Kohler’s disease
Kohler’s disease is an avascular necrosis of the navicular bone at the arch of the foot only seen in pediatric patients 1. X-rays show that this bone is initially compressed and later breaks into pieces before healing and hardening back into bone. Kohler’s disease occurs most frequently in children between the ages of 5 and 10 years. Signs and symptoms of Kohler’s disease include swelling, redness and/or tenderness of the affected foot which can lead to a limp or abnormal gait (style of walking). Although the exact underlying cause of Kohler disease is unknown, some scientists suspect that it may be caused by excessive strain on the tarsal navicular bone and its associated blood vessels before the bone is completely ossified (hardened). This leads to blood flow abnormalities resulting in avascular necrosis.
Kohler disease is typically unilateral, although one report in the literature found that 25% of Kohler disease is bilateral 1. Patients typically present with medial-sided foot pain, swelling of the medial foot, and/or a limp. On plain films, the navicular will have standard characteristics of avascular necrosis (AVN), including sclerosis, fragmentation, and flattening. Kohler disease is a self-limiting condition with an excellent prognosis. There have been no reported cases of Kohler disease developing long-term clinical or radiologic abnormalities 2.
The incidence of Kohler disease is not well known, considering that not all patients with Kohler disease are symptomatic. One publication estimated Kohler disease to be present in 2% of all children. Kohler disease is five times more likely to affect males than females, and it is most commonly seen in children 4 to 7 years old 1.
Kohler’s disease typically resolves on its own with or without treatment; however, pain relievers, rest, avoidance of weight-bearing activities, and/or casting may be recommended to help manage symptoms 3. Children appear to grow out of the disorder, and the affected bones usually regain their size, density and structure within three months. Rarely, symptoms may last as long as two years 4.
Figure 1. Kohler’s disease
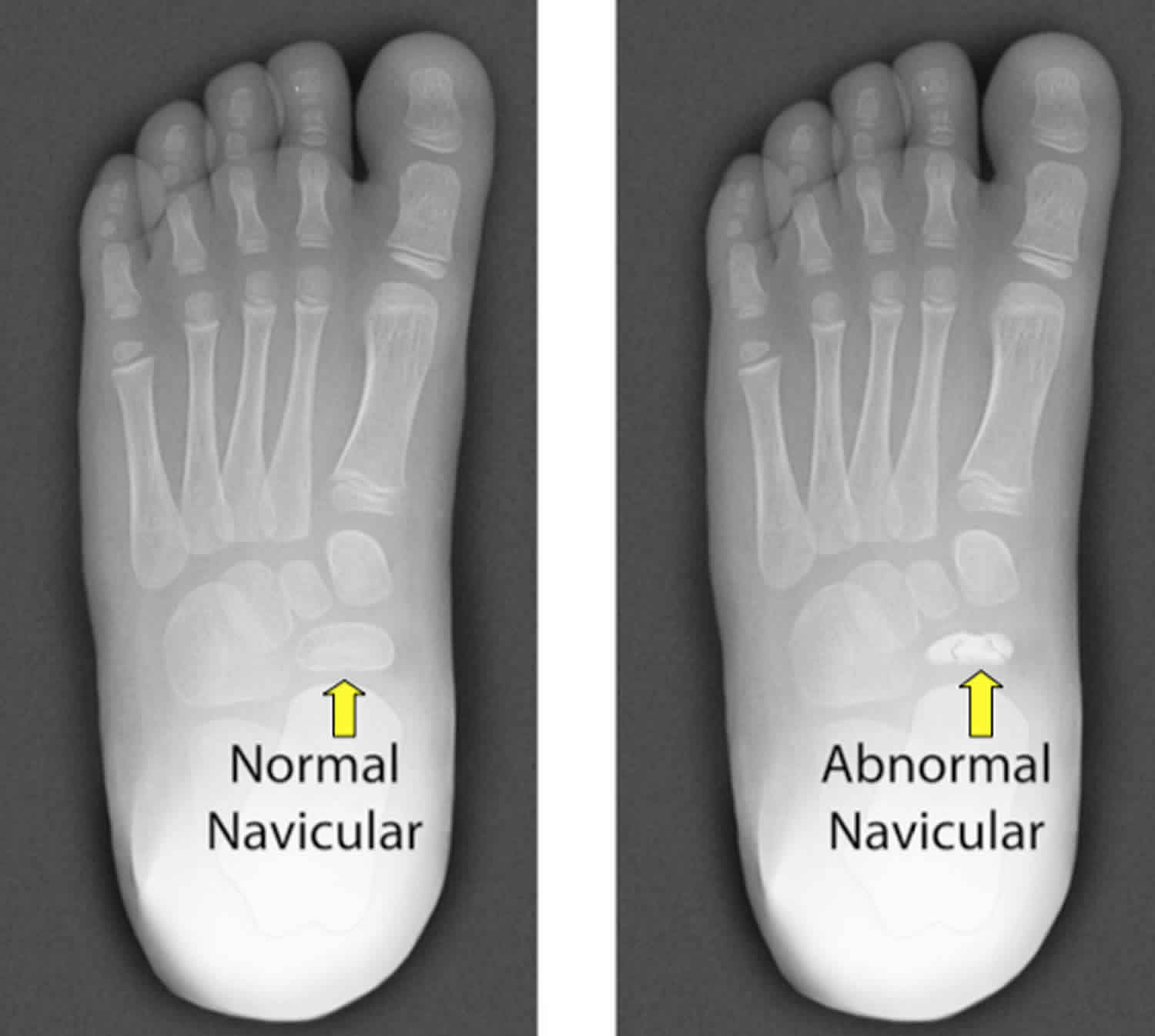
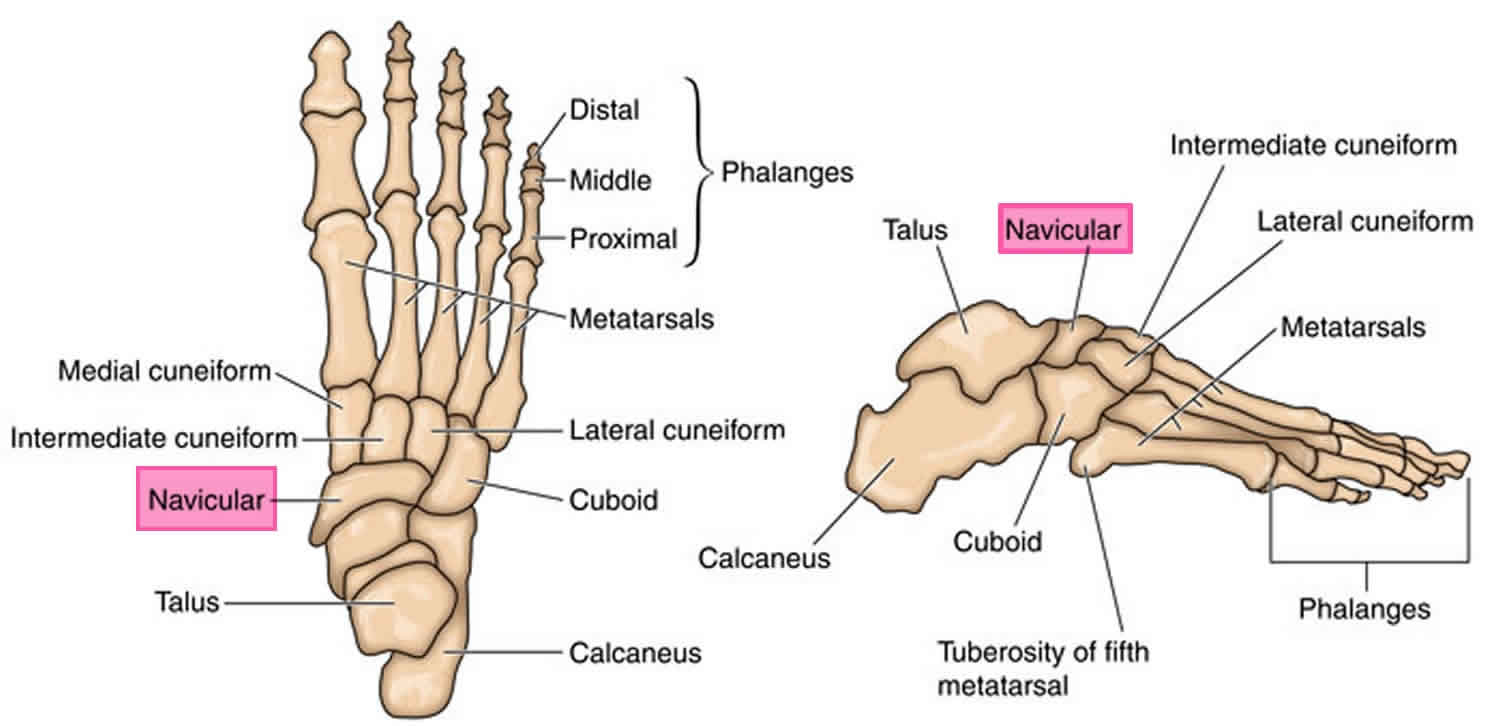
Figure 2. Navicular bone
Is Kohler disease hereditary?
The exact underlying cause of Kohler disease is currently unknown. Although some scientists have suggested that genetic factors may play a role in the development of Kohler disease, no disease-causing gene has been identified 5.
How common is Kohler disease?
The incidence of Kohler disease is not well known, considering that not all patients with Kohler disease are symptomatic. One publication estimated Kohler disease to be present in 2% of all children. Kohler disease is five times more likely to affect males than females, and it is most commonly seen in children 4 to 7 years old 1.
What is osteochondrosis?
Kohler disease is considered a type of osteochondrosis, which refers to a group of conditions that affect immature skeletal systems. In people affected by osteochondrosis, an ossification center undergoes degeneration (breakdown) followed by calcification. An ossification center is a point within a developing bone where bone formation (ossification) begins. Osteochondrosis most commonly affects the epiphyses of long bones in children 6.
What is osteonecrosis?
Osteonecrosis also known as avascular necrosis (AVN) is a medical term that refers to bone death caused by reduced blood flow to the bones of the joints. This condition can occur in virtually any bone of the body; however, the upper leg, upper arm, knee, shoulder and ankle are the most commonly affected. Although men and women of all ages can develop this condition, it generally occurs in people between the ages of thirty and fifty 7.
Kohler’s disease causes
The exact underlying cause of Kohler disease is currently unknown, but the condition is thought to result from compressive stress-related injury at a critical time of growth 8. Vascular insults, retarded bone age, and genetic predilection have also been implicated 9. Although some scientists have suggested that genetic factors may play a role in the development of Kohler disease, no disease-causing gene has been identified 10.
The navicular bone possesses a dual blood supply. A branch of dorsalis pedis artery supplies the dorsal aspect of the bone, while the plantar blood supply arises from the medial plantar branch of the posterior tibial artery. Both the dorsal and plantar blood supplies enter the navicular and branch to supply the medial and lateral thirds of the bone. This creates an avascular zone in the central one-third of the bone. Vascular foramina help to supply this avascular area and are found on the dorsal, plantar, medial, and lateral surfaces of the navicular bone. However, in a study of 100 cadaveric navicular bones, 97% of vascular foramina were smaller than 1 millimeter in adults. In theory, any compression of these small vascular foramina could result in decreased blood flow and put the navicular bone at risk for avascular necrosis.
Some orthopedic specialists think that Kohler disease may be related to an injury in the area around the navicular bone in the foot and may be the result of delayed bone formation (ossification). In children, the navicular bone is the last of the tarsal bones to ossify. In girls, the navicular bone ossifies between 18 to 24 months and in boys 30 to 36 months old. This theory points out that given the navicular bone’s slow ossification, it is weaker than the other tarsal bones. As the child grows and becomes heavier, the navicular can be compressed between the already ossified talus and cuneiform bones. The compression of the non-ossified navicular results in the squeezing of the perforating vessels in the central spongy bone, which could lead to ischemia and later avascular necrosis 11.
Kohler’s disease symptoms
Kohler disease can be asymptomatic. However, children often present to their pediatrician with concerns for dorsomedial midfoot pain. On physical exam, the patient may have point tenderness over the navicular with or without redness, warmth, and swelling. When asked to walk, the child may show an antalgic limp in which they walk on the lateral side of their foot.
Putting weight on the foot or walking is difficult, causing further discomfort and a limp. Usually, symptoms will be mild, and patients may not seek treatment until the pain and swelling have persisted for a while.
The signs and symptoms of Kohler disease vary, but may include 10:
- Swelling of the foot
- Redness of the affected area
- Tenderness, particularly along the length of the arch
- Limp or abnormal gait (style of walking)
Symptoms may worsen if weight is put on the affected foot, which can make walking painful and difficult 8.
For reasons that are not understood, the flow of blood to one of the bones in the foot (navicular bone) is interrupted, resulting in progressive degeneration of that bone. In a relatively short time, however, the bone heals itself.
Kohler’s disease diagnosis
A diagnosis of Kohler disease is suspected based on the presence of characteristic signs and symptoms. An x-ray of the foot can be used to confirm the diagnosis and evaluate the progression of the condition 10.
Plain radiographic images are the imaging modality of choice in the diagnosis of Kohler disease. The navicular will appear wafer-thin with bony collapse. The bone will appear fragmented with a loss of a trabecular pattern. There will be patchy sclerosis of the bone and increased radiodensity. Soft tissue swelling around the affected navicular bone can also be seen on plain radiographs. Advanced imaging such as CT and MRI are not required for diagnosis, although they may become necessary if the patient’s symptoms do not improve with treatment. While navicular sclerosis may be consistent with a normal variant in asymptomatic patients, it is important to correlate radiographic findings with clinical suspicions.
Basic labs, such as a complete blood count (CBC), C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR) are needed in cases in which an infection is suspected. If any of these are elevated, further diagnostic testing is warranted.
Kohler’s disease differential diagnosis
Kohler disease is often misdiagnosed as osteomyelitis in children. However, basic labs (white blood cell count, CRP, ESR) will help to differentiate between the two diagnoses. If a child has an elevated ESR or CRP, there should be a high index of suspicion for infection. Kohler disease will not have elevated inflammatory markers, and a pediatric patient should not have elevated inflammatory markers. If an infection is suspected, bone aspiration, bone biopsy, or blood cultures may be warranted.
Kohler’s disease treatment
If Kohler disease is suspected, patients should be referred to a pediatric orthopedic surgeon for further evaluation 12.
The treatment of Kohler disease is conservative. Nonsteroidal anti-inflammatory drugs (NSAIDs) can be used to decrease symptoms but have not been shown to shorten the duration of disease symptoms. Immobilization via a short leg walking cast for 4 to 6 weeks can be used in patients to shorten the duration of symptoms. The effect of weight-bearing casts compared to non-weight bearing casts is unclear and often surgeon dependent. Some reports of using offloading orthotics for symptomatic relief has been reported; however, it does not appear orthotics shorten the duration of symptoms.
There is no indication for surgery in Kohler disease. If symptoms do not improve, physicians should consider an alternative diagnosis. Both symptoms and radiographs should start to show improvement in around six months.
Kohler’s disease prognosis
The long-term outlook (prognosis) for people with Kohler disease is usually excellent and to date, there have been no reports of long-term symptoms or disability in children with Kohler disease 1. Radiographs will improve around 6 to 48 months from the onset of symptoms. Without casting, symptoms typically resolve in 6 to 9 months. In a review of case reports, patients treated in plaster casts (non-weight bearing) were pain-free at an average of 3 months. Arch support orthopedics were shown to decreased local pain but found that symptoms lasted an average of 7 months.
Symptoms can last from a few days to two years; however, most cases resolve within a year. People affected by the condition typically recover all function of the affected foot and have no lasting consequences 10. The evolution of the x-ray appearance in Köhler disease is variable. Normal x-rays may be obtained 6-18 months following onset. At adulthood, the navicular bone is expected to be normal. Patients recover excellent function 13.
- Trammell AP, Scott AT. Kohler Disease. [Updated 2019 Nov 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507831[↩][↩][↩][↩][↩]
- Barbuto L, Di Serafino M, Della Vecchia N, Rea G, Esposito F, Vezzali N, Ferro F, Caprio MG, Vola EA, Romeo V, Vallone G. Pediatric musculoskeletal ultrasound: a pictorial essay. J Ultrasound. 2019 Dec;22(4):491-502.[↩]
- Kohler Disease. https://emedicine.medscape.com/article/1234753-overview[↩]
- Kohler disease. https://rarediseases.org/rare-diseases/kohler-disease[↩]
- Kohler disease. https://emedicine.medscape.com/article/1234753-overview[↩]
- Osteochondroses. https://emedicine.medscape.com/article/1254668-overview[↩]
- Osteonecrosis. https://medlineplus.gov/ency/article/007260.htm[↩]
- Kohler Disease. https://rarediseases.org/rare-diseases/kohler-disease[↩][↩]
- Tsirikos AI, Riddle EC, Kruse R. Bilateral Köhler’s disease in identical twins. Clin Orthop Relat Res. 2003 Apr. 195-8.[↩]
- Kohler’s disease. https://emedicine.medscape.com/article/1234753-overview[↩][↩][↩][↩]
- Riaz S, Bashir H, Hassan A, Khan AH. Kohler disease: Imaging King Tut’s foot in 21st century. J Pak Med Assoc. 2018 May;68(5):822.[↩]
- Aktaş E, Ayanoğlu T, Hatipoğlu Y, Kanatlı U. Spontaneous and bilateral avascular necrosis of the navicula: Müller-Weiss disease. Eklem Hastalik Cerrahisi. 2016 Dec;27(3):179-82.[↩]
- Borges JL, Guille JT, Bowen JR. Köhler’s bone disease of the tarsal navicular. J Pediatr Orthop. 1995 Sep-Oct. 15(5):596-8.[↩]





{kind=link}