
Photoaging
Photoaging is premature aging of the skin or damage to the skin caused by repeated exposure to ultraviolet radiation (UVR), primarily from the sun but also from artificial ultraviolet (UV) sources. Photoaging differs from chronologic aging: the damaging effects of UV rays – from the sun or artificial tanning sources – alter normal skin structures. Responsible for 90 percent of visible changes to the skin, photoaging is a direct result of cumulative sun damage you’ve been exposed to throughout your life. Chronological skin aging, on the other hand, is characterized by laxity and fine wrinkles, as well as development of benign growths such as seborrheic keratoses and angiomas, but it is not associated with increased/decreased pigmentation or with deep wrinkles that are characteristic for photoaging 1. Seborrheic keratoses are regarded as best biomarker of intrinsic skin aging since their appearance is independent on sun exposure 2. While intrinsically aged skin does not show vascular damage, photodamaged skin does.
Lifetime exposure to sunlight is a key risk factor for photoaging. Intrinsic ageing results in thinning of the epidermis and dermis, structural defects and immunological failure. These features are exaggerated in photo-aged skin, accompanied by lines, color changes and neoplasia. Clinical signs of photoaging include wrinkles, mottled pigmentation (hypo- or hyperpigmentation), rough skin, loss of the skin tone, dryness, sallowness, deep furrows, severe atrophy, telangiectasias, laxity, leathery appearance, solar elastosis, actinic purpura, precancerous lesions, skin cancer, and melanoma 3. Sun-exposed areas of the skin, such as the face, neck, upper chest, hands, and forearms, are the sites where these changes occur most often 4.
Unlike chronological aging, which is predetermined by individual’s physiological predisposition, photoaging depends primarily on the degree of sun exposure and on an amount of melanin in the skin 2. Individuals who have a history of intensive sun exposure, live in sunny geographical areas, and have fair skin will experience the greatest amount of ultraviolet radiation (UVR) skin load and consequently severe photoaging 5.
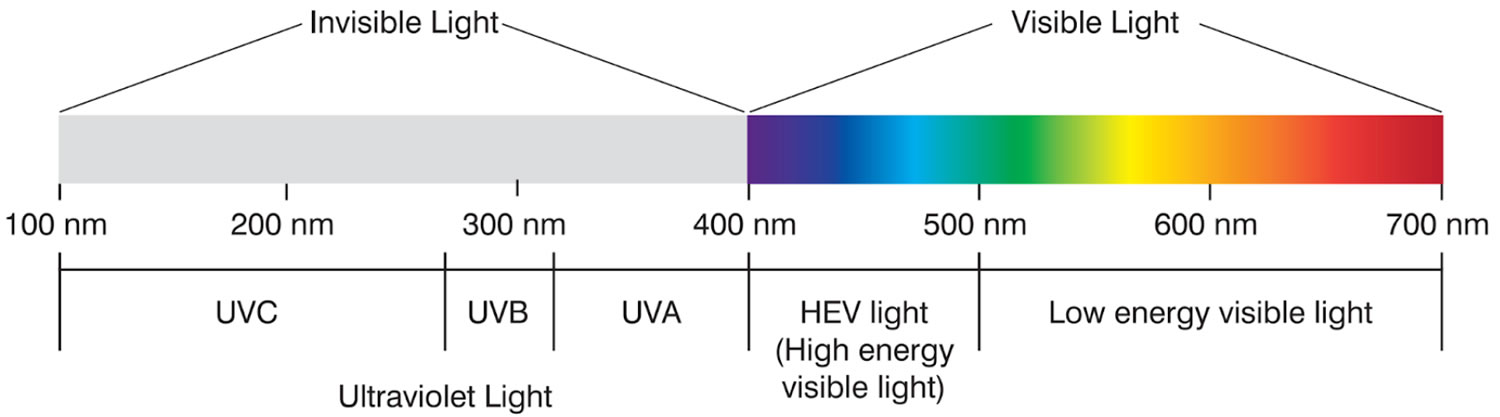
While sunlight is the number one cause of skin aging, about 10 percent comes from high-energy visible light (HEV light, in the violet/blue band from 400 to 450 nm in the visible spectrum) and infrared light. High-energy visible light or high-energy (blue) visible light, which emits from the sun and devices such as your phone or computer and can be seen by the human eye. This light doesn’t stop when the sun goes down. Infrared light is invisible to the eye and rather is felt as heat, like in a microwave.
Fortunately, neither of these has been linked to skin cancer, but they have been shown to break down collagen and skin elasticity. In recent years, some research is focusing on the additional effects of these other light forms may have on the skin. According to a 2014 study 6 in the journal Photodermatology, Photoimmunology & Photomedicine, non-UV solar radiation significantly contributes to photoaging and needs to be taken into consideration when formulating a skin-protective regimen.
Ultraviolet radiation causes biological effects on various tissues when it is absorbed. Injury to nucleic acids results in abnormal structures such as cyclobutane dimers and adducts. There are several repair mechanisms in normal individuals but their malfunction results in the development of aging changes and skin cancer.
Figure 1. Spectrum of solar radiation

Figure 2. Ultraviolet radiation
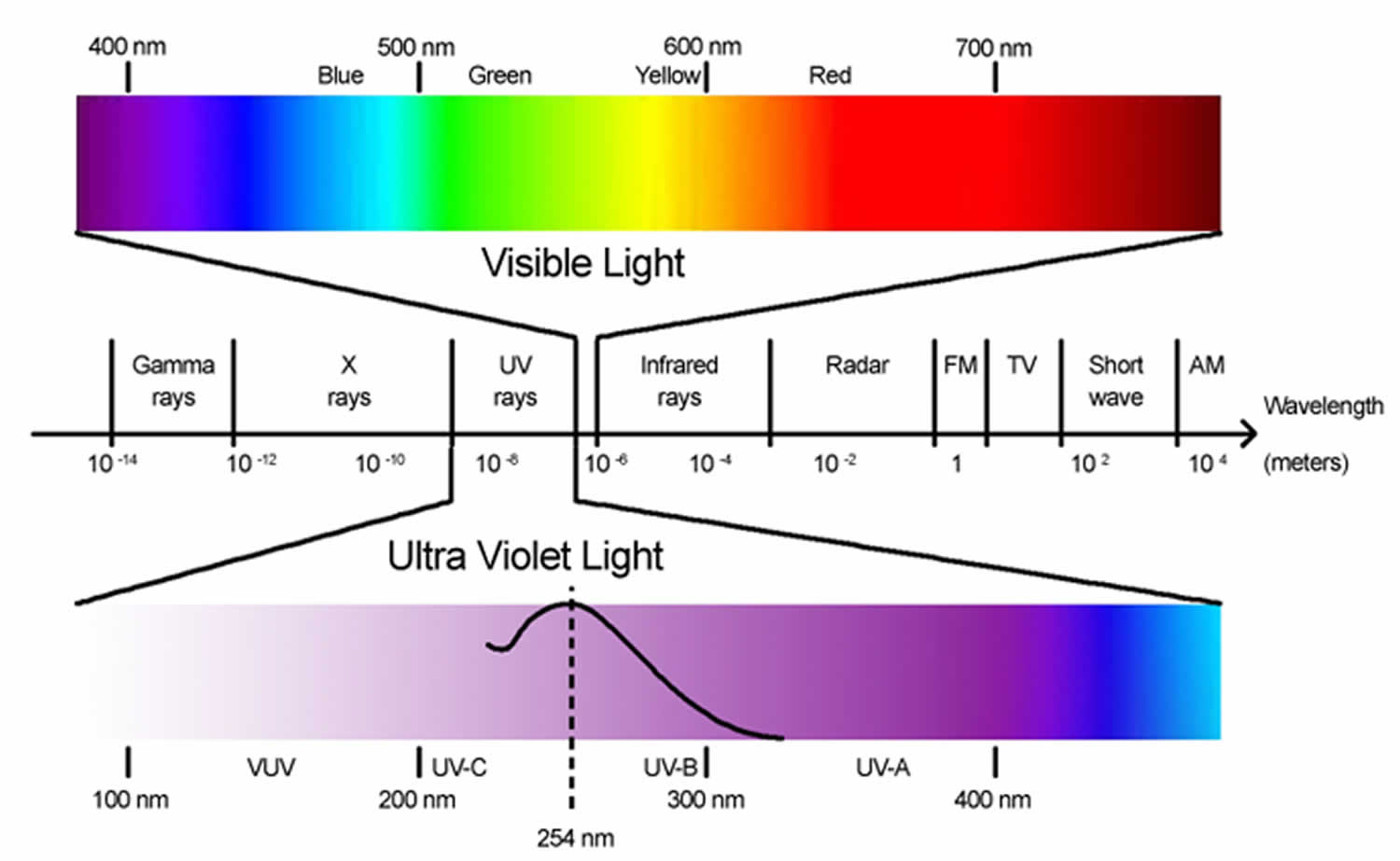
Figure 3. Visible light spectrum
Skin anatomy
The skin (integument) is your body’s largest and heaviest organ. In adults, the skin covers an area of 1.5 to 2.0 m2 and accounts for about 15% of the body weight.
The skin consists of two layers:
- a stratified squamous epithelium called the Epidermis and
- a deeper connective tissue layer called the Dermis (Figure 4).
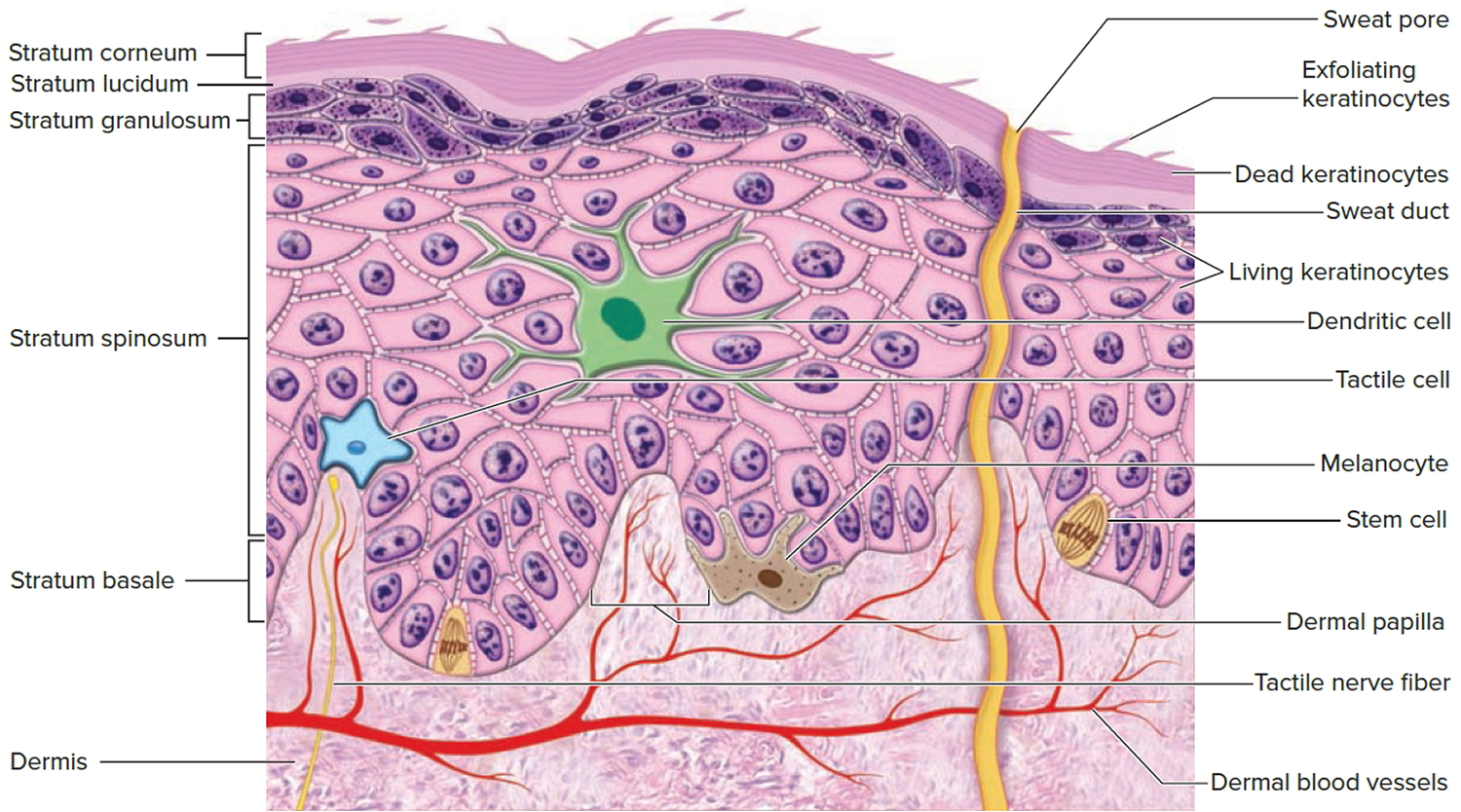
Figure 4. Skin structure

Below the dermis is another connective tissue layer, the hypodermis, which is not part of the skin but is customarily studied in conjunction with it. Most of the skin is 1 to 2 mm thick, but it ranges from less than 0.5 mm on the eyelids to 6 mm between the shoulder blades. The difference is due mainly to variation in thickness of the dermis, although skin is classified as thick or thin based on the relative thickness of the epidermis alone.
Thick skin covers the palms, soles, and corresponding surfaces of the fingers and toes. Its epidermis alone is about 0.5 mm thick, due to a very thick surface layer of dead cells called the stratum corneum (see Figure 5). Thick skin has sweat glands but no hair follicles or sebaceous (oil) glands. The rest of the body is covered with thin skin, which has an epidermis about 0.1 mm thick, with a thin stratum corneum. It possesses hair follicles, sebaceous glands, and sweat glands.
The accessory structures include hair, nails, and a variety of multicellular exocrine glands. These structures are located in the dermis and protrude through the epidermis to the surface.
Figure 5. Structure and skin cells of the Epidermis
Skin phototypes
Fitzpatrick skin phototypes 1 to 6 are used to classify the effect of sun exposure on an individual’s skin. Types 1 and 2 are at high risk of skin cancer, particularly when exposed to intense sunlight.
Table 1. Skin phototypes
| Type 1 | Very fair. Burns easily, doesn’t tan |
| Type 2 | Fair. Burns easily, tans lightly |
| Type 3 | Olive. Burns somewhat, tans readily |
| Type 4 | Light brown. Burns rarely, tans well |
| Type 5 | Dark brown. Doesn’t burn, tans deeply |
| Type 6 | Black |
Figure 6. Skin phototypes

Photoaging causes
Your skin is composed of three layers: the epidermis, or outermost layer; the dermis, or middle layer; and the subcutis, or bottom most layer. The dermis contains collagen, elastin and other fibers that support the skin’s structure. It is these elements that give skin its smooth and youthful appearance — and that are damaged by UV radiation. UV radiation is at its greatest on the earth’s surface when the sun is vertically overhead as it passes through thinner atmosphere than when the sun is at a greater angle.
There is also greater total UV:
- When the conditions are clear, compared with cloud or smog
- With a reflective surface such as snow or sand
- On a mountain compared with at sea level
- Outdoors compared with behind window glass
Ultraviolet radiation results in profound alterations of both local and systemic immune responses:
- The immune changes are mainly mediated by cytokines released from epidermal cells, but also by neuropeptides released from sensory nerves in the skin;
- The function of antigen-presenting cells (Langerhans’s cells) is reduced;
- Ultraviolet radiation prevents primary contact sensitization to surface antigens;
- It inhibits histamine release from mast cells;
- Suppressor T cells may induce tolerance contributing to eventual development of skin cancers.
The UV radiation that affects your skin is composed of two different types of waves, ultraviolet-A (UVA) and ultraviolet-B (UVB). When UV rays hit your skin, they damage its DNA, and cells in the dermis scramble to produce melanin in the epidermis to prevent further damage. This is the process that gives you a tan, which is really just your skin attempting to block the radiation from penetrating your skin.
Ultraviolet-B (UVB) (290 to 320 nm) rays are shorter than ultraviolet-A (UVA) (320 to 400 nm) rays, and are the main culprit behind sunburn. The ultraviolet-A (UVA) rays, with their longer wavelength, are responsible for much of the damage associated with photoaging. Ultraviolet-A (UVA) (320 to 400 nm) rays penetrate deep into the dermis, where they damage the collagen fibers. This damage causes increased production of abnormal elastin. The unusual amounts of elastin result in the production of enzymes called metalloproteinases (matrix metalloproteinase-1). These enzymes, which rebuild damaged collagen, often malfunction and degrade the collagen, resulting in incorrectly rebuilt skin. As this process is repeated with daily UVA exposure, the incorrectly rebuilt skin forms wrinkles, and the depleted collagen results in leathery skin.
Photoaging of the skin depends primarily on the degree of ultraviolet radiation and on an amount of melanin in the skin (skin phototype) 2. In addition to direct or indirect DNA damage, ultraviolet radiation activates cell surface receptors of keratinocytes and fibroblasts in the skin, which leads to a breakdown of collagen in the extracellular matrix and a shutdown of new collagen synthesis. It is hypothesized that dermal collagen breakdown is followed by imperfect repair that yields a deficit in the structural integrity of the skin, formation of a solar scar, and ultimately clinically visible skin atrophy and wrinkles. Many studies confirmed that acute exposure of human skin to ultraviolet radiation leads to oxidation of cellular biomolecules that could be prevented by prior antioxidant treatment and to depletion of endogenous antioxidants. Skin has a network of all major endogenous enzymatic and nonenzymatic protective antioxidants, but their role in protecting cells against oxidative damage generated by UV radiation has not been elucidated. It seems that skin’s antioxidative defence is also influenced by vitamins and nutritive factors and that combination of different antioxidants simultaneously provides synergistic effect.
Studies in humans and in the albino and hairless mice showed that acute and chronic ultraviolet-B (UVB) irradiation greatly increases skin vascularization and angiogenesis 7. The sun is the main source of ultraviolet radiation and the main contributor to the photoaging. Ultraviolet-C (UVC) radiation (100 to 290 nm) is almost completely absorbed by the ozone layer and does not affect the skin. Ultraviolet-B (UVB) (290 to 320 nm) affects the superficial layer of the skin (epidermis) and causes sunburns. Ultraviolet-B (UVB) is the most intense between 10 am and 2 pm, during summer months, does not penetrate through the glass, and accounts for 70% of a person’s yearly average cumulative UVB dose. Ultraviolet-A (UVA) (320 to 400 nm) was believed to have a minor effect on the skin, but studies showed that they penetrate deeper in the skin (e.g., about 20% at 365 nm), are more abundant in sunlight (95% of UVA and 5% of UVB), and therefore exhibit more severe damage 8. Significantly more photons in the UVA are needed to cause the same degree of damage compared to UVB since they are less energetic, but they are present in much higher quantities in sunlight and are more penetrant than in UVB 9. Until recently, it has become evident that also infrared radiation (IR) could induce skin damage and contribute to the skin photoaging. While proton energy of infrared radiation is low, total amount of infrared radiation which reaches humans’ skin accounts approximately for 54% (compared to 5–7% of UV rays). Most of the infrared radiation lies within the infrared radiation-A (IR-A) band (λ = 760 to 1440 nm), which represents approximately 30% of total solar energy, and penetrates human skin deeply compared to infrared radiation-B (IR-B) and infrared radiation-C (IR-C), which only penetrate the upper skin layers. In comparison, infrared radiation-A penetrates the skin deeper than UV, and approximately 50% of it reaches the dermis. Molecular mechanisms of damaging effect of infrared radiation-A on the skin are attributed to induction of matrix metalloproteinase-1, as well as to generation of reactive oxygen species (ROS). The exposure of human to environmental and artificial ultraviolet radiation has increased significantly in the last 50 years. This is due to an increased solar ultraviolet radiation as a consequence of the stratospheric ozone depletion, use of sunscreens, false believe of being well protected while exposed to sun for longer time, outdoor leisure activities, and prolonged life expectancy in industrialized countries 10.
What causes the skin to age?
Intrinsic ageing is defined by the clinical, histological and physiological changes that occur in sun-protected areas of skin of older individuals. Intrinsic ageing can be compounded by other environmental factors.
Ultraviolet radiation
UV radiation attacks the integrity of the skin.
- It causes thousands of alterations in the DNA of each cell every day.
- The multi-hit model, which has been proposed to describe how UV radiation interacts with components of the extracellular matrix, results in the deposition of a disorganized, elastic-fibre rich matrix (solar elastosis).
Menopause
The signs of intrinsic ageing begin at around 50–60 years of age. Women develop these signs earlier than men, which is attributed to a decrease in the protective effects of oestrogen during menopause.
Smoking
Smoking exposes the skin to several damaging factors.
- Nicotine narrows blood vessels and blood flow, reducing the amount of oxygen and nutrients that reach the cells.
- Many other chemicals in tobacco smoke increase dermal MMPs and degrade collagen and elastin.
- The heat from burning cigarettes and the facial muscle movements associated with smoking contribute to wrinkles.
- Chemicals such as nitrosamines and tar are carcinogens.
Nutrition
Nutrition is known to affect extrinsic ageing.
- Fruits, vegetables, legumes, herbs, and teas contain antioxidative compounds.
- Higher levels of vitamin C and increased linoleic acid intake have been associated with decreased wrinkling, dryness, and atrophy of the skin.
- In a nutritional study that recruited Greek, Australian, and Swedish subjects, resilience to photoageing was associated with a higher intake of vegetables, olive oil, fish, and legumes such as chicpeas, beans, peas, and lentils, and a lower intake of margarine, sugar and dairy products.
- A higher fat and carbohydrate intake has been associated with an increased risk of wrinkles and skin atrophy.
- Vitamin A, which can be applied topically, has been observed to decrease the production of MMPs.
- The consumption of fish oil can also confer some sun protection.
Immune dysfunction
- Skin ageing can be a symptom of immune deficiency diseases, immunosuppressive agents, and chronic psychological stress.
Photoaging prevention
Anti-aging skin care tips
Tips on how you can prevent photoaging:
- Protect your skin from the sun. Sun protection forms the foundation of every anti-aging skin-care plan. The sun’s rays make your skin age more quickly. There are now so much evidence that the sun prematurely ages your skin that there is actually a word to describe this effect. This word is “photoaging.” To help protect your skin from the sun and other harmful UV rays, dermatologists offer these tips:
- Seek shade whenever possible, including from trees, shade coverings, buildings, etc. Be sure to seek shade especially between 10 a.m. and 3 p.m. when the sun’s UV rays are strongest and whenever your shadow looks shorter than you are.
- Cover up in style. Whenever possible, wear a wide-brimmed hat (at least five-inch-wide), pants, and long sleeves. Gloves help to minimize common signs of aging on our hands such as age spots. Sunglasses help reduce fine lines around your eyes.
- Slather on the sunscreen every day before going outdoors. To protect your skin, apply sunscreen to all skin that clothing will not cover. You want to use a sunscreen that offers broad-spectrum protection, SPF 30 (or higher) that protects against UVB and UVA and water resistance. Reapply after swimming or heavy exertion. Look for the FDA’s logo for effective products that meet these criteria.
- Apply sunscreen liberally to get its intended effect. Protect especially well the face, ears, neck and hands. These areas are exposed the most, and show sun damage first. Women should include the exposed upper chest. Lips are also very prone to photoaging.
- Use cosmetics such as moisturizer, foundation, lipstick, hand cream and body lotion that contain SPF 30. These should be used in addition to a broad spectrum sunscreen.
- Apply an SPF 30+ lip balm.
- Consult the UV Index daily reports, and take appropriate precautions based on predicted UV levels.
- Avoid indoor tanning. The sun, tanning beds, and sun lamps expose you to harmful ultraviolet (UV) rays. These rays accelerate skin aging.
- Apply moisturizer every day. As you age, skin becomes drier. Fine lines and wrinkles appear. Moisturizer traps water in our skin, giving it a more youthful appearance. For best results, use a facial moisturizer, body moisturizer, and lip balm.
- Wash away dirt and grime twice a day. How you wash your face can affect your appearance. For best results, you want to wash with warm water and a mild cleanser rather than soap. You also should avoid scrubbing your skin clean.
- Stop smoking. Tobacco smoke contains toxins that can lead to smoker’s face. Signs of smoker’s face include dull and dry complexion, loss of skin’s firmness, premature lines and wrinkles, and leathery skin.
- Eat healthy foods. A healthy diet promotes healthy skin. Make sure you eat plenty of fruits and vegetables, lean proteins, and healthy fats.
- Get enough sleep. It’s called beauty rest for a reason. Sleep gives your body time to refresh and renew itself.
Given that ultraviolet radiation is the major environmental risk factor for the development of skin cancers – as well as for sunburn and signs of photoaging that include rhytides, telangiectasia, and dyspigmentation – dermatologists employ a multi-pronged approach to minimizing ultraviolet radiation exposure 11. Strategies to minimize ultraviolet radiation exposure include lifestyle modifications, ultraviolet radiation protective clothing, and topically applied sun-protective products, i.e. sunscreen.
There are two major types of UV light in relation to skin cancer:
- UVB that is the main cause of sunburn and non-melanoma skin cancers.
- UVA that is also carcinogenic and the main cause of photo-ageing.
Sunscreens are either:
- Physical Sunscreens that physically reflect both UVA and UVB. Typical ingredients are Zinc Oxide or Titanium Dioxide.
- Organic Sunscreens that absorb different types of UV radiation. Examples are octinoxate, salicylates or benzophenones.
Wearing sunscreen every day can do more than prevent skin cancer — it can prevent signs of photoaging as well. In fact, many people tout sunscreen for being their go-to antiaging weapon, and for good reason. Regular use has been shown to keep photodamage at bay for a longer period of time.
Some sunscreens now contain DNA repair enzymes that help undo previous damage by using nearby undamaged DNA to fix the area. A 2017 study 12 in the Journal of Drugs in Dermatology showed these products can enhance antiaging regimens and, more specifically, reduce risk of developing actinic keratoses.
If you’re already experiencing some signs of photoaging, you’ll also want to incorporate skin care products designed to reverse sun damage. Certain ingredients such as vitamin C and E and green tea are antioxidants that stabilize the skin and help brighten dark spots. An antiaging hero, retinol, used nightly, will boost cell turnover to create a healthy and youthful appearance.
Vitamin B3
Vitamin B3 also called Nicotinamide and there has been evidence for some time that Vitamin B3 can help protect the skin from UV light.
There’s good news. A trial published in the coveted New England Journal of Medicine 2015 (probably the most highly respected medical journal in the world) was very encouraging 13. People who had at least two non-melanoma skin cancers in the previous 5 years were randomized to either placebo or Nicotinamide 500mg twice daily. After 12 months, there were 23% fewer non-melanoma skin cancers in those who had taken the nicotinamide.
What does this mean? There is solid evidence to recommend Vitamin B3 (Nicotinamide) 500mg twice daily in anyone who has had at least 2 skin cancers in the last 5 years. This includes basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). The same dose of Vitamin B3 had previously been reported to reduce Sunspots in people with pre-existing solar keratosis.
You can buy Vitamin B3 tablets at the chemist & there are a variety of brands to choose from. Just make sure you get the 500mg strength tablet.
Skin antioxidants protect against ultraviolet radiation
Ultraviolet radiation exposure affects the skin antioxidants. Ascorbate, glutathione, superoxide dismutase, catalase, and ubiquinol are depleted in all layers of the UVB-exposed skin. Studies of cultured skin cells and murine skin in vivo have indicated that ultraviolet radiation-induced damage involves the generation of ROS and depletion of endogenous antioxidants 14. In the study by Shindo et al. 15, enzymatic and nonenzymatic antioxidants in the epidermis and dermis and their responses to ultraviolet light of hairless mice were compared. Mice were exposed to solar light and subsequently examined for UV-induced damage of their skin. After irradiation, epidermal and dermal catalase and superoxide dismutase activities were greatly decreased. Alpha-tocopherol, ubiquinol 9, ubiquinone 9, ascorbic acid, dehydroascorbic acid, and reduced glutathione decreased in both epidermis and dermis by 26% to 93%. Oxidized glutathione showed a slight nonsignificant increase. Because the reduction in total ascorbate and catalase was much more prominent in epidermis than dermis, the authors concluded that UV light is more damaging to the antioxidant defences in the epidermis than in the dermis. Many other studies confirmed that acute exposure of human skin to ultraviolet radiation in vivo leads to oxidation of cellular biomolecules that could be prevented by prior antioxidant treatment. There have been many studies performed where different antioxidants or combinations of antioxidants and different phytochemicals were tested in order to find evidence against reactive oxygen species (ROS)-induced damage. Some of them are presented in Tables 1 and and 2.
Table 1. Exogenous antioxidants with photoprotective or damage protective effects
| Antioxidants | Outcome of the study | Study |
|---|---|---|
| Ascorbic acid | Topical vitamin C 5% cream applied for six months led to clinical improvement in the appearance of photoaged skin | |
| Topical vitamin C stimulates the collagen-producing activity of the dermis | ||
| Magnesium ascorbyl phosphate administration immediately after exposure in hairless mice significantly delayed skin tumor formation and hyperplasia induced by chronic exposure to UV radiation | Elmore, 2005 16. | |
| Ascorbic acid was a photoprotectant when applied to mice and pig skin before exposure to ultraviolet (UV) radiation | Elmore, 2005 16. | |
| Vitamin E | UV-induced vitamin E depletion | Packer and Valacchi, 2002 17 |
| The interaction of vitamin E with the eicosanoid system may result in an anti-inflammatory effect and thereby complement the photoprotective effects of other antioxidants in the skin | Boelsma et al., 2001 18 | |
| Vitamin E has skin barrier-stabilizing properties | Packer et al., 2001 19 | |
| Lycopene | UV light decreased skin lycopene concentrations more so than skin β-carotene concentrations | Ribaya-Mercadoet al., 1995 20 |
| Lycopene protects against UV-induced erythema in humans | ||
| Carotenoids (carotene, β-carotene, and carotenoid mix) | Carotenoids are efficient in photoprotection, scavenging singlet oxygen, and peroxyl radicals. Supplements or a carotenoid-rich diet decreased sensitivity against UV-induced erythema | Sies and Stahl, 2004 21 |
| Supplementation with carotenoids contributes to basal protection of the skin but is not sufficient to obtain complete protection against severe UV irradiation | Stahl and Krutmann, 2006 22 | |
| Dietary beta-carotene has effect on wrinkles and elasticity, procollagen gene expression, and ultraviolet (UV)-induced DNA damage in human skin | Cho et al., 2010 23 | |
| Erythema-protective effect of a carotenoid mix inhibited serum lipid peroxidation | Heinrich et al., 1998 24, Heinrich et al., 2003 25, Lee et al., 2000 26 | |
| Presupplementation with β-carotene before and during sunlight exposure provides protection against sunburn | Gollnick et al., 1996 27 | |
| Inhibition of UV-induced epidermal damage and tumor formation in mouse models | Mathews-Roth and Krinsky, 1987 28 | |
| Tretinoin | Topical tretinoin ameliorates the clinical signs of photoaging | Cordero, 1983 29, Kligman et al., 1986 30 |
| The treatment of photodamaged skin with tretinoin increased collagen I formation. | Griffiths et al., 1993 31 | |
| Topical tretinoin is safe and effective in the treatment of photodamage | Gilchrest, 1997 32 | |
| Improvement in photodamaged skin | Weinstein et al., 1991 33 | |
| Topical tretinoin reduced the effects of photoaging | Voorhees, 1990 34 | |
| Topical tretinoin in combination with sun protection as a useful approach to the treatment of sun-damaged skin | Leyden, 1998 35 | |
| Coenzyme Q10 (CoQ10) | Topical application of CoQ10 has the beneficial effect of preventing photoaging | Hoppe et al., 1999 36 |
| Coenzyme Q10 protects against oxidative stress-induced cell death and enhances the synthesis of basement membrane components in dermal and epidermal cells | Muta-Takada et al., 2009 37 | |
| CoQ10 was shown to reduce UVA-induced MMPs in cultured human dermal fibroblasts | Inui et al., 2008 38 | |
| Glutathione | Glutathione is a photoprotective agent in skin cells | Connor and Wheeler, 1987 39 |
| Zinc | Zn-treated fibroblasts were more resistant to UVR than cells grown in normal medium | Richard et al., 1993 40 |
| Zn can positively influence the effects of oxidative stress on cultured human retinal pigment epithelial (RPE) cells | Tate et al., 1999 41 | |
| Resveratrol | Application of resveratrol to the skin of hairless mice effectively prevented the UVB-induced increase in skin thickness and the development of the skin edema | Afaq and Mukhtar, 2002 42 |
| Green tea | Green tea polyphenols were shown to reduce UV light-induced oxidative stress and immunosuppression | Katiyar et al., 2000 43 |
| Topical treatment or oral consumption of green tea polyphenols (GTP) inhibits chemical carcinogen- or UV radiation-induced skin carcinogenesis in different laboratory animal models | Katiyar, 2003 44 | |
| Green tea or caffeine | Oral administration of green tea or caffeine in amounts equivalent to three or five cups of coffee per day to UVB-exposed mice increased levels of p53, slowed cell cycling, and increased apoptotic sun burn cells in the epidermis | Lu et al., 2008 45 |
| Sylimarin | Silymarin strongly prevents both photocarcinogenesis and skin tumor promotion in mice | Singh and Agarwal, 2002 46 |
| Skin cancer chemopreventive effects | Ahmad et al., 1998 47 | |
| Genistein | Antioxidant and anticarcinogenic effects on skin | Wei et al., 1995 48 |
| Cocoa | Dietary flavanols from cocoa contribute to endogenous photoprotection, improve dermal blood circulation, and affect cosmetically relevant skin surface and hydration variables | Heinrich et al., 2006 49 |
| Photoprotection against UV-induced erythema | Heinrich et al., 2006 49 | |
Table 2. Exogenous antioxidant’s mixtures with photoprotective or damage protective effects
| Antioxidant mixtures | Outcome of the study | Study |
|---|---|---|
| Oral vitamin E and beta-carotene supplementation | Ultraviolet radiation-induced oxidative stress in human skin | McArdle et al., 2004 50 |
| Carotenoids and tocopherols | Scavenging reactive oxygen species generated during photooxidative stress | Stahl et al., 2000 51 |
| Beta-carotene, lutein, and lycopene | UV irradiation induced intensity of erythema was diminished | Albanes et al., 1996 52 |
| Tomato extract and a drink containing solubilized Lyc-o-Mato | Reduction in erythema formation following UV irradiation | Aust et al., 2005 53 |
| Quercetin, hesperetin and naringenin | Protective agents in certain skin diseases caused, initiated, or exacerbated by sunlight irradiation | Bonina et al., 1996 54 |
| α-Tocopherol and ascorbate | MEDs increased markedly after intake of the combination of α-tocopherol and ascorbate | Fuchs and Kern, 1998 55 |
| Combination of vitamins C and E | Mean MEDs increased in group receiving vitamins compared with baseline | Eberlein-Konig et al., 1998 56 |
| Vitamin C, vitamin E, lycopene, beta-carotene, the rosemary polyphenol, and carnosic acid | Vitamin C, vitamin E, and carnosic acid showed photoprotective potential human dermal fibroblasts exposed to ultraviolet-A (UVA) | Offord et al., 2002 57 |
| Lycopene, beta-carotene, alpha-tocopherol, and selenium | Many parameters of the epidermal defense against UV-induced damage were significantly improved | Cesarini et al., 2003 58 |
| β-Carotene, lycopene, tocopherol, and ascorbic acid | Significant increase of melanin concentrations in skin was found | Postaire et al., 1997 59 |
| Carotenoids (beta-carotene and lycopene), vitamins C and E, selenium, and proanthocyanidins | A selective protection of the skin against irradiation was confirmed | Greul et al., 2002 60 |
Compounds derived from the diet with photoaging or damage protective effects
Natural antioxidants are generally considered to be beneficial fruit and vegetable components. It seems that skin’s antioxidative defence is also influenced by nutritive factors. Besides vitamins A, C, and E, η-3 fatty acids certain nonvitamin plant-derived ingredients might have beneficial effect on skin aging, skin sun protection, or skin cancer. The laboratory studies conducted in animal models suggest that many plant compounds have the ability to protect the skin from the adverse effects of ultraviolet radiation. The proliferation of products, however, can cause confusion among consumers, who often ask their dermatologists for advice as to which antiaging products they should choose. Ideally, the antiaging claims of cosmeceutical formulations and their components should be demonstrated in controlled clinical trials 61, but there is a lack of such studies due to their high costs. Since cosmeceutical products are claiming that they therapeutically affect the structure and function of the skin, it is rational and necessary to hold them to specified scientific standards that substantiate efficacy claims 62.
Many studies have found that vitamin C can increase collagen production, protect against damage from UVA and UVB rays, correct pigmentation problems, and improve inflammatory skin conditions (Table 1) 63.
Topical retinoids remain the mainstay for treating photoaging given their proven efficacy in both clinical and histological outcomes. The application of retinoids might not only clinically and biochemically repair photoaged skin, but their use might also prevent photoaging 64. Retinoid-mediated improvement of photoaging is associated with increased collagen I synthesis 31, reorganization of packed collagen fibres 65, and increased number of type VII anchoring fibrils 66. However, up to 92% of subjects who used tretinoin in various clinical studies have reported “retinoid dermatitis,” that is, erythema and scaling at the site of application 67. Irritation can be minimized by reducing dose and frequency of treatments.
It seems that the biochemistry of CoQ10 may inhibit the production of IL-6, which stimulates fibroblasts in dermis by paracrine manner to upregulate MMPs production, and contribute to protecting dermal fibrous components from degradation, leading to rejuvenation of wrinkled skin 68. It was reported that CoQ10 strongly inhibits oxidative stress in the skin induced by UVB via increasing SOD2 and GPx 69. It was reported that it is considered that CoQ10 appears to have also a cutaneous healing effect in vivo 70.
Green tea polyphenols have received attention as protective agents against UV-induced skin damage. Analysis of published studies demonstrates that green tea polyphenols have anti-inflammatory and anticarcinogenic as well as anti-aging properties. These effects appear to correlate with antioxidant properties of green tea polyphenols, which could be used as new photoprotection agents (Table 1).
A number of experimental studies indicate protective effects of beta-carotene against acute and chronic manifestations of skin photodamage. However, most clinical studies have failed to convincingly demonstrate its beneficial effects so far. Studies on skin cells in culture have revealed that beta-carotene acts not only as an antioxidant but also has unexpected prooxidant properties 71. For this reason, further studies with focus on in vivo β-carotene-induced prooxidative properties and its relevance on human health are needed. Another problem represents the dosage. Although studies convincingly showed that vitamin supplementation effectively protects the skin against sunburn, the doses of vitamins used were generally much higher than amounts generally ingested from habitual diets 18. Additionally, it was shown that the combination of different antioxidants applied simultaneously can provide a synergistic effect 63. Antioxidants are most effective when used in combination (Table 2). Vitamin C regenerates vitamin E, and selenium and niacin are required to keep glutathione in its active form. It has been demonstrated that vitamin C can regenerate α-tocopherol from its chromanoxyl radical 72 and that the vitamin C radical may be recycled by glutathione nonenzymatically under slightly acidic conditions 73 that are present in the stratum corneum 74. Werninghaus et al. 75 reported that vitamin E given orally at 400 IU/day for a period of six months affords no significant increase in UV protection. Similarly, in a study with 12 volunteers, vitamin C given at 500 mg/day over eight weeks had no effect on the UV-induced erythemal response 50, indicating again the importance of antioxidants to be supplemented together to obtain the synergistic effect.
Photoaging signs and symptoms
The effects of photoaging can manifest in many ways. Melasma, freckles, actinic keratoses and texture changes are all signs of photoaging damage. The type of damage you’ll have, however, is unpredictable and dependent on the individual.
For example, sun exposure (and hormonal changes) can cause melasma, which is a condition causing grayish-brown patches to appear on skin. Actinic keratoses or precancerous spots, directly correlate to chronic sun exposure, which can increase your chance of developing skin cancer. Textural changes in the form of deep lines, waxiness or a leather-looking appearance can lead to uneven, dull looking skin. Remember the cute freckles you got as kids? Those were actually warning signs from your body saying you’d had a lot of sun exposure. Broken blood vessels that exist as redness or blotchiness on the nose, cheeks or neck may resemble a slight burn and are another sign of sun damage.
Photoaging appears on the most visible parts of the body — face, neck and back of the hand. These areas often receive significant sun exposure. In women, the exposed upper chest is another area where photoaging is seen. The lips can also show signs of excessive sun damage.
The acute response of the skin to exposure to ultraviolet radiation has rapid onset (minutes to days) and short duration (hours to weeks).
- Redness (sunburn)
- Immediate pigmentation (due to ultraviolet-A [UVA] and visible light in darker skin types)
- Delayed pigmentation (suntan)
- Vitamin D production from precursors
- Skin thickening
Redness mainly results from ultraviolet-B (UVB) i.e. wavelengths <320nm. It arises from dilation of the superficial blood vessels produced by cytokines. Solar-induced erythema is delayed by a few hours after exposure. Delayed tanning is noticeable two days after exposure and most intense a week afterwards. It is due to melanogenesis and distribution of melanin to keratinocytes throughout the epidermis. UVA and even visible radiation may cause melanogenesis, but UVB is the most effective in initiating it.
Further exposure to ultraviolet radiation causes less damage:
- Melanin absorbs the ultraviolet radiation preventing it from reaching lower layers of the skin;
- Epidermal keratinocytes proliferate so the skin becomes thicker (acanthosis).
UVB converts precursors in the skin into vitamin-D. The liver, then the kidneys, change vitamin-D into calcitriol (1,25 dihydroxycholecalciferol), which is required for calcium homeostasis.
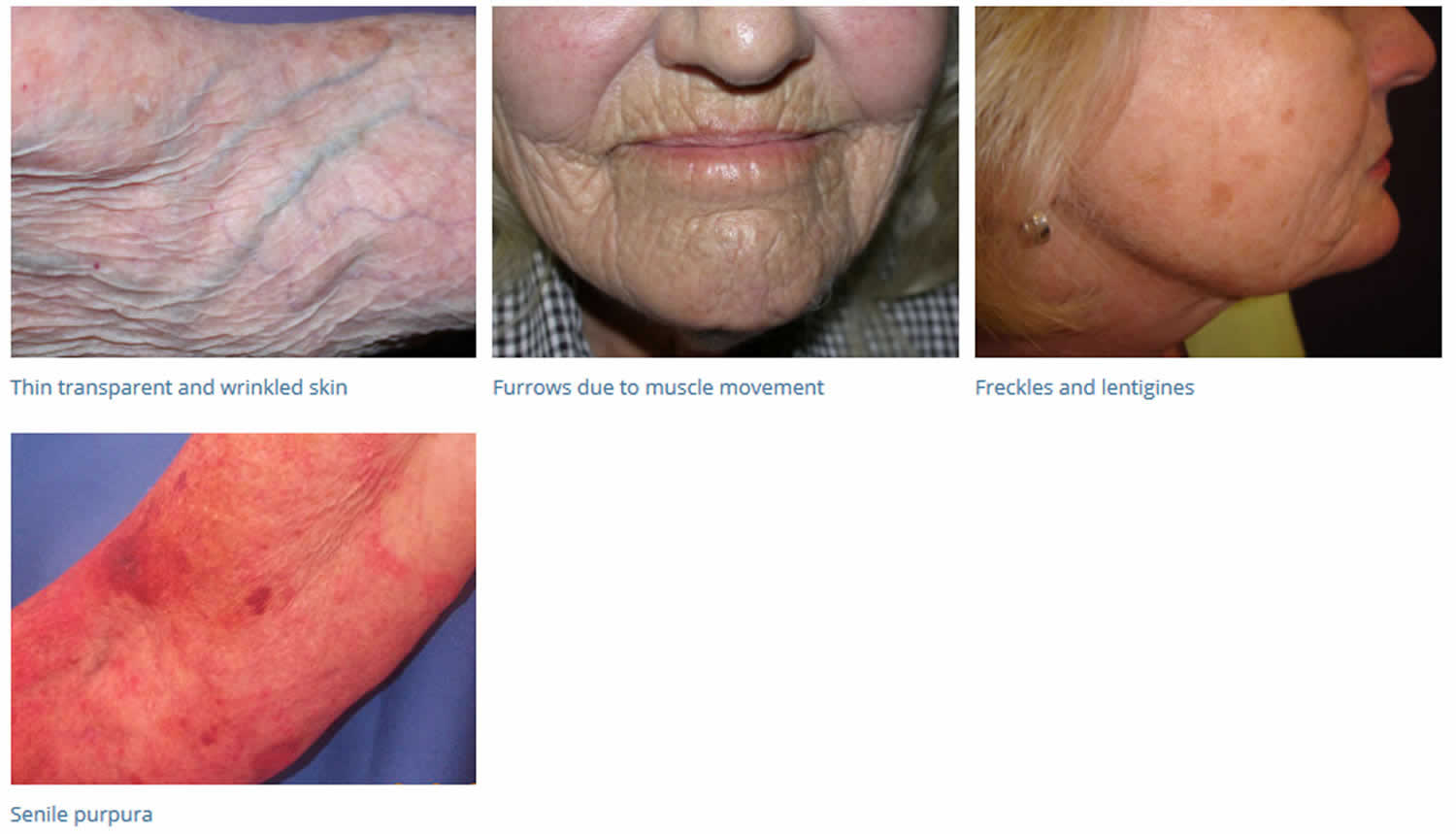
Photoaging or sun damage includes:
- Dry coarse leathery appearance
- General loss of skin tone in sun-exposed areas or loss of skin elasticity
- With continued sun exposure over several years, wrinkles around the eyes and mouth increase in number and become deep creases; forehead frown lines set in and are visible when not frowning
- Dilated capillaries and easy bruising (senile purpura)
- Spider veins on the nose, cheeks and neck
- Thin, transparent, fragile tissue
- Various pigmented spots, such as freckles, solar lentigines (known as age or liver spots), and uneven skin color
- Red, rough scaly spots called actinic (sun-related) keratoses may appear; these may be precancerous and require treatment
- Skin cancer (melanoma, basal cell carcinoma, squamous cell carcinoma)
Glogau skin types
Glogau skin types refer to the degree of photoaging:
- Mild (age 28-35 years): Few wrinkles, no keratoses
- Moderate (age 35-50 years): Early wrinkling, sallow complexion with early actinic keratoses
- Advanced (age 50-60 years): Persistent wrinkling, discolouration of the skin with telangiectases and actinic keratoses
- Severe (age 65-70 years): Severe wrinkling, photoaging, gravitational and dynamic forces affecting skin, actinic keratoses with or without skin cancer
Skin cancers are due to progressive mutations in DNA. They are induced by:
- UVB definitely
- UVA probably
- Injury, sometimes.
Figure 7. Photoaging signs
Photoaging diagnosis
The features of ageing skin are diagnosed clinically. Lesions suspicious of skin cancer present as growing lumps or sores that fail to heal. Such lesions often undergo diagnostic biopsy before or as part of treatment.
Photoaging treatment
Various treatments available for sun-damaged skin include: injections of botulinum toxin, dermal fillers, laser treatment, dermabrasion and chemical peels. Some skin preparations can help restore skin to a more youthful appearance (vitamin A preparations).
A certified dermatologist can help you decide which treatment regimen will work best for you.
Cancerous and precancerous lesions
- Actinic keratoses and intraepidermal squamous cell carcinomas (SCCs) are most often removed by cryotherapy or treated topically.
- Basal cell carcinoma (BCC) is most often removed by minor surgery. Superficial BCC can be treated topically or by cryotherapy.
- Cutaneous squamous cell carcinoma and melanoma are nearly always surgically excised.
Dry and discolored skin
- Moisturizers will help improve dry and flaky skin.
- Alpha hydroxy acids, vitamin C, lipoic acid, soy isoflavones or retinoid creams applied regularly long term reduce dryness. They may also reduce the number of fine wrinkles and even out pigmentation.
- Many other products are under investigation, but their benefits are unclear.
Facial rejuvenation
Procedures that aim to rejuvenate photoaged skin include:
- Fillers (eg, hyaluronic acid, polytetrafluoroethylene and fat grafts) to disguise facial expression lines
- Botulinum toxin injections to reduce frowning and lessen deep furrows
- Vascular laser treatment and sclerotherapy (the injection of inflammatory agent into veins) to remove facial veins and angiomas
- Resurfacing procedures (eg, dermabrasion, chemical peels, and laser resurfacing)
- Cosmetic surgery to remove redundant sagging skin, including surgical or laser blepharoplasty for baggy eyelids, and meloplasty (face lift) to tighten jowls.
- Yaar M, Lee MS, Rünger TM, Eller MS, Gilchrest B. Telomere mimetic oligonucleotides protect skin cells from oxidative damage. Annales de Dermatologie et de Vénéréologie. 2002;129:1–18.[↩]
- Pandel R, Poljšak B, Godic A, Dahmane R. Skin photoaging and the role of antioxidants in its prevention. ISRN Dermatol. 2013;2013:930164. Published 2013 Sep 12. doi:10.1155/2013/930164 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3789494[↩][↩][↩]
- Yaar M, Eller MS, Gilchrest BA. Fifty years of skin aging. Journal of Investigative Dermatology Symposium Proceedings. 2002;7(1):51–58.[↩]
- Helfrich YR, Sachs DL, Voorhees JJ. Overview of skin aging and photoaging. Dermatology Nursing. 2008;20(3):177–184.[↩]
- Fisher GJ, Kang S, Varani J, et al. Mechanisms of photoaging and chronological skin aging. Archives of Dermatology. 2002;138(11):1462–1470.[↩]
- Grether-Beck S, Marini A, Jaenicke T, Krutmann J. Photoprotection of human skin beyond ultraviolet radiation. Photodermatol Photoimmunol Photomed. 2014;30(2-3):167–174. doi:10.1111/phpp.12111 https://doi.org/10.1111/phpp.12111[↩]
- Yano K, Oura H, Detmar M. Targeted overexpression of the angiogenesis inhibitor thrombospondin-1 in the epidermis of transgenic mice prevents ultraviolet-B-induced angiogenesis and cutaneous photo-damage. Journal of Investigative Dermatology. 2002;118(5):800–805.[↩]
- Halliwell B, Gutteridge J. Free Radicals in Biology and Medicine. 4th edition. New York, NY, USA: Oxford University Press; 2007.[↩]
- Laurent-Applegate LE, Schwarzkopf S. Photooxidative stress in skin and regulation of gene expression. In: Fuchs J, Packer L, editors. Environmental Stressors in Health and Disease. New York, NY, USA: Marcel Dekker; 2001.[↩]
- Grether-Beck S, Wlaschek M, Krutmann J, Scharffetter-Kochanek K. Photodamage and photoaging—prevention and treatment. Journal der Deutschen Dermatologischen Gesellschaft. 2005;3(2):S19–S25.[↩]
- Rittie L, Fisher GJ. Natural and sun-induced aging of human skin. Cold Spring Harb Perspect Med. 2015;5(1):a015370.[↩]
- A Novel Technology: Sunscreen With Actinic Damage Repair. May 2017, Vol 16, Issue 5https://jddonline.com/articles/dermatology/S1545961617S0059X/1[↩]
- A Phase 3 Randomized Trial of Nicotinamide for Skin-Cancer Chemoprevention. N Engl J Med 2015; 373:1618-1626 DOI: 10.1056/NEJMoa1506197[↩]
- McArdle F, Rhodes LE, Parslew R, Jack CIA, Friedmann PS, Jackson MJ. UVR-induced oxidative stress in human skin in vivo: effects of oral vitamin C supplementation. Free Radical Biology and Medicine. 2002;33(10):1355–1362.[↩]
- Shindo Y, Witt E, Packer L. Antioxidant defense mechanisms in murine epidermis and dermis and their responses to ultraviolet light. Journal of Investigative Dermatology. 1993;100(3):260–265.[↩]
- Elmore AR. Final report of the safety assessment of L-ascorbic acid, calcium ascorbate, magnesium ascorbate, magnesium ascorbyl phosphate, sodium ascorbate, and sodium ascorbyl phosphate as used in cosmetics. International Journal of Toxicology. 2005;24(2):51–111.[↩][↩]
- Packer L, Valacchi G. Antioxidants and the response of skin to oxidative stress: vitamin E as a key indicator. Skin Pharmacology and Applied Skin Physiology. 2002;15(5):282–290.[↩]
- Boelsma E, Hendriks HFJ, Roza L. Nutritional skin care: health effects of micronutrients and fatty acids. American Journal of Clinical Nutrition. 2001;73(5):853–864.[↩][↩]
- Packer L, Weber SU, Rimbach G. Molecular aspects of α-tocotrienol antioxidant action and cell signalling. Journal of Nutrition. 2001;131(2):369S–373S.[↩]
- Ribaya-Mercado JD, Garmyn M, Gilchrest BA, Russell RM. Skin lycopene is destroyed preferentially over β-carotene during ultraviolet irradiation in humans. Journal of Nutrition. 1995;125(7):1854–1859.[↩]
- Sies H, Stahl W. Carotenoids and UV protection. Photochemical and Photobiological Sciences. 2004;3(8):749–752.[↩]
- Stahl W, Krutmann J. Systemic photoprotection through carotenoids. Hautarzt. 2006;57(4):281–285.[↩]
- Cho S, Lee DH, Won C-H, et al. Differential effects of low-dose and high-dose beta-carotene supplementation on the signs of photoaging and type I procollagen gene expression in human skin in vivo . Dermatology. 2010;221(2):160–171.[↩]
- Heinrich U, Wiebusch M, Tronnier H. Photoprotection from ingested carotenoids. Cosmetics & Toiletries. 1998;113:61–70.[↩]
- Heinrich U, Gärtner C, Wiebusch M, et al. Supplementation with β-carotene or a similar amount of mixed carotenoids protects humans from UV-induced erythema. Journal of Nutrition. 2003;133(1):98–101.[↩]
- Lee J, Jiang S, Levine N, Watson RR. Carotenoid supplementation reduces erythema in human skin after simulated solar radiation exposure. Proceedings of the Society for Experimental Biology and Medicine. 2000;223(2):170–174.[↩]
- Gollnick HPM, Hopfenmüller W, Hemmes C, et al. Systemic beta carotene plus topical UV-sunscreen are an optimal protection against harmful effects of natural UV-sunlight: results of the Berlin-Eilath study. European Journal of Dermatology. 1996;6(3):200–205.[↩]
- Mathews-Roth MM, Krinsky NI. Carotenoids affect development of UV-B induced skin cancer. Photochemistry and Photobiology. 1987;46(4):507–509.[↩]
- Cordero A., Jr. La vitamina a acida en la piel senile. Actualizaciones Ter Dermatologica. 1983;6:49–54.[↩]
- Kligman AM, Grove GL, Hirose R, Leyden JJ. Topical tretinoin for photoaged skin. Journal of the American Academy of Dermatology. 1986;15(4):836–859.[↩]
- Griffiths CEM, Russman AN, Majmudar G, Singer RS, Hamilton TA, Voorhees JJ. Restoration of collagen formation in photodamaged human skin by tretinoin (retinoic acid) The New England Journal of Medicine. 1993;329(8):530–535.[↩][↩]
- Gilchrest BA. Treatment of photodamage with topical tretinoin: an overview. Journal of the American Academy of Dermatology. 1997;36(3, part 2):S27–S36.[↩]
- Weinstein GD, Nigra TP, Pochi PE, et al. Topical tretinoin for treatment of photodamaged skin: a multicenter study. Archives of Dermatology. 1991;127(5):659–665.[↩]
- Voorhees JJ. Clinical effects of long-term therapy with topical tretinoin and cellular mode of action. Journal of International Medical Research. 1990;18(3):26C–28C.[↩]
- Leyden JJ, Heffel DF, Miller TA. Treatment of photodamaged skin with topical tretinoin: an update. Plastic and Reconstructive Surgery. 1998;102(5):1672–1675.[↩]
- Hoppe U, Bergemann J, Diembeck W, et al. Coenzyme Q10, a cutaneous antioxidant and energizer. BioFactors. 1999;9(2-4):371–378.[↩]
- Muta-Takada K, Terada T, Yamanishi H, et al. Coenzyme Q10 protects against oxidative stress-induced cell death and enhances the synthesis of basement membrane components in dermal and epidermal cells. BioFactors. 2009;35(5):435–441.[↩]
- Inui M, Ooe M, Fujii K, Matsunaka H, Yoshida M, Ichihashi M. Mechanisms of inhibitory effects of CoQ10 on UVB-induced wrinkle formation in vitro and in vivo . BioFactors. 2008;32(1-4):237–243.[↩]
- Connor MJ, Wheeler LA. Depletion of cutaneous glutathione by ultraviolet radiation. Photochemistry and Photobiology. 1987;46(2):239–245.[↩]
- Richard M-J, Guiraud P, Leccia M-T, Beani J-C, Favier A. Effect of zinc supplementation on resistance of cultured human skin fibroblasts toward oxidant stress. Biological Trace Element Research. 1993;37(2-3):187–199.[↩]
- Tate DJ, Jr., Miceli MV, Newsome DA. Zinc protects against oxidative damage in cultured human retinal pigment epithelial cells. Free Radical Biology and Medicine. 1999;26(5-6):704–713.[↩]
- Afaq F, Mukhtar H. Photochemoprevention by botanical antioxidants. Skin Pharmacology and Applied Skin Physiology. 2002;15(5):297–306.[↩]
- Katiyar SK, Ahmad N, Mukhtar H. Green tea and skin. Archives of Dermatology. 2000;136(8):989–994.[↩]
- Katiyar SK. Skin photoprotection by green tea: antioxidant and immunomodulatory effects. Current drug targets. Immune, endocrine and metabolic disorders. 2003;3(3):234–242.[↩]
- Lu Y-P, Lou Y-R, Peng Q-Y, Xie J-G, Nghiem P, Conney AH. Effect of caffeine on the ATR/Chk1 pathway in the epidermis of UVB-irradiated mice. Cancer Research. 2008;68(7):2523–2529.[↩]
- Singh RP, Agarwal R. Flavonoid antioxidant silymarin and skin cancer. Antioxidants and Redox Signaling. 2002;4(4):655–663.[↩]
- Ahmad N, Gali H, Javed S, Agarwal R. Skin cancer chemopreventive effects of a flavonoid antioxidant silymarin are mediated via impairment of receptor tyrosine kinase signaling and perturbation in cell cycle progression. Biochemical and Biophysical Research Communications. 1998;247(2):294–301.[↩]
- Wei H, Bowen R, Cai Q, Barnes S, Wang Y. Antioxidant and antipromotional effects of the soybean isoflavone genistein. Proceedings of the Society for Experimental Biology and Medicine. 1995;208(1):124–130.[↩]
- Heinrich U, Neukam K, Tronnier H, Sies H, Stahl W. Long-term ingestion of high flavanol cocoa provides photoprotection against UV-induced erythema and improves skin condition in women. Journal of Nutrition. 2006;136(6):1565–1569.[↩][↩]
- McArdle F, Rhodes LE, Parslew RAG, et al. Effects of oral vitamin E and β-carotene supplementation on ultraviolet radiation-induced oxidative stress in human skin. American Journal of Clinical Nutrition. 2004;80(5):1270–1275.[↩][↩]
- Stahl W, Heinrich U, Jungmann H, Sies H, Tronnier H. Carotenoids and carotenoids plus vitamin E protect against ultraviolet light-induced erythema in humans. American Journal of Clinical Nutrition. 2000;71(3):795–798.[↩]
- Albanes D, Heinonen OP, Taylor PR, et al. α-tocopherol and β-carotene supplements and lung cancer incidence in the alpha-tocopherol, beta-carotene cancer prevention study: effects of base- line characteristics and study compliance. Journal of the National Cancer Institute. 1996;88(21):1560–1570.[↩]
- Aust O, Stahl W, Sies H, Tronnier H, Heinrich U. Supplementation with tomato-based products increases lycopene, phytofluene, and phytoene levels in human serum and protects against UV-light-induced erythema. International Journal for Vitamin and Nutrition Research. 2005;75(1):54–60.[↩]
- Bonina F, Lanza M, Montenegro L, et al. Flavonoids as potential protective agents against photo-oxidative skin damage. International Journal of Pharmaceutics. 1996;145(1-2):87–94.[↩]
- Fuchs J, Kern H. Modulation of UV-light-induced skin inflammation by D-alpha-tocopherol and L-ascorbic acid: a clinical study using solar simulated radiation. Free Radical Biology and Medicine. 1998;25(9):1006–1012.[↩]
- Eberlein-Konig B, Placzek M, Przybilla B. Protective effect against sunburn of combined systemic ascorbic acid (vitamin C) and d-α-tocopherol (vitamin E) Journal of the American Academy of Dermatology. 1998;38(1):45–48.[↩]
- Offord EA, Gautier J-C, Avanti O, et al. Photoprotective potential of lycopene, β-carotene, vitamin E, vitamin C and carnosic acid in UVA-irradiated human skin fibroblasts. Free Radical Biology and Medicine. 2002;32(12):1293–1303.[↩]
- Césarini JP, Michel L, Maurette JM, Adhoute H, Béjot M. Immediate effects of UV radiation on the skin: modification by an antioxidant complex containing carotenoids. Photodermatology Photoimmunology and Photomedicine. 2003;19(4):182–189.[↩]
- Postaire E, Jungmann H, Bejot M, Heinrich U, Tronnier H. Evidence for antioxidant nutrients-induced pigmentation in skin: results of a clinical trial. Biochemistry and Molecular Biology International. 1997;42(5):1023–1033.[↩]
- Greul A-K, Grundmann J-U, Heinrich F, et al. Photoprotection of UV-irradiated human skin: an antioxidative combination of vitamins E and C, carotenoids, selenium and proanthocyanidins. Skin Pharmacology and Applied Skin Physiology. 2002;15(5):307–315.[↩]
- Bruce S. Cosmeceuticals for the attenuation of extrinsic and intrinsic dermal aging. Journal of Drugs in Dermatology. 2008;7(2, supplement):s17–s22.[↩]
- Levin J, del Rosso JQ, Momin SB. How much do we really know about our favorite cosmeceutical ingredients? Journal of Clinical and Aesthetic Dermatology. 2010;3(2):22–41.[↩]
- Poljsak B. Skin Aging, Antioxidants and Free Radicals. New York, NY, USA: Nova Science; 2012.[↩][↩]
- Serri R, Iorizzo M. Cosmeceuticals: focus on topical retinoids in photoaging. Clinics in Dermatology. 2008;26(6):633–635.[↩]
- Yamamoto O, Bhawan J, Solares G, Tsay AW, Gilchrest BA. Ultrastructural effects of topical tretinoin on dermo-epidermal junction and papillary dermis in photodamaged skin. A controlled study. Experimental Dermatology. 1995;4(3):146–154.[↩]
- Chen M, Goyal S, Cai X, O’Toole EA, Woodley DT. Modulation of type VII collagen (anchoring fibril) expression by retinoids in human skin cells. Biochimica et Biophysica Acta. 1997;1351(3):333–340.[↩]
- Rittie L, Fisher GJ, Voorhees J. Retinoid therapy for photoaging. In: Gilchrest B, Krutmann J, editors. Skin Aging. Berlin, Germany: Springer; 2006.[↩]
- Inui M, Ooe M, Fujii K, Matsunaka H, Yoshida M, Ichihashi M. Mechanisms of inhibitory effects of CoQ10 on UVB-induced wrinkle formation in vitro and in vivo . BioFactors. 2008;32(1–4):237–243.[↩]
- Kim D-W, Hwang IK, Kim DW, et al. Coenzyme Q10 effects on manganese superoxide dismutase and glutathione peroxidase in the hairless mouse skin induced by ultraviolet B irradiation. BioFactors. 2007;30(3):139–147.[↩]
- Choi BS, Song HS, Kim HR, et al. Effect of coenzyme Q10 on cutaneous healing in skin-incised mice. Archives of Pharmacal Research. 2009;32(6):907–913.[↩]
- Biesalski HK, Obermueller-Jevic UC. UV light, beta-carotene and human skin—beneficial and potentially harmful effects. Archives of Biochemistry and Biophysics. 2001;389(1):1–6.[↩]
- Packer JE, Slater TF, Willson RL. Direct observation of a free radical interaction between vitamin E and vitamin C. Nature. 1979;278(5706):737–738.[↩]
- Stocker R, Weidemann MJ, Hunt NH. Possible mechanisms responsible for the increased ascorbic acid content of Plasmodium vinckei-infected mouse erythrocytes. Biochimica et Biophysica Acta. 1986;881(3):391–397.[↩]
- Ohman H, Vahlquist A. in vivo studies concerning a pH gradient in human stratum corneum and upper epidermis. Acta Dermato-Venereologica. 1994;74(5):375–379.[↩]
- Werninghaus K, Meydani M, Bhawan J, Margolis R, Blumberg JB, Gilchrest BA. Evaluation of the photoprotective effect of oral vitamin E supplementation. Archives of Dermatology. 1994;130(10):1257–1261.[↩]





{kind=link}