
What is essential tremor
Essential tremor also known as benign essential tremor, familial tremor or hereditary tremor, is a nervous system or neurological disorder that causes involuntary and rhythmic shaking (tremor) that you can’t control and can affect almost any parts of your body (hands, head, voice, legs or trunk), but the tremor happens most often in your hands 1, 2, 3, 4, 5, 6, 7, 8, 9. The tremor is typically most noticeable when holding your outstretched hands or making fine hand movements, such as holding a cup, drinking from a glass, using a spoon, writing or tying shoelaces 2. The tremor usually stops if your hands or arms are completely relaxed, such as when resting in your lap. Anxiety, fatigue or stress often makes the tremor temporarily worse.
Essential tremor is distinguished from tremor that results from other disorders or known causes, such as Parkinson’s disease or head trauma.
When doctors diagnose essential tremor, they analyze the way the tremors happen. Two key components of tremors are their frequency and their amplitude. The following example explains these terms and what they look like in a hand tremor 10:
- Amplitude: The amplitude of a tremor is the end-to-end distance your hand travels during a tremor. The larger the distance, the greater the tremor’s amplitude. The tremor amplitude usually increases as the essential tremor progresses and may vary in certain circumstances such as with action or posture.
- Frequency: Each shake of your hand is one tremor cycle. The frequency of a tremor is how many cycles you have in one second. The international unit for cycles per second is a Hertz (abbreviated Hz). Essential tremor usually causes 4 to 12 tremor cycles per second (4 to 12 Hz), but this usually slows down as tremor amplitude increases and can vary from person to person.
Essential tremor is a common disorder. Essential tremor is the most common neurological cause of postural or action tremor, affecting up to 10 million people in the United States. Estimates of its prevalence vary widely estimated prevalence of up to 10% of the population in the US because several other disorders, as well as other factors such as certain medications, can result in similar tremors. In addition, mild cases are often not brought to medical attention, or may not be detected in clinical exams that do not include the particular circumstances in which an individual’s tremor occurs. Severe cases are often misdiagnosed as Parkinson disease. The worldwide estimated prevalence of essential tremor is up to 5% of the population 1.
Essential tremor may appear at any age, but the age of onset for essential tremor has a bimodal distribution, dividing essential tremor into young onset vs. old onset essential tremor 11. Essential tremor most common in people age 40 and older with an average age of onset of 35-45 years old. Young onset essential tremor cases are more likely to have a family history of tremor 12, whereas old onset essential tremor cases often have faster disease progression 13. If a person were to have essential tremor, the disease would be prominent by 65 years of age, and virtually almost always present by 70 years old. Some studies have suggested that people with essential tremor have a higher than average risk of developing neurological conditions including Parkinson disease or sensory problems such as hearing loss, especially in individuals whose tremor appears after age 65.
Essential tremor affects both sexes equally. However, the site of involvement of the tremor is different depending on different gender. Head tremor may be more frequent in women while postural hand tremor is more frequent in men.
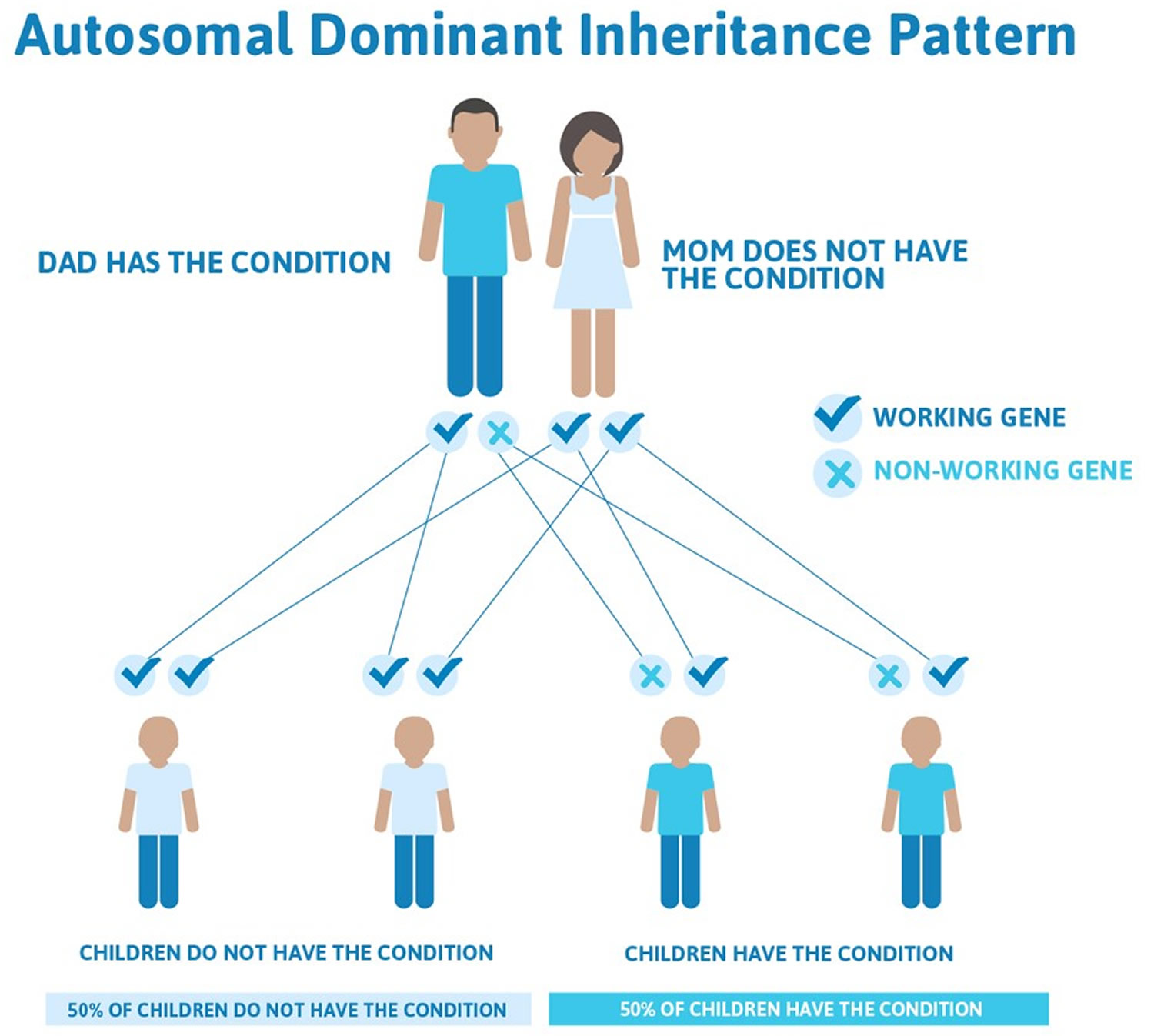
Sometimes essential tremor can be a familial disorder, in which a strong family history is seen. It is then called familial essential tremor or familial tremor. Essential tremor can be passed through generations in families, but the inheritance pattern varies. In most affected families, essential tremor appears to be inherited in an autosomal dominant pattern, which means one copy of an altered gene in each cell is sufficient to cause the disorder, although no genes that cause essential tremor have been identified. In other families, the inheritance pattern is unclear. Essential tremor may also appear in people with no history of the disorder in their family.
In some families, some individuals have essential tremor while others have other movement disorders, such as involuntary muscle tensing (dystonia). The potential genetic connection between essential tremor and other movement disorders is an active area of research.
Essential tremor usually occurs alone, without other neurological signs or symptoms. However, some experts think that essential tremor can include additional features, such as mild balance problems.
Essential tremor usually occurs with movements and can occur during many different types of activities, such as eating, drinking, or writing. Essential tremor can also occur when the muscles are opposing gravity, such as when the hands are extended. It is usually not evident at rest.
In addition to the hands and arms, muscles of the trunk, face, head, and neck may also exhibit tremor in essential tremor; the legs and feet are less often involved. Head tremor may appear as a “yes-yes” or “no-no” movement while the affected individual is seated or standing. In some people with essential tremor, the tremor may affect the voice (vocal tremor).
The exact mechanism of essential tremor is unknown 14, 15 . It is thought that certain pathways in the brain are affected where the control of fine movement occurs. However, no pathology has been identified with essential tremor.
Essential tremor does not shorten the lifespan, but essential tremor typically worsens over time and can be severe in some people. However, essential tremor may interfere with fine motor skills such as using eating utensils, writing, shaving, or applying makeup, and in some cases these and other activities of daily living can be greatly impaired. Symptoms of essential tremor may be aggravated by emotional stress, anxiety, fatigue, hunger, caffeine, cigarette smoking, or temperature extremes.
Are there different kinds of tremor?
Yes, many things can cause tremor. Not all tremors are essential tremors. For example, Parkinson’s disease causes tremor that you might notice when your hands are resting in your lap or at the sides of your body. A stroke can cause tremor that gets worse when you reach for something. Thyroid problems or low blood sugar can cause mild tremor. Tremor can be caused by some medicines. These include heart medicines, decongestants, medicines for breathing problems, and tricyclic antidepressants. Drinks that contain caffeine also may cause a tremor.
Essential tremor is just one kind of tremor. Other things that can cause a tremor (non essential tremor) include:
- Parkinson’s disease
- Multiple sclerosis (MS)
- Fatigue after exercise
- Extreme emotional stress, brain tumors
- Some prescription medicines
- Alcohol or drug withdrawal.
Is essential tremor a form of Parkinson’s disease?
No. Essential tremor is about 10 times more common than Parkinson’s disease. Unlike essential tremor, the hand tremor of Parkinson’s disease is most obvious when a patient’s hands are relaxed and not when they are being used for activities also known as resting tremor. Other signs of Parkinson’s disease, but not essential tremor, include slowness of movement (bradykinesia), shuffling gait, rigidity or stiffness and slowness and poverty of movement (hypokinesia), e.g. loss of facial expression and arm swing, difficulty with fine movements.
Is essential tremor contagious?
Experts don’t know exactly why essential tremor happens or if there are triggers that cause them to happen. However, essential tremor isn’t contagious, and you can’t catch it from or spread it to other people.
How long does essential tremor last, and can it go away?
Essential tremor is a permanent, life-long condition once it starts. It’s not curable, and it doesn’t go away on its own.
Essential tremor starts small and usually only affects your hands at first. Over time, usually many years, the tremors may spread to affect your arm and head. As the condition progresses, you may begin to struggle with certain activities and may need help to do them.
People with more severe tremors struggle with activities such as cooking, using kitchen utensils, drinking from a cup, hygiene activities, grooming and dressing. Some people who have essential tremor eventually can’t live independently and need to live with family or in an assisted living or skilled nursing facility setting.
Essential tremor vs Parkinson’s disease
Many people associate essential tremor with Parkinson’s disease, but the two conditions differ in key ways 16, 17:
- Timing of tremors. Essential tremor of the hands usually occurs when you use your hands also called an action tremor. Tremors from Parkinson’s disease are most prominent when your hands are at your sides or resting in your lap also called resting tremor.
- Associated conditions. Essential tremor doesn’t cause other health problems, but Parkinson’s disease is associated with stooped posture, slow movement (bradykinesia) and shuffling gait. However, people with essential tremor sometimes develop other neurological signs and symptoms, such as an unsteady gait (ataxia).
- Parts of body affected. Essential tremor mainly involves your hands, head and voice. Parkinson’s disease tremors usually start in your hands, and can affect your legs, chin and other parts of your body, and patients with Parkinson’s disease rarely have head or voice tremor.
The characteristics listed in the table below can help differentiate between Parkinson’s disease and essential tremor, but a medical professional should be consulted for proper diagnosis.
Many differences exist between essential tremor and Parkinson’s disease with essential tremor being at least eight times more common than Parkinson’s disease. Up to 20% of patients with essential tremor may develop Parkinson’s disease, and 10% report a family history of Parkinson’s disease. Some studies have shown a higher proportion of patients with essential tremor developing Parkinson’s disease than would be expected, ranging from 3.1 to 20.8% of those included in these studies 18, 19, 20, 21. In one study, which followed patients with and without essential tremor for several years, patients with essential tremor were four times as likely to develop Parkinson’s disease (3.0% of essential tremor patients versus 0.7% of patients without essential tremor) 18. Several families have been noted to have members with both essential tremor and Parkinson’s disease 22. In one study, patients with Parkinson’s disease were more likely to have a family history of essential tremor 23. Another study compared patients with and without Parkinson’s disease, and those with Parkinson’s disease were over 7 times as likely to have a tremor 10 years before their diagnosis, although it’s unclear if this tremor was essential tremor or an early isolated tremor 24. Both essential tremor and Parkinson’s disease can have similar “non-motor” features, such as thinking and memory changes, mood issues, and dream-enactment behavior 25. However, whether essential tremor is a risk factor for Parkinson’s disease remains an unresolved and somewhat controversial issue 26.
As essential tremor progresses, tremor frequency (number of repetitions per second) may decrease; however, tremor amplitude (magnitude/strength) may increase. Increased amplitude is associated with a decreased ability to manage fine, discrete motor tasks.
In those with Parkinson’s disease the most disabling symptoms are generally slowness, stiffness and problems with walking and balance, although tremor can also cause some disability. In Parkinson’s disease, writing often becomes very small (micrographia) and therefore difficult to read.
The severity of essential tremor and level of disability can vary greatly among patients. Some patients have a very mild tremor and therefore minimal to no disability. Others who have a severe tremor often cannot perform the majority of their daily activities and require help.
The writing of a person with essential tremor tends to be large and tremulous rather than slow and small as in Parkinson’s disease.
Anxiety can increase both essential tremor and Parkinson’s disease.
Clarifying the relationship between essential tremor and Parkinson’s disease is challenging as there is no specific diagnostic test or biomarker that reliably differentiates these two conditions 17. Many studies looking at the rates of Parkinson’s disease in patients with essential tremor are “retrospective”, meaning that they gather data from looking in the past through patients’ charts. Data that is more reliable comes from “prospective” studies that follow groups over time, but these studies are often difficult to undertake 17. Complicating matters further, essential tremor patients can sometimes have parkinsonian symptoms such as rest tremor, slowness of movement and loss or balance 27. If someone develops a rest tremor, it can sometimes be difficult to say whether their essential tremor is getting worse or whether they are beginning to show signs of Parkinson’s disease 17. In a detailed review of 300 patients followed at the Parkinson’s Disease Center and Movement Disorders Clinic, Baylor College of Medicine in Houston, Texas, 26% had evidence of associated Parkinson’s disease 17.
If there is any concern for symptoms of Parkinson’s disease, the first step is to seek out evaluation from an experienced neurologist, and preferably one with additional training in movement disorders 17. The diagnosis of Parkinson’s disease can typically be made by listening to a patient’s history and performing a physical examination, where the neurologist will look closely at your type of tremor and see if you have any slowness, stiffness, changes in your walking, or other signs of Parkinson’s disease 17. However, if there is any uncertainty about the diagnosis, the neurologist may order a DaTscan (Dopamine Transporter Scan – a diagnostic imaging procedure that visualizes the dopamine system in the brain using a radioactive tracer and a SPECT scanner) to look for evidence of decreased dopamine neurons, which would be suggestive of Parkinson’s disease.
In addition to medications and botulinum toxin, deep brain stimulation (DBS) and focused ultrasound have been used for patients with disabling tremor due to essential tremor or Parkinson’s disease 28, 29.
Essential tremor is often associated with a strong family history known as familial tremor, but no specific essential tremor-related gene has been identified.
Table 1. How Essential tremor differ from Parkinson’s disease
| Parkinson’s disease tremor signs and symptoms | Essential tremor signs and symptoms |
|---|---|
| High amplitude. Lower, slower frequency. | Low amplitude. Amplitude is more variable, ranging from barely perceptible tremor to a high amplitude tremor. Higher, faster frequency. |
| Mostly seen at rest. | Mostly seen during action. |
| Generally involves slow movements (bradykinesia), rigidity (stiffness), and problems with walking or balance. | Tremor is primary symptom – slowness, stiffness, walking and balance problems are not commonly seen. |
| Rarely a family history (<10%). | Family history of tremor reported in the majority of patients (>50%). |
| Resting and postural (re-emergent); postural tremor observable after mean latency of 5 seconds; rarely kinetic. | Postural, kinetic; postural tremor immediately observable; resting tremor less common. |
| Onset generally at ages between 55-65. | Onset most common in middle age but can occur at any time in the lifespan. |
| Usually starts on one side of the body and progresses to the other side; usually remains asymmetrical. | Usually affects both sides of the body initially (bilateral; symmetrical). |
| No effect from consumption of alcohol. | Alcohol often improves tremor. |
| Usually improves with levodopa treatment. | Improves with primidone and propranolol in some cases. |
| Hands affected more than legs, voice and head almost never affected. | Hands predominantly affected, but tremor also present in the head and voice; rarely in the legs. |
| Worsens with emotional stress. | Worsens with emotional stress. |
Essential tremor causes
The causes of essential tremor are unknown 1, 2, 30, 31, 32, 33, 34. About 50-70% of essential tremor cases appear to result from a genetic mutation, although a specific gene hasn’t been identified 35, 36, 37. This form is referred to as familial tremor. It isn’t clear what causes essential tremor in people without a known genetic mutation.
Researchers are studying several areas (loci) on particular chromosomes that may be linked to essential tremor, but no specific genetic associations have been confirmed. Several genes as well as environmental factors likely help determine an individual’s risk of developing this complex condition. Current studies suggest an autosomal dominant inheritance pattern with low penetrance in familial essential tremor, and a non‐Mendelian pattern, for example, multifactorial inheritance in sporadic essential tremor 38. Inherited neurological channelopathies may also contribute to disease pathogenesis, supported with recent functional data 39. The presence of complex non‐Mendelian inheritance patterns or environmental confounding may be contributing factors.
Researchers think essential tremor develops in your brain, but patients’ brain scans appear normal. The specific changes in the nervous system that account for the signs and symptoms of essential tremor are unknown. Some reports suggest that the neuropathology of essential tremor is localized in the brainstem at the locus coeruleus and cerebellum 4, 40, 41, 42, 43, 44, but the presence of cerebellar pathology is controversial 1.
It is believed that essential tremor is a risk factor for the development of Parkinson disease. Up to 20% of patients with essential tremor may develop Parkinson’s disease, and 10% report a family history of Parkinson’s disease. Some studies have shown a higher proportion of patients with essential tremor developing Parkinson’s disease than would be expected, ranging from 3.1 to 20.8% of those included in these studies 18, 19, 20, 21. In one study, which followed patients with and without essential tremor for several years, patients with essential tremor were four times as likely to develop Parkinson’s disease (3.0% of essential tremor patients versus 0.7% of patients without essential tremor) 18. Several families have been noted to have members with both essential tremor and Parkinson’s disease 22. In one study, patients with Parkinson’s disease were more likely to have a family history of essential tremor 23. Another study compared patients with and without Parkinson’s disease, and those with Parkinson’s disease were over 7 times as likely to have a tremor 10 years before their diagnosis, although it’s unclear if this tremor was essential tremor or an early isolated tremor 24. Both essential tremor and Parkinson’s disease can have similar “non-motor” features, such as thinking and memory changes, mood issues, and dream-enactment behavior 25. However, whether essential tremor is a risk factor for Parkinson’s disease remains an unresolved and somewhat controversial issue 26.
In addition, there has also been an association between essential tremors and dystonic movements.
Figure 1. Familial tremor autosomal dominant inheritance pattern
Environmental and Lifestyle factors
Nongenetic factors may have significant effects on essential tremor, suggested by the high prevalence of essential tremor cases without family history or affected relatives, together with reported 60–63% concordance in monozygotic twins in twin studies 45, 46
Lifestyle and environmental factors are known to play an important role in other neurological disorders. Earlier studies in essential tremor have investigated effects of dietary factors including beta‐carboline alkaloids, meat, caffeine, and alcohol intake, as well as smoking habits and occupational toxin exposures of pesticides and solvents.
Diet
Diet is a key component of life. The effects of beta‐carboline alkaloids found in meat and dietary antioxidants have been studied with no clear conclusion. New evidence suggests that ethanol (drinking alcohol), previously thought to have tremor‐relieving effects, may be a risk factor as a cerebellar toxin. Evidence on the protective effects of caffeine consumption remains inconclusive. The studies on dietary components in essential tremor have been summarized (Tables 2 and 3 below).
Table 2. Dietary exposure case‐control studies in essential tremor
| Categories | Authors | Year | Sample size | Country | Exposure | Results |
|---|---|---|---|---|---|---|
| Antioxidants | Scarmeas & Louis 47 | 2007 | 148 essential tremor, 250 controls | USA | Mediterranean diet | Higher adherence to diet was associated with lower odds for essential tremor [0.78 (0.61–0.99); P = 0.042]. Compared to lowest adherence tertile, middle tertile [0.41 (0.16–1.05)], and highest tertile [0.29 (0.10–0.82)] had a lower essential tremor odds [P for trend 0.021] |
| Louis et al. 48 | 2005 | 156 cases, 220 controls | USA | Vitamin E, vitamin C | No significant difference in vitamin E and C consumption between essential tremor cases and controls | |
| Meat (harmane) | Louis et al. 49 | 2008 | 125 cases, 125 controls | USA | Meat consumptions, meat doneness level |
|
| Louis et al. 50 | 2005 | 106 cases, 161 controls | USA | Blood harmane concentration, animal protein intake |
| |
| Harmane | Louis et al. 51 | 2013 | 130 cases, 138 controls | Spain | Blood harmane concentration | Blood harmane concentrations higher in essential tremor compared to controls, but did not reach statistical significance |
| Louis et al. 52 | 2013 | 70 cases, 27 controls | USA | Brain harmane concentration |
| |
| Louis et al. 53 | 2008 | 150 cases, 135 controls | USA | Blood harmane concentration |
| |
| Louis et al. 54 | 2002 | 100 cases, 100 controls | USA | Blood harmane concentration |
| |
| Caffeine | Prakash et al. 5566 | 2006 | 79 cases, 100 controls | Singapore | Caffeine consumption |
|
| Louis et al. 56 | 2004 | 130 cases, 175 controls | USA | Caffeine consumption |
|
Footnotes: Odds ratio (OR) is a statistical measure that quantifies the strength of association between an exposure and an outcome. Odds ratio (OR) represents the odds of an event happening in one group compared to the odds of the same event happening in another group, typically used in case-control studies 57:
Odds Ratio = (odds of the event in the exposed group) / (odds of the event in the non-exposed group)
- An OR = 1 means there’s no association between the exposure and the outcome; the odds are the same in both groups.
- An OR > 1 suggests a positive association; the odds of the outcome are higher in the exposed group.
- An OR < 1 suggests a negative association; the odds of the outcome are lower in the exposed group
Table 3. Studies on alcohol in essential tremor
| Authors | Year | Study type | Sample size | Country | Exposure | Results |
|---|---|---|---|---|---|---|
| Nicoletti et al. 58 | 2011 | Case‐control | 83 cases, 245 controls | Italy | Wine |
|
| Louis & Michalec 59 | 2014 | Case‐control | 354 cases, 370 controls | USA | Ethanol |
|
| Louis et al. 60 | 2009 | Prospective cohort study | 3285 (76 essential tremor cases) | Spain | Ethanol |
|
| Jiménez‐Jiménez et al. 61 | 2007 | Case‐control | 142 cases, 284 controls | Spain | Ethanol |
|
| Louis et al. 56 | 2004 | Case‐control | 130 cases, 175 controls | USA | Ethanol |
|
Footnotes:
Odds ratio (OR) is a statistical measure that quantifies the strength of association between an exposure and an outcome. Odds ratio (OR) represents the odds of an event happening in one group compared to the odds of the same event happening in another group, typically used in case-control studies 57:
Odds Ratio = (odds of the event in the exposed group) / (odds of the event in the non-exposed group)
- An OR = 1 means there’s no association between the exposure and the outcome; the odds are the same in both groups.
- An OR > 1 suggests a positive association; the odds of the outcome are higher in the exposed group.
- An OR < 1 suggests a negative association; the odds of the outcome are lower in the exposed group
Relative risk (RR) is a ratio of the probability of an event occurring in the exposed group versus the probability of the event occurring in the non-exposed group. Relative risk (RR) is essentially a ratio of probabilities, quantifying the effect of exposure on the outcome 62. For example, the relative risk of developing lung cancer (event) in smokers (exposed group) versus non-smokers (non-exposed group) would be the probability of developing lung cancer for smokers divided by the probability of developing lung cancer for nonsmokers. If a study shows smokers have twice the risk of lung cancer compared to non-smokers, the relative risk (RR) would be 2. The relative risk (RR) does not provide any information about the absolute risk of the event occurring, but rather the higher or lower likelihood of the event in the exposure versus the non-exposure group 63, 64.
- An RR of 1 indicates that the risk of the event is the same in both groups.
- An RR > 1 means the exposed group has a higher risk of the event than the unexposed group.
- An RR < 1 means the exposed group has a lower risk of the event than the unexposed group, suggesting a protective effect of the exposure.
Smoking
The protective effect of smoking has been reported by a series of Spanish case‐control studies (Table 4). A Spanish population‐based study reported that ever‐smokers had half the risk of essential tremor compared to never‐smokers. A dose‐dependent response was reported in the same study, with smokers in the highest pack‐year having only one‐third the risk of essential tremor compared to never‐smokers 65. In the same cohort, smoking was associated with slightly lower risk of incident essential tremor, and adjusted Cox proportional hazards model analysis supported a similar dose‐dependent association 66. Another Spanish study reported a correlation between increased period of smoking exposure and earlier age of essential tremor onset, although there were no significant associations with the amount of smoking exposure 61.
To date, the protective effect of smoking on essential tremor has been shown in studies limited to Spain and within a similar cohort 32. Studies from other populations are lacking. We cannot exclude the possibility that the protective effect of smoking may be specific to genetic or other environmental factors limited to this selected Spanish population 32. Future prospective studies in other cohorts and countries would be useful in confirming the generalizability of these findings.
Table 4. Studies on environmental exposures in essential tremor
| Authors | Year | Study type | Sample size | Country | Exposure | Results |
|---|---|---|---|---|---|---|
| Louis et al. 66 | 2008 | Prospective cohort study | 3348 (77 essential tremor cases) | Spain | Smoking |
|
| Benito‐Leon et al. 65 | 2008 | Case‐control | 221 cases, 663 controls | Spain | Smoking |
|
| Jiménez‐Jiménez et al. 61 | 2007 | Case‐control | 142 cases, 284 controls | Spain | Smoking | Time of exposure to smoking was correlated with age at onset of essential tremor. No associations found with total amount of smoking. |
| Azevedo & Meyer 67 | 2017 | Case‐control | 51 cases, 204 controls | Portugal | Pesticide exposure | Exposure to 16 to 16.9 years of pesticide use had highest odds of essential tremor (ORadj 4.60; 95% CI: 1.29–16.41) No significant correlation of essential tremor with other durations of pesticide exposure, no clear dose‐response trend. |
| Yao et al. 68 | 2015 | Cross‐sectional | 5932 (216 essential tremor cases) | China | Pesticide exposure | Past pesticide exposure was found to be greater in essential tremor compared to controls. |
| Dogu et al. 69 | 2007 | Case‐control | 105 cases, 105 controls | Turkey | Lead exposure | Higher median blood lead concentration in essential tremor cases (2.7 microg/dL) compared to controls (1.5 microg/dL) |
| Louis et al. 70 | 2006 | Case‐control | 136 cases, 144 controls | USA | Pesticide exposure | No significant difference in serum concentrations of organochlorine pesticides between essential tremor cases and controls. |
Footnotes:
Odds ratio (OR) is a statistical measure that quantifies the strength of association between an exposure and an outcome. Odds ratio (OR) represents the odds of an event happening in one group compared to the odds of the same event happening in another group, typically used in case-control studies 57:
Odds Ratio = (odds of the event in the exposed group) / (odds of the event in the non-exposed group)
- An OR = 1 means there’s no association between the exposure and the outcome; the odds are the same in both groups.
- An OR > 1 suggests a positive association; the odds of the outcome are higher in the exposed group.
- An OR < 1 suggests a negative association; the odds of the outcome are lower in the exposed group
Relative risk (RR) is a ratio of the probability of an event occurring in the exposed group versus the probability of the event occurring in the non-exposed group. Relative risk (RR) is essentially a ratio of probabilities, quantifying the effect of exposure on the outcome 62. For example, the relative risk of developing lung cancer (event) in smokers (exposed group) versus non-smokers (non-exposed group) would be the probability of developing lung cancer for smokers divided by the probability of developing lung cancer for nonsmokers. If a study shows smokers have twice the risk of lung cancer compared to non-smokers, the relative risk (RR) would be 2. The relative risk (RR) does not provide any information about the absolute risk of the event occurring, but rather the higher or lower likelihood of the event in the exposure versus the non-exposure group 63, 64.
- An RR of 1 indicates that the risk of the event is the same in both groups.
- An RR > 1 means the exposed group has a higher risk of the event than the unexposed group.
- An RR < 1 means the exposed group has a lower risk of the event than the unexposed group, suggesting a protective effect of the exposure.
Pesticides and farming
Pesticide exposure, particularly organochlorine pesticides, has been linked to tremors. However, current evidence has been inconclusive. There was no difference in serum concentrations of six organochlorine pesticides in essential tremor cases compared to controls 70. A similar lack of association with self‐reported pesticide exposure was reported by two case‐control studies in Spain and Singapore 61, 55.
In contrast to these earlier studies, a large study cohort in China reported a positive association between self‐reported pesticide exposure and essential tremor 68. Another study in Portugal reported significantly higher pesticide exposure in essential tremor 67. Although this study reported that having 16–16.9 years of exposure led to highest essential tremor risk, there was no significant dose‐dependent trend noted across the range of exposure durations reported 67, making it difficult to interpret these results in the context of other studies. A major limitation of these two studies is that they were not published in English, hence details of the study could not be assessed. Larger studies are needed to reassess the effect of pesticide exposure in essential tremor, and more quantitative methods of assessing pesticide exposure are required. Self‐reported values may not be sufficiently sensitive to detect differences between essential tremor and controls. Future studies may consider the use of surrogate measures such as occupational exposures or serum biomarkers together with self‐reported exposures.
Lead and heavy metals exposures
Exposure to heavy metals, specifically lead and manganese, has been studied in a small number of studies. Lead exposure has been shown to cause neurological disorders with tremors. essential tremor patients had higher blood lead concentrations compared to controls, reported in studies conducted in New York 71 and Turkey 69. The effect of lead toxicity may be explained by its destructive effects on cerebellar tissue and Purkinje neurons. Subsequently, no new studies have investigated the effects of lead exposure in essential tremor.
Besides lead, the role of exposures to other metals and solvents in essential tremor is inconclusive. Case‐control studies have found no significant difference in occupational exposure to manganese and organic solvents 72 or iron–manganese alloys 61 in essential tremor cases compared to controls, although iron–manganese alloy exposure was associated with increased age of essential tremor onset 61.
There is a lack of studies evaluating these toxic exposures, likely due to the difficulties in quantifying these exposures accurately. The use of serum biomarker levels may be more reliable markers of such exposures as opposed to questionnaires.
Risk factors for essential tremor
Known risk factors for essential tremor include:
- Genetic mutation. The inherited variety of essential tremor (familial tremor) is an autosomal dominant disorder. A defective gene from just one parent is needed to pass on the condition. If you have a parent with a genetic mutation for essential tremor, you have a 50 percent chance of developing the disorder yourself.
- Age. Essential tremor is more common in people age 40 and older.
Genetic mutation
The genetics basis of essential tremor has been supported by evidence of heredity in familial essential tremor. Linkage studies have mapped susceptibility loci at gene regions on chromosome 3q13 (ETM1) in Icelandic families 73, chromosome 2p22‐25 (ETM2) in American families 74 and chromosome 6p23 in North American families (ETM3) 75. Genome‐wide association studies identified mutations in the Leucine‐rich repeat and Ig domain‐containing Nogo receptor interacting protein‐1 gene (LINGO1) 76 and solute carrier family 1‐glial affinity glutamate transporter‐member 2 (SLC1A2) gene 77. Exome sequencing studies identified mutations in the fused in sarcoma/translated in liposarcoma (FUS/TLS) gene in a Canadian family 78, the HTRA2 gene in a Turkish family 79 and variants of TENM4 gene in the Spanish population 80.
Essential tremor pathophysiology
The pathophysiology of essential tremor has been debated. Some studies establish evidence of a degenerative process, while others suggest functional dysregulation of neuronal transmission 32. Postmortem studies report two main subgroups of pathology, one with the presence of Lewy bodies in the brainstem, and the other without Lewy bodies but with degenerative changes of the cerebellum, marked by Purkinje cells loss and axonal swelling 81, 82. Some hypothesized that Purkinje cell pathology may be part of the cellular cascade leading to essential tremor, causing remodeling of the cerebellar cortex leading to cerebellar degeneration 83.
The presence of Lewy bodies and protein aggregation in brain tissue supports an anatomical basis for clinical similarities between essential tremor and Parkinson’s disease such as common feature of tremor 84, although Lewy bodies are reported only in a small proportion of essential tremor patients 85. Essential tremor patients are more likely to develop Parkinson’s disease compared to healthy individuals 18, suggesting that early cellular degenerative changes may be common to both diseases. Neuroimaging has demonstrated iron accumulation in basal ganglia of essential tremor patients 86, a finding that has been similarly observed in other neurodegenerative diseases including Parkinson’s disease.
Essential tremor prevention
Doctors don’t know exactly what causes essential tremor, so it can’t be prevented. If your doctor determines you tremor is caused by medicine or caffeine, you may be able to avoid essential tremor in the future by avoiding those substances.
Essential tremor symptoms
The key symptom of essential tremor is shaking — usually your hands — when you’re trying to use them. That shaking can take different forms and usually happens under certain circumstances.
- Action tremor: This is a form of essential tremor that happens during actions, such as reaching for an object.
- Postural tremor: This is shaking that happens when you hold part of your body in a specific pose, such as holding a hand outstretched and keeping it at the same height.
Essential tremor signs and symptoms:
- Begin gradually. They usually are more noticeable on one side of the body.
- Worsen with movement
- Usually occur in the hands first, affecting one hand or both hands
- Can include a “yes-yes” or “no-no” double nodding or shaking motion of the head.
- Quivering voice
- Tremors worsen with purposeful movement
- Rest helping to relieve tremors.
- Tremors may be aggravated by emotional stress, fatigue, caffeine, certain medications, low blood sugar, or temperature extremes.
Often, tremors are the only symptom you have when you have essential tremor. Other conditions that cause tremors come with other symptoms.
Essential tremor almost always affects both sides of your body but often affects one side more than the other. In addition to your hands, tremors can affect other parts of your body such as your head, voice, face and trunk.
The tremor itself isn’t dangerous, but it can cause problems with everyday activities as the condition worsens. Eventually, people with essential tremor may have trouble with activities such as eating with utensils and drinking from a glass, dressing themselves and writing.
Essential tremor complications
Essential tremor isn’t life-threatening, but symptoms often worsen over time. If the tremors become severe, you might find it difficult to:
- Hold a cup or glass without spilling
- Eat normally
- Put on makeup or shave
- Talk, if your voice box or tongue is affected
- Write legibly
Essential tremor diagnosis
Diagnosing essential tremor involves reviewing your medical history, family history and symptoms and conducting a physical examination.
There are no medical tests to diagnose essential tremor. Diagnosing it is often a matter of ruling out other conditions that could be causing your symptoms. To do this, your doctor may suggest the following tests:
Neurological examination
In a neurological examination, your doctor surveys your nervous system functioning, including checking your:
- Tendon reflexes
- Muscle strength and tone
- Ability to feel certain sensations
- Posture and coordination
- Gait
Laboratory tests
Your blood and urine may be tested for several factors, including:
- Thyroid disease
- Metabolic problems e.g. Wilson’s disease
- Drug side effects
- Alcohol levels
- Levels of metals like lead or manganese that may cause tremor
- Genetic testing. This tests for gene changes if there is a known family history of Parkinson’s disease or if you have familial tremor.
- Alpha-synuclein test. Alpha-synuclein test also called an alpha-synuclein seed amplification assay, detects Parkinson’s disease before symptoms begin. Alpha-synuclein clumps are a hallmark sign of Parkinson’s disease. Doctor can test for Parkinson’s disease in the skin or spinal fluid. Alpha-synuclein is found in Lewy bodies. It forms clumps that the body can’t break down. The clumps spread and damage brain cells. In a 2023 study, researchers tested the spinal fluid of more than 1,000 people to look for clumps of the protein alpha-synuclein. The alpha-synuclein test accurately identified people with Parkinson’s disease 87.7% of the time. Alpha-synuclein test also was highly sensitive for detecting people at risk of Parkinson’s disease. This study of the alpha-synuclein seed amplification assay was the largest so far. Some researchers say the study may be a breakthrough for Parkinson’s disease diagnosis, research and treatment trials. But larger studies are needed. There’s hope among researchers that in the future, the alpha-synuclein test could be done using blood samples rather than spinal fluid.
Imaging tests
These imaging tests can help rule out other conditions:
- Computerized tomography (CT) scan. A head CT (computed tomography) scan, also known as a CAT scan, is a medical imaging technique that uses X-rays to create detailed 3D images of the brain, skull, and surrounding structures, helping to diagnose various conditions like strokes, tumors, and injuries. These scans provide a more detailed view than a regular X-ray and can be used to diagnose a wide range of conditions.
- Magnetic resonance imaging (MRI). An head MRI (Magnetic Resonance Imaging) scan is a non-invasive medical imaging technique that uses strong magnetic fields and radio waves to create detailed images of the body’s internal structures. Your doctor can order MRI of your brain and surrounding nerve tissue inside your head using MRI.
- Positron emission tomography (PET) scan. A positron emission tomography (PET) scan is a nuclear medicine imaging technique that uses radioactive tracers to visualize and measure changes in metabolic processes within the body. These scans can help diagnose diseases, monitor treatment effectiveness, and assess organ function. Your doctor may order a PET scan to check for signs of brain disorders such as brain tumors, epilepsy, dementia and Alzheimer’s disease.
- A specific single-photon emission computerized tomography (SPECT) scan called a dopamine transporter (DAT) scan. This can help support the suspicion that you have Parkinson’s disease and help identify different types of tremor. But it is your symptoms and the results of your neurological exam that determine your diagnosis. Most people do not require a DAT scan.
Performance tests
To evaluate the tremor itself, your doctor may ask you to:
- Drink from a glass
- Hold your arms outstretched
- Write
- Draw a spiral
If your doctor is still unsure if your tremor is essential tremor or Parkinson’s disease, he or she might order a dopamine transporter scan (DaTscan). This can tell the difference between the two types of tremor. A special picture or scan of the brain that measures the uptake of dopamine, such as DaTscan, can help to differentiate between essential tremor and Parkinson’s disease tremor. Dopamine is depleted in patients with Parkinson’s disease but not in patients with essential tremor; therefore, scans showing depletion in dopamine are most likely Parkinson’s disease and normal scans would suggest a more likely diagnosis of essential tremor. These scans are used as a tool to help the physician make an accurate diagnosis in difficult cases.
Essential tremor diagnostic criteria
The Movement Disorders Society diagnostic criteria include 27, 87:
- Tremor is bilateral, symmetrical, and postural
- The tremor involves the forearms and hand
- Is persistent and visible
- It may be associated with isolated head tremor
- The absence of other neurological signs, such as dystonia, ataxia, and parkinsonism.
While these criteria provide useful research guidelines, it is increasingly recognized that 54–85% patients who otherwise fit the essential tremor diagnostic criteria have above-mentioned neurological signs (e.g., dystonia, ataxia, and parkinsonism) and some experts categorize this group of patients with a controversial term: essential tremor-plus 88, 31.
Essential tremor treatment
Some people with essential tremor don’t require treatment if their symptoms are mild and early treatment does not stop or slow essential tremor symptomatic progression. But if your essential tremor is making it difficult to work or perform daily activities, discuss treatment options with your doctor. Only consider starting medication treatment when the tremor affects your daily activities or causes problems for you.
Essential tremor medications
- Beta blockers. Normally used to treat high blood pressure, beta blockers such as propranolol (Inderal) help relieve tremors in some people. This is the most common medication used for treatment of essential tremor. Multiple studies have shown that propanolol improves the symptoms ranging from 50-70% of the patients. However, no long term study has been conducted regarding the effect of propanolol in essential tremor. Other beta-blockers include atenolol, metoprolol, sotalol and nadolol. Beta blockers may not be an option if you have asthma or certain heart problems. Side effects may include fatigue, lightheadedness or heart problems.
- Anti-seizure medications. Epilepsy drugs, such as primidone (Mysoline), may be effective in people who don’t respond to beta blockers. The exact mechanism is unknown. Other medications that might be prescribed include gabapentin (Gralise, Neurontin) and topiramate (Topamax, Qudexy XR). However most of these anticonvulsants are not well studied – only small and short trials have been done to evaluate their effectiveness. Side effects include drowsiness and nausea, which usually disappear within a short time.
- Tranquilizers (benzodiazepines). Doctors may use drugs such as alprazolam (Xanax) and clonazepam (Klonopin) to treat people for whom tension or anxiety worsens tremors. Side effects can include fatigue or mild sedation. These medications should be used with caution because they can be habit-forming (addictive).
- OnabotulinumtoxinA (Botox) injections. Botulinum toxin is injected into the muscles that cause the tremor, temporarily weakening the muscle to reduce the tremor. Botox injections might be useful in treating some types of tremors, especially head and voice tremors. Botox injections can improve tremors for up to three months at a time. However, if Botox is used to treat hand tremors, it can cause weakness in your fingers. If it’s used to treat voice tremors, it can cause a hoarse voice and difficulty swallowing.
Essential tremor natural remedies
Lifestyle changes are often recommended to prevent the tremor from getting worse. Your doctor will ask you to avoid caffeine, cold medicines and certain other medicines if they seem to make your tremor worse. These medicines won’t make your tremor go away. However, the medicine may control the tremor enough to allow you to do normal activities without frustration or embarrassment.
To reduce or relieve tremors:
- Avoid caffeine. Caffeine and other stimulants can increase tremors.
- Use alcohol sparingly, if at all. Some people notice that their tremors improve slightly after they drink alcohol, but drinking isn’t a good solution. Tremors tend to worsen once the effects of alcohol wear off. Also, increasing amounts of alcohol eventually are needed to relieve tremors, which can lead to alcoholism.
- Learn to relax. Stress and anxiety tend to make tremors worse, and being relaxed may improve tremors. Although you can’t eliminate all stress from your life, you can change how you react to stressful situations using a range of relaxation techniques, such as massage or meditation.
- Make lifestyle changes. Use the hand less affected by tremor more often. Find ways to avoid writing with the hand affected by tremor, such as using online banking and debit cards instead of writing checks. Try voice-activated dialing on your cellphone and speech-recognition software on your computer.
Physical therapy
Doctors might suggest physical or occupational therapy. Physical therapists can teach you exercises to improve your muscle strength, control and coordination.
Occupational therapists can help you adapt to living with essential tremor. Therapists might suggest adaptive devices to reduce the effect of tremors on your daily activities, including:
- Heavier glasses and utensils
- Wrist weights
- Wider, heavier writing tools, such as wide-grip pens.
Nerve stimulation devices
A wearable electronic peripheral nerve stimulation device (Cala Trio, Cala kIQ) is a newer treatment option for people with essential tremor. The device is worn as a wristband for 40 minutes twice a day. It works by stimulating nerves and muscles to create a muscle response that reduces tremors. Studies have found that the device can bring some improvement for tremors.
Focused ultrasound thalamotomy
Focused ultrasound thalamotomy is a non-invasive neurosurgical procedure that uses focused ultrasound waves that travel through the skin and skull to target and destroy specific areas of the thalamus, a part of the brain involved in motor control, to reduce or eliminate tremors, particularly those associated with essential tremor or Parkinson’s disease 89, 90. During a focused ultrasound thalamotomy procedure a surgeon uses Magnetic Resonance Imaging (MRI – a medical imaging technique that uses strong magnetic fields and radio waves to create detailed, cross-sectional images of the body’s internal structures) to target the correct area of the brain and to be sure the sound waves are generating the exact amount of heat needed for the procedure.
Focused ultrasound thalamotomy is done on one side of the brain. The surgery affects the other side of the body from the one where it’s done. For example, focused ultrasound thalamotomy on the right thalamus affects the left side of your body. This is due to a phenomenon called contralateral control, where nerve pathways cross over in the brainstem, connecting the brain hemispheres to the opposite sides of the body where the left side of your brain generally controls the right side of your body, and the right side of your brain controls the left side of your body.
Focused ultrasound thalamotomy creates a lesion that can result in permanent changes to brain function. Some people have experienced altered sensation, trouble with walking or difficulty with movement. However, most complications go away on their own or are mild enough that they don’t interfere with quality of life.
Deep brain stimulation (DBS)
Deep brain stimulation (DBS) might be an option if your tremors are severely disabling and you don’t respond to medications 91. The surgical procedures are stereotactic thalamotomy or thalamic deep brain stimulation. Excellent results have been reported from these surgeries.
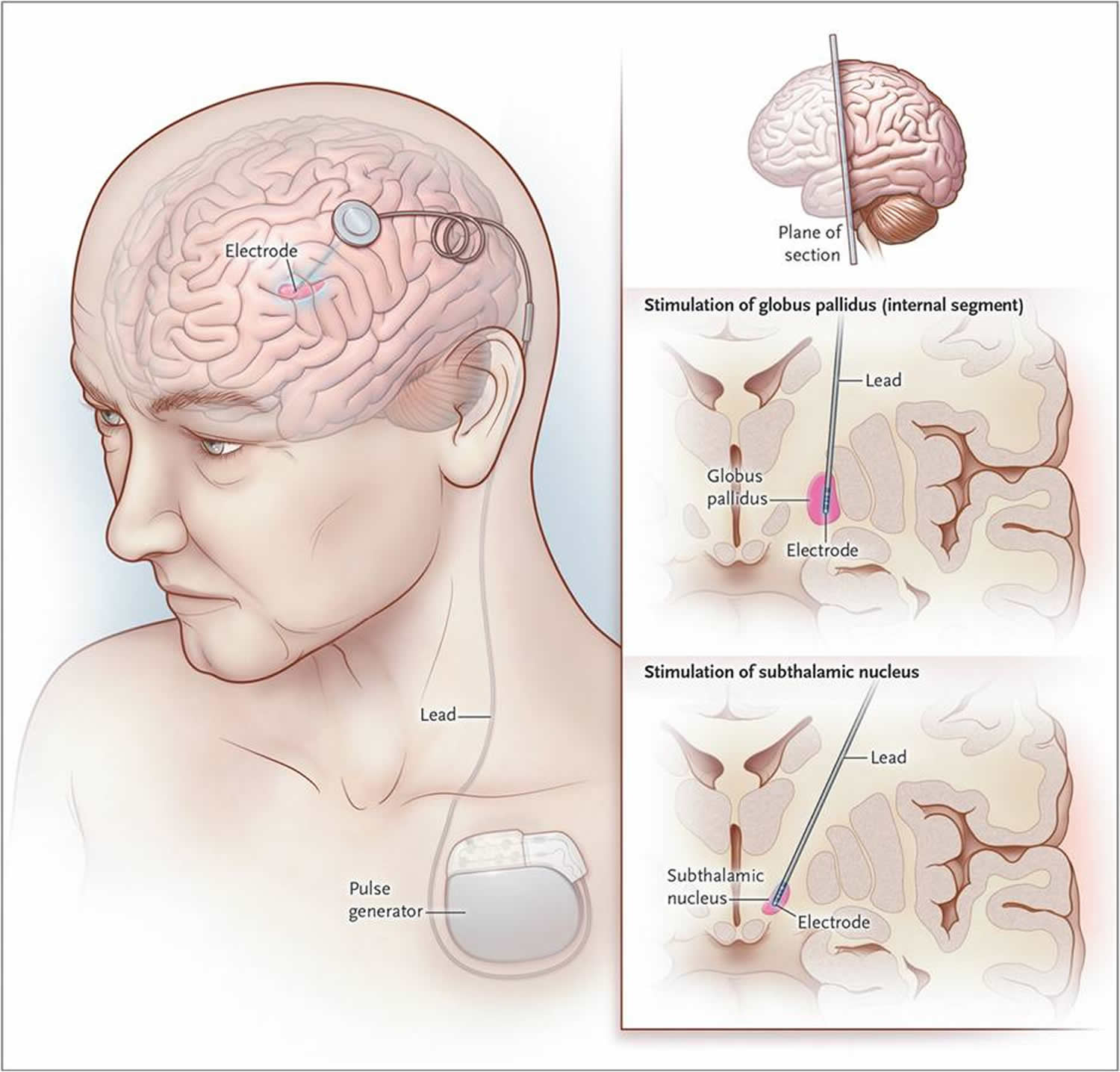
In deep brain stimulation, doctors insert a long, thin electrical probe into the portion of your brain that causes your tremors (thalamus). A wire from the probe runs under your skin to a pacemaker-like device (neurostimulator) implanted in your chest. This device transmits painless electrical pulses to interrupt signals from your thalamus that may be causing your tremors.
Side effects of surgery can include equipment malfunction; problems with motor control, speech or balance; headaches; and weakness. Side effects often go away after some time or adjustment of the device.
Figure 2. Deep brain stimulation
Coping and support
For many people, essential tremor can have serious social and psychological consequences. If the effects of essential tremor make it difficult to live your life as fully as you once did, consider joining a support group like International Essential Tremor Foundation (https://www.essentialtremor.org/).
Support groups aren’t for everyone, but you might find it helpful to have the encouragement of people who understand what you’re going through. Or see a counselor or social worker who can help you meet the challenges of living with essential tremor.
Essential tremor prognosis
Essential tremor is not a life-threatening condition. Survival in essential tremor does not differ from the general population 1, 2. Although there is no associated death rate, it can cause significant inconvenience to the patients and the overall quality of life can be significantly impaired with essential tremor 2. This is due to the social and functional embarrassment that usually occur in activities of daily living such as employment, normal outing activities such as difficulty writing, eating, and drinking, attending parties, shopping alone, etc. As much as 85% of the patients with essential tremor reported that this condition affected their lifestyle in certain ways. Essential tremor symptoms are typically progressive and potentially disabling, often forcing patients to change jobs or seek early retirement 92, 93, 94, 95.
Although prospective longitudinal data are limited, the usual course of essential tremor is one of slow, gradual progression 96, 1. The average rate that arm or hand tremors get worse is between 1.5% and 5% a year. As essential tremor progresses, tremor frequency (number of repetitions per second) may decrease; however, tremor amplitude (magnitude/strength) may increase. Increased amplitude is associated with a decreased ability to manage fine, discrete motor tasks. Essential tremor starts small and usually only affects your hands at first. Over time, usually many years, the tremors may spread to affect your arm and head. As the condition progresses, you may begin to struggle with certain activities and may need help to do them.
Essential tremor may remain stable in a minority of patients. However, a stable course should raise suspicion for an alternative diagnosis such as an enhanced, physiologic tremor or drug-induced tremor rather than an essential tremor 1. While prospective data are limited, essential tremors may be associated with an increased risk for developing Parkinson disease 1.
- Agarwal S, Biagioni MC. Essential Tremor. [Updated 2023 Jul 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499986[↩][↩][↩][↩][↩][↩][↩][↩]
- Essential Tremor: Essential Facts for Patients. https://www.movementdisorders.org/MDS-Files1/Resources/PDFs/Essentialtremorpatientleaflet.pdf[↩][↩][↩][↩][↩]
- Elble RJ. What is essential tremor? Curr Neurol Neurosci Rep. 2013 Jun;13(6):353. doi: 10.1007/s11910-013-0353-4[↩]
- Louis ED, Faust PL. Essential tremor: the most common form of cerebellar degeneration? Cerebellum Ataxias. 2020 Aug 14;7:12. doi: 10.1186/s40673-020-00121-1[↩][↩]
- Ray A, Biswas DA. Association of Diet With Essential Tremor: A Narrative Review. Cureus. 2022 Sep 14;14(9):e29168. doi: 10.7759/cureus.29168[↩]
- Health Quality Ontario. Magnetic Resonance-Guided Focused Ultrasound Neurosurgery for Essential Tremor: A Health Technology Assessment. Ont Health Technol Assess Ser. 2018 May 3;18(4):1-141. https://pmc.ncbi.nlm.nih.gov/articles/PMC5963668[↩]
- Alonso-Navarro H, García-Martín E, Agúndez JAG, Jiménez-Jiménez FJ. Current and Future Neuropharmacological Options for the Treatment of Essential Tremor. Curr Neuropharmacol. 2020;18(6):518-537. doi: 10.2174/1570159X18666200124145743[↩]
- Hopfner F, Deuschl G. Managing Essential Tremor. Neurotherapeutics. 2020 Oct;17(4):1603-1621. doi: 10.1007/s13311-020-00899-2. Erratum in: Neurotherapeutics. 2021 Jul;18(3):2132. doi: 10.1007/s13311-021-01131-5[↩]
- Pan MK, Kuo SH. Essential tremor: Clinical perspectives and pathophysiology. J Neurol Sci. 2022 Apr 15;435:120198. doi: 10.1016/j.jns.2022.120198[↩]
- Wagle Shukla A. Diagnosis and Treatment of Essential Tremor. Continuum (Minneap Minn). 2022 Oct 1;28(5):1333-1349. doi: 10.1212/CON.0000000000001181[↩]
- Louis ED, Dogu O, Does age of onset in essential tremor have a bimodal distribution? Data from a tertiary referral setting and a population-based study, Neuroepidemiology 29 (2007) 208–212, 10.1159/000111584[↩]
- Hopfner F, et al. , Early- and late-onset essential tremor patients represent clinically distinct subgroups, Mov. Disord 31 (2016) 1560–1566, 10.1002/mds.26708[↩]
- Louis ED, et al. , Older onset essential tremor: more rapid progression and more degenerative pathology, Mov. Disord 24 (2009) 1606–1612, 10.1002/mds.22570[↩]
- McKinnon C, Gros P, Lee DJ, Hamani C, Lozano AM, Kalia LV, Kalia SK. Deep brain stimulation: potential for neuroprotection. Ann Clin Transl Neurol. 2018 Nov 8;6(1):174-185. doi: 10.1002/acn3.682[↩]
- Vogelnik K, Kojovic M. From beta-blockers to Parkinson’s disease in respect of essential tremor. Mov Disord. 2019 Jan;34(1):153. doi: 10.1002/mds.27586[↩]
- Essential tremor. https://www.mayoclinic.org/diseases-conditions/essential-tremor/symptoms-causes/syc-20350534[↩]
- The Relationship Between Essential Tremor and Parkinson’s Disease. https://essentialtremor.org/the-relationship-between-essential-tremor-and-parkinsons-disease[↩][↩][↩][↩][↩][↩][↩]
- Benito-León J, Louis ED, Bermejo-Pareja F; Neurological Disorders in Central Spain Study Group. Risk of incident Parkinson’s disease and parkinsonism in essential tremor: a population based study. J Neurol Neurosurg Psychiatry. 2009 Apr;80(4):423-5. doi: 10.1136/jnnp.2008.147223[↩][↩][↩][↩][↩]
- Koller WC, Busenbark K, Miner K. The relationship of essential tremor to other movement disorders: report on 678 patients. Essential Tremor Study Group. Ann Neurol. 1994 Jun;35(6):717-23. doi: 10.1002/ana.410350613[↩][↩]
- Geraghty JJ, Jankovic J, Zetusky WJ. Association between essential tremor and Parkinson’s disease. Ann Neurol. 1985 Apr;17(4):329-33. doi: 10.1002/ana.410170404[↩][↩]
- Tan EK, Lee SS, S FC, Lum SY. Evidence of increased odds of essential tremor in Parkinson’s disease. Mov Disord. 2008 May 15;23(7):993-997. doi: 10.1002/mds.22005[↩][↩]
- van der Stouwe AMM, Everlo CSJ, Tijssen MAJ. Which disease features run in essential tremor families? A systematic review. Parkinsonism Relat Disord. 2019 Dec;69:71-78. doi: 10.1016/j.parkreldis.2019.10.017[↩][↩]
- Spanaki C, Plaitakis A. Essential tremor in Parkinson’s disease kindreds from a population of similar genetic background. Mov Disord. 2009 Aug 15;24(11):1662-8. doi: 10.1002/mds.22655[↩][↩]
- Schrag A, Horsfall L, Walters K, Noyce A, Petersen I. Prediagnostic presentations of Parkinson’s disease in primary care: a case-control study. Lancet Neurol. 2015 Jan;14(1):57-64. doi: 10.1016/S1474-4422(14)70287-X[↩][↩]
- Tarakad A, Jankovic J. Essential Tremor and Parkinson’s Disease: Exploring the Relationship. Tremor Other Hyperkinet Mov (N Y). 2019 Jan 9;8:589. doi: 10.7916/D8MD0GVR[↩][↩]
- Fekete R, Jankovic J. Revisiting the relationship between essential tremor and Parkinson’s disease. Mov Disord. 2011 Feb 15;26(3):391-8. doi: 10.1002/mds.23512[↩][↩]
- Bhatia KP, Bain P, Bajaj N, Elble RJ, Hallett M, Louis ED, Raethjen J, Stamelou M, Testa CM, Deuschl G; Tremor Task Force of the International Parkinson and Movement Disorder Society. Consensus Statement on the classification of tremors. from the task force on tremor of the International Parkinson and Movement Disorder Society. Mov Disord. 2018 Jan;33(1):75-87. doi: 10.1002/mds.27121[↩][↩]
- Mittal SO, Lenka A, Jankovic J. Botulinum toxin for the treatment of tremor. Parkinsonism Relat Disord. 2019 Jun;63:31-41. doi: 10.1016/j.parkreldis.2019.01.023[↩]
- Jankovic J, Tan EK. Parkinson’s disease: etiopathogenesis and treatment. J Neurol Neurosurg Psychiatry. 2020 Aug;91(8):795-808. doi: 10.1136/jnnp-2019-322338[↩]
- Benito-León J, Serrano JI, Louis ED, Holobar A, Romero JP, Povalej-Bržan P, Kranjec J, Bermejo-Pareja F, Del Castillo MD, Posada IJ, Rocon E. Essential tremor severity and anatomical changes in brain areas controlling movement sequencing. Ann Clin Transl Neurol. 2018 Nov 8;6(1):83-97. doi: 10.1002/acn3.681[↩]
- Prasad S, Pal PK. Reclassifying essential tremor: Implications for the future of past research. Mov Disord. 2019 Mar;34(3):437. doi: 10.1002/mds.27615[↩][↩]
- Ong YL, Deng X, Tan EK. Etiologic links between environmental and lifestyle factors and Essential tremor. Ann Clin Transl Neurol. 2019 May 1;6(5):979-989. doi: 10.1002/acn3.758[↩][↩][↩][↩][↩][↩][↩]
- Louis ED, Eliasen EH, Ferrer M, Iglesias Hernandez D, Gaini S, Jiang W, Zheng W, Nielsen F, Petersen MS. Blood Harmane (1-Methyl-9H-Pyrido[3,4-b]indole) and Mercury in Essential Tremor: A Population-Based, Environmental Epidemiology Study in the Faroe Islands. Neuroepidemiology. 2020;54(3):272-280. doi: 10.1159/000505874[↩]
- Deuschl G, Petersen I, Lorenz D, Christensen K. Tremor in the elderly: Essential and aging-related tremor. Mov Disord. 2015 Sep;30(10):1327-34. doi: 10.1002/mds.26265[↩]
- Siokas V, Aloizou AM, Tsouris Z, Liampas I, Aslanidou P, Dastamani M, Brotis AG, Bogdanos DP, Hadjigeorgiou GM, Dardiotis E. Genetic Risk Factors for Essential Tremor: A Review. Tremor Other Hyperkinet Mov (N Y). 2020 Jun 11;10:4. doi: 10.5334/tohm.67[↩]
- Liao C, Castonguay CE, Heilbron K, et al. 23andMe Research Team. Association of Essential Tremor With Novel Risk Loci: A Genome-Wide Association Study and Meta-analysis. JAMA Neurol. 2022 Feb 1;79(2):185-193. doi: 10.1001/jamaneurol.2021.4781. Erratum in: JAMA Neurol. 2022 Mar 1;79(3):313. doi: 10.1001/jamaneurol.2021.5444[↩]
- Sailani MR, Jahanbani F, Abbott CW, Lee H, Zia A, Rego S, et al. (2020) Candidate variants in TUB are associated with familial tremor. PLoS Genet 16(9): e1009010. https://doi.org/10.1371/journal.pgen.1009010[↩]
- Ma S, Davis TL, Blair MA, Fang JY, Bradford Y, Haines JL, Hedera P. Familial essential tremor with apparent autosomal dominant inheritance: should we also consider other inheritance modes? Mov Disord. 2006 Sep;21(9):1368-74. doi: 10.1002/mds.20950[↩]
- Smith P, Arias R, Sonti S, Odgerel Z, Santa-Maria I, McCabe BD, Tsaneva-Atanasova K, Louis ED, Hodge JJL, Clark LN. A Drosophila Model of Essential Tremor. Sci Rep. 2018 May 16;8(1):7664. doi: 10.1038/s41598-018-25949-w[↩]
- Benito-Leon J, Labiano-Fontcuberta A. Linking Essential Tremor to the Cerebellum: Clinical Evidence. Cerebellum. 2016;15(3):253–262. doi: 10.1007/s12311-015-0741-1[↩]
- Cerasa A, Quattrone A. Linking Essential Tremor to the Cerebellum-Neuroimaging Evidence. Cerebellum. 2016;15(3):263–275. doi: 10.1007/s12311-015-0739-8[↩]
- Marin-Lahoz J, Gironell A. Linking Essential Tremor to the Cerebellum: Neurochemical Evidence. Cerebellum. 2016;15(3):243–252. doi: 10.1007/s12311-015-0735-z[↩]
- Maas R, Helmich RCG, van de Warrenburg BPC. The role of the cerebellum in degenerative ataxias and essential tremor: Insights from noninvasive modulation of cerebellar activity. Mov Disord. 2020;35(2):215–227. doi: 10.1002/mds.27919[↩]
- Mavroudis I, Petridis F, Kazis D. Neuroimaging and neuropathological findings in essential tremor. Acta Neurol Scand. 2019;139(6):491–496. doi: 10.1111/ane.13101[↩]
- Tanner CM, Goldman SM, Lyons KE, Aston DA, Tetrud JW, Welsh MD, Langston JW, Koller WC. Essential tremor in twins: an assessment of genetic vs environmental determinants of etiology. Neurology. 2001 Oct 23;57(8):1389-91. doi: 10.1212/wnl.57.8.1389[↩]
- Lorenz D, Frederiksen H, Moises H, Kopper F, Deuschl G, Christensen K. High concordance for essential tremor in monozygotic twins of old age. Neurology. 2004 Jan 27;62(2):208-11. doi: 10.1212/01.wnl.0000103236.26934.41[↩]
- Scarmeas N, Louis ED. Mediterranean diet and essential tremor. A case-control study. Neuroepidemiology. 2007;29(3-4):170-7. doi: 10.1159/000111579[↩]
- Louis ED, Jurewicz EC, Parides MK. Case-control study of nutritional antioxidant intake in essential tremor. Neuroepidemiology. 2005;24(4):203-8. doi: 10.1159/000084713[↩]
- Louis ED, Keating GA, Bogen KT, Rios E, Pellegrino KM, Factor-Litvak P. Dietary epidemiology of essential tremor: meat consumption and meat cooking practices. Neuroepidemiology. 2008;30(3):161-6. doi: 10.1159/000122333[↩]
- Louis ED, Zheng W, Applegate L, Shi L, Factor-Litvak P. Blood harmane concentrations and dietary protein consumption in essential tremor. Neurology. 2005 Aug 9;65(3):391-6. doi: 10.1212/01.wnl.0000172352.88359.2d[↩]
- Louis ED, Benito-León J, Moreno-García S, Vega S, Romero JP, Bermejo-Pareja F, Gerbin M, Viner AS, Factor-Litvak P, Jiang W, Zheng W. Blood harmane (1-methyl-9H-pyrido[3,4-b]indole) concentration in essential tremor cases in Spain. Neurotoxicology. 2013 Jan;34:264-8. doi: 10.1016/j.neuro.2012.09.004[↩]
- Louis ED, Factor-Litvak P, Liu X, Vonsattel JP, Galecki M, Jiang W, Zheng W. Elevated brain harmane (1-methyl-9H-pyrido[3,4-b]indole) in essential tremor cases vs. controls. Neurotoxicology. 2013 Sep;38:131-5. doi: 10.1016/j.neuro.2013.07.002[↩]
- Louis ED, Jiang W, Pellegrino KM, Rios E, Factor-Litvak P, Henchcliffe C, Zheng W. Elevated blood harmane (1-methyl-9H-pyrido[3,4-b]indole) concentrations in essential tremor. Neurotoxicology. 2008 Mar;29(2):294-300. doi: 10.1016/j.neuro.2007.12.001[↩]
- Louis ED, Zheng W, Jurewicz EC, Watner D, Chen J, Factor-Litvak P, Parides M. Elevation of blood beta-carboline alkaloids in essential tremor. Neurology. 2002 Dec 24;59(12):1940-4. doi: 10.1212/01.wnl.0000038385.60538.19[↩]
- Prakash KM, Fook-Choong S, Yuen Y, Tan EK. Exploring the relationship between caffeine intake and essential tremor. J Neurol Sci. 2006 Dec 21;251(1-2):98-101. doi: 10.1016/j.jns.2006.09.007[↩][↩]
- Louis ED, Jurewicz EC, Applegate L, Luchsinger JA, Factor-Litvak P, Parides M. Semiquantitative study of current coffee, caffeine, and ethanol intake in essential tremor cases and controls. Mov Disord. 2004 May;19(5):499-504. doi: 10.1002/mds.20035[↩][↩]
- Tenny S, Hoffman MR. Odds Ratio. [Updated 2023 May 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431098[↩][↩][↩]
- Nicoletti A, Mostile G, Cappellani R, Contrafatto D, Arabia G, Lamberti P, Marconi R, Morgante L, Barone P, Quattrone A, Zappia M. Wine drinking and essential tremor: a possible protective role. Mov Disord. 2011 Jun;26(7):1310-5. doi: 10.1002/mds.23603[↩]
- Louis ED, Michalec M. Semi-quantitative data on ethanol consumption in 354 ET cases and 370 controls. J Neurol Sci. 2014 Dec 15;347(1-2):174-8. doi: 10.1016/j.jns.2014.09.042[↩]
- Louis ED, Benito-León J, Bermejo-Pareja F. Population-based study of baseline ethanol consumption and risk of incident essential tremor. J Neurol Neurosurg Psychiatry. 2009 May;80(5):494-7. doi: 10.1136/jnnp.2008.162701[↩]
- Jiménez-Jiménez FJ, de Toledo-Heras M, Alonso-Navarro H, Ayuso-Peralta L, Arévalo-Serrano J, Ballesteros-Barranco A, Puertas I, Jabbour-Wadih T, Barcenilla B. Environmental risk factors for essential tremor. Eur Neurol. 2007;58(2):106-13. doi: 10.1159/000103646[↩][↩][↩][↩][↩][↩]
- Tenny S, Hoffman MR. Relative Risk. [Updated 2023 Mar 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430824[↩][↩]
- Andrade C. Understanding relative risk, odds ratio, and related terms: as simple as it can get. J Clin Psychiatry. 2015 Jul;76(7):e857-61. doi: 10.4088/JCP.15f10150[↩][↩]
- Simon SD. Understanding the odds ratio and the relative risk. J Androl. 2001 Jul-Aug;22(4):533-6. https://onlinelibrary.wiley.com/doi/epdf/10.1002/j.1939-4640.2001.tb02212.x[↩][↩]
- Benito-León J, Louis ED, Bermejo-Pareja F; Neurological Disorders in Central Spain (NEDICES) Study Group. Population-based case-control study of cigarette smoking and essential tremor. Mov Disord. 2008 Jan 30;23(2):246-52. doi: 10.1002/mds.21810[↩][↩]
- Louis ED, Benito-León J, Bermejo-Pareja F; Neurological Disorders in Central Spain (NEDICES) Study Group. Population-based prospective study of cigarette smoking and risk of incident essential tremor. Neurology. 2008 May 6;70(19):1682-7. doi: 10.1212/01.wnl.0000311271.42596.32[↩][↩]
- Azevedo MFA, Meyer A. Tremor essencial em guardas de endemias expostos a agrotóxicos: estudo caso-controle [Essential tremor in endemic disease control agents exposed to pesticides: a case-control study]. Cad Saude Publica. 2017 Aug 21;33(8):e00194915. Portuguese. doi: 10.1590/0102-311X00194915[↩][↩][↩]
- Yao Y, Wang Y, Yang X. [Related factors and prevalence for the essential tremor disease of Uygur residents in Hetian, Xinjiang UygurAutonomous Region]. Zhonghua Yi Xue Za Zhi. 2015 Jan 6;95(1):69-72. Chinese.[↩][↩]
- Dogu O, Louis ED, Tamer L, Unal O, Yilmaz A, Kaleagasi H. Elevated blood lead concentrations in essential tremor: a case-control study in Mersin, Turkey. Environ Health Perspect. 2007 Nov;115(11):1564-8. doi: 10.1289/ehp.10352[↩][↩]
- Louis ED, Factor-Litvak P, Parides M, Andrews L, Santella RM, Wolff MS. Organochlorine pesticide exposure in essential tremor: a case-control study using biological and occupational exposure assessments. Neurotoxicology. 2006 Jul;27(4):579-86. doi: 10.1016/j.neuro.2006.03.005[↩][↩]
- Louis ED, Jurewicz EC, Applegate L, Factor-Litvak P, Parides M, Andrews L, Slavkovich V, Graziano JH, Carroll S, Todd A. Association between essential tremor and blood lead concentration. Environ Health Perspect. 2003 Nov;111(14):1707-11. doi: 10.1289/ehp.6404[↩]
- Louis ED, Applegate LM, Factor-Litvak P, Parides MK, Andrews L. Essential tremor: occupational exposures to manganese and organic solvents. Neurology. 2004 Dec 14;63(11):2162-4. doi: 10.1212/01.wnl.0000145600.91491.f2[↩]
- Gulcher JR, Jónsson P, Kong A, Kristjánsson K, Frigge ML, Kárason A, Einarsdóttir IE, Stefánsson H, Einarsdóttir AS, Sigurthoardóttir S, Baldursson S, Björnsdóttir S, Hrafnkelsdóttir SM, Jakobsson F, Benedickz J, Stefánsson K. Mapping of a familial essential tremor gene, FET1, to chromosome 3q13. Nat Genet. 1997 Sep;17(1):84-7. doi: 10.1038/ng0997-84[↩]
- Higgins JJ, Pho LT, Nee LE. A gene (ETM) for essential tremor maps to chromosome 2p22-p25. Mov Disord. 1997 Nov;12(6):859-64. doi: 10.1002/mds.870120605[↩]
- Shatunov A, Sambuughin N, Jankovic J, Elble R, Lee HS, Singleton AB, Dagvadorj A, Ji J, Zhang Y, Kimonis VE, Hardy J, Hallett M, Goldfarb LG. Genomewide scans in North American families reveal genetic linkage of essential tremor to a region on chromosome 6p23. Brain. 2006 Sep;129(Pt 9):2318-31. doi: 10.1093/brain/awl120[↩]
- Stefansson H, Steinberg S, Petursson H, et al. Variant in the sequence of the LINGO1 gene confers risk of essential tremor. Nat Genet. 2009 Mar;41(3):277-9. doi: 10.1038/ng.299. Erratum in: Nat Genet. 2009 Apr;41(4):504.[↩]
- Thier S, Lorenz D, Nothnagel M, et al. Polymorphisms in the glial glutamate transporter SLC1A2 are associated with essential tremor. Neurology. 2012 Jul 17;79(3):243-8. doi: 10.1212/WNL.0b013e31825fdeed[↩]
- Merner ND, Girard SL, Catoire H, et al. Exome sequencing identifies FUS mutations as a cause of essential tremor. Am J Hum Genet. 2012 Aug 10;91(2):313-9. doi: 10.1016/j.ajhg.2012.07.002[↩]
- Unal Gulsuner H, Gulsuner S, Mercan FN, Onat OE, Walsh T, Shahin H, Lee MK, Dogu O, Kansu T, Topaloglu H, Elibol B, Akbostanci C, King MC, Ozcelik T, Tekinay AB. Mitochondrial serine protease HTRA2 p.G399S in a kindred with essential tremor and Parkinson disease. Proc Natl Acad Sci U S A. 2014 Dec 23;111(51):18285-90. doi: 10.1073/pnas.1419581111[↩]
- Hor H, Francescatto L, Bartesaghi L, et al. Missense mutations in TENM4, a regulator of axon guidance and central myelination, cause essential tremor. Hum Mol Genet. 2015 Oct 15;24(20):5677-86. doi: 10.1093/hmg/ddv281[↩]
- Louis ED, Faust PL, Vonsattel JP. Purkinje cell loss is a characteristic of essential tremor. Parkinsonism Relat Disord. 2011 Jul;17(6):406-9. doi: 10.1016/j.parkreldis.2011.05.004[↩]
- Louis ED, Faust PL, Ma KJ, Yu M, Cortes E, Vonsattel JP. Torpedoes in the cerebellar vermis in essential tremor cases vs. controls. Cerebellum. 2011 Dec;10(4):812-9. doi: 10.1007/s12311-011-0291-0[↩]
- Louis ED. From neurons to neuron neighborhoods: the rewiring of the cerebellar cortex in essential tremor. Cerebellum. 2014 Aug;13(4):501-12. doi: 10.1007/s12311-013-0545-0[↩]
- Ghika A, Kyrozis A, Potagas C, Louis ED. Motor and Non-motor Features: Differences between Patients with Isolated Essential Tremor and Patients with Both Essential Tremor and Parkinson’s Disease. Tremor Other Hyperkinet Mov (N Y). 2015 Aug 14;5:335. doi: 10.7916/D83777WK[↩]
- Louis ED, Faust PL, Vonsattel JP, Honig LS, Rajput A, Robinson CA, Rajput A, Pahwa R, Lyons KE, Ross GW, Borden S, Moskowitz CB, Lawton A, Hernandez N. Neuropathological changes in essential tremor: 33 cases compared with 21 controls. Brain. 2007 Dec;130(Pt 12):3297-307. doi: 10.1093/brain/awm266[↩]
- Sharifi S, Nederveen AJ, Booij J, van Rootselaar AF. Neuroimaging essentials in essential tremor: a systematic review. Neuroimage Clin. 2014 May 9;5:217-31. doi: 10.1016/j.nicl.2014.05.003[↩]
- Tremor & Essential Tremor. https://www.movementdisorders.org/MDS/About/Movement-Disorder-Overviews/Tremor–Essential-Tremor.htm[↩]
- Rajalingam R, Breen DP, Lang AE, Fasano A. Essential tremor plus is more common than essential tremor: Insights from the reclassification of a cohort of patients with lower limb tremor. Parkinsonism Relat Disord. 2018 Nov;56:109-110. doi: 10.1016/j.parkreldis.2018.06.029[↩]
- Parkinson’s Disease. https://www.fusfoundation.org/diseases-and-conditions/parkinsons-disease[↩]
- Focused Ultrasound for Parkinson’s and Essential Tremor. https://www.barrowneuro.org/treatment/focused-ultrasound-thalamotomy[↩]
- Neudorfer C, Kultas-Ilinsky K, Ilinsky I, Paschen S, Helmers AK, Cosgrove GR, Richardson RM, Horn A, Deuschl G. The role of the motor thalamus in deep brain stimulation for essential tremor. Neurotherapeutics. 2024 Apr;21(3):e00313. doi: 10.1016/j.neurot.2023.e00313[↩]
- Pahwa R, Dhall R, Ostrem J, Gwinn R, Lyons K, Ro S, Dietiker C, Luthra N, Chidester P, Hamner S, Ross E, Delp S. An Acute Randomized Controlled Trial of Noninvasive Peripheral Nerve Stimulation in Essential Tremor. Neuromodulation. 2019 Jul;22(5):537-545. doi: 10.1111/ner.12930[↩]
- Prasad S, Bhalsing KS, Jhunjhunwala K, Lenka A, Binu VS, Pal PK. Phenotypic Variability of Essential Tremor Based on the Age at Onset. Can J Neurol Sci. 2019 Mar;46(2):192-198. doi: 10.1017/cjn.2018.384[↩]
- Brogley JE. DaTQUANT: The Future of Diagnosing Parkinson Disease. J Nucl Med Technol. 2019 Mar;47(1):21-26. doi: 10.2967/jnmt.118.222349[↩]
- Iacono MI, Atefi SR, Mainardi L, Walker HC, Angelone LM, Bonmassar G. A Study on the Feasibility of the Deep Brain Stimulation (DBS) Electrode Localization Based on Scalp Electric Potential Recordings. Front Physiol. 2019 Jan 4;9:1788. doi: 10.3389/fphys.2018.01788[↩]
- Putzke JD, Whaley NR, Baba Y, Wszolek ZK, Uitti RJ, Essential tremor: predictors of disease progression in a clinical cohort, J. Neurol. Neurosurg. Psychiatry 77 (2006) 1235–1237, 10.1136/jnnp.2006.086579[↩]





{kind=link}