Fordyce spots
Fordyce spots also known as Fordyce glands, are enlarged sebaceous glands without hair follicles, commonly seen around the vermilion border of the lips and oral mucosa and in the genital area 1. They may occur as a solitary lesion or more frequently in crops of about 50–100. They are easier to see when the skin is stretched. Fordyce spots lack an association with hair follicles and have ducts opening directly onto the cutaneous surface. Fordyce spots are probably present at birth but they are not obvious until puberty when they enlarge in response to the gonadal and adrenal androgenic hormones. Fordyce spots increases with age, being more common in adults than in children 2. The prevalence in adults is 70 to 80% 3. The male to female ratio is approximately 2:1 4.
Sometimes Fordyce spots cause anxiety but they are completely harmless whether on the lips or on the genitals. They are not a sexually transmitted disease and they are not infectious.
Clinically, Fordyce spots appear as asymptomatic, isolated or scattered, minute (1–5mm), creamy yellow and discrete papules. Fordyce spots occur most commonly and most conspicuously on the vermilion border of the lips and inside of the cheeks and less commonly, on the penis, scrotum, and vulva of the female. The lesions are usually bilateral and symmetrical. Treatment is usually not necessary apart from reassurance about the benign nature of the condition. Various destructive modalities have been employed by dermatologists with some success, some patients opt for laser removal or electrodessication for cosmetic reasons 5.
The importance of recognizing these papules as Fordyce spots is in the differential diagnosis of other conditions that may appear similar. Some sexually transmitted diseases (STDs) may start off looking like Fordyce spots on the genitals so it is essential to get a proper diagnosis from your doctor. STDs need to be treated appropriately with medication.
Figure 1. Sebaceous gland
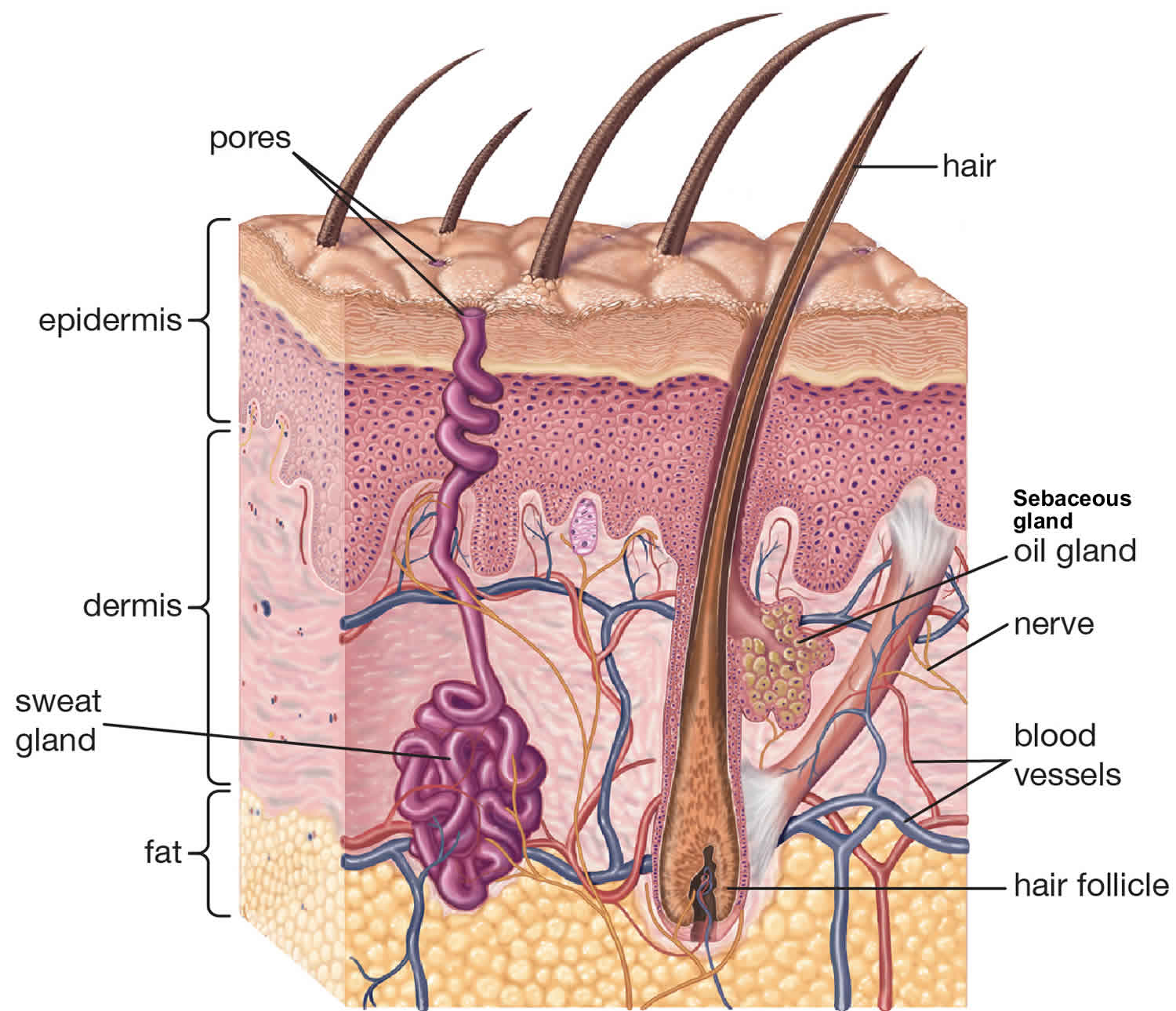
Figure 2. Fordyce spots lips

Footnote: Fordyce spots on the upper lip.
[Source 1 ]Figure 3. Fordyce spots on balls (scrotum)

Figure 4. Fordyce spots on penile shaft

Figure 5. Fordyce spots inside of the cheeks

Are Fordyce spots contagious?
No. Fordyce spots are enlarged sebaceous glands (small oil-producing gland present in the skin) without hair follicles. Fordyce spots are typically multiple, asymptomatic, and benign. They are not a sexually transmitted disease and they are not infectious. No treatment is generally advised.
Fordyce spots causes
Fordyce spots are enlarged sebaceous glands without hair follicles that can occur on various body parts such as the lips, oral mucosa, penis, and labia of the female. Some authors suggest that Fordyce spots are ectopic/heterotopic sebaceous glands 4. Other authors suggest that the lesions are not necessarily ectopic/heterotopic as it is not uncommon to have subtle or invisible sebaceous glands on the lips 6. In one study, normal sebaceous glands were present on the vermilion border of the lips in 80 to 95% of adults 7. A recent study showed that individuals with elevated lipid profile tend to have higher numbers of oral Fordyce spots 8. Further studies are necessary to confirm or refute this finding.
Fordyce spots lack an association with hair follicles and have ducts opening directly onto the cutaneous surface 9. Although these sebaceous glands are present at birth, they are not obvious until puberty when they enlarge in response to gonadal and adrenal androgenic hormones 9.. Enlargement of sebaceous glands renders them visible throughout the overlying epithelium 7.
Histological examination of the lesions show enlarged cutaneous sebaceous glands, consisting of a group of mature sebaceous lobes surrounding small ducts that emerge at the epithelial surface 10. These sebaceous glands lack an association with a hair follicle 3. Pathological alterations are rare 4.
Fordyce spots symptoms
Clinically, Fordyce spots appear as asymptomatic, isolated or grouped, minute (pinhead-sized), creamy yellow, discrete papules 6. Occasionally, the papules are lobulated or form plaques 2. They occur most commonly and most conspicuously on the vermilion border of the lips (Figure 1) and oral mucosa (Figure 5) and, less commonly, on the penis (Figure 4), scrotum (Figure 3), and labia 6. The lesions are usually bilateral and symmetrical 9. On the penile shaft, these papules are more obvious when the foreskin is stretched or during penile erection
11. A thick, chalky or cheesy material can sometimes be expressed by squeezing the lesion 11.
Fordyce spots can be cosmetically unsightly. Rarely, penile lesions may cause discomfort during sexual intercourse 12. Usually, they are of no clinical significance and are not associated with systemic disease. A recent study showed that individuals with elevated lipid profile tend to have higher numbers of oral Fordyce spots 8. Further studies are necessary to confirm or refute this finding.
Fordyce spots diagnosis
Fordyce spots diagnosis is mainly clinical. No investigation is necessary. If diagnosis or treatment is uncertain, referral to a dermatologist should be considered.
Fordyce spots differential diagnosis
Fordyce spots should be differentiated from milia and sebaceous hyperplasia. Milia are small, white, benign, dome-shaped, superficial keratinous cysts. Histologically, they appear as small infundibular cysts that are lined with stratified squamous epithelium with a granular cell layer. The cyst contains laminated layers of keratin. Primary milia may be congenital (congenital primary milia) or have onset later on in life (benign primary milia of children and adults). Congenital primary milia are present in approximately 40% of newborn infants with no sex predilection. While congenital primary milia favor the nose, benign primary milia of children and adults favor the eyelids. Secondary milia may occur in association with disease, medication, or trauma. Milia often exfoliate and resolve spontaneously. Clinically, sebaceous hyperplasia more commonly present as multiple, asymptomatic, discrete, yellow or flesh-colored, dome-shaped papules. Some of the lesions will have central umbilication. Individual lesions are usually 2 to 5 mm in diameter but may be larger in size. The face, in particular the forehead, cheeks, and nose, is most commonly affected. The condition is seen mainly in middle-aged and elderly individuals. Other differential diagnoses include syringomas, molluscum contagiosum, lichen nitidus, closed comedones, cutaneous myxomas, and calcinosis cutis.
Fordyce spots treatment
Fordyce spots are generally harmless and do not require any treatment. Typically dermatologists provide the treatments where requested. Avoid picking or squeezing the spots.
Fordyce spots can be a cause of cosmetic concern for some patients. Electrosurgery and vaporising laser treatment (CO2 laser) have been used successfully to remove the spots. Other reported treatments for Fordyce spots include bichloracetic acid, photodynamic therapy, micro-punch excision surgery and oral isotretinoin.
- Leung, Alexander & Barankin, Benjamin. (2015). Fordyce Spots. Clinical Case Reports and Reviews. 1. 10.15761/CCRR.1000140.[↩][↩]
- Chern PL, Arpey CJ (2008) Fordyce spots of the lip responding to electrodesiccation and curettage. Dermatol Surg 34: 960-962.[↩][↩]
- Plotner AN, Brodell RT (2008) Treatment of Fordyce spots with bichloracetic acid. Dermatol Surg 34: 397-399.[↩][↩]
- Baeder FM, Pelino JE, de Almeida ER, Duarte DA, Santos MT (2010) High-power diode laser use on Fordyce granule excision: a case report. J Cosmet Dermatol 9: 321-324.[↩][↩][↩]
- Wootton, Catriona & Saihan, Eric. (2015). Fordyce spots. BMJ. 350. h2545-h2545. 10.1136/bmj.h2545.[↩]
- Mutizwa MM, Berk DR (2014) Dichotomous long-term response to isotretinoin in two patients with fordyce spots. Pediatr Dermatol 31: 73-75.[↩][↩][↩]
- Elston DM, Meffert J (2001) Photo quiz. What is your diagnosis? Fordyce spots. Cutis 68: 24, 49.[↩][↩]
- Gaballah KY, Rahimi I (2014) Can presence of oral Fordyce’s granules serve as a marker for hyperlipidemia? Dent Res J (Isfahan) 11: 553-558.[↩][↩]
- Mansur AT, Aydingoz IE (2012) Unilateral buccal fordyce spots with ipsilateral facial paralysis: a sign of neuro-sebaceous connection? Acta Derm Venereol 92: 177-178.[↩][↩][↩]
- Ocampo-Candiani J, Villarreal-Rodríguez A, Quiñones-Fernández AG, Herz-Ruelas ME, Ruíz-Esparza J (2003) Treatment of Fordyce spots with CO2 laser. Dermatol Surg 29: 869-871.[↩]
- Rane V, Read T (2013) Penile appearance, lumps and bumps. Aust Fam Physician 42: 270-274.[↩][↩]
- Pallua N, Stromps JP (2013) Micro-punch technique for treatment of Fordyce spots: Aesthet Surg 66: e8-11[↩]





{kind=link}