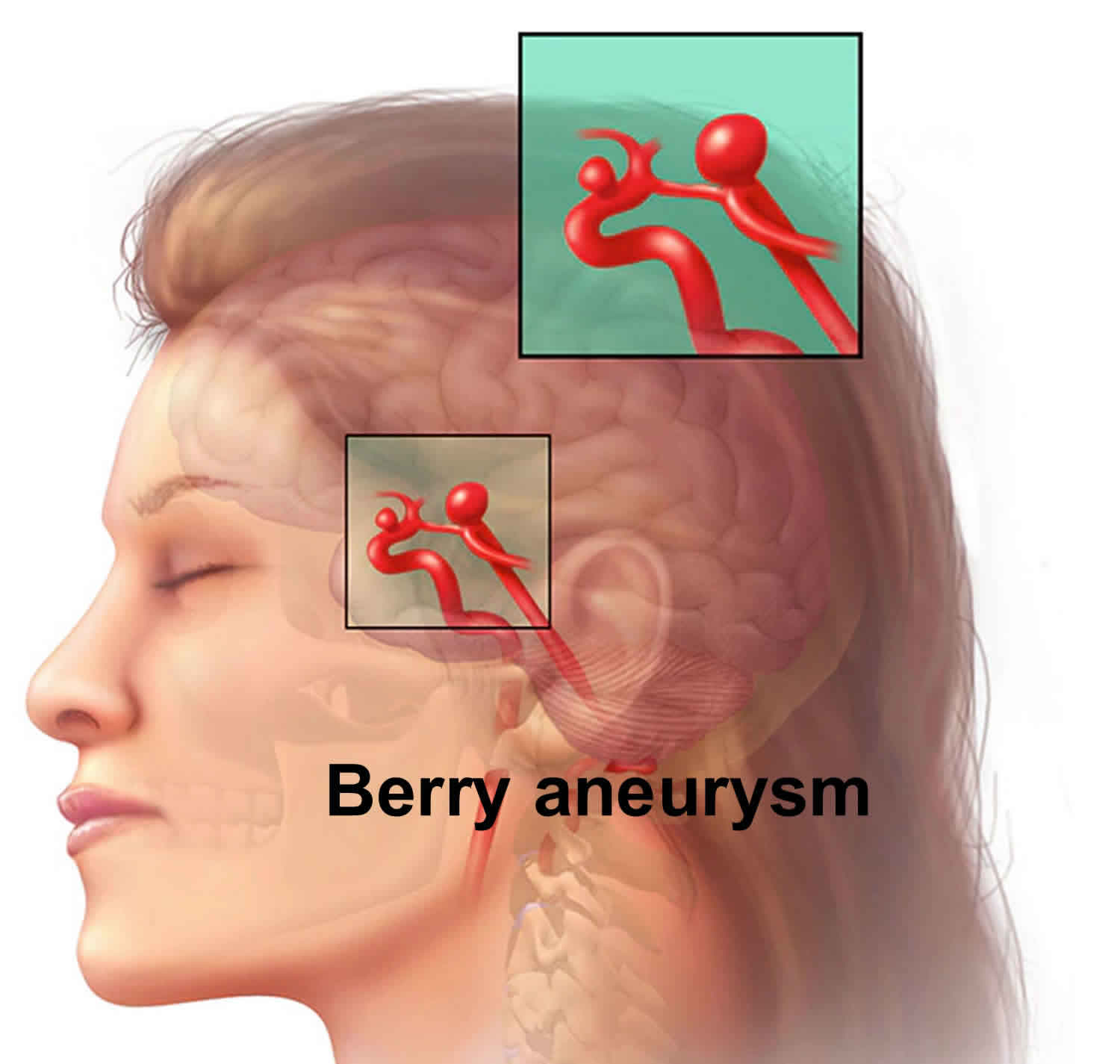
What is a berry aneurysm
Berry aneurysm also known as a saccular aneurysm, forms 97% of all brain aneurysms and are the most common cause of non-traumatic subarachnoid hemorrhage (SAH). A berry aneurysm is a rounded sac containing blood, that is attached to a main artery or one of its branches. Berry aneurysms occur most often in adults. A brain aneurysm is an abnormal bulge or “ballooning” in the wall of an artery in the brain. Brain aneurysms are sometimes called berry aneurysms because they are often the size of a small berry hanging on a stem. Those larger than 25 mm in the maximal dimension are called giant cerebral aneurysms. Charcot-Bouchard aneurysms are minute brain aneurysms which develop as a result of chronic hypertension and appear most commonly in the basal ganglia and other areas such as the thalamus, pons, and cerebellum, where there are small penetrating vessels (diameter <300 micrometers).
Most berry aneurysms produce no symptoms until they become large, begin to leak blood, or burst. A berry aneurysm can leak or rupture, causing bleeding into the brain (hemorrhagic stroke). Most often a ruptured berry aneurysm occurs in the space between the brain and the thin tissues covering the brain. This type of hemorrhagic stroke is called a subarachnoid hemorrhage (SAH). Up to 80% of patients with a spontaneous subarachnoid hemorrhage have ruptured an aneurysm and 90% of these aneurysms are located in the anterior circulation (carotid system), with 10% are found in the posterior circulation (vertebrobasilar system).
A ruptured berry aneurysm quickly becomes life-threatening and requires prompt medical treatment. Once an aneurysm bleeds, the chance of death is about 40 percent and the chance of some brain damage is about 66 percent, even if the aneurysm is treated. If the aneurysm isn’t treated quickly enough, another bleed may occur from the already ruptured aneurysm.
Most brain aneurysms, however, don’t rupture, create health problems or cause symptoms. Such aneurysms are often detected during tests for other conditions.
If a berry aneurysm presses on nerves in your brain, it can cause signs and symptoms. These can include
- A droopy eyelid
- Double vision or other changes in vision
- Pain above or behind the eye
- A dilated pupil
- Numbness or weakness on one side of the face or body
Prevalence of berry aneurysms in the asymptomatic general population has been reported over a wide range (0.2-8.9%) when examined angiographically, and in 15-30% of these patients, multiple aneurysms are found 1.
A familial tendency to aneurysms is also well recognized, with patients who have more than one first-degree relative affected, having a ~30% (range 17-44%) chance of themselves having an aneurysm 1.
Berry aneurysm treatment depends on the size and location of the berry aneurysm, whether it is infected, and whether it has burst. If a brain aneurysm bursts, symptoms can include a sudden, severe headache, nausea and vomiting, stiff neck, loss of consciousness, and signs of a stroke. Any of these symptoms requires immediate medical attention.
Treatment for an unruptured berry aneurysm may be appropriate in some cases and may prevent a rupture in the future. Talk with your doctor to ensure you understand the best options for your specific needs.
Are people born with berry aneurysm?
People usually aren’t born with brain aneurysms. Most brain aneurysms develop after age 40. Berry aneurysms usually develop at branching points of arteries and are caused by constant pressure from blood flow. Berry aneurysms often enlarge slowly and become weaker as they grow, just as a balloon becomes weaker as it stretches. Berry aneurysms may be associated with other types of blood vessel disorders, such as fibromuscular dysplasia, cerebral arteritis or arterial dissection, but these are very unusual. Some brain aneurysms are due to infections, drugs such as amphetamines and cocaine, or direct brain trauma from an accident.
Why is the brain damage so extensive after berry aneurysm ruptured?
When a berry aneurysm ruptures, the bleeding usually lasts only a few seconds. The blood can cause direct damage to surrounding cells, and the bleeding can damage or kill other cells. It also increases pressure inside the skull.
If the pressure becomes too elevated, the blood and oxygen supply to the brain may be disrupted to the point that loss of consciousness or even death may occur.
After blood enters the brain and the space around it, direct damage to the brain tissue and brain function results. The amount of damage is usually related to the amount of blood. Damage is due to the increased pressure and swelling from bleeding directly into the brain tissue, or from local cellular damage to brain tissue from irritation of blood in the space between the brain and the skull.
Blood can also irritate and damage the normal blood vessels and cause vasospasm (constriction). This can interrupt normal blood flow to the healthy brain tissue and can cause even more brain damage. This is called an “ischemic stroke.”
Will treating a ruptured berry aneurysm reverse or improve brain damage?
Once an aneurysm bleeds and brain damage occurs, treating the berry aneurysm will not reverse the damage. Treatment helps prevent more bleeding.
Berry aneurysm causes
The causes of brain aneurysm are unknown, but a range of factors may increase your risk. Berry aneurysms form when the walls of the arteries in the brain become thin and weaken. Berry aneurysms typically form at branch points in arteries because these sections are the weakest. Occasionally, cerebral aneurysms may be present from birth, usually resulting from an abnormality in an artery wall.
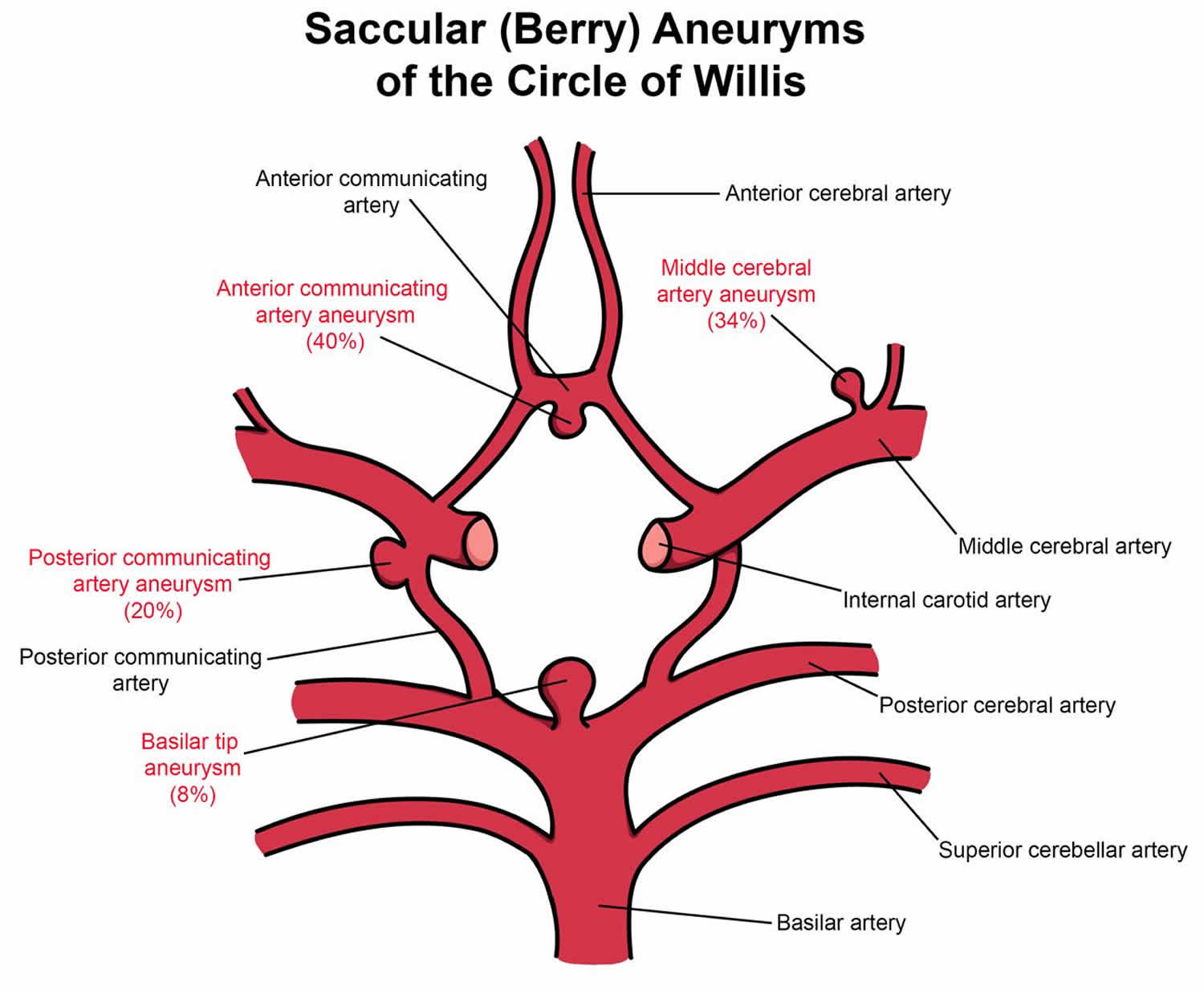
Figure 1. Berry aneurysm locations
Risk factors for developing berry aneurysm
A number of factors can contribute to weakness in an artery wall and increase the risk of a brain aneurysm or aneurysm rupture. Brain aneurysms are more common in adults than in children and more common in women than in men.
Some of these risk factors develop over time; others are present at birth.
Sometimes berry aneurysms are the result of inherited risk factors, including:
- genetic connective tissue disorders that weaken artery walls
- polycystic kidney disease (in which numerous cysts form in the kidneys)
- arteriovenous malformations (snarled tangles of arteries and veins in the brain that disrupt blood flow. Some arteriovenous malformations (AVMs) develop sporadically, or on their own.)
- history of aneurysm in a first-degree family member (child, sibling, or parent).
Other risk factors develop over time and include:
- untreated high blood pressure
- cigarette smoking
- drug abuse, especially cocaine or amphetamines, which raise blood pressure to dangerous levels. Intravenous drug abuse is a cause of infectious mycotic aneurysms.
- age over 40.
Less common risk factors include:
- head trauma
- brain tumor
- infection in the arterial wall (mycotic aneurysm).
Additionally, high blood pressure, cigarette smoking, diabetes, and high cholesterol puts one at risk of atherosclerosis (a blood vessel disease in which fats build up on the inside of artery walls), which can increase the risk of developing a fusiform aneurysm.
Risk factors for berry aneurysm to rupture
Not all berry aneurysms will rupture. Aneurysm characteristics such as size, location, and growth during follow-up evaluation may affect the risk that an aneurysm will rupture. In addition, medical conditions may influence aneurysm rupture.
Risk factors include:
- Smoking. Smoking is linked to both the development and rupture of cerebral aneurysms. Smoking may even cause multiple aneurysms to form in the brain.
- Heavy alcohol consumption.
- High blood pressure (hypertension). High blood pressure damages and weakens arteries, making them more likely to form and to rupture.
- Drug abuse, particularly the use of cocaine.
- Size. The largest aneurysms are the ones most likely to rupture in a person who previously did not show symptoms.
- Location. Aneurysms located on the posterior communicating arteries (a pair of arteries in the back part of the brain) and possibly those on the anterior communicating artery (a single artery in the front of the brain) have a higher risk of rupturing than those at other locations in the brain.
- Growth. Aneurysms that grow, even if they are small, are at increased risk of rupture.
- Family history. A family history of aneurysm rupture suggests a higher risk of rupture for aneurysms detected in family members.
- The greatest risk occurs in individuals with multiple aneurysms who have already suffered a previous rupture or sentinel bleed.
Some types of aneurysms may occur after a head injury (dissecting aneurysm) or from certain blood infections (mycotic aneurysm).
Risk factors present at birth
Selected conditions that date to birth can be associated with an elevated risk of developing a brain aneurysm. These include:
- Inherited connective tissue disorders, such as Ehlers-Danlos syndrome, that weaken blood vessels
- Polycystic kidney disease, an inherited disorder that results in fluid-filled sacs in the kidneys and usually increases blood pressure
- Abnormally narrow aorta (coarctation of the aorta), the large blood vessel that delivers oxygen-rich blood from the heart to the body
- Cerebral arteriovenous malformation (brain AVM), an abnormal connection between arteries and veins in the brain that interrupts the normal flow of blood between them
- Family history of brain aneurysm, particularly a first-degree relative, such as a parent, brother, sister, or child
What causes berry aneurysm to bleed?
Scientists usually don’t know why an aneurysm bleeds or exactly when it will bleed. Scientists do know what increases the chance for bleeding:
- High blood pressure is the leading cause of subarachnoid hemorrhage. Heavy lifting or straining can cause pressure to rise in the brain and may lead to an aneurysm rupture.
- Strong emotions, such as being upset or angry, can raise blood pressure and can subsequently cause aneurysms to rupture.
- Blood thinners (such as warfarin), some medications and prescription drugs (including diet pills that act as stimulants such as ephedrine and amphetamines), and harmful drugs like cocaine can cause aneurysms to rupture and bleed.
What are the chances that an unruptured aneurysm may bleed?
Many factors determine whether an aneurysm is likely to bleed. These include the size, shape and location of the aneurysm and symptoms that it causes. Smaller aneurysms that are uniform in size may be less likely to bleed than larger, irregularly shaped ones. Once an aneurysm has bled, there’s a very high chance of re-bleeding.
What happens if an aneurysm bleeds?
If an aneurysm ruptures, it leaks blood into the space around the brain. This is called a “subarachnoid hemorrhage.” Depending on the amount of blood, it can produce:
- a sudden severe headache that can last from several hours to days
- nausea and vomiting drowsiness and/or coma
The hemorrhage may also damage the brain directly, usually from bleeding into the brain itself. This is called a “hemorrhagic stroke.” This can lead to:
- weakness or paralysis of an arm or leg
- trouble speaking or understanding language
- vision problems
- seizures
Berry aneurysm symptoms
Unruptured berry aneurysm
An unruptured berry aneurysm may produce no symptoms, particularly if it’s small. However, a larger unruptured aneurysm may press on brain tissues and nerves, possibly causing:
- Pain above and behind one eye
- A dilated pupil
- Change in vision or double vision
- Numbness of one side of the face
- Paralysis on one side of the face
- Weakness
Ruptured berry aneurysm
A sudden, severe headache is the key symptom of a ruptured berry aneurysm. This headache is often described as the “worst headache” ever experienced.
Common signs and symptoms of a ruptured berry aneurysm include:
- Sudden, extremely severe headache
- Nausea and vomiting
- Stiff neck
- Blurred or double vision
- Sensitivity to light
- Seizure
- A drooping eyelid
- Loss of consciousness (this may happen briefly or may be prolonged)
- Confusion
- Cardiac arrest
Leaking berry aneurysm
Sometimes a berry aneurysm may leak a small amount of blood into the brain called a sentinel bleed. Sentinel or warning headaches may result from brain aneurysm that suffers a tiny leak, days or weeks prior to a significant rupture. However, only a minority of individuals have a sentinel headache prior to rupture. This leaking (sentinel bleed) may cause only a:
- Sudden, extremely severe headache
- A more severe rupture often follows leaking.
If you experience a sudden, severe headache, especially when it is combined with any other symptoms, you should seek immediate medical attention.
Ruptured berry aneurysm complications
Berry aneurysms may rupture and bleed into the space between the skull and the brain (subarachnoid hemorrhage) and sometimes into the brain tissue (intracerebral hemorrhage). These are forms of stroke called hemorrhagic stroke. The bleeding into the brain can cause a wide spectrum of symptoms, from a mild headache to permanent damage to the brain, or even death.
After a berry aneurysm has ruptured it may cause serious complications such as:
- Rebleeding. Once it has ruptured, an aneurysm may rupture again before it is treated, leading to further bleeding into the brain, and causing more damage or death.
- Hyponatremia. Subarachnoid hemorrhage from a ruptured brain aneurysm can disrupt the balance of sodium in the blood. This may occur from damage to the hypothalamus, an area near the base of the brain. A drop in blood-sodium levels (hyponatremia) can lead to swelling of brain cells and permanent damage.
- Hydrocephalus (enlargement of the spaces within the brain that produce cerebrospinal fluid). Subarachnoid hemorrhage can cause hydrocephalus. Hydrocephalus is a buildup of too much cerebrospinal fluid in the brain, which causes pressure that can lead to permanent brain damage or death. Hydrocephalus occurs frequently after subarachnoid hemorrhage because the blood blocks the normal flow of cerebrospinal fluid. If left untreated, increased pressure inside the head can cause coma or death.
- Vasospasm. This occurs frequently after subarachnoid hemorrhage when the bleeding causes the arteries in the brain to contract and limit blood flow to vital areas of the brain. This can cause strokes from lack of adequate blood flow to parts of the brain.
- Seizures. Aneurysm bleeding can cause seizures (convulsions), either at the time of bleed or in the immediate aftermath. While most seizures are evident, on occasion they may only be seen by sophisticated brain testing. Untreated seizures or those that do not respond to treatment can cause brain damage.
Berry aneurysm diagnosis
Most berry aneurysms go unnoticed until they rupture or are detected during medical imaging tests for another condition.
If you have experienced a severe headache or have any other symptoms related to a ruptured brain aneurysm your doctor will order tests to determine if blood has leaked into the space between the skull bone and brain.
Several tests are available to diagnose brain aneurysms and determine the best treatment. These include:
- Computed tomography (CT). This fast and painless scan is often the first test a physician will order to determine if blood has leaked into the brain. CT uses x-rays to create two-dimensional images, or “slices,” of the brain and skull. Occasionally a contrast dye is injected into the bloodstream prior to scanning to assess the arteries, and look for a possible aneurysm. This process, called CT angiography (CTA), produces sharper, more detailed images of blood flow in the brain arteries. CTA can show the size, location, and shape of an unruptured or a ruptured aneurysm.
- Magnetic resonance imaging (MRI). An MRI uses computer-generated radio waves and a magnetic field to create two- and three-dimensional detailed images of the brain and can determine if there has been bleeding into the brain. Magnetic resonance angiography (MRA) produces detailed images of the brain arteries and can show the size, location, and shape of an aneurysm.
- Cerebral angiography. This imaging technique can find blockages in arteries in the brain or neck. It also can identify weak spots in an artery, like an aneurysm. The test is used to determine the cause of the bleeding in the brain and the exact location, size, and shape of an aneurysm. Your doctor will pass a catheter (long, flexible tube) typically from the groin arteries to inject a small amount of contrast dye into your neck and brain arteries. The contrast dye helps the X-ray create a detailed picture of the appearance of an aneurysm and a clear picture of any blockage in the arteries.
- Cerebrospinal fluid (CSF) analysis. This test measures the chemicals in the fluid that cushions and protects the brain and spinal cord (cerebrospinal fluid). Most often a doctor will collect the CSF by performing a spinal tap (lumbar puncture), in which a thin needle is inserted into the lower back (lumbar spine) and a small amount of fluid is removed and tested. The results will help detect any bleeding around the brain. If bleeding is detected, additional tests would be needed to identify the exact cause of the bleeding.
Berry aneurysm treatment
Not all berry aneurysms require treatment. Some very small unruptured berry aneurysms that are not associated with any factors suggesting a higher risk of rupture may be safely left alone and monitored with MRA or CTA to detect any growth. It is important to aggressively treat any coexisting medical problems and risk factors.
Treatments for unruptured berry aneurysms that have not shown symptoms have some potentially serious complications and should be carefully weighed against the predicted rupture risk.
How is a treatment method for a berry aneurysm chosen?
Doctors must evaluate the risk factors that favor treatment vs. non-treatment and decide which technique may be best. It’s important to consult with experts in this field. This should include a cerebrovascular neurosurgeon who specializes in surgically clipping aneurysms, a neurosurgeon with endovascular expertise and training, a neurointerventionalist (a neurologist with endovascular training) or a neuroradiologist who specializes in the less invasive treatment of cerebral aneurysms by coiling.
Treatment considerations for unruptured berry aneurysms
Surgical clipping or endovascular coiling or a flow diverter can be used to seal off an unruptured brain aneurysm and help prevent a future rupture. However, in some unruptured berry aneurysms, the known risks of the procedures may outweigh the potential benefit.
A neurologist, in collaboration with a neurosurgeon or interventional neuroradiologist, can help you determine whether the treatment is appropriate for you.
A doctor will consider a variety of factors when determining the best option for treating an unruptured berry aneurysm, including:
- type, size, and location of the aneurysm
- risk of rupture
- the person’s age and health
- personal and family medical history
- risk of treatment.
Individuals should also take the following steps to reduce the risk of berry aneurysm rupture:
- carefully control blood pressure
- stop smoking
- avoid cocaine use or other stimulant drugs.
If you have high blood pressure, talk to your doctor about medication to manage the condition. If you have a brain aneurysm, proper control of blood pressure may lower the risk of rupture.
In addition, if you smoke cigarettes, talk with your doctor about strategies to stop smoking since cigarette smoking is a risk factor for formation, growth and rupture of the aneurysm.
If you have an unruptured brain aneurysm, you may lower the risk of its rupture by making these lifestyle changes:
- Don’t smoke or use recreational drugs. If you smoke or use recreational drugs, talk to your doctor about strategies or an appropriate treatment program to help you quit.
- Eat a healthy diet and exercise. Changes in diet and exercise can help lower blood pressure. Talk to your doctor about changes appropriate for you.
Treatments for unruptured and ruptured berry aneurysms
Surgery, endovascular treatments, or other therapies are often recommended to manage symptoms and prevent damage from unruptured and ruptured berry aneurysms.
Surgery
There are a few surgical options available for treating berry aneurysms. These procedures carry some risk such as possible damage to other blood vessels, the potential for aneurysm recurrence and rebleeding, and a risk of stroke.
- Microvascular clipping. This procedure involves cutting off the flow of blood to the aneurysm and requires open brain surgery. A doctor will locate the blood vessels that feed the aneurysm and place a tiny, metal, clothespin-like clip on the aneurysm’s neck to stop its blood supply. Clipping has been shown to be highly effective, depending on the location, size, and shape of the aneurysm. In general, aneurysms that are completely clipped do not recur.
Endovascular treatment
- Platinum coil embolization. This procedure is a less invasive procedure than microvascular surgical clipping. A doctor will insert a hollow plastic tube (a catheter) into an artery, usually in the groin, and thread it through the body to the brain aneurysm. Using a wire, the doctor will pass detachable coils (tiny spirals of platinum wire) through the catheter and release them into the aneurysm. The coils block the aneurysm and reduce the flow of blood into the aneurysm. The procedure may need to be performed more than once during the person’s lifetime because aneurysms treated with coiling can sometimes recur.
- Flow diversion devices. Other endovascular treatment options include placing a small stent (flexible mesh tube) similar to those placed for heart blockages, in the artery to reduce blood flow into the aneurysm. A doctor will insert a hollow plastic tube (a catheter) into an artery, usually in the groin, and thread it through the body to the artery on which the aneurysm is located. This procedure is used to treat very large aneurysms and those that cannot be treated with surgery or platinum coil embolization.
Other treatments
Other treatments for a ruptured berry aneurysm aim to control symptoms and reduce complications. These treatments include:
- Antiseizure drugs (anticonvulsants). These drugs may be used to prevent seizures related to a ruptured aneurysm. These medications include levetiracetam (Keppra), phenytoin (Dilantin, Phenytek, others), valproic acid (Depakene) and others. Their use has been debated by several experts, and is generally subject to your doctor’s discretion, based on your medical needs.
- Calcium channel-blocking drugs. Risk of stroke by vasospasm can be reduced with calcium channel-blocking drugs. One of these medications, nimodipine (Nymalize, Nimotop), has been shown to reduce the risk of delayed brain injury caused by insufficient blood flow after subarachnoid hemorrhage from a ruptured aneurysm.
- Ventricular or lumbar draining catheters and shunt surgery, which funnels cerebrospinal fluid from the brain to elsewhere in the body, may be surgically inserted into the brain following rupture if the buildup of cerebrospinal fluid (hydrocephalus) is causing harmful pressure on surrounding brain tissue. A catheter may be placed in the spaces filled with fluid inside of the brain (ventricles) or surrounding your brain and spinal cord to drain the excess fluid into an external bag. Sometimes it may then be necessary to introduce a shunt system — which consists of a flexible silicone rubber tube (shunt) and a valve — that creates a drainage channel starting in your brain and ending in your abdominal cavity.
- Pain relievers, such as acetaminophen (Tylenol, others), may be used to treat headache pain.
Rehabilitative therapy. Individuals who have suffered a subarachnoid hemorrhage often need physical, speech, and occupational therapy to regain lost function and learn to cope with any permanent disability.
Berry aneurysm prognosis
An unruptured berry aneurysm may go unnoticed throughout a person’s lifetime and not cause symptoms.
After a berry aneurysm bursts, the person’s prognosis largely depends on:
- age and general health
- preexisting neurological conditions
- location of the aneurysm
- extent of bleeding (and rebleeding)
- time between rupture and medical attention
- successful treatment of the aneurysm.
About 25 percent of individuals whose cerebral aneurysm has ruptured do not survive the first 24 hours; another 25 percent die from complications within 6 months. People who experience subarachnoid hemorrhage may have permanent neurological damage. Other individuals recover with little or no disability. Diagnosing and treating a cerebral aneurysm as soon as possible will help increase the chances of making a full recovery.
Recovery from treatment or rupture may take weeks to months.



{kind=link}