
What is anagen effluvium
Anagen effluvium refers to hair loss that arises during the anagen phase or growth stage of the hair cycle. Anagen effluvium is often referred to as chemotherapy-induced hair loss (alopecia), as it can be triggered by antimetabolites, alkylating agents and mitotic inhibitors administered as chemotherapeutic therapy 1. Anagen effluvium is most often secondary to chemotherapy, but it has also been associated with radiotherapy, heavy metal poisoning, protein malnutrition, or systemic diseases 2. Any of these factors may cause abrupt cessation of mitosis in the hair matrix 3. Hair shedding usually takes place within 14 days of administration of the offending drug. Since 80-90% of scalp hairs are in the anagen phase, a large number of hairs are affected. Patients with 10% to 20% of their hair remaining after an insult almost certainly have an anagen effluvium 2. However, in many instances it is reversible, with hair regrowth growth upon discontinuation of the offending agent. Anagen effluvium may lead to diffuse non-scarring alopecia (baldness). This is in contrast to telogen effluvium or hair shedding that arises during the telogen or resting stage of the hair cycle.
Hair loss occurs when something stops the hair from growing. The most common causes of anagen effluvium include:
- Hereditary hair loss
- Immune system overreacts
- Some drugs and treatments
- Hairstyles that pull on the hair
- Harsh hair care products
- Compulsion to pull out one’s hair
If you have anagen effluvium, your hair will not grow until the cause stops. For example, people who undergo chemotherapy or radiation treatments often lose a lot of hair. When the treatment stops, their hair tends to regrow.
If you suspect that a treatment or drug is causing your hair loss, talk with your doctor. Serious side effects can occur if you immediately stop a treatment or drug.
Many new moms see noticeable hair loss a few months after having a baby. This is normal — and not true hair loss. Dermatologists refer to this condition as excessive hair shedding. The excessive shedding is caused by falling estrogen levels. The good news is that this excessive shedding is temporary, and you do not have to do anything to remedy it. Most women see their hair return to its normal fullness by their child’s first birthday. Many women regain normal fullness even earlier.
Other causes of anagen effluvium may require treatment. Many people who have hereditary hair loss continue to lose hair without treatment. A woman who inherits the genes for hereditary hair loss may notice gradual thinning. Men who have hereditary hair loss tend to develop a receding hairline or bald patch that begins in the center of the scalp.
Chemotherapy-induced hair loss has a great impact on the quality of life in patients; it is considered to be one of the most traumatic factors in care of these patients. It has a negative impact on individual perceptions of appearance, body image, sexuality, and self-esteem. In a study, 47% of female patients considered hair loss to be the most traumatic aspect of chemotherapy and 8% declined chemotherapy due to fears of hair loss 4.
Treatment helps many people who have hair loss, but not everyone. A dermatologist can tell you what to expect.
Figure 1. Anagen effluvium

Hair Growth Cycle
Hair follicles extend deep into the dermis, often projecting into the underlying subcutaneous layer. The epithelium at the follicle base surrounds a small hair papilla, a peg of connective tissue containing capillaries and nerves. The hair bulb consists of epithelial cells that surround the papilla.
Hair production involves a specialized keratinization process. The hair matrix is the epithelial layer involved in hair production. When the superficial basal cells divide, they produce daughter cells that are pushed toward the surface as part of the developing hair. Most hairs have an inner medulla and an outer cortex. The medulla contains relatively soft and flexible soft keratin. Matrix cells closer to the edge of the developing hair form the relatively hard cortex. The cortex contains hard keratin, which gives hair its stiffness. A single layer of dead, keratinized cells at the outer surface of the hair overlap and form the cuticle that coats the hair.
The hair root anchors the hair into the skin. The root begins at the hair bulb and extends distally to the point where the internal organization of the hair is complete, about halfway to the skin surface. The hair shaft extends from this halfway point to the skin surface, where we see the exposed hair tip.
The size, shape, and color of the hair shaft are highly variable.
Growth and Replacement of Hair
A hair in the scalp grows for two to five years, at a rate of around 0.33 mm/day (about 1/64 inch). Variations in hair growth rate and the duration of the hair growth cycle account for individual differences in uncut hair length. A given hair goes through a hair cycle consisting of three developmental stages (see Figure 2):
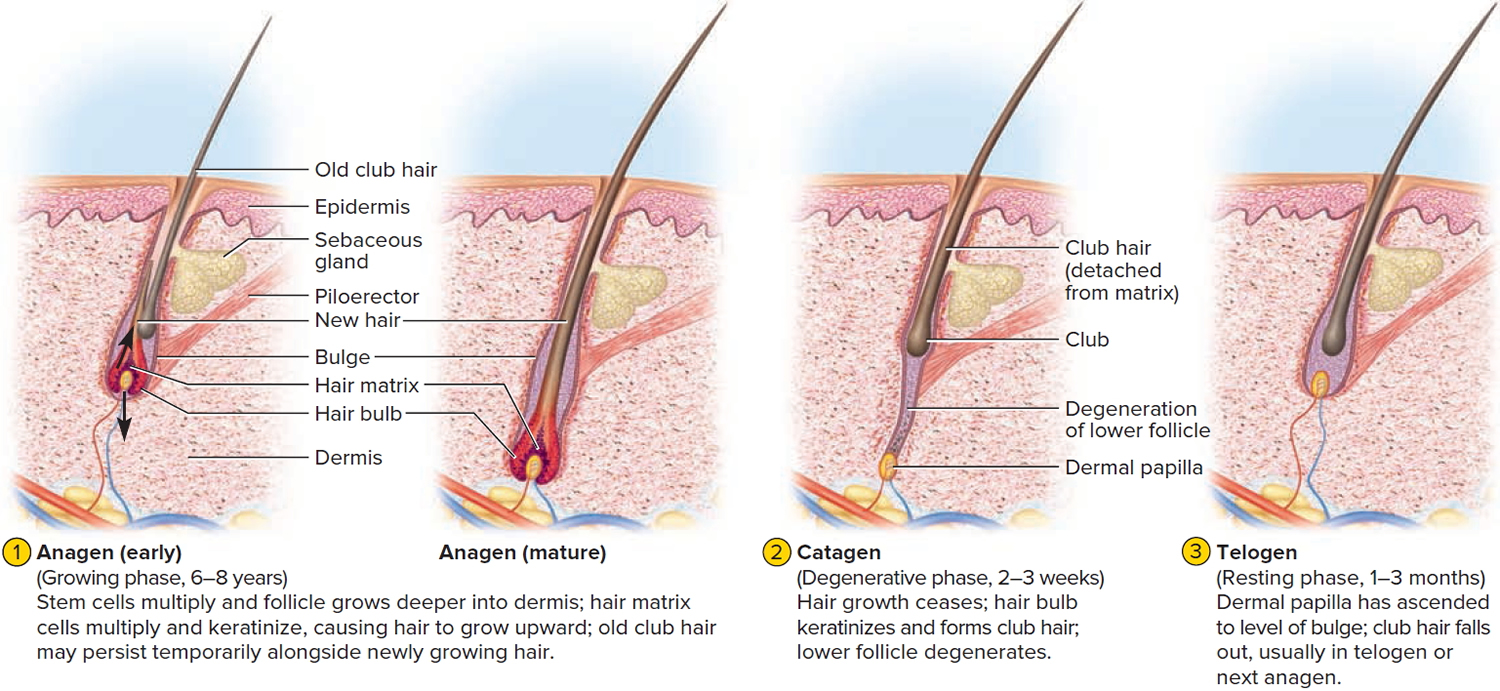
- Anagen (growing phase). The anagen phase constitutes about 90% (1000 days or more) of the growth cycle 5. Anagen hairs are anchored deeply into the subcutaneous fat and cannot be pulled out easily.
- Catagen (involuting phase). The catagen phase is a much shorter phase, lasting three to six weeks. During this phase, the hair follicles go through a process of programmed cell death (apoptosis) 6.
- Telogen (resting phase). The telogen phase lasts for around three to five months, and 10% of the scalp hair are in this phase. During this phase, the hair shaft matures into a club hair, which is eventually shed from the follicle. If the percentage of scalp follicles present in the telogen phase increases, this results in excessive shedding of hair 5.
At any given time, about 90% of the scalp follicles are in the anagen stage. In this stage, stem cells from the bulge in the follicle multiply and travel downward, pushing the dermal papilla deeper into the skin and forming the epithelial root sheath. Root sheath cells directly above the papilla form the hair matrix. Here, sheath cells transform into hair cells, which synthesize keratin and then die as they are pushed upward away from the papilla. The new hair grows up the follicle, often alongside an old club hair left from the previous cycle.
The catagen phase (10 days) and telogen phase (100 days) constitute only 10% of the hair growth cycle. During the catagen and telogen phase of the hair growth cycle, as hairs are at the shedding and rest-from-growth period, no bald spots are shown as hairs are randomly distributed over the scalp.
In the catagen stage, mitosis in the hair matrix ceases and sheath cells below the bulge die. The follicle shrinks and the dermal papilla draws up toward the bulge. The base of the hair keratinizes into a hard club and the hair, now known as a club hair, loses its anchorage. Club hairs are easily pulled out by brushing the hair, and the hard club can be felt at the hair’s end. When the papilla reaches the bulge, the hair goes into a resting period called the telogen stage. Eventually, anagen begins anew and the cycle repeats itself. A club hair may fall out during catagen or telogen, or as it is pushed out by the new hair in the next anagen phase.
You lose about 50 to 100 scalp hairs daily. In a young adult, scalp follicles typically spend 6 to 8 years in anagen, 2 to 3 weeks in catagen, and 1 to 3 months in telogen. Scalp hairs grow at a rate of about 1 mm per 3 days (10–18 cm/yr) in the anagen phase.
Hair grows fastest from adolescence until the 40s. After that, an increasing percentage of follicles are in the catagen and telogen phases rather than the growing anagen phase. Hair follicles also shrink and begin producing wispy vellus hairs instead of thicker terminal hairs. Thinning of the hair, or baldness, is called alopecia. It occurs to some degree in both sexes and may be worsened by disease, poor nutrition, fever, emotional stress, radiation, or chemotherapy. In the great majority of cases, however, it is simply a matter of aging.
Pattern baldness (androgenic alopecia) is the condition in which hair is lost unevenly across the scalp rather than thinning uniformly. It results from a combination of genetic and hormonal influences. The relevant gene has two alleles: one for uniform hair growth and a baldness allele for patchy hair growth. The baldness allele is dominant in males and is expressed only in the presence of the high level of testosterone characteristic of men. In men who are either heterozygous or homozygous for the baldness allele, testosterone causes terminal hair to be replaced by vellus hair, beginning on top of the head and later the sides. In women, the baldness allele is recessive. Homozygous dominant and heterozygous women show normal hair distribution; only homozygous recessive women are at risk of pattern baldness. Even then, they exhibit the trait only if their testosterone levels are abnormally high for a woman (for example, because of a tumor of the adrenal gland, a woman’s principal source of testosterone). Such characteristics in which an allele is dominant in one sex and recessive in the other are called sex-influenced traits.
Excessive or undesirable hairiness in areas that are not usually hairy, especially in women and children, is called hirsutism. It tends to run in families and usually results from either masculinizing ovarian tumors or hypersecretion of testosterone by the adrenal cortex. It is often associated with menopause.
Contrary to popular misconceptions, hair and nails do not continue to grow after a person dies, cutting hair does not make it grow faster or thicker, and emotional stress cannot make the hair turn white overnight.
Figure 2. Hair growth cycle
Anagen effluvium causes
The main causes of anagen effluvium are an infection, drugs, toxins, radiation to the head and neck and autoimmune disease 7, 8. Several chemotherapy antimetabolites, alkylating agents, and mitotic inhibitors have been implicated in the pathogenesis of anagen effluvium 1. Doxorubicin, the nitrosoureas, and cyclophosphamide have been implicated too. Several other drugs such as isoniazid (INH), levodopa, colchicine, cyclosporine, and toxic heavy metals such as thallium, mercury, boron, bismuth, copper, and cadmium have also been implicated in triggering anagen effluvium 1. Once chemotherapy has been initiated, anagen effluvium presents within days to a few weeks. The severity of hair loss differs between patients, but it is not unusual for a patient to have complete hair loss within 2 to 3 months of beginning chemotherapy.
Anagen effluvium can also be seen in inflammatory disorders such as alopecia areata, systemic lupus erythematosus (SLE) and syphilis secondary to inflammatory insult to the hair bulb resulting in anagen arrest 9. Pemphigus vulgaris can also cause anagen effluvium, as desmosomal proteins are expressed in the epithelium of the hair follicle 10. Anagen effluvium has also been described following severe dietary protein malnutrition states (e.g., Kwashiorkor). Radiation has also been shown to cause both reversible and permanent alopecia. Permanent destruction of the hair follicle occurs when hair follicle stem cells are damaged, and this usually occurs with greater than 30 Gray of deep x-rays 11.
Anagen effluvium has been described in a 2-year old male with severe hypotension and hypoxia requiring extracorporeal membrane oxygenation (ECMO) 12.
Infections may interrupt hair growth in a localized area resulting in a single bald patch or several bald patches. Loose hairs can readily be extracted from the infected area, which may be swollen, boggy and crusted. Examples include:
- Boils and abscesses
- Fungal hair infection: tinea capitis or kerion.
Toxins that can interrupt hair growth include:
- Toxicity due to chemotherapy agents, usually prescribed to treat cancer, especially when multiple drugs are used or they are in high dose. Severe hair loss is reported from doxorubicin, the nitrosoureas, and cyclophosphamide. Other causes are bleomycin, dactinomycin, daunorubicin, systemic fluorouracil, and high-dose methotrexate.
- Other medicines such as colchicine and ciclosporin (which more often causes increased hair growth)
- Poisons such as thallium, arsenic, gold and bismuth.
Alopecia develops within 2 to 4 weeks of chemotherapy. It affects most parts of the scalp, but other sites may be affected, such as eyebrows, armpits and genital area.
Radiation to the scalp can result in anagen effluvium. Regrowth of hair may be incomplete or may not occur.
Autoimmune hair loss includes alopecia areata and its variants, alopecia totalis and alopecia universalis. Anagen effluvium may also occur in the rare immunobullous disease, pemphigus vulgaris.
Anagen effluvium pathophysiology
The anagen phase of the hair is characterized by proliferation of the epithelial compartment, with the bulb matrix cells exhibiting the greatest proliferative activity in building up the hair shaft. Any insult that impairs mitosis of hair follicle keratinocytes can cause anagen effluvium. Disruption to cell division in the hair matrix makes the hair narrowed at its base and susceptible to breakage just above the zone of keratinization 13. The necrotic matrix forms plugs consisting of melanin, keratin and inner root sheath which are extruded through the follicular opening. This process is known as trichomalacia.
The hair bulb itself may be damaged and the hairs may separate at the bulb and fall out. The insult is severe enough to cause a change in the rate of hair growth but does not convert the hair follicle to a different growth phase, as occurs in telogen effluvium. Hair shedding usually begins 1 to 3 weeks after this incident. Due to its long anagen phase, the scalp is the most common location for hair loss, while other terminal hairs are variably affected depending on the percentage of hairs in anagen. Normally, up to 90% of scalp hairs are in the anagen phase, and as such, hair loss is usually copious and results in alopecia that is quite obvious. In addition, chemotherapy given at high doses for a sufficiently long duration and with multiple exposures may also affect hairs of the beard, eyebrows, and eyelashes, as well as axillary and pubic regions 7.
The severity of hair loss after chemotherapy or radiation depends on timing, dose, and duration of the treatment and synchronization of hair cycle. When hair is in late anagen phase, during which the mitotic rate slows down spontaneously, it simply accelerates its normal path to telogen like in androgenetic alopecia. Furthermore, synchronization of hair cycles also plays a role like in androgenetic alopecia, duration of anagen is shortened and even a minor antimitotic insult can produce marked hair loss 14.
In anagen effluvium, only the proliferating cells in the bulb are affected, the quiescent stem cells of the bulge that are responsible for reinitiating follicle growth are spared, so hair loss is usually completely reversible. The hair follicle resumes normal cycling within a few weeks of cessation of insult/event and regrowth is apparent within 1-3 months 15. The new hair may have different characteristics like graying, curling, or straightening effect, which is likely due to differential effects of chemotherapy or radiotherapy on hair follicle melanocytes and inner root sheath epithelium 7.
Radiation-induced alopecia may be reversible or permanent. Radiation-induced temporary hair loss may be observed following neuroradiologically guided embolization procedures 2. Regrowth after radiation therapy depends on type, depth, and dose-fractionation. Permanent follicular destruction is commonly seen, most likely due to irreversible damage to hair follicle stem cells. Permanent alopecia occurs with >30 Gray of deep X-rays or >50 Gray of soft X-rays 2. Persistent radiation-induced inflammatory changes that progressively damage the stem cells may lead to scarring alopecia even after cessation of radiation therapy 8.
Many heavy metals are capable of disrupting the formation of hair shaft by binding with the sulphydryl group of the keratins in the hair. Thallium, mercury, bismuth, copper, and cadmium are the most common metals responsible for this kind of hair loss. Mercury intoxication can occur through chronic industrial exposure, consumption of polluted water/seafood and exposure to mercury-containing antiseptics or fungicides. It can lead to hair loss with or without other symptoms of mercury poisoning 16. Elevated mercury levels in hair, blood, or urine are considered diagnostic.
Boric acid intoxication may be due to pesticides or ingestion of household products where boric acid is a preservative. Patients may develop hair loss along with other signs and symptoms like gastrointestinal, central nervous system, and renal symptoms; a hemorrhagic diathesis; and exfoliation or bullae 17. Blood boric acid levels are elevated in affected patients.
Thallium poisoning can cause anagen hair loss within 2 to 3 weeks after exposure 18. Patient usually presents with primarily neurologic symptoms like irritability, dysesthesia, ataxia, convulsions and coma. However, arsenic exposure does not cause hair loss, instead, arsenic is concentrated in the hair, which facilitates a diagnosis long after intoxication may have occurred 13.
Alopecia areata is a common cause of dystrophic anagen effluvium in a healthy child or adult 19. Alopecia areata is a good illustration of importance of hair cycle disturbances in hair loss. The inflammatory cell infiltrate almost exclusively attacks anagen hair bulbs; this immune attack then catapults anagen follicles into a dystrophic catagen, causing a major hair cycle disturbance and rapid shedding of the insufficiently anchored, improperly formed hair shafts. Dystrophic anagen hairs have also been observed in patients with alopecia areata incognita by Quercetani et al. 19 and they proposed that in some patients with diffuse hair loss diagnosed as telogen effluvium some patients may have alopecia areata incognita. Similar may be the case in pemphigus 10. The hair follicle is a preferential target for pemphigus autoantibodies because the desmosomal proteins are overexpressed in the follicular epithelium. The hairs may come out from the lesional and perilesional areas with their outer root sheath and showing a normal anagen pattern. The normal anagen effluvium suggests a subclinical involvement of the hair follicle and can be considered a Nikolsky sign of the scalp. It may even herald pemphigus 10.
Anagen effluvium symptoms
Anagen effluvium refers to hair shedding that arises during the anagen or growth stage of the hair cycle. It may lead to diffuse non-scarring alopecia (baldness).
Anagen effluvium presents with abrupt shedding of much of or all of the hair on the scalp, and often from the entire body including eyebrows, eyelashes and body hair. Anagen effluvium may leave the scalp partially or completely bald shortly after the traumatic event with up to 90% hair loss over a period of weeks.
Other features depend on the cause of the hair shedding.
Anagen effluvium types
Anagen effluvium is categorized into two types: The common dystrophic anagen effluvium and the loose anagen syndrome 13.
Dystrophic anagen effluvium
Although many drugs have been occasionally described to produce hair loss, the relationship between drug intake and hair loss has only been proven for a few agents. The type of hair loss (i.e. telogen effluvium, anagen effluvium, or both) depends on the medication, its dosage, and patient susceptibility 7.
Anagen effluvium is more common and severe with combination chemotherapy than with the use of a single drug, and the severity is generally dose dependent 7. While hair loss from anticancer therapy has traditionally been categorized as dystrophic anagen effluvium, more recently, it has been suggested that the hair follicle may respond to the same insult that is capable of stopping mitosis with both shedding patterns, i.e. dystrophic anagen effluvium and telogen effluvium 20. Accordingly, the hair may fall out very quickly in clumps or gradually depending on the mitotic activity of the hair follicle at the moment of the insult.
Diffuse, reversible alopecia was reported in 50% of patients receiving treatment with tyrosine kinase inhibitors such as sorafenib and sunitinib 21 and in 65% of patients treated with vismodegib (approved for advanced basal cell cancer) that inhibits sonic hedgehog signaling 22. Similarly, small molecule inhibitors of the epidermal growth factor receptor (EGFR) as well as monoclonal antibodies targeting the EGFR like cetuximab can induce a constellation of cutaneous symptoms known by the acronym PRIDE (Papulopustules and/or paronychia, Regulatory abnormalities of hair growth, Itching and Dryness due to EGFR inhibitors) 23. Mice with a targeted deletion in the EGFR gradually develop scarring alopecia 24. These findings suggest that tyrosine kinase inhibitors and EGFR may be important molecular targets in drug-induced anagen hair loss or permanent alopecia.
The overall incidence of chemotherapy-induced hair loss is estimated to be 65% 7. The prevalence and severity of hair loss is variable and dependent on chemotherapeutic agent and treatment protocol. There are multiple classes of anticancer drugs that can induce alopecia, with different frequencies of hair loss across the four major drug classes: More than 80% for antimicrotubule agents (e.g. paclitaxel), 60-100% for topoisomerase inhibitors (e.g. doxorubicin), >60% for alkylators (e.g. cyclophosphamide), and 10-50% for antimetabolites (e.g. 5-fluorouracil plus leucovorin) 7.
The majority of chemotherapy-induced alopecia is reversible once therapy is discontinued, with the possible exception of the epidermal growth factor receptor (EGFR) inhibitors, chemotherapy with busulfan and cyclophosphamide, and following bone marrow transplantation 25 and it has also been associated with certain risk factors, including chronic graft-versus-host reaction, previous exposure to X-ray and age of patients 7.
Loose Anagen Hair Syndrome
The loose anagen hair syndrome is a rare sporadic or autosomal dominant disorder with incomplete penetrance characterized by loosely anchored anagen hairs that can be easily and painlessly pulled from the scalp. It primarily affects light-haired children, with a female predominance (female to male ratio is 6:1), but rarely adults may also be affected 26. Loose anagen syndrome may result from premature and abnormal keratinization of the inner root sheath, leading to clefts between the inner and outer sheath and the hair shaft. In some patients this may result from hereditary keratin defects in the inner root sheath and/or the apposed companion layer (e.g. in families with diffuse partial woolly hair with loose anagen hair syndrome) 27.
The typical profile of patient with loose anagen syndrome is a young girl with short blond hair that does not grow long, but loose anagen hair syndrome can affect children with dark hair as well. They may have sparse hair that does not grow long and have patches of dull, unruly, or matted hair with increased hair shedding. Examination shows diffuse thinning and irregular bald patches due to traumatic painless extraction of hairs. Most cases are isolated, but it can occur in hereditary or developmental disorders including coloboma, Noonan′s syndrome, and hypohidrotic ectodermal dysplasia 28. Loose anagen syndrome like changes have also been associated with AIDS (AIDS trichopathy) 29.
The key to diagnosing loose anagen hair syndrome is a high index of suspicion during the examination of an infant or toddler with diffuse nonscarring alopecia. In a study of 374 children and teenagers with hair loss, approximately 10% had loose anagen hair syndrome, which made it a common diagnosis 30.
Unlike other nonscarring childhood hair disorders that may have associated autoimmune or hormonal findings and may require further laboratory testing based on clinical presentation and family history, most patients with loose anagen hair syndrome have no associated laboratory test result abnormalities 31.
Microscopic examination shows anagen hair without sheath. The bulb is often misshapen, and its proximal portion often shows a visible ruffled cuticle. The hair pull test in normal children shows one or two loose anagen hairs. However, mere presence of anagen hair is not diagnostic; loose anagen hair syndrome should only be diagnosed microscopically when there is a predominance (>50%) of loose anagen hairs on a trichogram 30.
Most cases of loose anagen hair syndrome resolve spontaneously by adulthood or adolescence; so observation is the treatment of choice; however, minoxidil therapy in infants may be a reasonable therapeutic option in patients with severe disease 30.
Anagen effluvium diagnosis
The diagnosis is usually made by taking a careful history, particularly of recent medicines, and by examining the scalp and shed hair. It is possible to identify anagen and telogen hairs with the naked eye alone. However, it can be helpful to observe hair microscopically.
In anagen effluvium, the hallmark physical exam finding is the end of the hair that comes from the scalp is tapered, narrowed, irregular, or broken off. Anagen hairs have long roots covered with the inner and outer root sheaths and are pigmented. In contrast, telogen hair is a roundish bulb or club-shaped roots, no inner or outer root sheaths and depigmentation of the proximal part of the shaft. The follicular openings remain in both conditions.
A trichogram (forcible hair plucking within a unit area to determine the ratio of anagen to telogen hair) will show a large proportion of dystrophic anagen hairs.
A biopsy is rarely necessary, as a diagnosis can usually be made on history and physical exam findings alone. If a biopsy is requested or necessary for diagnosis, it can help exclude telogen effluvium. In anagen effluvium, histopathologic evaluation of a punch biopsy of the scalp will exhibit a normal anagen-to-telogen ratio, which is less than 15% telogen hair follicles. If greater than 15% of the hair follicles are in the telogen phase, this more supports a diagnosis of telogen effluvium.
Other tests may be arranged to rule out other causes of hair loss, including iron deficiency, thyroid disease, systemic lupus and infections (e.g., syphilis).
Anagen effluvium treatments
The management of anagen effluvium should be aimed at limiting the amount of time the patient suffers from alopecia. To date, several agents have been studied; unfortunately, no treatment appears to be effective in preventing or stopping the hair loss.
Anagen effluvium due to chemotherapy is expected to recover fully within 3-6 months of stopping it. The hair nearly always grows back normally, but sometimes patients with straight hair develop curly hair when it regrows. Hair color may also change.
Suggested treatments for anagen effluvium include:
- Topical minoxidil solution. It has been suggested that topical minoxidil is effective in reducing the period of baldness by an average of fifty days.
- Scalp cooling during chemotherapy. Inducing scalp hypothermia to a scalp temperature of fewer than 24 degrees Celsius during chemotherapy has shown success with daunorubicin, doxorubicin, paclitaxel, vincristine, vinblastine, mechlorethamine, actinomycin D, and epirubicin 32. At this time, scalp cooling in the US with the newer systems costs about $1500 to $3000 total per person and so far is not likely to be reimbursed by health insurance, according to an editorial accompanying the studies 33, 34. However, some doctors have been concerned they could interfere with chemotherapy by keeping it from reaching any stray cancer cells lurking in the scalp. Some believe that the scalp cooling might protect any cancer cells there and allow them to survive the chemo and keep growing. However, recent studies have shown no link between scalp cooling and cancer cells spreading to the scalp, or decreased survival among women with breast cancer. None of the women in the Journal of the American Medical Association studies developed cancer spread to the scalp during the 2-to-3-year study periods; researchers will continue to monitor them for up to 5 years.
- Cosmetic camouflage to eyebrows.
- Several studies have described limiting drug delivery to the scalp by using a scalp tourniquet during chemotherapy. It should be noted, however, that if scalp or brain metastases are a possibility, this method should not be used to allow penetration of the chemotherapeutic agent.
Other things you can do when you have hair loss
- Your scalp may feel itchy or sensitive. Be gentle when brushing and washing your hair. Using a wide-toothed comb may help.
- Hair loss might be somewhat reduced by avoiding too much brushing or pulling (which can happen when making braids or ponytails, using rollers, blow drying, or using curling or flat irons).
- If your hair becomes very thin or is completely gone during chemo, be sure to protect the skin on your scalp from heat, cold, and sun. Use a broad-spectrum sunscreen with a sun protection factor (SPF) of at least 30 and wear a hat. In cold weather, wear a hat or scarf to cover your head and stay warm.
- When new hair starts to grow, it may break easily at first. Avoid perms and dyes for the first few months. Keep hair short and easy to style.
- If you’re going to buy a wig, try on different styles until you find one you really like. Consider buying 2 wigs, one for everyday use and one for special occasions. Synthetic wigs need less care and styling than human hair wigs. They also cost less and may be easier to manage if your energy is low during cancer treatment.
- Some people find wigs are hot or itchy, and use turbans or scarves instead. Cotton fabrics tend to stay on a smooth scalp better than nylon or polyester.
- Wear a hair net at night, or sleep on a satin pillowcase to keep hair from coming out in clumps. Be gentle with eyelashes and eyebrows, which might also be affected.
- Your new hair may be curlier or straighter, thicker or finer—or even a new color. Usually this change is short term; with time your hair will very likely go back to the way it was before treatment.
Anagen effluvium prognosis
Anagen effluvium is reversible. The hair follicle resumes normal activity after any toxic agent is withdrawn. Complete regrowth occurs after 3–6 months after chemotherapy in most cases. Sometimes the hair regrows despite the continuation of chemotherapy.
Anagen effluvium due to alopecia areata may persist; recovery is unpredictable.
- Saleh D, Nassereddin A, Cook C. Anagen Effluvium. [Updated 2021 Aug 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482293[↩][↩][↩]
- Trüeb RM. Diffuse hair loss. In: Blume-Peytavi U, Tosti A, Whiting DA, Trüeb RM, editors. Hair Growth and Disorders. Berlin: Springer; 2008. p. 259-72.[↩][↩][↩][↩]
- Fonia A, Cota C, Setterfield JF, Goldberg LJ, Fenton DA, Stefanato CM. Permanent alopecia in patients with breast cancer after taxane chemotherapy and adjuvant hormonal therapy: Clinicopathologic findings in a cohort of 10 patients. J Am Acad Dermatol. 2017 May;76(5):948-957. doi: 10.1016/j.jaad.2016.12.027[↩]
- McGarvey EL, Baum LD, Pinkerton RC, Rogers LM. Psychological sequelae and alopecia among women with cancer. Cancer Pract 2001;9:283-9.[↩]
- Shapiro, J., Wiseman, M., & Lui, H. (2000). Practical management of hair loss. Canadian family physician Medecin de famille canadien, 46, 1469–1477. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2144852/pdf/canfamphys00029-0071.pdf[↩][↩]
- Lindner, G., Botchkarev, V. A., Botchkareva, N. V., Ling, G., van der Veen, C., & Paus, R. (1997). Analysis of apoptosis during hair follicle regression (catagen). The American journal of pathology, 151(6), 1601–1617. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1858357/pdf/amjpathol00024-0099.pdf[↩]
- Trüeb R. Chemotherapy-induced Hair Loss. Skin Therapy Lett 2010;15:5-7.[↩][↩][↩][↩][↩][↩][↩][↩]
- Sinclair R, Grossman KL, Kvedar JC. Anagen hair loss, in Disorders of Hair Growth: Diagnosis and Treatment. In: Olsen EA, editor. McGraw-Hill: New York; 2002.p. 275.[↩][↩]
- Sperling LC. Hair and systemic disease. Dermatol Clin 2001;19:711-26.[↩]
- Delmonte S, Semino MT, Parodi A, Rebora A. Normal anagen effluvium: A sign of pemphigus vulgaris. Br J Dermatol 2000;142:1244-5.[↩][↩][↩]
- Sonthalia S, Daulatabad D. Azathioprine-associated anagen effluvium. Indian J Dermatol Venereol Leprol. 2016 May-Jun;82(3):322-4. doi: 10.4103/0378-6323.174411[↩]
- Cotter L, Cheng K, Kirkorian AY. Anagen Effluvium in Association With Extracorporeal Membrane Oxygenation. Pediatr Dermatol. 2017 Jul;34(4):e201-e202. doi: 10.1111/pde.13183[↩]
- Paus R, Olsen EA, Messenger AG. Hair Growth Disorders. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Zller AS, Leffell DJ, editors. Fitzpatrick′s Dermatology in General Medicine. 7 th ed., vol. 2. New York: McGraw-Hill; 2008. p. 753-77.[↩][↩][↩]
- Tosti A, Pazzaglia M. Drug reactions affecting hair: Diagnosis. Dermatol Clin 2007;25:223-31.[↩]
- Vowels M, Chan LL, Giri N, Russell S, Lam-Po-Tang R. Factors affecting hair regrowth after bone marrow transplantation. Bone Marrow Transplant 1993;12:347-50.[↩]
- Elhassani SB. The many faces of methyl mercury poisoning. J Toxicol Clin Toxicol 1982;19:875-906.[↩]
- Stein KM, Odom RB, Justice GR, Martin GC. Toxic alopecia from ingestion of boric acid. Arch Dermatol 1973;108:95-7.[↩]
- Bank WJ, Pleasure DE, Suzuki K, Nigro M, Katz R. Thallium poisoning. Arch Neurol 1972;26:456-64.[↩]
- Quercetani R, Rebora AE, Fedi MC, Carelli G, Mei S, Chelli A, et al. Patients with profuse hair shedding may reveal anagen hair dystrophy: A diagnostic clue of alopecia areata incognita. J Eur Acad Dermatol Venereol 2011;25:808-10.[↩][↩]
- Trueb RM. Chemotherapy-induced anagen effluvium: Diffuse or patterned? Dermatology 2007;215:1-2.[↩]
- Robert C, Mateus C, Spatz A, Wechsler J, Escudier B. Dermatologic symptoms associated with the multikinase inhibitor sorafenib. J Am Acad Dermatol 2009;60:299-305.[↩]
- O′Bryan KW, Ratner D. The role of targeted molecular inhibitors in the management of advanced nonmelanoma skin cancer. Semin Cutan Med Surg 2011;30:57-61.[↩]
- Donovan JC, Ghazarian DM, Shaw JC. Scarring alopecia associated with use of the epidermal growth factor receptor inhibitor gefitinib. Arch Dermatol 2008;144:1524-5.[↩]
- Murillas R, Larcher F, Conti CJ, Santos M, Ullrich A, Jorcano JL. Expression of a dominant negative mutant of epidermal growth factor receptor in the epidermis of transgenic mice elicits striking alterations in hair follicle development and skin structure. EMBO J 1995;14:5216-23.[↩]
- Palamaras I, Misciali C, Vincenzi C, Robles WS, Tosti A. Permanent chemotherapy-induced alopecia: A review. J Am Acad Dermatol 2011;64:604-6.[↩]
- Tosti A, Piraccini BM. Loose anagen hair syndrome and loose anagen hair. Arch Dermatol 2002;138:521-2.[↩]
- Chapalain V, Winter H, Langbein L, Le Roy JM, Labrèze C, Nikolic M, et al. Is the loose anagen hair syndrome a keratin disorder? A clinical and molecular study. Arch Dermatol 2002;138:501-6.[↩]
- Hansen LK, Brandrup F, Clemmensen O. Loose anagen syndrome associated with colobomas and dysmorphic features. Clin Dysmorphol 2004;13:31-2.[↩]
- Sadick NS. Clinical and laboratory evaluation in AIDS trichopathy. Int J Dermatol 1993;32:33-8.[↩]
- Cantatore-Francis JL, Orlow SJ. Practical guidelines for evaluation of loose anagen hair syndrome. Arch Dermatol 2009;145:1123-8.[↩][↩][↩]
- Hillmann K, Blume-Peytavi U. Diagnosis of hair disorders. Semin Cutan Med Surg 2009;28:33-8.[↩]
- Kanwar AJ, Narang T. Anagen effluvium. Indian J Dermatol Venereol Leprol. 2013 Sep-Oct;79(5):604-12. doi: 10.4103/0378-6323.116728[↩]
- Nangia J, Wang T, Osborne C, et al. Effect of a Scalp Cooling Device on Alopecia in Women Undergoing Chemotherapy for Breast Cancer: The SCALP Randomized Clinical Trial. JAMA. 2017;317(6):596–605. doi:10.1001/jama.2016.20939[↩]
- Rugo, H. S., Klein, P., Melin, S. A., Hurvitz, S. A., Melisko, M. E., Moore, A., Park, G., Mitchel, J., Bågeman, E., D’Agostino, R. B., Jr, Ver Hoeve, E. S., Esserman, L., & Cigler, T. (2017). Association Between Use of a Scalp Cooling Device and Alopecia After Chemotherapy for Breast Cancer. JAMA, 317(6), 606–614. https://doi.org/10.1001/jama.2016.21038[↩]





{kind=link}