What is SIADH
SIADH is short for syndrome of inappropriate antidiuretic hormone secretion also called syndrome of inappropriate antidiuresis (SIAD), is a condition in which your body makes too much antidiuretic hormone (ADH) also called vasopressin (arginine vasopressin or AVP) from the pituitary gland or nonpituitary sources such as lung cancer despite normal or increased plasma volume 1, 2, 3, 4. Antidiuretic hormone (ADH) is naturally produced in an area of your brain called the hypothalamus (anterior hypothalamus). Antidiuretic hormone (ADH) is then stored and released by the posterior pituitary gland at the base of your brain. Antidiuretic hormone (ADH) helps your kidneys control the amount of water your body loses through the urine. When antidiuretic hormone (ADH) is released by the posterior pituitary gland at the base of your brain more water is reabsorbed from the distal and collecting tubule in your kidneys; it increases water reabsorption and leads to concentrated urine and more water in the blood circulation. SIADH (syndrome of inappropriate antidiuretic hormone secretion) causes your body to retain too much water, resulting in low blood sodium also called hyponatremia (ie, serum sodium [Na+] less than 135 mmol/L) with serum hypo-osmolality (a condition where the levels of electrolytes, proteins, and nutrients in your blood are lower than normal, serum osmolality < 280 mOsm/kg) and high urine osmolality (a condition where the levels of electrolytes, proteins, and nutrients in your urine are higher than normal) which are the hallmark of SIADH 1.
Sodium (Na+) is an electrolyte (mineral). Sodium (Na+) is very important for maintaining your blood pressure. Sodium is also needed for nerves, muscles, and other body tissues to work properly. A normal blood sodium level is between 136 and 145 millimoles per liter (mmol/L). When the amount of sodium in fluids outside cells drops below normal such as in hyponatremia (serum sodium [Na+] less than 135 mmol/L), water moves into the cells. This causes the cells to swell with too much water. Brain cells are especially sensitive to swelling, and this causes many of the symptoms of low blood sodium (hyponatremia).
Hyponatremia signs and symptoms may include:
- Nausea and vomiting
- Headache
- Problems with balance that may result in falls
- Mental changes, such as confusion, memory problems, strange behavior
- Loss of energy, drowsiness and fatigue
- Restlessness and irritability
- Muscle weakness, spasms or cramps
- Seizures or coma in severe cases.
With SIADH not enough water is excreted in your urine resulting in very concentrated urine and there is too much water in your blood. This dilutes many substances in the blood such as sodium (hyponatremia). A low blood sodium level (hyponatremia) is the most common cause of symptoms of too much ADH. It is also the most common clue that a person may have SIADH.
When your body’s sodium level drops too much (hyponatremia), it can be a life-threatening emergency. Contact your doctor right away if you have symptoms of SIADH.
The first published cases of SIADH were 2 patients with lung cancer with hyponatremia, yet ongoing renal sodium loss, described by Schwartz et al in 1957 4. They developed the classic Schwartz and Bartter criteria for the diagnosis of SIADH, which has not changed. SIADH is characterized by impaired water excretion leading to hyponatremia with fluid overload (hypervolemia) or normal volume of fluids in the body (euvolemia) 5, 6, 7.
The incidence of SIADH increases with age but, recently, a higher incidence of SIADH has been reported in children 2. Children and older adults are more hyponatremic, particularly when hospitalized for lung and central nervous system (brain and spinal cord) infections like pneumonia or meningitis. SIADH is also more common in hospitalized, post-operative patients due to the administration of hypotonic fluids, drugs, and the body’s response to stress 2.
SIADH treatment depends on the cause of the problem. For example, surgery is done to remove a tumor producing ADH. Or, if a medicine is the cause, its dosage may be changed or another medicine may be tried.
In all cases, the first step is to limit fluid intake. This helps prevent excess fluid from building up in the body. Your doctor will tell you what your total daily fluid intake should be. The restriction is not just for water, but for almost all fluids (coffee, tea, juice, soda, etc.).
If you have severe symptoms, it is a medical emergency. This is usually treated with salt solution (3% saline) given through an IV into the veins (intravenous) in the hospital.
Medicines may be needed to block the effects of ADH on the kidneys so that excess water is excreted by the kidneys. These medicines may be given as pills or as injections given into the veins.
Figure 1. Antidiuretic hormone (ADH) production
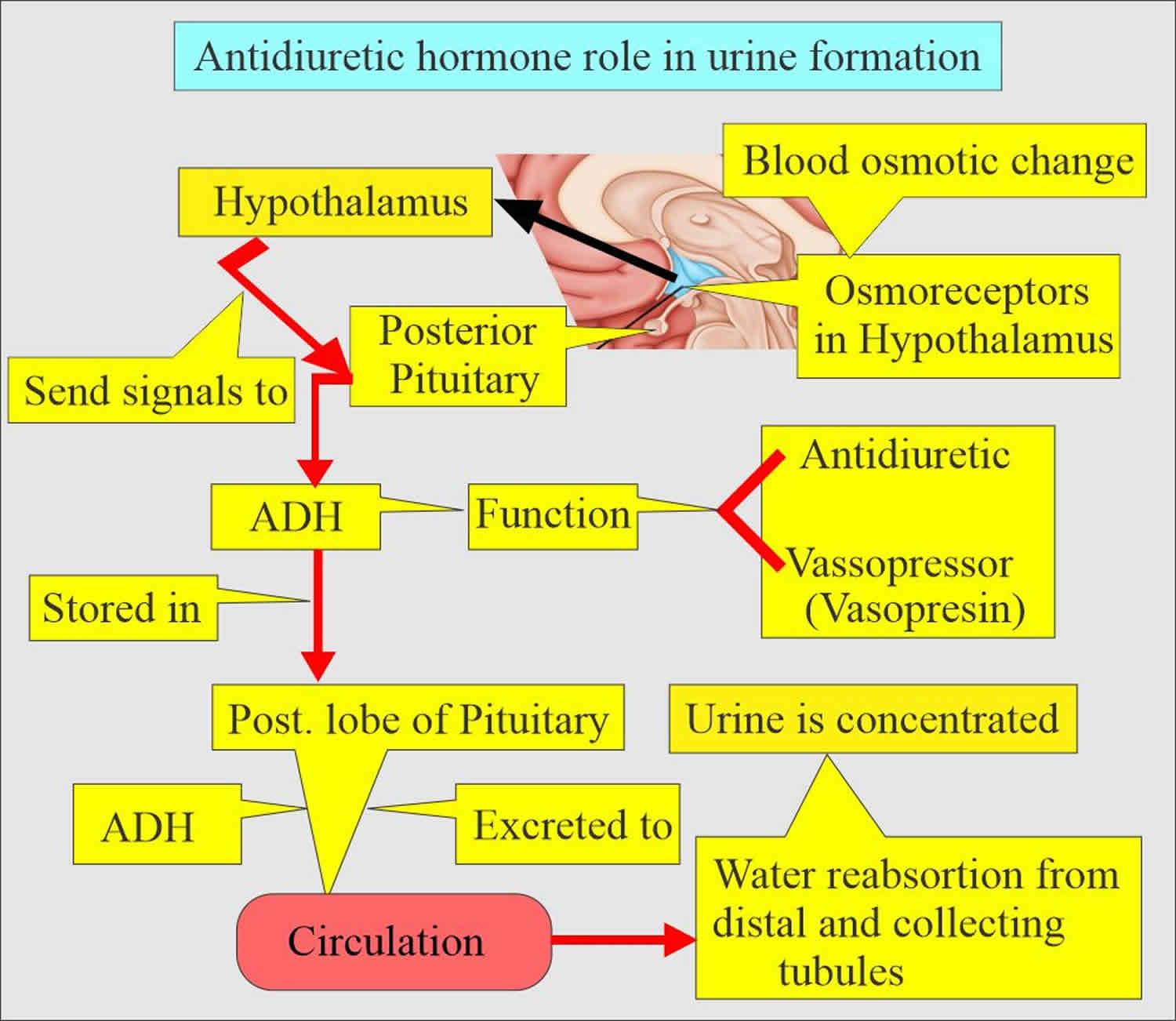
Figure 2. Antidiuretic hormone (ADH) or arginine vasopressin (AVP) action at kidney V2 receptors
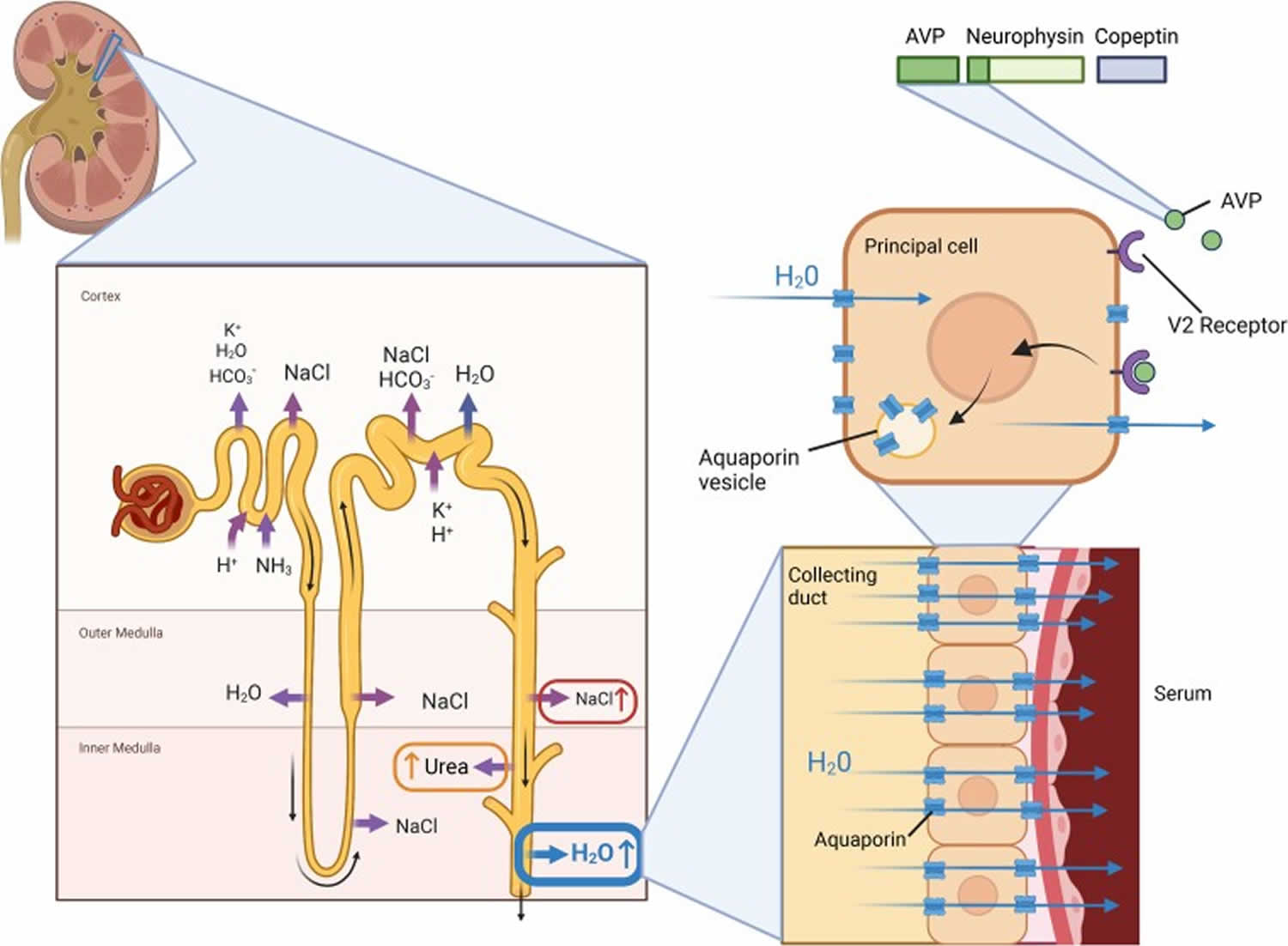
Footnotes: Antidiuretic hormone (ADH) or arginine vasopressin (AVP) interacts with the vasopressin V2 receptor on the principal cells of the renal collecting duct. When the G protein-coupled receptor V2 receptor is activated, cyclic adenosine monophosphate signaling leads to increased synthesis and deployment of aquaporins, which are stored in intracellular vesicles which then merge with the luminal cell wall. Aquaporins allow the resorption of solute-free water out of the filtrate and into serum, resulting in more concentrated urine excretion. Antidiuretic hormone (ADH) or arginine vasopressin (AVP) also acts on epithelial sodium channel (ENaC) urea transporters to increase sodium and urea resorption to increase medullary interstitial osmolality and hence urinary concentrating gradient. Persistent antidiuretic hormone (ADH) or arginine vasopressin (AVP) stimulation “inappropriate” with respect to serum osmolality will lead to excessive water retention and a fall in serum osmolality and serum sodium concentration.
[Source 1 ]Figure 3. Hyponatremia types
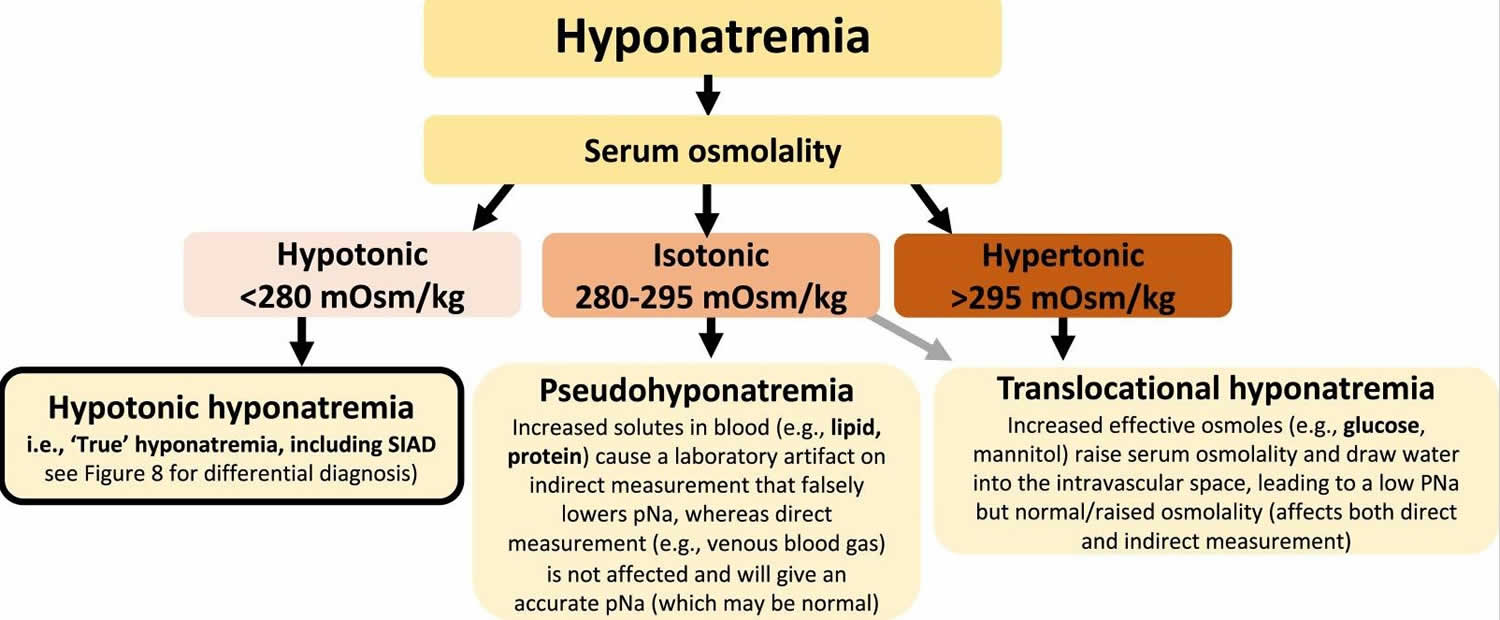
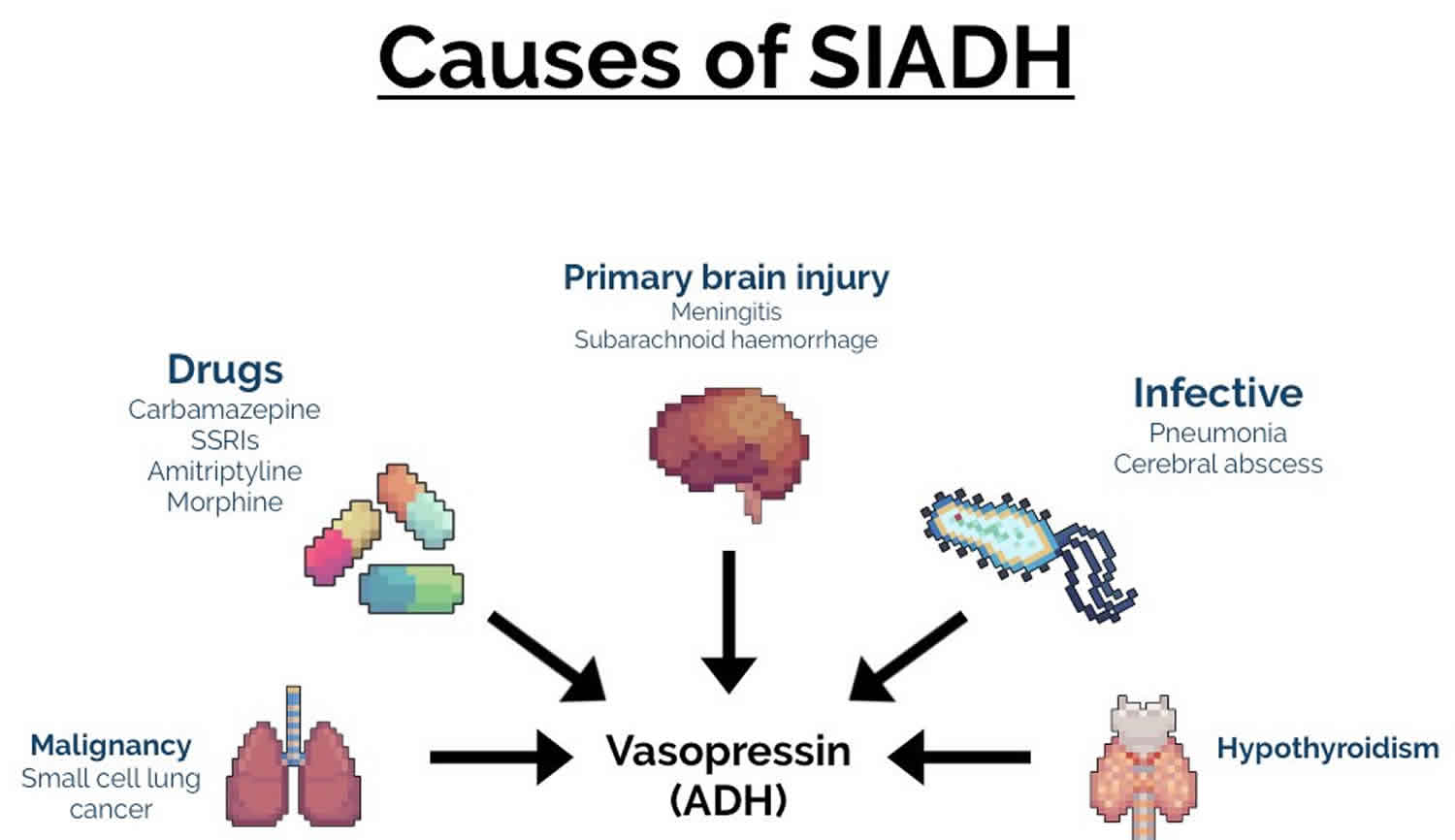
Figure 4. SIADH causes
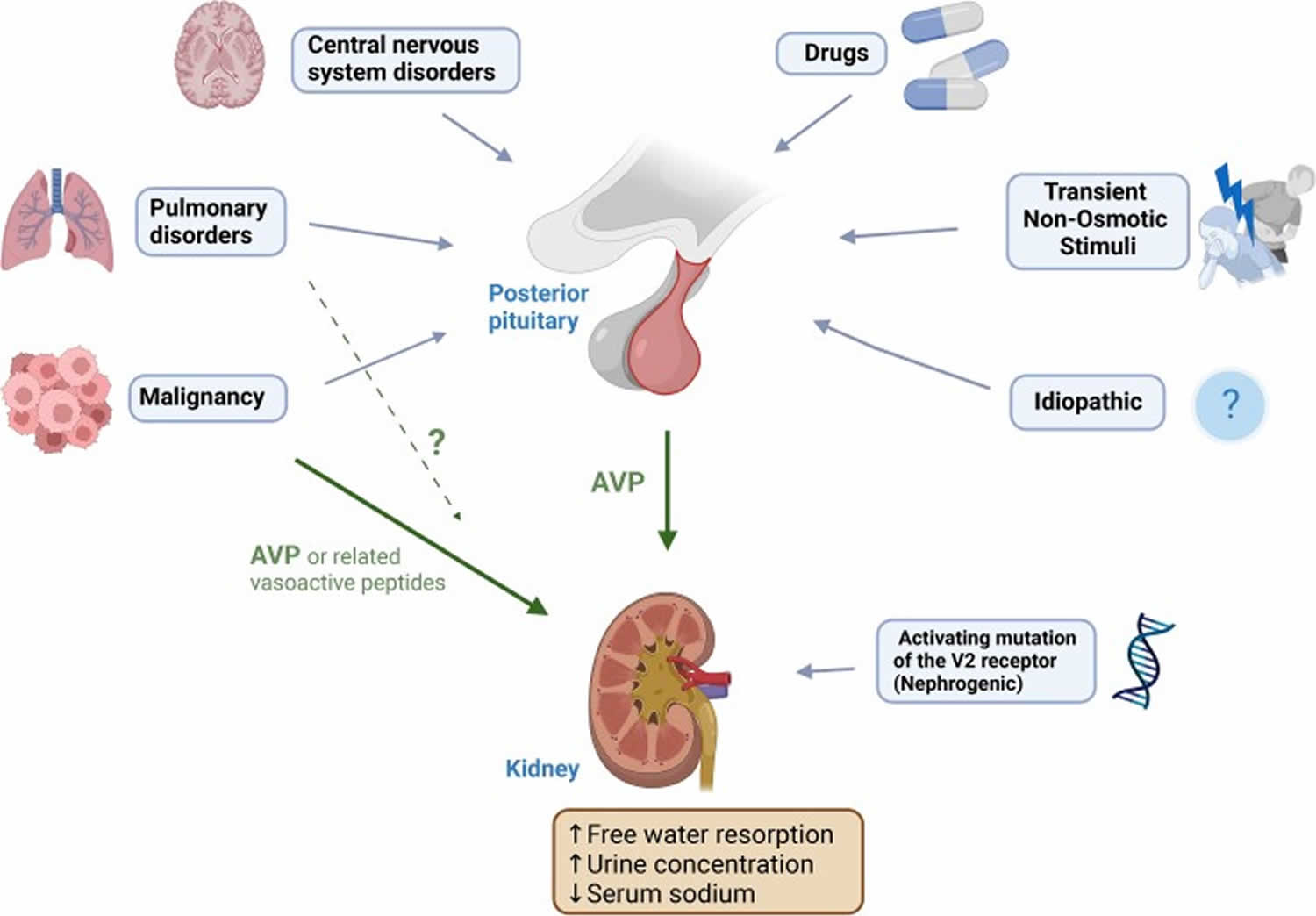
Footnotes: Causes of SIADH. Cancer (solid organ particularly lung and nasopharyngeal, lymphoma). Lung disorders (infection, asthma, cystic fibrosis, respiratory failure). Central nervous system disorders (infection, hemorrhage, thrombosis, trauma, tumour, hydrocephalus, autoimmune (multiple sclerosis, Guillain-Barré syndrome), multiple system atrophy, delirium tremens). Transient stimuli (nausea, pain, stress, prolonged endurance exercise, general anesthesia, pituitary surgery). Drugs. Idiopathic (“reset osmostat,” cause not yet apparent). Hereditary (nephrogenic SIAD).
Abbreviation: AVP = arginine vasopressin.
[Source 1 ]Figure 5. Acute vs chronic onset of hyponatremia
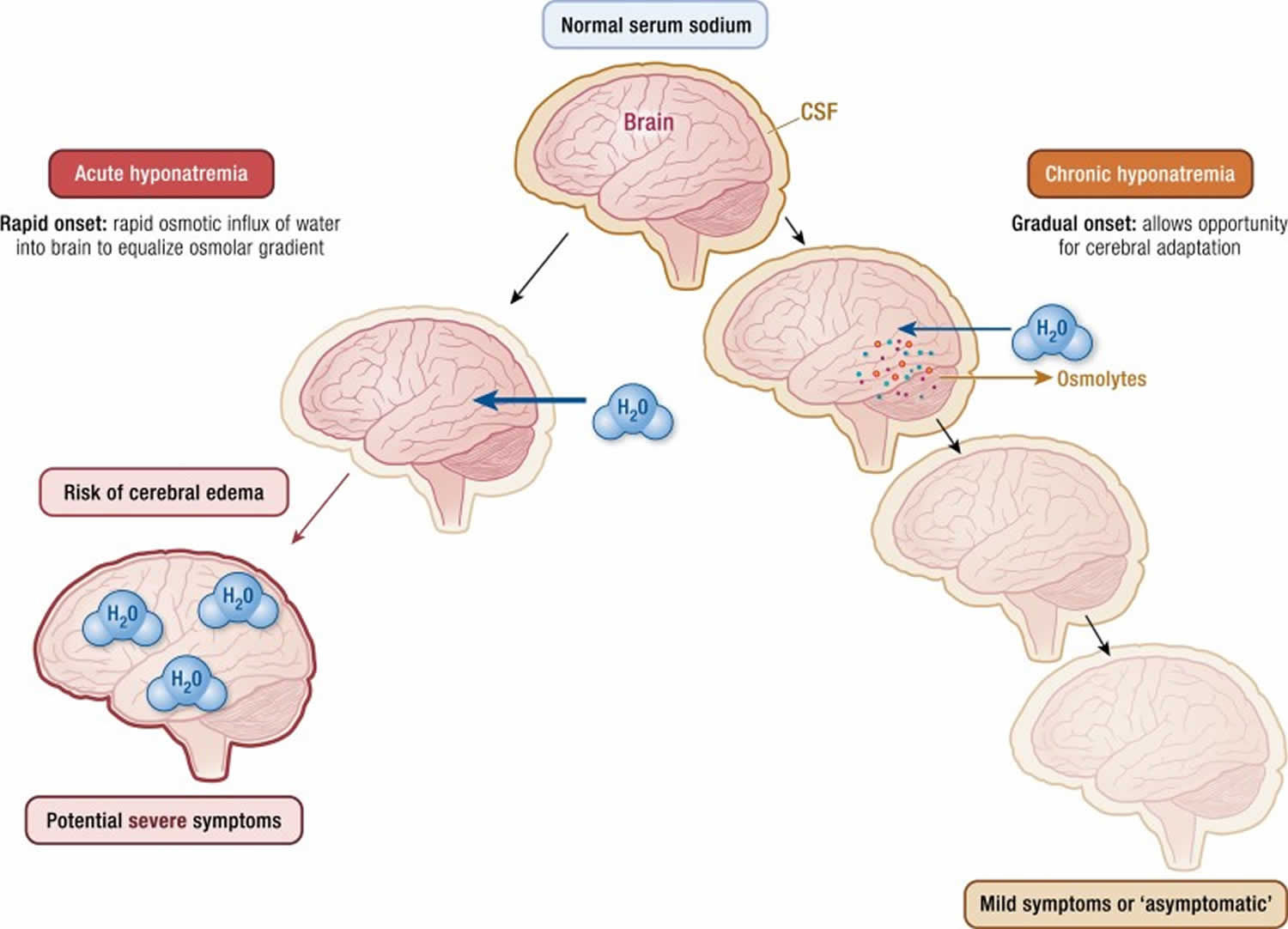
Footnotes: Schematic diagram of the development of acute vs chronic onset of hyponatremia, explaining typical difference in symptom severity. Intensity of shading is a visual representation of osmolality. Acute hyponatremia results in relatively hypotonic serum/cerebrospinal fluid (CSF) compared to brain tissue, leading to osmotic influx of water into glial cells to equalise osmolar gradient, which may cause cerebral edema and potential seizure, coma, and death. Chronic hyponatremia often occurs more gradually. As serum/CSF osmolality falls, water enters the brain more slowly and is matched by export or deactivation of brain osmolytes including sodium, potassium, and organic osmolytes (eg, myoinositol, glycerophosphorylcholine, creatine, glutamate, glutamine, taurine) to equalize the osmolar gradient (116). The resulting hypotonic brain is vulnerable to rapid correction if the reverse process happens too rapidly, which may cause osmotic demyelination syndrome or central pontine myelinolysis (CPM).
[Source 1 ]What is the function of antidiuretic hormone (ADH)?
Antidiuretic hormone (ADH) also called vasopressin (arginine vasopressin or AVP) main function is to help control the body’s water balance or osmoregulation. Osmoregulation is the process of maintaining salt and water balance (osmotic balance) across membranes within the body. Normally, when a person’s fluid intake is low or when a lot of fluid is lost (for example, through sweating), the posterior pituitary gland releases more ADH into the bloodstream. High levels of antidiuretic hormone (ADH) direct the kidneys to reabsorb more water and to make less urine. When fluid intake is adequate, the pituitary gland releases less ADH. Lower levels of antidiuretic hormone (ADH) cause the kidneys to reabsorb less water and to make more urine.
Osmoreceptors detect the change in effective plasma osmolality in the hypothalamus. A decrease in tonicity prevents ADH release and prevents water retention. An increase in tonicity causes ADH release, which acts on V2 receptors on the luminal surface of cortical and medullary collecting tubular cells. Under the influence of ADH, unique aquaporin-2 water channels are formed by the fusion of pre-formed cytoplasmic vesicles in the tubular cells, and water is absorbed down the concentration gradient. Once the water is absorbed, these channels are removed by endocytosis and returned to the cytoplasm. The osmoreceptors are extremely sensitive, responding to alterations in the plasma tonicity of as little as 1% 9. The osmotic threshold for ADH release in humans is about 280 to 290 mOsmol/kg. There is little circulating ADH below this level, and the urine should be maximally diluted with an osmolality below 100 mOsmol/kg. Above the osmotic threshold, there is a relatively linear rise in ADH secretion. This system is so efficient that the plasma osmolality does not typically vary by more than 1% to 2%, despite wide water intake fluctuations 10.
In patients with SIADH, levels of ADH are high even in the presence of decreased plasma osmolality and/or hyponatremia. Excess water absorption keeps the blood volume high or normal.
An acute drop in blood pressure as sensed by ” volume receptors” rather than “osmoreceptors” causes ADH release (along with other hormones like rennin and epinephrine), which generates free water absorption from the kidneys. This can potentially lead to hyponatremia and a decrease in effective extracellular fluid (ECF) osmolality. So, the main focus in rapid and/or substantial decrease in blood volume is “volume regulation,” even at the cost of osmolality. This effect is more prominent in patients with liver disease or cardiac disease, and hyponatremia in such patients is the direct predictor of a worse prognosis 11.
SIADH causes
SIADH is most often caused by either inappropriate hypersecretion of ADH from its normal hypothalamic source or by ectopic production. Most commonly, SIADH occurs secondary to another disease process elsewhere in your body. Common causes of SIADH (syndrome of inappropriate antidiuretic hormone secretion) include:
- Medicines. A number of drugs associated with SIADH act by enhancing the release or effect of ADH. The most common drugs include carbamazepine, oxcarbazepine, chlorpropamide, cyclophosphamide, and selective serotonin reuptake inhibitors (SSRI). Carbamazepine and oxcarbazepine act in part by increasing the sensitivity to ADH. Chlorpropamide increases the number of V2 receptors in collecting tubules. As high-dose intravenous cyclophosphamide is given with a fluid load to prevent hemorrhagic cystitis, SIADH in such patients is a particular problem, leading to potentially fatal hyponatremia. SSRIs cause SIADH by an unknown mechanism, but people above 65 years of age are more at risk. “Ecstasy” (methylenedioxymethamphetamine), a drug of abuse, is particularly associated with the direct release of ADH. (It also stimulates thirst, which further worsens hyponatremia.) Less commonly, non-steroidal anti-inflammatory drugs (NSAIDs), opiates, interferons, methotrexate, vincristine, vinblastine, ciprofloxacin, haloperidol, and high dose imatinib have been linked with SIADH.
- Surgery under general anesthesia. Surgical procedures are often associated with hypersecretion of ADH, a response that is probably mediated by pain afferents 12.
- Any central nervous system (CNS) abnormality can enhance ADH-release from the pituitary gland, leading to SIADH. Central nervous system disorders include stroke, hemorrhage, infection, trauma, mental illness, and psychosis.
- Brain surgery in the region of the hypothalamus
- Tuberculosis, cancer, chronic infections, and lung disease, such as pneumonia
- Pulmonary diseases, particularly pneumonia (viral, bacterial, tuberculous), can lead to SIADH by unknown mechanisms. A similar response has infrequently been seen in patients with asthma, atelectasis, acute respiratory failure, and pneumothorax.
- Substance use disorder
Rare causes of SIADH (syndrome of inappropriate antidiuretic hormone secretion) include:
- Rare diseases of the hypothalamus or pituitary
- Leukemia and ectopic production of the ADH, like carcinoma of the lung, cancer of the small intestine, thymus, lymphoma, carcinoma of the pancreas and brain cancer. Small cell lung cancer (SCLC) is the most common tumor leading to ectopic ADH production. Less commonly, extrapulmonary small cell carcinomas, head and neck cancers, and olfactory neuroblastomas also cause ectopic ADH release.
- Mental disorders
- Hormone deficiency: Both hypopituitarism and hypothyroidism may be accompanied by hyponatremia and a SIADH picture that can be corrected by hormone replacement.
- Hormone administration: SIADH can be induced by exogenous hormone administration, as with vasopressin (to control gastrointestinal bleeding), desmopressin (dDAVP, to treat von Willebrand disease, hemophilia, or platelet dysfunction), and oxytocin (to induce labor). All three act by increasing the activity of the vasopressin-2 (V2; antidiuretic) receptors.
- Human Immunodeficiency Virus (HIV) infection: A common laboratory manifestation seen in HIV infection, either with the acquired immune deficiency syndrome (AIDS) or early symptomatic HIV infection, is hyponatremia. It can be due to SIADH, or it can be due to volume depletion, secondary to adrenal insufficiency or gastrointestinal losses. Pneumonia, due to Pneumocystis carinii or other organisms and central nervous system infections by opportunistic pathogens, is also responsible for SIADH 13.
- Hereditary SIADH, also known as nephrogenic SIADH, has been ascribed to the gain of function mutation in vasopressin 2 (V2) receptors in the kidneys 14. A gain of function mutation in the AVPR2 gene that encodes the V2 receptor (located on the X chromosome) is responsible for hereditary SIADH. The AVPR2 gene mutation leads to constant activation of the V2 receptors in the renal collecting duct, leading to excessive water absorption and hyponatremia resembling chronic SIADH, which in turn is resistant to vasopressin receptor antagonists. Overt cases present in infancy and can be associated with severe cerebral edema. There is high phenotypic variability, however, with some cases minimally symptomatic and diagnosed only after challenge with a water load 15. Genetic testing in patients with SIADH is infrequent, hence the proportion of nephrogenic SIADH is unknown, but it is estimated to affect fewer than 1 per million population. A low serum copeptin concentration (eg, < 2.0 pmol/L, with low serum sodium and osmolality) may provide a clue to this diagnosis and prompt genetic testing 16.
Central nervous system disorders
Central nervous system (brain and spinal cord) disorders causing SIADH include:
- Acute psychosis
- Acute intermittent porphyria
- Brain abscess
- Cavernous sinus thrombosis
- Cerebellar and cerebral atrophy
- Cerebrovascular accident
- Central nervous system lupus
- Delirium tremens
- Encephalitis (viral or bacterial)
- Epilepsy
- Guillain-Barré syndrome
- Head trauma
- Herpes zoster (chest wall)
- Hydrocephalus
- Hypoxic ischemic encephalopathy
- Meningitis (viral, bacterial, tuberculous, and fungal)
- Midfacial hypoplasia
- Multiple sclerosis
- Perinatal hypoxia
- Rocky Mountain spotted fever
- Schizophrenia
- Shy-Drager syndrome
- Subarachnoid hemorrhage
- Subdural hematoma
- Ventriculoatrial shunt obstruction
- Wernicke encephalopathy
Medications
Medications are a common cause of SIADH 17, 18. The list of drugs that can induce SIADH is long. However, a study of 146 cases of drug‐associated SIADH found that the following five drug classes were implicated in 82.3% of patients 19:
- Antidepressants (eg, citalopram, escitalopram, venlafaxine, amitriptyline)
- Anticonvulsants (eg, carbamazepine, phenytoin, valproate)
- Antipsychotic agents (eg, risperidone, haloperidol, quetiapine)
- Cytotoxic agents (eg, vincristine, cyclophosphamide, cisplatin, ifosfamide)
- Pain medications (eg, duloxetine, pregabalin, tramadol)
Many chemotherapeutic drugs cause nausea, which is a powerful stimulus of ADH release or vasopressin secretion. SIADH is also a leading cause of hyponatremia in children following chemotherapy or stem cell transplantation.
Drugs that stimulate ADH release (AVP release) are as follows:
- Acetylcholine
- Chemotherapy agents – Adenine arabinoside, cyclophosphamide, ifosfamide, vincristine, vinblastine
- Barbiturates
- Bromocriptine
- Carbachol
- Chlorpropamide
- Clofibrate
- Cyclopropane
- Dibenzazepines (eg, carbamazepine, oxcarbazepine)
- Halothane
- Haloperidol
- Histamine
- Isoproterenol
- Lorcainide
- Opiates (eg, morphine)
- Nicotine (inhaled tobacco smoke)
- Nitrous oxide
- Phenothiazines (eg, thioridazine)
- Thiopental
- Monoamine oxidase inhibitors (eg, tranylcypromine)
- Tricyclic antidepressants (eg, amitriptyline, desipramine)
Drugs that potentiate the effects of ADH action (primarily facilitate peripheral action of ADH) are as follows:
- Clofibrate
- Griseofulvin
- Hypoglycemic agents – Metformin, phenformin, tolbutamide
- Oxytocin (large doses)
- Prostaglandin synthetase inhibitors (inhibit renal PGE 2 synthesis) – Indomethacin, aspirin, nonsteroidal anti-inflammatory drugs
- Theophylline
- Triiodothyronine
- Vasopressin analogs (eg, AVP, DDAVP)
Drugs with an uncertain mechanism are as follows:
- Amiodarone 20
- Antineoplastic agents – Cisplatin, melphalan, methotrexate, imatinib
- Ciprofloxacin
- Clomipramine
- 3,4-methylenedioxymethamphetamine (MDMA; ecstasy)
- Phenoxybenzamine
- Antiepilepsy drugs – Sodium valproate, lamotrigine, levetiracetam, gabapentin
- Selective serotonin reuptake inhibitors (SSRIs; eg, sertraline, fluoxetine, paroxetine)
- Thiothixene
Cancer
Neoplastic disorders causing SIADH include:
- Pulmonary – Lung carcinoma and mesothelioma
- Gastrointestinal – Carcinomas of the duodenum, pancreas, and colon
- Genitourinary – Adrenocortical carcinoma; carcinomas of cervix, ureter/bladder, and prostate; and ovarian tumors
- Other – Brain tumors, carcinoid tumors, Ewing sarcoma, leukemia, lymphoma, nasopharyngeal carcinoma, neuroblastoma (olfactory), and thymoma
Lung disorders
Pulmonary disorders causing SIADH include:
- Acute bronchitis/bronchiolitis
- Acute respiratory failure
- Aspergillosis (cavitary lesions)
- Asthma
- Atelectasis
- Bacterial pneumonia
- Chronic obstructive lung disease
- Cystic fibrosis
- Emphysema
- Empyema
- Pneumonia (viral including COVID-19, bacterial [mycoplasmal], fungal)
- Pneumothorax
- Positive pressure ventilation
- Pulmonary abscess
- Pulmonary fibrosis
- Sarcoidosis
- Tuberculosis
- Viral pneumonia
Miscellaneous causes
Miscellaneous causes causing SIADH include:
- Giant cell arteritis
- HIV infection – Hyponatremia has been reported in as many as 40% of adult patients with HIV infection. Patients with acquired immunodeficiency syndrome (AIDS) can have many potential causes for increased ADH secretion, including volume depletion and infection of the lungs and the central nervous system 13. Although one third of the hyponatremic patients with AIDS are clinically hypovolemic, the remaining hyponatremic patients fulfill most of the criteria for SIADH.
SIADH signs and symptoms
SIADH signs and symptoms can be due to hyponatremia and decreased extracellular fluid (ECF) osmolality, which causes the water to move into the cells causing cerebral edema 2. SIADH signs and symptoms depend upon the rate and severity of hyponatremia and the degree of cerebral edema. Often, there are no symptoms from a mildly low sodium level. More symptoms occur the lower the level of the sodium.
When symptoms do occur, low blood sodium (hyponatremia) may include any of the following:
- Nausea and vomiting
- Headache
- Problems with balance that may result in falls
- Mental changes, such as confusion, memory problems, strange behavior
- Loss of energy, drowsiness and fatigue
- Restlessness and irritability
- Muscle weakness, spasms or cramps
- Seizures or coma in severe cases.
The earliest signs and symptoms of acute hyponatremia include nausea and malaise, which may be seen when the serum sodium concentration falls below 125 to 130 mmol/L (normal 135 to 145 mmol/L) 2. Vomiting is an ominous sign for patients with acute hyponatremia. With a more severe and acute fall in sodium concentration, headache, lethargy, obtundation, and eventually, seizures can occur. Coma and respiratory arrest can occur if the serum sodium level falls below 115 to 120 mmol/L. Acute hyponatremia encephalopathy may be reversible, but permanent neurologic damage or death can occur, particularly in premenopausal women.
Chronic hyponatremia allows brain adaptation, and the patients remain asymptomatic despite a serum sodium concentration below 120 mmol/L. Nonspecific symptoms like nausea, vomiting, gait disturbances, memory, cognitive problems, fatigue, dizziness, confusion, and muscle cramps can occur with chronic hyponatremia. Sign and symptoms or mild and chronic hyponatremia are often subtle and missed during the history and physical examination. Nausea and vomiting affect approximately one-third of patients with chronic hyponatremia who have a serum sodium concentration of less than 120 mmol/L.
Idiopathic SIADH is more common in patients over 65 years of age, and mild to moderate hyponatremia in such patients may contribute to fractures in addition to a higher risk of falls and gait problems.
SIADH complications
In severe cases, low sodium can lead to:
- Decreased consciousness, hallucinations or coma
- Brain herniation
- Death
Low sodium that occurs rapidly, in less than 48 hours (acute hyponatremia), is more dangerous than low sodium that develops slowly over time. In acute hyponatremia, sodium levels drop rapidly — resulting in potentially dangerous effects, such as rapid brain swelling, which can result in a coma and death. When the sodium level falls slowly over days or weeks (chronic hyponatremia), the brain cells have time to adjust and the acute symptoms such as brain swelling don’t occur. Chronic hyponatremia is associated with nervous system problems such as poor balance and poor memory. Rapid correction of chronic hyponatremia can also cause dangerous complications called osmotic demyelination syndrome or central pontine myelinolysis (CPM) 21, 22. Central pontine myelinolysis (CPM) is the feared complication of excessive, overly rapid correction of hyponatremia. Typical features are disorders of upper motor neurons, including spastic quadriparesis and pseudobulbar palsy, as well as mental disorders ranging from confusion to coma 23. The risk is increased in persons with liver failure, potassium depletion, large burns, and malnutrition 17. Premenopausal women appear to be at the greatest risk of hyponatremia-related brain damage. Premenopausal patients undergoing surgery, especially gynecologic or related procedures, and those with serum sodium of less than 105 mmol/L may also have an increased risk. This may be related to the effect of women’s sex hormones on the body’s ability to balance sodium levels. Once central pontine myelinolysis (CPM) occurs as a complication, there is no proven treatment.
SIADH diagnosis
Your doctor will start by asking about your medical history and will perform a complete physical examination to help determine the cause of your symptoms. Establishing fluid status (dehydration, volume overload, normal volume) is an important part of making the correct diagnosis.
Because the signs and symptoms of hyponatremia occur in many conditions, it’s impossible to diagnose the condition based on a physical exam alone. There is no single best test to diagnose SIADH. To confirm low blood sodium, your doctor will order blood tests and urine tests.
Lab tests that can confirm and help diagnose low sodium include:
- Comprehensive metabolic panel (includes blood sodium)
- Serum osmolality and serum sodium
- Urine sodium concentration and osmolality
- Urine potassium
- Toxicology screens for certain medicines
- Renal function tests: BUN and creatinine
- BSR (Blood sugar random)
- Thyroid profile
- Serum cortisol
- Serum K+, bicarbonate, chloride
- Fasting lipid profile
- Liver function tests
- Lung and brain imaging tests in children suspected of having SIADH
ADH can be measured in the blood, but is difficult to process for many labs and takes up to two weeks to get a result. Serum co-peptin can be used to estimate the ADH level in the blood.
Your doctor must rule out hypothyroidism (underactive thyroid) and adrenal insufficiency before labeling the patient with SIADH. Further tests are required to find out underlying causes according to history. Patients with long-standing smoking history, weight loss, or pulmonary symptoms must have a chest X-ray and CT scan to look for small cell lung cancer (SCLC).
SIADH consists of hyponatremia, inappropriately elevated urine osmolality (greater than 100 mOsm/kg), and decreased serum osmolality in a euvolemic patient. SIADH should be diagnosed when these findings occur in the setting of otherwise normal cardiac, renal, adrenal, hepatic, and thyroid function; in the absence of diuretic therapy; and in absence of other factors known to stimulate ADH secretion, such as hypotension, severe pain, nausea, and stress.
Diagnosis of SIADH and its characteristic features:
- Hyponatremia.
- Continued renal excretion of sodium (Na+) despite the hyponatremia (sodium [Na+] less than 135 mmol/L).
- Serum hyposmolality (serum osmolality less than 280 mOsm/kg)
- Urine osmolality shows a significant degree of concentration instead of what one would expect to have dilute urine.
- No evidence of blood volume depletion.
- There is a normal renal and adrenal function that will differentiate from other causes.
- These criteria will demonstrate that ADH is secreted despite the hemodilution, decreased serum osmolality, or both.
- Most of these patients do not have edema because interstitial fluid expansion is usually moderate in degree.
- The water load test means ADH suppression differentiates the SIADH from the other causes of hyponatremia and/or edematous conditions.
- Measure urine and serum osmolarity.
- Patients with SIADH secrete very little or none of the water overload.
- Urine osmolarity will never be less than 100 mmol/kg
- The urine/serum ratio is greater than 100.
- Measure urine and serum osmolarity.
Schwartz and Bartter Clinical Criterion
Schwartz and Bartter made a clinical criterion in 1967 for diagnosis of SIADH, which is still valid today 24, 25, 26.
- Serum sodium less than 135 mmol/L
- Serum osmolality less than 275 mOsm/kg
- Urine sodium excretion greater than 30 mmol/L with normal salt and water intake
- Urine osmolality greater than 100 mOsm/kg
- Clinical euvolemiaa (absence of signs of hypovolemia or hypervolemia). The absence of clinical evidence of volume depletion – normal skin turgor, blood pressure within the reference range
- The absence of other causes of hyponatremia – adrenal insufficiency, hypothyroidism, cardiac failure, pituitary insufficiency, renal disease with salt wastage, hepatic disease, drugs that impair renal water excretion.
- Normal renal function and absence of diuretic use (particularly thiazide diuretics)
- Correction of hyponatremia by fluid restriction
Renal function tests and random blood sugar tests are necessary to check hyperglycemia and uremia as these are the potential causes of pseudohyponatremia.
SIADH differential diagnoses
The differential diagnoses of SIADH (syndrome of inappropriate antidiuretic hormone secretion) include other hyponatremic conditions, which can be divided into those that cause impairment in urinary water excretion and those in which kidney handling of water is normal 27. All patients with hyponatremia should have a plasma osmolality measured to confirm hypo-osmolality.
Conditions in which kidney water handling is impaired include the following:
- Effective circulating volume depletion – gastrointestinal losses (eg, diarrhea, vomiting), renal losses (eg, diuretic therapy, adrenal insufficiency, primary renal salt wasting), skin losses, edematous disorders (congestive heart failure, cirrhosis with portal hypertension, severe nephrotic syndrome)
- Kidney failure – Acute kidney injury (AKI) or chronic kidney disease (CKD)
- Other states of ADH excess – Cortisol deficiency, hypothyroidism, exogenous ADH (eg, deamino-D-arginine-vasopressin, vasopressin, oxytocin)
Decreased solute intake - Nephrogenic syndrome of inappropriate anti-diuresis (NSIAD)
Disorders with normal water excretion include the following:
- Primary polydipsia
- Reset osmostat
- Cerebral salt wasting
Pseudohyponatremia
Extreme elevations in plasma lipids or proteins can increase the plasma volume and can reduce the measured plasma sodium (Na+) concentration. Sodium (Na+) is contained in the aqueous phase of plasma; the proteins and lipids cause an increase in the nonaqueous phase of plasma, leading to an overall increase in plasma volume without an actual decrease or dilution of sodium (Na+) in the aqueous phase. This was more of an issue in the past in the United States, when the conventional method of measuring sodium (Na+) (ie, flame-emission spectrophotometry) measured the aqueous and nonaqueous phases of plasma. The correction factors are as follows:
- Plasma triglycerides (g/L) x 0.002 = mEq/L decrease in sodium (Na+)
- Plasma protein level – 8 (g/L) x 0.025 = mEq/L decrease in sodium (Na+)
The newer method (using ion-specific Na+ electrodes) measures the sodium (Na+) in the aqueous phase only, thus avoiding the error of pseudohyponatremia. Pseudohyponatremia should be suspected when the measured plasma osmolality is normal in the presence of hyponatremia. Pseudohyponatremia may continue to be a problem in parts of the world where flame photometry is still used to measure sodium (Na+).
Hyperglycemia
Elevated glucose levels decrease the measured serum sodium (Na+) levels by 1.6 mmol/L for every 100 mg/dL increase in glucose. This results from the osmotic effect of glucose drawing water into the intravascular space. Plasma osmolality is high in this situation. This is a form of transient hyponatremia that corrects itself as hyperglycemia is reversed 17. A similar form of hyponatremia can occur with any osmotically active substance in plasma, such as mannitol or dextran.
Exercise-induced hyponatremia
Exercise-induced hyponatremia has been reported during prolonged exercise such as in marathon runners and triathletes, usually in warmer climates, which can lead to severe hyponatremia associated with neurologic symptoms 28. The syndrome appears to arise because of excessive water consumption during the physical exercise coupled with loss of sodium chloride in sweat and nonosmotic stimulation of ADH secretion (from stress, volume contraction, nausea, and nonsteroidal anti-inflammatory drugs [NSAIDs]). A postulated factor is fructose-induced vasopressin secretion, resulting from ingestion of fructose-containing drinks or endogenous fructose production 29.
Some athletes with cerebral edema also develop noncardiogenic pulmonary edema 30.
Cerebral salt wasting
The term cerebral salt wasting was introduced in the 1950s to describe an entity seen with certain cerebral disorders that can impair the ability of the kidneys to conserve sodium (Na+), with resultant salt wasting and polyuria. Cerebral salt wasting is defined as the renal loss of sodium (Na+) with intracranial disease, which leads to hyponatremia and a decrease in extracellular fluid volume 31, 32.
Vasopressin-resistant polyuria with hyponatremia, particularly in the setting of cerebral injury or cerebral disease or when accompanied by dehydration, should prompt consideration of CSW in the differential diagnosis. Cerebral salt wasting must be distinguished from SIADH because management of these 2 conditions differs significantly.
The differences and similarities in findings for cerebral salt wasting and SIADH are itemized as follows:
- Hyponatremia – Present in both cerebral salt wasting and SIADH
- Urine Na – Increased in both cerebral salt wasting and SIADH
- Volume – Reduced in cerebral salt wasting and normal or increased in SIADH
- Salt wasting – Gross in cerebral salt wasting and self-limited in SIADH
- Urine output – Polyuria in cerebral salt wasting and variable in SIADH
- Hypouricemia – Occasional in cerebral salt wasting and frequent in SIADH
Over the years, much debate has been focused on the existence of this entity. The evidence in favor of cerebral salt wasting rests on the following points:
- The presence of a negative salt balance
- The development of volume contraction (by definition, patients with SIADH are euvolemic)
- The fact that patients with cerebral salt wasting respond to salt and volume replacement rather than to fluid restriction
Various mechanisms have been postulated, including the roles of natriuretic peptides and neural regulatory mechanisms. Measurement of ADH or atrial natriuretic peptide levels is not helpful because they have been known to vary even in persons with SIADH.
Cerebral salt wasting is treated with sodium (Na+) replacement, which is diametrically opposite to that for SIADH. Sodium (Na+) administration in persons with cerebral salt wasting corrects the hyponatremia and the fluid loss; however, in patients with SIADH, the effect is temporary. The mineralocorticoid fludrocortisone has been used as part of the treatment of cerebral salt wasting 32.
Adrenal insufficiency
Cortisol has a negative feedback effect on ADH and corticotropin-releasing hormone. The absence of cortisol thus removes this inhibitory effect, increasing the release of ADH.
Kidney disease
With declining kidney function, the ability to excrete free water decreases, and the more advanced the reduction in glomerular filtration rate (GFR), the easier it is for patients to become hyponatremic with unrestricted fluid intake. In patients on long-term dialysis with no urine output, fluid intake no greater than insensible losses leads to a predictable fall in serum Na, which, however, is not sustained because of regular maintenance dialysis.
Reset osmostat
Persons with this entity have a normal response to changes in osmolality, but their threshold for ADH release is reduced. Therefore, they have a lower, but stable, plasma sodium (Na+) concentration. Some individuals probably carry a nonsynonymous polymorphism (P19S) in the transient receptor potential vanilloid 4 (TRPV4) channel, part of the osmoreceptor system, since this mutation has been shown to be associated with hyponatremia 33.
The reset osmostat has been observed in pregnant women. Increased human chorionic gonadotropin levels have been implicated in this condition. The serum sodium (Na+) concentration falls by approximately 5 mEq/L in the first 2 months of pregnancy and remains stable until after delivery, when it returns to normal levels. Recognizing this entity is important because it does not require treatment.
Psychogenic polydipsia
Psychogenic polydipsia is characterized by an increase in water intake attributed to a defect in the thirst mechanism. In some patients, the osmotic threshold for thirst is reset below the reset for release of ADH. Psychogenic polydipsia is mostly observed in patients with psychosis.
Water excretion is normal in these patients, and water restriction corrects the hyponatremia. In a patient on a normal diet and an average solute (protein and salts) intake, a substantial amount of water must be imbibed for hyponatremia to develop. Consider an individual who has 700 mOsm (primarily consisting of urea, sodium, potassium, and chloride) to excrete per day. Ordinarily, these individuals can vary their urine osmolality between 50 and 1400 mOsm/L and thus can excrete the osmotic load in a minimum of 500 mL and a maximum of 14 L. As long as their fluid intake is between these extremes, they adjust urine osmolality to excrete the load. To become hyponatremic, such an individual must drink more than 14 L a day.
Decreased solute intake
Decreased solute intake is observed in persons who drink hyponatremic fluids without adequate food intake. Decreased solute intake is described in individuals who drink beer (beer potomania) and thrive on little else and thus have substantially reduced protein and salt intake. The daily solute intake directly influences the osmotic load to be excreted. With poor nutritional intake, the osmotic load may be as little as 200 mOsm; in this situation, it can be excreted in a maximum of 4 L. Ingestion of a larger quantity of solute-free fluids without other avenues for water loss can result in the development of hyponatremia.
Diuretics and hyponatremia
Diuretics can cause mild-to-severe hyponatremia. Thiazide diuretics cause hyponatremia more often than loop diuretics. This is related to the different sites of action of these agents.
Loop diuretics act in the medullary thick ascending limb and prevent sodium (Na+) absorption in the medullary thick ascending limb. This interferes with the concentrating ability by diminishing medullary osmolality. The sodium (Na+) can be reabsorbed once it reaches the distal tubule and the collecting duct.
The thiazide diuretics prevent sodium (Na+) absorption in the distal tubule and do not interfere with the medullary concentrating ability or the effect of ADH. However, the distal tubule is the diluting segment of the nephron, and diminished sodium (Na+) absorption here increases urine osmolality and prevents the excretion of hypotonic urine. In patients who are susceptible to this effect, hyponatremia is usually observed within 2 weeks. After that, a new steady state is reached and further changes in serum sodium (Na+) only occur with an added stimulus such as vomiting and diarrhea.
Nephrogenic syndrome of inappropriate antidiuresis
Nephrogenic syndrome of inappropriate antidiuresis (NSIAD) is a rare X-linked recessive genetic disease arising from gain-of-function mutations in the V2 receptor, resulting in a spontaneously active receptor and unregulated water reabsorption. The laboratory features are identical to those of SIADH, with euvolemic hyponatremia, plasma hypo-osmolality, and increased urinary osmolality. Nephrogenic syndrome of inappropriate antidiuresis (NSIAD) is likely to present in early infancy, although some adults have been described with this disorder 14, 34 If ADH levels are measured, they are predicted to be low.
Hypervolemic hyponatremia
Other conditions to consider in the differential diagnosis of hyponatremia are those that are associated with hypervolemia in which the baroreceptors perceive reduced effective circulating volume and stimulate ADH secretion. These conditions include congestive heart failure, cirrhosis, and nephrotic syndrome. These should be evident on clinical examination because of the presence of peripheral edema with elevated jugular venous pressure, pulmonary rales, ascites, or stigmata of advanced liver disease.
SIADH treatment
SIADH treatment is aimed at addressing the underlying cause, if possible 1. If cancer is the cause of the SIADH, then radiation, chemotherapy, or surgery to remove the tumor may correct the sodium imbalance.
Other treatments depend on the specific type of hyponatremia.
Hyponatremia treatments may include:
- Fluid restriction. Fluid restriction helps prevent excess fluid from building up in your body. Your doctor will tell you what your total daily fluid intake should be. The restriction is not just for water, but for almost all fluids (coffee, tea, juice, soda, etc.).
- Fluid restriction of less than 1000 mL/day is the first-line therapy for chronic SIADH endorsed by current guidelines, but is effective in only around half of cases
- Medicines to relieve symptoms. You may take medications to manage the signs and symptoms of hyponatremia, such as headaches, nausea and seizures.
- Fluids through a vein (IV). Your doctor may recommend IV sodium solution to slowly raise the sodium levels in your blood. This requires a stay in the hospital for frequent monitoring of sodium levels as too rapid of a correction is dangerous.
Emergency care
Aggressive treatment of hyponatremia should always be weighed against the risk of inducing central pontine myelinolysis (CPM). A rare but serious complication, central pontine myelinolysis can develop 1 to several days after aggressive treatment of hyponatremia. Aggressive management of hyponatremia is indicated in patients with severe symptoms such as seizures, stupor, coma, and respiratory arrest, regardless of the degree of hyponatremia. Emergent treatment should also be strongly considered for those with moderate-to-severe hyponatremia with a documented duration of less than 48 hours.
The goal is to correct hyponatremia at a rate that does not cause neurologic complications. The objective is to raise serum sodium (Na+) levels by 0.5-1 mmol/hour and not more than 10-12 mmol in the first 24 hours, to bring the sodium (Na+) value to a maximum level of 125 -130 mmol/L. Administration of 3% hypertonic saline should be restricted to these emergent circumstances, and both neurological symptoms and serum sodium (Na+) should be monitored frequently to achieve the desired target and to prevent overcorrection.
Correction of serum sodium (Na+) levels by 6 mmol/L in 24 hours has been dubbed the “rule of sixes.” The rule states that, “Six a day makes sense for safety; 6 in 6 hours for severe symptoms and stop” 35.
Other authors have recommended a rate of initial correction of 1-2 mmol/L/hour in severely symptomatic patients until symptoms resolve (or for the first 3-4 hour). However, total correction in the first 24 hours must not exceed 10-12 mmol. Central pontine myelinolysis has been reported in cases in which the initial correction exceeded 12 mmol and even in cases in which the correction was 9-10 mmol/24 h. This has led some authors to recommend a lower target of 8 mmol in 24 hours. In the special situation of exercise-induced hyponatremia with neurological symptoms, some authors recommend an immediate bolus of 100 mL of 3% hypertonic saline repeated every 10 minutes until symptoms resolve 28.
Formulas for the dose and rate of hypertonic saline have been proposed based on a sodium (Na+) deficit to calculate the rate of administration of hypertonic fluids 17, 36. However, they have not been prospectively studied. Despite the correct use of these formulas, hyponatremia is often corrected too rapidly. Therefore, these formulas should serve only as guidelines. Patients still require frequent retesting of their serum sodium (Na+) concentration 37.
The approximate sodium (Na+) deficit can be estimated by using the following formula (0.5 L/kg for females):
- Sodium Deficit (mmol) = (Desired sodium (Na+) – Measured sodium (Na+)) x 0.6 L/kg x Weight (kg)
Three-percent hypertonic saline has 513 mmol/L each of sodium (Na+) and Cl- and has an osmolality of 1026 mOsm/L. The volume of hypertonic saline needed to correct that deficit can be calculated as follows:
- Volume of 3% Saline = (sodium deficit)/513 mmol/L sodium
Assuming a rate of correction of chronic hyponatremia of 0.5 mmol/L per hour, the amount of time needed to correct a given degree of hyponatremia is as follows:
- Time Needed for Correction = (Desired sodium (Na+) – Measured sodium (Na+))/0.5 mmol/L per hour
The rate of infusion of hypertonic saline is as follows:
- Rate = (Volume of 3% Saline)/(Time Needed for Correction)
Furosemide increases excretion of free water and has been used along with hypertonic saline in severe cases to limit treatment-induced volume expansion. The diuresis induced by furosemide has a urine solute concentration roughly equivalent to half-normal saline; thus, excretion of free water occurs. Electrolyte free water intake can be restricted. Combining furosemide with hypertonic saline and water restriction may lead to a faster rate of correction of serum Na and requires that serum sodium (Na+) osmolality and urine osmolality be checked frequently to monitor the change in serum sodium (Na+) values and to prevent overcorrection. Attention should also be paid to the prevention of severe hypokalemia in conjunction with treatment of hyponatremia.
Figure 6. Useful formulas in the management of hyponatremia
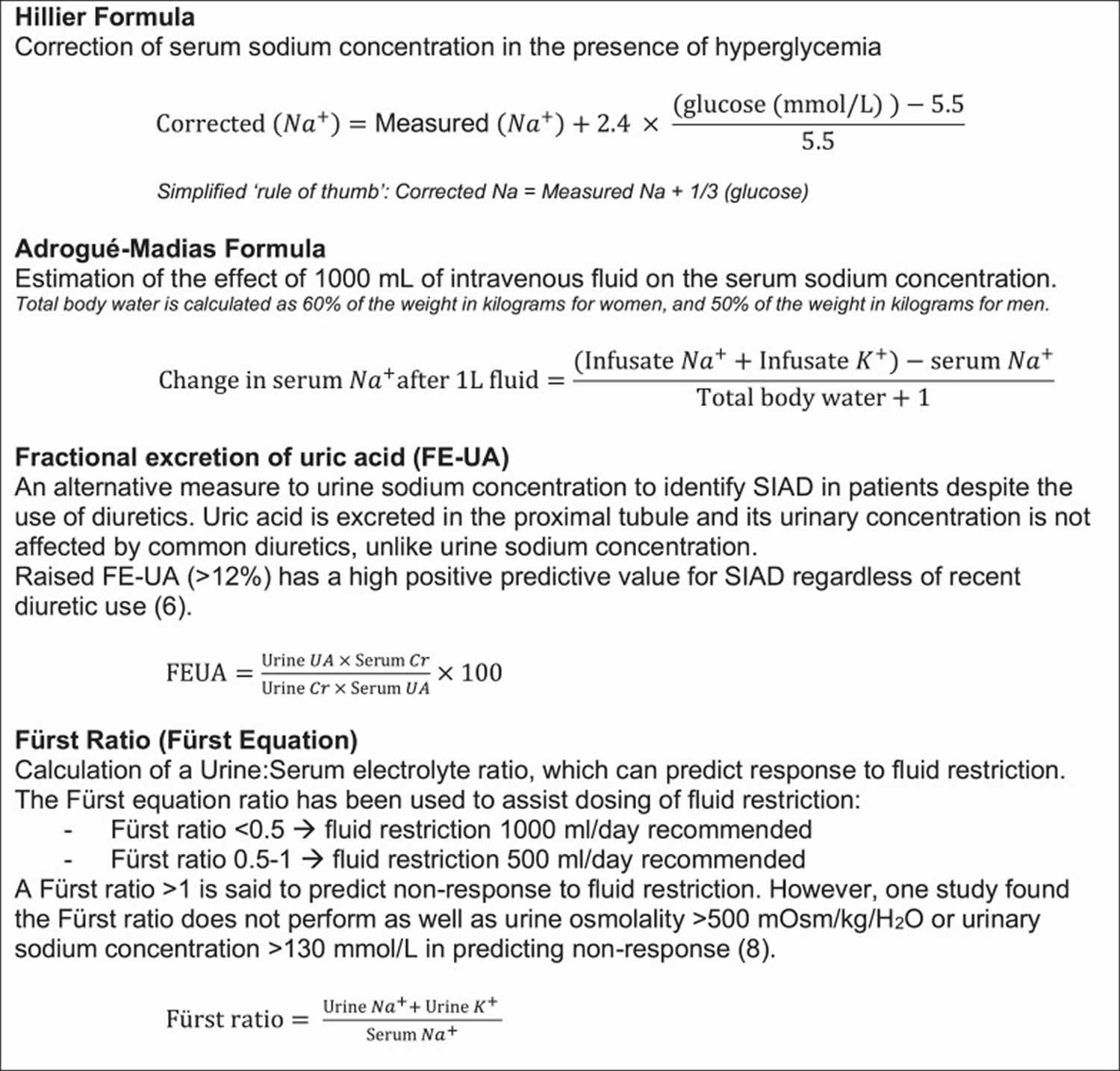
Abbreviations: Cr = creatinine; FEUA = fractional excretion of uric acid; mOsm = milliosmoles; Na+ = sodium; UA = uric acid.
[Source 1 ]Acute hyponatremia
In the acute setting (ie, less than 48 hours since onset) with moderate symptoms such as confusion, delirium, disorientation, nausea, and vomiting, the treatment options for the hyponatremia include 3% hypertonic saline (513 mmol/L), loop diuretics with saline, vasopressin-2 receptor antagonists (aquaretics), and water restriction.
Depending on the rate of development of hyponatremia, the approach to correction varies. If an acute onset and moderate neurologic symptoms have occurred, the use of hypertonic saline may be warranted. If symptoms are less severe (headache, irritability, inability to concentrate, altered mood) or absent, then vasopressin-2 receptor antagonists (aquaretics) or water restriction are both options. The patient’s serum sodium (Na+) level and clinical status must be monitored often to determine the need for continued aggressive therapy.
Water restriction
The degree of water restriction depends on the prior water intake, the expected ongoing fluid losses, and the degree of hyponatremia. Water restriction to about 500-1500 mL/day (or even lower in some cases) is usually prescribed. Although easier to maintain in the hospital setting, this becomes difficult for patients to follow in an outpatient setting.
One of the functions of the kidneys is to excrete solutes in varying amounts of water. In persons with SIADH, urine osmolality is fixed at a certain value; for the kidneys to eliminate an “X” amount of solutes, a certain volume of water must be excreted. If water intake is lowered below total obligatory fluid losses (insensible losses plus volume of urine required to excrete the osmolar load), then serum osmolality rises because a net loss of water occurs. The insensible losses of relatively hypotonic fluids also contribute to net water loss. The key is sufficient restriction of water intake so that the excretion of free water from all sources is in excess of that taken in.
For example, consider a patient who has a net solute load of 900 mOsm/kg/day that must be excreted, and, because of SIADH, his or her urine osmolality is fixed at 600 mOsm/kg. This patient then excretes the solute load in 1.5 L of urine. On the other hand, if the urine osmolarity is fixed at 300 mOsm/kg, then 3 L of urine is required to excrete the same osmolar load. When water intake is restricted, the body mobilizes the free water already present to excrete this load. Thus, if urine output (plus insensible losses) exceeds water intake, a net water loss occurs and the serum sodium (Na+) level returns towards normal. For that reason when the sum of urinary sodium (Na+) and K+ is greater than serum sodium (Na+) concentration, fluid restriction alone is unlikely to be effective 18.
Vasopressin receptor antagonists
Vasopressin receptor antagonists inhibit the AVP V2 receptor, reducing the number of aquaporin-2 water channels in the renal collecting duct and decreasing the water permeability of the collecting duct. Collectively, agents that competitively block ADH action and increase water excretion are called aquaretics, and they are useful in the treatment of the hyponatremia in SIADH. The term “vaptan” has been coined to officially name all the members of this new class of drugs 38.
Two aquaretics are currently approved by the US Food and Drug Administration (FDA). Conivaptan is a parenteral nonpeptide dual AVP V1a- and V2-receptor antagonist that is approved for use in hospitalized patients with euvolemic (dilutional) and hypervolemic hyponatremia. The drug is given as a 20-mg loading dose followed by a continuous infusion or as intermittent boluses, but it should not be used for more than 4 days. The pivotal studies in euvolemic hyponatremia showed that compared with fluid restriction alone, conivaptan together with a 2 L fluid restriction over 4 days increased serum Na by 6 mEq/L, with a median increase of 4 mEq/L by 23 hours 39.
Tolvaptan is a selective oral V2 receptor antagonist also approved for use in hospitalized patients for hypervolemia and euvolemic hyponatremia 40. Tolvaptan is started at 15 mg once daily and titrated up to 60 mg daily as required, and it is best to avoid fluid restriction during the dose-finding phase. In the pivotal studies, which included patients with heart failure, cirrhosis, and SIADH, tolvaptan compared with fluid restriction alone increased serum Na by 8 mEq/L over 30 days, although with withdrawal of the drug, serum sodium (Na+) falls back to that seen in the placebo group 41.
Tolvaptan is a useful drug to consider in a patient in whom serum sodium (Na+) does not rise by 2 mEq in the first 24 hrs after a 1000-mL fluid restriction. Once the drug is initiated, the patient can be discharged in 24-48 hours if neurological symptoms have resolved or the patient was asymptomatic at presentation. If the underlying cause of SIADH has resolved, the drug can be withdrawn after 2-4 weeks, while carefully monitoring serum sodium (Na+) daily for the next 5 days. If the serum sodium (Na+) falls again and if is less than 125 for more than 48 hours, the patient may need to be admitted again before reinitiating tolvaptan. Tolvaptan can also be considered for long-term therapy of chronic hyponatremia 42.
Results of a study by Morris et al suggest that low baseline serum sodium (Na+) and serum urea nitrogen (SUN) values can identify patients with SIADH who are likely to experience rapid correction of hyponatremia with tolvaptan, and who are thus at risk of overcorrection. In their study, which included 28 patients with SIADH treated with tolvaptan, the rate of increase in serum sodium (Na+) concentration was significantly greater (mean 24-hour increase of 15.4 mEq/L) in patients with baseline serum sodium (Na+) of 121 mEq/L or less and baseline SUN of 10 mg/dL or less, than it was in patients with higher baseline sodium (Na+) and SUN concentrations 43.
The vaptans can have a profound effect on serum sodium and they should be used by physicians experienced in the management of hyponatremia. These drugs should be avoided in hypovolemic hyponatremia. The vaptans are more likely to be effective compared with fluid restriction alone in patients in whom the sum of urinary potassium and sodium (Na+) concentration is greater than the plasma concentration. They offer the benefit of prompt correction of serum sodium (Na+), producing water excretion without electrolyte excretion and eliminating the need for fluid restriction. The primary risk of using these drugs is an excessively rapid rate of correction of the serum sodium concentration.
Furosemide
Furosemide and other loop diuretics can be used to increase the excretion of free water. Excess water that must be removed to correct the hyponatremia can be calculated using total body water (TBW). Total body water equals body weight in kg multiplied by 0.6, assuming that the total body solute or water has not changed. The diuresis induced by furosemide has a urine solute concentration roughly equivalent to half-normal saline; thus, excretion of free water occurs. The excreted sodium (Na+) is replaced with 3% hypertonic saline or with normal saline (NaCl 154 mEq/L), thus avoiding a net sodium (Na+) loss while effecting a loss of free water.
Other sources of free water intake should be restricted as well. If the measured sum of urinary potassium and sodium (Na+) with furosemide is greater than the plasma Na, then hypertonic saline rather than normal saline should be used to replace excreted Na. Serum sodium (Na+) and osmolality and urine osmolality should be checked frequently to monitor the change in serum sodium (Na+) and the rate of correction.
Empagliflozin
The sodium–glucose cotransporter 2 (SGLT2) inhibitor empagliflozin has shown benefit in patients with SIADH, as empagliflozin can promote osmotic diuresis by inducing glucosuria 44. In a randomized controlled trial by Refardt et al in 87 hospitalized patients with SIADH-induced hyponatremia, patients who received 4 days of empagliflozin had a significantly larger increase in plasma sodium compared with those who received placebo (10 versus 7 mmol/L, respectively). The likelihood of response to empagliflozin was greater in patients with profound hyponatremia (< 125 mmol/L) and lower baseline osmolality levels 45.
Chronic hyponatremia
Asymptomatic patients with chronic SIADH, the principal options are fluid restriction and V2 receptor antagonists (see Acute Setting). If V2 receptor antagonists are not available or if local experience with these agents is very limited, other therapeutic modalities include chronic loop diuretics with increased salt intake, urea, mannitol, and demeclocycline.
Urea
Urea is a solute that must be excreted by the kidneys. Because urine osmolality is fixed in persons with SIADH, the obligatory urine volume can be increased by increasing the osmotic or solute load. Increased urinary loss of water decreases free water retention. This therapy can be used in chronic and acute settings if the urine osmolality is low and can increase the serum sodium (Na+) by up to 5 mEq/L/day. Urea is a relatively nontoxic compound and, as opposed to sodium chloride treatment, does not cause edema or increase body weight.
Urea can be administered on a long-term basis (0.5 g/kg body weight) without major adverse effects. Urea is available as a powder, which is dissolved in water and taken orally during or after meals. To avoid gastric upset, it can be taken with an antacid. Urea can also be used continuously in patients with cerebral hemorrhage via a gastric tube or intravenously to prevent a rapid fall in intracranial pressure.
Urea should be used with great care in patients with serum creatinine of 2 mg/dL or more, BUN 80 mg/dL or more, or bilirubin of 2 mg/dL or more, to avoid progressive azotemia, hyperammonemia, and hepatic encephalopathy. Hypernatremia and dehydration may occur if the patient does not have free access to water.
SIADH prognosis
SIADH prognosis (outcome) depends on the underlying cause and to the effects of severe hyponatremia and its overzealous correction 46. Many causes of SIADH are reversible. Rapid and complete recovery tends to be the rule with drug-induced SIADH when the offending drug is withdrawn. Successful treatment of pulmonary or central nervous system infection also can lead to correction of SIADH. However, patients who present with neurologic symptoms or have severe hyponatremia even without symptoms may develop permanent neurologic impairment. Patients whose serum sodium (Na+) is rapidly corrected, especially those who are asymptomatic, can also develop permanent neurologic impairment from central pontine myelinolysis 46.
Previously, mild hyponatremia was considered relatively asymptomatic. However, evidence suggests that even mild hyponatremia can cause significant impairment, such as unsteady gait, and lead to frequent falls. This effect may be greater in elderly persons, who are more sensitive to changes in serum sodium (Na+) 47. Hyponatremia may also be a risk factor for osteoporosis and bone fracture 48.
The mortality of patients with hyponatremia (sodium (Na+) less than 130 mmol/L) is increased 60-fold compared with that of patients without documented hyponatremia, although this may be partly related to their comorbid conditions rather than to the hyponatremia itself. Predictors for higher morbidity and mortality rates include being hospitalized, acute onset, and severity of hyponatremia 49. When the sodium (Na+) concentration drops below 105 mmol/L, life-threatening complications are much more likely to occur 17.
In a retrospective case note review by Clayton and colleagues 37, patients with a multifactorial cause for hyponatremia in an inpatient setting had significantly higher mortality rates. The cause of hyponatremia was a more important prognostic indicator than the level of absolute serum sodium (Na+) in the patients. The outcome was least favorable in patients with normal sodium levels on admission who became hyponatremic during the course of their hospitalization 37.
- Warren AM, Grossmann M, Christ-Crain M, Russell N. Syndrome of Inappropriate Antidiuresis: From Pathophysiology to Management. Endocr Rev. 2023 Sep 15;44(5):819-861. doi: 10.1210/endrev/bnad010[
 ][][][][][][][]
][][][][][][][] - Yasir M, Mechanic OJ. Syndrome of Inappropriate Antidiuretic Hormone Secretion. [Updated 2023 Mar 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507777[][][][][]
- Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH). https://emedicine.medscape.com/article/246650-overview[]
- SCHWARTZ WB, BENNETT W, CURELOP S, BARTTER FC. A syndrome of renal sodium loss and hyponatremia probably resulting from inappropriate secretion of antidiuretic hormone. Am J Med. 1957 Oct;23(4):529-42. doi: 10.1016/0002-9343(57)90224-3[][]
- Lockett J, Berkman KE, Dimeski G, Russell AW, Inder WJ. Urea treatment in fluid restriction-refractory hyponatraemia. Clin Endocrinol (Oxf). 2019 Apr;90(4):630-636. doi: 10.1111/cen.13930[]
- Monden MAH, van der Vorst LP, Martens HJM, van der Wolk A. Het syndroom van inadequate secretie van het antidiuretisch hormoon (SIADH) met letale afloop tijdens gebruik van paliperidon en lamotrigine [The syndrome of inappropriate diuretic hormone secretion (SIADH) ending lethal during the use of paliperidon and lamotrigine]. Tijdschr Psychiatr. 2018;60(12):848-851. Dutch.[]
- Baba Y, Harada H, Shimada S, Sasaki Y, Murai S, Abe M, Fujiwara S, Arai N, Kawaguchi Y, Kabasawa N, Tsukamoto H, Uto Y, Ariizumi H, Yanagisawa K, Hattori N, Saito B, Nakamaki T. [Syndrome of inappropriate secretion of antidiuretic hormone in multiple myeloma patients treated with bortezomib, lenalidomide, and dexamethasone combination therapy]. Rinsho Ketsueki. 2018;59(11):2423-2427. Japanese. doi: 10.11406/rinketsu.59.2423[]
- Antidiuretic Hormone (ADH, Vasopressin, Arginine Vasopressin), Diabetes Insipidus. https://labpedia.net/antidiuretic-hormone-adh-vasopressin-arginine-vasopressin-hormone-diabetes-insipidus[]
- Robertson GL, Shelton RL, Athar S. The osmoregulation of vasopressin. Kidney Int. 1976 Jul;10(1):25-37. doi: 10.1038/ki.1976.76[]
- Robertson GL. Regulation of arginine vasopressin in the syndrome of inappropriate antidiuresis. Am J Med. 2006 Jul;119(7 Suppl 1):S36-42. doi: 10.1016/j.amjmed.2006.05.006[]
- Cooke CR, Turin MD, Walker WG. The syndrome of inappropriate antidiuretic hormone secretion (SIADH): pathophysiologic mechanisms in solute and volume regulation. Medicine (Baltimore). 1979 May;58(3):240-51. doi: 10.1097/00005792-197905000-00004[]
- Steele A, Gowrishankar M, Abrahamson S, Mazer CD, Feldman RD, Halperin ML. Postoperative hyponatremia despite near-isotonic saline infusion: a phenomenon of desalination. Ann Intern Med. 1997 Jan 1;126(1):20-5. doi: 10.7326/0003-4819-126-1-199701010-00003[]
- Vitting KE, Gardenswartz MH, Zabetakis PM, et al. Frequency of Hyponatremia and Nonosmolar Vasopressin Release in the Acquired Immunodeficiency Syndrome. JAMA. 1990;263(7):973–978. doi:10.1001/jama.1990.03440070061033[][]
- Feldman BJ, Rosenthal SM, Vargas GA, Fenwick RG, Huang EA, Matsuda-Abedini M, Lustig RH, Mathias RS, Portale AA, Miller WL, Gitelman SE. Nephrogenic syndrome of inappropriate antidiuresis. N Engl J Med. 2005 May 5;352(18):1884-90. doi: 10.1056/NEJMoa042743[][]
- Decaux G, Vandergheynst F, Bouko Y, Parma J, Vassart G, Vilain C. Nephrogenic syndrome of inappropriate antidiuresis in adults: high phenotypic variability in men and women from a large pedigree. J Am Soc Nephrol. 2007 Feb;18(2):606-12. doi: 10.1681/ASN.2006090987[]
- Fenske WK, Christ-Crain M, Hörning A, Simet J, Szinnai G, Fassnacht M, Rutishauser J, Bichet DG, Störk S, Allolio B. A copeptin-based classification of the osmoregulatory defects in the syndrome of inappropriate antidiuresis. J Am Soc Nephrol. 2014 Oct;25(10):2376-83. doi: 10.1681/ASN.2013080895[]
- Ellison DH, Berl T. Clinical practice. The syndrome of inappropriate antidiuresis. N Engl J Med. 2007 May 17;356(20):2064-72. doi: 10.1056/NEJMcp066837[][][][][]
- Verbalis JG, Goldsmith SR, Greenberg A, Korzelius C, Schrier RW, Sterns RH, Thompson CJ. Diagnosis, evaluation, and treatment of hyponatremia: expert panel recommendations. Am J Med. 2013 Oct;126(10 Suppl 1):S1-42. doi: 10.1016/j.amjmed.2013.07.006[][]
- Shepshelovich D, Schechter A, Calvarysky B, Diker-Cohen T, Rozen-Zvi B, Gafter-Gvili A. Medication-induced SIADH: distribution and characterization according to medication class. Br J Clin Pharmacol. 2017 Aug;83(8):1801-1807. doi: 10.1111/bcp.13256[]
- Marcelino GP, Collantes CMC, Oommen JK, Wang S, Baldassari H, Muralidharan R, Hanna A. Amiodarone-Induced Syndrome of Inappropriate Antidiuretic Hormone: A Case Report and Review of the Literature. P T. 2019 Jul;44(7):416-423 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6590929[]
- Singh TD, Fugate JE, Rabinstein AA. Central pontine and extrapontine myelinolysis: a systematic review. Eur J Neurol. 2014 Dec;21(12):1443-50. doi: 10.1111/ene.12571[]
- Lampl C, Yazdi K. Central pontine myelinolysis. Eur Neurol. 2002;47(1):3-10. doi: 10.1159/000047939[]
- Kumar S, Fowler M, Gonzalez-Toledo E, Jaffe SL. Central pontine myelinolysis, an update. Neurol Res. 2006 Apr;28(3):360-6. doi: 10.1179/016164106X110346[]
- Silveira MAD, Seguro AC, da Silva JB, Arantes de Oliveira MF, Seabra VF, Reichert BV, Rodrigues CE, Andrade L. Chronic Hyponatremia Due to the Syndrome of Inappropriate Antidiuresis (SIAD) in an Adult Woman with Corpus Callosum Agenesis (CCA). Am J Case Rep. 2018 Nov 12;19:1345-1349. doi: 10.12659/AJCR.911810[]
- Rondon-Berrios H, Tandukar S, Mor MK, Ray EC, Bender FH, Kleyman TR, Weisbord SD. Urea for the Treatment of Hyponatremia. Clin J Am Soc Nephrol. 2018 Nov 7;13(11):1627-1632. doi: 10.2215/CJN.04020318[]
- Berardi R, Antonuzzo A, Blasi L, Buosi R, Lorusso V, Migliorino MR, Montesarchio V, Zilembo N, Sabbatini R, Peri A. Practical issues for the management of hyponatremia in oncology. Endocrine. 2018 Jul;61(1):158-164. doi: 10.1007/s12020-018-1547-y[]
- Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) Differential Diagnoses. https://emedicine.medscape.com/article/246650-differential[]
- Hew-Butler T, Noakes TD, Siegel AJ. Practical management of exercise-associated hyponatremic encephalopathy: the sodium paradox of non-osmotic vasopressin secretion. Clin J Sport Med. 2008 Jul;18(4):350-4. doi: 10.1097/JSM.0b013e3181802c6d. Erratum in: Clin J Sport Med.2008 Sep;18(5):382.[][]
- Johnson RJ, Lee SMK, Sánchez-Lozada LG, Kanbay M, Bansal A, Tolan DR, Bjornstad P, Lanaspa MA, Maesaka J. Fructose: A New Variable to Consider in SIADH and the Hyponatremia Associated With Long-Distance Running? Am J Kidney Dis. 2023 Jul;82(1):105-112. doi: 10.1053/j.ajkd.2023.01.443[]
- Ayus JC, Varon J, Arieff AI. Hyponatremia, cerebral edema, and noncardiogenic pulmonary edema in marathon runners. Ann Intern Med. 2000 May 2;132(9):711-4. doi: 10.7326/0003-4819-132-9-200005020-00005[]
- Sterns RH, Silver SM. Cerebral salt wasting versus SIADH: what difference? J Am Soc Nephrol. 2008 Feb;19(2):194-6. doi: 10.1681/ASN.2007101118[]
- Yee AH, Burns JD, Wijdicks EF. Cerebral salt wasting: pathophysiology, diagnosis, and treatment. Neurosurg Clin N Am. 2010 Apr;21(2):339-52. doi: 10.1016/j.nec.2009.10.011[][]
- Tian W, Fu Y, Garcia-Elias A, Fernández-Fernández JM, Vicente R, Kramer PL, Klein RF, Hitzemann R, Orwoll ES, Wilmot B, McWeeney S, Valverde MA, Cohen DM. A loss-of-function nonsynonymous polymorphism in the osmoregulatory TRPV4 gene is associated with human hyponatremia. Proc Natl Acad Sci U S A. 2009 Aug 18;106(33):14034-9. doi: 10.1073/pnas.0904084106[]
- Powlson AS, Challis BG, Halsall DJ, Schoenmakers E, Gurnell M. Nephrogenic syndrome of inappropriate antidiuresis secondary to an activating mutation in the arginine vasopressin receptor AVPR2. Clin Endocrinol (Oxf). 2016 Aug;85(2):306-12. doi: 10.1111/cen.13011[]
- Sterns RH, Hix JK, Silver S. Treating profound hyponatremia: a strategy for controlled correction. Am J Kidney Dis. 2010 Oct;56(4):774-9. doi: 10.1053/j.ajkd.2010.04.020[]
- Voets PJGM, Vogtländer NPJ. A quantitative approach to intravenous fluid therapy in the syndrome of inappropriate antidiuretic hormone secretion. Clin Exp Nephrol. 2019 Aug;23(8):1039-1044. doi: 10.1007/s10157-019-01741-6[]
- Clayton JA, Le Jeune IR, Hall IP. Severe hyponatraemia in medical in-patients: aetiology, assessment and outcome. QJM. 2006 Aug;99(8):505-11. doi: 10.1093/qjmed/hcl071[][][]
- Verbalis JG. Disorders of water balance. Skorecki K, Chertow GM, Marsden PA, Yu ASL, Taal MW. Brenner & Rector’s The Kidney. 10th ed. Philadelphia, PA: Elsevier; 2016. Vol 1: 460-510.[]
- Zeltser D, Rosansky S, van Rensburg H, Verbalis JG, Smith N; Conivaptan Study Group. Assessment of the efficacy and safety of intravenous conivaptan in euvolemic and hypervolemic hyponatremia. Am J Nephrol. 2007;27(5):447-57. doi: 10.1159/000106456[]
- Nemerovski C, Hutchinson DJ. Treatment of hypervolemic or euvolemic hyponatremia associated with heart failure, cirrhosis, or the syndrome of inappropriate antidiuretic hormone with tolvaptan: a clinical review. Clin Ther. 2010 Jun;32(6):1015-32. doi: 10.1016/j.clinthera.2010.06.015[]
- Schrier RW, Gross P, Gheorghiade M, Berl T, Verbalis JG, Czerwiec FS, Orlandi C; SALT Investigators. Tolvaptan, a selective oral vasopressin V2-receptor antagonist, for hyponatremia. N Engl J Med. 2006 Nov 16;355(20):2099-112. doi: 10.1056/NEJMoa065181[]
- Berl T, Quittnat-Pelletier F, Verbalis JG, Schrier RW, Bichet DG, Ouyang J, Czerwiec FS; SALTWATER Investigators. Oral tolvaptan is safe and effective in chronic hyponatremia. J Am Soc Nephrol. 2010 Apr;21(4):705-12. doi: 10.1681/ASN.2009080857. Epub 2010 Feb 25. Erratum in: J Am Soc Nephrol. 2010 Aug;21(8):1407.[]
- Morris JH, Bohm NM, Nemecek BD, Crawford R, Kelley D, Bhasin B, Nietert PJ, Velez JCQ. Rapidity of Correction of Hyponatremia Due to Syndrome of Inappropriate Secretion of Antidiuretic Hormone Following Tolvaptan. Am J Kidney Dis. 2018 Jun;71(6):772-782. doi: 10.1053/j.ajkd.2017.12.002[]
- Carney EF. Efficacy of empagliflozin for syndrome of inappropriate antidiuresis. Nat Rev Nephrol. 2023 Feb;19(2):73. doi: 10.1038/s41581-022-00673-x[]
- Refardt J, Imber C, Sailer CO, Jeanloz N, Potasso L, Kutz A, Widmer A, Urwyler SA, Ebrahimi F, Vogt DR, Winzeler B, Christ-Crain M. A Randomized Trial of Empagliflozin to Increase Plasma Sodium Levels in Patients with the Syndrome of Inappropriate Antidiuresis. J Am Soc Nephrol. 2020 Mar;31(3):615-624. doi: 10.1681/ASN.2019090944[]
- Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH). https://emedicine.medscape.com/article/246650-overview#a7[][]
- Renneboog B, Musch W, Vandemergel X, Manto MU, Decaux G. Mild chronic hyponatremia is associated with falls, unsteadiness, and attention deficits. Am J Med. 2006 Jan;119(1):71.e1-8. doi: 10.1016/j.amjmed.2005.09.026[]
- Usala RL, Fernandez SJ, Mete M, Cowen L, Shara NM, Barsony J, Verbalis JG. Hyponatremia Is Associated With Increased Osteoporosis and Bone Fractures in a Large US Health System Population. J Clin Endocrinol Metab. 2015 Aug;100(8):3021-31. doi: 10.1210/jc.2015-1261[]
- Stelfox HT, Ahmed SB, Khandwala F, Zygun D, Shahpori R, Laupland K. The epidemiology of intensive care unit-acquired hyponatraemia and hypernatraemia in medical-surgical intensive care units. Crit Care. 2008;12(6):R162. doi: 10.1186/cc7162[]





{kind=link}