
Poroma
Poromas are a group of benign growths of poroid differentiation, i.e. derived from cells of the terminal duct and connected to the epidermis. They can be of either eccrine or apocrine lineage. They may present as papules (bumps), plaques (thickened patches like seborrhoeic keratoses), or nodules (lumps). Names used to describe poromas include:
- Eccrine poroma
- Dermal duct tumor (intradermal or dermal eccrine poroma)
- Hidroacanthoma simplex (intraepidermal eccrine poroma)
- Syringoacanthoma
- Syringofibroadenoma.
Poromas usually have a reddish color due to prominent underlying blood vessels and may resemble pyogenic granuloma. They may also appear darker than surrounding skin.
Poromas may arise on any skin surface but those with eccrine differentiation are most commonly found on the palms, soles and scalp. When multiple, they are sometimes described as poromatosis.
Skin biopsy of poroma shows a growth of terminal duct cells. The report may describe a circumscribed proliferation of compact cuboidal keratinocytes with small monomorphous nuclei and scant eosinophilic cytoplasm. The narrow ducts are often lined by a row of cuboidal cells. Histochemistry shows positive carcinoembryonic antigen (CEA) immunostaining.
Poromas are usually removed by surgical excision and electrosurgical destruction.
Eccrine poroma
Eccrine poroma is a benign adnexal tumor derived from the intra-epidermal eccrine sweat gland duct epithelium 1. Eccrine poroma was first reported by Pinkus et al. in 1956. Sweat gland tumors represent 1% of all primary skin lesions, and eccrine poroma makes up 10% of these 2. Eccrine poroma usually occurs as a solitary, dome-shaped, skin-colored or pigmented, slow-growing, sessile papule or nodule, situated mostly on the soles or sides of the feet. However, eccrine poromas have been found on hairless surfaces of the extremities, chest, back, head, and neck 3. Eccrine poroma is an uncommon pathologic condition that appears predominantly between the fourth and sixth decades of life 2. There is a malignant variant, eccrine porocarcinoma, which may be a primary tumor, but generally results from the malignant transformation of eccrine poroma 4 affecting most often people in the 6th-7th decades of life 1. Both commonly occur in the palms or sides of the feet; these areas have a high concentration of eccrine sweat glands.
Although eccrine poroma is known to be benign, it can slowly become a malignant tumor. The ratio of malignant transformation from eccrine poroma into eccrine porocarcinoma is 18%, as reported by Robson et al.5. However, eccrine porocarcinoma does not always arise from eccrine poroma. Eccrine porocarcinoma sometimes develops de novo, without any preexisting lesion.
It is not difficult to differentiate eccrine porocarcinoma from eccrine poroma, but eccrine porocarcinoma can be confused with other malignant diseases, such as squamous cell carcinoma and ulcerated basal cell carcinoma. A good resectional biopsy is necessary, and the existence of ductual differentiation under microscopic examination may be helpful. However, some variants of eccrine poroma exhibit malignant biological behaviors, such as an infiltrative growth pattern 6. Importantly, while a bleeding tendency is seen as a hallmark of malignant transformation in tumors, this does not necessarily apply in this context. Because the lesions which clinically presented as verrucous plaques or polypoid growths are frequently ulcerated and occasionally bled upon trauma 7.
Figure 1. Eccrine poroma
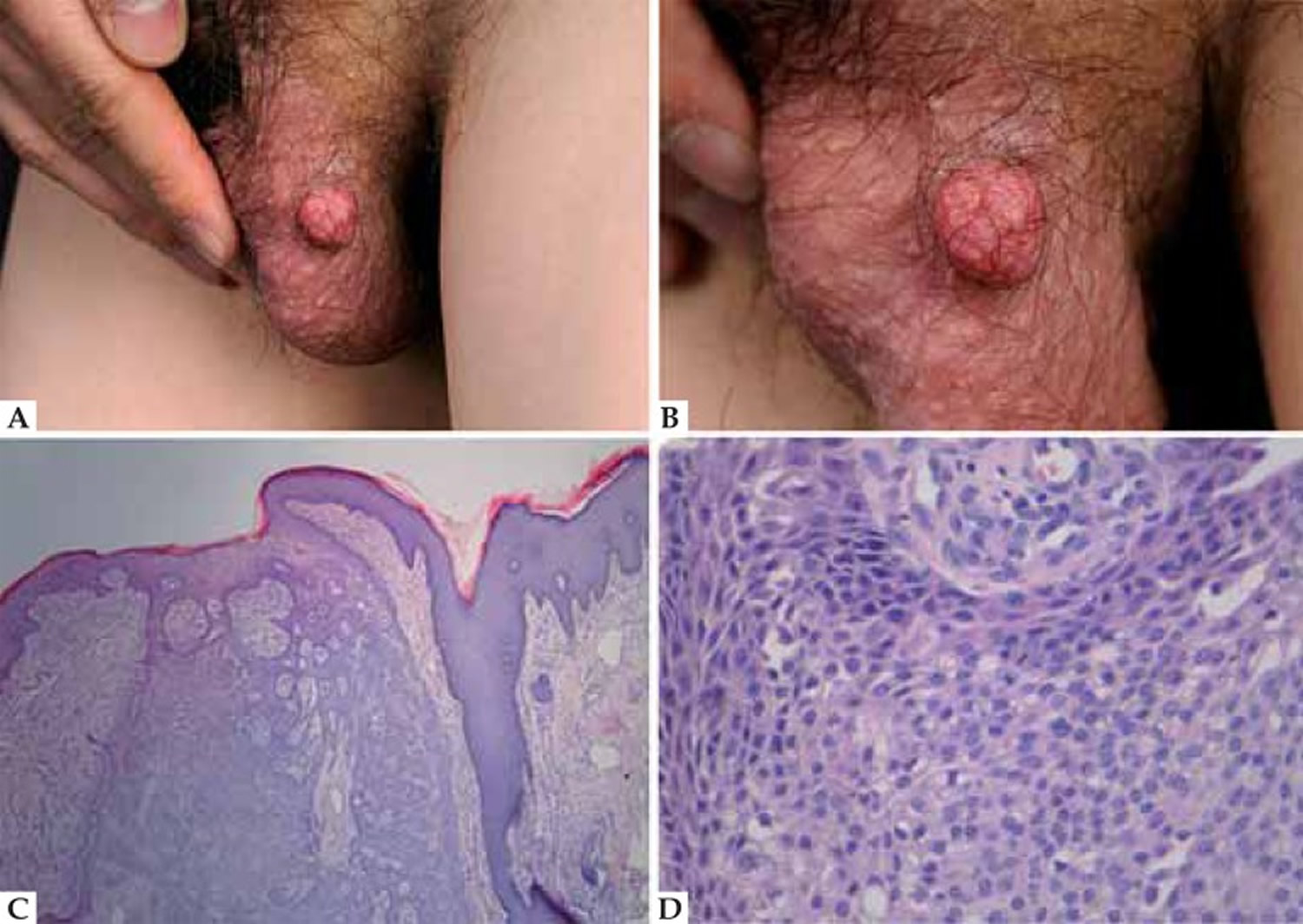
Footnote: A. Reddish mass on the left scrotum; B. Irregular surface; C. Hematoxylin & eosin: well circumscribed nodule with tubular structures and cystic spaces; D. Hematoxylin & eosin: small, cuboidal poroid cells with eosinophilic cytoplasm and monomorphic nuclei
[Source 2 ]What causes eccrine poroma
The pathogenesis of eccrine poroma and eccrine porocarcinoma is unknown. Actinic damage, trauma, radiation and the human papilloma virus (HPV) are believed to be involved 8. Chen SY et al. 9 reported that cyclin D1, p-pRb, p53, p63 and p73 may play a role in the tumorigenesis of eccrine poroma and eccrine porocarcinoma. In particular, overexpressed p53, p63 and p73 might contribute to the formation of both eccrine poroma and eccrine porocarcinoma; they also reported that activation of cyclin D1-p-pRb, possibly in conjunction with p53 dysfunctions and/or its family, may play a role in malignant transduction to eccrine porocarcinoma from eccrine duct cells or preexisting eccrine poroma.
Eccrine poroma treatment
Surgical excision with histologically clear margins is the optimal management for eccrine poroma undergoing recent changes, as an incisional biopsy may appear falsely benign 9. In early eccrine porocarcinoma lesions, cure is possible in up to 70-80% of patients, although a high recurrence rate of up to 20% has been reported 10. For patients with metastasis, there is no adjuvant therapy with strong evidence for the management of eccrine porocarcinoma.
- Concomitant poroma and porocarcinoma. An Bras Dermatol. 2017 Jul-Aug; 92(4): 550–552. doi: 10.1590/abd1806-4841.20175719 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5595608[↩][↩]
- Eccrine poroma and porocarcinoma on the same unusual location: report on two cases. An Bras Dermatol. 2015 May-Jun; 90(3 Suppl 1): 69–72. doi: 10.1590/abd1806-4841.20153415 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4540512[↩][↩][↩]
- A rapidly growing eccrine poroma in a pregnant woman. Guimerá Martín-Neda F, García Bustínduy M, Noda Cabrera A, Sánchez González R, García Montelongo R. J Am Acad Dermatol. 2004 Jan; 50(1):124-6.[↩]
- Pigmented eccrine poroma: report of an atypical case with the use of dermoscopy. Almeida FC, Cavalcanti SM, Medeiros AC, Teixeira MA. An Bras Dermatol. 2013 Sep-Oct; 88(5):803-6.[↩]
- Eccrine porocarcinoma (malignant eccrine poroma): a clinicopathologic study of 69 cases. Robson A, Greene J, Ansari N, Kim B, Seed PT, McKee PH, Calonje E. Am J Surg Pathol. 2001 Jun; 25(6):710-20.[↩]
- Robson A, Greene J, Ansari N, Kim B, Seed PT, McKee PH, et al. Eccrine porocarcinoma (malignant eccrine poroma): a clinicopathologic study of 69 cases. Am J Surg Pathol. 2001;25:710–720.[↩]
- Shaw M, McKee PH, Lowe D, Black MM. Malignant eccrine poroma: a study of twenty-seven cases. Br J Dermatol. 1982;107:675–680.[↩]
- Johnson RC, Rosenmeier GJ, Keeling 3rd JH. A painful step. Eccrine poroma. Arch Dermatol. 1992;128:1530–1533.[↩]
- Chen SY, Takeuchi S, Moroi Y, Kido M, Hayashida S, Qian Y, et al. Significance of cyclin D1-, product of retinoblastoma (pRb), p53, p63 and p73 expression in eccrine poroma and eccrine porocarcinoma. J Dermatol Sci. 2009;56:69–72.[↩][↩]
- Brown CW Jr, Dy LC. Eccrine porocarcinoma. Dermatol Ther. 2008;21:433–438[↩]





{kind=link}