What can cause “pimples” near vaginal area
Without looking at what people call “pimples” near the vaginal area, it’s very difficult to make any diagnosis.
To get started, lets learn about the female external genitalia.
The Female External Genitalia
The external genitalia occupy most of the perineum and are collectively called the vulva or pudendum; they include the mons pubis, labia majora and minora, clitoris, vaginal orifice, and accessory glands and erectile tissues (Figure 1).
The mons pubis consists mainly of an anterior mound of adipose (fatty) tissue overlying the pubic symphysis, bearing most of the pubic hair.
Labia Majora
From the mons pubis, two longitudinal folds of skin, the labia majora (labia = lips; majora = larger), extend inferiorly and posteriorly. The singular term is labium majus. The labia majora are covered by pubic hair and contain an abundance of adipose tissue, sebaceous (oil) glands, and apocrine sudoriferous (sweat) glands. They are homologous to the scrotum.
Labia Minora
Medial to the labia majora are two smaller folds of skin called the labia minora (minora = smaller). The singular term is labium minus. Unlike the labia majora, the labia minora are devoid of pubic hair and fat and have few sudoriferous glands, but they do contain many sebaceous glands which produce antimicrobial substances and provide some lubrication during sexual intercourse.
Clitoris
The clitoris is a small cylindrical mass composed of two small erectile bodies, the corpora cavernosa, and numerous nerves and blood vessels. The clitoris is located at the anterior junction of the labia minora. A layer of skin called the prepuce of the clitoris is formed at the point where the labia minora unite and covers the body of the clitoris. The exposed portion of the clitoris is the glans clitoris. The clitoris is homologous to the glans penis in males. The clitoris actually extends internally and is full of nerve endings- 15,000 of them- and the tip of the clitoris is usually the most sensitive area on the vulva and is the only organ on the entire body that’s sole purpose is sexual arousal.
The region between the labia minora is the vestibule. Within the vestibule are the hymen (if still present), the vaginal orifice, the external urethral orifice, and the openings of the ducts of several glands. The vaginal orifice, the opening of the vagina to the exterior, occupies the greater portion of the vestibule and is bordered by the hymen. Anterior to the vaginal orifice and posterior to the clitoris is the external urethral orifice, the opening of the urethra to the exterior. On either side of the external urethral orifice are the openings of the ducts of the paraurethral glands or Skene’s glands. These mucus-secreting glands are embedded in the wall of the urethra. On either side of the vaginal orifice itself are the greater vestibular glands or Bartholin’s glands, which open by ducts into a groove between the hymen and labia minora. They produce a small quantity of mucus during sexual arousal and intercourse that adds to cervical mucus and provides lubrication. The greater vestibular glands are homologous to the bulbourethral glands in males. Several lesser vestibular glands also open into the vestibule.
Figure 1. Female external genitalia
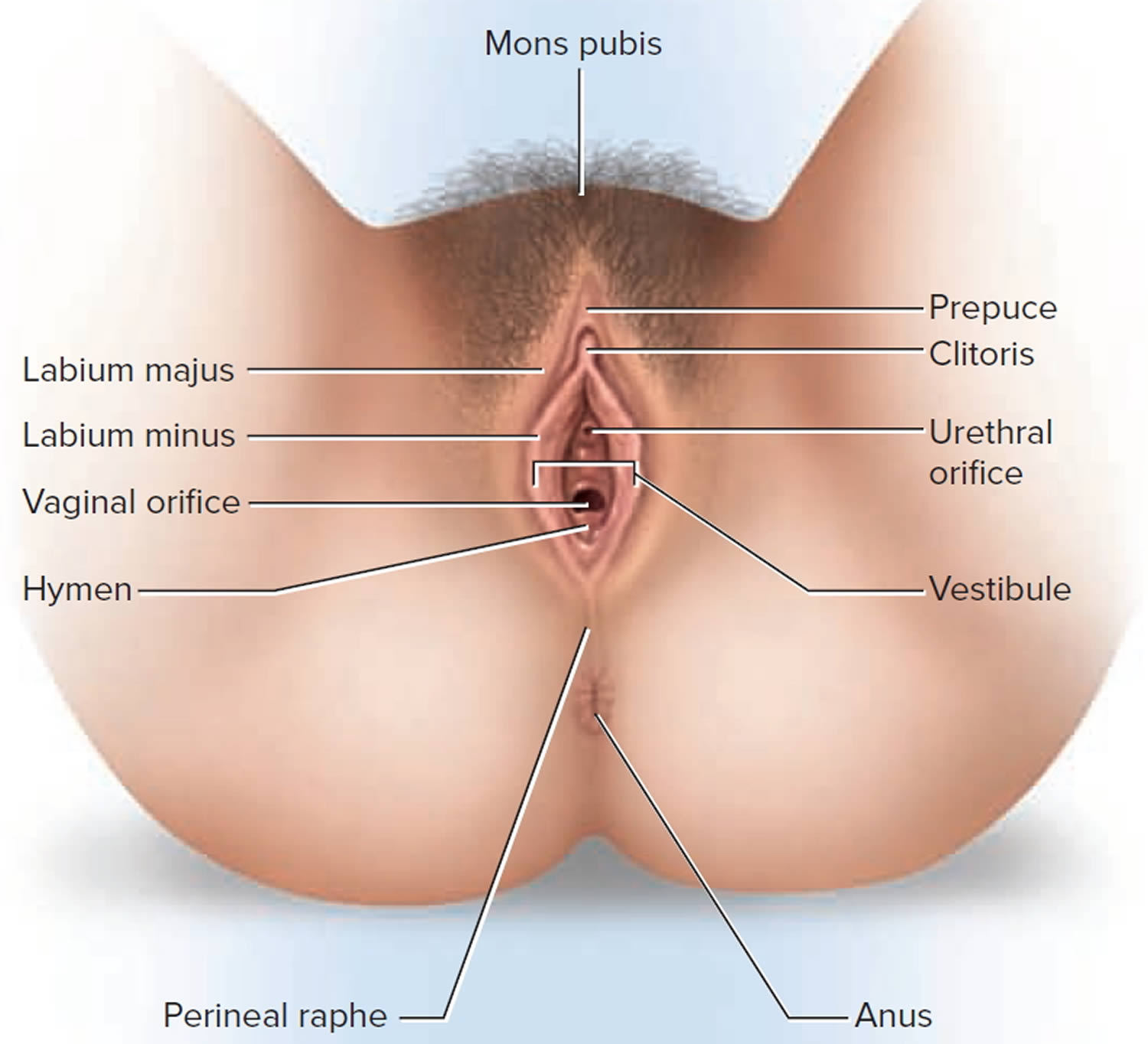
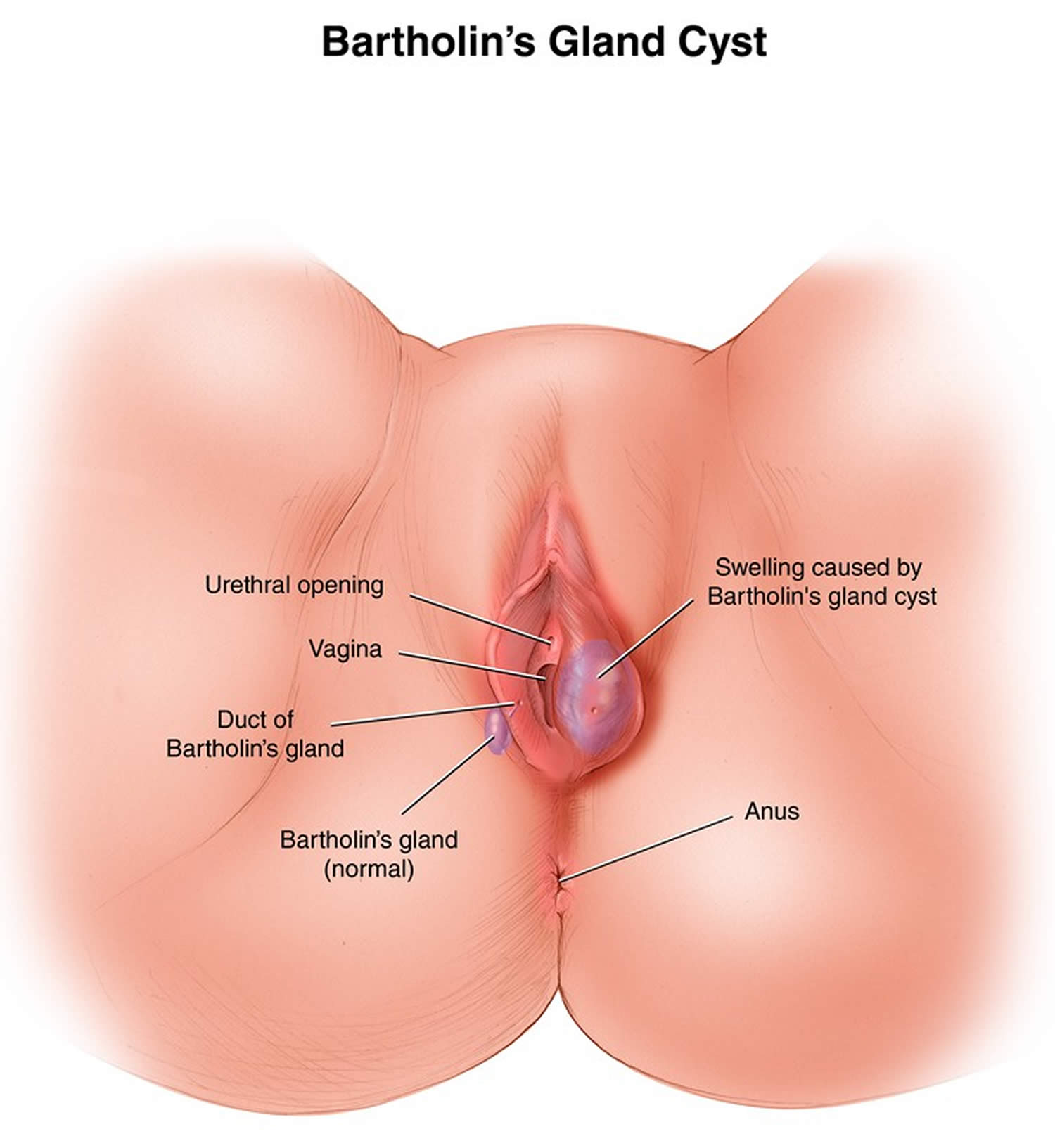
Figure 2. Bartholin’s glands and cyst
Vulval lumps and bumps
Genital skin problems are very common and can be very itchy or painful, distressing and embarrassing. They can interfere with sexual functioning, self-image and interpersonal relationships. Some genital disorders are contagious, including sexually transmitted diseases.
Proliferative lesions affecting the vulva may originate from skin, mucosa or underlying connective tissue.
Skin lesions are mainly typical of those found elsewhere on the body, and are found on the outer aspects of the vulva, the labia majora, extending to the groin. They include benign (harmless) and malignant (cancerous) tumours. They are often classified according to cell of origin.
Table 1. Causes of vulval lumps and bumps
| Lesion | Location | Characteristics |
|---|---|---|
| Cystic lesions | ||
| Bartholin’s duct cyst | Vestibule | Usually unilateral; asymptomatic if remains small |
| Epidermal inclusion cyst | Labia majora (usually) | Benign, mobile, nontender; caused by trauma or obstruction of pilosebaceous ducts |
| Mucous cyst of the vestibule | Labia minora, vestibule, periclitoral area | Soft, less than 2 cm in diameter, smooth surface, superficial location; solitary or multiple; usually asymptomatic |
| Hidradenoma papilliferum | Between labia majora and labia minora | Benign, slow-growing, small nodule (2 mm to 3 cm); arises from apocrine sweat glands |
| Cyst of the canal of Nuck | Labia majora, mons pubis | Soft, compressible; peritoneum entrapped within round ligament; may mimic inguinal hernia |
| Skene’s duct cyst | Adjacent to urethral meatus in vestibule | Benign, asymptomatic; if large, may cause urethral obstruction and urinary retention |
| Solid lesions | ||
| Fibroma | Labia majora, perineal body, introitus | Firm, asymptomatic; may develop pedicle; may undergo myxomatous degeneration; potential for malignancy |
| Lipoma | Labia majora, clitoris | Benign, slow-growing; sessile or pedunculated |
| Leiomyoma | Labia majora | Rare; solitary, firm; arises from smooth muscle |
| Acrochordon | Labia majora | Benign, fleshy, variable size; usually pedunculated but may be sessile; polypoid in appearance |
| Neurofibroma | Multicentric | Small, fleshy; polypoid in appearance; multiple; associated with von Recklinghausen’s disease |
| Angiokeratoma | Multicentric | Rare, benign; vascular; variable size and shape; single or multiple; associated with and aggravated by pregnancy; associated with Fabry’s disease |
| Squamous cell carcinoma | Multicentric | Related to benign epithelial disease in older women and to human papillomavirus infection in young women |
Bacterial infection
Bacterial skin infections include:
- Boils (deep infection of hair follicle)
- Folliculitis (surface infection of hair follicle)
- Impetigo (school sores)
- Erythrasma (dry brown patches)
- Cutaneous tuberculosis (rare)
- Bacterial vaginosis (cause of frothy discharge)
Fungal infections
Fungal skin infections include:
- Tinea cruris (Jock itch)
- Vulvovaginal candidiasis (thrush)
Viral infections
Viral skin infections include:
- Genital herpes, the commonest cause of recurrent blisters or sores
- Genital warts, the commonest cause of papules in this region
- Herpes zoster (shingles)
- Molluscum contagiosum.
Infestations
The groin is also a favoured site for some parasitic infestations:
- Pubic lice
- Scabies
- Schistosomiasis
- Amoebiasis
- Filariasis
- Leishmaniasis
Sexually transmitted infections
Important sexually transmitted infections (STIs) include:
- Syphilis
- Gonorrhoea
- Lymphogranuloma venereum
- Chancroid
- Granuloma inguinale (donovanosis)
- Trichomoniasis
Mucosal lesions occur in the inner aspects of the vulva, where the tissue is nonkeratinised (ie, not scaly).
- Fordyce spots
- Bartholin cyst
- Hidrocystadenoma papilliferum
- Vulval intraepithelial neoplasia (VIN)
- Squamous cell carcinoma
- Sebaceous adenitis
- Sebaceous carcinoma.
What is Folliculitis ?
Folliculitis is the name given to a group of skin conditions in which there are inflamed hair follicles. The result is a tender red spot, often with a surface pustule.
Folliculitis may be superficial or deep. It can affect anywhere there are hairs, including chest, back, buttocks, arms and legs. Acne and its variants are also types of folliculitis.
Figure 3. Folliculitis

What causes folliculitis ?
Folliculitis can be due to infection, occlusion (blockage), irritation and various skin diseases.
Folliculitis due to infection
To determine if folliculitis is due to an infection, swabs should be taken from the pustules for cytology and culture in the laboratory.
Bacteria
Bacterial folliculitis is commonly due to Staphylococcus aureus. If the infection involves the deep part of the follicle, it results in a painful boil. Recommended treatment includes careful hygiene, antiseptic cleanser or cream, antibiotic ointment, and/or oral antibiotics.
Spa pool folliculitis is due to infection with Pseudomonas aeruginosa, which thrives in inadequately chlorinated warm water. Gram negative folliculitis is a pustular facial eruption also due to infection with Pseudomonas aeruginosa or other similar organisms. When it appears, it usually follows tetracycline treatment of acne, but is quite rare.
Yeasts
The most common yeast to cause a folliculitis is Pityrosporum ovale, also known as Malassezia. Malassezia folliculitis (Pityrosporum folliculitis) is an itchy acne-like condition usually affecting the upper trunk of a young adult. Treatment includes avoiding moisturisers, stopping any antibiotics and topical antifungal or oral antifungal medication for several weeks.
Candida albicans can also provoke a folliculitis in skin folds (intertrigo) or in the beard area. It is treated with topical or oral antifungal agents.
Fungi
Ringworm of the scalp (tinea capitis) usually results in scaling and hair loss, but sometimes results in folliculitis. In New Zealand, cat ringworm (Microsporum canis) is the commonest organism causing scalp fungal infection. Other fungi such as Trichophyton tonsurans are increasingly reported. Treatment is with oral antifungal agents for several months.
Viral infections
Folliculitis may caused by herpes simplex virus. This tends to be tender, and resolves without treatment in around 10 days. Severe recurrent attacks may be treated with aciclovir and other antiviral agents.
Herpes zoster (the cause of shingles) may also present as folliculitis with painful pustules and crusted spots within a dermatome (an area of skin supplied by a single nerve). It is treated with hihg-dose aciclovir.
Molluscum contagiosum, common in young children, may also cause follicular umbilicated papules, usually clustered in and around a body fold. Molluscum may provoke dermatitis.
Parasitic infection
Folliculitis on the face or scalp of older or immunosuppressed adults may be due to colonisation by hair follicle mites (demodex). This is known as demodicosis.
The human infestation, scabies, often provokes folliculitis, as well as non-follicular papules, vesicles and pustules.
Folliculitis due to irritation from regrowing hairs
Folliculitis may arise as hairs regrow after shaving, waxing, electrolysis or plucking. Swabs taken from the pustules are sterile ie there is no growth of bacteria or other organisms. In the beard area irritant folliculitis is known as pseudofolliculitis barbae.
Irritant folliculitis is also common on the lower legs of women (shaving rash). It is frequently very itchy. Treatment is by stopping hair removal, and not beginning again for about three months after the folliculitis has settled. To prevent reoccurring irritant folliculitis, use a gentle hair removal method, such as a lady’s electric razor. Avoid soap and apply plenty of shaving gel, if using a blade shaver.
Folliculitis due to contact reactions
Occlusion
Paraffin-based ointments, moisturisers, and adhesive plasters may all result in a sterile folliculitis. If a moisturiser is needed, choose an oil-free product, as it is less likely to cause occlusion.
Chemicals
Coal tar, cutting oils and other chemicals may cause an irritant folliculitis. Avoid contact with the causative product.
Topical steroids
Overuse of topical steroids may produce a folliculitis. Perioral dermatitis is a facial folliculitis provoked by moisturisers and topical steroids. Perioral dermatitis is treated with tetracycline antibiotics for six weeks or so.
Folliculitis due to immunosuppression
Eosinophilic folliculitis is a specific type of folliculitis that may arise in some immune suppressed individuals such as those infected by human immunodeficiency virus (HIV) or those who have cancer.
Folliculitis due to drugs
Folliculitis may be due to drugs, particularly corticosteroids (steroid acne), androgens (male hormones), ACTH, lithium, isoniazid (INH), phenytoin and B-complex vitamins. Protein kinase inhibitors (epidermal growth factor receptor inhibitors) and targeted therapy for metastatic melanoma (vemurafenib, dabrafenib) nearly always result in folliculitis.
Folliculitis due to inflammatory skin diseases
Certain uncommon inflammatory skin diseases may cause permanent hair loss and scarring because of deep seated sterile folliculitis. These include:
- Lichen planus
- Discoid lupus erythematosus
- Folliculitis decalvans
- Folliculitis keloidalis
Treatment depends on the underlying condition and its severity. A skin biopsy is often necessary to establish the diagnosis.
Acne variants
Acne and acne-like or acneform disorders are also forms of folliculitis. These include:
- Acne vulgaris
- Nodulocystic acne
- Rosacea
- Scalp folliculitis
- Chloracne
The follicular occlusion syndrome refers to:
- Hidradenitis suppurativa (acne inversa)
- Acne conglobata (a severe form of nodulocystic acne)
- Dissecting cellulitis (perifolliculitis capitis abscedens et suffodiens)
- Pilonidal sinus.
Treatment of the acne variants may include topical therapy as well as long courses of tetracycline antibiotics, isotretinoin (vitamin-A derivative) and in women, antiandrogenic therapy.
What are boils ?
Boils (also called furuncles) are a deep bacterial infection of hair follicles.
What are the clinical features of boils ?
Boils present as one or more tender red spots, lumps or pustules. Careful inspection reveals that the boil is centred on a hair follicle. A boil is a deep form of bacterial folliculitis; superficial folliculitis is sometimes present at the same time. Staphylococcus aureus can be cultured from the skin lesions.
If there are multiple heads, the lesion is called a “carbuncle”. Large boils form abscesses, defined as an accumulation of pus within a cavity. Cellulitis may also occur, i.e. infection of the surrounding tissues, and this may cause fever and illness.
Figure 4. Boil

Why do boils occur ?
Most people with boils are otherwise healthy and have good personal hygiene. They do however carry Staphylococcus aureus on the surface of their skins (staphylococcal carrier state). Why this occurs is usually not known, but it is estimated that 10–20% of the population are staphylococcal carriers.
Staphylococcus aureus is most commonly carried in the nostrils, armpits, between the legs and in the cleft between the buttocks. It may be transferred to other sites from the nostrils via the finger nails.
Tiny nicks or grazes or something rubbing against the skin can innoculate the bacteria into the wall of a hair follicle which is a weak point in the skin’s defences. Once innoculated, the bacteria cause a boil which goes on to run its usual course of about 10 days.
Although most people with boils are otherwise healthy, boils are sometimes related to immune deficiency, anaemia, diabetes, smoking or iron deficiency.
What is the treatment for boils ?
Medical treatment of boils
Treatment of boils depends on their severity. Your doctor may give you specific advice and medical treatment, some are listed below:
- Antiseptic or antibacterial soap in your daily bath or shower for a week then twice weekly for several weeks. The cleanser may cause a little dryness.
- Use a hand sanitiser regularly to reduce the chance of reinfecting yourself or others with contaminated hands.
- Antiseptic or antibiotic ointment or gel to apply to the inside of the nostrils.
- Wipe the entire skin surface daily for a week with 70% isopropyl alcohol in water (this will make the skin dry).
- Apply a topical antiseptic such as povidone iodine or chlorhexidine cream to the boils and cover with a square of gauze.
- Your doctor may prescribe an oral antibiotic (usually the penicillin antibiotic flucloxacillin), sometimes for several weeks.
- Other members of the family with boils should also follow a skin cleansing regime. Your doctor may also advise the family to apply topical antibiotic to their nostrils in case they are Staphylococcus aureus carriers as well.
- If the boils fail to clear up, a swab should be taken for microbiological culture, in case of methicillin (meticillin) resistant staphylococci.
- Sometimes, special antibiotics may be prescribed on the recommendation of a specialist, including fusidic acid, clindamycin, rifampicin and cephalosporins.
General measures to prevent boils
- Consult your doctor about your general health.
- If you are overweight, try to reduce your weight; take regular exercise.
- Follow a balanced healthy diet with meat, plenty of fruit and vegetables.
- Avoid smoking.
- Wash your whole body once a day with soap or cleanser and water. Wash your hands several times daily or use antiseptic hand rubs.
- Don’t share your flannel or towel with other family members.
- Maintain a clean handkerchief and don’t pick your nose!
- Change your underclothes and night attire regularly.
- Consider modifying leisure activities that cause sweating and friction from clothing, such as squash and jogging.
- If you are iron deficient, a course of iron tablets may help reduce infection.
- 1000 mg of vitamin C each day has also been advocated to improve deficient neutrophil function.
What is sebaceous adenitis ?
Sebeceous adenitis is a skin disease in which there is inflammation of the sebaceous glands (found on histopathological examination of the affected skin).
Sebaceous adenitis has rarely been described on the face in males and females and on the vulva of women. It has been more commonly described in dogs, which present with quite different symptoms – dandruff and hair loss.
What are sebaceous glands ?
Sebaceous glands secrete sebum, an oily substance, to lubricate the skin and hair. This helps waterproof the skin and protect it from drying out and from infection. The greatest number of sebaceous glands is found on the scalp and face. There are none on the palms and soles. Sebaceous glands are most active before birth and after puberty, continuing to excrete sebum until menopause in women and throughout adult life in men.
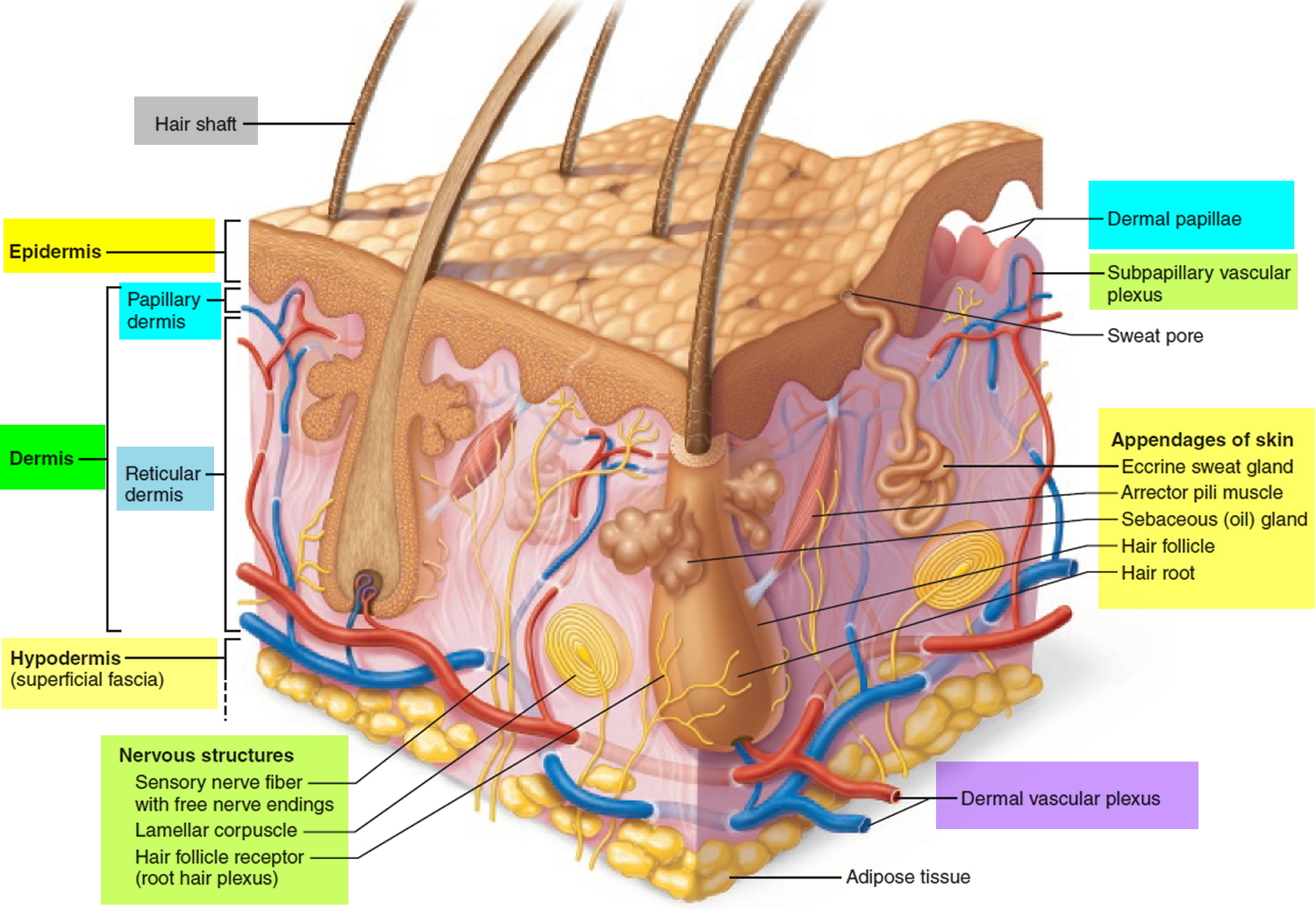
Sebaceous glands usually drain into the hair follicle. Sebaceous glands in hairless skin (e.g eyelids, lips, nipples, penis and vulva) drain directly onto the skin surface.
Figure 5. Skin
What causes sebaceous adenitis ?
The exact cause of sebaceous adenitis is not known. The following may play a role in its development:
- Sun exposure (facial rash)
- Hormones (females with vulval lesions)
- Innate immune system (non-allergic inflammation)
Infection has not been shown to cause sebaceous adenitis.
What are the signs and symptoms of sebaceous adenitis ?
Facial sebaceous adenitis
Facial sebaceous adenitis has been described as an asymptomatic, recurrent, erythematous (red), annular (ring-shaped) rash affecting males and females.
Vulval sebaceous adenitis
Vulval sebaceous adenitis is characterised by recurrent tender papules (a small pimple or bump on the skin) or nodules (small lumps) on the mucosal aspect of the labia minora – these are the hairless inner lips of the vulva of women. Pus may be expressed from the papules. Sebaceous adenitis occurs after puberty and lesions may recur for years.
How is sebaceous adenitis diagnosed ?
The diagnosis may be suspected clinically in a typical case with negative culture of bacterial and viral swabs. Vulval sebaceous adenitis should be distinguished from hidradenitis suppurativa (on hair-bearing skin), inflamed Bartholin cyst and genital Crohn disease.
Biopsy of a papule shows an inflammatory infiltrate around and within sebaceous glands. There may be focal necrosis (death) of sebocytes (the cells that produce sebum).
What is the treatment for sebaceous adenitis ?
As the disorder has rarely been described, the best treatment is uncertain. Sebaceous adenitis may recur when treatment is stopped. The following treatments have used in reported cases.
Vulval sebaceous adenitis
- Hormonal treatment using spironolactone and/or ethinyl oestrodiol/cyproterone acetate
- Topical antibiotics eg clindamycin
- Oral antibiotics eg doxycycline
What is Bartholin’s Duct Cyst and Gland Abscess ?
Bartholin’s glands (greater vestibular glands) are located bilaterally at the posterior introitus and drain through ducts that empty into the vestibule at approximately the 4 o’clock and 8 o’clock positions (see Figure 2). At puberty, these glands begin to function, providing moisture for the vestibule.
The Bartholin’s glands develop from buds in the epithelium of the posterior area of the vestibule. The glands are located bilaterally at the base of the labia minora and drain through 2- to 2.5-cm–long ducts that empty into the vestibule at about the 4 o’clock and 8 o’clock positions (Figure 2). The glands are usually the size of a pea and rarely exceed 1 cm. They are not palpable except in the presence of disease or infection.
Bartholin’s duct cysts, the most common cystic growths in the vulva 2, occur in the labia majora 3. Two percent of women develop a Bartholin’s duct cyst or gland abscess at some time in life. Abscesses are almost three times more common than cysts. One case-control study 4 found that white and black women were more likely to develop Bartholin’s cysts or abscesses than Hispanic women, and that women of high parity were at lowest risk.
Gradual involution of the Bartholin’s glands can occur by the time a woman reaches 30 years of age 5. This may account for the more frequent occurrence of Bartholin’s duct cysts and gland abscesses during the reproductive years, especially between 20 and 29 years of age.
Because a vulvar mass in a postmenopausal woman can be cancer, excisional biopsy may be required. Some investigators 6 have suggested that surgical excision is unnecessary because of the low risk of Bartholin’s gland cancer (0.114 cancers per 100,000 woman-years). However, if the diagnosis of cancer is delayed, the prognosis can be poor.
Causes of Bartholin’s Duct Cyst and Gland Abscess
Obstruction of the distal Bartholin’s duct may result in the retention of secretions, with resultant dilation of the duct and formation of a cyst. The cyst may become infected, and an abscess may develop in the gland. A Bartholin’s duct cyst does not necessarily have to be present before a gland abscess develops 7.
Bartholin’s gland abscesses are polymicrobial 8. Although Neisseria gonorrhoeae (a sexually transmitted infection – gonorrhea) is the predominant aerobic isolate, anaerobes are the most common pathogens 9. Chlamydia trachomatis (a sexually transmitted infection – chlamydia) also may be a causative organism 10. However, Bartholin’s duct cysts and gland abscesses are no longer considered to be exclusively the result of sexually transmitted infections 11. Vulvovaginal surgery is an uncommon cause of these cysts and abscesses 12.
Table 2. Bacteria isolated from Bartholin’s Gland Abscesses
| Aerobic organisms | Anaerobic organisms |
|---|---|
| Neisseria gonorrhoeae | Bacteroides fragilis |
| Staphylococcus aureus | Clostridium perfringens |
| Streptococcus faecalis | Peptostreptococcus species |
| Escherichia coli | Fusobacterium species |
| Pseudomonas aeruginosa | - |
| Chlamydia trachomatis | - |
Treatment of a Bartholin’s duct cyst and gland abscess
The treatment of a Bartholin’s duct cyst depends on the patient’s symptoms. An asymptomatic cyst may require no treatment 13, but symptomatic Bartholin’s duct cysts and gland abscesses require drainage. Unless spontaneous rupture occurs, an abscess rarely resolves on its own.
Although incision and drainage is a relatively quick and easy procedure that provides almost immediate relief to the patient, this approach should be discouraged because there is a tendency for the cyst or abscess to recur 14. One investigator 15 reported a 13 percent failure rate for the procedure. Furthermore, incision and drainage may make later Word catheter placement or marsupialization difficult 16.
Definitive drainage involves Word catheter placement for Bartholin’s duct cysts and gland abscesses, and marsupialization for duct cysts.
Word Catheter
A Word catheter is commonly used to treat Bartholin’s duct cysts and gland abscesses 17. The stem of this rubber catheter is 1 inch long and the diameter of a no. 10 French Foley catheter. The small, inflatable balloon tip of the Word catheter can hold about 3 mL of saline.
If a Bartholin’s cyst or abscess is too deep, Word catheter placement is impractical, and other options must be considered.10
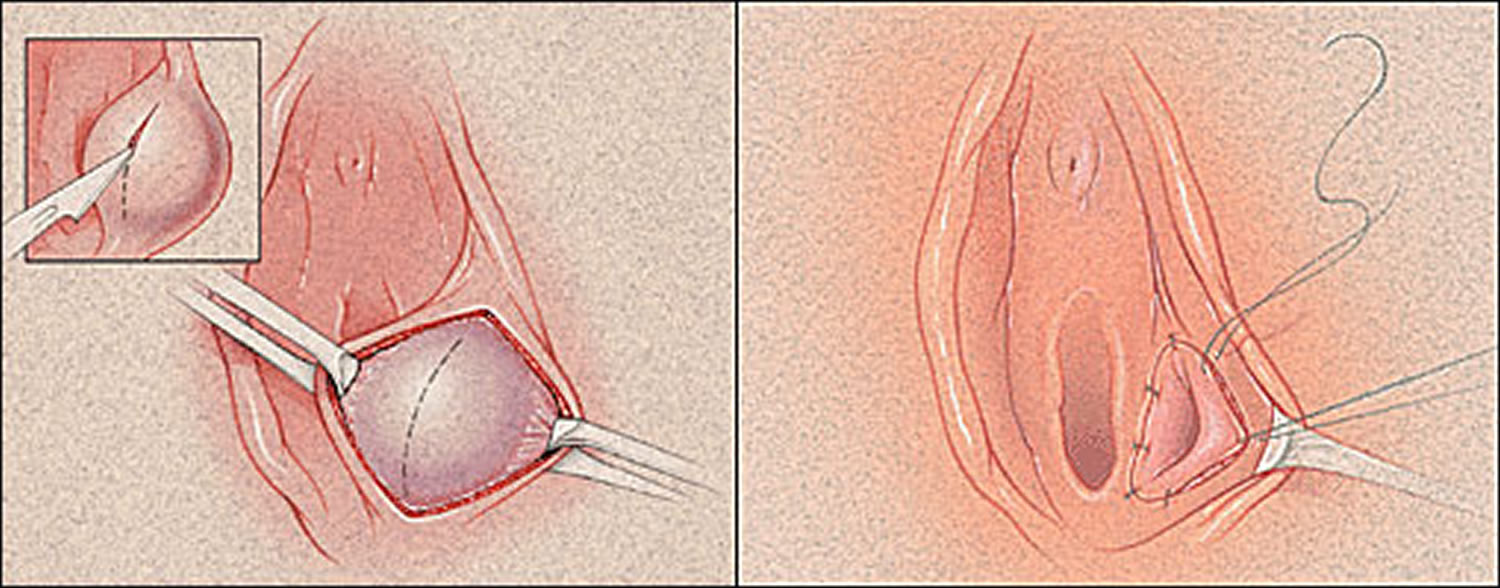
Marsupialization
An alternative to Word catheter placement is marsupialization of a Bartholin’s cyst. This procedure should not be used when an abscess is present 7. Marsupialization can be performed in the office or if the cyst is deeply seated, in an outpatient surgical suite.
After the cyst is vertically excised, the cavity drains spontaneously. The cavity also may be irrigated with saline solution and, if necessary, loculations can be broken up with a hemostat. The cyst wall is then everted and approximated to the edge of the vestibular mucosa with interrupted 2-0 absorbable suture 18. Daily sitz baths should begin on the first postoperative day.
Approximately 5 to 15 percent of Bartholin’s duct cysts recur after marsupialization.18 Complications associated with the procedure include dyspareunia, hematoma, and infection 14.
Figure 6. Marsupialization of Bartholins duct cyst
Excision
Although Bartholin’s gland abscesses may rupture and drain spontaneously, recurrence is likely, and surgical excision may be necessary. Excision is not an office-based procedure.
Cultures for N. gonorrhoeae and C. trachomatis may be obtained. However, Bartholin’s gland abscesses tend to be polymicrobial, and empiric broad-spectrum antibiotic therapy should be used.
Excision of the Bartholin’s gland should be considered in patients who do not respond to conservative attempts to create a drainage tract, but the procedure should be performed when there is no active infection 14. If multiple attempts have been made to drain a cyst or an abscess, adhesions may be present, making excision difficult and resulting in postoperative scarring and chronic pain in the area 13.
Some investigators 13, 7 recommend excision of the Bartholin’s gland to exclude adenocarcinoma when cysts or abscesses occur in patients more than 40 years of age. Even though adenocarcinoma of the Bartholin’s gland is rare, gynecologic oncology referral should be considered for older patients with Bartholin’s duct cysts or gland abscesses.
References- Management of Bartholin’s Duct Cyst and Gland Abscess. Am Fam Physician. 2003 Jul 1;68(1):135-140. http://www.aafp.org/afp/2003/0701/p135.html
- Kovar WR, Scott JC Jr. A practical, inexpensive office management of Bartholin’s cyst and abscess. Nebr Med J. 1983;68:254–5.
- Kaufman RH. Benign diseases of the vulva and vagina. 4th ed. St Louis: Mosby, 1994:168–248.
- Aghajanian A, Bernstein L, Grimes DA. Bartholin’s duct abscess and cyst: a case-control study. South Med J. 1994;87:26–9.
- Stillman FH, Muto MG. The vulva. In: Ryan KJ, Berkowitz RS, Barbieri RL, eds. Kistner’s Gynecology: principles and practice. 6th ed. St. Louis: Mosby, 1995:66–8.
- Visco AG, Del Priore G. Postmenopausal Bartholin gland enlargement: a hospital-based cancer risk assessment. Obstet Gynecol. 1996;87:286–90.
- Wilkinson EJ, Stone IK. Atlas of vulvar disease. 5th ed. Baltimore: Williams & Wilkins, 1995:11–5.
- Cheetham DR. Bartholin’s cyst: marsupialization or aspiration?. Am J Obstet Gynecol. 1985;152:569–70.
- Brook I. Aerobic and anaerobic microbiology of Bartholin’s abscess. Surg Gynecol Obstet. 1989;169:32–4.
- Saul HM, Grossman MB. The role ofChlamydia trachomatis in Bartholin’s gland abscess. Am J Obstet Gynecol. 1988;158(3 pt 1):76–7.
- Azzan BB. Bartholin’s cyst and abscess. A review of treatment of 53 cases. Br J Clin Pract. 1978;32(4):101–2.
- Peters WA 3d. Bartholinitis after vulvovaginal surgery. Am J Obstet Gynecol. 1998;178:1143–4.
- Hill DA, Lense JJ. Office management of Bartholin gland cysts and abscesses. Am Fam Physician. 1998;57:1611–6.1619–20.
- Stenchever MA. Comprehensive gynecology. 4th ed. St. Louis: Mosby, 2001:482–6,645–6.
- Mathews D. Marsupialization in the treatment of Bartholin’s cysts and abscesses. J Obstet Gynaecol Br Commonw. 1966;73:1010–2.
- Apgar BS. Bartholin’s cyst/abscess: Word catheter insertion. In: Pfenninger JL, Fowler GC, eds. Procedures for primary care physicians. St. Louis: Mosby, 1994:596–600.
- Word B. Office treatment of cyst and abscess of Bartholin’s gland duct. South Med J. 1968;61:514–8.
- Horowitz IR, Buscema J, Woodruff JD. Surgical conditions of the vulva. In: Rock JA, Thompson JD, eds. Te Linde’s Operative gynecology. 8th ed. Philadelphia: Lipincott-Raven, 1997:890–3.





{kind=link}