Cervical effacement
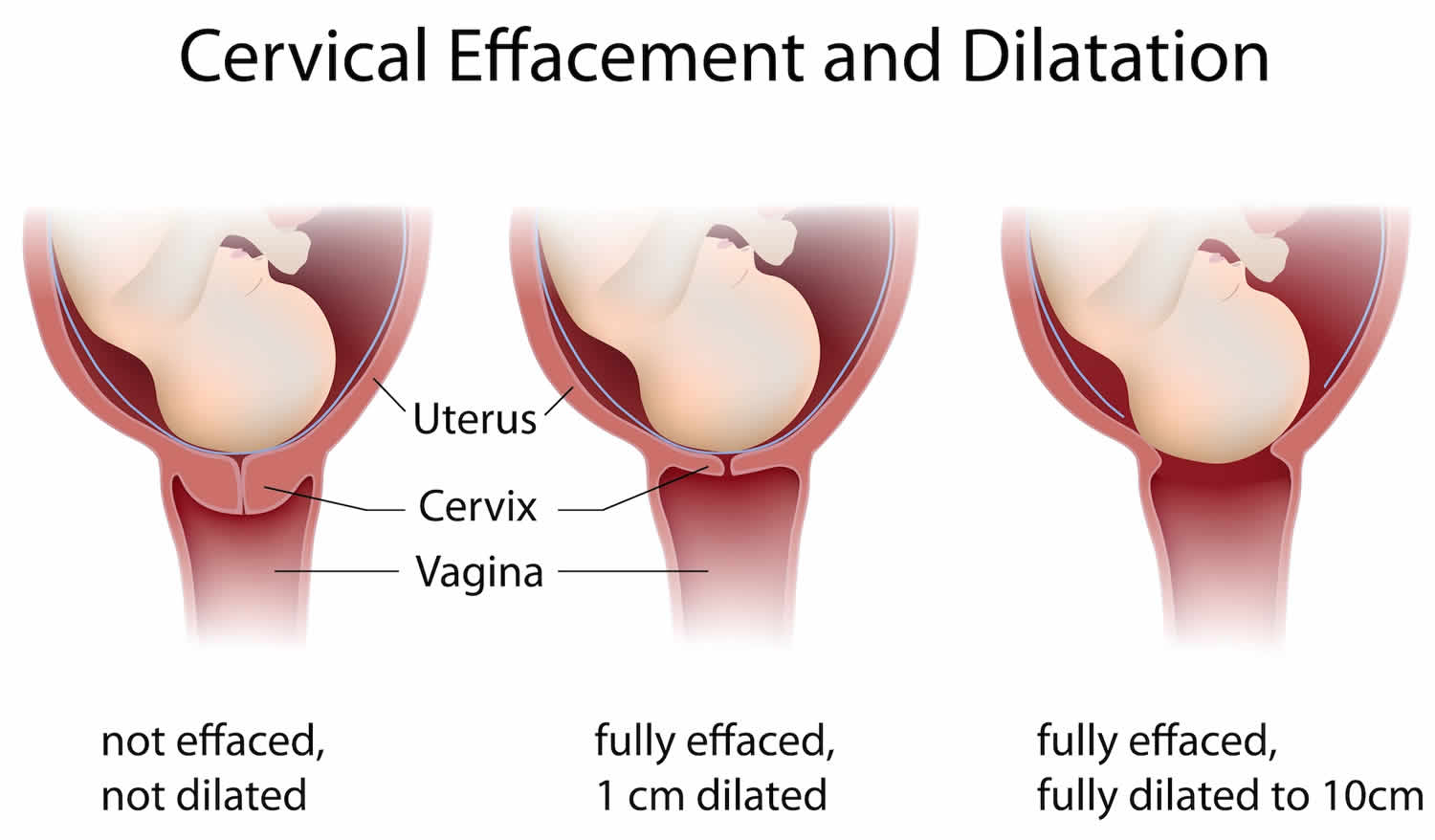
Cervical effacement is the thinning or shortening of the cervix that is graded 0-100 percent of the whole cervix that occurs throughout the first stage of labor. Zero percent cervical effacement means the cervix is a normal, pre-labor length. Fifty percent cervical effacement means the cervix is at half of the expected length. If the cervix is 100% effaced, it is paper thin. Cervical effacement refers to the cervical length in the anterior-posterior plane 1. Cervix effacement is measured by estimating the percentage remaining of the length of the thinned cervix compared to the uneffaced cervix. As you may know from childbirth class, the cervix is the gateway between the uterus and the vagina. The cervix needs to soften, thin (efface) and dilate (open), to allow the baby to enter the birth canal. The whole process is called cervical ripening.
Figure 1. Cervical effacement
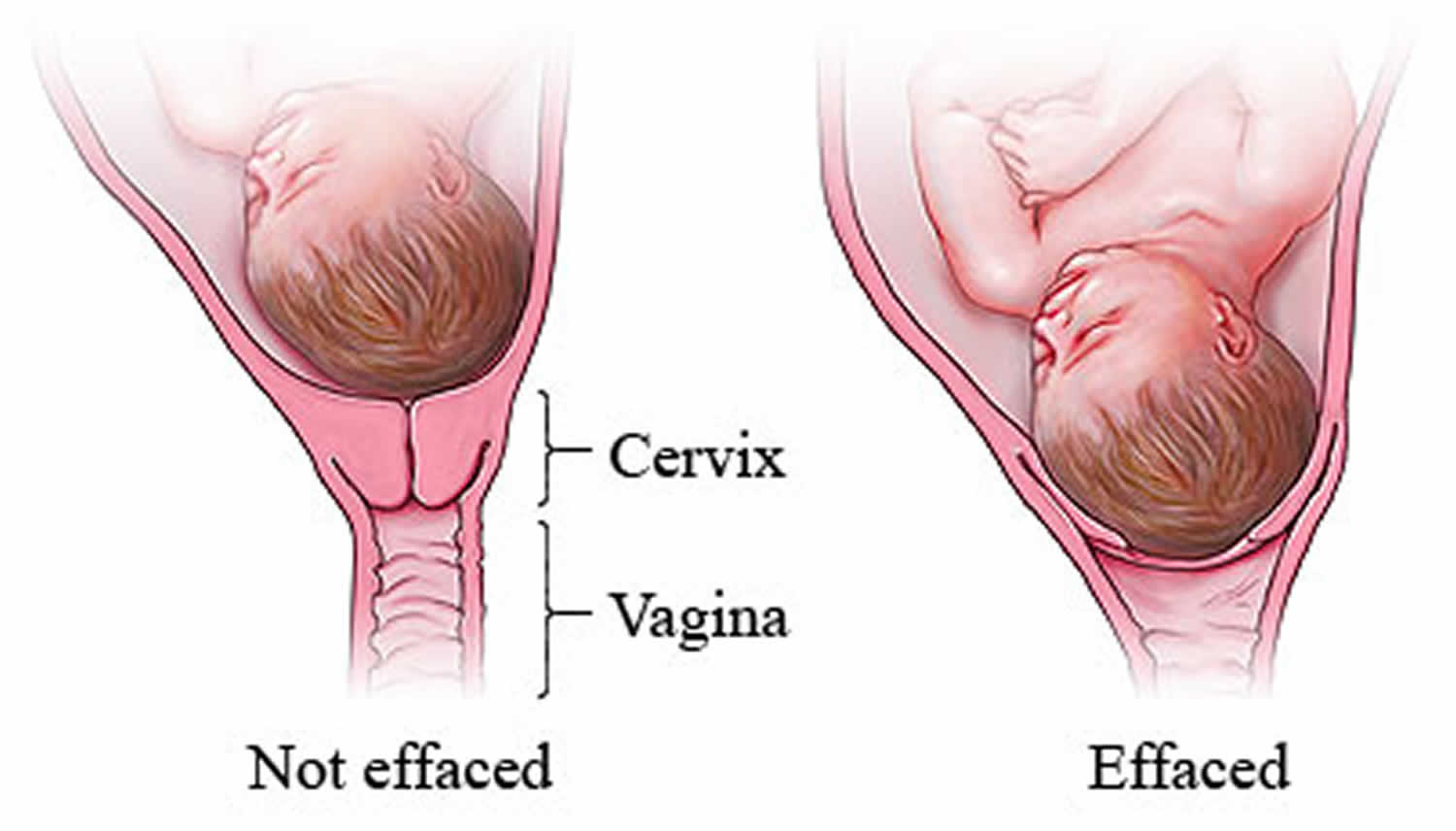
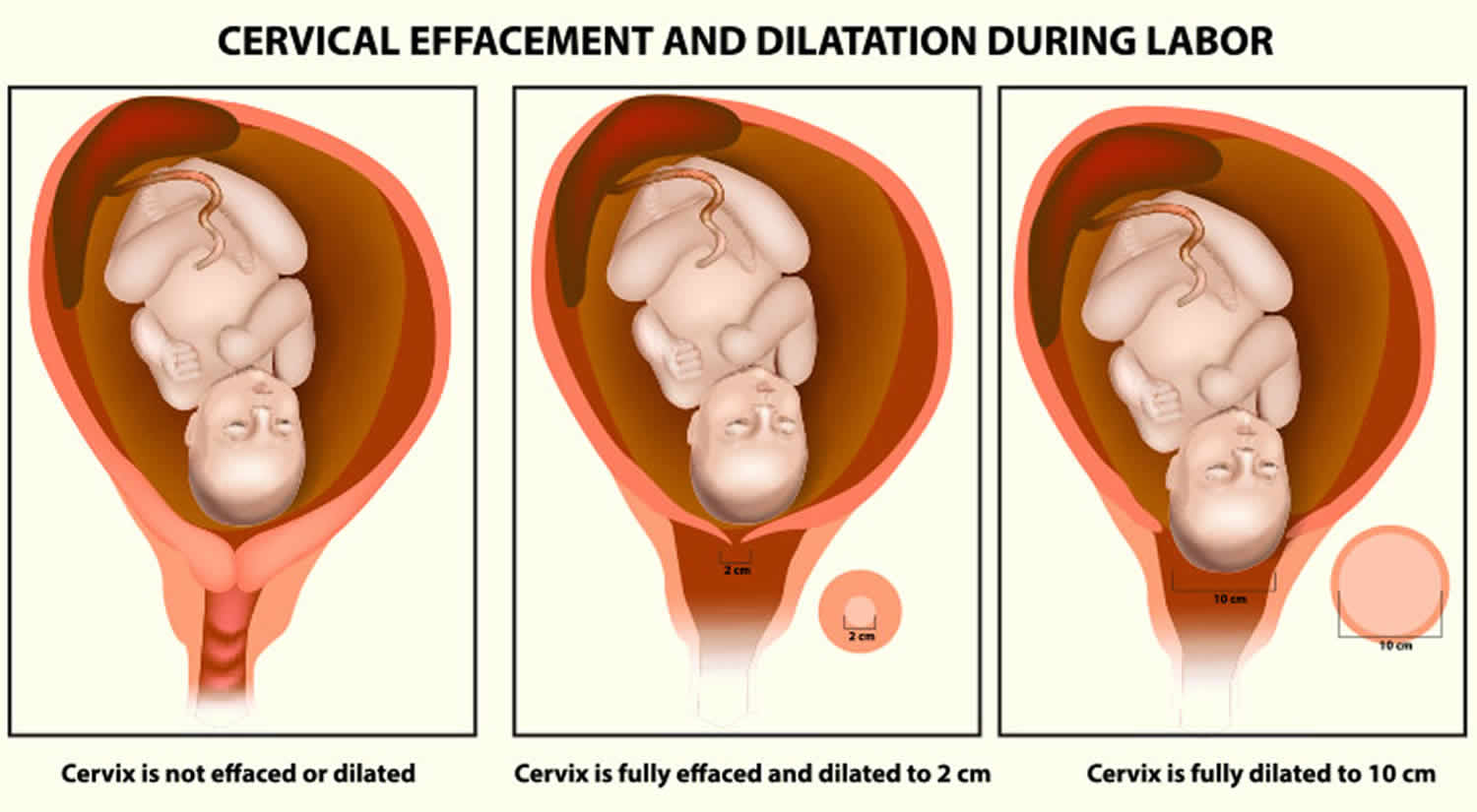
Figure 2. Cervical dilation
Footnote: As labor nears, the fetus’s head drops down into the pelvis and pushes against the cervix. The cervix begins to thin (efface) and open (dilate), sometimes over a few weeks.
Signs cervix is thinning
You can’t feel cervix effacement as it’s happening, at least not definitively. But you might notice a few signs your cervix is doing the ripening. As you approach your due date, you will be looking for any little sign that labor is about to start. You might notice that your baby has “dropped” or moved lower into your pelvis. This is called “lightening.” If you have a pelvic exam during your prenatal visit, your doctor might report changes in your cervix that you cannot feel, but that suggest your body is getting ready. For some women, a flurry of energy and the impulse to cook or clean, called “nesting,” is a sign that labor is approaching.
Some signs suggest that labor will begin very soon. Call your doctor or midwife if you have any of the following signs of labor. Call your doctor even if it’s weeks before your due date — you might be going into preterm labor. Your doctor or midwife can decide if it’s time to go to the hospital or if you should be seen at the office first.
- You have contractions that become stronger at regular and increasingly shorter intervals.
- You have lower back pain and cramping that does not go away.
- Your water breaks (can be a large gush or a continuous trickle).
- You have a bloody (brownish or red-tinged) mucus discharge. This is probably the mucus plug that blocks the cervix. Losing your mucus plug usually means your cervix is dilating (opening up) and becoming thinner and softer (effacing). Labor could start right away or may still be days away.
It’s not always easy to know if your water breaks. If your water breaks it could be a gush or a slow trickle of amniotic fluid. Rupture of membranes is the medical term for your water breaking. Let your doctor know the time your water breaks and any color or odor. Also, call your doctor if you think your water broke, but are not sure. An easy test can tell your doctor if the leaking fluid is urine (many pregnant women leak urine) or amniotic fluid. Often a woman will go into labor soon after her water breaks. When this doesn’t happen, her doctor may want to induce (bring about) labor. This is because once your water breaks, your risk of getting an infection goes up as labor is delayed.
Throughout pregnancy, women may experience painful contractions which do not lead to cervical dilation or effacement, referred to as false labor.
False labor
Many women, especially first-time mothers-to-be, think they are in labor when they’re not. This is called false labor. “Practice” contractions called Braxton Hicks contractions are common in the last weeks of pregnancy or earlier. The tightening of your uterus might startle you. Some might even be painful or take your breath away. It’s no wonder that many women mistake Braxton Hicks contractions for the real thing. So don’t feel embarrassed if you go to the hospital thinking you’re in labor, only to be sent home.
So, how can you tell if your contractions are true labor?
Time them. Use a watch or clock to keep track of the time one contraction starts to the time the next contraction starts, as well as how long each contraction lasts. With true labor, contractions become regular, stronger, and more frequent. Braxton Hicks contractions are not in a regular pattern, and they taper off and go away. Some women find that a change in activity, such as walking or lying down, makes Braxton Hicks contractions go away. This won’t happen with true labor. Even with these guidelines, it can be hard to tell if labor is real. If you ever are unsure if contractions are true labor, call your doctor.
Women will often self-present to obstetrical triage with concern for the onset of labor. Common chief complaints include painful contractions, vaginal bleeding/bloody show, and leakage of fluid from the vagina 1. It is up to the clinician to determine if the patient is in labor, defined as regular, clinically significant contractions with an objective change in cervical dilation and/or effacement 2.
How to check cervix dilation and effacement
How to check if you have an effaced cervix? Your doctor will likely check for you at your appointments as you near your due date. Wearing a sterile glove, they’ll insert fingers into the vagina and feel the cervix to gauge dilation and effacement.
It is possible to check your own cervix for dilation and effacement, though it might be tricky to reach if you’re not in labor yet, and some women just don’t feel comfortable doing it. Plus, you don’t need to keep super close tabs on effacement and dilation. It’s more essential to keep a lookout for other signs of labor: regular contractions and water breaking are the two biggies.
Many pregnant women want to know what to do if they’re effaced but not dilated—but really there’s nothing “to do.” It’s normal for a cervix to start effacement before it starts dilating. And—especially if this is your first birth—the process may take up to a few weeks. It’s tough, but try to be patient!
Some women try to jump start labor naturally using techniques such as walking, squatting, having sex or getting acupuncture. You’ll want to get an OK from your doctor before trying any induction technique, and it might not help, but you can certainly try.
Ripening the cervix
Ripening the cervix is a procedure that helps the cervix soften and thin out so that it will dilate (open) during labor. Before inducing labor, your obstetrician–gynecologist (ob-gyn) or other health care professional may check to see if your cervix is ready using the Bishop score. With this scoring system, a number ranging from 0 to 13 is given to rate the condition of the cervix. A score of 6 or less means that your cervix is not yet ready for labor. If the cervix is not ready, ripening may be done.
Ripening of the cervix may be done in the following ways:
- Using medications that contain prostaglandins. These drugs can be inserted into the vagina or taken by mouth.
- Using a thin tube that has an inflatable balloon on the end. The tube is inserted into the cervix and then expanded. This helps widen the cervix.
When not to check your cervix during pregnancy?
The cervix should not be checked either by you or by a healthcare professional in these cases.
- In case you have had bad experiences with checking the cervix for dilation, you should avoid trying it again.
- If it causes too much pain, then stop doing it.
- When the placenta is covering the cervix (placenta previa), it is not recommended to check the cervix.
- If you have any sutures, you shouldn’t check your cervix.
If your doctor finds it risky to check cervical dilation, then do not attempt it. Cervical dilation should only be done when your medical professional has recommended it. Otherwise, do not attempt it.
- Hutchison J, Mahdy H, Hutchison J. Stages of Labor. [Updated 2019 Aug 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544290[↩][↩]
- Liao JB, Buhimschi CS, Norwitz ER. Normal labor: mechanism and duration. Obstet. Gynecol. Clin. North Am. 2005 Jun;32(2):145-64, vii.[↩]





{kind=link}