
What is a heart murmur ?
A heart murmur is a sound made by turbulent blood flow within the heart 1. Murmurs sometimes sound like a whooshing or swishing noise — made by turbulent blood in or near your heart. These sounds can be heard with a stethoscope. A normal heartbeat makes two sounds like “lubb-dupp” (sometimes described as “lub-DUP”), which are the sounds of your heart valves closing 2. Your doctor hears this sound with a stethoscope. A murmur can occur in a normal heart. Or it may indicate some problem within the heart. Heart murmurs are almost always closely associated with a disease. However, benign (innocent) murmurs also called Still’s murmur, can be auscultated commonly in healthy children 3 to 7 years old, but it can be present at any age 3.
Heart murmurs are often described regarding the location on the thoracic cage in which it is auscultated, its pitch and volume, and in which phase of the cardiac cycle it was heard. Unique characteristics of the murmur should also be documented. For example, the murmur heard from aortic stenosis is usually described as a high pitched mid-systolic murmur that radiates to the carotid arteries. It is heard loudest at the right second intercostal space.
Heart murmurs can be divided into three categories based on where they occur in the cardiac cycle:
- Systolic murmur
- Diastolic murmur
- Continuous murmur (holosystolic)
Heart murmurs are graded on the Levine scale from 1 to 6 in intensity. They are dynamic findings that can be altered with specific maneuvers for a more accurate diagnosis. According to multiple major guidelines, further evaluation with an echocardiogram is indicated when any concerning murmur is auscultated 4.
Murmurs are classified (“graded”) depending on how loud the murmur sounds with a stethoscope. Systolic murmurs are graded on a six-point scale.
- Grade 1 just audible with a good stethoscope in a quiet room
- Grade 2 quiet but readily audible with a stethoscope
- Grade 3 easily heard with a stethoscope
- Grade 4 a loud, obvious murmur with a palpable thrill
- Grade 5 very loud, heard only over the pericardium but elsewhere in the body
- Grade 6 heard with stethoscope off chest
All murmurs louder than grade 3 are pathologic. An example of a murmur description is a “grade 2/6 murmur.” This means the murmur is grade 2 on a scale of 1 to 6.
Heart murmurs can be present at birth (congenital) or develop later in life 2. A heart murmur isn’t a disease — but murmurs may indicate an underlying heart problem.
Most often, the turbulence is normal. And the sound is called a benign flow or innocent murmur. Harmless murmurs may not cause symptoms and can happen when blood flows more rapidly than normal through the heart, for example in a person who is anxious, during exercise or has just finished exercising, pregnancy, has a high fever or rapid growth in children. About 10% of adults and 30% of children (most between the ages of 3 and 7) have a harmless murmur produced by a normal heart 5.
Abnormal murmurs may be a sign of a more serious heart condition, such as a congenital heart defect that is present since birth or heart valve disease.
Depending on the heart problem causing the abnormal murmurs, the murmurs may be associated with other symptoms such as shortness of breath, dizziness or fainting, bluish skin, or a chronic cough.
If a heart murmur is detected, your doctor will listen to the loudness, location and timing of your murmur to find out whether it is harmless or a sign of a more serious condition. If your doctor thinks you may have a more serious condition, your doctor may refer you to a cardiologist, or a doctor who specializes in the heart. The cardiologist may have you do other tests such as an electrocardiogram (EKG) or echocardiogram to look for heart rhythm or structural problems and see how well your heart is working.
A heart murmur itself does not require treatment. If it is caused by a more serious heart condition, your doctor may recommend treatment for that heart condition. Treatment may include medicines, cardiac catheterization, or surgery. The outlook and treatment for abnormal heart murmurs depend on the type and severity of the heart condition that is causing the murmur.
- Symptoms such as chest pain
- Family history of Marfan syndrome or sudden death in young family members
- Malformation syndrome (e.g., Down syndrome)
- Increased precordial activity
- Decreased femoral pulses
- Abnormal second heart sound
- Clicks
- Loud or harsh murmur
- Increased intensity of murmur when patient stands
A patient who has a pathologic cardiac examination or who has cardiac symptoms and questionable findings on the cardiac examination should be referred to a pediatric cardiologist. A child with a malformation syndrome associated with congenital heart disease should also be referred for additional evaluation. Conversely, an asymptomatic patient whose physical findings on a conscientiously performed cardiac examination indicate a low probability of cardiac pathology should be followed by the primary care physician. Referral is indicated if possibly pathologic findings emerge on serial examinations 6.
Heart murmur in babies and children
About 1 out of every 100 babies is born with a structural heart problem, or congenital heart defect 7. These babies may show signs of the defect as early as the first few days of life or not until later in childhood. Some kids won’t have any symptoms beyond a heart murmur, while others will such signs as:
- rapid breathing
- difficulty feeding
- blueness in the lips (called cyanosis)
- failure to thrive
An older child or teen might:
- be very tired
- have trouble exercising or doing physical activity
- have chest pain
See your doctor if your child has any of these symptoms.
What are heart valves?
Your heart is a strong muscle about the size of the palm of your hand. Your body depends on the heart’s pumping action to deliver oxygen- and nutrient-rich blood to the body’s cells. When the cells are nourished properly, the body can function normally. Just like an engine makes a car go, the heart keeps your body running. The heart has two pumps separated by an inner wall called the septum. The right side of the heart pumps blood to the lungs to pick up oxygen. The left side of the heart receives the oxygen-rich blood from the lungs and pumps it to the body.
The heart has four chambers 8, two on the right and two on the left:
- Two upper chambers are called atrium (two is called an atria). The atria collect blood as it flows into the heart.
- Two lower chambers are called ventricles. The ventricles pump blood out of the heart to the lungs or other parts of the body.
The heart also has four valves that open and close to let blood flow from the atria to the ventricles and from the ventricles into the two large arteries connected to the heart in only one direction when the heart contracts (beats). The four heart valves are:
- Tricuspid valve, located between the right atrium and right ventricle
- Pulmonary or pulmonic valve, between the right ventricle and the pulmonary artery. This artery carries blood from the heart to the lungs.
- Mitral valve, between the left atrium and left ventricle
- Aortic valve, between the left ventricle and the aorta. This aorta carries blood from the heart to the body.
Each valve has a set of flaps (also called leaflets or cusps). The mitral valve has two flaps; the others have three. Valves are like doors that open and close. They open to allow blood to flow through to the next chamber or to one of the arteries. Then they shut to keep blood from flowing backward. Blood flow occurs only when there’s a difference in pressure across the valves, which causes them to open. Under normal conditions, the valves permit blood to flow in only one direction.
The heart four chambers and four valves and is connected to various blood vessels. Veins are blood vessels that carry blood from the body to the heart. Arteries are blood vessels that carry blood away from the heart to the body.
The heart pumps blood to the lungs and to all the body’s tissues by a sequence of highly organized contractions of the four chambers. For the heart to function properly, the four chambers must beat in an organized way.
When the heart’s valves open and close, they make a “lub-DUB” sound that a doctor can hear using a stethoscope 9.
- The first sound (S1) —the “lub”—is made by the mitral and tricuspid valves closing at the beginning of systole. Systole is when the ventricles contract, or squeeze, and pump blood out of the heart.
- The second sound (S2)—the “DUB”—is made by the aortic and pulmonary valves closing at the beginning of diastole. Diastole is when the ventricles relax and fill with blood pumped into them by the atria.
Normal heart sounds [first sound (S1) and second sound (S2)]
Figure 1. The anatomy of the heart valves
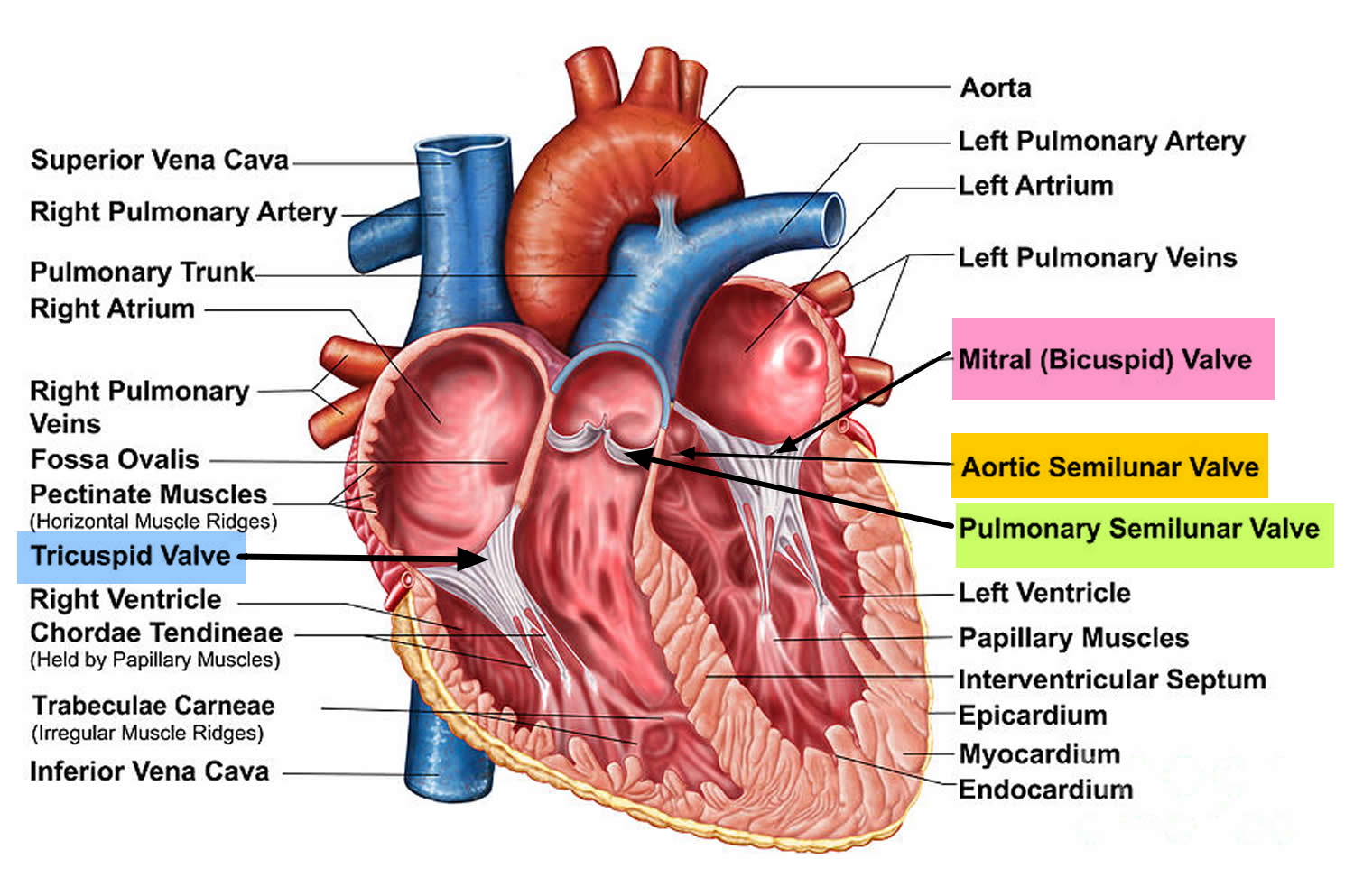
Figure 2. Top view of the 4 heart valves
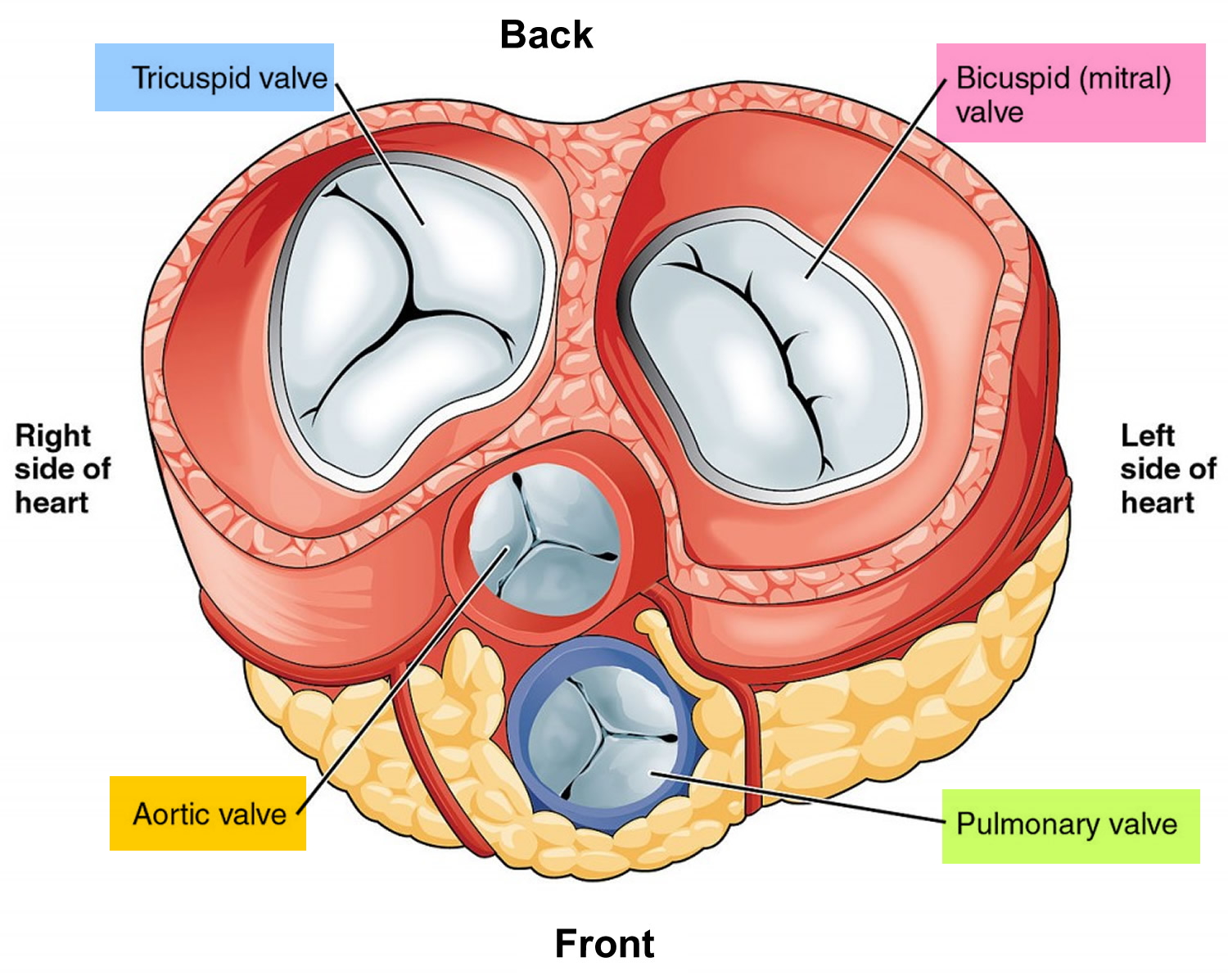
Figure 3. Normal heart blood flow

Figure 4. Heart valves function
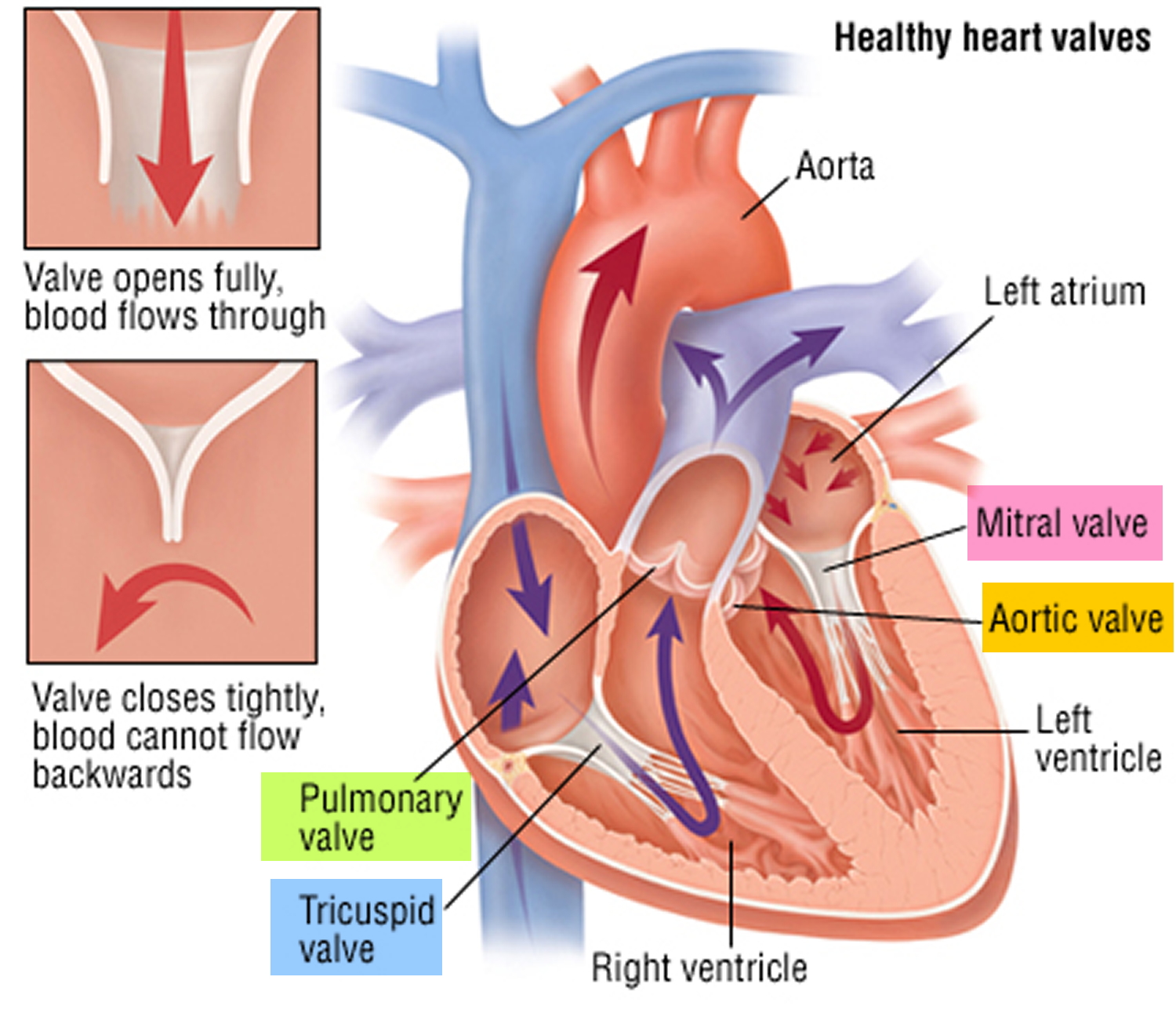
Heart valves function
Blood Flow
- The Right Side of Your Heart
In figure 3 above, the superior and inferior vena cavae are shown in blue to the left of the heart muscle as you look at the picture. These veins are the largest veins in your body.
After your body’s organs and tissues have used the oxygen in your blood, the vena cavae carry the oxygen-poor blood back to the right atrium of your heart.
The superior vena cava carries oxygen-poor blood from the upper parts of your body, including your head, chest, arms, and neck. The inferior vena cava carries oxygen-poor blood from the lower parts of your body.
The oxygen-poor blood from the vena cavae flows into your heart’s right atrium. From the right atrium, blood is pumped into the right ventricle. And then from the right ventricle, blood is pumped to your lungs through the pulmonary arteries (shown in blue in the center of figure 3).
Once in the lungs, the blood travels through many small, thin blood vessels called capillaries. There, the blood picks up more oxygen and transfers carbon dioxide to the lungs—a process called gas exchange.
The oxygen-rich blood passes from your lungs back to your heart through the pulmonary veins (shown in red to the left of the right atrium in figure 3).
- The Left Side of Your Heart
Oxygen-rich blood from your lungs passes through the pulmonary veins (shown in red to the right of the left atrium in figure 3 above). The blood enters the left atrium and is pumped into the left ventricle.
From the left ventricle, the oxygen-rich blood is pumped to the rest of your body through the aorta. The aorta is the main artery that carries oxygen-rich blood to your body.
Like all of your organs, your heart needs oxygen-rich blood. As blood is pumped out of your heart’s left ventricle, some of it flows into the coronary arteries (shown in red in figure 3).
Your coronary arteries are located on your heart’s surface at the beginning of the aorta. They carry oxygen-rich blood to all parts of your heart.
For the heart to work well, your blood must flow in only one direction. Your heart’s valves make this possible. Both of your heart’s ventricles have an “in” (inlet) valve from the atria and an “out” (outlet) valve leading to your arteries.
Healthy valves open and close in exact coordination with the pumping action of your heart’s atria and ventricles. Each valve has a set of flaps called leaflets or cusps that seal or open the valve. This allows blood to pass through the chambers and into your arteries without backing up or flowing backward.
Heart murmur symptoms
If you have a harmless heart murmur, more commonly known as an innocent heart murmur, you likely won’t have any other signs or symptoms.
An abnormal heart murmur may cause no obvious other signs or symptoms, aside from the unusual sound your doctor hears when listening to your heart with a stethoscope 2. But if you have these signs or symptoms 2, they may indicate a heart problem:
- Skin that appears blue, especially on your fingertips and lips (cyanosis)
- Swelling or sudden weight gain
- Shortness of breath
- Chronic cough
- Enlarged liver
- Enlarged neck veins
- Poor appetite and failure to grow normally (in infants)
- Heavy sweating with minimal or no exertion
- Chest pain
- Dizziness
- Fainting
Can you die from a heart murmur ?
Most heart murmurs aren’t serious, but if you think you or your child has a heart murmur, make an appointment to see your family doctor 2. Your doctor can tell you if your heart murmur is innocent and doesn’t require any further treatment or if an underlying heart problem needs to be further examined.
Diagnosis of Heart Murmurs
Heart murmurs are usually detected when your doctor listens to your heart using a stethoscope during a physical exam. If a heart murmur is detected, your doctor will listen to the loudness, location and timing of your murmur to find out whether it is harmless or a sign of a more serious condition.
Your doctor will also look for other signs and symptoms of heart problems and ask about your medical history and whether other family members have had heart murmurs or other heart conditions.
If your doctor thinks you may have a more serious condition, your doctor may refer you to a cardiologist, or a doctor who specializes in the heart.
The cardiologist may have you do other tests 10 such as:
- Chest X-ray. A chest X-ray shows an image of your heart, lungs and blood vessels. It can reveal if your heart is enlarged, which may mean an underlying condition is causing your heart murmur.
- Electrocardiogram (ECG). In this noninvasive test, a technician will place probes on your chest that record the electrical impulses that make your heart beat. An ECG records these electrical signals and can help your doctor look for heart rhythm and structure problems.
- Echocardiogram. This type of testing uses ultrasound waves to show detailed images of your heart’s structure and function. Echocardiography can help identify abnormal heart valves, such as those that are hardened (calcified) or leaking, and can also detect most heart defects.
- Cardiac catheterization. In this test, a catheter is inserted into a vein or artery in your leg or arm until it reaches your heart. The pressures in your heart chambers can be measured, and dye can be injected.The dye can be seen on an X-ray, which helps your doctor see the blood flow through your heart, blood vessels and valves to check for problems. This test is generally used when other tests have been inconclusive.
Causes of heart murmur
There are two types of heart murmurs 11:
- Innocent murmurs: a person with an innocent murmur has a normal heart. This type of heart murmur is common in newborns and children.
- Abnormal murmurs: an abnormal heart murmur is more serious. In children, abnormal murmurs are usually caused by congenital heart disease. In adults, abnormal murmurs are most often due to acquired heart valve problems.
Innocent heart murmurs
An innocent murmur can occur when blood flows more rapidly than normal through the heart. Conditions that may cause rapid blood flow through your heart, resulting in an innocent heart murmur, include:
- Physical activity or exercise
- Pregnancy
- Fever
- Not having enough healthy red blood cells to carry adequate oxygen to your body tissues (anemia)
- An excessive amount of thyroid hormone in your body (hyperthyroidism)
- Phases of rapid growth, such as adolescence
Innocent heart murmur is usually mid-systolic and arises from increased blood flow due to increased cardiac output. Innocent heart murmur occurs in children and patients with anemia or thyrotoxicosis. Innocent heart murmur is also present in up to 80% of pregnant women. A flow murmur may also be called a Still’s murmur. Both of these are benign and are also known as innocent murmurs. Crucially, a murmur is only genuinely innocent if it has no associated symptoms. Any murmur auscultated in diastole cannot be a benign murmur. Innocent or flow murmurs usually resolve during childhood. Any concern by medical professionals or the presence of any symptomology warrants further investigation of the murmur.
Innocent heart murmurs may disappear over time, or they may last your entire life without ever causing further health problems.
Abnormal heart murmurs
The most common cause of abnormal murmurs in children is when babies are born with structural problems of the heart (congenital heart defects).
Common congenital heart defects that cause heart murmurs include:
- Holes in the heart or cardiac shunts. Known as septal defects, holes in the heart may or may not be serious, depending on the size of the hole and its location.
Atrial septal defect murmur
An atrial septal defect is congenital. It is located between the left and right atria that allows blood to flow freely between them. It will present as a loud S1 and a wide, fixed split S2 heart sound, and will be loudest at the upper left sternal border. Large atrial septal defects are quieter, while small ones are louder and have a harsh quality. The sound is different because blood will flow with much less turbulence through a larger, unrestrictive space. Atrial septal defects are usually detected in utero or early in childhood through either ultrasound or physical examination.
Ventricular septal defect murmur
Ventricular septal defect is holosystolic. Similarly to atrial septal defects, smaller ventricular septal defects are louder and have a harsher quality, while large ones are quieter but more symptomatic. In a child, a closing atrial or ventricular septal defect will get progressively louder until it closes. A distinguishing trait of ventricular septal defects is the location of the murmur. This type of murmur is loudest at the apex, while an atrial septal defect is loudest at the upper left sternal border.
Patent ductus arteriosus
Patent ductus arteriosus will present with a continuous machine-like murmur in a newborn that is loudest at the upper left sternal border. If the newborn has no other comorbidities, it may be closed with NSAIDs such as indomethacin. However, if the patient has other cardiac abnormalities, the patent ductus arteriosus may be critical to the patient’s survival and should not be closed.
Cardiac shunts occur when there’s an abnormal blood flow between the heart chambers or blood vessels, which may lead to a heart murmur.
- Heart valve abnormalities. Congenital heart valve abnormalities are present at birth, but sometimes aren’t discovered until much later in life. Examples include valves that don’t allow enough blood through them (stenosis) or those that don’t close properly and leak (regurgitation), such as mitral valve prolapse.
Other causes of abnormal heart murmurs include infections and conditions that damage the structures of the heart and are more common in older children or adults. For example:
- Valve calcification. This hardening or thickening of valves, as in mitral stenosis or aortic valve stenosis, can occur as you age. Valves may become narrowed (stenotic), making it harder for blood to flow through your heart, resulting in murmurs.
- Endocarditis. This infection of the inner lining of your heart and valves typically occurs when bacteria or other germs from another part of your body, such as your mouth, spread through your bloodstream and lodge in your heart. The murmur from infective endocarditis is due to the growth of bacterial vegetations on the heart valves, most commonly the tricuspid valve. Tricuspid valve vegetations usually occur in intravenous drug users with infective endocarditis, leading to the development of tricuspid stenosis and tricuspid regurgitation.
Left untreated, endocarditis can damage or destroy your heart valves. This condition usually occurs in people who already have heart valve abnormalities.
- Rheumatic fever. Although now rare in the United States, rheumatic fever is a serious condition that can occur when you don’t receive prompt or complete treatment for a strep throat infection. It can permanently affect the heart valves and interfere with normal blood flow through your heart. Chronic rheumatic heart disease is a complication of untreated streptococcal pharyngitis and acute rheumatic fever. Chronic auto-immune attack of cardiac tissue causes it due to the molecular similarity between the tissue and streptococcal M protein. Mitral stenosis, mitral regurgitation, aortic stenosis, and aortic regurgitation can develop because of this chronic valve inflammation.
Murmurs may indicate valve problems including:
- Stenosis: a narrowing or stiffening of the valve that prevents adequate blood supply from flowing through.
Aortic stenosis
Aortic stenosis is the narrowing of the aortic valve. It is the most common valvular heart disease in the developed world. The condition is described as a harsh crescendo-decrescendo systolic murmur heard best at the right upper sternal border, with radiation of the murmur to the carotid arteries. It may arise from valve calcification over time due to aging or to having a congenital bicuspid aortic valve. Chronic rheumatic heart disease is also a cause of aortic stenosis.
Aortic stenosis (early)
Aortic stenosis (late)
Mitral stenosis
Mitral stenosis is a diastolic murmur best heard at the apex. Worldwide, mitral stenosis is most commonly caused by chronic rheumatic heart disease. It is also observed in cases of infective endocarditis and chronic rheumatic heart disease.
Pulmonary stenosis
Pulmonic stenosis murmur is described as a crescendo-decrescendo systolic ejection murmur heard loudest at the upper left sternal border. Its causes include Tetralogy of Fallot, where a congenitally stenotic pulmonary valve is present; carcinoid syndrome, where a carcinoid tumor secretes serotonin and causes vegetation growth on the pulmonary valves; congenital rubella syndrome, a multi-organ congenital syndrome; and Noonan syndrome, an inherited genetic disease. Pulmonic stenosis is most commonly a congenital finding. However, it may also arise in a patient with a chronic rheumatic disease.
Tricuspid stenosis
Tricuspid stenosis is a diastolic murmur best heard at the lower left sternal border. It is often associated with intravenous drug abusers that present with symptoms of infective endocarditis and in carcinoid syndrome patients. Prolonged tricuspid stenosis will lead to right atrial enlargement and possibly arrhythmias.
- Regurgitation: when valves allow blood to flow backward into the chamber.
Mitral regurgitation
This type of murmur is systolic and is best heard at the apex with radiation to the left axilla. Mitral regurgitation is observed in patients with infective endocarditis, chronic rheumatic heart disease, degenerative valve disease, Ehlers-Danlos syndrome, Marfan syndrome, and systemic lupus erythematosus. The sudden onset of acute, severe mitral regurgitation occurs in some patients that have suffered an inferior wall myocardial infarct. This effect is due to the rupture of the chordae tendineae after the myocardial infarct has weakened the tissue structure.
Aortic regurgitation
Also known as aortic insufficiency, aortic regurgitation is a diastolic murmur. It develops due to aortic valve failure during diastole, causing blood to leak back into the ventricles from the aorta in a turbulent manner. The most common causes of aortic regurgitation in the developed world are aortic root dilation, bicuspid aortic valve, and calcific valve disease. Aortic regurgitation is described as a decrescendo blowing diastolic murmur heard best at the left lower sternal border.
Tricuspid regurgitation
This type of murmur is systolic. It is best appreciated at the lower left sternal border. Tricuspid regurgitation may be auscultated due to vegetative growth both in intravenous drug abusers that present with infective endocarditis and in patients with carcinoid syndrome.
- Prolapse: a valve that has improperly closing leaflets.
Mitral valve prolapse
This valvular disease occurs most commonly due to idiopathic myxomatous valve degeneration. Mitral valve prolapse can also be caused by acute rheumatic fever, chronic rheumatic disease, endocarditis, and Ebstein’s anomaly. It presents as an early systolic click heard best at the apex. It often is accompanied by a late systolic murmur indicative of mitral regurgitation occurring after mitral valve prolapse. As with other valvular diseases, mitral valve prolapse is only definitively diagnosed with imaging.
- Atresia: a valve that is improperly formed or missing.
Causes of Heart Valve Problems 12
The causes of valve problems can often be linked to birth abnormalities, related to age, or brought on by another condition.
Congenital heart defects (abnormalities present at birth):
- Aortic valve stenosis
- Ebstein’s anomaly
- Pulmonary valve stenosis
Aging and age-related valve disease, such as:
- Degenerative valve disease — Most commonly affecting the mitral valve, over time valves can slowly degenerate. For example, mitral valve prolapse, a condition that affects nearly 2 percent of the general population, may eventually turn into mitral valve regurgitation requiring treatment.
- Calcification due to aging — Sometimes calcium can accumulate on the heart’s valves, most commonly affecting the aortic valve, and can lead to aortic stenosis.
- Mediastinal radiation therapy (radiation to the chest) – Studies have shown that survivors of childhood cancer who had radiation therapy for their cancer have an increased prevalence of valve disease later in life.
Related illnesses and conditions that can cause valve problems:
- Infective endocarditis
- Injury
- Rheumatic fever
These conditions can cause one or more of the heart valves to leak blood back into the heart chambers or fail to open fully, making your heart work harder and lessening its ability to pump blood. Although valve problems can potentially be severe and life-threatening, most valve conditions are also highly treatable.
Risk factors for developing a heart murmur 13
There are risk factors that increase your chances of developing a heart murmur, including:
- Family history of a heart defect. If blood relatives have had a heart defect, that increases the likelihood you or your child may also have a heart defect and heart murmur.
- Certain medical conditions, including uncontrolled high blood pressure (hypertension), hyperthyroidism, an infection of the lining of the heart (endocarditis), high blood pressure in the lungs (pulmonary hypertension), carcinoid syndrome, hypereosinophilic syndrome, systemic lupus erythematosus, rheumatoid arthritis, a weakened heart muscle or a history of rheumatic fever, can increase your risk of a heart murmur later in life.
Factors that increase your baby’s risk of developing a heart murmur include:
- Illnesses during pregnancy. Having some conditions during pregnancy, such as uncontrolled diabetes or a rubella infection, increases your baby’s risk of developing heart defects and a heart murmur.
- Taking certain medications or illegal drugs during pregnancy. Use of certain medications, alcohol or drugs can harm a developing baby, leading to heart defects.
Heart murmur treatment
An innocent heart murmur generally doesn’t require treatment because the heart is normal. If innocent murmurs are the result of an illness, such as fever or hyperthyroidism, the murmurs will go away once that condition is treated 14.
If you or your child has an abnormal heart murmur, treatment may not be necessary. Your doctor may want to monitor the condition over time. If treatment is necessary, it depends on what heart problem is causing the murmur and may include medications or surgery.
The outlook and treatment for abnormal heart murmurs depend on the type and severity of the heart condition that is causing the murmur.
Medications
The medication your doctor prescribes depends on the specific heart problem you have. Some medications your doctor might give you include:
- Medications that prevent blood clots (anticoagulants). Your doctor may prescribe anticoagulants, such as aspirin, warfarin (Coumadin, Jantoven) or clopidogrel (Plavix). An anticoagulant prevents blood clots from forming in your heart and causing a heart attack or stroke.
- Water pills (diuretics). Diuretics remove excess fluid from your body, which can help treat other conditions that might worsen a heart murmur, such as high blood pressure.
- Angiotensin-converting enzyme (ACE) inhibitors. ACE inhibitors lower your blood pressure. High blood pressure can worsen underlying conditions that cause heart murmurs.
- Statins. Statins help lower your cholesterol. Having high cholesterol seems to worsen some heart valve problems, including some heart murmurs.
Beta blockers. These drugs lower your heart rate and blood pressure. They’re used for some types of heart valve problems.
Surgery
Many valve conditions can’t be treated with medications alone. Depending on your heart condition, your doctor may recommend one of these options to treat a damaged or leaky valve:
Valve repair
To repair a valve, your doctor may recommend one of the following procedures:
- Balloon valvuloplasty. This procedure is performed to relieve a narrowed valve. During a balloon valvuloplasty, a small catheter containing an expandable balloon is threaded into your heart, placed into the valve and then expanded to help widen the narrowed valve.
- Annuloplasty. In this procedure, your surgeon tightens the tissue around the valve by implanting an artificial ring. This allows the leaflets to come together and close the abnormal opening through the valve.
- Repair of structural support. In this procedure, your surgeon replaces or shortens the cords that support the valves (chordae tendineae and papillary muscles) to repair the structural support. When the cords and muscles are the right length, the valve leaflet edges meet and eliminate the leak.
- Valve leaflet repair. In valve leaflet repair, your surgeon surgically separates, cuts or pleats a valve flap (leaflet).
Valve replacement
In many cases, the valve has to be replaced. Options include:
- Open-heart surgery. This is the primary surgical treatment for severe valve stenosis. Your surgeon removes the narrowed valve and replaces it with a mechanical valve or a tissue valve.
Mechanical valves, made from metal, are durable, but carry the risk of blood clots forming. If you receive a mechanical valve, you’ll need to take an anticoagulant medication, such as warfarin (Coumadin, Jantoven), for life to prevent blood clots.
Tissue valves — which may come from a pig, cow or human deceased donor — often eventually need replacement. Another type of tissue valve replacement that uses your own pulmonary valve (autograft) is sometimes possible.
- Transcatheter aortic valve replacement (TAVR). A less invasive approach, transcatheter aortic valve replacement involves replacing the aortic valve with a prosthetic valve via an artery in your leg or in a small incision in your chest.
In some cases, a valve can be inserted via a catheter into a tissue replacement valve that needs to be replaced (valve-in-valve procedure).
Transcatheter aortic valve replacement is usually reserved for individuals with severe aortic valve stenosis who are at increased risk of complications from aortic valve surgery.
Doctors used to recommend that most people with abnormal heart murmurs take antibiotics before visiting the dentist or having surgery due to possible complications from a bacterial infection that affects the lining of your heart (infective endocarditis).
Doctors no longer recommend antibiotics before procedures, except for people at highest risk of complications of infective endocarditis, such as those who have an artificial heart valve or people with certain congenital heart defects 15.
Prevention
While there’s not much you can do to prevent a heart murmur, it is reassuring to know that heart murmurs are not a disease and are often harmless. For children, many murmurs go away on their own as children grow 16. For adults, murmurs may disappear as the underlying condition causing them improves.
- National Institutes of Health. Heart Murmur. https://www.nhlbi.nih.gov/health/health-topics/topics/heartmurmur[↩]
- Mayo Foundation for Medical Education and Research. Heart murmurs. http://www.mayoclinic.org/diseases-conditions/heart-murmurs/basics/definition/con-20028706[↩][↩][↩][↩][↩]
- Innocent murmurs: a suspect diagnosis in non-pregnant adults. Am J Cardiol. 2009 Sep 1;104(5):735-7. doi: 10.1016/j.amjcard.2009.04.031. Epub 2009 Jun 24. https://www.ajconline.org/article/S0002-9149(09)00999-0/fulltext[↩]
- Liu Q, Wu X, Ma X. An automatic segmentation method for heart sounds. Biomed Eng Online. 2018 Aug 06;17(1):106.[↩]
- Harvard University. Harvard Health Publications. Heart Murmur. https://www.health.harvard.edu/heart-health/heart-murmur[↩]
- Rosenthal A. How to distinguish between innocent and pathologic murmurs in childhood. Pediatr Clin North Am. 1984;31:1229–40.[↩]
- The Nemours Foundation. Kids Health. Heart Murmurs. https://kidshealth.org/en/parents/murmurs.html[↩]
- American Heart Association. About Arrhythmia. http://www.heart.org/HEARTORG/Conditions/Arrhythmia/AboutArrhythmia/About-Arrhythmia_UCM_002010_Article.jsp[↩]
- Centers for Disease Control and Prevention. Division of Birth Defects and Developmental Disabilities. Congenital Heart Defects (CHDs). https://www.cdc.gov/ncbddd/heartdefects/index.html[↩]
- Mayo Foundation for Medical Education and Research. Tests and diagnosis for heart murmurs. http://www.mayoclinic.org/diseases-conditions/heart-murmurs/basics/tests-diagnosis/con-20028706[↩]
- Mayo Foundation for Medical Education and Research. Causes of heart murmurs. http://www.mayoclinic.org/diseases-conditions/heart-murmurs/basics/causes/con-20028706[↩]
- American Heart Association. Understanding Heart Valve Problems and Causes. http://www.heart.org/HEARTORG/Conditions/More/HeartValveProblemsandDisease/Understanding-Heart-Valve-Problems-and-Causes_UCM_450360_Article.jsp[↩]
- Mayo Foundation for Medical Education and Research. Risk factors for developing a heart murmur. http://www.mayoclinic.org/diseases-conditions/heart-murmurs/basics/risk-factors/con-20028706[↩]
- Mayo Foundation for Medical Education and Research. Treatments and drugs for heart murmurs. http://www.mayoclinic.org/diseases-conditions/heart-murmurs/basics/treatment/con-20028706[↩]
- National Institute for Health and Clinical Excellence. Prophylaxis Against Infective Endocarditis. https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0009942/[↩]
- Mayo Foundation for Medical Education and Research. Prevention of heart murmur. http://www.mayoclinic.org/diseases-conditions/heart-murmurs/basics/prevention/con-20028706[↩]





{kind=link}