
What is Ghee Butter ?
Ghee, also known as clarified butter or anhydrous milk fat, is prepared by heating butter or cream to just over 100°C to remove water content by boiling and evaporation, then filtering out the precipitated milk solids 1. Ghee has been utilized for thousands of years in Ayurveda as a therapeutic agent. In ancient India, ghee was the preferred cooking oil. In the last several decades, however, ghee has been implicated in the increased prevalence of coronary artery disease in Asian Indians due to its content of saturated fatty acids and cholesterol and, in heated ghee, cholesterol oxidation products 1.
The American Heart Association recommends limiting the consumption of saturated fats to less than 7% of energy to reduce the risk of cardiovascular disease 2.
Ghee is heavily utilized in Ayurveda for numerous medical applications, including the treatment of allergy, skin, and respiratory diseases. Many Ayurvedic preparations are made by cooking herbs into ghee. Ghee carries the therapeutic properties of herbs to all the body’s tissues. It is an excellent anupana (vehicle) for transporting herbs to the deeper tissue layers of the body 3. Proper digestion, absorption, and delivery to a target organ system are crucial in obtaining the maximum benefit from any therapeutic formulation; the lipophilic action of ghee facilitates transportation to a target organ and final delivery inside the cell since the cell membrane also contains lipid 4. A study that compared different forms of herbs and herb extracts found that the efficacy increased when they were used with ghee, compared to usage in powder or tablet form 5.
What is Saturated Fat ?
Saturated fat is a type of dietary fat. It is one of the unhealthy fats, along with trans fat. These fats are most often solid at room temperature. Foods like dairy butter, ghee butter, palm oil, palm kernel oil, beef tallow and coconut oil, cheese, pork lard and red meat have high amounts of saturated fat 6.
Too much saturated fat in your diet can lead to heart disease and other health problems.
In large randomized clinical trials that used polyunsaturated fat to replace saturated fat reduced the incidence of cardiovascular disease 7, 8. Cardiovascular disease is the leading global cause of death, accounting for 17.3 million deaths per year, comprising 31.5% of total global deaths in 2013. Nearly 808 000 people in the United States died of heart disease, stroke, and other cardiovascular diseases in 2014, translating to about 1 of every 3 deaths.
This large cohort study 9 found that higher intake of saturated fat (found in foods like butter, lard, tallow and red meat) and especially trans fat (predominantly from partially hydrogenated vegetable oil), was associated with greater risk of mortality (death) when compared with the same number of calories from carbohydrate. When compared with carbohydrates, every 5% increase of total calories from saturated fat was associated with an 8% higher risk of overall mortality, and every 2% higher intake of trans fat was associated with a 16% higher risk of overall mortality 9. The study investigated 83,349 women from the Nurses’ Health Study (July 1, 1980, to June 30, 2012) and 42,884 men from the Health Professionals Follow-up Study (February 1, 1986, to January 31, 2012) who were free of cardiovascular disease, cancer, and types 1 and 2 diabetes at baseline 9. Dietary fat intake was assessed at baseline and updated every 2 to 4 years. Information on mortality was obtained from systematic searches of the vital records of states and the National Death Index, supplemented by reports from family members or postal authorities. Of the 126,233 participants who were followed up for as long as 32 years, the study found that higher intakes of saturated fat and trans-fat were associated with increased mortality, whereas higher intakes of polyunsaturated (PUFA) and monounsaturated (MUFA) fatty acids were associated with lower mortality. Replacing 5% of energy from saturated fats with equivalent energy from PUFA and MUFA was associated with reductions in total mortality of 27% and 13%, respectively 9.
People who replaced saturated fats with carbohydrates had only slightly lower mortality risk. In addition, replacing total fat with carbohydrates was associated with modestly higher mortality. This was not surprising, the authors said, because carbohydrates in the American diet tend to be primarily refined starch and sugar, which have a similar influence on mortality risk as saturated fats.
“Our study shows the importance of eliminating trans fat and replacing saturated fat with unsaturated fats, including both omega-6 and omega-3 polyunsaturated fatty acids. In practice, this can be achieved by replacing animal fats with a variety of liquid vegetable oils,” said senior author Frank Hu, professor of nutrition and epidemiology at Harvard Chan School and professor of medicine at Harvard Medical School.
This study is the most detailed and powerful examination to date on how dietary fats impact health. It suggests that replacing saturated fats like butter, lard, and fat in red meat with unsaturated fats from plant-based foods—like olive oil, canola oil, and soybean oil—can confer substantial health benefits and should continue to be a key message in dietary recommendations.
Meaning: Different types of dietary fat had different associations with mortality, the researchers found. Trans fats—on their way to being largely phased out of food—had the most significant adverse impact on health. Every 2% higher intake of trans fat was associated with a 16% higher chance of premature death during the study period. Higher consumption of saturated fats was also linked with greater mortality risk. When compared with the same number of calories from carbohydrate, every 5% increase in saturated fat intake was associated with an 8% higher risk of overall mortality.
Conversely, intake of high amounts of unsaturated fats—both polyunsaturated and monounsaturated—was associated with between 11% and 19% lower overall mortality compared with the same number of calories from carbohydrates. Among the polyunsaturated fats, both omega-6, found in most plant oils, and omega-3 fatty acids, found in fish and soy and canola oils, were associated with lower risk of premature death.
Figure 1. Dietary Fats and Mortality Rates
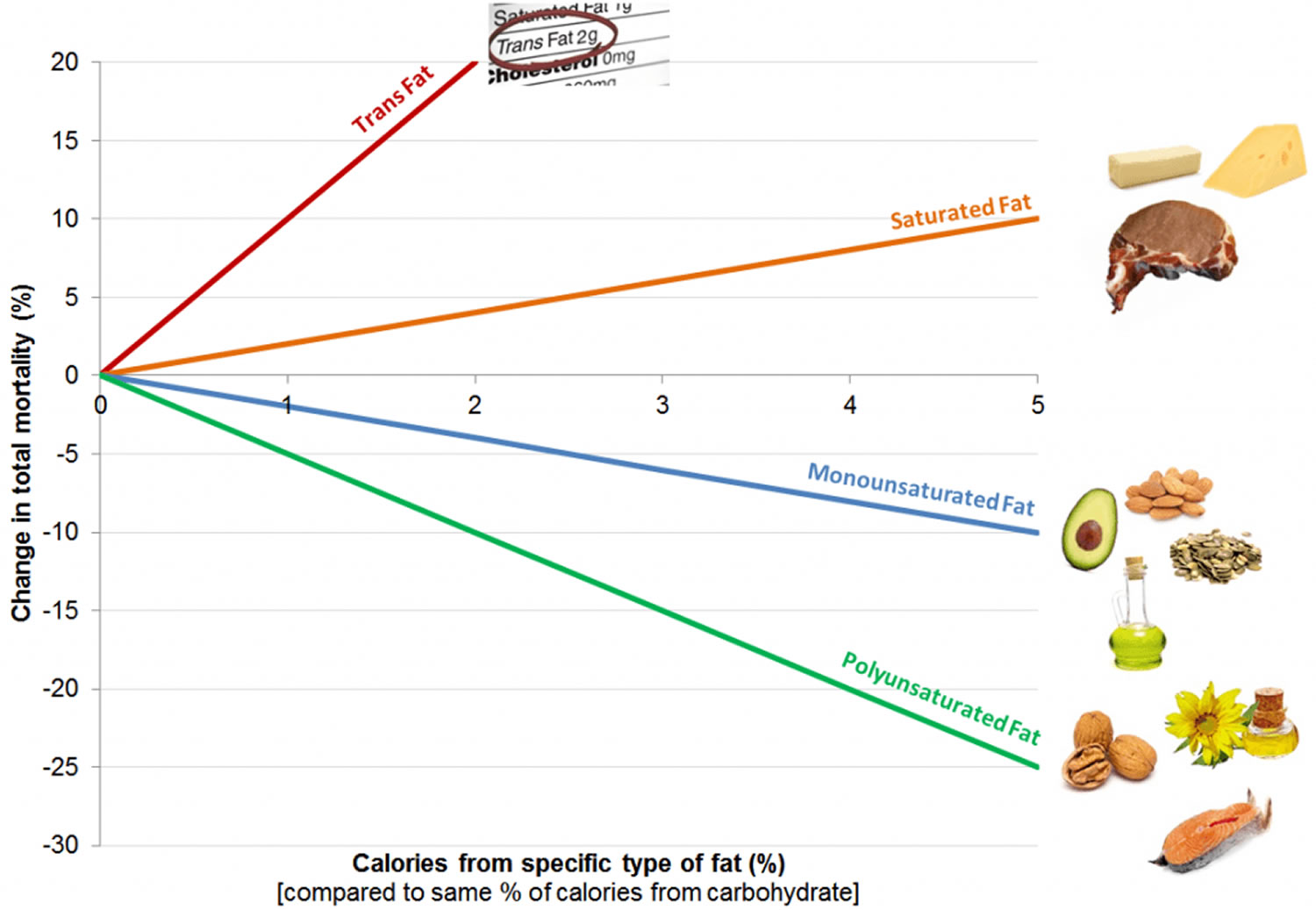
These findings support current dietary recommendations to replace saturated fat and trans-fat with unsaturated fat.
- Scientists concluded that saturated fat should be no more than 5 percent to 6 percent of daily calories. So, for a diet of 2,000 calories a day, that would mean no more than 120 of them should come from saturated fats. That’s about 13 grams of saturated fats a day 11.
Saturated fats are found in all animal foods, and some plant sources.
The following foods are high in saturated fats. Many of them are also low in nutrients and have extra calories from sugar:
- Baked goods (cake, doughnuts, Danish)
- Fried foods (fried chicken, fried seafood, French fries)
- Fatty or processed meats (bacon, sausage, chicken with skin, cheeseburger, steak)
- Whole-fat dairy products (butter, ice cream, pudding, cheese, whole milk)
- Solid fats such as coconut oil, palm, and palm kernel oils (found in packaged foods)
Here are some examples of popular food items with the saturated fat content in a typical serving:
- 12 ounces (oz), or 340 g, steak — 20 g
- 12 oz (340 g) cream of mushroom soup — 22 g
- Cheeseburger — 10 g
- Vanilla shake — 8 g
- 1 tablespoon (15 mL) butter — 7 g
It is fine to treat yourself to these types of foods once in a while. But, it is best to limit how often you eat them and limit portion sizes when you do.
How Saturated Fats Affect Your Health
Saturated fats are bad for your health in several ways:
- Heart disease risk. Your body needs healthy fats for energy and other functions. But too much saturated fat can cause cholesterol to build up in your arteries (blood vessels). Saturated fats raise your LDL, or bad, cholesterol. High LDL cholesterol increases your risk for heart disease and stroke.
- Weight gain. Many high-fat foods such as pizza, baked goods, and fried foods have a lot of saturated fat. Eating too much fat can cause you to gain weight. All fats contain 9 calories per gram of fat. This is more than twice the amount found in carbohydrates and protein.
Cutting out high-fat foods can help keep your weight in check and keep your heart healthy. Staying at a healthy weight can reduce your risk of diabetes, heart disease, and other health problems.
The most recent American Heart Association and American College of Cardiology advisory 11, reaffirms that longstanding advice. Here are some of the scientific highlights:
- Randomized controlled trials that lowered intake of dietary saturated fat and replaced it with polyunsaturated vegetable oil reduced cardiovascular disease by about 30 percent – similar to results achieved by some cholesterol-lowering drugs known as statins 12.
- Prospective observational studies in many populations showed that a lower intake of saturated fat with a higher intake of polyunsaturated and monounsaturated fat is associated with lower rates of cardiovascular disease 13.
- Several studies found that coconut oil – which is predominantly saturated fat but has been widely touted recently as healthy – raised LDL cholesterol to the same degree as other saturated fats found in butter, beef fat, ghee and palm oil.
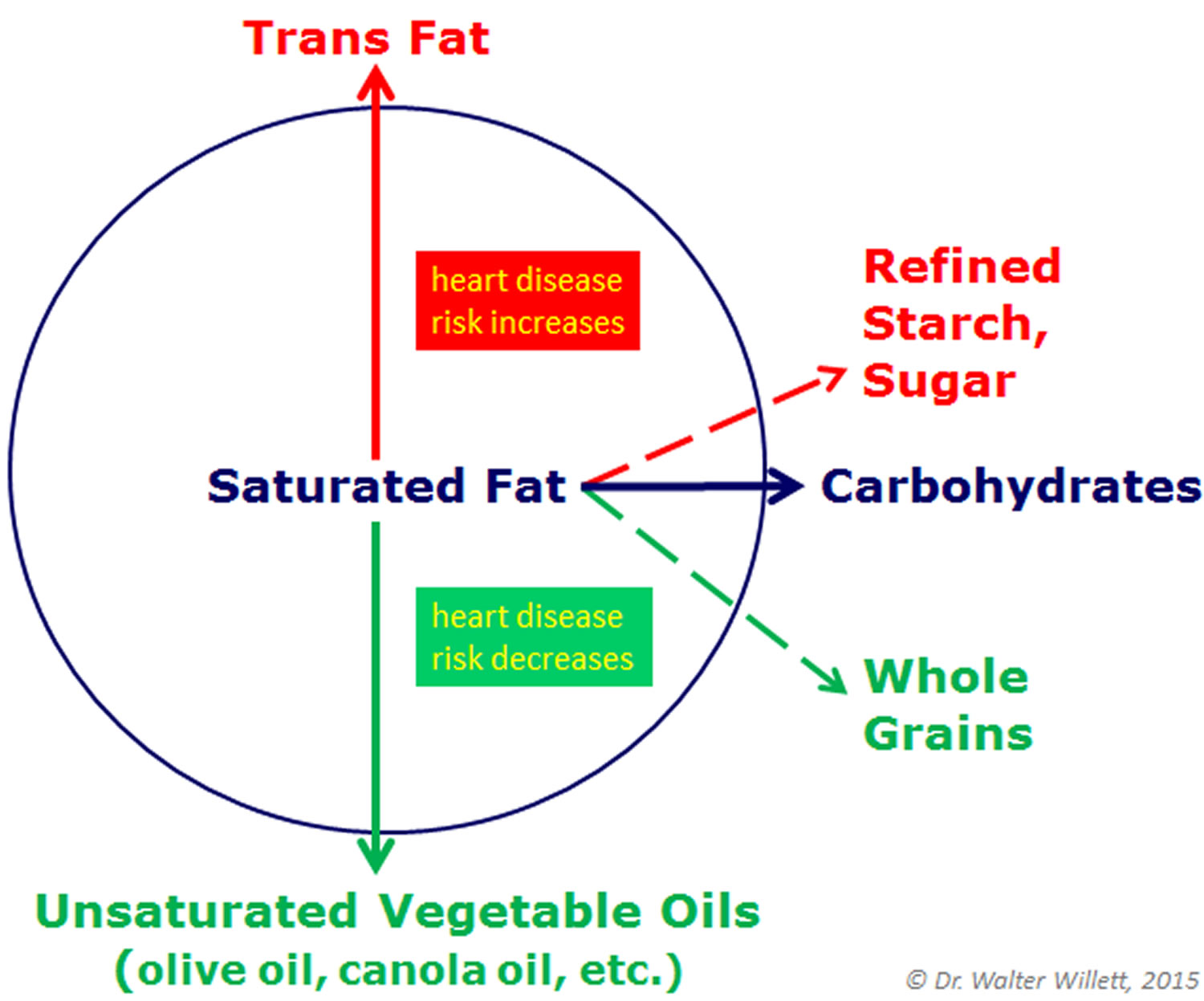
- Replacing saturated fat with mostly refined carbohydrate and sugars does not lower rates of heart disease, but replacing these fats with whole grains is associated with lower rates. This indicates that saturated fat and refined carbohydrate are equally bad relative to heart disease risk.
What is Cholesterol ?
Cholesterol is a waxy substance that your body needs it to build cells. But too much cholesterol can be a problem 14.
Cholesterol comes from two sources. Your body (specifically your liver) makes all the cholesterol you need. The rest you get from foods. For example, meat, poultry, ghee, butter, pork lard, beef tallow and full-fat dairy products contain cholesterol (called dietary cholesterol). More importantly, these foods are high in saturated and trans fat. That’s a problem because these fats cause your liver to make more cholesterol than it otherwise would. For some people, this added production means they go from a normal cholesterol level to one that’s unhealthy.
Some tropical oils, such as palm oil, palm kernel oil and coconut oil, also can trigger your liver to make more cholesterol. These oils are often found in baked goods.
There are actually two types of cholesterol: “bad” and “good.” LDL cholesterol is the “bad” kind. HDL is the “good” kind. Too much of the bad kind (LDL cholesterol) — or not enough of the good kind (HDL cholesterol) — increases the chances that cholesterol will start to slowly build up in the inner walls of arteries that feed the heart and brain. We talk more about these two kinds of cholesterol here: What is Cholesterol and Is there good and bad cholesterol ?
High LDL “bad” cholesterol is one of the major controllable risk factors for coronary heart disease, heart attack and stroke. High LDL “bad” cholesterol contributes to fatty buildups in arteries (atherosclerosis). Plaque buildups narrow arteries and raise the risk for heart attack, stroke and peripheral artery disease can narrowed arteries in the legs. If the blocked artery supplies the heart or brain, a heart attack or stroke occurs. If an artery supplying oxygen to the extremities (often the legs) is blocked, gangrene can result. Gangrene is tissue death. If you have other risk factors such as smoking, high blood pressure or diabetes, this risk increases even more. The more risk factors you have and the more severe they are, the more your overall risk rises.
Keeping your cholesterol levels healthy is a great way to keep your heart healthy – and lower your chances of getting heart disease or having a stroke.
Why cholesterol matters
Cholesterol circulates in the blood, and as blood cholesterol levels rise, so does the risk to your health. That’s why it’s important to have your cholesterol tested so you can know your levels.
Together with other substances, LDL “bad” cholesterol can form a thick, hard deposit that can narrow the arteries and make them less flexible. This condition is known as atherosclerosis. If a clot forms and blocks a narrowed artery, a heart attack or stroke can result.
A diet high in saturated (e.g. ghee, butter, beef tallow, pork lard) and trans fat is unhealthy because it tends to raise LDL “bad” cholesterol.
High LDL “bad” cholesterol is one of the major controllable risk factors for coronary heart disease, heart attack and stroke. If you have other risk factors such as smoking, high blood pressure or diabetes, this risk increases even more. The more risk factors you have and the more severe they are, the more your overall risk rises.
A low LDL cholesterol level is considered good for your heart health.
A Scientific Statement From the American Heart Association Nutrition Committee recommendations 2 are:
- to balance caloric intake and physical activity to achieve and maintain a healthy body weight;
- consume a diet rich in vegetables and fruits;
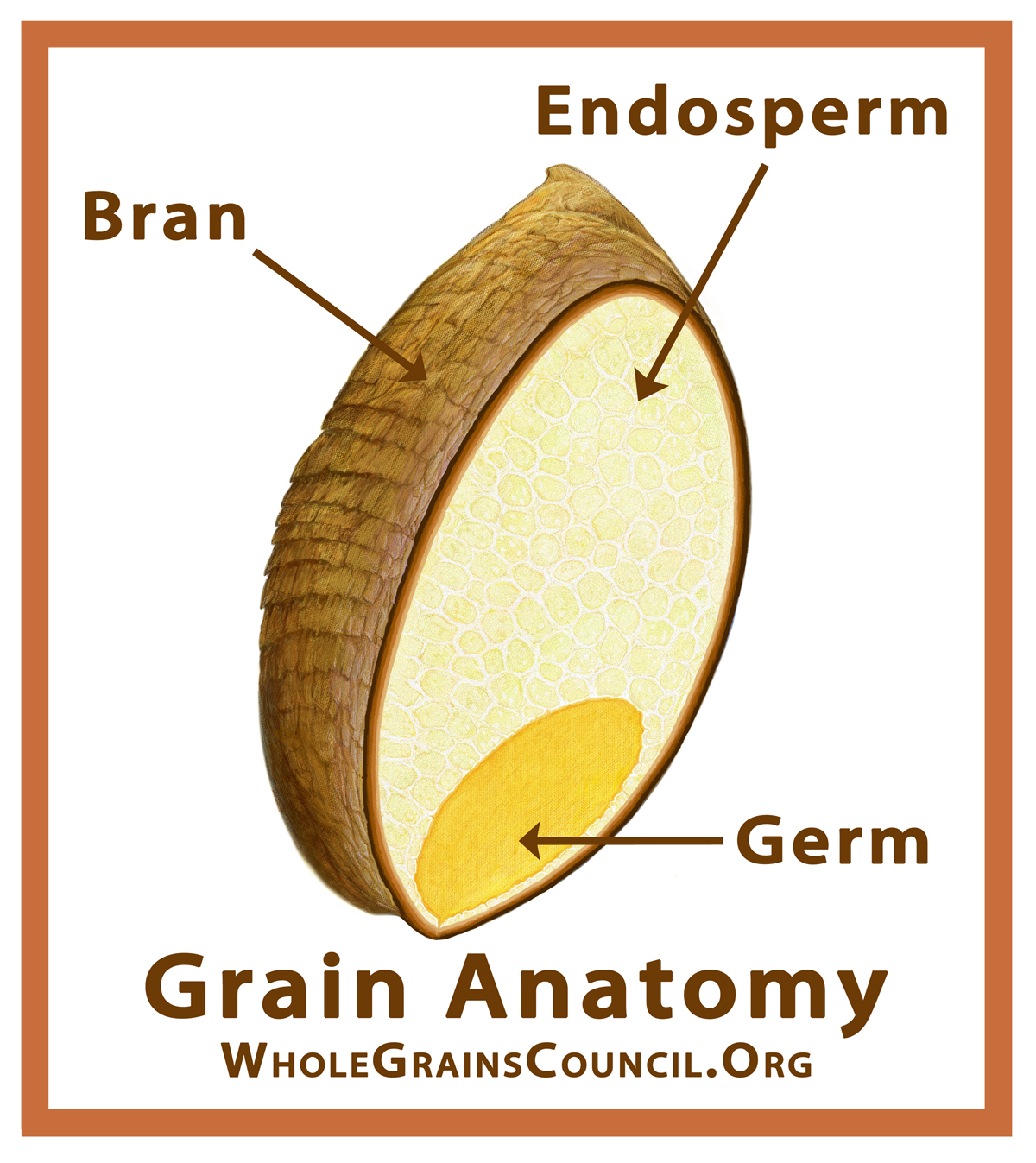
- choose whole-grain, high-fiber foods;
- consume fish, especially oily fish, at least twice a week;
- limit intake of saturated fat to <7% of energy, trans fat to <1% of energy, and cholesterol to <300 mg/day by choosing lean meats and vegetable alternatives, fat-free (skim) or low-fat (1% fat) dairy products and minimize intake of partially hydrogenated fats;
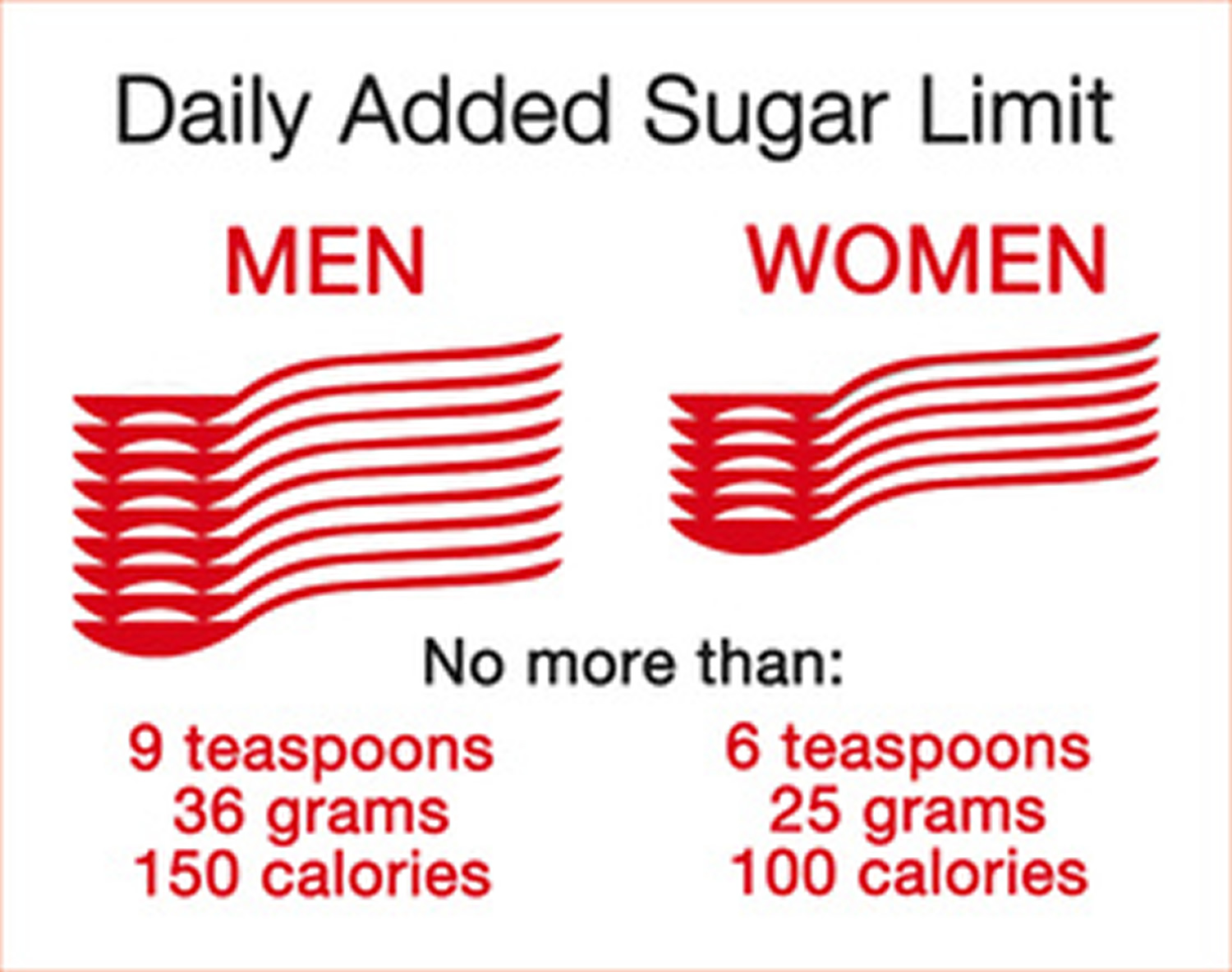
- minimize intake of beverages and foods with added sugars; choose and prepare foods with little or no salt.
Ghee Nutrition Content
Table 1. Ghee Nutrition Content
Nutrient | Unit | 14 g | Value per 100 g | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Approximates | |||||||||||||||||||
| Energy | kcal | 126 | 900 | ||||||||||||||||
| Protein | g | 0.00 | 0.00 | ||||||||||||||||
| Total lipid (fat) | g | 14.00 | 100.00 | ||||||||||||||||
| Carbohydrate, by difference | g | 0.00 | 0.00 | ||||||||||||||||
| Fiber, total dietary | g | 0.0 | 0.0 | ||||||||||||||||
| Sugars, total | g | 0.00 | 0.00 | ||||||||||||||||
| Minerals | |||||||||||||||||||
| Calcium, Ca | mg | 0 | 0 | ||||||||||||||||
| Iron, Fe | mg | 0.00 | 0.00 | ||||||||||||||||
| Sodium, Na | mg | 95.2 | 680 | ||||||||||||||||
| Vitamins | |||||||||||||||||||
| Vitamin C, total ascorbic acid | mg | 0.0 | 0.0 | ||||||||||||||||
| Vitamin A, IU | IU | 560 | 4000 | ||||||||||||||||
| Lipids | |||||||||||||||||||
| Fatty acids, total saturated | g | 8.40 | 60.000 | ||||||||||||||||
| Fatty acids, total trans | g | 0.000 | 0.000 | ||||||||||||||||
| Cholesterol | mg | 28 | 200 | ||||||||||||||||
Is ghee healthy ?
Consuming high amounts of saturated fats linked to increased heart disease risk ! 16, 17, 18, 19.
In a new study appearing online in the Journal of the American College of Cardiology, Dr. Frank Hu and colleagues found that people who replace saturated fat (primarily found in meats and dairy foods) with refined carbohydrates do not lower their risk of heart disease, whereas those who replace saturated fats with unsaturated fats or whole grains lower their heart disease risk 20.
Previous studies have shown that individual saturated fatty acids have different effects on blood lipids, but little is known about associations between individual saturated fatty acid intake and coronary heart disease risk. However, in a study that appeared online on 23rd November 2016, in The British Medical Journal 21, where the researchers analyzed data from 73,147 women involved in the Nurses’ Health Study between 1984 and 2012, and 42,635 men who were in the Health Professionals Follow-up Study between 1986 and 2010. Participants reported their diet and health status on questionnaires completed every four years. The study found that a higher intake of the most commonly consumed major saturated fatty acids—lauric acid, myristic acid, palmitic acid, and stearic acid—was associated with a 18% increased relative risk of coronary heart disease 21. This study dispels the notion that ‘butter is good’, said Dr. Hu the study co-author. Dr. Hu added, “individual saturated fatty acids share the same food sources, such as red meat, dairy, butter, lard, and palm oil. Therefore it is impractical to differentiate the types of saturated fatty acids in making dietary recommendations, an idea that some researchers have put forth. Instead, it is healthier to replace these fatty acids with unsaturated fats from vegetable oils, nuts, seeds, and seafood as well as high quality carbohydrates” 21. “Replacing sources of saturated fat in our diets with unsaturated fats is one of the easiest ways to reduce our risk of heart disease,” said Walter Willett, a co-author and professor of epidemiology and nutrition.
Replacing just 1% of daily consumption of these fatty acids with equivalent calories from polyunsaturated fats, whole grain carbohydrates, or plant proteins, was estimated to reduce relative coronary heart disease risk by 6%-8%. Replacing palmitic acid—found in palm oil, meat, and dairy fat—was associated with the strongest risk reduction.
Although fat is an important part of a healthy diet, it’s even more important to focus on eating beneficial “good” fats and avoiding harmful “bad” fats. Choose foods with “good” unsaturated fats, limit foods high in saturated fat, and avoid “bad” trans fat.
- “Good” unsaturated fats — Monounsaturated and polyunsaturated fats — lower disease risk. Foods high in good fats include vegetable oils (such as olive oil, canola oil, sunflower oil, peanut oil, safflower, soybean oil, walnut oil and corn oil), nuts (peanuts,almonds, cashews, hazelnuts, pistachios and pecans), seeds, avocado and fish.
- “Bad” fats — trans fats — increase disease risk, even when eaten in small quantities. Foods containing trans fats are primarily in processed foods made with trans fat from partially hydrogenated oil. Fortunately, trans fats have been eliminated from many of these foods.
- “Bad” Saturated fats, while not as harmful as trans fats, by comparison with unsaturated fats negatively impact health and are best consumed in moderation. Foods containing large amounts of saturated fat include red meat, butter, ghee, coconut oil, palm oil, cheese and ice cream.
When you cut back on foods like red meat and butter, replace them with oily fish, beans, nuts, and healthy oils instead of refined carbohydrates.
Most foods have a combination of different fats. You are better off choosing foods higher in healthier fats, such as monounsaturated and polyunsaturated fats. These fats tend to be liquid at room temperature.
The latest Dietary Guidelines for Americans 22 Key Recommendations for healthy eating pattern limits:
- Saturated fats and trans fats, added sugars, and sodium.
- Consume less than 10 percent of calories per day from saturated fats.
- To further reduce your heart disease risk, limit saturated fats to less than 7% of your total daily calories.
- Consume less than 10 percent of calories per day from added sugars.
- Consume less than 2,300 milligrams (mg) per day of sodium (salt).
- If alcohol is consumed, it should be consumed in moderation—up to one drink per day for women and up to two drinks per day for men—and only by adults of legal drinking age.
You can cut how much saturated fat you eat by substituting healthier foods for less healthy options. Replace foods high in saturated fats with foods that have polyunsaturated and monounsaturated fats. Here is how to get started:
- Replace red meats with skinless chicken or fish a few days a week.
- Use canola or olive oil instead of butter, ghee and other solid fats.
- Replace whole-fat diary with low-fat or nonfat milk, yogurt, and cheese.
- Eat more fruits, vegetables, whole grains, and other foods with low or no saturated fat.

Ghee vs Butter
Ghee has slightly more vitamin A 560 IU vs butter with only 400 IU per tablespoon.
However, both are high in saturated fat and cholesterol.
Table 2. Butter (Unsalted) Nutrition Content
Nutrient | Unit | 14 g | Value per 100 g | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Approximates | |||||||||||||||||||
| Energy | kcal | 100 | 714 | ||||||||||||||||
| Protein | g | 0.00 | 0.00 | ||||||||||||||||
| Total lipid (fat) | g | 11.00 | 78.57 | ||||||||||||||||
| Carbohydrate, by difference | g | 0.00 | 0.00 | ||||||||||||||||
| Minerals | |||||||||||||||||||
| Sodium, Na | mg | 0 | 0 | ||||||||||||||||
| Vitamins | |||||||||||||||||||
| Vitamin A, IU | IU | 400 | 2857 | ||||||||||||||||
| Lipids | |||||||||||||||||||
| Fatty acids, total saturated | g | 7.000 | 50.000 | ||||||||||||||||
| Fatty acids, total trans | g | 0.000 | 0.000 | ||||||||||||||||
| Cholesterol | mg | 30 | 214 | ||||||||||||||||
Ghee vs Polyunsaturated Oils (Olive Oil & Peanut Oil)
Both olive and peanut oils are low in saturated fat and has O (zero) cholesterol. And from heart and cardiovascular point of view, they are much healthier for you than ghee or butter.
- An analysis of more than 100 published research studies dating as far back as the 1950s, pointed out there are great benefits to replacing saturated fats – such as coconut oil, butter, ghee, beef fat or palm oil – with healthier polyunsaturated fats.
- The American Heart Association, the American College of Cardiology and the U.S. Department of Agriculture’s Dietary Guidelines for Americans have been issuing dietary recommendations for decades. In 1961, the American Heart Association recommended for the first time that vegetable oils replace saturated fats. Governments, including in the United States and internationally, as well as other nonprofits have been cautioning about saturated fats, too.
- The basis for the American Heart Association’s advice about nutrition is a systematic review of the best available scientific information, conducted by volunteer committees of expert researchers and physicians. More information on the American Heart Association’s statements and guidelines development is available online here 23. –> American Heart Association. About GUIDELINES & Statements. http://professional.heart.org/professional/GuidelinesStatements/UCM_316885_Guidelines-Statements.jsp
Table 3. Olive Oil Nutrition Content
Nutrient | Unit | 15 ml | Value per 100 ml | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Approximates | |||||||||||||||||||
| Energy | kcal | 126 | 840 | ||||||||||||||||
| Protein | g | 0.00 | 0.00 | ||||||||||||||||
| Total lipid (fat) | g | 14.00 | 93.33 | ||||||||||||||||
| Carbohydrate, by difference | g | 0.00 | 0.00 | ||||||||||||||||
| Minerals | |||||||||||||||||||
| Sodium, Na | mg | 0 | 0 | ||||||||||||||||
| Lipids | |||||||||||||||||||
| Fatty acids, total saturated | g | 1.999 | 13.330 | ||||||||||||||||
| Fatty acids, total monounsaturated | g | 11.000 | 73.330 | ||||||||||||||||
| Fatty acids, total polyunsaturated | g | 1.000 | 6.670 | ||||||||||||||||
| Fatty acids, total trans | g | 0.000 | 0.000 | ||||||||||||||||
| Cholesterol | mg | 0 | 0 | ||||||||||||||||
Table 4. Peanut Oil Nutrition Content
Nutrient | Unit | 14 g | Value per 100 g | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Proximates | |||||||||||||||||||
| Energy | kcal | 120 | 857 | ||||||||||||||||
| Protein | g | 0.00 | 0.00 | ||||||||||||||||
| Total lipid (fat) | g | 14.00 | 100.00 | ||||||||||||||||
| Carbohydrate, by difference | g | 0.00 | 0.00 | ||||||||||||||||
| Minerals | |||||||||||||||||||
| Sodium, Na | mg | 0 | 0 | ||||||||||||||||
| Lipids | |||||||||||||||||||
| Fatty acids, total saturated | g | 2.500 | 17.860 | ||||||||||||||||
| Fatty acids, total monounsaturated | g | 6.000 | 42.860 | ||||||||||||||||
| Fatty acids, total polyunsaturated | g | 4.999 | 35.710 | ||||||||||||||||
| Fatty acids, total trans | g | 0.000 | 0.000 | ||||||||||||||||
| Cholesterol | mg | 0 | 0 | ||||||||||||||||
- Sharma H, Zhang X, Dwivedi C. The effect of ghee (clarified butter) on serum lipid levels and microsomal lipid peroxidation. Ayu. 2010;31(2):134-140. doi:10.4103/0974-8520.72361. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3215354/
- Diet and lifestyle recommendations revision 2006: a scientific statement from the American Heart Association Nutrition Committee. American Heart Association Nutrition Committee., Lichtenstein AH, Appel LJ, Brands M, Carnethon M, Daniels S, Franch HA, Franklin B, Kris-Etherton P, Harris WS, Howard B, Karanja N, Lefevre M, Rudel L, Sacks F, Van Horn L, Winston M, Wylie-Rosett J. Circulation. 2006 Jul 4; 114(1):82-96. http://circ.ahajournals.org/content/114/1/82.long
- Lad V. New York: Harmony Books; 1998. The Complete Book of Ayurvedic Home Remedies.
- Sharma HM. Butter oil (ghee) – Myths and facts. Indian J Clin Pract. 1990;1:31–2.
- Illingworth D, Patil GR, Tamime AY. Anhydrous milk fat manufacture and fractionation. In: Tamime AY, editor. Dairy Fats and Related Products. Chichester, West Sussex: Wiley-Blackwell; 2009.
- U.S. National Library of Medicine. Facts about saturated fats. https://medlineplus.gov/ency/patientinstructions/000838.htm
- Mozaffarian D, Micha R, Wallace S. Effects on coronary heart disease of increasing polyunsaturated fat in place of saturated fat: a systematic review and meta-analysis of randomized controlled trials. PLoS Med. 2010;7:e1000252. doi: 10.1371/journal. pmed.1000252.
- Hooper L, Martin N, Abdelhamid A, Davey Smith G. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst Rev. 2015:CD011737. doi: 10.1002/14651858. CD011737.
- Wang DD, Li Y, Chiuve SE, Stampfer MJ, Manson JE, Rimm EB, Willett WC, Hu FB. Association of Specific Dietary Fats With Total and Cause-Specific Mortality. JAMA Intern Med. 2016;176(8):1134–1145. doi:10.1001/jamainternmed.2016.2417. http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2530902
- Harvard University, Harvard School of Public Health. Different Dietary Fat, Different Risk of Mortality. https://www.hsph.harvard.edu/nutritionsource/2016/07/05/different-dietary-fat-different-risk-of-mortality/
- American Heart Association. Cutting through the saturated fat – meats, butter and tropical oils still need limits. http://news.heart.org/cutting-saturated-fat-meats-butter-tropical-oils-still-need-limits/
- American Heart Association. Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association. http://circ.ahajournals.org/content/early/2017/06/15/CIR.0000000000000510
- American Heart Association. Advisory: Replacing saturated fat with healthier fat could lower cardiovascular risks. http://news.heart.org/advisory-replacing-saturated-fat-with-healthier-fat-could-lower-cardiovascular-risks/
- American Heart Association. About Cholesterol. http://www.heart.org/HEARTORG/Conditions/Cholesterol/AboutCholesterol/About-Cholesterol_UCM_001220_Article.jsp
- United States Department of Agriculture, Agriculture Research Service. USDA Food Composition Databases. https://ndb.nal.usda.gov/ndb/
- Siri-Tarino, P.W., et al., Saturated fatty acids and risk of coronary heart disease: modulation by replacement nutrients. Curr Atheroscler Rep, 2010. 12(6): p. 384-90.
- Hu, F.B., et al., Dietary fat intake and the risk of coronary heart disease in women. N Engl J Med, 1997. 337(21): p. 1491-9.
- Ascherio, A., et al., Dietary fat and risk of coronary heart disease in men: cohort follow up study in the United States. BMJ, 1996. 313(7049): p. 84-90.
- Hu, F.B., J.E. Manson, and W.C. Willett, Types of dietary fat and risk of coronary heart disease: a critical review. J Am Coll Nutr, 2001. 20(1): p. 5-19.
- Journal of the American College of Cardiology Volume 66, Issue 14, October 2015. DOI: 10.1016/j.jacc.2015.07.055. Saturated Fats Compared With Unsaturated Fats and Sources of Carbohydrates in Relation to Risk of Coronary Heart Disease. http://www.onlinejacc.org/content/66/14/1538
- BMJ 2016;355:i5796. Intake of individual saturated fatty acids and risk of coronary heart disease in US men and women: two prospective longitudinal cohort studies. http://www.bmj.com/content/355/bmj.i5796
- 2015–2020 Dietary Guidelines for Americans, https://health.gov/dietaryguidelines
- American Heart Association. About GUIDELINES & Statements. http://professional.heart.org/professional/GuidelinesStatements/UCM_316885_Guidelines-Statements.jsp





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}