
Urinary urgency
Urinary urgency is a symptom of the inability to postpone urination once the sudden, strong need to urinate has been felt. This causes a discomfort in your bladder. Urinary urgency makes it difficult to delay using the toilet to urinate.
How a healthy bladder works
The urinary tract is your body’s drainage system for removing wastes and extra fluids. The urinary tract includes two kidneys, two ureters, a bladder, and a urethra.
You have 2 kidneys that filter wastes and fluids to produce urine. The urine travels from your kidneys down two narrow tubes called the ureters into your bladder. The urine is then stored in a hollow, muscular, balloon-shaped organ called the bladder. When the bladder empties, urine flows out of your body through a tube called the urethra at the bottom of the bladder. A muscle in the urethra called the sphincter opens to release urine out of the body.
In women, the urethral opening is located just above the vaginal opening. In men, the urethral opening is at the tip of the penis.
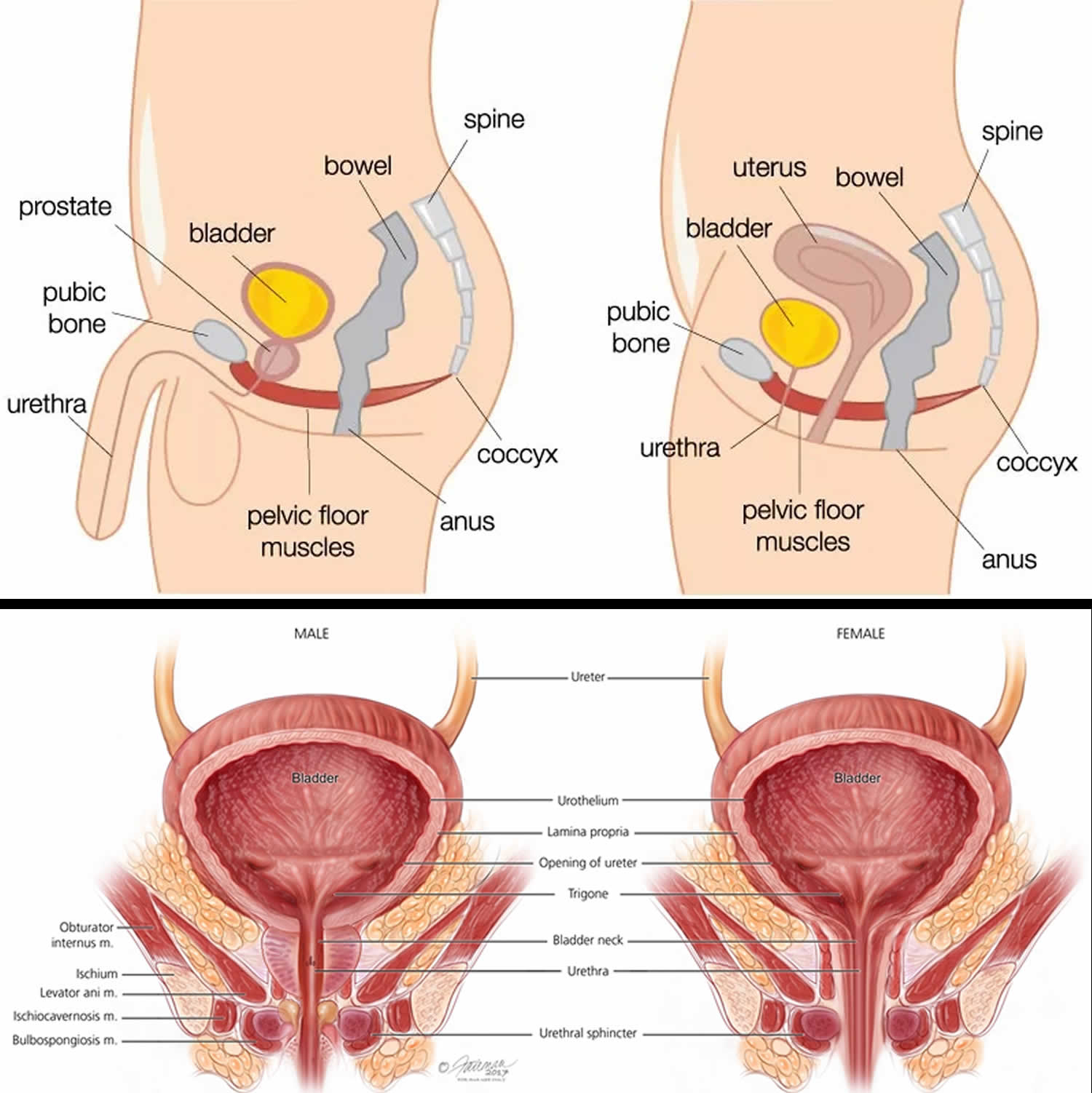
As your bladder fills, nerve signals sent to your brain eventually trigger the need to urinate. When you urinate, these nerve signals coordinate the relaxation of the pelvic floor muscles and the muscles of the urethra (urinary sphincter muscles). The muscles of the bladder tighten (contract), pushing the urine out.
Figure 1. Male and female urinary system
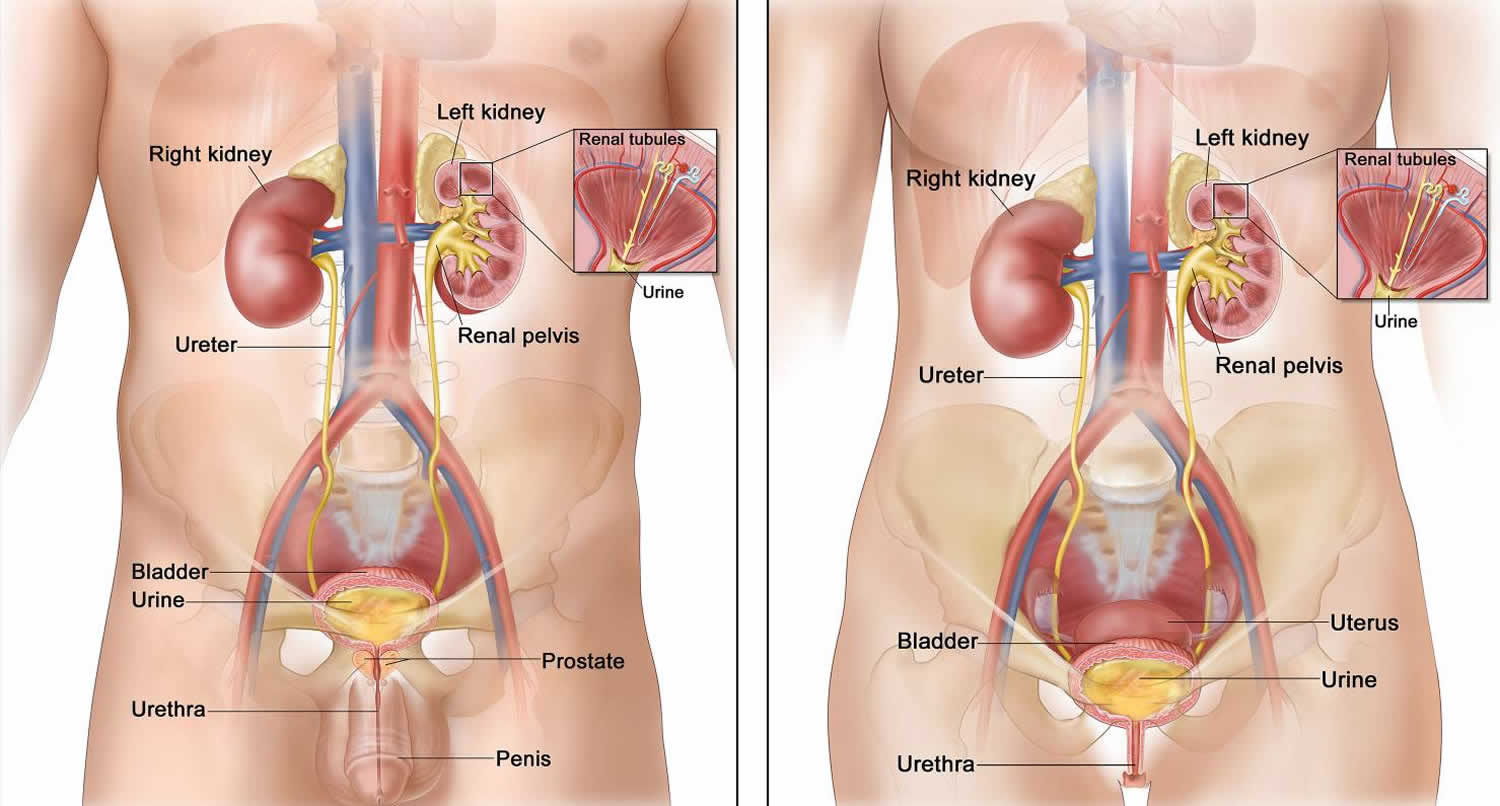
Figure 2. Pelvic floor muscles
What are normal bladder habits?
It is normal to:
- empty your bladder about four to six times through the day
- empty your bladder before you go to bed at night
- empty your bladder once overnight
- empty your bladder when you get out of bed in the morning
A healthy bladder holds about one and a half to two cups of urine. This is equal to 300–400 mls. Your bladder holds this much during the day. It holds more during the night, before you feel the need to pass urine.
This pattern may change in older people. Older people may make more urine at night. This means they may have to pass more urine through the night than they do in the day.
Urinary urgency causes
Common causes of urinary urgency are:
- Urinary tract infection (UTI)
- Enlarged prostate in middle-aged and older men
- Swelling and infection of the urethra
- Vaginitis (swelling or discharge of the vulva and vagina)
- Nerve related problems
- Caffeine intake
Less common causes of urinary urgency include:
- Alcohol use
- Anxiety
- Bladder cancer (not common)
- Spine problems
- Diabetes that is not well controlled
- Pregnancy
- Interstitial cystitis
- Medicines such as water pills (diuretics)
- Overactive bladder syndrome (OAB)
- Radiation therapy to the pelvis, which is used to treat certain cancers
- Stroke and other brain or nervous system diseases
- Tumor or growth in the pelvis
Overactive bladder
Overactive bladder, also called OAB, is a condition in which the muscles of your bladder (detrusor muscle) start to contract on their own even when the volume of urine in your bladder is low. These are called involuntary contractions, and they create an urgent need to urinate that may be difficult to control. You may feel like you need to pass urine many times during the day and night, and may also experience unintentional loss of urine (urgency incontinence).
With overactive bladder, your brain tells your bladder to empty – even when it isn’t full. Or the bladder muscles are too active. They contract (squeeze) to pass urine before your bladder is full. This causes the urge (need) to urinate.
You may have overactive bladder if you have two or more of these symptoms:
- You urinate eight or more times in 24 hours
- You wake up more than two times in the night to urinate (nocturia)
- You have the sudden, strong need to urinate immediately that’s difficult to control
- You experience unintentional loss of urine immediately after an urgent need to urinate (urgency incontinence)
Nerve problems, too much fluid, or too much caffeine can cause it. Often the cause is unknown.
Some people may have a common combination of bladder storage problems and bladder-emptying issues. The bladder may cause a lot of urgency and even incontinence, but it doesn’t empty well. A specialist may be able to help you with this combination of bladder problems.
Women who have an overactive bladder may also have a disorder called mixed incontinence, when both urgency and stress incontinence occur. Stress incontinence is the unintentional loss of urine prompted by physical movement or activity that puts pressure on your bladder, such as coughing, sneezing, laughing or exercising. Treatment of stress incontinence is not likely to help overactive bladder symptoms. Similarly, treatment of overactive bladder is not likely to improve stress incontinence symptoms.
Even if you are able to get to the toilet in time when you sense an urge to urinate, unexpected frequent urination and nighttime urination can disrupt your life.
If you have an overactive bladder, you may feel embarrassed, isolate yourself, or limit your work and social life. The good news is that a brief evaluation can determine whether there’s a specific cause for your overactive bladder symptoms.
You may be able to manage symptoms of an overactive bladder with simple behavioral strategies, such as dietary changes, timed voiding and bladder-holding techniques using your pelvic floor muscles. If these initial efforts don’t help enough with your overactive bladder symptoms, additional treatments are available.
Your doctor may prescribe a medicine that can calm muscles and nerves. The medicine may come as a pill, a liquid, or a patch. The medicines can cause your eyes to become dry. They can also cause dry mouth and constipation. To deal with these effects, use eye drops to keep your eyes moist, chew sugarless gum or suck on sugarless hard candy if dry mouth bothers you, and take small sips of water throughout the day.
Overactive bladder causes
Overactive bladder happens when the muscles of the bladder start to contract on their own even when the volume of urine in your bladder is low. These are called involuntary contractions, and they create an urgent need to urinate.
Several conditions may contribute to signs and symptoms of overactive bladder, including:
- Neurological disorders, such as stroke, Parkinson disease and multiple sclerosis
- Diabetes
- Urinary tract infections that can cause symptoms similar to those of an overactive bladder
- Hormonal changes during menopause in women
- Conditions affecting the bladder, such as tumors or bladder stones
- Factors that get in the way of urine leaving the bladder, such as enlarged prostate, constipation or previous surgery to treat incontinence
Overactive bladder symptoms may also be associated with:
- Medications that cause your body to make a lot of urine or require that you take them with lots of fluids
- Drinking too much caffeine or alcohol
- Declining cognitive function due to aging, which may make it more difficult for your bladder to understand the signals it receives from your brain
- Difficulty walking, which can lead to bladder urgency if you’re unable to get to the bathroom quickly
- Incomplete bladder emptying, which may lead to symptoms of overactive bladder, as you have little urine storage space left
The specific cause of an overactive bladder may be unknown.
Risk factors for overactive bladder
As you age, you’re at increased risk of developing overactive bladder. You’re also at higher risk of diseases and disorders, such as enlarged prostate and diabetes, which can contribute to other problems with bladder function.
Many people with cognitive decline — for instance, those who have had a stroke or have Alzheimer’s disease — develop an overactive bladder. Incontinence that results from situations like this can be managed with fluid schedules, timed and prompted voiding, absorbent garments, and bowel programs.
Some people with an overactive bladder also have bowel control problems; tell your doctor if this is a problem for you.
Overactive bladder symptoms
You may have overactive bladder if you have two or more of these symptoms:
- You urinate eight or more times in 24 hours
- You wake up more than two times in the night to urinate (nocturia)
- You have the sudden, strong need to urinate immediately that’s difficult to control
- You experience unintentional loss of urine immediately after an urgent need to urinate (urgency incontinence)
Overactive bladder prevention
These healthy lifestyle choices may reduce your risk of overactive bladder:
- Maintain a healthy weight.
- Get regular, daily physical activity and exercise.
- Limit caffeine and alcohol.
- Quit smoking.
- Manage chronic conditions, such as diabetes, that might contribute to overactive bladder symptoms.
- Do exercises to make the pelvic floor muscles stronger. These exercises are called Kegel exercises.
Overactive bladder complications
Any type of incontinence can affect your overall quality of life. If your overactive bladder symptoms cause disruption to your life, you might also have:
- Emotional distress or depression
- Anxiety
- Sleep disturbances and interrupted sleep cycles
- Issues with sexuality
In some cases, treatment of these associated conditions may help with your urinary symptoms.
Urinary urgency symptoms
Urinary urgency is a symptom of the inability to postpone urination once the sudden, strong need to urinate has been felt. This causes a discomfort in your bladder. Urinary urgency makes it difficult to delay using the toilet.
Urinary urgency diagnosis
If you have unusual urges to urinate, your doctor will take a medical history and do a physical exam, which may include a rectal exam and a pelvic exam in women.
Your doctor will check you to make sure that you don’t have an infection or blood in your urine. Your doctor may also want to make sure that you’re emptying your bladder completely when you urinate.
Your doctor will look for clues that might also indicate contributing factors. Your appointment will likely include a:
- Urine sample to test for infection, traces of blood or other abnormalities
- Focused neurological exam that may identify sensory issues or reflex problems (for some urgency problems)
Bladder diary
You may be asked to keep a Bladder Diary for a few weeks. With this, you will note how often you go to the bathroom and any time you leak urine. This will help your health care provider learn more about your day-to-day symptoms. The bladder diary helps you track:
- When and how much fluid you drink
- When and how much you urinate
- How often you have that “gotta go” urgency feeling
- When and how much urine you may leak
Having a Bladder Diary during your first visit can be helpful because it describes your daily habits, your urinary symptoms, and shows your provider how they affect your life. Your doctor will use this information to help treat you.
Lab tests
Tests that may be done include:
- Urine test: Your health care provider may ask you to leave a sample of your urine to test for infection or blood.
- Urinalysis. Urinalysis can test your urine for a bladder infection, a kidney problem, or diabetes.
- Urine culture
- Blood tests can show problems with how well your kidneys work or a chemical imbalance in your body.
- Cystoscopy. Cystoscopy is a procedure that uses a cystoscope—a long, thin instrument—to look inside the urethra and bladder.
Imaging studies
Imaging tests can be used to take pictures of the inside of the body, including the urinary tract and nervous system.
- X-rays. Two common x-ray procedures used for urinary tract imaging include:
- Intravenous pyelogram (IVP) to help locate problems in the kidneys, ureters, or bladder that may be caused by urinary retention or urinary reflux
- Voiding cystourethrogram (VCUG) to view images of the bladder and urethra taken while the bladder is full and during urination.
- Ultrasound (such as an abdominal ultrasound or a pelvic ultrasound). Ultrasound uses a hand-held device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. The health care professional can move the transducer at different angles to examine different organs. This procedure is painless, poses no risk of radiation, needs no anesthesia, and allows you to return to daily tasks immediately. Doctors use specific types of abdominal ultrasounds to look at different parts of the urinary tract.
- Bladder ultrasound can give information about the bladder wall, diverticula (pouches) of the bladder, bladder stones, and large tumors in the bladder.
- Bladder scan: This type of ultrasound shows how much urine is still in the bladder after you go to the bathroom.
- Kidney ultrasound can show if the kidneys are in the right place or if they have blockages, kidney stones, or tumors.
- Magnetic resonance imaging (MRI) scans. Magnetic resonance imaging (MRI) takes pictures of the body’s internal organs and soft tissues without using x-rays. MRI machines use radio waves and magnets to produce detailed pictures of the body’s internal organs and soft tissues. During an MRI, a special dye known as a contrast medium may be injected into the blood before the test, usually intravenously (IV) through a vein in the hand or forearm. The dye helps the radiologist see certain areas more clearly.
- Magnetic resonance urography (MRU). An magnetic resonance urography (MRU) is a type of MRI used to evaluate patients with blood in the urine, known as hematuria. MRU is also used when following up with patients who have a history of urinary tract cancers and to identify abnormalities in patients with recurrent urinary tract infections.
- Magnetic resonance angiography (MRA). An magnetic resonance angiography (MRA) is a type of MRI that provides the most detailed view of kidney arteries, which are the blood vessels that supply blood to your kidneys. An magnetic resonance angiography (MRA) can also show renal artery stenosis.
- CT scans. A CT scan combines x-rays with computer technology to create three-dimensional (3-D) images. These scans can show stones in the urinary tract, as well as obstructions, infections, cysts, tumors, and traumatic injuries. Imaging for urinary stone disease can be done with low or ultra-low dose CT scans.
- Radionuclide scans also called a nuclear scan or radioisotope scan, detects small amounts of radiation after radioactive material is injected into the blood. This scan provides information about how your kidneys function and helps health care professionals diagnose many conditions, including cancers, injuries, and infections.
- Renal scan also called kidney scan. Your health care professional might use a renal scan to check your kidneys and the urinary system. This type of exam includes injecting a small amount of radioactive material into the blood and using a special camera and computer. There are different types of renal scans, and they can be used to check the kidneys along with other imaging methods such as ultrasound, CT scans, and MRIs. Sometimes they can provide unique information that is hard to get from other imaging procedures.
Your doctor will determine which imaging tests will provide the best to find the cause of your urinary urgency.
Tests of bladder function
Your doctor may recommend urodynamic testing and electromyography to assess how well your bladder is functioning and its ability to empty steadily and completely (urodynamic tests). These tests usually require a referral to a specialist, but testing may not be necessary to make a diagnosis or begin treatment.
Urodynamic tests include:
- Measuring urine left in the bladder. This test is important if there’s concern about your ability to empty your bladder completely when you urinate. Remaining urine in the bladder (post-void residual urine) may cause symptoms identical to those of an overactive bladder. To measure residual urine after you have voided, your doctor may request an ultrasound scan of your bladder. The ultrasound scan translates sound waves into an image, showing how much urine is left in your bladder after you urinate. In some cases, a thin tube (catheter) is passed through the urethra and into your bladder to drain the remaining urine, which can then be measured.
- Measuring urine flow rate. To measure the volume and speed of your voiding, you may be asked to urinate into a device (uroflowmeter). A uroflowmeter catches and measures the urine, and translates the data into a graph of changes in your flow rate.
- Testing bladder pressures or cystometry. Cystometry is a test that measures pressure in your bladder and in the surrounding region as your bladder fills. During cystometry, your doctor uses a thin tube (catheter) to fill your bladder slowly with warm fluid. Another catheter with a pressure-measuring sensor is placed in the rectum in men or in the vagina, for women. The sensor tells how much pressure your bladder has to exert to empty completely. This procedure can identify whether you have involuntary muscle contractions or a stiff bladder that’s not able to store urine under low pressure.
Your doctor will review the results of any tests with you and suggest a treatment strategy.
Urinary urgency treatment
Urinary urgency treatment depends on the cause of the urinary urgency and/or frequency. Follow the advice of your doctor to treat the cause of the problem. You may need to take antibiotics and medicine to ease your discomfort. A combination of treatment strategies may be the best approach to relieve overactive bladder symptoms.
It may help to write down the times when you urinate and the amount of urine you produce. Bring this record to your visit with the provider. This is called a voiding diary.
In some cases, you may have problems controlling urine (incontinence) for a period of time. You may need to take steps to protect your clothing and bedding.
For nighttime urination, avoid drinking too much fluid before going to bed. Cut down on the amount of liquids you drink that contain alcohol or caffeine.
Lifestyle Changes
For overactive bladder syndrome treatment, health care providers may first ask a patient to make lifestyle changes. These changes may also be called behavioral therapy. This could mean you eat different foods, change drinking habits, and pre-plan bathroom visits to feel better. Many people find these changes help.
Behavioral interventions may include:
- Limit food and drinks that bother the bladder. There are certain foods and drinks known to irritate the bladder. You can start by avoiding diuretics – these drinks include caffeine and alcohol which encourage your body to make more urine. You can also try taking several foods out of your diet, and then add them back one at a time. This will show you which foods make your symptoms worse, so you can avoid them. You can add fiber to your diet to improve digestion. Oatmeal and whole grains are good. Fresh and dried fruit, vegetables, and beans may help. Many people feel better when they change the way they eat and drink. Some foods and drinks that may affect your bladder:
- Coffee/caffeine
- Tea
- Alcohol
- Soda and other fizzy drinks
- Some citrus fruits
- Tomato-based foods
- Chocolate (not white chocolate)
- Some spicy foods
- Keep a bladder diary. Writing down when you make trips to the bathroom for a few days can help you understand your body better. This diary may show you things that make symptoms worse. For example, are your symptoms worse after eating or drinking a certain kind of food? Are they worse when you don’t drink enough liquids?
- Scheduled toilet trips. Setting a schedule for toileting — for example, every two to four hours — gets you on track to urinate at the same times every day rather than waiting until you feel the urge to urinate.
- Bladder training. Bladder training involves training yourself to delay voiding when you feel an urge to urinate. The aim of bladder training is to improve symptoms of overactive bladder. Bladder training teaches you how to hold more urine in your bladder without feelings of urgency. You begin with small delays, such as 30 minutes, and gradually work your way up to urinating every three to four hours. Bladder training is possible only if you’re able to tighten (contract) your pelvic floor muscles successfully.
- Double voiding. This is when you empty your bladder twice. This may be helpful for people who have trouble fully emptying their bladder. After you go to the bathroom, you wait a few seconds and then try again.
- Delayed voiding. This is when you practice waiting before you go to the bathroom, even when you have to go. At first, you wait just a few minutes. Gradually, you may be able to wait two to three hours at a time. Only try this if your health care provider tells you to. Some people feel worse or have urine leaks when they wait too long to go to the bathroom.
- Timed urination. This means you follow a daily bathroom schedule. Instead of going when you feel the urge, you go at set times during the day. You and your health care provider will create a reasonable schedule. You may try to go every two to four hours, whether you feel you have to or not. The goal is to prevent that urgent feeling and to regain control.
- Kegel exercises or pelvic floor muscle exercises: tightening and holding your pelvic muscles tight, to strengthen the pelvic floor. Kegel exercises strengthen your pelvic floor muscles and urinary sphincter. These strengthened muscles can help you stop the bladder’s involuntary contractions. Your doctor or a physical therapist can help you learn how to do Kegel exercises correctly. Just like any other exercise routine, how well Kegel exercises work for you depends on whether you perform them regularly.
- There are several ways to find your pelvic floor muscles. When using the pelvic floor muscles, women will feel a slight pulling in the rectum and vagina. Men will feel a pulling-in of the anus and the penis will move. Every person is unique, and different techniques work for different people.
- To do Kegel exercise, imagine that you are in a crowded room and feel as if you must pass gas or “wind.” Most of people will squeeze the muscles of their rectum and anus (back passage) to prevent passing gas. The muscles you squeeze are the pelvic floor muscles. If you feel a “pulling” sensation at the anus, you are using the right muscles. In the majority of patients, this is the most successful technique.
- Technique for Women. Lie down and insert a finger into your vagina. Try to squeeze around your finger with your vaginal muscles. You should be able to feel the sensation in your vagina, and you may also be able to feel the pressure on your finger. If you can feel this, you are using the right muscles. If you cannot detect any movement with 1 finger, try 2 fingers.
- Technique for Men. Stand in front of a mirror and watch your penis. Try to make your penis move up and down without moving the rest of your body. If you can do this, you are using the right muscles. You may not find your pelvic floor muscles immediately. Many people have to take their time with this.
- Once you have located your pelvic floor muscles and you are able to squeeze them without using your other, stronger muscles, you are ready to begin your daily exercise program.
- You should exercise daily for two reasons:
- Exercise increases the strength of your pelvic floor muscles so that they will be strong enough to prevent urine leakage.
- Through repeated practice you gain control over these muscles. Then you can use them quickly to prevent urine loss or to decrease the urge to pass urine.
- For each exercise, you will squeeze the muscles for 5 seconds and then relax the muscles for 5 seconds. It is common for most people not to take the time to relax between squeezes. You must allow the muscles to relax between squeezes so that they can rest before squeezing again.
- To make your pelvic floor muscles stronger alternate between squeezing and relaxing them. Follow the steps below to help:
- Squeeze your muscles for one second and hold
- Relax your muscles for two seconds
- Each time you squeeze and relax, it counts as one set
- Complete five sets
- When you can do the exercises easily, increase to doing them 10 times per day. When that gets easy, try to squeeze and hold the muscles for 3 seconds and then relax the muscles for 3 seconds. As your pelvic muscles get stronger, you can progress to longer squeezes for about 10 seconds. Be sure to relax between squeezes so that your muscles can rest before squeezing again. Remember, each squeeze and relaxation counts as 1 complete set. Do the exercises in three different positions every day– 10 exercises lying down, 10 sitting, and 10 standing. The exact time of day is not crucial. What is crucial is that you develop the habit of doing the exercises every day. At first, you will need to set aside time to concentrate while you do the exercises. Find a cue or regular activity that will remind you to practice. For example, you may want to exercise just before you get up in the morning and before you fall asleep at night.
- Using Your Pelvic Muscles to Control the “Urge”. Many people think that the only way to relieve the uncomfortable sudden feeling of urgency is to empty the bladder, but this is not so. Urges can come and go without your emptying the bladder. Urges are simply messages telling you that eventually you will need to urinate. If you have an overactive bladder, the urges are often “false” messages that you need to go now. Urges, however, should not be commands. They should be an early warning system, getting you ready to find a place to urinate—-after you have relaxed and suppressed the urge. To reduce or eliminate the urge to urinate, you will use your pelvic floor muscles. You will need to squeeze your pelvic floor muscles quickly several times when you get the urge feeling. To do this, tighten/squeeze and relax the pelvic muscle as rapidly as possible. Do not relax fully in between squeezes. Try this now. Squeezing your pelvic floor muscles in this way sends a message to your nervous system and back to your bladder to stop contracting. As your bladder stops contracting and starts relaxing, the urge feeling will subside. Once the urge to urinate is gone, you have a safe period when the bladder is calm. This “calm period” is the best time to go to the bathroom.
- Make the exercises part of your daily life so that exercising becomes a habit, almost like a reflex action. Do your exercises during your daily activities or routines. After 6 weeks of practice, the exercises will require less effort, and you will no longer need to set aside special times to concentrate on them. For example, tighten the muscles when you walk, before you cough, as you stand up, and on the way to the bathroom. Try to tighten the muscle when you get a strong urge that you cannot control. It just takes practice. Do your exercises when:
- standing at the sink and brushing your teeth
- getting up in the morning
- washing dishes
- putting on your makeup
- sitting in the car at a stoplight
- sitting and having dinner
- reading a book in bed
- watching TV – during each commercial
- going for a walk
- talking on the phone
- having sex
- You do not have to keep a formal count of the number of times you do each exercise. Just do it several times in a row. Do them often enough to make them a habit.
- Healthy weight. If you’re overweight, losing weight may ease symptoms. Weight loss may help if you also have stress urinary incontinence.
- Intermittent catheterization. If you are not able to empty your bladder well, using a catheter periodically to empty your bladder completely helps your bladder do what it can’t do by itself. Ask your doctor if this approach is right for you.
- Absorbent pads. Wearing absorbent pads or undergarments can protect your clothing and help you avoid embarrassing incidents, which means that you won’t have to limit your activities. Absorbent garments come in a variety of sizes and absorbency levels.
- Quick flicks are when you quickly squeeze and relax your pelvic floor muscles over and over again. So, when you feel the urge to go, a number of quick flicks may help control that “gotta go” feeling. It helps to be still, relax and focus on just the exercise. Your health care provider or a physical therapist can help you learn these exercises.
- Biofeedback may also help you learn about your bladder. Biofeedback uses computer graphs and sounds to monitor muscle movement. During biofeedback, you’re connected to electrical sensors that help you measure and receive information about your body. It can help teach you how your pelvic muscles move and how strong they are. The biofeedback sensors teach you how to make subtle changes in your body, such as strengthening your pelvic muscles so that when you have feelings of urgency you’re better able to suppress them.
Bladder retraining
If you have conditions that produce urinary urgency or frequency, such as interstitial cystitis, you can use bladder retraining to learn to control your urge to urinate and improve your symptoms, once your pain is under control.
Bladder retraining involves learning to urinate (void) on a set schedule, not when your bladder tells you to. Bladder retraining is usually part of an overall interstitial cystitis treatment plan that includes other therapies, but if you have no pain and only mild urinary urgency and frequency symptoms, bladder retraining may be the only therapy you need.
If your symptoms are varied and pain is your major symptom, you and your healthcare professional need to address the pain before you attempt bladder retraining.
Whenever you experience pain or urgency in the bladder, the normal impulse is to urinate to stop the symptom. This establishes a pattern of frequent voiding, which can be difficult to reverse, even after your pain is controlled. To retrain your bladder, you will follow a series of simple steps to achieve longer and longer periods between urinations. Increasing bladder capacity is the objective, meaning that you will be able to hold more urine in your bladder and will not need to go as often.
Ask your healthcare provider to help you develop a bladder retraining program that suits your needs. If your symptoms are mild, you can even attempt bladder retraining on your own. Working with your healthcare team will encourage your success with bladder retraining methods and can help you stay with the program. Or, ask your healthcare provider for written instructions to explain the best approach for you and schedule regular follow-up visits to monitor your progress and encourage you. Keeping a bladder retraining diary can also help you monitor your progress and stay on track.
Often, programs begin with a four-week period of holding your urine for a set amount of time that is somewhat longer than your average voiding interval. For example, if you tend to void every 30 minutes, at your 30-minute mark, wait to void for 15 more minutes. Although the goal is to try to wait for the specified amount of time, even if you have the urge to void, go ahead and void if you have pain or discomfort before the time is up. On the other hand, if you feel the urge to urinate diminish after you wait, then try to keep waiting to stay on schedule.
Usually, after one month of training, you will increase your wait time, and after another month, you will increase it again. Although you will be trying to meet your voiding interval most of the time, it is okay if intervals are occasionally longer or shorter. Also, you don’t need to practice this technique throughout the night. The progress that you make during the day will help you to achieve a better voiding pattern around the clock.
Urinary urgency medication
When lifestyle changes aren’t enough, the next step may be to take medicine. Your doctor can tell you about special drugs for overactive bladder syndrome.
There are several drug types that can relax the bladder muscle. These drugs, like anti-muscarinics and beta-3 agonists, can help stop your bladder from squeezing when it’s not full. Some are taken as pills, by mouth. Others are gels or a sticky transdermal patch to give you the drug through your skin.
Anti-muscarinics and beta-3 adrenoceptor agonists can relax the bladder muscle and increase the amount of urine your bladder can hold and empty. Combination drugs, like using both anti-muscarinics and – beta-3 adrenoceptor agonists together may help control overactive bladder syndrome when one option alone isn’t working.
Medications that relax the bladder can be helpful for relieving symptoms of overactive bladder and reducing episodes of urge incontinence include:
- Tolterodine (Detrol)
- Oxybutynin, which can be taken as a pill (Ditropan XL) or used as a skin patch (Oxytrol) or gel (Gelnique)
- Trospium
- Solifenacin (Vesicare)
- Fesoterodine (Toviaz)
- Mirabegron (Myrbetriq)
Common side effects of most of these drugs include dry eyes and dry mouth, but drinking water to quench thirst can aggravate symptoms of overactive bladder. Constipation — another potential side effect — can aggravate your bladder symptoms. Extended-release forms of these medications, including the skin patch or gel, may cause fewer side effects.
Your doctor may recommend that you sip small amounts of water or suck on a piece of sugar-free candy or chew sugar-free gum to relieve dry mouth, and use eyedrops to keep your eyes moist. Over-the-counter preparations, such as Biotene products, can be helpful for long-term dry mouth. To avoid constipation, your doctor might recommend a fiber-rich diet or use of stool softeners.
After menopause, vaginal estrogen therapy can help strengthen the muscles and tissues in the urethra and vaginal area. Vaginal estrogen comes in the form of cream, suppository, tablet, or ring, and can significantly improve symptoms of overactive bladder.
Bladder Botox treatment
If lifestyle changes and medicine aren’t working, Botox injections may be offered. Used in small doses directly injected into bladder tissues, Botox relaxes the muscles. A trained urologist for men and women, or a female pelvic medicine and reconstructive surgeon can help with this.
Botox works for the bladder by relaxing the muscle of the bladder wall to reduce urinary urgency and urge incontinence. It can help the bladder muscles from squeezing too much. To put botulinum toxin into the bladder, your doctor will use a cystoscope passed into the bladder so the doctor can see inside the bladder. Then, the doctor will inject tiny amounts of botulinum toxin into the bladder muscle. This procedure is performed in the office with local anesthesia. The effects of Botox last up to six months. Repeat treatments will be necessary when overactive bladder syndrome symptoms return.
Your health care provider will want to know if the botulinum toxin treatment works for you. They will check to see if you get relief, or if you aren’t holding in too much urine. If urine is not releasing well, you may need to use a catheter temporarily.
Studies show that Botox injections may be useful for severe urge incontinence. The temporary effects generally last six months or more, but repeat injections are necessary.
Side effects from these injections include urinary tract infections and urinary retention. If you’re considering Botox treatments, you should be willing and able to catheterize yourself if urinary retention occurs.
Nerve stimulation
Another treatment for people who need extra help is nerve stimulation, also called neuromodulation therapy. This type of treatment sends electrical pulses to nerves that share the same path for the bladder. In overactive bladder syndrome, the nerve signals between your bladder and brain do not communicate correctly. These electrical pulses help the brain and the nerves to the bladder communicate so the bladder can function properly and improve overactive bladder syndrome symptoms.
There are two types:
- Percutaneous tibial nerve stimulation (PTNS). Percutaneous tibial nerve stimulation (peripheral) is a way to correct the nerves in your bladder. Percutaneous tibial nerve stimulation is done by placing a small electrode in your lower leg near your ankle to send electrical stimulation from a nerve in your leg (tibial nerve) to your spine, where it connects with the nerves that control the bladder. The tibial nerve runs along your knee to nerves in your lower back. The pulses help control the signals that aren’t working right. Often, patients receive percutaneous tibial nerve stimulation treatments once a week for 12 weeks, depending on how it’s working. You will likely need maintenance treatments every three to four weeks to keep symptoms under control.
- Sacral neuromodulation. Sacral neuromodulation (central) changes how the sacral nerve works. The sacral nerve carries signals between the spinal cord and the bladder. Its job is to help hold and release urine. In overactive bladder syndrome, the sacral nerve signals aren’t doing what they should. Sacral neuromodulation uses a bladder pacemaker to control these signals to stop overactive bladder syndrome symptoms. Sacral neuromodulation is a two-step surgical process. The first step is to implant an electrical wire under the skin in your lower back. This wire is first connected to a handheld pacemaker to send pulses to the sacral nerve. You and your doctor will test whether or not this pacemaker can help you. If it helps, the second step is to implant a permanent pacemaker (battery-powered pulse generator) that can regulate the nerve rhythm.
Surgery
Surgery is only used in very rare and serious cases. Surgery to treat overactive bladder is reserved for people with severe symptoms who don’t respond to other treatments. The goal is to improve the bladder’s ability to store urine and reduce pressure in the bladder. However, these procedures won’t help relieve bladder pain. There are two types of surgery available.
- Surgery to increase bladder capacity (augmentation cystoplasty). Augmentation cystoplasty procedure uses pieces of your bowel to replace a portion of your bladder. This surgery is used only in cases of severe urge incontinence that doesn’t respond to any other, more-conservative treatment measures. If you have this surgery, you may need to use a catheter intermittently for the rest of your life to empty your bladder.
- Bladder removal. This procedure is used as a last resort and involves removing the bladder and surgically constructing a replacement bladder (neobladder) or an opening in the body (stoma) to attach a bag on the skin to collect urine.
There are many risks to these surgeries, so it is offered only when no other option can help.
Alternative medicine
No complementary or alternative therapies have been proved to successfully treat overactive bladder.
Research has suggested that acupuncture might help ease the symptoms of overactive bladder. Acupuncture practitioners treat you using extremely thin, disposable needles.
Complementary treatments may not be covered by insurance, so check with your insurance company first.





{kind=link}