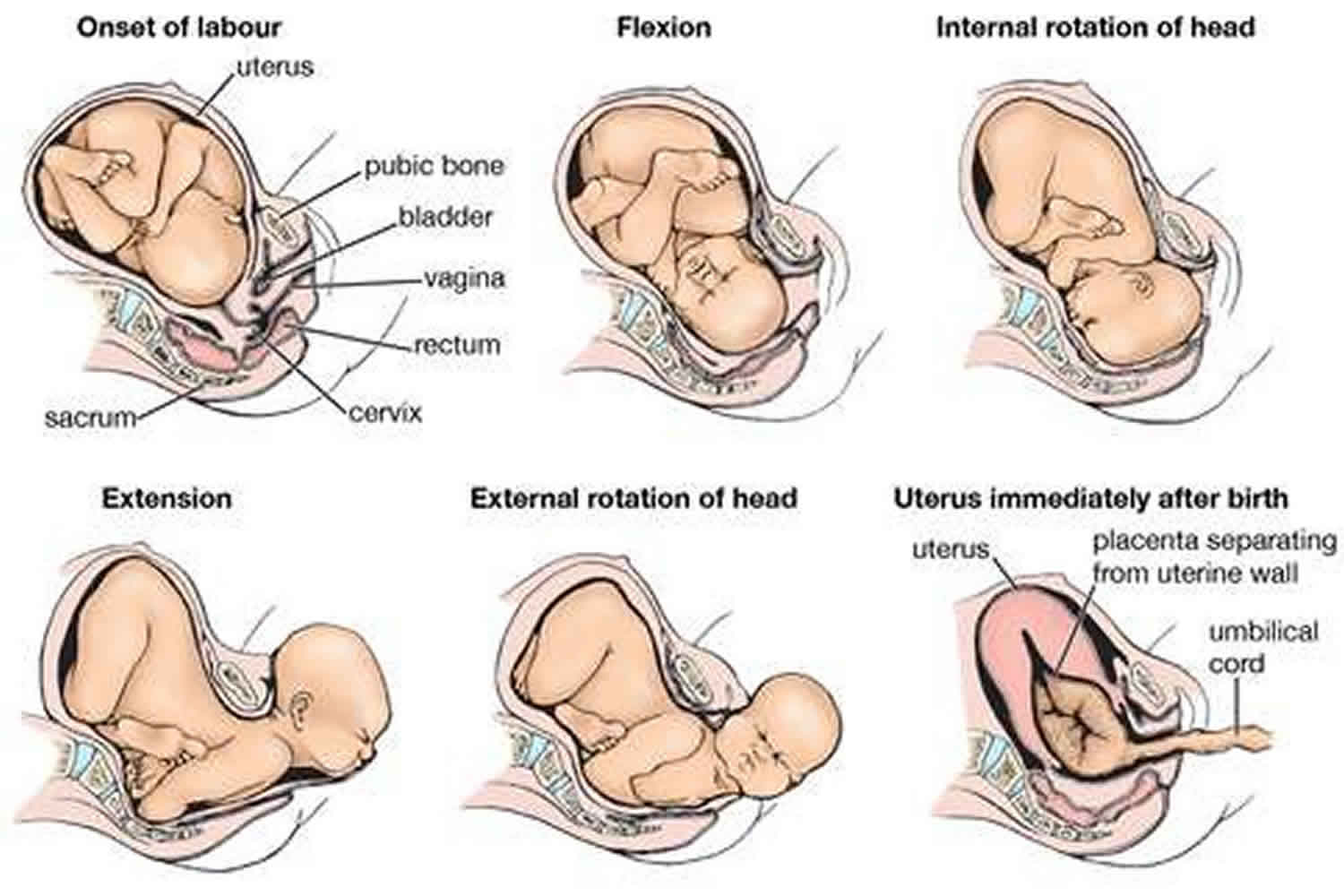
Cephalic presentation
A cephalic presentation or head presentation or head-first presentation is a situation at childbirth where the fetus is in a longitudinal lie and the head enters the pelvis first; the most common form of cephalic presentation is the vertex presentation where the occiput is the leading part (the part that first enters the birth canal). All other presentations are abnormal (malpresentations) which are either more difficult to deliver or not deliverable by natural means. Non-cephalic presentations are the breech presentation (3.5%) and the shoulder presentation (0.5%). In vertex presentations the head of the fetus most commonly faces to the right and slightly to the rear. This position is said to be the most usual one because the fetus is thus best accommodated to the shape of the uterus. In face presentation it may be necessary to turn the fetus before delivery if the chin is directed backward.
Bedside ultrasound can be employed to confirm the presentation and position of the fetal presenting part. Particular mention should be noted in the case of breech presentation due to its increased risks regarding fetal morbidity and mortality compared with the cephalic presenting fetus. In breech presentation the buttocks or the legs are the first to pass through the pelvis. The feet may be alongside the buttocks, or the legs may be extended against the face. Because the head is the last part of the fetus to be delivered in breech birth, there is some danger that the fetus will be asphyxiated; there is also danger that the umbilical cord will be compressed during birth of the head. About 25% of fetuses will be in breech presentation at 28 weeks, and this decreases to about 3% to 4% of term pregnancies 1. Most of these patients will be delivered by cesarean delivery. Transverse presentation, which occurs only once in several hundred labors, requires turning of the fetus before vaginal delivery or else delivery by cesarean section.
The movement of the fetus to cephalic presentation is called head engagement. It occurs in the third trimester. In head engagement, the fetal head descends into the pelvic cavity so that only a small part (or none) of it can be felt abdominally. The perineum and cervix are further flattened and the head may be felt vaginally. Head engagement is known colloquially as the baby drop, and in natural medicine as the lightening because of the release of pressure on the upper abdomen and renewed ease in breathing. However, it severely reduces bladder capacity, increases pressure on the pelvic floor and the rectum, and the mother may experience the perpetual sensation that the fetus will “fall out” at any moment.
In the vertex presentation the head is flexed and the occiput leads the way. This is the most common configuration and seen at term in 95% of singletons. If the head is extended, the face becomes the leading part. Face presentations account for less than 1% of presentations at term. In the sinicipital presentation the large fontanelle is the presenting part; with further labor the head will either flex or extend more so that in the end this presentation leads to a vertex or face presentation. In the brow presentation the head is slightly extended, but less than in the face presentation. The chin presentation is a variant of the face presentation with maximum extension of the head.
Many factors determine the optimal way to deliver a baby. A vertex presentation is the ideal situation for a vaginal birth, however, occiput posterior positions tend to proceed more slowly, often requiring an intervention in the form of forceps, vacuum extraction, or Cesarean section 2. In a large study, a majority of brow presentations were delivered by Cesarean section, however, because of ‘postmaturity’, factors other than labor dynamics may have played a role 3. Most face presentations can be delivered vaginally as long as the chin is anterior; there is no increase in fetal or maternal mortality 4. Mento-posterior positions cannot be delivered vaginally in most cases (unless rotated) and are candidates for Cesarean section in contemporary management 4.
Vertex presentation
The vertex is the area of the vault bounded anteriorly by the anterior fontanelle and the coronal suture, posteriorly by the posterior fontanelle and the lambdoid suture and laterally by 2 lines passing through the parietal eminences.
In the vertex presentation the occiput typically is anterior and thus in an optimal position to negotiate the pelvic curve by extending the head. In an occiput posterior position, labor becomes prolonged and more operative interventions are deemed necessary. The prevalence of the persistent occiput posterior is given as 4.7%.
The vertex presentations are further classified according to the position of the occiput, it being right, left, or transverse, and anterior or posterior:
- Left Occipito-Anterior (LOA), Left Occipito-Posterior (LOP), Left Occipito-Transverse (LOT);
- Right Occipito-Anterior (ROA), Right Occipito-Posterior (ROP), Right Occipito-Transverse (ROT);
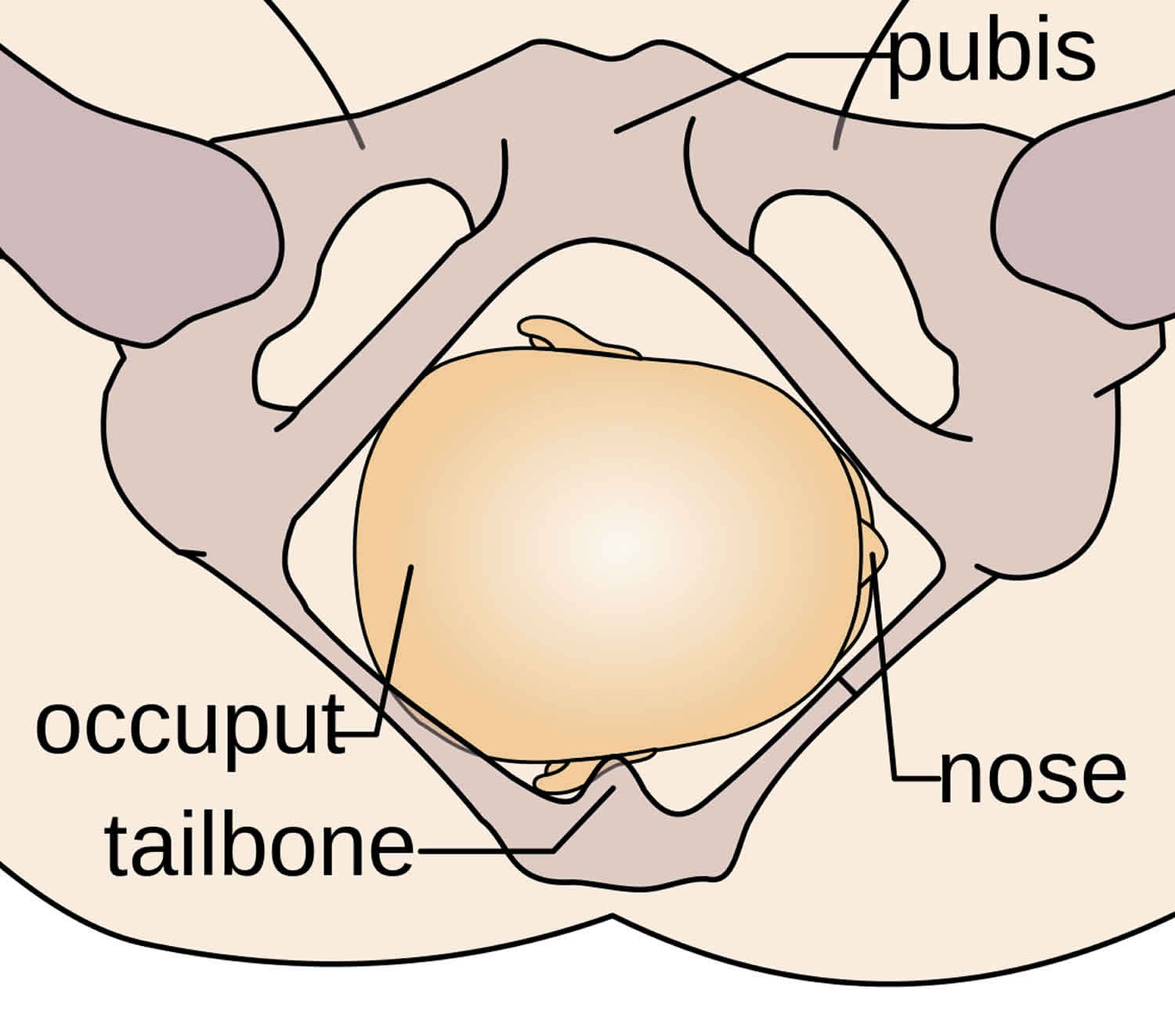
The Occipito-Anterior position is ideal for birth – it means that the baby is lined up so as to fit through the pelvis as easily as possible. The baby is head down, facing the spine, with its back anterior. In this position, the baby’s chin is tucked onto its chest, so that the smallest part of its head will be applied to the cervix first. The position is usually “Left Occiput Anterior”, or LOA. Occasionally, the baby may be “Right Occiput Anterior”, or ROA.
Figure 1. Vertex presentation
Face presentation
Factors that predispose to face presentation are prematurity, macrosomia, anencephaly and other malformations, cephalopelvic disproportion, and polyhydramnios 5. In an uncomplicated face presentation duration of labor is not altered. Perinatal losses with face presentation occur with traumatic version and extraction and midforceps procedures. Duff 6 indicates that the prevalence of face presentations is about 1/500–600, while Benedetti et al. 7 found it to be 1/1,250 term deliveries.
Face presentations are classified according to the position of the chin (mentum):
- Left Mento-Anterior (LMA), Left Mento-Posterior (LMP), Left Mento-Transverse (LMT);
- Right Mento-Anterior (RMA), Right Mento-Posterior (RMP), Right Mento-Transverse (RMT);
Brow presentation
While some consider the brow presentation as an intermediate stage towards the face presentation, others disagree. Thus Bhal et al. indicated that both conditions are about equally common (1/994 face and 1/755 brow positions), and that prematurity was more common with face while postmaturity was more common with brow positions 3.
Oskie presentation
The Oskie presentation is similar to the Occipito-Anterior position, where the baby is head down, facing the spine, with back on the ventral side of the uterus; however, in this position, while the torso is aligned with the mother’s longitudinal axis, the legs of the fetus are extended straight along the frontal axis of the mother, as if the baby is creating a right angle with its body. For the Oskie position to occur the baby’s head must be far down the pelvis in order to allow room for leg extension, typically the arms are bent, tucked against the baby’s body. There are no known complications for labor and delivery. This presentation is rare and is not well researched.
- Shanahan MM, Gray CJ. External Cephalic Version. [Updated 2019 Jun 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482475[↩]
- [Effects of persistent occiput posterior presentation on mode of delivery]. Z Geburtshilfe Perinatol. 1994 Aug;198(4):117-9. https://www.ncbi.nlm.nih.gov/pubmed/7975796[↩]
- A population study of face and brow presentation. J Obstet Gynaecol. 1998 May;18(3):231-5. https://www.ncbi.nlm.nih.gov/pubmed/15512065[↩][↩]
- [Face presentation: retrospective study of 32 cases at term]. Gynecol Obstet Fertil. 2006 May;34(5):393-6. Epub 2006 Apr 21. https://www.ncbi.nlm.nih.gov/pubmed/16630740[↩][↩]
- Face and brow presentation: independent risk factors. J Matern Fetal Neonatal Med. 2008 Jun;21(6):357-60. doi: 10.1080/14767050802037647. https://www.ncbi.nlm.nih.gov/pubmed/18570114[↩]
- Diagnosis and management of face presentation. Obstet Gynecol. 1981 Jan;57(1):105-12. https://www.ncbi.nlm.nih.gov/pubmed/7005774[↩]
- Face presentation at term. Obstet Gynecol. 1980 Feb;55(2):199-202. https://www.ncbi.nlm.nih.gov/pubmed/7352081[↩]




{kind=link}