
What is Duodenitis
Duodenitis is inflammation of the duodenum, the first part of your small intestine (see below) 1, 2, 3, 4, 5, 6, 7. Your duodenum is the initial C-shaped segment of the small intestine and is a continuation of the pylorus (the part that’s closest to your stomach) 8. Your duodenum helps to further digest food coming from your stomach. It absorbs nutrients (vitamins, minerals, carbohydrates, fats, proteins) and water from food so they can be used by your body. Your duodenum has a protective lining that keeps out germs like bacteria, viruses and parasites. Your duodenum also shields against damage from your stomach’s highly acidic digestive juices. Duodenitis is similar to gastritis, which is inflammation of the stomach lining. Common causes of duodenitis include Helicobacter pylori infection, certain medications like nonsteroidal anti-inflammatory drugs (NSAIDs), and autoimmune disorders (a group of disorders where your body’s immune system mistakenly attacks its own healthy cells and tissues leading to inflammation, damage, and a range of symptoms depending on the affected organ or system) 9, 10. Duodenitis symptoms can include abdominal pain, bloating, nausea, and bloody stools. Duodenitis treatment often involves medications to reduce stomach acid or antibiotics if Helicobacter pylori infection is present.
Duodenitis doesn’t always cause symptoms. When it does, people experience duodenitis differently. Duodenitis symptoms may come and go. They may be ongoing but mild. Or you may have sudden, severe symptoms that alert you that it’s time to see your doctor.
Duodenitis symptoms may include:
- Upper abdominal pain (a gnawing or burning sensation called indigestion that improves when you eat).
- Bloating (tight, full or painful feeling in your upper abdomen after eating).
- Nausea and vomiting.
- Diarrhea.
- Fatigue.
- Gas.
- Loss of appetite.
Bleeding in your digestive tract is sometimes a sign of severe duodenitis. Signs include:
- Blood in your vomit (may look like coffee grounds).
- Blood in your poop (may look dark-colored or tarry).
You should see a doctor if you notice these signs, which may mean you have duodenitis or another digestive system condition that needs treatment.
Your doctor is likely to suspect duodenitis after talking to you about your medical history and performing an exam. If your doctor suspects duodenitis, he/she will perform tests to figure out what’s causing the inflammation. Tests may include:
- Tests for H. pylori. Your doctor may recommend tests such as a stool test or breath test to determine whether you have H. pylori infection. Which type of test you have depends on your situation. For the breath test, you drink a small glass of clear, tasteless liquid that contains radioactive carbon. H. pylori germs break down the test liquid in your stomach. Later, you blow into a bag, which is then sealed. If you’re infected with H. pylori, your breath sample will contain the radioactive carbon.
- Blood tests: A blood sample can show if you have a germ, like H. pylori, that’s causing an infection. A blood test can also show if you have antibodies for gluten as in celiac disease. Antibodies are proteins your immune system makes to fight germs. Antibody blood tests are usually the first tests that are ordered to diagnose celiac disease. These tests look for proteins created during the body’s immune response, known as antibodies, that are present in most people with celiac disease.
- Stool test: Your poop can show if you have an H. pylori infection.
- Passing a thin, flexible scope down the throat, called an upper endoscopy. Endoscopy is a procedure to examine the digestive system with a long, thin tube with a tiny camera, called an endoscope. The endoscope passes down the throat, into the esophagus, stomach and small intestine. Using the endoscope, your doctor looks for signs of inflammation. The scope contains instruments that can take tissue samples for lab testing. Depending on your age and medical history, your doctor may recommend this as a first test instead of testing for H. pylori.
- Upper GI series: This series of X-rays takes images of your upper digestive system. You may have to swallow a white, metallic liquid that contains barium. The liquid coats your digestive tract and makes an ulcer more visible. This procedure is called a barium swallow. It can show how these organs work together so your doctor can better understand what’s causing inflammation in your duodenum.
If a suspicious area is found, your doctor may remove small tissue samples, called a biopsy, to test in a lab. A biopsy also can identify the presence of H. pylori in your duodenum lining.
Treatment of duodenitis depends on the specific cause. Acute duodenitis caused by nonsteroidal anti-inflammatory drugs (NSAIDs) or alcohol may be relieved by stopping use of those substances.
Medicines used to treat duodenitis include:
- Antibiotics to kill Helicobacter pylori. For H. pylori in your digestive tract, your doctor may recommend a combination of antibiotics to kill the Helicobacter pylori bacteria. Be sure to take the full antibiotic prescription, usually for 7 to 14 days. You also may take a medicine to block acid production. Once treated, your doctor will retest you for H. pylori to be sure it has been destroyed.
- Medicines that block acid production and promote healing. Medicines called proton pump inhibitors (PPIs) help reduce acid. They do this by blocking the action of the parts of cells that produce acid. You may get a prescription for proton pump inhibitors (PPIs) or you can buy them without a prescription. Long-term use of proton pump inhibitors (PPIs), particularly at high doses, may increase your risk of hip, wrist and spine fractures. Ask your doctor whether a calcium supplement may reduce this risk.
- Medicines to reduce acid production. Acid blockers, also called histamine blockers or H2 blockers, reduce the amount of acid released into your digestive tract. Reducing acid relieves duodenitis pain and encourages healing. You may get a prescription for an acid blocker, or you can buy one without a prescription.
- Medicines that neutralize stomach acid. Your doctor may include an antacid in your treatment. Antacids neutralize existing stomach acid and can provide rapid pain relief. These help with immediate symptom relief but are generally not used as a primary treatment. Side effects of antacids can include constipation or diarrhea, depending on the main ingredients. Proton pump inhibitors and acid blockers are more effective and have fewer side effects.
Is duodenitis serious?
For most people, duodenitis is short-term and isn’t serious and improves quickly with treatment. The inflammation of your duodenum goes away on its own. Long-lasting symptoms are a sign of chronic duodenitis 11. Chronic duodenitis requires medical treatment, which may involve taking one or more medicines. Treating duodenitis usually eases the inflammation and prevents complications, like damage to your duodenum’s lining.
Is duodenitis contagious?
The duodenitis or inflammation of your duodenum isn’t contagious, but the Helicobacter pylori bacteria that usually cause the inflammation are. Helicobacter pylori bacteria spread from person to person through saliva (spit), poop and contaminated food and water. For example, you can contract H. pylori from kissing. You can also get it from eating food prepared by an infected person who didn’t wash their hands after going to the bathroom.
How can I lower my risk of duodenitis?
You can follow good hygiene practices to reduce your risk of infection. Make sure you live a healthy lifestyle.
- Wash your hands. Proper handwashing techniques done at the right times can keep you from getting sick. Wash your hands when you’re preparing food and before eating. Wash your hands each time you finish using the toilet.
- Don’t smoke. If you do smoke, work with your healthcare provider on a plan to quit.
- Don’t drink alcohol. Alcohol can irritate the mucous lining of your stomach and duodenum.
- Don’t overuse nonsteroidal anti-inflammatory drugs (NSAIDs). Don’t take an NSAID for more than three days for fever or more than 10 days for pain unless your doctor says it’s OK.
- Consider switching pain relievers. If you use pain relievers that increase your risk of gastritis, ask your doctor whether acetaminophen (paracetamol) may be an option for you. This medicine is less likely to stir up your stomach and duodenum problem.
- Don’t consume food or drinks that irritate your gut. This includes gluten if you have celiac disease and foods you’re allergic to.
What foods should I eat or avoid with duodenitis?
You can:
- Steer clear of foods that can irritate your gut, including spicy foods and highly acidic foods like citrus or tomato-based foods.
- Avoid drinks that can irritate your gut, including caffeinated drinks like coffee, tea or soda.
- Stop drinking alcohol or reduce your intake.
Try switching to bland foods until your symptoms improve. It’s a good idea to try the BRAT diet, which stands for bananas, rice, applesauce and toast. Gradually, you can include foods with a bit more nutritional value, like chicken soup and broth. Instead of eating big meals, aim for a few smaller meals spread out throughout the day so you’re not stressing your digestive system.
Regardless of what you eat, try not to eat anything three hours before bedtime. Allow your digestive system plenty of time to wind down so you can sleep easily.
What is duodenum
The duodenum is the first portion of the small intestine. The duodenum is the initial C-shaped segment of the small intestine and is a continuation of the pylorus (part of stomach) 8. Distally, duodenum is in continuation with the jejunum and ileum, with the proximal segment being the shortest and widest. Positioned inferiorly to the stomach, the duodenum is approximately 25 to 30 cm long. Interestingly enough, this portion of the small intestine got its name due to its length. In Latin, the term “duodenum” means 12 fingers, which is roughly the length of the duodenum. The 4 segments of the duodenum include the following:
- The duodenal bulb, which connects to the undersurface of the liver via the hepatoduodenal ligament, which contains the portal vein, the hepatic artery, and common bile duct.
- The second or descending segment is just above the inferior vena cava and right kidney, with the head of the pancreas lying in a C-shaped concavity.
- The third segment runs from right to left in front of the aorta and inferior vena cava, with the superior mesenteric vessels in front of it.
- The fourth segment continues as the jejunum.
The walls of the duodenum are made up of 4 layers of tissue that are identical to the other layers of the gastrointestinal (GI) tract. From innermost to the outermost layer, these are the mucosa, submucosa, muscularis, and serosa layers. The mucosal layer lines the inner surface of the duodenum and is made of simple columnar cells with microvilli and numerous mucous glands. The submucosal layer is mostly a layer of connective tissue where blood vessels and nerves travel through. The muscularis layer contains the smooth muscle of the duodenum and allow mixing and forward peristaltic movement of chyme. The serosal layer is characterized by squamous epithelium that acts as a barrier for the duodenum from other organs within the human body.
The duodenojejunal flexure is the sudden turn which is usually identified during surgery by the location of the inferior mesenteric vein, which is located to the immediate left. The duodenojejunal flexure is attached to the posterior abdominal wall by the ligament of Treitz. Except for the first segment, the rest of the duodenum is retroperitoneal and has no mesentery and is fixed to the posterior abdominal cavity.
The distal end of the common bile duct joins with the pancreatic duct to form the biliopancreatic ampulla which opens on the dome of the major duodenal papilla, located on the second segment of the C-shaped duodenum. This anatomical landmark is important for gastroenterologists as they do endoscopic retrograde cholangiopancreatography (ERCP) procedures to cannulate the major papilla of the duodenum.
Figure 1. Small intestine
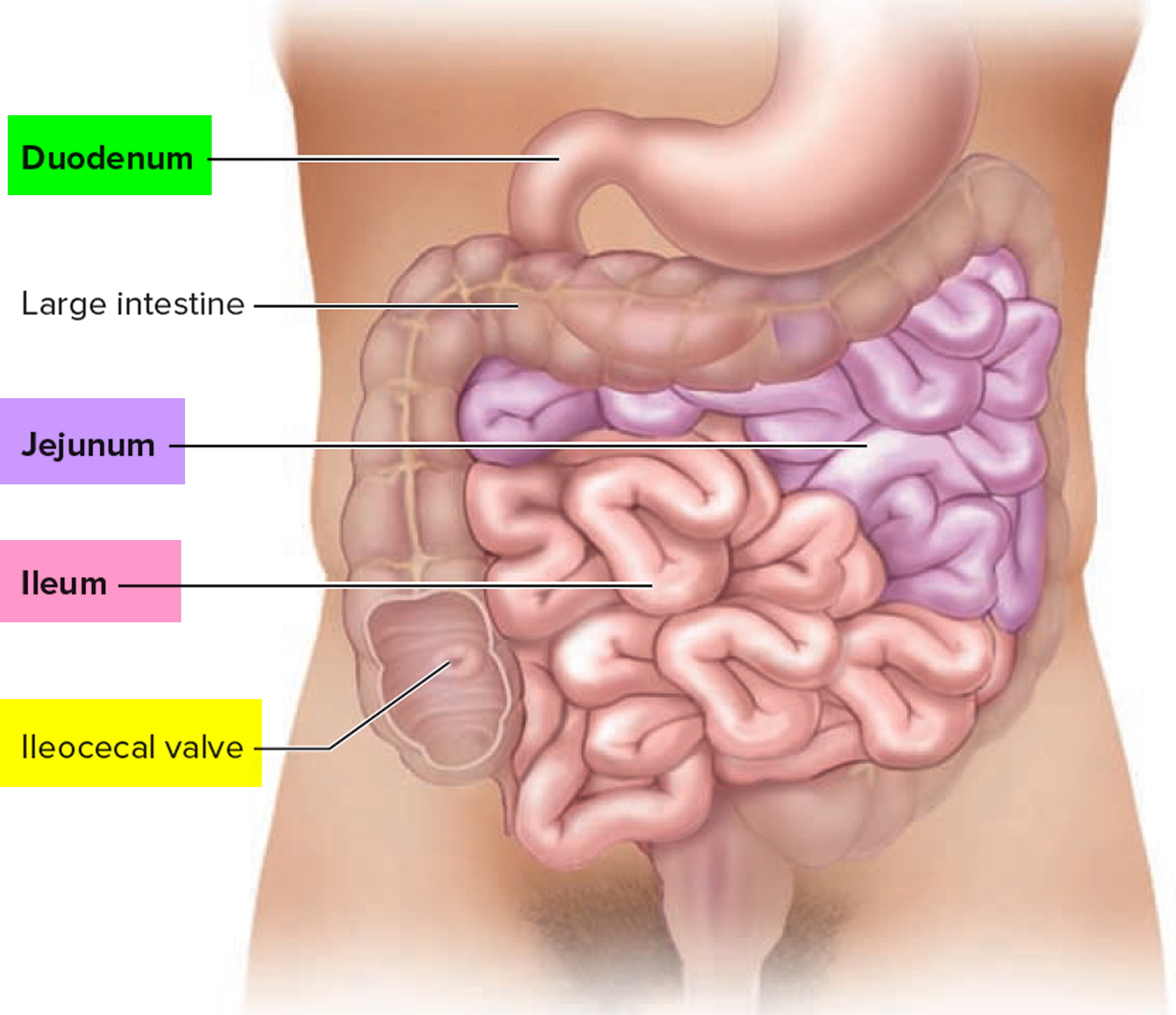
Figure 2. Duodenum location
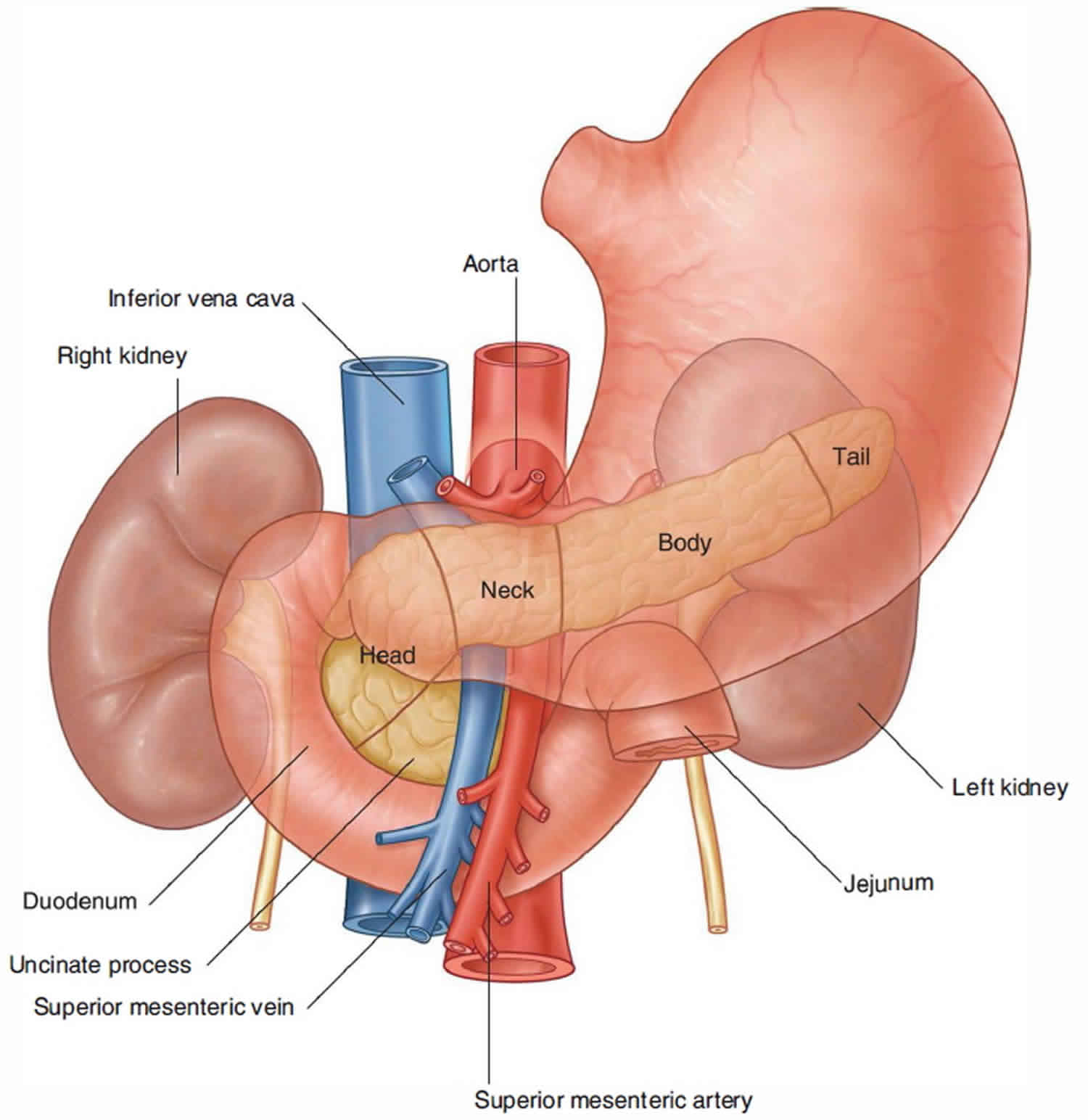
Figure 3. Relationship of the duodenum to the pancreas, liver and gallbladder
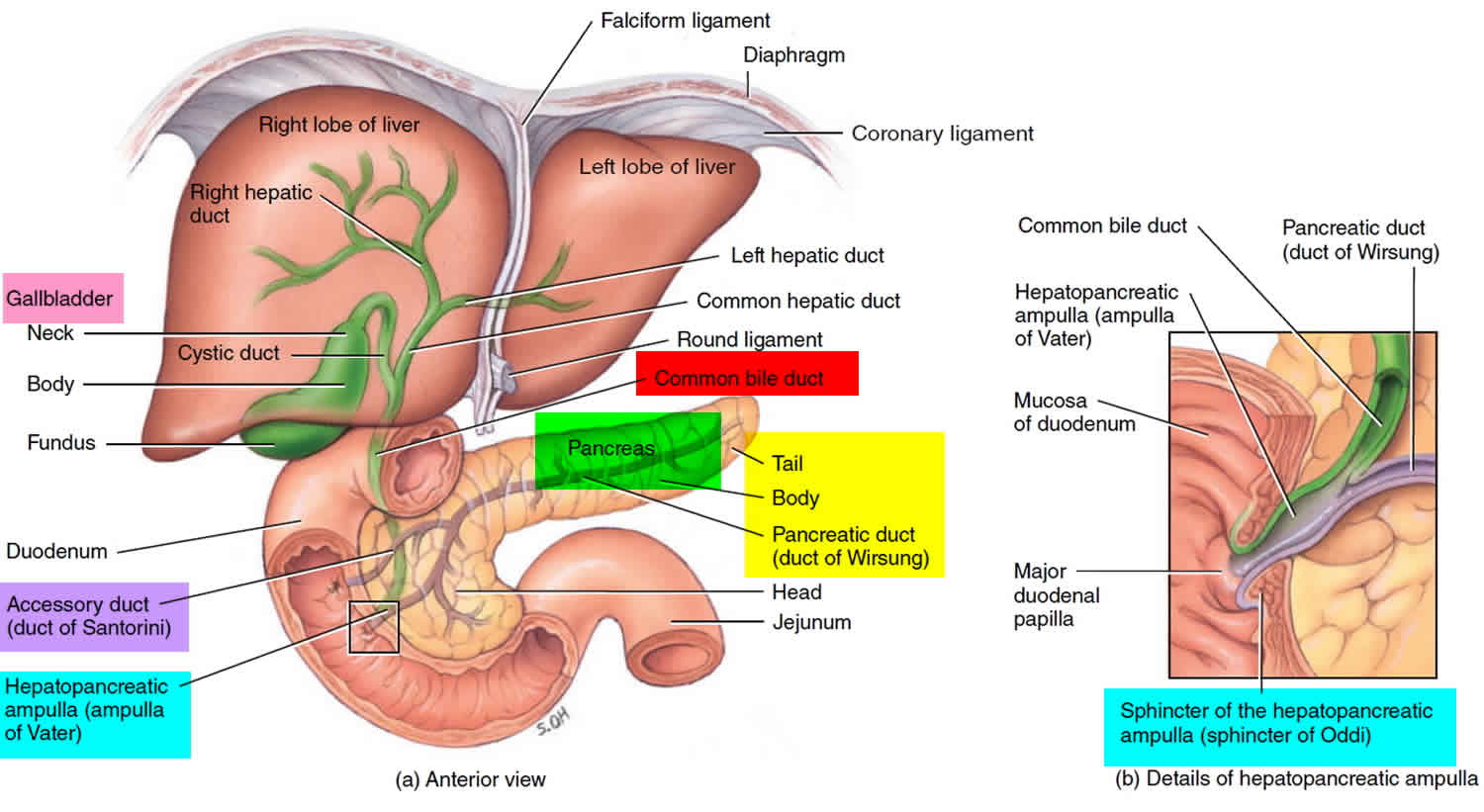
Figure 4. Duodenum anatomy
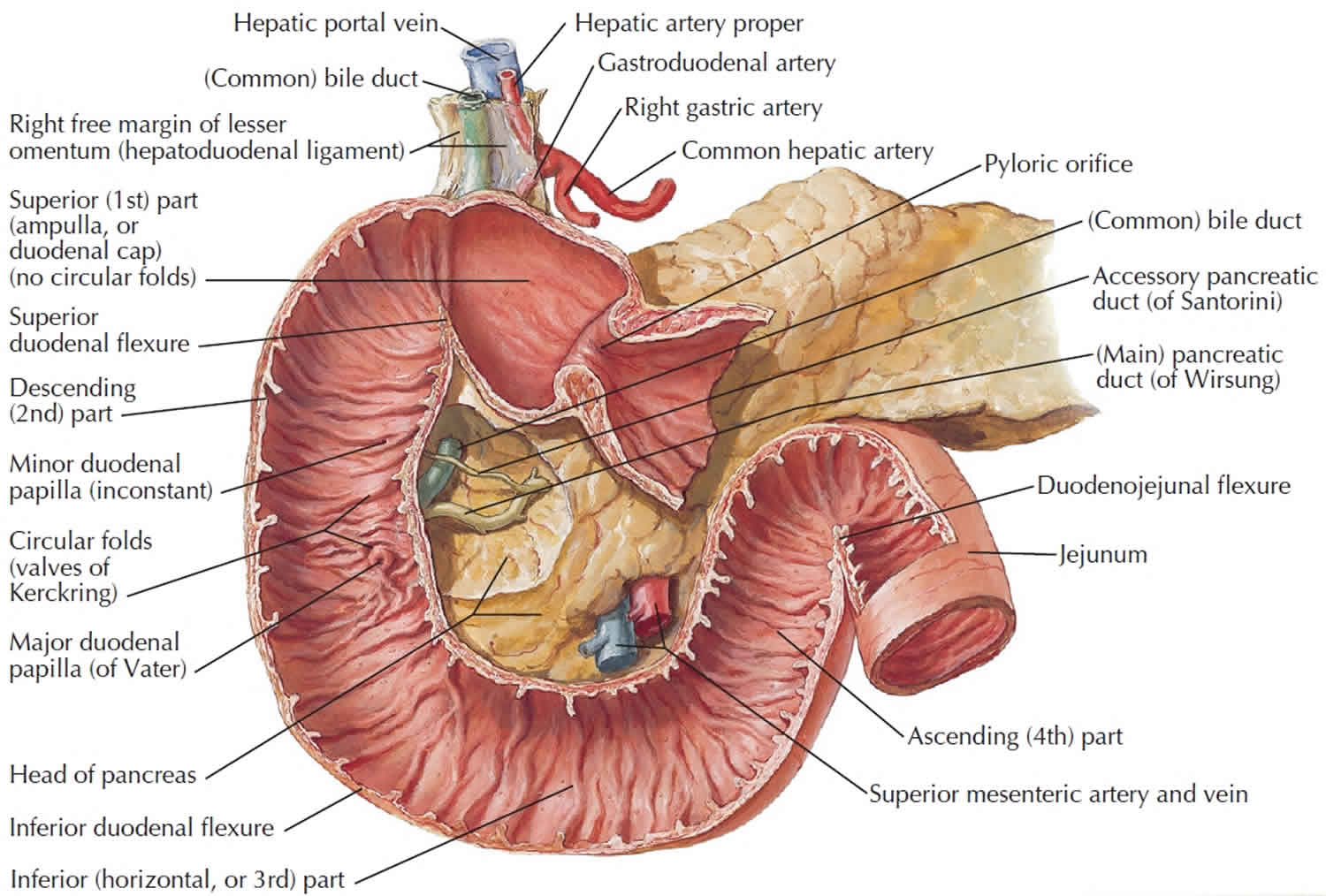
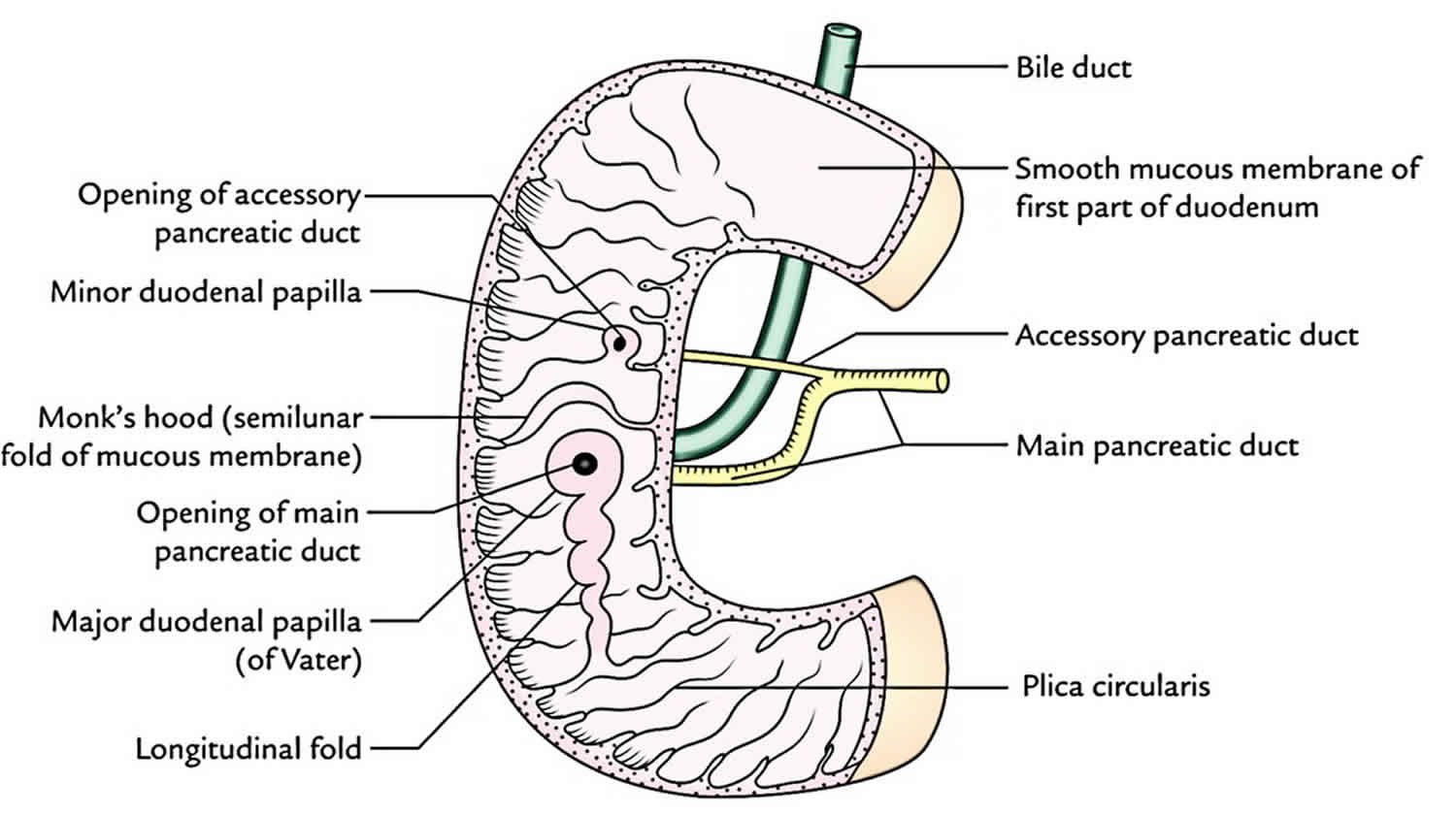
Figure 5. Duodenum anatomy (anatomical layers)
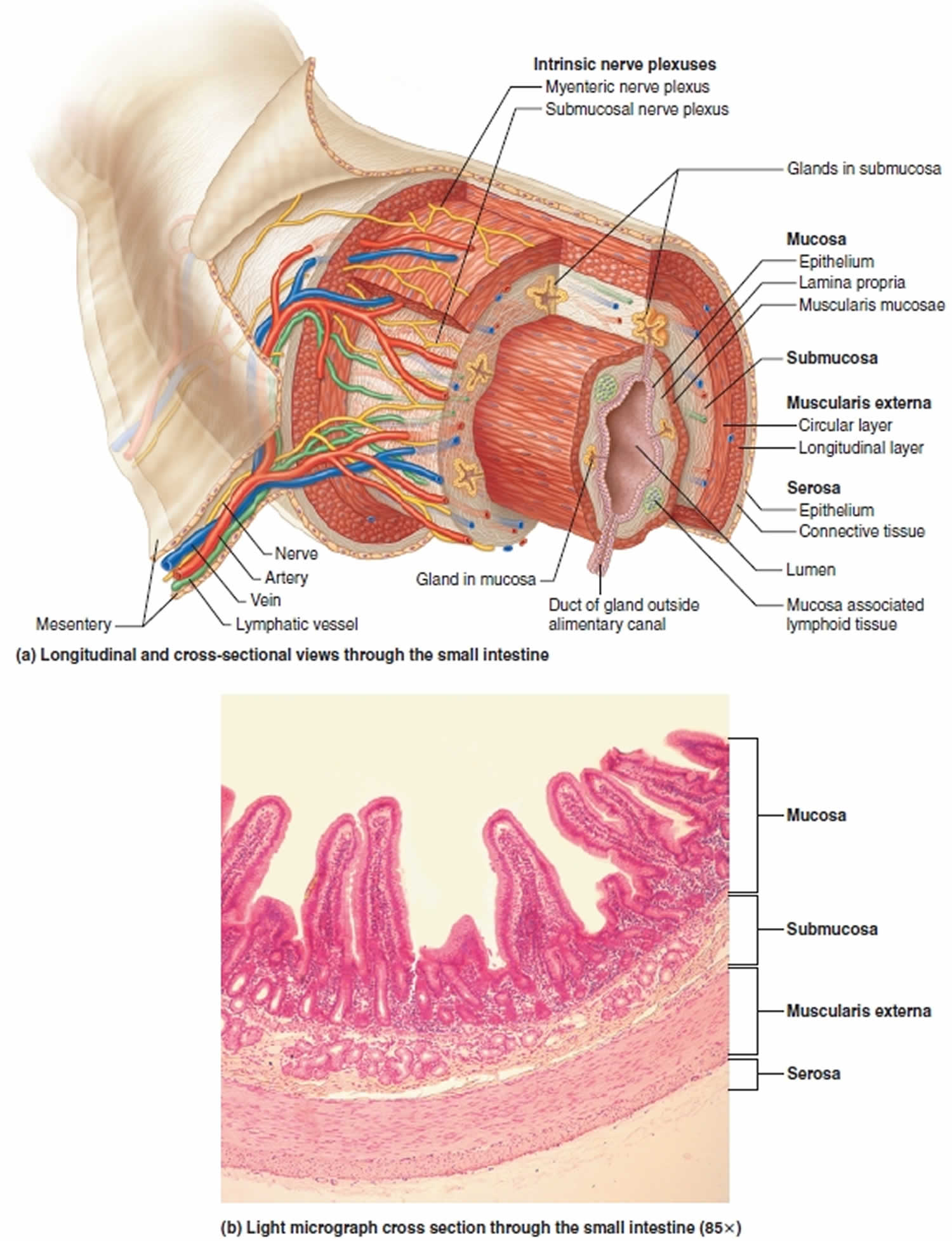 Figure 6. Duodenum blood supply
Figure 6. Duodenum blood supply
What does the duodenum do?
The duodenum is the mixing pot of the small intestine. Duodenum receives chyme from the stomach, which is a mixture of food products and acid, through a controlled valve between the stomach and the duodenum called the pylorus. Pancreatic enzymes enter the duodenum as well, releasing enzymes to break down the products from the stomach, and bicarbonate to neutralize the acid from the stomach before reaching the jejunum. Here the liver introduces bile which allows for the breakdown and absorption of fat from food products. The digestion inside of the duodenum is facilitated by the digestive enzymes and intestinal juices secreted by the intestinal wall as well as fluids received from the gallbladder, liver, and pancreas. This is received into the duodenum by the major and minor papilla in the second part of the duodenum. The duodenal papilla is surrounded by a semicircular fold superiorly and the sphincter of Oddi which is the muscle that prevents reflux of duodenal secretions into the bile and pancreatic ducts.
The duodenum also has the unique ability to regulate its environment with hormones that are released from the duodenal epithelium. One of those hormones is secretin, which is released when the pH of the duodenum decreases to a less than desirable level 8. The secretin hormone acts to neutralize the pH of the duodenum by stimulating water and bicarbonate secretion into the duodenum. In the duodenum there are tubular duodenal glands, whose ducts open into the intestinal crypts. These glands secrete an alkaline,
bicarbonate-rich mucus that helps neutralize the acidity of the chyme from the stomach and contributes to the protective layer of mucus on the inner surface of the small intestine. This also aids in the digestion process as pancreatic amylase and lipase require a certain pH to function optimally. Another hormone that is released by the duodenal epithelium is cholecystokinin (CCK). Cholecystokinin is released in the presence of fatty acids and amino acids inside of the duodenum and acts to inhibit gastric emptying and also to stimulate contraction of the gallbladder while simultaneously causing relaxation of the sphincter of Oddi to allow delivery of bile into the duodenum to aid in digestion and absorption of nutrients.
Duodenitis causes
Duodenitis happens when something threatens your duodenum’s protective lining. By far, the 2 most common causes of inflammation in your duodenum is Helicobacter pylori infection and the use of nonsteroidal anti-inflammatory drugs (NSAIDs) 12, 9, 10. H. pylori is a bacteria that’s present in 50% to 75% of the world’s population. H. pylori is usually in your stomach, but it can travel to your duodenum. For most people, it doesn’t cause problems. But H. pylori bacteria that multiply out of control can cause an infection that eats away at your duodenum lining. H. pylori causes mucosal inflammation, leading to epithelial cell degeneration and injury. Overusing nonsteroidal anti-inflammatory drugs (NSAIDs) like aspirin, ibuprofen and naproxen sodium can eat away at your duodenum or stomach lining, triggering inflammation. Nonsteroidal anti-inflammatory drugs (NSAIDs) cause mucosal injury by blocking the cyclooxygenase-1 (COX-1) pathway, leading to inhibition of prostaglandin synthesis. Prostaglandins are necessary molecules that maintain the mucosal barrier 12.
Other causes of duodenitis include:
- Small intestinal bacterial overgrowth (SIBO) and giardiasis (an infection caused by the giardia parasite) can cause duodenitis.
- Excess stomach acid. Stomach acid can leak into your duodenum and wear away the lining. The damage triggers inflammation.
- Autoimmune diseases. Celiac disease can lead to duodenitis 6. Celiac disease is an autoimmune disease where the body’s immune system mistakenly attacks its own tissues, specifically the lining of the small intestine. Celiac disease is triggered when you eat gluten, a protein found in wheat, rye, and barley. It causes the body’s immune system to attack the small intestine when gluten is consumed, leading to inflammation and damage that prevents proper nutrient absorption. The condition can affect people of all ages and genders, and it can develop at any point in life.
- Crohn’s disease. Crohn’s disease is a type of inflammatory bowel disease (IBD) that causes chronic inflammation in the digestive tract 13, 14. Crohn’s disease can affect any part of your digestive system, but often affects the last part of the small intestine (ileum) and the colon (large intestine). Symptoms include diarrhea, abdominal pain, fatigue, and weight loss.
- Ulcerative colitis. Ulcerative colitis is a type of inflammatory bowel disease (IBD) that causes inflammation and ulceration in the large intestine (colon and rectum) 15, 13, 14. It’s characterized by symptoms like diarrhea, blood or mucus in stool, and abdominal pain.
- Gastroesophageal reflux disease (GERD). Gastroesophageal reflux disease (GERD) is a chronic digestive disorder where stomach contents, including acid, flow back up into the esophagus. This backwash, or reflux, can cause symptoms like heartburn and regurgitation. If not managed, GERD can lead to complications like inflammation and even permanent damage to the esophagus.
- Consuming foods or drinks that irritate your gut. Food allergies, including food sensitivities to milk and soy, can cause inflammation. Certain drinks, like caffeinated beverages (coffee, tea) can also irritate your gut and lead to duodenitis.
- Smoking and drinking too much alcohol. The chemicals from smoking tobacco can irritate your gut. Excessive alcohol can cause problems, too.
- Cancer treatments. Radiation therapy and chemotherapy treatments that kill cancer cells can also cause inflammation in your digestive tract, including your duodenum.
Duodenitis signs and symptoms
Duodenitis doesn’t always cause symptoms. When it does, people experience duodenitis differently. Duodenitis symptoms may come and go. They may be ongoing but mild. Or you may have sudden, severe symptoms that alert you that it’s time to see your doctor.
Duodenitis symptoms may include:
- Upper abdominal pain (a gnawing or burning sensation called indigestion that improves when you eat).
- Bloating (tight, full or painful feeling in your upper abdomen after eating).
- Nausea and vomiting.
- Diarrhea.
- Fatigue.
- Gas.
- Loss of appetite.
Bleeding in your digestive tract is sometimes a sign of severe duodenitis. Signs include:
- Blood in your vomit (may look like coffee grounds).
- Blood in your poop (may look dark-colored or tarry).
You should see a doctor if you notice these signs, which may mean you have duodenitis or another digestive system condition that needs treatment.
Seek medical attention right away if you have severe pain or if you have vomiting where you cannot hold any food down. Also seek medical attention right away if you feel lightheaded or dizzy. Tell your doctor if your stomach discomfort happens after taking medicines, especially aspirin or other pain relievers.
If you are vomiting blood, have blood in your stools or have stools that appear black and a fever higher than 102 degrees Fahrenheit (39 degrees Celsius), see your doctor right away to find the cause.
Duodenitis complications
Left untreated, duodenitis can progress to:
- Peptic duodenitis: Excess stomach acid can lead to long-term and severe inflammation in your duodenum. Risk factors include H. pylori infection, overusing nonsteroidal anti-inflammatory drugs (NSAIDs) and smoking.
- Duodenal ulcers and duodenal bleeding: Eventually, the damage to your duodenal lining can lead to painful, open sores called duodenal ulcers. These are similar to peptic (stomach) ulcers. These sores sometimes bleed. Blood in your poop or vomit may mean you have a duodenal ulcer.
Vomiting and diarrhea associated with duodenitis can also cause dehydration or not having enough fluid. Dehydration is especially dangerous in children and adults age 65 or older.
Inflammation can also prevent your duodenum from doing one of its most important jobs — helping you absorb nutrients like iron from food. Duodenitis can prevent you from absorbing enough iron. Iron is a key ingredient your body needs to make red blood cells. This can lead to iron-deficiency anemia.
Duodenitis diagnosis
Your doctor is likely to suspect duodenitis after talking to you about your medical history and performing an exam. If your doctor suspects duodenitis, he/she will perform tests to figure out what’s causing the inflammation. Tests may include:
- Tests for H. pylori. Your doctor may recommend tests such as a stool test or breath test to determine whether you have H. pylori infection. Which type of test you have depends on your situation. For the breath test, you drink a small glass of clear, tasteless liquid that contains radioactive carbon. H. pylori germs break down the test liquid in your stomach. Later, you blow into a bag, which is then sealed. If you’re infected with H. pylori, your breath sample will contain the radioactive carbon.
- Blood tests: A blood sample can show if you have a germ, like H. pylori, that’s causing an infection. A blood test can also show if you have antibodies for gluten as in celiac disease. Antibodies are proteins your immune system makes to fight germs. Antibody blood tests are usually the first tests that are ordered to diagnose celiac disease. These tests look for proteins created during the body’s immune response, known as antibodies, that are present in most people with celiac disease.
- Stool test: Your poop can show if you have an H. pylori infection.
- Passing a thin, flexible scope down the throat, called an upper endoscopy. Endoscopy is a procedure to examine the digestive system with a long, thin tube with a tiny camera, called an endoscope. The endoscope passes down the throat, into the esophagus, stomach and small intestine. Using the endoscope, your doctor looks for signs of inflammation. The scope contains instruments that can take tissue samples for lab testing. Depending on your age and medical history, your doctor may recommend this as a first test instead of testing for H. pylori.
- Upper GI series: This series of X-rays takes images of your upper digestive system. You may have to swallow a white, metallic liquid that contains barium. The liquid coats your digestive tract and makes an ulcer more visible. This procedure is called a barium swallow. It can show how these organs work together so your doctor can better understand what’s causing inflammation in your duodenum.
If a suspicious area is found, your doctor may remove small tissue samples, called a biopsy, to test in a lab. A biopsy also can identify the presence of H. pylori in your duodenum lining.
Duodenitis treatment
Duodenitis often improves on its own in time. If it doesn’t, treatment depends on the cause. You may need antibiotics to kill H. pylori bacteria or medicines reduce stomach acid damaging your duodenum lining. You may need to make lifestyle changes to protect your gut from becoming irritated and inflamed.
Duodenitis treatments include:
- Antibiotics. These medicines kill H. pylori bacteria.
- Stomach acid reducers. Medicines may include antacids and proton pump inhibitors.
- Lifestyle changes. You may need to stop taking NSAIDs if overuse is causing duodenitis. You may need to steer clear of gluten if you have celiac disease. Changing what you eat, quitting cigarettes and cutting back on alcohol can also help.
If you have severe damage to your duodenum, you may need surgery to repair the tissue. But this is rare.
Helicobacter pylori Infection Treatment
Regimens for eradication of Helicobacter pylori infection are typically chosen empirically, on the basis of regional bacterial resistance patterns, local recommendations, and drug availability 16. Therapy for Helicobacter pylori infection has undergone major changes, based on application of the principles of antimicrobial stewardship and increased availability of susceptibility testing. Common initial choices for empiric treatment include a 14-day bismuth-based quadruple therapy or rifabutin-based triple therapy. However, clinicians should use regimens shown to be highly effective locally 16. In addition, doctors should ask their patients about any prior antibiotic use or exposure, and take that information into consideration in the choice of a treatment regimen 17.
The following regimens are described below 18:
- Triple therapy
- Proton pump inhibitor (PPI) based triple therapy for H. pylori infection remains an option for first-line therapy in areas of low (< 15%) clarithromycin resistance and consists of the following 19, 20, 17, 21, 22, 23, 24:
- Proton pump inhibitor (PPI) (e.g., omeprazole 20 mg BID, lansoprazole 30 mg BID, esomeprazole 40 mg QD, pantoprazole 40 mg QD, rabeprazole 20 mg BID) PLUS
- Clarithromycin 500 mg BID (first-line and continues to be recommended in areas where H. pylori clarithromycin resistance is less than 15% and in patients without previous macrolide exposure) or metronidazole 500 mg BID (when clarithromycin resistance is increasing) PLUS
- Amoxicillin 1000 mg BID or metronidazole 500 mg BID (if not already selected)
- Duration: A Cochrane meta-analysis of 55 studies concluded that 14 days is the optimal duration of triple therapy, achieving an H. pylori eradication rate of 81.9%, whereas 7 days attains an eradication rate of only 72.9% 25. In more recent studies, the H. pylori eradication rate with 14-day triple therapy is not significantly different from that with 10-day sequential therapy (amoxicillin and a PPI for 5 days followed by a PPI, clarithromycin and metronidazole for another 5 days) or 10-day concomitant non-bismuth quadruple therapy 26, 27.
- Proton pump inhibitor (PPI) based triple therapy for H. pylori infection remains an option for first-line therapy in areas of low (< 15%) clarithromycin resistance and consists of the following 19, 20, 17, 21, 22, 23, 24:
- Non-bismuth quadruple therapy
- Non-bismuth quadruple therapy may be given sequentially or concomitantly 18, 17:
- Sequential therapy
- Sequential therapy (a suggested first-line option) is superior to standard triple therapy, according to two systematic reviews and consists of the following 28, 29:
- Proton pump inhibitor (PPI) plus amoxicillin for 5-7 days (eg, pantoprazole 40 mg BID and amoxicillin 1 g BID for 7 days), then PPI plus 2 other antibiotics for the next 5-7 days; clarithromycin and metronidazole are the antibiotics usually chosen, but levofloxacin-based regimens (see below) and tetracycline-based regimens (eg, pantoprazole 40 mg BID, tetracycline 500 mg QID, and metronidazole 500 mg BID) [22] are superior to 14-day triple therapy, based on a meta-analysis of 21 trials 28, 30, 31, 32. Eradication rates with different durations of sequential therapy are as follows:
- Sequential therapy (a suggested first-line option) is superior to standard triple therapy, according to two systematic reviews and consists of the following 28, 29:
- Concomitant therapy
- Concomitant therapy is better for clarithromycin-resistant H. pylori strains and 14 days of concomitant therapy is superior to 14-day triple therapy, with cure rates of ≥90% 35, 36, 37, 38, 39, 40.
- Concomitant therapy (an alternative first-line option) consists of the following (using dosages similar to those in triple therapy; or all drugs BID in one study):
- Novel concomitant therapy consists of the following agents, which are given for 10 days 42:
- PPI (eg, rabeprazole 20 mg TID) plus
- Amoxicillin 1 g TID for 10 days (or, if penicillin allergic, bismuth subcitrate 240 mg QID plus
- Rifabutin 150 mg BID plus
- Ciprofloxacin 500 mg BID
- A small randomized trial in Taiwan reported that 14-day high-dose dual therapy with esomeprazole (40 mg TID) and amoxicillin (750 mg QID) as first-line treatment yielded an eradication rate similar to that of a 7-day non-bismuth quadruple therapy 43.
- Hybrid therapy
- Hybrid therapy is a combination of sequential and concomitant therapy as follows 18, 44, 45:
- Proton pump inhibitor (PPI) plus amoxicillin for 3-7 days (the latter recommended as another suggested first-line option in the 2017 American College of Gastroenterology guideline), then proton pump inhibitor (PPI) plus amoxicillin plus 2 other antibiotics (usually, clarithromycin and metronidazole) for 7 days
- There is evidence that H. pylori eradication rates with 10-day, 12-day, and 14-day regimens are comparable, at 95.0%, 95.1%, and 93.4%, respectively. This suggests that the optimal duration of hybrid therapy is 12 days, since high rates of eradication are still achieved.
- When compared with 14 days of bismuth-containing quadruple therapy, a 14-day hybrid therapy regimen (7 days of dual therapy with pantoprazole plus amoxicillin, followed by 7 days of quadruple therapy with pantoprazole plus amoxicillin, clarithromycin, and metronidazole) showed comparable drug adherence and eradication rates, but with a significantly lower rate of adverse effects (15.7%, versus 55.5% with bismuth-containing quadruple therapy) 46.
- Hybrid therapy is a combination of sequential and concomitant therapy as follows 18, 44, 45:
- Reverse hybrid therapy
- Reverse hybrid therapy is a combination of sequential and concomitant therapy, using the same drugs as hybrid therapy but in reverse sequence, as follows 45:
- Proton pump inhibitor (PPI) plus amoxicillin plus 2 other antibiotics (usually, clarithromycin and metronidazole) for 7 days then
- Proton pump inhibitor (PPI) plus amoxicillin for 3–7 days
- Helicobacter pylori eradication rate achieved with 12 days of reverse hybrid therapy is similar to that with 12 days of hybrid therapy (95.7% vs. 95.1%, respectively). Fourteen-day reverse hybrid therapy as first-line treatment has equivalent efficacy but less adverse effects than 14-day concomitant therapy, according to a randomized, controlled trial from Taiwan 47.
- Reverse hybrid therapy is a combination of sequential and concomitant therapy, using the same drugs as hybrid therapy but in reverse sequence, as follows 45:
- Sequential therapy
- Non-bismuth quadruple therapy may be given sequentially or concomitantly 18, 17:
- Bismuth-based therapy
- Bismuth-based therapy is an alternative first-line therapy (in areas with high clarithromycin and metronidazole resistance, and in patients with prior macrolide exposure or penicillin-allergic) or second-line therapy (see below). Bismuth-based therapy consists of the following 48, 49, 27, 21:
- Proton pump inhibitor (PPI) or H2 receptor antagonist (eg, lansoprazole 30 mg BID or famotidine20 mg BID) plus
- Bismuth subsalicylate 525 mg QID (or bismuth tripotassium dicitrate 300 mg QID) plus
- Metronidazole 250 mg QID or 500 mg TID (or levofloxacin 500 mg QD) plus
- Tetracycline 500 mg QID
- Duration is 10-14 days. The Helicobacter pylori eradication rate was 90.4% for 10 days of bismuth quadruple therapy, while extending therapy to 14 days achieved an eradication rate of 97.1% 50.
- Chinese researchers reported that the following regimen provides effective first-line treatment in a population with high antibiotic resistance 51:
- Rabeprazole 10 mg BID plus
- Bismuth potassium citrate 220 mg BID plus
- Amoxicillin 1000 mg BID plus
- Clarithromycin 500 mg BID
- Duration is 10 days. Rabeprazole and bismuth were given 30 min before the morning and evening meals. Antibiotics were given 30 min after the morning and evening meals 51.
- Researchers in Turkey, however, reported that a 14-day regimen of lansoprazole 30 mg BID, amoxicillin 1000 mg BID, clarithromycin 500 mg BID, bismuth subsalicylate 600 mg BID was not significantly superior to a 7-day regimen (81.4% vs. 80%) 52.
- Bismuth-based therapy is an alternative first-line therapy (in areas with high clarithromycin and metronidazole resistance, and in patients with prior macrolide exposure or penicillin-allergic) or second-line therapy (see below). Bismuth-based therapy consists of the following 48, 49, 27, 21:
- Levofloxacin-containing therapy
- Levofloxacin-containing therapy is an alternative first-line regimen and consists of a proton pump inhibitor (PPI) plus amoxicillin 1 g BID plus levofloxacin 500 mg QD 53, 21, 31.
- Duration options are as follows:
- Sequential therapy, an alternative first-line regimen, is as follows (eradication rates of up to 86.5%):
- Proton pump inhibitor (PPI) (esomeprazole 20 mg or 40 mg BID) plus amoxicillin (1 g BID) for 5-7 days, then
- Proton pump inhibitor (PPI) (esomeprazole 20 mg or 40 mg BID) plus levofloxacin (250 mg or 500 mg BID) plus a nitroimidazole antibiotic (eg, tinidazole 500 mg BID) for 5-7 days
- A randomized trial investigated the role of bismuth in levofloxacin-containing 14-day sequential therapy, and concluded that adding bismuth did not significantly improve eradication rates (85.2% vs. 82.6%).
- Concomitant therapy, another alternative first-line regimen, is as follows (eradication rates of up to 96.5%) 56: proton pump inhibitor (PPI) (esomeprazole 40 mg BID) plus amoxicillin (1 g BID) plus levofloxacin (500 mg QD) plus another antibiotic (eg, tinidazole 500 mg BID) for 5 days.
- Concomitant bismuth- and levofloxacin-containing therapy
- A group of Chinese researchers reported that the following concomitant bismuth- and levofloxacin-containing therapy regimen also provided satisfactory eradication rates in a population with high antibiotic resistance 57:
- Esomeprazole 20 mg BID plus
- Levofloxacin 500 mg BID plus
- Bismuth 220 mg BID plus
- Amoxicillin 1000 mg BID or cefuroxime 500 mg BID
- Duration: 14 days. Eradication rates were not significantly different between the amoxicillin and cefuroxime groups (83.5% vs 81%) 57.
- An open-label, randomized trial conducted in China reported acceptable eradication rates even for the following 1-week bismuth-containing regimen 58:
- Esomeprazole 20 mg BID plus
- Colloidal bismuth pectin 200 mg BID plus
- Amoxicillin 1000 mg BID plus
- Levofloxacin 500 mg OD or clarithromycin 500 mg BID
- The above levofloxacin-based concomitant quadruple regimen demonstrated a higher eradication rate (86.66% vs 76.22%) 58.
- A group of Chinese researchers reported that the following concomitant bismuth- and levofloxacin-containing therapy regimen also provided satisfactory eradication rates in a population with high antibiotic resistance 57:
- Second-line therapy
- Second-line therapy should avoid repeating first-line regimens that were already used, and should incorporate at least one different antibiotic 59, 18. Bismuth-based therapy or levofloxacin-containing triple therapy can be used (same regimens as above, if not used previously) 59.
- In a meta-analysis of 115 heterogeneous studies, per protocol analysis showed that quadruple therapies have better cure rate than triple (83% vs 76%) and 14-day quadruple treatment than 7-day regimens (91% vs 81%) 60.
- Rescue or third-line therapy
- Rifabutin-based therapy is recommended as rescue or salvage therapies when first-line agents fail 20, 17. A rifabutin-based triple-therapy regimen consists of the following three agents given together every 8 hours for 14 days 61:
- Amoxicillin 1 g plus
- Omeprazole 40 mg plus
- Rifabutin 50 mg
- Rifabutin-based therapy regimen is available prepackaged as Talicia. The US Food and Drug Administration (FDA) approved Talicia for treatment of H. pylori infection in 2019, based in part on results of two phase 3 studies that showed eradication rates of 84.1% and 90.3% 61, 62.
- Vonoprazan-based therapy is yet to be included in the H. pylori treatment guidelines. Vonoprazan triple therapy has been proposed as an alternative first-line regimen for clarithromycin-sensitive strains, given its similar or greater effectiveness as proton pump inhibitors (PPIs) 63, 64. The first potassium-competitive acid blocker (PCAB)–based therapy was approved by the FDA in May 2022 and consists of triple therapy for 14 days with the following 65:
- Vonoprazan (PCAB) 20 mg BID plus
- Amoxicillin 1000 mg BID plus
- Clarithromycin 500 mg BID
- Vonoprazan-based therapy regimen has been packaged in the Voquezna Triple Pak. Vonaoprazan plus amoxicillin was also approved by the FDA and has been packaged in the Voquezna Dual Pak. However, neither product has been released on the market, due to the detection of trace levels of a nitrosamine impurity 66.
- Rifabutin-based therapy is recommended as rescue or salvage therapies when first-line agents fail 20, 17. A rifabutin-based triple-therapy regimen consists of the following three agents given together every 8 hours for 14 days 61:
How long does it take to cure duodenitis?
It depends on what’s causing your duodenum inflammation and how severe it is. If you have an H. pylori infection, you may need to take antibiotics for two weeks to clear things up (see treatment above). You should take all medications as prescribed, even if your symptoms improve.
Duodenitis prognosis
For most people, duodenitis is short-term and isn’t serious and improves quickly with treatment. The inflammation of your duodenum goes away on its own. If you take your medicines, there is a good chance that the H. pylori infection will be cured. Sometimes, H. pylori can be hard to fully cure. Repeated courses of different treatments may be needed. A duodenal biopsy (a procedure where a small tissue sample is taken from the duodenum) will sometimes be done to test the germ to see which antibiotic might work best. This can help guide future treatment. In some cases, H. pylori can’t be cured with any therapy, though the symptoms may be reduced. If cured, reinfection may occur in areas where sanitary conditions are poor.
Chronic duodenitis requires medical treatment, which may involve taking one or more medicines 11. Treating duodenitis usually eases the inflammation and prevents complications, like damage to your duodenum’s lining.
- Dellon ES, Bortey E, Chang AT, Paterson CA, Turner K, Genta RM. Determination of Optimal Eosinophil Thresholds for Diagnosis of Eosinophilic Gastritis and Duodenitis: A Pooled Analysis of 4 Prospective Studies. Clin Transl Gastroenterol. 2024 Jan 1;15(1):e00656. doi: 10.14309/ctg.0000000000000656[↩]
- Lewis S, Stableforth W, Awasthi R, Awasthi A, Pitts N, Ottaway J, Sherwood A, Robertson N, Cochrane S, Wilkinson S. An examination of the relationship between the endoscopic appearance of duodenitis and the histological findings in patients with epigastric pain. Int J Clin Exp Pathol. 2012;5(6):581-7. Epub 2012 Jul 29. https://pmc.ncbi.nlm.nih.gov/articles/PMC3430111[↩]
- Stanley AJ, Laine L. Management of acute upper gastrointestinal bleeding. BMJ. 2019 Mar 25;364:l536. doi: 10.1136/bmj.l536[↩]
- Cooper AS. Interventions for Preventing Upper Gastrointestinal Bleeding in People Admitted to Intensive Care Units. Crit Care Nurse. 2019 Apr;39(2):102-103. doi: 10.4037/ccn2019916[↩]
- Thomson WO, Joffe SN, Robertson AG, Lee FD, Imrie CW, Blumgart LH. Is duodenitis a dyspeptic myth? Lancet. 1977 Jun 4;1(8023):1197-8. doi: 10.1016/s0140-6736(77)92729-5[↩]
- Alper A, Hardee S, Rojas-Velasquez D, Escalera S, Morotti RA, Pashankar DS. Prevalence and Clinical, Endoscopic, and Pathological Features of Duodenitis in Children. J Pediatr Gastroenterol Nutr. 2016 Feb;62(2):314-6. doi: 10.1097/MPG.0000000000000942[↩][↩]
- Serra S, Jani PA. An approach to duodenal biopsies. J Clin Pathol. 2006 Nov;59(11):1133-50. doi: 10.1136/jcp.2005.031260[↩]
- Lopez PP, Bhimji SS. Anatomy, Abdomen and Pelvis, Duodenum. [Updated 2018 Sep 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482390[↩][↩][↩]
- Caselli M, Gaudio M, Chiamenti CM, Trevisani L, Sartori S, Saragoni L, Boldrini P, Dentale A, Ruina M, Alvisi V. Histologic findings and Helicobacter pylori in duodenal biopsies. J Clin Gastroenterol. 1998;26:74–80. doi: 10.1097/00004836-199801000-00020[↩][↩]
- Mirbagheri SA, Khajavirad N, Rakhshani N, Ostovaneh MR, Hoseini SM, Hoseini V. Impact of Helicobacter pylori infection and microscopic duodenal histopathological changes on clinical symptoms of patients with functional dyspepsia. Dig Dis Sci. 2012;57:967–972. doi: 10.1007/s10620-011-1960-z[↩][↩]
- Beck IT, Kahn DS, Lacerte M, Solymar J, Callegarini U, Geokas MC. ‘Chronic duodenitis’: a clinical pathological entity? Gut. 1965 Aug;6(4):376-83. https://pmc.ncbi.nlm.nih.gov/articles/instance/1552305/pdf/gut00724-0078.pdf[↩][↩]
- Narayanan M, Reddy KM, Marsicano E. Peptic Ulcer Disease and Helicobacter pylori infection. Mo Med. 2018 May-Jun;115(3):219-224. https://pmc.ncbi.nlm.nih.gov/articles/PMC6140150[↩][↩]
- Tobin JM, Sinha B, Ramani P, et al. Upper gastrointestinal mucosal disease in Pediatric Crohn disease and ulcerative colitis: A blinded study. J Pediatr Gastroenterol Nutr. 2001;32:443–8. doi: 10.1097/00005176-200104000-00010[↩][↩]
- Hummel TZ, ten Kate FJW, Reitsma JB, et al. Additional value of upper GI tract endoscopy in the diagnostic assessment of childhood IBD. J Pediatr Gastroenterol Nutr. 2012;54:753–7. doi: 10.1097/MPG.0b013e318243e3e3[↩][↩]
- Sonoda A, Yoshimura N, Sako M, Okano S, Saito S, Takazoe M, Furukawa S, Okamoto K, Yamana T, Tachimori H, Fukata M. Severe Disease Activity May Predispose Patients to Post-colectomy Duodenitis Associated with Ulcerative Colitis. Intern Med. 2024 May 15;63(10):1337-1343. doi: 10.2169/internalmedicine.2134-23[↩]
- Shiotani A, Roy P, Lu H, Graham DY. Helicobacter pylori diagnosis and therapy in the era of antimicrobial stewardship. Therap Adv Gastroenterol. 2021 Dec 21;14:17562848211064080. doi: 10.1177/17562848211064080[↩][↩]
- Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am J Gastroenterol. 2017 Feb;112(2):212-239. doi: 10.1038/ajg.2016.563. Epub 2017 Jan 10. Erratum in: Am J Gastroenterol. 2018 Jul;113(7):1102. doi: 10.1038/s41395-018-0132-6[↩][↩][↩][↩][↩][↩][↩]
- O’Connor A, Molina-Infante J, Gisbert JP, O’Morain C. Treatment of Helicobacter pylori infection 2013. Helicobacter. 2013 Sep;18 Suppl 1:58-65. doi: 10.1111/hel.12075[↩][↩][↩][↩]
- Parikh NS, Ahlawat R. Helicobacter Pylori. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534233[↩]
- Malfertheiner P, Megraud F, O’Morain CA, et al. European Helicobacter and Microbiota Study Group and Consensus panel. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut. 2017 Jan;66(1):6-30. doi: 10.1136/gutjnl-2016-312288[↩][↩]
- Chey WD, Wong BC; Practice Parameters Committee of the American College of Gastroenterology. American College of Gastroenterology guideline on the management of Helicobacter pylori infection. Am J Gastroenterol. 2007 Aug;102(8):1808-25. doi: 10.1111/j.1572-0241.2007.01393.x[↩][↩][↩][↩]
- Sánchez-Delgado J, García-Iglesias P, Castro-Fernández M, Bory F, Barenys M, Bujanda L, Lisozain J, Calvo MM, Torra S, Gisbert JP, Calvet X. High-dose, ten-day esomeprazole, amoxicillin and metronidazole triple therapy achieves high Helicobacter pylori eradication rates. Aliment Pharmacol Ther. 2012 Jul;36(2):190-6. doi: 10.1111/j.1365-2036.2012.05137.x[↩]
- Nishizawa T, Maekawa T, Watanabe N, Harada N, Hosoda Y, Yoshinaga M, Yoshio T, Ohta H, Inoue S, Toyokawa T, Yamashita H, Saito H, Kuwai T, Katayama S, Masuda E, Miyabayashi H, Kimura T, Nishizawa Y, Takahashi M, Suzuki H. Clarithromycin Versus Metronidazole as First-line Helicobacter pylori Eradication: A Multicenter, Prospective, Randomized Controlled Study in Japan. J Clin Gastroenterol. 2015 Jul;49(6):468-71. doi: 10.1097/MCG.0000000000000165[↩]
- Malfertheiner P, Mégraud F, O’Morain C, Bell D, Bianchi Porro G, Deltenre M, Forman D, Gasbarrini G, Jaup B, Misiewicz JJ, Pajares J, Quina M, Rauws E. Current European concepts in the management of Helicobacter pylori infection–the Maastricht Consensus Report. The European Helicobacter Pylori Study Group (EHPSG). Eur J Gastroenterol Hepatol. 1997 Jan;9(1):1-2. doi: 10.1097/00042737-199701000-00002[↩]
- Yuan Y, Ford AC, Khan KJ, Gisbert JP, Forman D, Leontiadis GI, Tse F, Calvet X, Fallone C, Fischbach L, Oderda G, Bazzoli F, Moayyedi P. Optimum duration of regimens for Helicobacter pylori eradication. Cochrane Database Syst Rev. 2013 Dec 11;2013(12):CD008337. doi: 10.1002/14651858.CD008337.pub2[↩]
- Nyssen OP, McNicholl AG, Megraud F, Savarino V, Oderda G, Fallone CA, Fischbach L, Bazzoli F, Gisbert JP. Sequential versus standard triple first-line therapy for Helicobacter pylori eradication. Cochrane Database Syst Rev. 2016 Jun 28;2016(6):CD009034. doi: 10.1002/14651858.CD009034.pub2[↩]
- Liou JM, Fang YJ, Chen CC, Bair MJ, et al. Taiwan Gastrointestinal Disease and Helicobacter Consortium. Concomitant, bismuth quadruple, and 14-day triple therapy in the first-line treatment of Helicobacter pylori: a multicentre, open-label, randomised trial. Lancet. 2016 Nov 12;388(10058):2355-2365. doi: 10.1016/S0140-6736(16)31409-X[↩][↩]
- Zullo A, De Francesco V, Hassan C, Ridola L, Repici A, Bruzzese V, Vaira D. Modified sequential therapy regimens for Helicobacter pylori eradication: a systematic review. Dig Liver Dis. 2013 Jan;45(1):18-22. doi: 10.1016/j.dld.2012.08.025[↩][↩]
- Zullo A, Hassan C, Ridola L, De Francesco V, Vaira D. Standard triple and sequential therapies for Helicobacter pylori eradication: an update. Eur J Intern Med. 2013 Jan;24(1):16-9. doi: 10.1016/j.ejim.2012.07.006[↩]
- Uygun A, Kadayifci A, Yesilova Z, Safali M, Ilgan S, Karaeren N. Comparison of sequential and standard triple-drug regimen for Helicobacter pylori eradication: a 14-day, open-label, randomized, prospective, parallel-arm study in adult patients with nonulcer dyspepsia. Clin Ther. 2008 Mar;30(3):528-34. doi: 10.1016/j.clinthera.2008.03.009[↩]
- Qian J, Ye F, Zhang J, Yang YM, Tu HM, Jiang Q, Shang L, Pan XL, Shi RH, Zhang GX. Levofloxacin-containing triple and sequential therapy or standard sequential therapy as the first line treatment for Helicobacter pylori eradication in China. Helicobacter. 2012 Dec;17(6):478-85. doi: 10.1111/j.1523-5378.2012.00993.x[↩][↩][↩]
- Liou JM, Chen CC, Chang CY, Chen MJ, Fang YJ, Lee JY, Chen CC, Hsu SJ, Hsu YC, Tseng CH, Tseng PH, Chang L, Chang WH, Wang HP, Shun CT, Wu JY, Lee YC, Lin JT, Wu MS; Taiwan Helicobacter Consortium. Efficacy of genotypic resistance-guided sequential therapy in the third-line treatment of refractory Helicobacter pylori infection: a multicentre clinical trial. J Antimicrob Chemother. 2013 Feb;68(2):450-6. doi: 10.1093/jac/dks407[↩]
- Liou JM, Chen CC, Chen MJ, Chen CC, Chang CY, Fang YJ, Lee JY, Hsu SJ, Luo JC, Chang WH, Hsu YC, Tseng CH, Tseng PH, Wang HP, Yang UC, Shun CT, Lin JT, Lee YC, Wu MS; Taiwan Helicobacter Consortium. Sequential versus triple therapy for the first-line treatment of Helicobacter pylori: a multicentre, open-label, randomised trial. Lancet. 2013 Jan 19;381(9862):205-13. doi: 10.1016/S0140-6736(12)61579-7. Erratum in: Lancet. 2013 Apr 13;381(9874):1276.[↩][↩]
- Manfredi M, Bizzarri B, de’Angelis GL. Helicobacter pylori infection: sequential therapy followed by levofloxacin-containing triple therapy provides a good cumulative eradication rate. Helicobacter. 2012 Aug;17(4):246-53. doi: 10.1111/j.1523-5378.2012.00945.x[↩]
- Malfertheiner P, Megraud F, O’Morain CA, Gisbert JP, Kuipers EJ, Axon AT, Bazzoli F, Gasbarrini A, Atherton J, Graham DY, Hunt R, Moayyedi P, Rokkas T, Rugge M, Selgrad M, Suerbaum S, Sugano K, El-Omar EM; European Helicobacter and Microbiota Study Group and Consensus panel. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut. 2017 Jan;66(1):6-30. doi: 10.1136/gutjnl-2016-312288[↩]
- Molina-Infante J, Pazos-Pacheco C, Vinagre-Rodriguez G, Perez-Gallardo B, Dueñas-Sadornil C, Hernandez-Alonso M, Gonzalez-Garcia G, Mateos-Rodriguez JM, Fernandez-Bermejo M, Gisbert JP. Nonbismuth quadruple (concomitant) therapy: empirical and tailored efficacy versus standard triple therapy for clarithromycin-susceptible Helicobacter pylori and versus sequential therapy for clarithromycin-resistant strains. Helicobacter. 2012 Aug;17(4):269-76. doi: 10.1111/j.1523-5378.2012.00947.x[↩][↩]
- Georgopoulos S, Papastergiou V, Xirouchakis E, Laoudi F, Lisgos P, Spiliadi C, Papantoniou N, Karatapanis S. Nonbismuth quadruple “concomitant” therapy versus standard triple therapy, both of the duration of 10 days, for first-line H. pylori eradication: a randomized trial. J Clin Gastroenterol. 2013 Mar;47(3):228-32. doi: 10.1097/MCG.0b013e31826015b0[↩]
- Kim SY, Lee SW, Hyun JJ, Jung SW, Koo JS, Yim HJ, Park JJ, Chun HJ, Choi JH. Comparative study of Helicobacter pylori eradication rates with 5-day quadruple “concomitant” therapy and 7-day standard triple therapy. J Clin Gastroenterol. 2013 Jan;47(1):21-4. doi: 10.1097/MCG.0b013e3182548ad4[↩]
- Yanai A, Sakamoto K, Akanuma M, Ogura K, Maeda S. Non-bismuth quadruple therapy for first-line Helicobacter pylori eradication: A randomized study in Japan. World J Gastrointest Pharmacol Ther. 2012 Feb 6;3(1):1-6. doi: 10.4292/wjgpt.v3.i1.1[↩]
- Molina-Infante J, Lucendo AJ, Angueira T, Rodriguez-Tellez M, Perez-Aisa A, Balboa A, Barrio J, Martin-Noguerol E, Gomez-Rodriguez BJ, Botargues-Bote JM, Gomez-Camarero J, Huerta A, Modolell I, Ariño I, Herranz-Bachiller MT, Bermejo F, McNicholl AG, O’Morain C, Gisbert JP; European Registry on H. pylori management (Hp‐EuReg). Optimised empiric triple and concomitant therapy for Helicobacter pylori eradication in clinical practice: the OPTRICON study. Aliment Pharmacol Ther. 2015 Mar;41(6):581-9. doi: 10.1111/apt.13069[↩]
- Kongchayanun C, Vilaichone RK, Pornthisarn B, Amornsawadwattana S, Mahachai V. Pilot studies to identify the optimum duration of concomitant Helicobacter pylori eradication therapy in Thailand. Helicobacter. 2012 Aug;17(4):282-5. doi: 10.1111/j.1523-5378.2012.00953.x[↩]
- Tay CY, Windsor HM, Thirriot F, Lu W, Conway C, Perkins TT, Marshall BJ. Helicobacter pylori eradication in Western Australia using novel quadruple therapy combinations. Aliment Pharmacol Ther. 2012 Dec;36(11-12):1076-83. doi: 10.1111/apt.12089[↩]
- Tai WC, Liang CM, Kuo CM, Huang PY, Wu CK, Yang SC, Kuo YH, Lin MT, Lee CH, Hsu CN, Wu KL, Hu TH, Chuah SK. A 14 day esomeprazole- and amoxicillin-containing high-dose dual therapy regimen achieves a high eradication rate as first-line anti-Helicobacter pylori treatment in Taiwan: a prospective randomized trial. J Antimicrob Chemother. 2019 Jun 1;74(6):1718-1724. doi: 10.1093/jac/dkz046[↩]
- Sardarian H, Fakheri H, Hosseini V, Taghvaei T, Maleki I, Mokhtare M. Comparison of hybrid and sequential therapies for Helicobacter pylori eradication in Iran: a prospective randomized trial. Helicobacter. 2013 Apr;18(2):129-34. doi: 10.1111/hel.12017[↩]
- Hsu PI, Kao SS, Wu DC, Chen WC, Peng NJ, Yu HC, Wang HM, Lai KH, Cheng JS, Chen A, Chuah SK, Tsay FW; Taiwan Acid-Related Disease (TARD) Study Group. A Randomized Controlled Study Comparing Reverse Hybrid Therapy and Standard Triple Therapy for Helicobacter pylori Infection. Medicine (Baltimore). 2015 Dec;94(48):e2104. doi: 10.1097/MD.0000000000002104[↩][↩]
- Tsay FW, Wu DC, Yu HC, Kao SS, Lin KH, Cheng JS, Wang HM, Chen WC, Sun WC, Tsai KW, Hsu PI. A Randomized Controlled Trial Shows that both 14-Day Hybrid and Bismuth Quadruple Therapies Cure Most Patients with Helicobacter pylori Infection in Populations with Moderate Antibiotic Resistance. Antimicrob Agents Chemother. 2017 Oct 24;61(11):e00140-17. doi: 10.1128/AAC.00140-17[↩]
- Hsu PI, Tsay FW, Kao JY, Peng NJ, Tsai KW, Tsai TJ, Kuo CH, Kao SS, Wang HM, Chen YH, Shie CB, Wu DC; Taiwan Acid-related Disease & Microbiota (TARD-M) Consortium. Equivalent efficacies of reverse hybrid and concomitant therapies in first-line treatment of Helicobacter pylori infection. J Gastroenterol Hepatol. 2020 Oct;35(10):1731-1737. doi: 10.1111/jgh.15034[↩]
- Liu WZ, Xiao SD, Hu PJ, Lu H, Cui Y, Tytgat GN. A new quadruple therapy for Helicobacter pylori using tripotassium dicitrato bismuthate, furazolidone, josamycin and famotidine. Aliment Pharmacol Ther. 2000 Nov;14(11):1519-22. doi: 10.1046/j.1365-2036.2000.00845.x[↩]
- Kuo CH, Hsu PI, Kuo FC, Wang SS, Hu HM, Liu CJ, Chuah SK, Chen YH, Hsieh MC, Wu DC, Tseng HH. Comparison of 10 day bismuth quadruple therapy with high-dose metronidazole or levofloxacin for second-line Helicobacter pylori therapy: a randomized controlled trial. J Antimicrob Chemother. 2013 Jan;68(1):222-8. doi: 10.1093/jac/dks361[↩]
- Salazar CO, Cardenas VM, Reddy RK, Dominguez DC, Snyder LK, Graham DY. Greater than 95% success with 14-day bismuth quadruple anti- Helicobacter pylori therapy: a pilot study in US Hispanics. Helicobacter. 2012 Oct;17(5):382-90. doi: 10.1111/j.1523-5378.2012.00962.x[↩]
- Xie Y, Zhu Z, Wang J, Zhang L, Zhang Z, Lu H, Zeng Z, Chen S, Liu D, Lv N; the Chinese Study Group on Helicobacter pylori, Chinese Society of Gastroenterology. Ten-Day Quadruple Therapy Comprising Low-Dose Rabeprazole, Bismuth, Amoxicillin, and Tetracycline Is an Effective and Safe First-Line Treatment for Helicobacter pylori Infection in a Population with High Antibiotic Resistance: a Prospective, Multicenter, Randomized, Parallel-Controlled Clinical Trial in China. Antimicrob Agents Chemother. 2018 Aug 27;62(9):e00432-18. doi: 10.1128/AAC.00432-18[↩][↩]
- Yagbasan A, Coşkun DÖ, Özbakir Ö, Deniz K, Gürsoy Ş, Yücesoy M. A Prospective, randomized study comparing 7-day and 14-day quadruple therapies as first-line treatments for helicobacter pylori infection in patients with functional dyspepsia. Niger J Clin Pract. 2018 Jan;21(1):54-58. doi: 10.4103/1119-3077.224784[↩]
- Shah A, Javid G, Zargar SA, Teli F, Khan BA, Yattoo GN, Gulzar GM, Sodhi JS, Khan MA, Shoukat A, Saif R. Safety and efficacy of 1-week levofloxacin-based triple therapy in first-line treatment for Helicobacter pylori-related peptic ulcer disease in Kashmir, India. Indian J Gastroenterol. 2013 Jan;32(1):32-6. doi: 10.1007/s12664-012-0285-y[↩][↩]
- Peedikayil MC, Alsohaibani FI, Alkhenizan AH. Levofloxacin-based first-line therapy versus standard first-line therapy for Helicobacter pylori eradication: meta-analysis of randomized controlled trials. PLoS One. 2014 Jan 21;9(1):e85620. doi: 10.1371/journal.pone.0085620[↩]
- Cuadrado-Lavín A, Salcines-Caviedes JR, Carrascosa MF, Dierssen-Sotos T, Cobo M, Campos MR, Ayestarán B, Fernández-Pousa A, González-Colominas E, Aresti-Zárate S, Hernández M, Pascual EL. Levofloxacin versus clarithromycin in a 10 day triple therapy regimen for first-line Helicobacter pylori eradication: a single-blind randomized clinical trial. J Antimicrob Chemother. 2012 Sep;67(9):2254-9. doi: 10.1093/jac/dks209[↩]
- Federico A, Nardone G, Gravina AG, Iovene MR, Miranda A, Compare D, Pilloni PA, Rocco A, Ricciardiello L, Marmo R, Loguercio C, Romano M. Efficacy of 5-day levofloxacin-containing concomitant therapy in eradication of Helicobacter pylori infection. Gastroenterology. 2012 Jul;143(1):55-61.e1; quize e13-4. doi: 10.1053/j.gastro.2012.03.043[↩]
- Fu W, Song Z, Zhou L, Xue Y, Ding Y, Suo B, Tian X, Wang L. Randomized Clinical Trial: Esomeprazole, Bismuth, Levofloxacin, and Amoxicillin or Cefuroxime as First-Line Eradication Regimens for Helicobacter pylori Infection. Dig Dis Sci. 2017 Jun;62(6):1580-1589. doi: 10.1007/s10620-017-4564-4[↩][↩]
- Su J, Zhou X, Chen H, Hao B, Zhang W, Zhang G. Efficacy of 1st-line bismuth-containing quadruple therapies with levofloxacin or clarithromycin for the eradication of Helicobacter pylori infection: A 1-week, open-label, randomized trial. Medicine (Baltimore). 2017 Feb;96(7):e5859. doi: 10.1097/MD.0000000000005859[↩][↩]
- Malfertheiner P, Megraud F, O’Morain CA, Atherton J, Axon AT, Bazzoli F, Gensini GF, Gisbert JP, Graham DY, Rokkas T, El-Omar EM, Kuipers EJ; European Helicobacter Study Group. Management of Helicobacter pylori infection–the Maastricht IV/ Florence Consensus Report. Gut. 2012 May;61(5):646-64. doi: 10.1136/gutjnl-2012-302084[↩][↩]
- Muñoz N, Sánchez-Delgado J, Baylina M, Puig I, López-Góngora S, Suarez D, Calvet X. Systematic review, meta-analysis, and meta-regression: Successful second-line treatment for Helicobacter pylori. Helicobacter. 2018 Jun;23(3):e12488. doi: 10.1111/hel.12488[↩]
- Graham DY, Canaan Y, Maher J, Wiener G, Hulten KG, Kalfus IN. Rifabutin-Based Triple Therapy (RHB-105) for Helicobacter pylori Eradication: A Double-Blind, Randomized, Controlled Trial. Ann Intern Med. 2020 Jun 16;172(12):795-802. doi: 10.7326/M19-3734[↩][↩]
- Kalfus IN, Graham DY, Riff DS, Panas RM. Rifabutin-Containing Triple Therapy (RHB-105) for Eradication of Helicobacter pylori: Randomized ERADICATE Hp Trial. Antibiotics (Basel). 2020 Oct 9;9(10):685. doi: 10.3390/antibiotics9100685[↩]
- Fallone CA. The Current Role of Vonoprazan in Helicobacter pylori Treatment. Gastroenterology. 2022 Sep;163(3):572-574. doi: 10.1053/j.gastro.2022.06.076[↩]
- Crowe SE. Helicobacter pylori Infection. N Engl J Med. 2019 Mar 21;380(12):1158-1165. doi: 10.1056/NEJMcp1710945[↩]
- Chey WD, Mégraud F, Laine L, López LJ, Hunt BJ, Howden CW. Vonoprazan Triple and Dual Therapy for Helicobacter pylori Infection in the United States and Europe: Randomized Clinical Trial. Gastroenterology. 2022 Sep;163(3):608-619. doi: 10.1053/j.gastro.2022.05.055[↩]
- Phathom Pharmaceuticals Provides Update on New Drug Application Review of Vonoprazan for Erosive Esophagitis. https://investors.phathompharma.com/news-releases/news-release-details/phathom-pharmaceuticals-provides-update-new-drug-application[↩]





{kind=link}