Central pontine myelinolysis
Central pontine myelinolysis (CPM) also known as osmotic demyelination syndrome, is a rare acute demyelinating brain disorder that occurs after rapid correction of sodium (Na+) in patients with chronic hyponatremia 1, 2, 3, 4, 5, 6, 7, 8, 9, 10. A demyelinating disease is any condition that causes damage to the protective covering (myelin sheath) that surrounds nerve fibers in your brain and spinal cord. Central pontine myelinolysis (CPM) lesions are usually located in the pons and the important affected structures include the corticospinal, corticobulbar, and corticopontine tracts at the basis pontis, which relays signals involving hearing, taste, movement, and other functions. Some individuals will also have damage in other areas of the brain, which is called extrapontine myelinolysis (EPM). Hyponatremia is defined as low level of sodium (Na+) in the blood of less than 135 mmol/L (Na+ < 135 mEq/L) caused by an excess of water relative to sodium. Hyponatremia is among the most common electrolyte abnormalities encountered in hospitalized patients 11, 12. Common causes of hyponatremia include consumption of too much fluids, use of diuretics (water pills), diarrhea, heart failure, liver disease, kidney failure, kidney disease and the syndrome of inappropriate antidiuretic hormone secretion (SIADH). In patients with hyponatremia, the brain adapts to a fall in serum sodium level, without developing brain swelling (cerebral edema), in about 48 hours. As a result, patients with chronic hyponatremia are mostly asymptomatic. Once the brain adapts to low serum sodium, the rapid correction of sodium leads to osmotic demyelination syndrome. The rapid rise in sodium concentration involves the movement of small molecules and pulls water from brain cells that leads to the destruction of myelin, a substance that surrounds and protects nerve fibers. Nerve cells (neurons) also can be damaged. Central pontine myelinolysis signs and symptoms are typically delayed by a few days and comprise several irreversible neurological symptoms, including seizures, disorientation, “locked-in syndrome” (which is the complete paralysis of all of the voluntary muscles in the body except for muscles that control the eyes), coma and death.
Anyone can develop hyponatremia (low level of sodium in the blood of less than 135 mmol/L) and osmotic demyelination syndrome can develop 1 to several days after aggressive treatment of hyponatremia. However, some individuals who are particularly vulnerable are those with chronic alcoholism or have had a liver transplant or liver or kidney disease. Although many affected people improve over weeks to months, some have permanent disability. Some also develop new symptoms later, including behavioral or intellectual impairment or movement disorders like parkinsonism or tremor.
During the early course of central pontine myelinolysis (CPM), classical symptoms like weakness in the muscles used for speech often causes slowed or slurred speech (dysarthria), difficulty swallowing (dysphagia), muscle weakness in both legs and both arms (quadriparesis), and abnormal increase in muscle tone or stiffness of muscle (spasticity) are present when the respective anatomic structures are involved 13, 14. During the later course of central pontine myelinolysis (CPM), the pontine tegmentum is also involved. “Locked-in syndrome” occurs in severely affected patients and is a characteristic presentation of central pontine myelinolysis (CPM), which refers to the situation where these patients are awake, have preserved cognitive function and oculomotor function, but patients are unable to move and cannot perform voluntary movements (e.g., movement of limbs, respiratory muscles) and can communicate with the help of their eyes only 15.
In the course of central pontine myelinolysis, imaging findings are often significantly delayed after the clinical presentation. Compared with conventional CT, brain MRI is more sensitive for lesion detection 16. Osmotic demyelination syndrome usually manifests as a low T1-weighted image (T1WI) signal intensity and high T2WI signal intensity in the affected area 17. Furthermore, there is no enhancement of lesions after intravenous gadolinium administration 17. In cases of central pontine myelinolysis (CPM), an oval-shaped or trident-shaped high signal intensity abnormality in central pons is observed using T2-weighted or FLAIR sequences 17. In extrapontine myelinolysis (EPM), symmetrical high signal intensity abnormalities are seen in the bilateral caudate nucleus and bilateral putamen with sparing of the globus pallidus in T2-weighted and FLAIR sequences 16. However, detection of lesions using conventional MRI sequences (T1WI, T2WI, FLAIR) usually takes 10-14 days after the onset of clinical symptoms and signs. In contrast, diffusion-weighted imaging (DWI) can detect abnormal diffusion restriction in demyelinated lesions within 24 hours after initial onset, which can increase diagnostic confidence 16.
Central pontine myelinolysis is a medical emergency that needs to be treated in the hospital, fortunately most people with this condition are already in the hospital for another problem.
There is no known cure for central pontine myelinolysis. Treatment is focused on relieving symptoms.
Physical therapy may help maintain muscle strength, mobility, and function in weakened arms and legs.
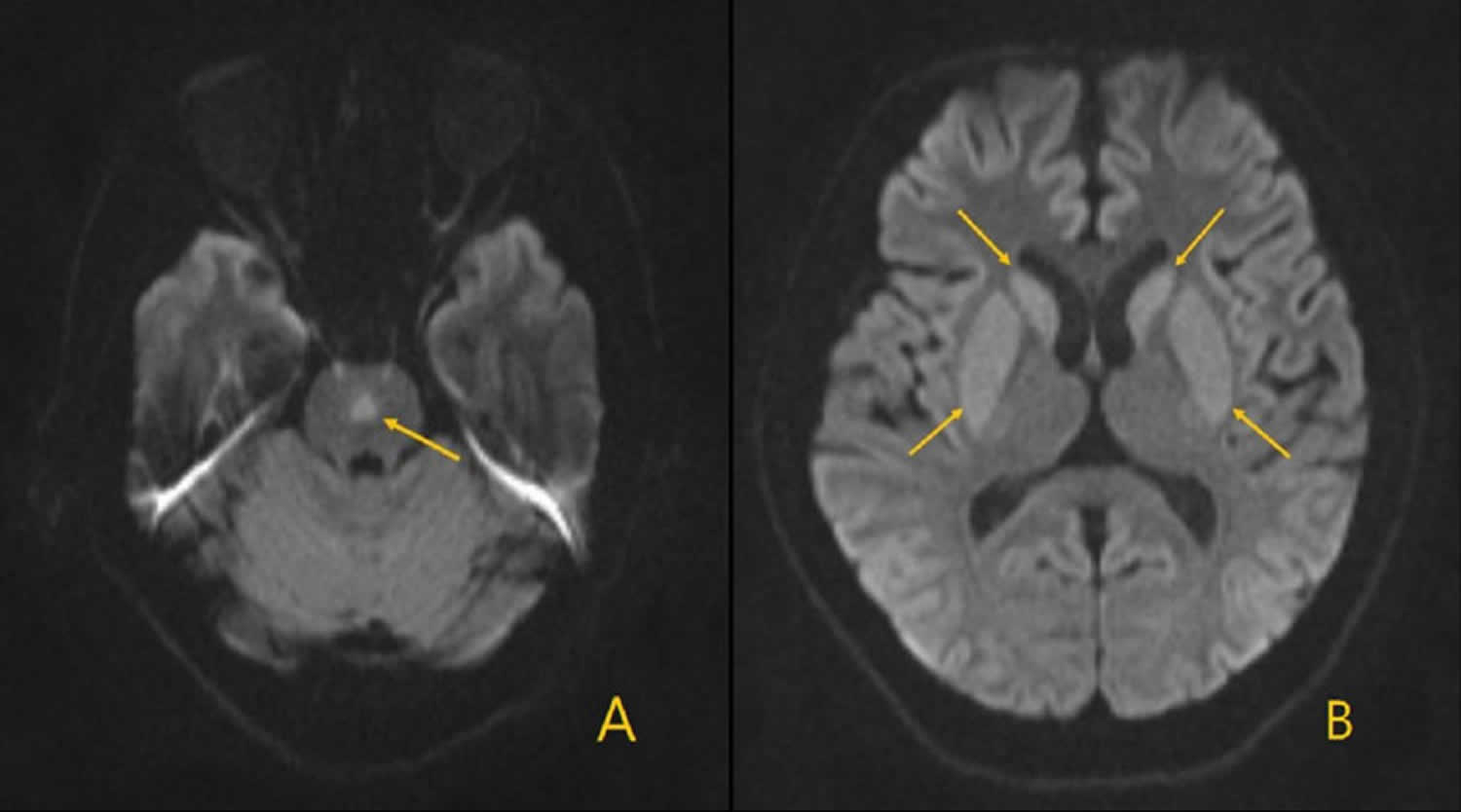
Figure 1. Central pontine myelinolysis
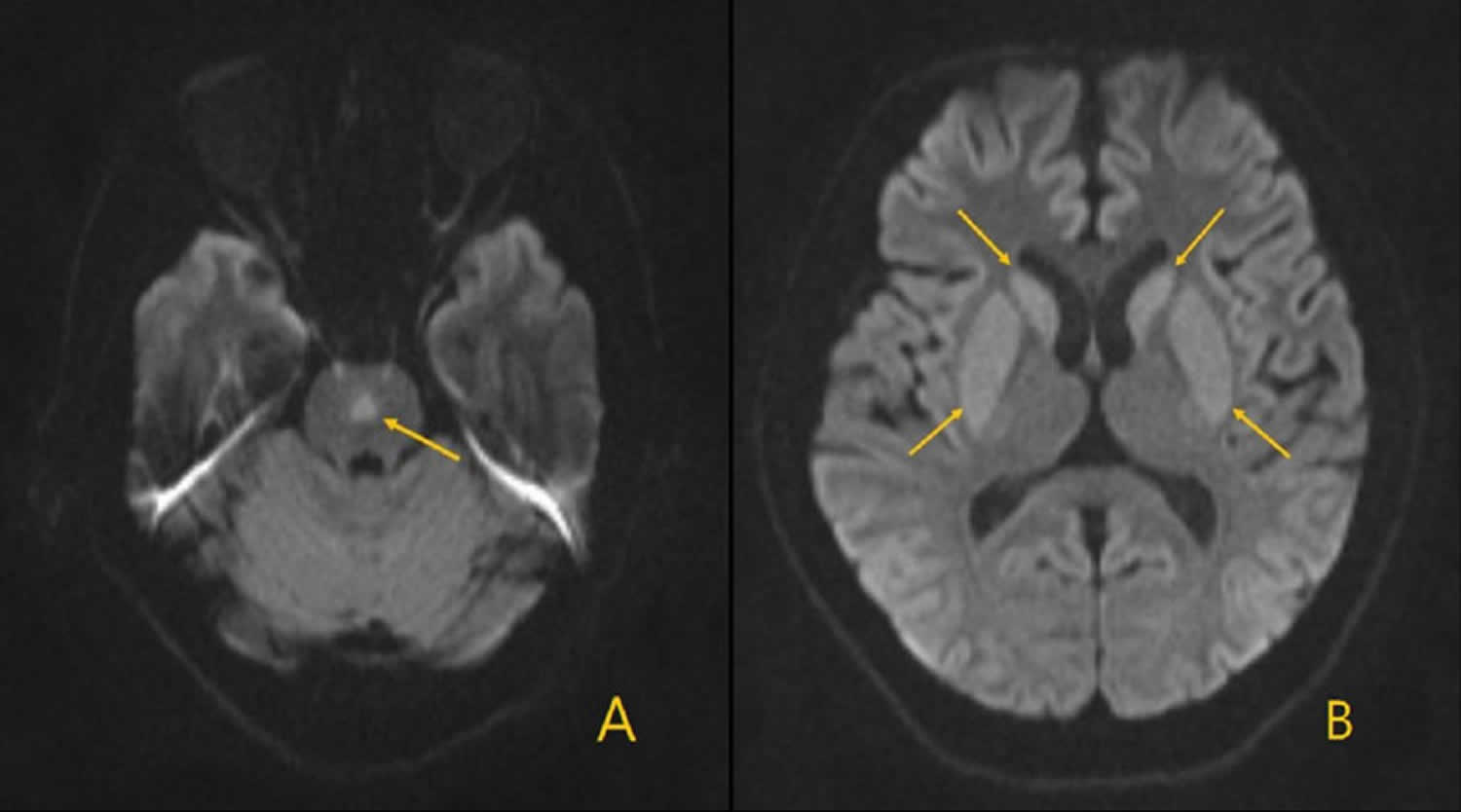
Footnotes: Brain MRI diffusion-weighted imaging (DWI) on day 12 of hospital admission. A 44-year-old male patient who was taken to the emergency department for unrelieved upper abdominal pain for the previous two days. Other reported symptoms included hiccups, constipation, nausea, and a poor appetite. He denied any seizure episodes, change in consciousness, or fever. Under the assumption of a diagnosis of syndrome of inappropriate antidiuretic hormone secretion (SIADH) related hyponatremia, sodium supplementation with 3% hypertonic saline and water restriction were given for treatment of severe hyponatremia. The axial view of the diffusion-weighted imaging (DWI) shows: (A) new high intensity lesion at the central pons, consistent with central pontine myelinolysis; and (B) the previous lesions at the bilateral caudate nucleus and putamen did not subside and became more conspicuous.
[Source 17 ]Central pontine myelinolysis cause
The most common cause of central pontine myelinolysis is a quick change in your body’s blood sodium levels. This most often occurs when someone is being treated for low blood sodium (hyponatremia) and the sodium is replaced too fast. Sometimes, central pontine myelinolysis occurs when a high level of sodium in the body (hypernatremia) is corrected too quickly.
Central pontine myelinolysis does not usually occur on its own. Most often, it’s a complication of treatment for other problems, or from the other problems themselves.
Patients with hypovolemic hyponatremia tend to have a rapid increase in plasma sodium concentration with saline therapy. This happens because of a rapid fall of arginine vasopressin levels with intravenous saline resulting in water diuresis. Hence sodium levels should be monitored frequently (2–4 hour) to guide further saline therapy.
The initial description of central pontine myelinolysis by Adams et al. in 1959 18 was entirely in a population of chronic alcoholics, and and malnourished patients. Since then central pontine myelinolysis has been increasingly recognized in other patient groups, but usually in the setting of rapidly corrected electrolyte disturbance 19:
- chronic alcoholics
- chronically debilitated patients
- transplant recipients
- pregnancy and vomiting during pregnancy
Risk factors for developing central pontine myelinolysis
Risk factors for developing central pontine myelinolysis include rapid correction of hyponatremia in people with 20:
- Alcohol use
- Liver disease
- Liver transplant
- Malnutrition from serious illnesses
- Radiation treatment of the brain
- Severe nausea and vomiting during pregnancy (hyperemesis gravidarum)
Central pontine myelinolysis pathophysiology
Central pontine myelinolysis pathophysiology is still uncertain. It is known that oligodendroglial cells are most susceptible to osmotic stresses, leading to their death. It is not surprising that the distribution of osmotic myelinolysis, parallels the distribution of these cells.
Hyponatremia is defined as serum sodium below 135 mmol/L. In response to decreased serum sodium, extracellular water will shift into cells where there is higher tonicity via the process of osmosis, in an attempt to normalize the gradient, thereby causing cerebral edema.
The brain is able to adapt to a decrease in serum tonicity by several proposed mechanisms. One protective mechanism is through the displacement of water from the cells into the cerebrospinal fluid. Another mechanism called volume regulatory decrease includes the removal of intracellular solutes and water via ion channels to reduce brain swelling and normalize brain volume. With chronic hyponatremia (greater than 48 hours in duration), other adaptive mechanisms include the efflux of organic osmolytes (glutamate, taurine, and glycine) with water, which also reduces cellular swelling 21. Therefore, patients with chronic hyponatremia have already developed compensatory mechanisms involving solute losses, which puts them at higher risk for the development of central pontine myelinolysis.
With the rapid correction of hyponatremia, the brain is unable to recapture lost osmolytes, leading to dehydration of brain tissue and demyelination of white matter. The main cells affected in the brain are the astrocytes. Recent studies in rat models that show that astrocyte apoptosis is preceded by myelin loss and was observed within 48-72 hours after the correction of hyponatremia 22. The main consequence of this is termed osmotic demyelination syndrome. The pons of the brain is the most susceptible region of the brain hence termed central pontine myelinolysis (CPM). Current recommendations are that the rate of sodium correction should not exceed 8-12 mEq/L/day to avoid these complications.
Histologically, osmotic demyelination syndrome is characterized by intramyelinic splitting, vacuolation, and myelin sheath rupture 16. After many days, lymphocytes and macrophages can be identified 23.
Central pontine myelinolysis prevention
Aggressive treatment of hyponatremia should always be weighed against the risk of inducing central pontine myelinolysis. In the hospital, slow, controlled treatment of a low sodium level (hyponatremia) may reduce the risk for nerve damage in the brain. Being aware of how some medicines can change sodium levels can prevent the sodium level from changing too quickly.
Aggressive management of hyponatremia is indicated in patients with severe symptoms such as seizures, stupor, coma, and respiratory arrest, regardless of the degree of hyponatremia. Emergency treatment should also be strongly considered for those with moderate-to-severe hyponatremia with a documented duration of less than 48 hours.
The goal is to correct hyponatremia at a rate that does not cause neurologic complications. The objective is to raise serum sodium (Na+) levels by 0.5-1 mmol/hour and not more than 10-12 mmol in the first 24 hours, to bring the sodium (Na+) value to a maximum level of 125 -130 mmol/L. Administration of 3% hypertonic saline should be restricted to these emergent circumstances, and both neurological symptoms and serum sodium (Na+) should be monitored frequently to achieve the desired target and to prevent overcorrection.
Correction of serum sodium (Na+) levels by 6 mmol/L in 24 hours has been dubbed the “rule of sixes.” The rule states that, “Six a day makes sense for safety; 6 in 6 hours for severe symptoms and stop” 24.
Other authors have recommended a rate of initial correction of 1-2 mmol/L/hour in severely symptomatic patients until symptoms resolve (or for the first 3-4 hour). However, total correction in the first 24 hours must not exceed 10-12 mmol. Central pontine myelinolysis has been reported in cases in which the initial correction exceeded 12 mmol and even in cases in which the correction was 9-10 mmol/24 h. This has led some authors to recommend a lower target of 8 mmol in 24 hours. In the special situation of exercise-induced hyponatremia with neurological symptoms, some authors recommend an immediate bolus of 100 mL of 3% hypertonic saline repeated every 10 minutes until symptoms resolve 25.
Formulas for the dose and rate of hypertonic saline have been proposed based on a sodium (Na+) deficit to calculate the rate of administration of hypertonic fluids 26, 27. However, they have not been prospectively studied. Despite the correct use of these formulas, hyponatremia is often corrected too rapidly. Therefore, these formulas should serve only as guidelines. Patients still require frequent retesting of their serum sodium (Na+) concentration 28.
The approximate sodium (Na+) deficit can be estimated by using the following formula (0.5 L/kg for females):
- Sodium Deficit (mmol) = (Desired sodium (Na+) – Measured sodium (Na+)) x 0.6 L/kg x Weight (kg)
Three-percent (3%) hypertonic saline has 513 mmol/L each of sodium (Na+) and Cl- and has an osmolality of 1026 mOsm/L. The volume of hypertonic saline needed to correct that deficit can be calculated as follows:
- Volume of 3% Saline = (sodium deficit)/513 mmol/L sodium
Assuming a rate of correction of chronic hyponatremia of 0.5 mmol/L per hour, the amount of time needed to correct a given degree of hyponatremia is as follows:
- Time Needed for Correction = (Desired sodium (Na+) – Measured sodium (Na+))/0.5 mmol/L per hour
The rate of infusion of hypertonic saline is as follows:
- Rate = (Volume of 3% Saline)/(Time Needed for Correction)
Furosemide increases excretion of free water and has been used along with hypertonic saline in severe cases to limit treatment-induced volume expansion. The diuresis induced by furosemide has a urine solute concentration roughly equivalent to half-normal saline; thus, excretion of free water occurs. Electrolyte free water intake can be restricted. Combining furosemide with hypertonic saline and water restriction may lead to a faster rate of correction of serum Na and requires that serum sodium (Na+) osmolality and urine osmolality be checked frequently to monitor the change in serum sodium (Na+) values and to prevent overcorrection. Attention should also be paid to the prevention of severe hypokalemia in conjunction with treatment of hyponatremia.
Figure 2. Useful formulas in the management of hyponatremia
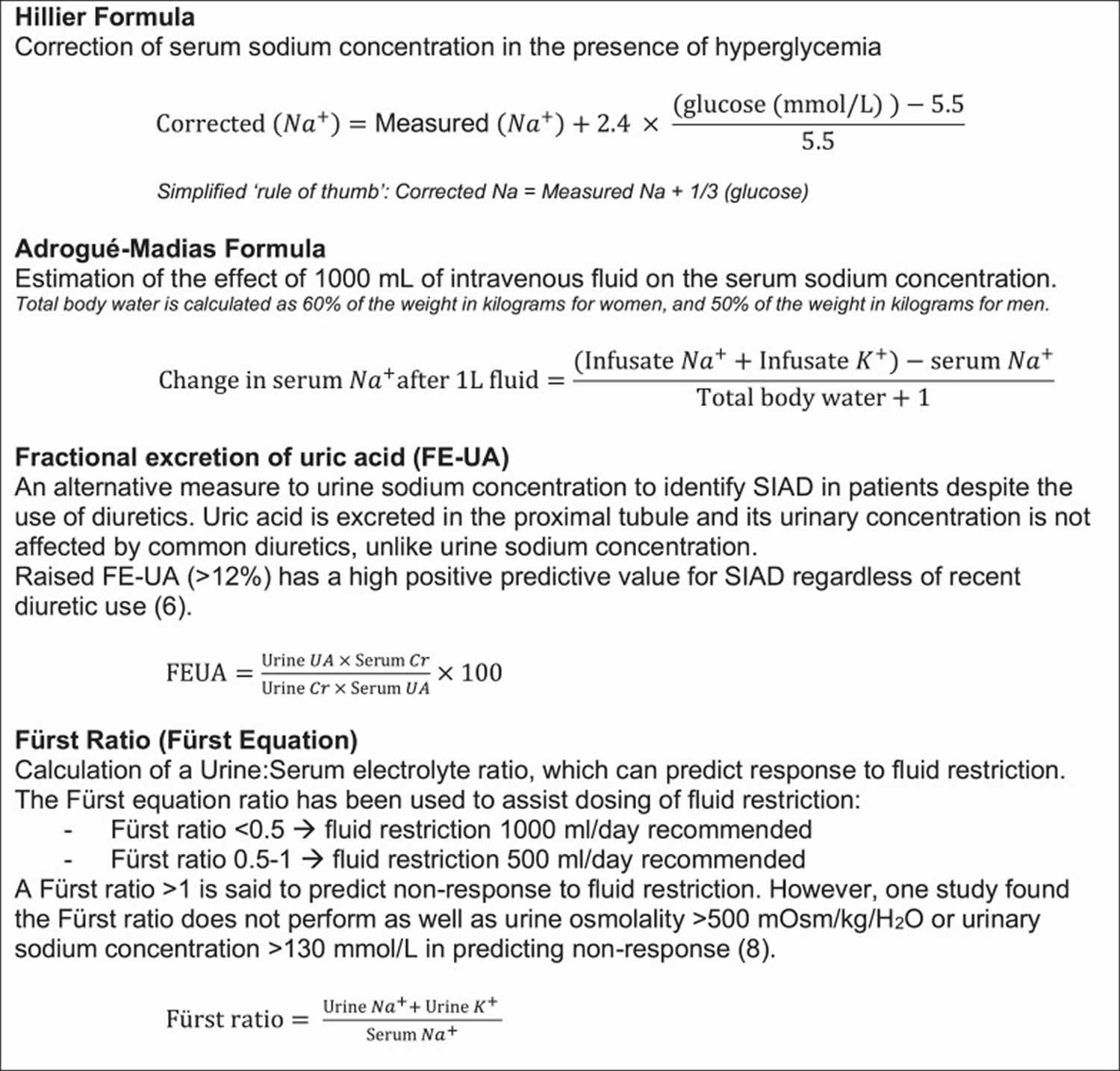
Abbreviations: Cr = creatinine; FEUA = fractional excretion of uric acid; mOsm = milliosmoles; Na+ = sodium; UA = uric acid.
[Source 29 ]Central pontine myelinolysis symptoms
Central pontine myelinolysis signs and symptoms appear two to three days after hyponatremia, or over the next one to two weeks may include any of the following:
- Confusion, delirium, hallucinations
- Impaired thinking
- Balance problems, tremor
- Difficulty with coordination
- Difficulty swallowing (dysphagia)
- Reduced alertness, depressed level of awareness, drowsiness or sleepiness, lethargy, poor responses
- Slurred speech
- Difficulty speaking
- Weakness or paralysis in the face, arms, or legs, usually affecting both sides of the body
- Muscle stiffness
- Impaired sensation
Patients most commonly have a history of rapid sodium correction, greater than 0.5-1.0 mEq/L per hour. The most susceptible patients are those with chronic hyponatremia (>48 hours) or those with severe hyponatremia (sodium less than 120 mEq/L).
The onset of symptoms is usually seen 1 to 14 days after electrolyte correction. Clinical features of central pontine myelinolysis reflect damage to upper motor neurons and generally present in a biphasic course. Initially, patients present with acute encephalopathy and seizures that typically resolve as normal sodium levels are restored. This is later followed by clinical deterioration 3 to 5 days later. Signs and symptoms include dysphagia, dysarthria, spastic quadriparesis, pseudobulbar paralysis, ataxia, lethargy, tremors, dizziness, catatonia, and in the most severe cases, locked-in-syndrome and coma 30, 31.
During the early course of central pontine myelinolysis (CPM), classical symptoms like weakness in the muscles used for speech often causes slowed or slurred speech (dysarthria), difficulty swallowing (dysphagia), muscle weakness in both legs and both arms (quadriparesis), and abnormal increase in muscle tone or stiffness of muscle (spasticity) are present when the respective anatomic structures are involved 13, 14. During the later course of central pontine myelinolysis (CPM), the pontine tegmentum is also involved. “Locked-in syndrome” occurs in severely affected patients and is a characteristic presentation of central pontine myelinolysis (CPM), which refers to the situation where these patients are awake, have preserved cognitive function and oculomotor function, but patients are unable to move and cannot perform voluntary movements (e.g., movement of limbs, respiratory muscles) and can communicate with the help of their eyes only 15.
Central pontine myelinolysis complications
Central pontine myelinolysis complications may include:
- Decreased ability to interact with others
- Decreased ability to work or care for self
- Inability to move, other than to blink eyes (“locked in syndrome”)
- Permanent nervous system damage
Secondary complications include venous thromboembolism (VTE), aspiration pneumonia, ventilator dependence, muscle atrophy, urinary tract infections, and decubitus ulcers.
Central pontine myelinolysis diagnosis
To diagnose central pontine myelinolysis your doctor will perform a physical exam and ask about your symptoms.
A head MRI scan may reveal a problem in the brainstem (pons) or other parts of the brain. This is the main diagnostic test. A head magnetic resonance imaging (MRI) scan may reveal a problem in the brainstem (pons) or other parts of the brain. This is the main diagnostic test. Characteristic findings on magnetic resonance imaging (MRI) are seen on diffusion-weighted imaging (DWI), showing diffusion restriction of the central pons with sparing of the periphery. These findings are usually seen within 24 hours of the onset of signs or symptoms. T2 and T2-flair images signal in a “bat-wing” shaped central pontine distribution and are generally seen later in presentation 14. Imaging findings can be delayed for up to 2 weeks, thus if imaging is negative, the diagnosis of central pontine myelinolysis is not excluded. If clinical suspicion for central pontine myelinolysis remains high, MRI should be repeated within two weeks 32.
Other tests may include:
- Brainstem auditory evoked response (BAER)
Lab tests that can confirm and help diagnose low sodium include:
- Comprehensive metabolic panel (includes blood sodium)
- Serum osmolality and serum sodium
- Urine sodium concentration and osmolality
- Urine potassium
- Toxicology screens for certain medicines
- Renal function tests: BUN and creatinine
- BSR (Blood sugar random)
- Thyroid profile
- Serum cortisol
- Serum K+, bicarbonate, chloride
- Fasting lipid profile
- Liver function tests
- Blood tests to check for bleeding disorders
Central pontine myelinolysis differential diagnosis
General imaging central pontine myelinolysis differential diagnosis include:
- Multiple sclerosis (MS)
- Hypertensive encephalopathy
- Pontine infarction from basilar perforators can be central, although usually, brainstem infarcts stop at the midline
- Pontine neoplasms including astrocytomas: brainstem is asymmetrically expanded with mass effect upon adjacent cisterns. local vessels may also be displaced
- Brainstem metastasis: usually enhances
- CNS lymphoma
- Progressive multifocal leukoencephalopathy
- Acute autoimmune or infectious encephalitis
- Mitochondrial encephalopathies
- CNS vasculitis
- Vigabatrin toxicity: bilateral dorsal pontine longitudinal restricted diffusion
Central pontine myelinolysis treatment
Central pontine myelinolysis is a medical emergency that needs to be treated in the hospital, fortunately most people with this condition are already in the hospital for another problem.
There is no known cure for central pontine myelinolysis. Treatment is focused on relieving symptoms.
Physical therapy may help maintain muscle strength, mobility, and function in weakened arms and legs.
Reintroduction of hyponatremia
5% dextrose in water (D5W) and desmopressin can be utilized with the goal of reintroducing hyponatremia to ensure that the rate of sodium correction will be 8-12 mEq/L when the rate of sodium correction has been too rapidly corrected 33. Desmopressin binds to V2 receptors of the renal collecting duct, which translocates aquaporin channels to the apical lumen of the collecting duct and increases water reabsorption. It can be given at a dose of 2 to 4 mcg intravenously or subcutaneously. 5% dextrose in water (D5W) at 6 mL/kg of lean body weight can be infused over 1 to 2 hours and should decrease serum sodium by 2 mEq/L. Infusion of 5% dextrose in water (D5W) is continued until goal serum sodium is reached 34.
Supportive care
Supportive care measures include ventilator support, intense physiotherapy and rehabilitation, and anti-parkinsonism drugs.
Experimental strategies
There have been no randomized control studies conducted to confirm the efficacy of these treatment modalities. However, they have been used in a small number of cases and have been shown to have positive outcomes.
Plasmapheresis has also been studied to improve neurologic complications of central pontine myelinolysis. In a small number of case studies in patients with severe hyponatremia, plasmapheresis was seen to improve neurologic manifestations from 10 days to 1-year post-therapy. Although patients improved clinically, MRI findings remained unchanged after plasmapheresis. These studies lead investigators to believe that therapeutic plasmapheresis could possibly reduce high-molecular myelinotoxic substances that are released during osmotic stress 35, 36.
The use of glucocorticoids, such as dexamethasone, has also been studied as glucocorticoids are known to impact the permeability of the blood-brain barrier. Studies done in rat models showed minimal neurologic impairment in rats that were treated with dexamethasone 2 mg/kg at 0 and 6 hours after hypertonic 3% saline was administered. The rats that were treated with dexamethasone also exhibited rare lesions on brain imaging in comparison to the untreated group, which exhibited numerous brain lesions. There have been few cases where dexamethasone was used in humans. However, this is not well studied, and further investigation is warranted 37.
Central pontine myelinolysis prognosis
The nerve damage caused by osmotic demyelination syndrome is often long-lasting. The disorder can cause serious long-term (chronic) disability. Some patients show complete recovery. Recent retrospective studies showing 94% survival. These studies cite that about 25%-40% make a complete recovery without deficits, and 25%-30% remain incapacitated 38, 39, 40.
Patients with risk factors for poor prognostic outcomes are those with serum sodium of <120 mEq/L, hypokalemia, and low Glasgow coma scale (GCS) during hospitalization. Autologous liver transplant patients who develop central pontine myelinolysis or osmotic demyelination syndrome were also reported to have worse outcomes, with a mortality of 63% at one year 41, 40.
Clinical and radiological features were not found to be of prognostic significance. Improving prognostic outcomes focuses on early recognition of those patients that are at higher risk of developing central pontine myelinolysis, avoiding rapid overcorrection of sodium, and making a prompt diagnosis of the condition. Favorable prognostic outcomes also include the avoidance of secondary complications of the condition such as aspiration pneumonia, urinary tract infection (UTI) or deep venous thrombosis (DVT) 38.
- Sterns RH. Adverse Consequences of Overly-Rapid Correction of Hyponatremia. Front Horm Res. 2019;52:130-142. doi: 10.1159/000493243[↩]
- Silver SM, Schroeder BM, Sterns RH, Rojiani AM. Myoinositol administration improves survival and reduces myelinolysis after rapid correction of chronic hyponatremia in rats. J Neuropathol Exp Neurol. 2006 Jan;65(1):37-44. doi: 10.1097/01.jnen.0000195938.02292.39[↩]
- Adams R.D., Victor M., Mancall E.L. Central pontine myelinolysis: a hitherto undescribed disease occurring in alcoholic and malnourished patients. AMA Arch Neurol Psychiatry. 1959;81:154–172.[↩]
- Tomlinson BE, Pierides AM, Bradley WG. Central pontine myelinolysis. Two cases with associated electrolyte disturbance. Q J Med. 1976 Jul;45(179):373-86.[↩]
- Kleinschmidt-DeMasters BK, Norenberg MD. Rapid correction of hyponatremia causes demyelination: relation to central pontine myelinolysis. Science. 1981 Mar 6;211(4486):1068-70. doi: 10.1126/science.7466381[↩]
- Kleinschmidt-DeMasters BK, Norenberg MD. Neuropathologic observations in electrolyte-induced myelinolysis in the rat. J Neuropathol Exp Neurol. 1982 Jan;41(1):67-80. doi: 10.1097/00005072-198201000-00007[↩]
- Laureno R. Central pontine myelinolysis following rapid correction of hyponatremia. Ann Neurol. 1983 Mar;13(3):232-42. doi: 10.1002/ana.410130303[↩]
- Sterns RH, Riggs JE, Schochet SS Jr. Osmotic demyelination syndrome following correction of hyponatremia. N Engl J Med. 1986 Jun 12;314(24):1535-42. doi: 10.1056/NEJM198606123142402[↩]
- Sterns RH. Severe symptomatic hyponatremia: treatment and outcome. A study of 64 cases. Ann Intern Med. 1987 Nov;107(5):656-64. doi: 10.7326/0003-4819-107-5-656[↩]
- Sterns RH. Neurological deterioration following treatment for hyponatremia. Am J Kidney Dis. 1989 May;13(5):434-7. doi: 10.1016/s0272-6386(89)80029-0[↩]
- Mohan S, Gu S, Parikh A, Radhakrishnan J. Prevalence of hyponatremia and association with mortality: results from NHANES. Am J Med. 2013 Dec;126(12):1127-37.e1. doi: 10.1016/j.amjmed.2013.07.021[↩]
- Upadhyay A, Jaber BL, Madias NE. Epidemiology of hyponatremia. Semin Nephrol. 2009 May;29(3):227-38. doi: 10.1016/j.semnephrol.2009.03.004[↩]
- Sciacca S, Lynch J, Davagnanam I, Barker R. Midbrain, Pons, and Medulla: Anatomy and Syndromes. Radiographics. 2019 Jul-Aug;39(4):1110-1125. doi: 10.1148/rg.2019180126[↩][↩]
- Martin RJ. Central pontine and extrapontine myelinolysis: the osmotic demyelination syndromes. J Neurol Neurosurg Psychiatry. 2004 Sep;75 Suppl 3(Suppl 3):iii22-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1765665/pdf/v075piii22.pdf[↩][↩][↩]
- Reijnders TDY, Janssen WMT, Niamut SML, Kramer AB. Role of Risk Factors in Developing Osmotic Demyelination Syndrome During Correction of Hyponatremia: A Case Study. Cureus. 2020 Jan 2;12(1):e6547. doi: 10.7759/cureus.6547[↩][↩]
- Ruzek KA, Campeau NG, Miller GM. Early diagnosis of central pontine myelinolysis with diffusion-weighted imaging. AJNR Am J Neuroradiol. 2004 Feb;25(2):210-3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7974598[↩][↩][↩][↩]
- Lee C, Ko C. Temporal Brain MRI Changes From Extrapontine Myelinolysis to Central Pontine Myelinolysis: A Case Report. Cureus. 2021 Nov 6;13(11):e19318. doi: 10.7759/cureus.19318[↩][↩][↩][↩]
- Adams RD, Victor M, Mancall EL. Central pontine myelinolysis: a hitherto undescribed disease occurring in alcoholic and malnourished patients. AMA Arch Neurol Psychiatry 1959;2013:154–72.[↩]
- Miller GM, Baker HL Jr, Okazaki H, Whisnant JP. Central pontine myelinolysis and its imitators: MR findings. Radiology. 1988 Sep;168(3):795-802. doi: 10.1148/radiology.168.3.3406409[↩]
- Singh N, Yu VL, Gayowski T. Central nervous system lesions in adult liver transplant recipients: clinical review with implications for management. Medicine (Baltimore). 1994 Mar;73(2):110-8. doi: 10.1097/00005792-199403000-00004[↩]
- Giuliani C, Peri A. Effects of Hyponatremia on the Brain. J Clin Med. 2014 Oct 28;3(4):1163-77. doi: 10.3390/jcm3041163[↩]
- Arieff AI, Llach F, Massry SG. Neurological manifestations and morbidity of hyponatremia: correlation with brain water and electrolytes. Medicine (Baltimore). 1976 Mar;55(2):121-9. doi: 10.1097/00005792-197603000-00002[↩]
- Haynes HR, Gallagher PJ, Cordaro A, Likeman M, Love S. A case of chronic asymptomatic central pontine myelinolysis with histological evidence of remyelination. Forensic Sci Med Pathol. 2018 Mar;14(1):106-108. doi: 10.1007/s12024-017-9933-y[↩]
- Sterns RH, Hix JK, Silver S. Treating profound hyponatremia: a strategy for controlled correction. Am J Kidney Dis. 2010 Oct;56(4):774-9. doi: 10.1053/j.ajkd.2010.04.020[↩]
- Hew-Butler T, Noakes TD, Siegel AJ. Practical management of exercise-associated hyponatremic encephalopathy: the sodium paradox of non-osmotic vasopressin secretion. Clin J Sport Med. 2008 Jul;18(4):350-4. doi: 10.1097/JSM.0b013e3181802c6d. Erratum in: Clin J Sport Med.2008 Sep;18(5):382.[↩]
- Ellison DH, Berl T. Clinical practice. The syndrome of inappropriate antidiuresis. N Engl J Med. 2007 May 17;356(20):2064-72. doi: 10.1056/NEJMcp066837[↩]
- Voets PJGM, Vogtländer NPJ. A quantitative approach to intravenous fluid therapy in the syndrome of inappropriate antidiuretic hormone secretion. Clin Exp Nephrol. 2019 Aug;23(8):1039-1044. doi: 10.1007/s10157-019-01741-6[↩]
- Clayton JA, Le Jeune IR, Hall IP. Severe hyponatraemia in medical in-patients: aetiology, assessment and outcome. QJM. 2006 Aug;99(8):505-11. doi: 10.1093/qjmed/hcl071[↩]
- Warren AM, Grossmann M, Christ-Crain M, Russell N. Syndrome of Inappropriate Antidiuresis: From Pathophysiology to Management. Endocr Rev. 2023 Sep 15;44(5):819-861. doi: 10.1210/endrev/bnad010[↩]
- Kleinschmidt-Demasters BK, Rojiani AM, Filley CM. Central and extrapontine myelinolysis: then…and now. J Neuropathol Exp Neurol. 2006 Jan;65(1):1-11. doi: 10.1097/01.jnen.0000196131.72302.68[↩]
- Odier C, Nguyen DK, Panisset M. Central pontine and extrapontine myelinolysis: from epileptic and other manifestations to cognitive prognosis. J Neurol. 2010 Jul;257(7):1176-80. doi: 10.1007/s00415-010-5486-7[↩]
- de Souza A. Movement disorders and the osmotic demyelination syndrome. Parkinsonism Relat Disord. 2013 Aug;19(8):709-16. doi: 10.1016/j.parkreldis.2013.04.005[↩]
- Danyalian A, Heller D. Central Pontine Myelinolysis. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551697[↩]
- Sterns RH, Hix JK, Silver SM. Management of hyponatremia in the ICU. Chest. 2013 Aug;144(2):672-679. doi: 10.1378/chest.12-2600[↩]
- Bibl D, Lampl C, Gabriel C, Jüngling G, Brock H, Köstler G. Treatment of central pontine myelinolysis with therapeutic plasmapheresis. Lancet. 1999 Apr 3;353(9159):1155. doi: 10.1016/S0140-6736(99)01145-9[↩]
- Grimaldi D, Cavalleri F, Vallone S, Milanti G, Cortelli P. Plasmapheresis improves the outcome of central pontine myelinolysis. J Neurol. 2005 Jun;252(6):734-5. doi: 10.1007/s00415-005-0738-7[↩]
- Sugimura Y, Murase T, Takefuji S, Hayasaka S, Takagishi Y, Oiso Y, Murata Y. Protective effect of dexamethasone on osmotic-induced demyelination in rats. Exp Neurol. 2005 Mar;192(1):178-83. doi: 10.1016/j.expneurol.2004.10.018[↩]
- Menger H, Jörg J. Outcome of central pontine and extrapontine myelinolysis (n = 44). J Neurol. 1999 Aug;246(8):700-5. doi: 10.1007/s004150050435[↩][↩]
- King JD, Rosner MH. Osmotic demyelination syndrome. Am J Med Sci. 2010 Jun;339(6):561-7. doi: 10.1097/MAJ.0b013e3181d3cd78[↩]
- Kallakatta RN, Radhakrishnan A, Fayaz RK, Unnikrishnan JP, Kesavadas C, Sarma SP. Clinical and functional outcome and factors predicting prognosis in osmotic demyelination syndrome (central pontine and/or extrapontine myelinolysis) in 25 patients. J Neurol Neurosurg Psychiatry. 2011 Mar;82(3):326-31. doi: 10.1136/jnnp.2009.201764[↩][↩]
- Morard I, Gasche Y, Kneteman M, Toso C, Mentha A, Meeberg G, Mentha G, Kneteman N, Giostra E. Identifying risk factors for central pontine and extrapontine myelinolysis after liver transplantation: a case-control study. Neurocrit Care. 2014 Apr;20(2):287-95. doi: 10.1007/s12028-013-9928-9[↩]





{kind=link}