Nephrostomy
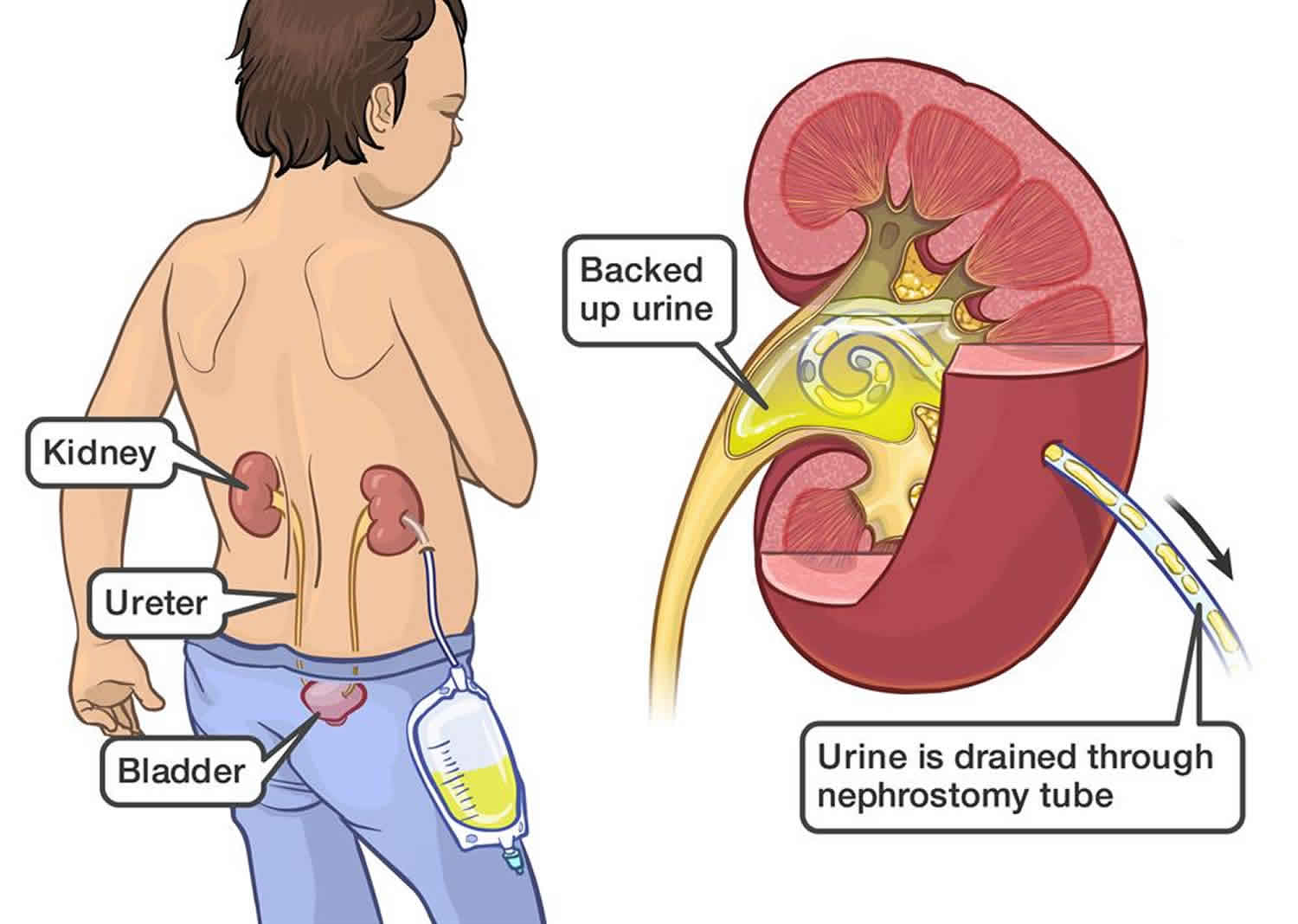
Nephrostomy also known as percutaneous nephrostomy, is a minimally invasive temporary or permanent procedure using ultrasound or x-ray guided (fluoroscopic or CT guidance) where a thin catheter, tube or stent is placed through the skin into your kidney in the renal pelvis or a calyx to drain urine. The nephrostomy has multiple functions but is used most frequently to provide urinary drainage when the ureter is obstructed and retrograde access is inadvisable or impossible, for example if you have a blockage or a hole in your urinary tract. The blockage may be caused by a kidney stone, infection, scar tissue, or a tumor. A nephrostomy can also be used to gain access to the upper urinary tract for various antegrade endourologic procedures, such as intracorporeal lithotripsy, chemical stone dissolution, antegrade radiologic studies of the ureter, and double-J stent placement.
You may have one tube in a kidney or two tubes, one in each kidney. The urine collects in a bag attached to the tube. In most cases, the bag is attached to your leg. Sometimes the catheter tube has a valve that lets you drain the urine into the toilet or other container. If you have only one tube, you still need to urinate. Your other kidney will still produce urine that will drain into your bladder.
Nephrostomy has several other functions, including the following:
- To remove or dissolve renal calculi
- To obtain direct access to the upper urinary tract for various endourologic procedures
- To diagnose ureteral obstruction, filling defects, and anomalies via antegrade radiography
- To deliver chemotherapeutic agents to the renal collecting system
- To provide prophylaxis after resection for local chemotherapy in patients with tumors of the renal pelvis
Having a nephrostomy tube in for a long time increases the risk of getting an infection.
Nephrostomy placement can potentially injure several surrounding organs and structures including the pleura, diaphragm, colon, spleen and liver. Of these, injuries to the pleura and diaphragm are the most common. The pleura extend to the lower margin of the 12th rib along the paravertebral line. Therefore, pleural injury is minimized when nephrostomy placement is below the 12th rib. Placement above the 12th rib will usually puncture the diaphragm.
The technical success rate for nephrostomy with dilated calyces without stones is usually at least 95% 1. However, the success in nondilated systems may decrease to around 80% 2.
Benefits of nephrostomy include the following 3:
- Can save nephrons immediately and give a greater chance than other interventions to save kidney function.
- Can relieve pain from an obstruction.
- Can create a better chance to treat infected urine than medicine alone.
- Is less likely to result in injury to abdominal organs, causes less muscle injury and pain, and leaves a much smaller scar than surgery.
- Less manipulation of ureteral stones. Can use a larger tube for improved drainage compared to transurethrally placed retrograde double J stents.
- When used for pyonephrosis and urosepsis, fever resolution and pain relief typically follow rapidly within just one to two days.
Nephrostomy indications
Percutaneous nephrostomy is occasionally essential, if not lifesaving, in the treatment of acute or chronic upper urinary tract obstruction. It is the first step in obtaining antegrade access to the kidney for various procedures. Specific indications for percutaneous nephrostomy include the following:
- Acute or chronic upper urinary tract obstruction in which access to the kidney is impossible from the lower urinary tract because of stones, infections, tumors, or anatomic anomalies, especially when a double-J stent cannot be placed through the ureter because of above-mentioned circumstances
- When a patient’s creatinine level is rising above the reference range and the urine cannot be drained through the ureter
- Renal pelvis disorders (eg, ureteropelvic junction obstruction, horseshoe kidneys, ureter duplex, ureter fissures, double renal collecting systems)
- Hydronephrosis in renal transplant allografts: When dilatation of the renal pelvis affects kidney function to the extent that double-J stent placement is difficult or impossible, percutaneous nephrostomy may be an easier option.
- Treatment of staghorn calculi and large or lower-pole kidney stones when a percutaneous nephrolithotomy is likely to be followed because of the stone burden and an extracorporeal shockwave lithotripsy (ESWL) is less likely to be successful
- Contraindications to extracorporeal shockwave lithotripsy (ie, size of patient): Most extracorporeal shockwave lithotripsy units have a weight limit of 140 kg (approximately 300 lb).
- Body habitus that prevents extracorporeal shockwave lithotripsy (eg, contractures): Disabled patients occasionally cannot be positioned on an extracorporeal shockwave lithotripsy unit in a prone or supine position.
- Stones or tumors associated with distal obstruction or a foreign body that cannot be removed through the ureter
- When rapid dilation of the nephrostomy tract is required (eg, when access is needed instantly for operative procedures within the renal collecting system [for stone removal or tumor ablation])
- Prolonged sequential dilatation: Gradually increasing the catheter size may be necessary when a nephrostomy tube is placed permanently for urine drainage in patients in whom a retrograde access to the kidney is impossible (eg, advanced metastatic tumors, loss of the total ureter, patients with a palliative nephrostomy tube whose cases are inoperable).
- A rare indication is antegrade nephrostomy to control a ureteral lesion after ureteral trauma that cannot be fixed in a retrograde fashion in a nonobstructed kidney. This can occur with a completely dissected ureter after gynecological, surgical, or urological procedures discovered after the procedure. Most likely, a urinoma has developed around the dissected ureter, with the kidney itself not being obstructed but in being need for a nephrostomy.
- In an emergency situation a nephrostomy may always be mandatory.
Drainage
Nephrostomy is the procedure of choice when transurethral access is impossible or has already failed at relieving an obstructed urinary system from extrinsic mass effect (e.g., pregnancy, malignancy, fluid collections such as cysts, abscesses, or urinomas) or intrinsic blockage (e.g., benign or malignant strictures). Drainage of an obstructed renal unit is the most common indication for nephrostomy accounting fo 85 to 90% of all nephrostomy placements 4. Unless infected, establishing drainage of an obstructed, hydronephrotic kidney is not an acute emergency. Even with complete obstruction for a full week, complete renal recovery is likely. the longer the obstruction beyond one week, the lower the eventual recovery rate. After 12 weeks of complete outlet obstruction, very little recovery of renal function in that kidney can be expected 5. Bilateral nephrostomy drainage is rarely indicated and should be reserved for special cases such as patients with intractable, severe hemorrhagic cystitis or bilateral, treatable malignant or benign disease 6.
Pyonephrosis and obstructive pyelonephritis
The most common reason for emergency nephrostomy placement is to provide drainage in an acutely obstructed, infected kidney (pyonephrosis or obstructive pyelonephritis) in a septic patient, due to the high mortality risk as well as the permanent renal impairment it can cause. In these cases, both percutaneous nephrostomy and transurethral retrograde Double J stenting are recommended. The decision of which one is preferred is usually determined by local technical expertise, equipment availability and individual patient factors. Nephrostomy is often preferred in the most seriously ill patients based on its reduced manipulation of the obstructed, infected ureter. The transurethral approach may not be successful in bypassing a severely obstructed ureteral stone which is not an issue for nephrostomy. Even when transurethral bypass of an obstructing stone is accomplished, nephrostomy generally offers the opportunity to use a larger caliber drainage catheter. However, in a morbidly obese patient with minimal hydronephrosis or in a patient with an uncorrected coagulopathy, transurethral Double J stenting would be preferred. Typically, urology will be involved in these emergency cases and make the final decision regarding the preferred therapeutic approach, usually in consultation with radiology 7.
Nephrolithiasis treatment
nephrostomy is the first step in accessing the renal collecting system to enable percutaneous insertion of devices to treat nephrolithiasis (percutaneous nephrolithotomy) for:
- Staghorn calculi
- Other large, renal, pelvis (usually greater than 2 cm) and lower pole (usually greater than 1 cm) stones
- Ureteral stones that are not amenable to transurethral manipulation due to distal ureteral strictures, tumors, reimplantation, etc.
- Complex or abnormal renal anatomy
- Pregnancy
Nephrostomy creates a tract through which lasers, ultrasonic probes, and retractable baskets can be inserted for mechanical crushing, vaporization and stone retreival. In this way, nephrostomy can be an adjunct therapy to percutaneous lithotomy or extracorporeal shock wave lithotripsy, which may cause a large stone to fragment into many smaller pieces that are still large enough together to result in obstruction. The overwhelming majority (90%) of percutaneous renal access prior to definitive percutaneous nephrolithotomy surgery is now done by interventional radiology 8.
Nephrostomy rarely may need to be used as part of the “primary treatment strategy” in persons with the recurrent stone formation, such as in the setting of mineral-forming metabolic disease. In such cases, 24 hour urine testing and optimal prophylactic therapy is recommended.
Pregnancy
Nephrolithiasis is the most common non-obstetrical complication of pregnancy. Double J stents and nephrostomy are considered equally safe and effective in relieving pain in pregnant nephrolithiasis patients who are not manageable with conservative measures alone. Double J stents are less well tolerated by most patients and are associated with increased rates of ascending urinary infection 9. nephrostomy has been associated with higher rates of septic complications and may more easily become dislodged. Both will require frequent replacement, usually every 4-6 weeks, due to very rapid encrustation which is peculiar to pregnancy.
Urinary diversion
Healing of injured urinary tract tissue, such as in the setting of urinary leak or fistula and hemorrhagic cystitis, may be accelerated if urine is preferentially rerouted away from the region of inflammation through bilateral nephrostomies. Urinary urokinase tends to promote bleeding which can be eliminated with bilateral nephrostomies. This is limited to severe and refractory cases of hemorrhagic cystitis 10.
Other Therapeutic Ureteral Interventions
Direct access to the collecting system percutaneously may be the least invasive (i.e., less than surgery and when transurethral access is not feasible) manner for introducing tools for treating strictures, fistulas, or infections. Pyeloplasty or urethroplasty may relieve a stricture that developed secondary to inflammation from stones, trauma or other causes. Stent insertion may allow a fistula to heal. Direct administration of a highly concentrated medication may help treat resistant infections (e.g., fungal) while reducing systemic toxicity. Percutaneous renal access can also help with uretero-enteric anastomotic strictures in post-cystectomy patients as retrograde access across such strictures is very problematic 11.
Nephrostomy contraindications
Nephrostomy should be avoided or delayed in certain circumstances but there are no absolute contraindications 4.
Nephrostomy contraindications:
- Bleeding diathesis (eg, hemophilia, thrombocytopenia) and uncontrolled hypertension
- Anticoagulant use (eg, aspirin [relative contraindication], heparin, warfarin)
As for all procedures, it is advisable to start with the least potentially harmful manner of therapy. Transurethral access should generally be considered as the first line whenever feasible to avoid the risks inherent with new percutaneous access procedures. Reconsider the procedure if the patient has a predicted very short-term survival.
Untreated urinary tract infections are a relative contraindication.
Attempting nephrostomy on a non-dilated system may be deferred temporarily if there is a chance that the calyces may increase in size with a short delay to make the procedure easier and possibly safer. Certain factors may need to be addressed prior to attempting the procedure, such as risk factors for hemorrhage and complications from sedation (as discussed below). Patients with obstructed urinary tracts may have renal dysfunction resulting in hyperkalemia, which can destabilize cardiac myocytes and cause a life-threatening arrhythmia if not addressed urgently. In the setting of severe hyperkalemia (i.e., potassium level greater than 7 mEq/L), hemodialysis should be performed before attempting nephrostomy.
During informed consent for the procedure, make the patient aware of the likelihood of having a new foreign body that requires maintenance for weeks or months and may necessitate prolonged nursing or family medical support with limited lifestyle functionality. The unwillingness of a patient to accept this or to accept the risks of the procedure is a contraindication to the procedure.
Specific concerns must be addressed before attempting the procedure, such as the risks of hemorrhage and complications from sedation, with such risks mitigated if possible. The Society of Interventional Radiology provides a list of recommendations for the cessation of antiplatelet and anticoagulant medications for interventional radiology procedures, which it categorizes based on hemorrhage risks from level 1 to level 3 12. The Society of Interventional Radiology classifies nephrostomy as a level 3 procedure.
For level 3 procedures, the Society of Interventional Radiology recommends that the international normalized ratio (INR) be no greater than 1.5, activated partial thromboplastin time (APTT) be no greater than 1.5 times the particular hospital’s standard of normal, and that the platelet count be at least 50,000 cells/cubic microliter 12.
The Society of Interventional Radiology also lists anticoagulants that should be withheld (or their side effects medically corrected) to reduce bleeding risks. Any dose of aspirin is recommended to be withheld for 5 days. Enoxaparin at prophylactic doses does not require delaying the procedure, but at therapeutic dosing should result in scheduling the procedure 24 hours later than the most recent dose when possible.
Nephrostomy procedure
Preprocedural workup consists of confirming the indication for the nephrostomy placement, assessing the risk of sedation and the procedure, and when possible, minimizing any factors contributing to increased risk. All available cross-sectional imaging should be reviewed to assess for any anatomic factors (described below), which may make the procedure more difficult or risky.
Nephrostomy involves creating an opening into the kidney to maintain temporary or permanent urinary drainage. The collecting system of the kidney is punctured percutaneously with a needle under fluoroscopic, ultrasonographic, or CT guidance. The needle is passed through the skin, subcutaneous tissue, external and internal muscle layers, and the renal parenchyma to reach the collecting system. When the needle has entered the renal collecting system, a guidewire is passed through the needle into the kidney and possibly down the ureter. Over the guidewire, various dilators can be used to establish and enlarge the nephrostomy tract, which is then maintained by a tube.
Alternatively, a nephrostomy tube can be placed during open surgery. In this procedure, a tube is placed into the renal pelvis, perforating the renal parenchyma and puncturing the flank musculature, subcutaneous tissues, and skin to create a direct passage between the renal collecting system and the external environment.
Anesthetic agents can be more hazardous in patients with overt renal shock. Therefore, performing the nephrostomy under local anesthesia is especially important when the procedure is potentially lifesaving.
Determination of periprocedural anesthesia risk is site dependent. Many hospitals require physicians to assess the patient using the American Society of Anesthesiology physical classification system and a Mallampati score. If the patient is American Society of Anesthesiology class 4 or higher and/or has any other anesthetic risk factors, such as an advanced airway, then some institutions and authors recommend that the patient should have anesthetic consultation prior even to “low risk” procedures such as nephrostomy 13.
Pre-procedure antibiotics are given an hour before the procedure if there is a suspicion of an infected collecting system, which is frequently the setting in which the request for nephrostomy is made. The main bacteria to cover empirically are gram-negative Escherichia coli, Proteus species, and Klebsiella species as well as gram-positive Enterococcus. Less common, but often resistant to early generation penicillins and cephalosporins, is Pseudomonas, a gram-negative rod with a beta-lactamase. Usually, anaerobic coverage is not needed. The Society of Interventional Radiology 14 lists 4 first-line antibiotic options, all of which contain a cephalosporin or penicillin, but not all of which typically provide coverage for Pseudomonas. The American Urological Association Best Practice Policy recommends a first or second generation cephalosporin, or clindamycin, or gentamycin and metronidazole 15. For patients who will be undergoing subsequent percutaneous nephrolithotomy procedures, renal pelvis urine cultures have been shown to be more sensitive and useful than bladder urine cultures in predicting urosepsis 16. Also, several clinical studies have demonstrated a benefit of one week of antibiotic treatment prior to percutaneous nephrolithotomy even when the initial urine culture is negative 17.
The patient may have some degree of renal failure-related metabolic imbalances that should be sought out and potentially corrected prior to initiating the nephrostomy procedure to decrease the risk of complications. Hyperkalemia or metabolic acidosis may induce arrhythmias. In this situation, it may be judicious to review an ECG. If no arrhythmia or symptoms/signs of hyperkalemia (usually nonspecific weakness, fatigue, and dyspnea; sometimes palpitations or chest pain) are present, then emergent treatment for hyperkalemia is not “needed” but should still be considered if the serum value is above 5.5 mEq/L. Due to the risk of sepsis/septic shock during the procedure, there should be a low threshold to request that an expert on the management of hypotension (such as an anesthesiologist) be present or immediately available.
When punctures are poorly placed, there is a greater risk of complications. This may impede the success of future interventions. Therefore, a cautious approach should be taken without too much guarantee of where needle placement will be attempted until imaging confirms the anatomic layout and what options for a planned puncture route are available and ideal. CT may be needed for treatment planning purposes in cases of aberrant anatomy, such as a horseshoe kidney or scoliosis causing the kidney to lie deeper than usual within the abdomen.
Ultrasound may be used in isolation to confirm that the colon is not in the line of puncture and to determine the degree of hydronephrosis. About 5% of patients will demonstrate a retrorenal colon when placed prone 18. This is more common in thinner patients with limited abdominal fat. It can be predicted by checking a cross-sectional axial CT image. If this is not available, the colon can usually be easily identified using fluoroscopy at the time of the nephrostomy as it will typically contain gas when patients are in the prone position 6.
Medications
- Most patients should receive broad-spectrum parenteral antibiotics.
- If drugs are administered, the authors recommend cephalosporin or a combination of penicillin and aminoglycoside prior to the procedure, depending on the patient’s allergies.
- In pediatric patients, adjust antibiotics for age and weight.
Drug contraindications include corresponding drug allergies and urinary tract infection in an elective setting, hepatic failure, and renal failure.
Pregnancy
- During pregnancy, nephrostomy is limited to only selected individuals, such as those with symptomatic renal obstruction and an inability to access the kidney from the bladder.
Nephrostomy technique
A target calyx is selected using either ultrasound or fluoroscopic guidance or both. Intravenous or retrograde contrast through a ureteral catheter can be used to help visualize the internal renal anatomy fluoroscopically.
Skin entry point selection is based on the renal anatomy, underlying problem and whether or not other associated procedures, such as percutaneous nephrolithotomy, are being planned. In general, the entry point should be below the 12th rib to minimize pleural and diaphragmatic trauma. If too medial a site is chosen, the patient will likely suffer more pain as the paraspinal muscles will tend to kink the nephrostomy tube and make supine positioning more uncomfortable. Too lateral an access site will increase the chances for accidental trauma to the colon.
A posterior calyx is usually preferred for entry as this will utilize Brodel’s line to minimize bleeding. Access through an infundibulum or renal pelvis is discouraged as it increases the risk of a vascular injury.
When percutaneous nephrolithotomy is anticipated, discussion with urology is recommended to optimize placement for stone fragmentation and removal. The planned nephrostomy approach should allow direct access to the area of largest stone burden with rigid instruments if possible, as this will greatly facilitate later stone fragmentation and removal by urology. Upper pole access is recommended for complex lower pole stones, calculi in horseshoe kidneys, complete staghorn stones and large proximal ureteral stones. If an intercostal approach (above the 12th rib) is used, a chest x-ray following the procedure is recommended
The most commonly performed technique for needle insertion is the “eye of the needle” approach. This uses the C-arm or fluoro placed so that the needle is parralel and pointed directly at the target calyx or stone. Depth of penetration is determined by rotation or angulation of the x-ray unit.
A one-stick or two-stick technique can be used. Typically, for percutaneous nephrolithotomy, there is an existing, radio-opaque stone that can be used as a target allowing the one-stick technique. In the two-stick method, the first needle puncture is used only to opacify the collecting system with contrast so that the final or definitive stick with another needle can be optimally directed. Since the first stick is just for opacification, a smaller needle is suggested and it can be targeted directly at the renal pelvis. A small amount of air or carbon dioxide can be injected into the renal pelvis to help visualize the posterior calyces as the gas will preferentially fill them in prone patients providing an obvious target 6.
A needle (usually 18-gauge or 21-gauge size) is inserted followed by aspiration of renal pelvis urine, contrast (optional) and a guidewire. If a renal stone is present, the needle can be targeted directly to the calculus. An 18-gauge needle can easily transmit a 0.035-inch guidewire. If a 21 gauge needle is used, then a transitional dilator is used to allow for a 0.035-inch guidewire to be passed. 18 gauge needles tuypically track straighter, pass easier through soft tissue and are better visualized using ultrasound They also do not need further dilation to pass a 0.035-inch guide wire. No increase in significant bleeding complications was noted between 18-gauge and 21-gauge needles when used for nephrostomy access 19.
The guidewire is directed to achieve stable purchase, ideally in the ureter, but sometimes out of necessity to a different calyx or the renal pelvis. An angled catheter may be used to redirect the guidewire. When the guidewire position is settled upon, sequential, transitional dilators (Amplatz) or a balloon dilator are used to open the track for the eventual nephrostomy catheter, which usually starts at about 8 French. Transurethrally placed double J stents are usually only 6 or 7 French but they can go up to a maximum of 8 French.
Nephrostomy complications
The Society of Interventional Radiology has published complication rates for nephrostomy. The rate of major complications is around 2% to 10%. Major complications include:
- Sepsis 2
- Hemorrhage, including subcapsular hematoma and pseudoaneurysm 20))
- Pneumothorax 21
- Puncture of adjacent organs 2
- Urine leak/urinoma
- Death
Transgression of blood vessels during nephrostomy is to be expected. Coagulation usually occurs successfully, and hemorrhage ceases entirely within 2 to 3 days. Bleeding through the catheter can occur if a catheter side hole is left in communication with a renal vessel or if a pseudoaneurysm develops. Minor, temporary bleeding after nephrostomy placement is expected and occurs in about 95% of cases. Significant bleeding requiring transfusion has been reported in 1 to 4% of patients while small retroperitoneal hematomas have been found in 13% 4.
In hemodynamically stable patients:
If arterial hemorrhage is obvious (such as bright red pulsatile blood is coming out of the tube), then the patient should be taken for emergent angiographic embolization.
If hemorrhage is suspected (such as from observing persistent hematuria, a falling hemoglobin level, or unstable vital signs), then CT angiography (CTA) can be considered as a first-line diagnostic tool. Digital subtraction angiography via arterial puncture can be performed after that for embolization treatment if evidence of bleeding is seen on the CT angiography. However, whenever there is strong clinical suspicion of bleeding in the absence of hemorrhage seen on CT angiography, then a fluoroscopic tractogram should be performed next.
If no vessels are opacified or if the drainage catheter side holes are found to lie outside the kidney, then the catheter should be repositioned and the tractogram repeated. If a vein is opacified, then the catheter should be upsized to tamponade the vein. Time should be given to see if the intervention worked. If an artery is opacified, then the catheter should be upsized to tamponade the artery. If blood can still be aspirated through the larger catheter, then angiographic embolization of the renal artery branch involved should be performed urgently.
In hemodynamically unstable patients:
A decision must be reached between the radiologist and surgeon whether the patient should go to surgery, to angiography, or both (if angiography can be performed in the operating room).
nephrostomy provides a conduit for bacteria to enter the urinary tract from an external source. Although nephrostomy may be performed to treat the obstruction that is the cause of sepsis, nephrostomy itself may also cause sepsis. Preventive measures include routine catheter exchange every 2 to 3 months and using a catheter that has a good chance at remaining patent. Pyelonephritis is treated with antibiotics (such as Unasyn). Intravenous (IV) fluids, oxygen, and vasopressors in the setting of an intensive care unit should also be considered.
Infections associated with nephrostomy should be treated with culture specific antibiotics. Once appropriate antibiotics have been administered, it is recommended that the nephrostomy tube be changed within four days 22.
Percutaneous nephrostomy catheters can become clogged with encrustations (usually calcium phosphate). Catheter flushing can help with an acute obstruction temporarily, but even routine flushing does not appear to affect the rate of encrustation. Only increased hydration has been shown to reduce the encrustation rate. In pregnancy, nephrostomy catheters should be changed every 4-6 weeks. For most other patients, routine changes every 3 months is typically suggested.
Nephrostomy care
- Wash your hands before you handle the nephrostomy tube.
- Clean the area around the tube with soap and water every day.
- Keep the drainage bag lower than your kidney to keep urine from backing up.
- If you have been instructed that you can reuse your bag, you can clean the bag after removing it from the tube. Use another container to collect your urine while you clean the bag. To clean the bag, fill it with 2 parts vinegar to 3 parts water, and let it stand for 20 minutes. Then empty it out, and let it air dry.
- Empty the drainage bag before it is completely full or every 2 to 3 hours.
- Do not swim or take baths while you have a nephrostomy tube. You can shower after wrapping the end of the nephrostomy tube with plastic wrap.
- Change the dressing around the nephrostomy tube about every 3 days or when it gets wet or dirty. A nurse will teach you how to change the dressing.
Over time, urine crystal deposition can lead to encrustation and tube obstruction. This occurs to a variable degree in each patient and is not significantly affected by frequency of catheter flushing between tube exchanges. Only improved hydration has been shown to reduce the encrustation rate. To prevent silent tube obstruction, routine nephrostomy exchange every 3 months is recommended 23.
Occasionally, catheters can become dislodged. The incidence ranges from less than 1% in the early postplacement period to 11 to 30% in the subsequent months 24. If nephrostomy tubes are dislodged or obstructed, patients are scheduled for replacement during normal daytime working hours unless they develop recurrent fever and flank pain, in which case they are instructed to report to the emergency room. Emergent nephrostomy tube replacement may be necessary when the clinical situation suggests an infected, obstructed system.
When you no longer needs the nephrostomy tube, you will not need another general anaesthetic in order to take it out. The nephrostomy tube is usually removed at you bedside and a bandage is put over the site. This does not take long and should not hurt. You will not need any stitches.
See your doctor now or seek immediate medical care if:
- You have new or worse symptoms of a kidney infection. These may include:
- Pain or burning when you urinate.
- A frequent need to urinate without being able to pass much urine.
- Pain in the flank, which is just below the rib cage and above the waist on either side of the back.
- Blood in the urine.
- A fever.
- You are vomiting or nauseated.
- Your tube leaks.
- Urine does not collect in the drainage bag.
- You have pain or bleeding around the tube.
Watch closely for changes in your health, and be sure to contact your doctor if:
- You do not get better as expected.
- Pabon-Ramos WM, Dariushnia SR, Walker TG, d’Othée BJ, Ganguli S, Midia M, Siddiqi N, Kalva SP, Nikolic B., Society of Interventional Radiology Standards of Practice Committee. Quality Improvement Guidelines for Percutaneous Nephrostomy. J Vasc Interv Radiol. 2016 Mar;27(3):410-4.[↩]
- Degirmenci T, Gunlusoy B, Kozacioglu Z, Arslan M, Ceylan Y, Ors B, Minareci S. Utilization of a modified Clavien Classification System in reporting complications after ultrasound-guided percutaneous nephrostomy tube placement: comparison to standard Society of Interventional Radiology practice guidelines. Urology. 2013 Jun;81(6):1161-7.[↩][↩][↩]
- Young M, Leslie SW. Percutaneous Nephrostomy. [Updated 2019 Jun 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK493205[↩]
- Ramchandani P, Cardella JF, Grassi CJ, Roberts AC, Sacks D, Schwartzberg MS, Lewis CA., Society of Interventional Radiology Standards of Practice Committee. Quality improvement guidelines for percutaneous nephrostomy. J Vasc Interv Radiol. 2003 Sep;14(9 Pt 2):S277-81.[↩][↩][↩]
- Sacks SH, Aparicio SA, Bevan A, Oliver DO, Will EJ, Davison AM. Late renal failure due to prostatic outflow obstruction: a preventable disease. BMJ. 1989 Jan 21;298(6667):156-9.[↩]
- Dagli M, Ramchandani P. Percutaneous nephrostomy: technical aspects and indications. Semin Intervent Radiol. 2011 Dec;28(4):424-37.[↩][↩][↩]
- Ramsey S, Robertson A, Ablett MJ, Meddings RN, Hollins GW, Little B. Evidence-based drainage of infected hydronephrosis secondary to ureteric calculi. J. Endourol. 2010 Feb;24(2):185-9.[↩]
- Bird VG, Fallon B, Winfield HN. Practice patterns in the treatment of large renal stones. J. Endourol. 2003 Aug;17(6):355-63.[↩]
- Rivera ME, McAlvany KL, Brinton TS, Gettman MT, Krambeck AE. Anesthetic exposure in the treatment of symptomatic urinary calculi in pregnant women. Urology. 2014 Dec;84(6):1275-8.[↩]
- Zagoria RJ, Hodge RG, Dyer RB, Routh WD. Percutaneous nephrostomy for treatment of intractable hemorrhagic cystitis. J. Urol. 1993 Jun;149(6):1449-51.[↩]
- Hyams ES, Winer AG, Shah O. Retrograde ureteral and renal access in patients with urinary diversion. Urology. 2009 Jul;74(1):47-50.[↩]
- Patel IJ, Davidson JC, Nikolic B, Salazar GM, Schwartzberg MS, Walker TG, Saad WE., Standards of Practice Committee, with Cardiovascular and Interventional Radiological Society of Europe (CIRSE) Endorsement. Standards of Practice Committee of the Society of Interventional Radiology. Addendum of newer anticoagulants to the SIR consensus guideline. J Vasc Interv Radiol. 2013 May;24(5):641-5.[↩][↩]
- Cohn S.L. (2011) Perioperative Medication Management. In: Cohn S. (eds) Perioperative Medicine. Springer, London https://doi.org/10.1007/978-0-85729-498-2_3[↩]
- Venkatesan AM, Kundu S, Sacks D, Wallace MJ, Wojak JC, Rose SC, Clark TW, d’Othee BJ, Itkin M, Jones RS, Miller DL, Owens CA, Rajan DK, Stokes LS, Swan TL, Towbin RB, Cardella JF., Society of Interventional Radiology Standards of Practice Committee. Practice guidelines for adult antibiotic prophylaxis during vascular and interventional radiology procedures. Written by the Standards of Practice Committee for the Society of Interventional Radiology and Endorsed by the Cardiovascular Interventional Radiological Society of Europe and Canadian Interventional Radiology Association [corrected]. J Vasc Interv Radiol. 2010 Nov;21(11):1611-30; quiz 1631.[↩]
- Wolf JS, Bennett CJ, Dmochowski RR, Hollenbeck BK, Pearle MS, Schaeffer AJ., Urologic Surgery Antimicrobial Prophylaxis Best Practice Policy Panel. Best practice policy statement on urologic surgery antimicrobial prophylaxis. J. Urol. 2008 Apr;179(4):1379-90.[↩]
- Kumar S, Bag S, Ganesamoni R, Mandal AK, Taneja N, Singh SK. Risk factors for urosepsis following percutaneous nephrolithotomy: role of 1 week of nitrofurantoin in reducing the risk of urosepsis. Urol. Res. 2012 Feb;40(1):79-86.[↩]
- Bag S, Kumar S, Taneja N, Sharma V, Mandal AK, Singh SK. One week of nitrofurantoin before percutaneous nephrolithotomy significantly reduces upper tract infection and urosepsis: a prospective controlled study. Urology. 2011 Jan;77(1):45-9.[↩]
- Hopper KD, Sherman JL, Luethke JM, Ghaed N. The retrorenal colon in the supine and prone patient. Radiology. 1987 Feb;162(2):443-6.[↩]
- Clark TW, Abraham RJ, Flemming BK. Is routine micropuncture access necessary for percutaneous nephrostomy? A randomized trial. Can Assoc Radiol J. 2002 Apr;53(2):87-91.[↩]
- ((Degirmenci T, Gunlusoy B, Kozacioglu Z, Arslan M, Ceylan Y, Ors B, Minareci S. Utilization of a modified Clavien Classification System in reporting complications after ultrasound-guided percutaneous nephrostomy tube placement: comparison to standard Society of Interventional Radiology practice guidelines. Urology. 2013 Jun;81(6):1161-7.[↩]
- Chalmers N, Jones K, Drinkwater K, Uberoi R, Tawn J. The UK nephrostomy audit. Can a voluntary registry produce robust performance data? Clin Radiol. 2008 Aug;63(8):888-94.[↩]
- Szvalb AD, El Haddad H, Rolston KV, Sabir SH, Jiang Y, Raad II, Viola GM. Risk factors for recurrent percutaneous nephrostomy catheter-related infections. Infection. 2019 Apr;47(2):239-245.[↩]
- Dagli M, Ramchandani P. Percutaneous nephrostomy: technical aspects and indications. Semin Intervent Radiol. 2011;28(4):424–437. doi:10.1055/s-0031-1296085 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3312169[↩]
- Farrell T A, Hicks M E. A review of radiologically guided percutaneous nephrostomies in 303 patients. J Vasc Interv Radiol. 1997;8(5):769–774.[↩]





{kind=link}