
What is albumin
Albumin is a protein made by the liver. Albumin makes up 40 to 60% of the total proteins in the blood and plays many roles. Albumin keeps fluid from leaking out of blood vessels; nourishes tissues; and transports hormones, vitamins, drugs, and substances like calcium throughout the body. Albumin binds and solubilizes various compounds, including bilirubin, calcium, long-chain fatty acids, toxic heavy metal ions, and numerous pharmaceuticals.
Levels of albumin may decrease, to a greater or lesser degree, when conditions interfere with its production by the liver, increase protein breakdown, increase protein loss via the kidneys, and/or expand plasma volume (diluting the blood).
- Because of albumin high concentration in the plasma and small molecular size, it is found in the most of the extravascular fluids, cerebrospinal fluid (CSF), amniotic fluid, urine and interstitial fluid.
- Albumin is highly water soluble due to its negative charge at normal pH.
- Albumin half-life is 15 to 19 days.
Normal albumin levels:
- Normal serum albumin range = 3.4 to 5.5 g/dl (35 to 55 g/L).
- Male = 4.2 to 5.5 g /dl
- Female = 3.7 to 5.3 g/dl
- Newborn = 2.8 to 4.8 g/dl
When plasma or serum albumin values fall below 2.0 g/dL, edema is usually present.
Cerebrospinal fluids (CSF) = 15 to 45 mg/dl
Urine albumin levels
- 1 to 14 mg/mL
- 15 to 45 mg /24 hours
- Males: <17 mg/g creatinine
- Females: <25 mg/g creatinine
If your albumin levels are lower than normal, it may indicate one of the following conditions:
- Liver disease, including cirrhosis
- Kidney disease
- Malnutrition
- Infection
- Inflammatory bowel disease
- Thyroid disease
Higher than normal levels of albumin may indicate dehydration or severe diarrhea.
If your albumin levels are not in the normal range, it doesn’t necessarily mean you have a medical condition needing treatment. Certain drugs, including steroids, insulin, and hormones, can raise albumin levels. Other drugs, including birth control pills, can lower your albumin levels.
Hypoalbuminemia (low albumin level) is caused by several factors: impaired synthesis due either to liver disease (primary) or due to diminished protein intake (secondary), increased catabolism as a result of tissue damage and inflammation, malabsorption of amino acids, and increased renal excretion (e.g, nephrotic syndrome).
Two important causes of low blood albumin include:
- Severe liver disease—since albumin is produced by the liver, its level can decrease with loss of liver function; however, this typically occurs only when the liver has been severely affected.
- Kidney disease—one of the many functions of the kidneys is to conserve plasma proteins such as albumin so that they are not released along with waste products when urine is produced. Albumin is present in high concentrations in the blood, and when the kidneys are functioning properly, virtually no albumin is lost in the urine. However, if a person’s kidneys become damaged or diseased, they begin to lose their ability to conserve albumin and other proteins. This is frequently seen in chronic diseases, such as diabetes and hypertension. In nephrotic syndrome, very high amounts of albumin are lost through the kidneys.
People who have chronic liver disease and kidney disorders are at highest risk for developing abnormal albumin levels. In addition, individuals whose gastrointestinal tract (GIT) doesn’t absorb nutrients properly and individuals who have prolonged diarrhea can develop abnormal albumin levels.
Is there a home test for albumin levels?
Not for blood albumin; you can test for high albumin levels in urine with a dipstick purchased in a drug store.
What does albumin do?
Albumin makes 40 to 60% of the total proteins in the blood and plays many roles.
Serum albumin is the main protein of human blood plasma. Albumin binds water, cations (such as Ca2+, Na+ and K+), fatty acids, hormones, bilirubin, thyroxine (T4) and pharmaceuticals (including barbiturates): its main function is to regulate the oncotic pressure of blood. Alpha-fetoprotein (alpha-fetoglobulin) is a fetal plasma protein that binds various cations, fatty acids and bilirubin. Vitamin D-binding protein binds to vitamin D and its metabolites, as well as to fatty acids.
- Albumin is needed to maintain the osmotic pressure in the blood vessels without which fluids will leak out.
- Albumin is extremely sensitive to liver damage.
- Albumin protein is synthesized in the liver and reflects the function of the liver, kidney, or malnutrition.
- Albumin binds bilirubin, free fatty acids, calcium, and a number of drugs.
- Low albumin results in edema.
- Decreased synthesis in the liver is seen in acute or chronic liver diseases, amyloidosis, malnutrition, and malignancy.
- Albumin’s role in transporting bilirubin, bile acids, metal ions, and drugs will be markedly affected by variation in its concentration.
- Albumin provides nutrition to the tissues and binds various molecules like hormones, vitamin, and drugs.
- Albumin acts as a carrier protein for bilirubin, calcium, progesterone, and drugs.
Figure 1. Albumin function
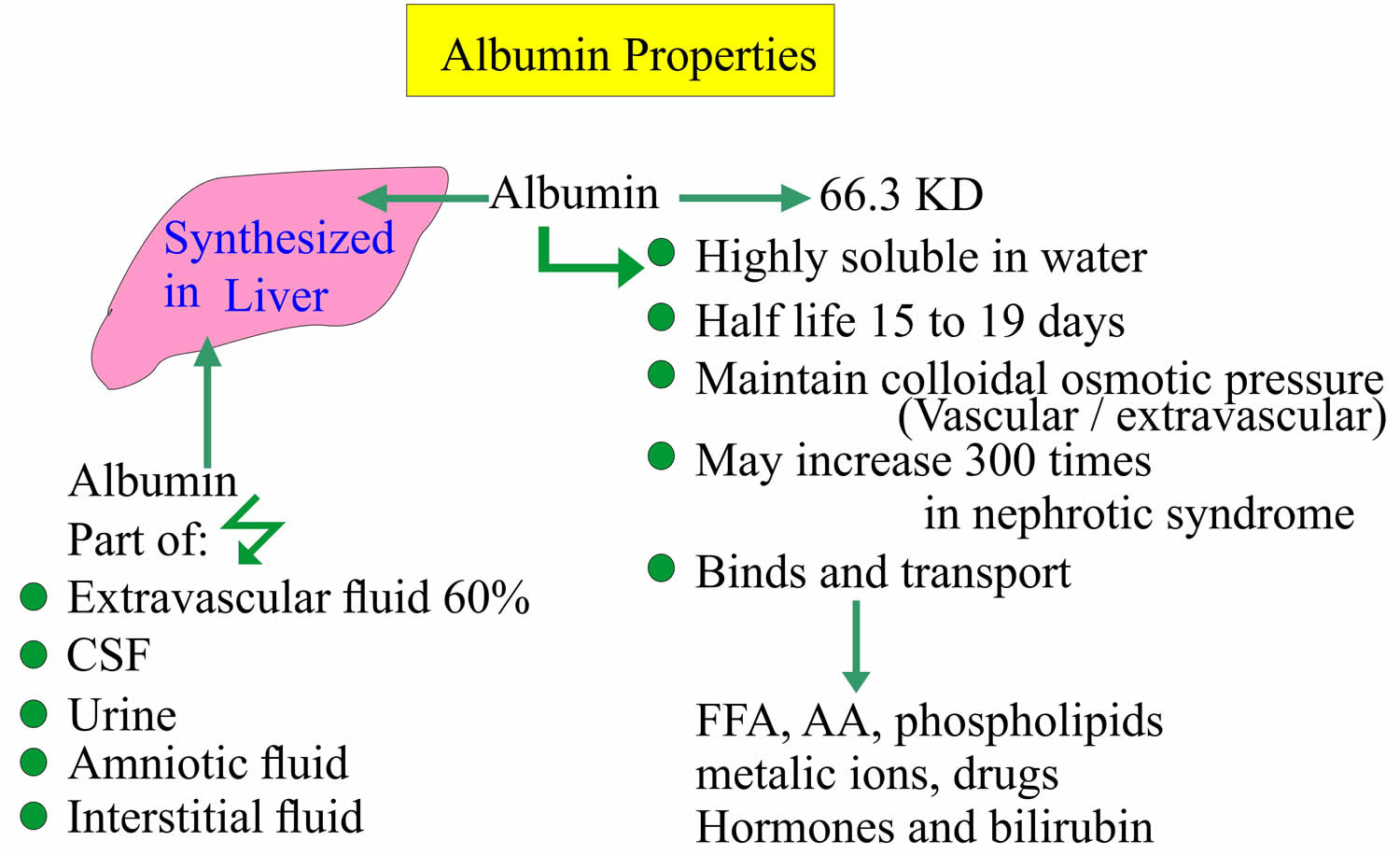
Abbreviations: CSF = cerebrospinal fluid; FFA = free fatty acid; AA = amino acids
Albumin blood test
Albumin blood test measures the level of albumin in the blood. An albumin test is routinely included in the panels of tests performed as part of a health examination, such as a comprehensive metabolic panel (CMP), so it is frequently used to help evaluate a person’s overall health status.
Additionally, since albumin can be low in many different diseases and disorders, it may be used in a variety of settings to help diagnose disease, to monitor changes in health status with treatment or with disease progression, and as a screen that may indicate the need for other kinds of testing.
Albumin is a protein made by the liver that keeps fluid from leaking out of blood vessels, nourishes tissues, and transports hormones, vitamins, drugs, and substances like calcium throughout the body.
An albumin test may be ordered as part of a liver panel to evaluate liver function or with a creatinine, blood urea nitrogen (BUN), or renal panel to evaluate kidney function. Albumin may also be ordered to evaluate a person’s nutritional status.
When is albumin test ordered?
An albumin test is frequently ordered as part of a panel of tests performed for a health screening.
Albumin may be ordered, along with other tests, when a person has symptoms of a liver disorder, such as:
- Yellowing of eyes or skin (jaundice)
- Weakness, fatigue
- Unexplained weight loss
- Loss of appetite
- Abdominal swelling and/or pain
- Dark urine and light-colored stool
- Itching (pruritus)
Albumin test may be ordered when a person has symptoms of nephrotic syndrome, such as:
- Swelling or puffiness, particularly around the eyes or in the face, wrists, abdomen, thighs or ankles
- Urine that is foamy, bloody, or coffee-colored
- A decrease in the amount of urine
- Problems urinating, such as a burning feeling or abnormal discharge during urination, or a change in the frequency of urination, especially at night
- Mid-back pain (flank), below the ribs, near where the kidneys are located
- High blood pressure (hypertension)
- Swelling around the abdomen, thighs, or face
- More frequent urination, especially at night
- Nausea
- Itchy skin
A healthcare practitioner may also order an albumin test to check or monitor a person’s nutritional status. However, since albumin concentrations respond to a variety of conditions in addition to malnutrition, a decrease in albumin needs to be evaluated carefully.
What is the difference between serum/plasma albumin, prealbumin, and urine albumin tests?
Although the names are similar, albumin and prealbumin are completely different molecules. They are both proteins made by the liver, however, and both have been used historically to evaluate nutritional status. Serum/plasma (or blood) albumin is now more often used to screen for and help diagnose liver or kidney disease and is tested on a blood sample. The urine albumin test (in the past, called a microalbumin test) detects and measures albumin in the urine as an early indicator of kidney damage.
High albumin levels
High albumin levels (hyperalbuminemia) can be seen with dehydration or any other cause leading to decrease in the plasma volume, although the albumin test is not typically used to monitor or detect this condition.
Certain drugs increase albumin in the blood, including anabolic steroids, androgens, growth hormones, and insulin.
Other cause of high albumin levels can be due to high protein diet. High albumin levels can even occur when the tourniquet is applied for a long time during a blood specimen collection.
Albumin levels may be up to 15% higher if the specimen is collected with the patient erect rather than supine.
If someone is receiving large amounts of intravenous fluids, the results of this test may be inaccurate.
Low albumin levels
A low albumin level (hypoalbuminemia) may be a warning and an indication that further investigation may be warranted. A low albumin may reflect a temporary condition that will resolve itself or may suggest an acute or chronic condition that requires medical intervention.
Levels of albumin may decrease, to a greater or lesser degree, when conditions interfere with its production, increase protein breakdown, increase protein loss, and/or expand plasma volume (diluting the blood). Depending on the person’s medical history, signs and symptoms, and physical exam, additional testing may be done to investigate a low result.
A low albumin can suggest liver disease. Liver enzyme tests or a liver panel may be ordered to determine exactly which type of liver disease may be present. A person may, however, have normal or near normal albumin levels with liver disease until the condition has reached an advanced stage. For example, in people with cirrhosis, albumin is typically (but not always) low whereas in most chronic liver diseases that have not progressed to cirrhosis, albumin is usually normal.
Low albumin levels can reflect diseases in which the kidneys cannot prevent albumin from leaking from the blood into the urine and being lost. In this case, the amount of albumin or protein in the urine also may be measured (see Urine Albumin) or tests for creatinine and BUN or a renal panel may be ordered.
Low albumin levels can also be seen in inflammation, shock, and malnutrition. They may be seen with conditions in which the body does not properly absorb and digest protein, such as Crohns disease or celiac disease, or in which large volumes of protein are lost from the intestines.
A low albumin may also be seen in several other conditions, such as:
- Infection
- Burns
- Surgery
- Chronic illness
- Cancer
- Diabetes
- Hypothyroidism
- Carcinoid syndrome
- Plasma volume expansion due to congestive heart failure, sometimes pregnancy
Low albumin causes
- Acute and chronic inflammations:
- Acute phase response
- The cause is hemodilution, loss into extravascular space, increased consumption by the cells and decreased synthesis.
- Rheumatoid arthritis, granulomatous process, most bacterial infections, vasculitis, ulcerative bowel disease, and certain parasitic infestation.
- Due to decreased synthesis by the liver:
- This may be due to the increased amount of immunoglobulins, loss of albumin into the extravascular space.
- This may be also due to the decreased synthesis because of toxins or alcohol.
- The liver can compensate the synthesis of albumin approximately up to 95% of the loss of liver function.
- In acute and chronic liver diseases, Amyloidosis, Malignancies, Congestive heart disease, and constrictive pericarditis.
- Chronic liver disease (e.g., cirrhosis and autoimmune hepatitis)
- Increased albumin loss via body fluids:
- In Nephrotic syndrome, thermal burns, trauma and crush injuries, and transudation and exudation from any hollow organs.
- Increased catabolism: leads to decrease albumins like fever, antimetabolites, thyrotoxicosis, and certain malignancies.
- A gastrointestinal loss:
- With the inflammatory disease of gastrointestinal tract (GIT).
- Chronic protein-losing enteropathy.
- Increased blood volume (hypervolemia): leads to decrease albumin-like pregnancy, exogenous estrogen therapy, Myeloma and congestive heart failure.
- Serum level decreases in pregnant ladies.
- The person on a low protein diet.
- Severe Malnutrition
- Severe/chronic illness
- Albumin decreases:
- After weight loss surgery.
- Whipple disease.
- Sprue.
- Crohn’s disease.
Albumin in urine
The urine albumin test detects and measures the amount of albumin in the urine. The presence of a small amount of albumin in the urine may be an early indicator of kidney disease. A small amount of albumin in the urine is sometimes referred to as urine microalbumin or microalbuminuria. “Microalbuminuria” is slowly being replaced with the term “albuminuria,” which refers to any elevation of albumin in the urine.
The preferred urine specimen is a 24-hour collection, but a random urine collection is acceptable. Studies have shown that correcting albumin for creatinine excretion rates has similar discriminatory value with respect to diabetic renal involvement. The albumin:creatinine ratio (ACR) from a random urine specimen is also considered a valid screening tool 1. Several studies have addressed whether the specimen needs to be a fasting urine, an exercised urine, or an overnight urine specimen. These studies have shown that the first-morning urine specimen is less sensitive, but more specific.
Plasma, the liquid portion of blood, contains many different proteins, including albumin. One of the many functions of the kidneys is to conserve plasma proteins so that they are not released along with waste products when urine is produced. There are two mechanisms that normally prevent protein from passing into urine:
- The glomeruli provide a barrier that keeps most large plasma proteins inside the blood vessels and
- The smaller proteins that do get through are almost entirely reabsorbed by the tubules.
Protein in the urine (proteinuria) most often occurs when either the glomeruli or tubules in the kidney are damaged. Inflammation and/or scarring of the glomeruli can allow increasing amounts of protein to leak into the urine. Damage to the tubules can prevent protein from being reabsorbed.
Albumin is a plasma protein that is present in high concentrations in the blood, and when the kidneys are functioning properly, virtually no albumin is present in the urine. If a person’s kidneys become damaged or diseased, however, they begin to lose their ability to conserve albumin and other proteins. This is frequently seen in chronic diseases, such as diabetes and hypertension, with increasing amounts of protein in the urine reflecting increasing kidney dysfunction.
Albumin is one of the first proteins to be detected in the urine with kidney damage. People who have consistently detectable small amounts of albumin in their urine (albuminuria) have an increased risk of developing progressive kidney failure and cardiovascular disease in the future.
A urine albumin test is used to screen for kidney disease in people with chronic conditions such as diabetes and high blood pressure. It can detect small amounts of albumin that escape from the blood through the kidneys into the urine several years before significant kidney damage becomes apparent. Most of the time, tests for albumin and creatinine are done on a urine sample collected randomly (not timed) and an albumin-to-creatinine ratio (ACR) is calculated. This is done to provide a more accurate indication of the how much albumin is being released into the urine.
Diabetic nephropathy is a complication of diabetes and is characterized by proteinuria (normal urinary albumin excretion is <30 mg/day; overt proteinuria is >300 mg/day). Before overt proteinuria develops, albumin excretion increases in those diabetic patients who are destined to develop diabetic nephropathy. Therapeutic maneuvers (e.g, aggressive blood pressure maintenance, particularly with angiotensin-converting enzyme inhibitors; aggressive blood sugar control; and possibly decreased protein intake) can significantly delay, or possibly prevent, development of nephropathy. Thus, there is a need to identify small, but abnormal, increases in the excretion of urinary albumin (in the range of 30-300 mg/day, i.e, microalbuminuria).
The National Kidney Foundation guidelines for the management of patients with diabetes and microalbuminuria recommend that all type 1 diabetic patients older than 12 years and all type 2 diabetic patients younger than 70 years have their urine tested for microalbuminuria yearly when they are under stable glucose control 2.
Studies also have shown that microalbuminuria is a marker of generalized vascular disease and is associated with stroke and heart disease.
When is urine albumin test ordered?
According to the American Diabetes Association and National Kidney Foundation, everyone with type 1 diabetes should get tested annually, starting 5 years after onset of the disease, and all those with type 2 diabetes should get tested annually, starting at the time of diagnosis. If albumin in the urine (albuminuria) is detected, it should be confirmed by retesting twice within a 3-6 month period. People with hypertension may be tested at regular intervals, with the frequency determined by their healthcare provider.
How is urine albumin test used?
The urine albumin test or albumin/creatinine ratio (ACR) is used to screen people with chronic conditions, such as diabetes and high blood pressure (hypertension) that put them at an increased risk of developing kidney disease. Studies have shown that identifying individuals in the very early stages of kidney disease helps people and healthcare providers adjust treatment. Controlling diabetes and hypertension by maintaining tight glycemic control and reducing blood pressure delay or prevent the progression of kidney disease.
Albumin is a protein that is present in high concentrations in the blood. Virtually no albumin is present in the urine when the kidneys are functioning properly. However, albumin may be detected in the urine even in the early stages of kidney disease.
If albumin is detected in a urine sample collected at random, over 4 hours, or overnight, the test may be repeated and/or confirmed with urine that is collected over a 24-hour period (24-hour urine).
Most of the time, both albumin and creatinine are measured in a random urine sample and an albumin/creatinine ratio (ACR) is calculated. This may be done to more accurately determine how much albumin is escaping from the kidneys into the urine. The concentration (or dilution) of urine varies throughout the day with more or less liquid being released in addition to the body’s waste products. Thus, the concentration of albumin in the urine may also vary.
Creatinine, a byproduct of muscle metabolism, is normally released into the urine at a constant rate and its level in the urine is an indication of the urine concentration. This property of creatinine allows its measurement to be used to correct for urine concentration in a random urine sample. The American Diabetes Association has stated a preference for the albumin/creatinine ratio for screening for albuminuria indicating early kidney disease. Since the amount of albumin in the urine can vary considerably, an elevated albumin/creatinine ratio should be repeated twice within 3 to 6 months to confirm the diagnosis.
What does abnormal urine albumin test result mean?
Moderately increased albumin levels (normal urinary albumin excretion is <30 mg/day; overt proteinuria is >300 mg/day) found in both initial and repeat urine tests indicate that a person is likely to have early kidney disease. Very high levels are an indication that kidney disease is present in a more severe form. Undetectable levels are an indication that kidney function is normal.
Different medicines can change the result of urine albumin test.
Cautions
- Urine collected during menses may contain excess albumin and collection during this time should be avoided.
- Heavy exercise may increase albumin excretion and should be avoided during collection. Normal values apply to a nonexercised state.
- Bilirubin at 20 mg/dL reduces creatinine by 15% to 20%.
The following may also interfere with urine albumin test results:
- Dehydration
- Dye (contrast media) if you have a radiology scan within 3 days before the urine test
- Strenuous exercise
- Urinary tract infection
- Urine contaminated with fluids from the vagina
The presence of blood in the urine, a urinary tract infection, vigorous exercise, and other acute illnesses may cause a positive test result that is not related to kidney disease. Testing should be repeated after these conditions have resolved.
Interpretation of urine albumin test results
- In random urine specimens, normal urinary albumin excretion is below 17 mg/g creatinine for males and below 25 mg/g creatinine for females 3.
- Microalbuminuria is defined as an albumin:creatinine ratio (ACR) of 17 to 299 for males and 25 to 299 for females.
- Microalbuminuria: 30 to 300 mg albumin/g creatinine
- Macroalbuminuria: > 300 mg albumin/g creatinine
- A ratio of albumin:creatinine (ACR) of 300 or higher is indicative of overt proteinuria.
- Due to biologic variability, positive results should be confirmed by a second, first-morning random or 24-hour timed urine specimen. If there is discrepancy, a third specimen is recommended. When 2 out of 3 results are in the microalbuminuria range, this is evidence for incipient nephropathy and warrants increased efforts at glucose control, blood pressure control, and institution of therapy with an angiotensin-converting-enzyme inhibitor (ACE inhibitor) if the patient can tolerate it.
Studies have shown that elevated levels of urinary albumin (albuminuria) in people with diabetes or hypertension are associated with increased risk of developing cardiovascular disease. More recently, research has been focused on trying to determine if increased levels of albumin in the urine are also indicative of cardiovascular disease risk in those who do not have diabetes or high blood pressure.
Is there anything I can do to prevent microalbuminuria?
Yes, if you are diabetic, follow your healthcare provider’s instructions for maintaining tight control over your blood glucose level. Keeping high blood pressure under control is also effective in preventing kidney damage that leads to microalbuminuria. Some studies have shown that those who have albuminuria can prevent it from worsening or may reverse it with good glycemic and blood pressure control, or by quitting smoking.
Are there other reasons for having increased urine albumin levels?
Yes, albuminuria is not specific for diabetes. It may also be associated with hypertension (high blood pressure), some lipid abnormalities, and several immune disorders. Elevated results may also be caused by vigorous exercise, blood in the urine, urinary tract infection, dehydration, and some drugs.
What is the difference between serum/plasma albumin, prealbumin, and urine albumin tests?
Although the names are similar, albumin and prealbumin are completely different molecules. They are both proteins made by the liver, however, and both have been used historically to evaluate nutritional status. Serum/plasma (or blood) albumin is now more often used to screen for and help diagnose liver or kidney disease and is tested on a blood sample. The urine albumin test (also called a microalbumin test) detects and measures albumin in the urine as an early indicator of kidney damage.
- Krolewski AS, Laffel LM, Krolewski M, et al: Glycosylated hemoglobin and the risk of microalbuminuria in patients with insulin-dependent diabetes mellitus. N Engl J Med 1995;332:1251-1255[↩]
- Bennett PH, Haffner S, Kasiske BL, et al: Screening and management of microalbuminuria in patients with diabetes mellitus: recommendations to the Scientific Advisory Board of the National Kidney Foundation from an ad hoc committee of the Council on Diabetes Mellitus of the National Kidney Foundation. Am J Kidney Dis 1995;25:107-112[↩]
- Zelmanovitz T, Gross JL, Oliveira JR, et al: The receiver operating characteristics curve in the evaluation of a random urine specimen as a screening test for diabetic nephropathy. Diabetes Care 1997;20:516-519[↩]





{kind=link}