
What is nail clubbing
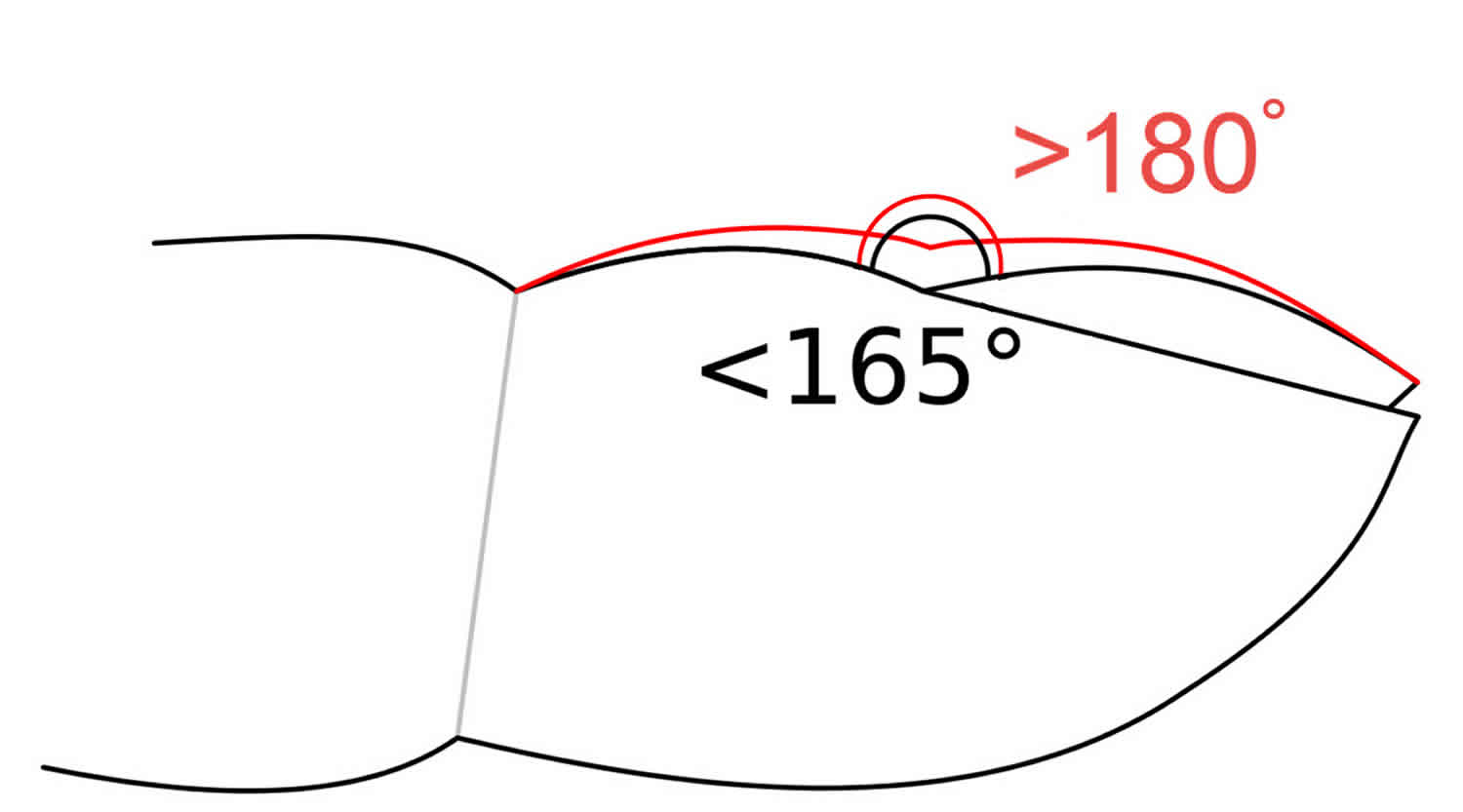
Nail clubbing is soft tissue swelling of the terminal phalanx resulting in straightening of the Lovibond angle that exists between the nail bed and the nail 1. The association of nail clubbing of the fingers with an underlying disease was known since the time of Hippocrates. Nail clubbing occurs in combination with other dermatologic and skeletal findings but can also less commonly occur in isolation. Although nail clubbing can present in many diverse conditions, it can be idiopathic or familial; the familial form frequently transmits as a dominant trait. Nail clubbing is sometimes the result of low oxygen in the blood and could be a sign of various types of lung disease. Nail clubbing is also associated with inflammatory bowel disease, cardiovascular disease, liver disease and AIDS.
Nail clubbing is a deformity of the nails characterized by:
- Loss of the Lovibond angle of the nail bed and the nail fold
- Thickening of the end of the finger
- Increase in nail fold convexity
- Soft boggy nail texture 2.
Nail clubbing is associated with a wide range of diseases, including the following heart and lung diseases:
- Lung cancer
- Interstitial lung disease, most commonly fibrosing alveolitis
- Tuberculosis (TB)
- Cystic fibrosis (CF)
- Suppurative (pus forming) lung disease, such as lung abscess, empyema, bronchiectasis
- Mesothelioma (tumor of the lining of the lung)
- Arteriovenous fistula/malformation (abnormal formation or connection between arteries and veins).
Figure 1. Nail clubbing
What causes nail clubbing?
Nail clubbing can be idiopathic or secondary to many underlying pathologies in various organ systems. There are several causes of acquired nail clubbing which include infectious, cancer, inflammatory, and vascular diseases 3. Isolated nail clubbing can be a benign hereditary condition but given the multiple associated conditions underlying etiology should be ruled out.
Causes of idiopathic or primary nail clubbing include pachydermoperiostosis, familial clubbing, and hypertrophic osteoarthropathy 4.
Causes of secondary clubbing include the following 5:
- Pulmonary disease – Lung cancer 6, cystic fibrosis, interstitial lung disease 7, idiopathic pulmonary fibrosis 8, sarcoidosis 9, lipoid pneumonia, empyema, pleural mesothelioma, pulmonary artery sarcoma 10, lung hydatid cysts 11 and pulmonary metastases.
- Cardiac disease – Cyanotic congenital heart disease 12, other causes of right-to-left shunting, and bacterial endocarditis; a scoring system for empiric treatment of infective endocarditis includes clubbing 13
- Gastrointestinal disease – Ulcerative colitis, Crohn disease, primary biliary cirrhosis, cirrhosis of the liver, hepatopulmonary syndrome 14, leiomyoma of the esophagus, achalasia, and peptic ulceration of the esophagus 15.
- Skin disease – Pachydermoperiostosis, Bureau-Barrière-Thomas syndrome, Fischer syndrome, palmoplantar keratoderma 16 and Volavsek syndrome
- Malignancies – Thyroid cancer, thymus cancer, Hodgkin lymphoma 17 and disseminated chronic myeloid leukemia, POEMS [polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes] syndrome is a rare paraneoplastic syndrome secondary to a plasma cell dyscrasia in which clubbing may be seen 18. Other findings including peripheral neuropathy, organomegaly, endocrinopathy, monoclonal plasma proliferative disorder, skin changes, sclerotic bone lesions, Castleman disease, thrombocytosis, papilledema, peripheral edema, pleural effusions, ascites, and white nails.)
- Miscellaneous conditions – Acromegaly, thyroid acropachy, pregnancy, an unusual complication of severe secondary hyperparathyroidism 19, sickle cell disease 20 and hypoxemia possibly related to long-term smoking of cannabis 21
Hypertrophic osteoarthropathy in adults is often a sign of internal cancer 22. Other stigmata may also be evident, such as acquired keratoderma taking on a yellow velvety appearance with accentuation of dermatoglyphic lines.
As a paraneoplastic syndrome, it is most commonly associated with non–small-cell lung cancer 23, although it may occur with metastatic melanoma and other cancers 24. Hypertrophic pulmonary osteoarthropathy is evident in 1- 5 % of all patients with non–small-cell lung cancer 25.
Among hemodialysis patients with end-stage renal disease, the finding of clubbing was linked with the calcium-phosphorus product 26.
Nail changes in 100 chronic renal failure patients undergoing hemodialysis and 100 matched controls were assessed 27. Nail disorders were more prevalent in the renal failure patients (76%) than in the control group (30%). The half-and-half nail was the most common finding (20%), followed by absent lunula, onycholysis, brittle nail, Beau lines, clubbing, longitudinal ridging, onychomycosis, subungual hyperkeratosis, koilonychias, total leukonychia, splinter hemorrhage, pitting, and pincer nail deformity.
Nail clubbing symptoms
Nail clubbing occurs when the tips of the fingers enlarge and the nails curve around the fingertips, usually over the course of years. The development of nail clubbing usually is gradual enough that many patients are unaware of its presence; however, some patients may report swelling of the distal portion of the digits, which may be bilateral or unilateral or may involve a single digit.
Although clubbing typically is painless, it rarely may present with pain in the fingertips.
Rapid postoperative resolution of clubbing in a few days was described in a patient with aortic and mitral valve replacement due to infective endocarditis 28.
Hypertrophic osteoarthropathy may occur as an isolated calcaneal periostitis bilaterally 29.
Finger clubbing may be a clue to an underlying systemic disorder, including vasculitis with chronic hepatitis C and type II mixed cryoglobulinemia 30.
Nail clubbing treatment
Treatment of the underlying pathological condition may decrease the nail clubbing or potentially, reverse it if performed early enough. Response to treatment will have a significant degree of variation depending on the underlying disease process. Once substantial chronic tissue changes, including increased collagen deposition, have occurred, reversal is unlikely. Data for the reversibility of clubbing is sparse. Clubbing reversibility has been reported in particular in patients undergoing prostaglandin therapy for liver disease who developed clubbing which reversed with the cessation of therapy 31.
Prognosis of the underlying disease should be determined on an individual basis.
- Burcovschii S, Aboeed A. Nail Clubbing. [Updated 2019 Apr 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539713[↩]
- Dermatologic Manifestations of Pulmonary Disease. https://emedicine.medscape.com/article/1094030-overview[↩]
- Myers KA, Farquhar DR. The rational clinical examination. Does this patient have clubbing? JAMA. 2001 Jul 18;286(3):341-7.[↩]
- Hugosson C, Bahabri S, Rifai A, al-Dalaan A. Hypertrophic osteoarthropathy caused by lipoid pneumonia. Pediatr Radiol. 1995. 25(6):482-3.[↩]
- Fawcett RS, Linford S, Stulberg DL. Nail abnormalities: clues to systemic disease. Am Fam Physician. 2004 Mar 15. 69(6):1417-24.[↩]
- Sridhar KS, Lobo CF, Altman RD. Digital clubbing and lung cancer. Chest. 1998 Dec. 114(6):1535-7.[↩]
- Grathwohl KW, Thompson JW, Riordan KK, Roth BJ, Dillard TA. Digital clubbing associated with polymyositis and interstitial lung disease. Chest. 1995 Dec. 108(6):1751-2.[↩]
- Kanematsu T, Kitaichi M, Nishimura K, Nagai S, Izumi T. Clubbing of the fingers and smooth-muscle proliferation in fibrotic changes in the lung in patients with idiopathic pulmonary fibrosis. Chest. 1994 Feb. 105(2):339-42.[↩]
- West SG, Gilbreath RE, Lawless OJ. Painful clubbing and sarcoidosis. JAMA. 1981 Sep 18. 246(12):1338-9.[↩]
- Loredo JS, Fedullo PF, Piovella F, Moser KM. Digital clubbing associated with pulmonary artery sarcoma. Chest. 1996 Jun. 109(6):1651-3.[↩]
- Smahi M, Lakranbi M, Choumi I, Elbiaz M, Amara B, Benjelloun MC. [Nail clubbing and lung hydatid cysts]. Rev Mal Respir. 2010. 27(1):99-101. [↩]
- Pineda CJ, Guerra J Jr, Weisman MH, Resnick D, Martinez-Lavin M. The skeletal manifestations of clubbing: a study in patients with cyanotic congenital heart disease and hypertrophic osteoarthropathy. Semin Arthritis Rheum. 1985 May. 14(4):263-73.[↩]
- Gouriet F, Tissot-Dupont H, Casalta JP, Hubert S, Fournier PE, Edouard S, et al. Marseille scoring system for empiric treatment of infective endocarditis. Eur J Clin Microbiol Infect Dis. 2018 Feb 3.[↩]
- Younis I, Sarwar S, Butt Z, Tanveer S, Qaadir A, Jadoon NA. Clinical characteristics, predictors, and survival among patients with hepatopulmonary syndrome. Ann Hepatol. 2015 May-Jun. 14 (3):354-60.[↩]
- Kitis G, Thompson H, Allan RN. Finger clubbing in inflammatory bowel disease: its prevalence and pathogenesis. Br Med J. 1979 Oct 6. 2(6194):825-8.[↩]
- Barraud-Klenovsek MM, Lübbe J, Burg G. Primary digital clubbing associated with palmoplantar keratoderma. Dermatology. 1997. 194(3):302-5.[↩]
- Mullins GM, Lenhard RE Jr. Digital clubbing in Hodgkin’s disease. Johns Hopkins Med J. 1971 Mar. 128(3):153-7.[↩]
- Miest RY, Comfere NI, Dispenzieri A, Lohse CM, El-Azhary RA. Cutaneous manifestations in patients with POEMS syndrome. Int J Dermatol. 2013 Apr 4.[↩]
- Grekas D, Avdelidou A. Digital clubbing as an unusual complication associated with severe secondary hyperparathyroidism: report of two cases. Hemodial Int. 2007 Apr. 11(2):193-7.[↩]
- Helvaci MR, Gokce C, Davran R, Acipayam C, Akkucuk S, Ugur M. Tonsilectomy in sickle cell diseases. Int J Clin Exp Med. 2015. 8 (3):4586-90.[↩]
- Schuller A, Cottin V, Hot A, Cordier JF. Finger clubbing and altered carbon monoxide transfer capacity in cannabis smokers. Eur Respir J. 2008 Feb. 31(2):473-4.[↩]
- El Bakkal A, Idrissi R, Meziane M, Mikou O, Sekal M, Belghiti H, et al. [Tripe palms and a hypertrophic osteoarthropathy syndrome revealing a neuroendocrine carcinoma of the lung]. Ann Dermatol Venereol. 2011 Oct. 138(10):668-72.[↩]
- Katsurada N, Tachihara M, Jimbo N, Koyama K, Nakata K, Nagano T, et al. Successful Treatment of ROS1-rearranged Lung Cancer Complicated by Hypertrophic Pulmonary Osteoarthropathy with Crizotinib Therapy: A Case Report. Intern Med. 2019 Jan 10.[↩]
- Thompson MA, Warner NB, Hwu WJ. Hypertrophic osteoarthropathy associated with metastatic melanoma. Melanoma Res. 2005 Dec. 15(6):559-61.[↩]
- Lommatzsch M, Julius P, Lück W, Bier A, Virchow JC. [Hypertrophic Pulmonary Osteoarthropathy as a Cue for NSCLC: Four Cases in the Light of the Current Literature]. Pneumologie. 2012 Feb. 66(2):67-73.[↩]
- Tajbakhsh R, Dehghan M, Azarhoosh R, Haghighi AN, Sadani S, Zadeh SS, et al. Mucocutaneous manifestations and nail changes in patients with end-stage renal disease on hemodialysis. Saudi J Kidney Dis Transpl. 2013 Jan. 24(1):36-40.[↩]
- Salem A, Al Mokadem S, Attwa E, Abd El Raoof S, Ebrahim HM, Faheem KT. Nail changes in chronic renal failure patients under haemodialysis. J Eur Acad Dermatol Venereol. 2008 Nov. 22(11):1326-31.[↩]
- Ozdemir B, Senturk T, Kaderli AA, et al. Postoperative regression of clubbing at an unexpected rate in a patient with aortic and mitral valve replacement due to infective endocarditis. Ir J Med Sci. 2008 Oct 9.[↩]
- Moralidis E, Gerasimou G, Theodoridou A, Hilidis I, Mylonaki E, Gotzamani-Psarrakou A. Hypertrophic osteoarthropathy manifested with isolated calcaneal periostitis in bone scintigraphy. Ann Nucl Med. 2010 Feb 2.[↩]
- Pinto-Almeida T, Caetano M, Alves R, Selores M. Cutaneous lesions and finger clubbing uncovering hypocomplementemic urticarial vasculitis and hepatitis C with mixed cryoglobulinemia. An Bras Dermatol. 2013 Nov-Dec. 88(6):973-6.[↩]
- Dubrey S, Pal S, Singh S, Karagiannis G. Digital clubbing: forms, associations and pathophysiology. Br J Hosp Med (Lond). 2016 Jul;77(7):403-8.[↩]





{kind=link}