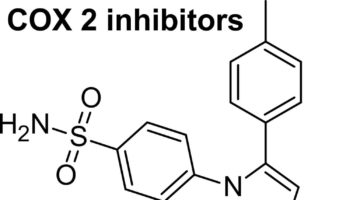
What is a COX-2 inhibitor COX-2 inhibitor is short for cyclooxygenase-2 selective inhibitor, is a non-steroidal anti-inflammatory drug (NSAID) that is the competitive inhibitor of
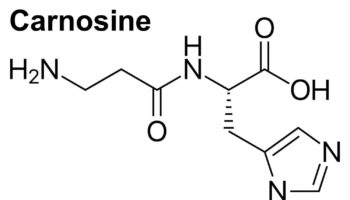
What is carnosine Carnosine (beta-alanyl-L-histidine) is a naturally occurring dipeptide neuropeptide (dipeptide of the amino acids beta-histidine and 3-methyl-L-histidine) found in mammalian tissues ((Hipkiss, A.R.;
What is sexsomnia Sexsomnia also called "sleep sex" or "atypical sexual behavior during sleep" or "somnambulistic sexual behavior", refers to sexual acts that are carried
What is overpronation Overpronation or excessive pronation or eversion in frontal plane at ankle joint in heel-toe running, refers to the tendency of the medial
What is pareidolia Pareidolia is the interpretation of previously unseen and unrelated objects as familiar due to previous learning ((Akdeniz G, Toker S, Atli I.
What is synesthesia Synesthesia is an extraordinary way of perceiving the world, involving experiences of connections between seemingly unrelated sensations, images or thoughts ((Brogaard B.
What are tonsil stones Tonsil stones are also known as tonsilloliths, are small white or yellow lumps of hardened material that can form in the palatine
{kind=link}





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}