
- uppermost fracture line can pass through the nasofrontal junction or the frontal process of the maxilla 3
Le Fort type III
- craniofacial disjunction
- transverse fracture line passes through nasofrontal suture, maxillo-frontal suture, orbital wall, and zygomatic arch / zygomaticofrontal suture
- because of the involvement of the zygomatic arch, there is a risk of the temporalis muscle impingement
A memory aid is:
- Le Fort I is a floating palate (horizontal)
- Le Fort II is a floating maxilla (pyramidal)
- Le Fort III is a floating face (transverse)
Any combination is possible. For example, there may be type 2 on one side and contralateral type 3, or there may be unilateral type 1 and 2 fractures. It should be noted that Le Fort fractures are often associated with other facial fractures, neuromuscular injury and dental avulsions.
- Adel H. Alsuhaibani, Orbital Fracture: Significance of lateral wall, In Saudi Journal of Ophthalmology, Volume 24, Issue 2, 2010, Pages 49-55, ISSN 1319-4534[↩]
- Anderson BW, Al Kharazi KA. Anatomy, Head and Neck, Skull. [Updated 2019 Feb 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499834[↩]
- Kim SM, Paek SH, Lee JH. Infratemporal fossa approach: the modified zygomatico-transmandibular approach. Maxillofac Plast Reconstr Surg. 2018 Dec;41(1):3[↩]
- Cantini Ardila JE, Mendoza MÁ, Ortega VG. Sphenoid sinus and sphenoid bone fractures in patients with craniomaxillofacial trauma. Craniomaxillofacial trauma & reconstruction. 6 (3): 179-86.[↩]
- Alsuhaibani AH. Orbital Fracture: Significance of lateral wall. Saudi journal of ophthalmology: official journal of the Saudi Ophthalmological Society. 24 (2): 49-55[↩]



{kind=link}