What is acne Acne, pimples or zits, is a chronic inflammatory disorder of pilosebaceous (sebaceous gland a small gland in the skin which secretes a lubricating
What is antiperspirant An antiperspirant is a chemical agent that reduces perspiration or sweating. The active ingredients of roll-on, spray and powder formulations are traditionally
What to do after a breakup A romantic relationship breakup, separation and divorce are one of the most stressful and emotional experiences in life. People
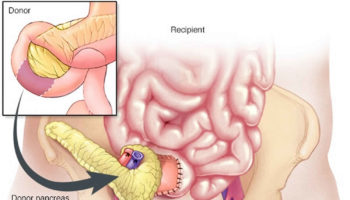
Can you get a pancreas transplant? Yes. More than 50,000 pancreas transplant have been performed worldwide (> 29,000 from the United States and >19,000 from
{kind=link}









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}