What is arthrocentesis
Arthrocentesis also called joint aspiration, is a procedure to remove fluid from a joint. Arthrocentesis is done most often in the knee, but it may also be done in the hip, ankle, shoulder, and toe. The fluid may be tested to see if you have a joint problem such as bleeding, infection, gout, or pseudogout. Arthrocentesis can also be done to remove extra fluid that causes pressure and pain in the joint.
Arthrocentesis is done to:
- understand why a joint is swollen or sore
- relieve pain by taking fluid out of a joint
Indications for arthrocentesis (synovial fluid aspiration) and analysis include the presentation of acute painful joint with surrounding warmth/erythema, suspicion of septic arthritis, suspicion for subacute or chronic periprosthetic joint infection, acute exacerbation of chronic knee pain from osteoarthritis or non-inflammatory arthritis, or acute trauma with painful effusion. In the clinical presentation of acute injury, often arthrocentesis of hemarthrosis can be therapeutic and provide significant pain relief in the acutely traumatic knee 1. Effusions from chronic inflammatory arthritis can undergo therapeutic aspiration for pain relief. A definitive diagnosis of gout or pseudogout is also an indication for aspiration. It is important to note that infection and gout can co-exist within a joint space. Effusions of unknown etiology warrant aspiration and analysis 2.
Potential diagnosis from arthrocentesis and synovial fluid analysis include:
- Inflammatory arthritis including gout, pseudogout, infection, or spondylarthritis, or non-inflammatory arthritis which can include effusion from osteoarthritis or meniscal tears
- Septic arthropathy: acute septic arthropathy, subacute or chronic septic arthropathy, or periprosthetic joint infection
- Hemorrhagic: traumatic, often seen with tendon, meniscal, or ligament injury
During an arthrocentesis, a doctor uses a needle to take fluid out of your joint. This might be done to test the fluid for infection or to find a cause for a joint problem. These problems may include bleeding, infection, gout, or pseudogout. Sometimes fluid is taken out to relieve pressure and pain from too much fluid in the joint.
The area where the needle is inserted may be numbed before the needle is put in. Then the needle is slowly put into the joint. A syringe attached to the needle is used to remove fluid. The fluid may be put in tubes or containers and sent to the lab. Sometimes an injection of steroid medicine is also given into the joint. This can help relieve inflammation and pain. It can also help prevent the fluid from building up again.
Call your doctor or nurse call line now or seek immediate medical care if:
- You have symptoms of infection, such as:
- Increased pain, swelling, warmth, or redness around the area.
- Red streaks leading from the area.
- Pus draining from the area.
- A fever.
Watch closely for changes in your health, and be sure to contact your doctor or nurse call line if you have any problems.
What are the risks of arthrocentesis?
Arthrocentesis is a safe procedure with very few risks and those that do occur are typically not severe. Potential complications include: bleeding and iatrogenic hemarthrosis, infection within the joint, cartilage damage from needle insertion (rare), pain at arthrocentesis site or local ecchymosis, skin reaction to antiseptics or soft bandage adhesive or allergic reaction can happen. The most common complication reported is reaccumulation of the joint effusion 3. Your doctor will review all risks with you before you have the arthrocentesis procedure.
Joint fluid analysis
Synovial fluid is a thick liquid that acts as a lubricant for the body’s major joints. It is found in small quantities in the spaces between the joints, where the fluid is produced and contained by synovial membranes. Synovial fluid cushions bone ends and reduces friction during joint movement in the knees, shoulders, hips, hands, and feet.
Synovial fluid analysis consists of a group of tests that detect synovial fluid changes and may indicate the presence of diseases affecting joint structure and function. The analysis usually involves an initial basic set of tests, followed by additional tests selected based on the results of the first set of tests, the person’s symptoms, and the disease that the healthcare practitioner suspects is causing the symptoms. Tests can be grouped according to:
- Physical characteristics—an evaluation of the fluid’s appearance
- Chemical tests—detect changes in the fluid’s chemical constituents
- Microscopic examination— cells and crystals that may be present are counted and identified by type under a microscope
- Infectious disease tests—detect and identify microbes, if present
Characteristics of normal synovial fluid analysis include:
- Clear appearance,
- White blood cell count less than 200 cells/microL, polymorphonuclear leukocytes less than 25%,
- Synovial lactate less than 5.6 mmol/L, and
- Glucose levels approximating serum glucose.
Characteristics of synovial fluid analysis in inflammatory conditions (e.g., osteoarthritis, trauma) include:
- Clear/yellow appearance,
- White blood cell count less than 2000 cells/microL, polymorphonuclear leukocytes less than 25%,
- High viscosity, and
- Glucose level approximating serum glucose.
Characteristics of synovial fluid analysis suggestive septic joint include:
- White blood cell count greater than 50,000 cells/microL (greater than 1,100 in a prosthetic joint) with greater than 90% polymorphonuclear leukocytes (greater than 65% in a prosthetic joint).
- Additional suggestive findings include synovial lactate greater than 5.56 mmol/L and LDH >250.
- It is important to note that the absence of one or more of these findings does not definitively differentiate reactive and inflammatory arthritis from infection. It is imperative that the gram stain is obtained if there is a suspicion of septic arthritis. If there is an insufficient quantity of synovial fluid to perform all of the recommended testings, Gram stain must be prioritized.
According to the American Rheumatologic Association guidelines 4:
- Non-inflammatory <200 to 2000 white blood cell count/mm³
- Inflammatory >2000 to 50,000 white blood cell count/mm³
- Infectious > 50,000 white blood cell count/mm³
Differential with polymorphonuclear leukocytes (polymorphic nuclear cells)
- >75 percent polymorphonuclear leukocytes indicative of bacterial joint infection 5
Crystal Analysis: Gout and Pseudogout
- Presence of monosodium urate crystals indicates a diagnosis of gout
- Presence of calcium pyrophosphate dihydrate crystals indicates a diagnosis of pseudogout
Gram stain and bacterial culture: synovial fluid aspirate is analyzed for gram stain and both aerobic and anaerobic culture to determine the presence of infection; the presence of any organism indicates abnormal findings.
Septic arthritis is typically mono-microbial and broken down into two categories, gonococcal and non-gonococcal based on age and history. Adults < 35 years old have infections from Neisseria gonorrhoeae 6. Adults > 35 years old are most likely to present with Staphylococcus aureus infections. History such as recent travel and immunocompromised states can clue the provider into other causative organisms including Strep species, aerobic gram negative, anaerobic gram negative, brucellosis, mycobacterial species, fungal, and Mycoplasma hominis. Crystalline arthritis and autoimmune disease can cause an inflammatory joint effusion. Trauma is the most common cause hemorrhagic joint effusion, but there are case reports of supratherapeutic INRs associated with spontaneous hemarthrosis.
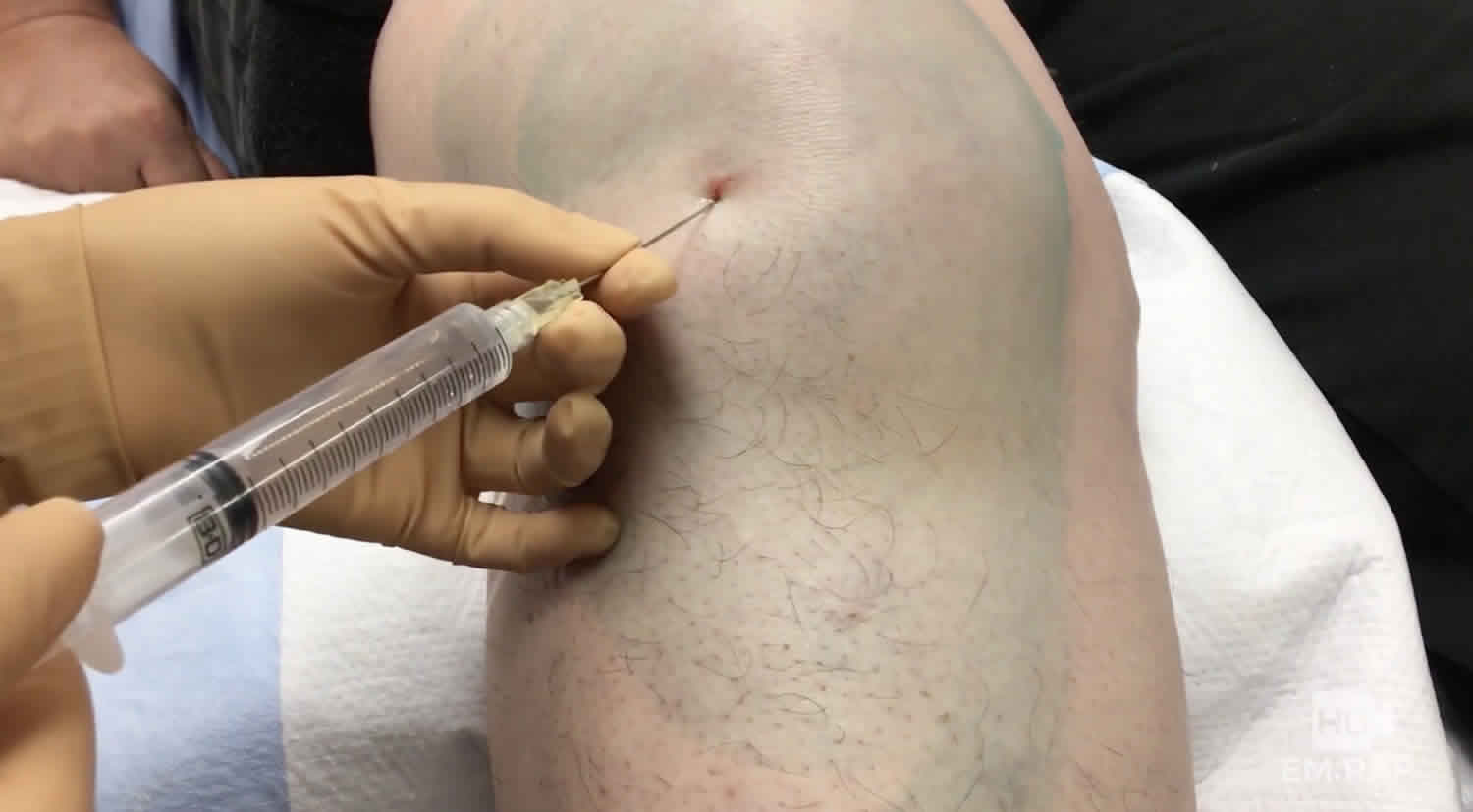
Arthrocentesis procedure
First, the area over the joint will be cleaned to help prevent an infection. Your doctor may then use a needle to numb the skin in the area.
The doctor will insert a different needle into the joint and remove fluid. The needle is slowly put into the joint. The doctor may use ultrasound to help guide the needle into the joint. You may feel some pressure or discomfort. A syringe attached to the needle is used to remove fluid. The fluid may be put in tubes or containers and sent to the lab for testing.
Sometimes pain medicine (local anesthetic) or a cortisone (steroid) shot is also given into the joint. It can help relieve inflammation and pain. It can also help prevent the fluid from building up again.
The whole procedure takes 10 to 30 minutes. But the injection itself takes only a few minutes.
What can you expect after arthrocentesis?
The area around the joint may feel numb for a few hours. If your arthrocentesis also included an injection of a pain reliever and a steroid, then the pain will probably go away right away. But it might come back after a few hours. This may happen when the pain reliever wears off before the steroid medicine starts to work. Steroids don’t always work. But when they do, the pain relief can last for several days to a few months or longer.
You can put ice or a cold pack on your joint for 10 to 20 minutes at a time. Put a thin cloth between the ice and your skin.
Follow-up care is a key part of your treatment and safety. Be sure to make and go to all appointments, and call your doctor or nurse call line if you are having problems. It’s also a good idea to know your test results and keep a list of the medicines you take.
How to you care for yourself at home:
- If you have bandages over the area, keep them clean and dry. You may remove them when your doctor tells you to.
- Put ice or a cold pack on the area for 10 to 20 minutes at a time. Put a thin cloth between the ice and your skin.
- Ask your doctor if you can take an over-the-counter pain medicine, such as acetaminophen (Tylenol), ibuprofen (Advil, Motrin), or naproxen (Aleve). Be safe with medicines. Read and follow all instructions on the label.
- Avoid strenuous activities for several days, especially those that put stress on the area where the needle was put in.
Shoulder arthrocentesis
Shoulder arthrocentesis (shoulder joint aspiration) is a necessary and practical skill in the hands of emergency physicians, surgeons, medical specialists and primary care providers 7. A clinically useful procedure for both diagnostic and therapeutic indications, shoulder arthrocentesis as a diagnostic procedure limited relative contraindications.
Shoulder arthrocentesis/injection techniques are commonly utilized in various treatment and management modalities. Arthrocentesis techniques are often used in clinical settings that require synovial fluid analysis to aid in the diagnosis of inflammatory or septic arthritis. In addition, shoulder arthrocentesis techniques can be used in rheumatologic and traumatic causes, such as when attempting to clinically differentiate between suspected cases of infection versus gout, pseudogout, and/or traumatic hemarthroses.
Therapeutically, the arthrocentesis is utilized to aspirate (or “drain”) shoulder joint effusions in addition to coupling the aspiration with the injection of a local steroid and/or anesthetic for pain relief and to facilitate shoulder reduction in an awake patient. The latter can be beneficial for the patient and help mitigate other risks associated with procedural sedation and IV pain medication use. Glenohumeral intra-articular injections can also be utilized in the setting of pain/symptomatic management of shoulder degenerative joint diseases 8.
In the setting of clinical suspicion for periprosthetic joint infections, in this case following either a standard total shoulder arthroplasty, reverse total shoulder arthroplasty (rTSA), or a shoulder hemiarthroplasty, aspirations sent for extended culture incubation time periods (i.e. 2 to 3 weeks) can be clinically useful to aid clinicians in the appropriate management of these conditions 9.
Shoulder arthrocentesis contraindications
The only absolute contraindication to the procedure is cellulitis overlying the entry point; however, known bacteremia is a relative risk as this procedure in the bacteremic patient could theoretically seed the joint space. High suspicion for bacterial joint infection should prompt synovial fluid analysis even in the bacteremic patient as the risks of improper or incomplete treatment of a septic joint far outweigh the theoretical risk of seeding the joint with bacteria. Another relative contraindication is a bleeding disorder or anticoagulant therapy as this could introduce hemarthroses; however, this risk is low compared to risks associated with bacterial joint infection. Prosthetic joints are considered to be a relative contraindication by some outside of a sterile, surgical environment. However, emergent arthrocentesis may be required if a sterile OR environment is not available.
Shoulder arthrocentesis procedure
Anesthesia
The skin overlying the area of injection can be anesthetized with localized infiltration of 1% lidocaine and a high gauge needle. Alternatively, rapidly evaporating coolants such as ethyl chloride work to provide short-acting anesthesia of the skin at the point of injection. These techniques can be used in combination to anesthetize the skin and underlying soft tissue in increase the comfort of the procedure.
Position
The patient should be seated upright with affected arm in a relaxed position. With the patient in a chair with armrests or on a stretcher with the head of bed elevated and guardrails up, if possible, this ensures that the patient is in a comfortable position to facilitate access to the glenohumeral joint. In addition, with the patient seated or lying down, this can be protective and prophylactic against any falls that may occur during a potential vaso-vagal syncopal episode.
Technique: Anterior Approach
After prepping, sterilizing and draping the skin, the most important step in the shoulder arthrocentesis technique is the proper identification of landmarks which will determine the point of entry into the joint. These landmarks include the humeral head, distal clavicle, and coracoid process. The point of entry is medial to humeral head and inferior/lateral to the coracoid process. Insert needle perpendicular to the skin and into the joint space as depicted in the figure. If you chose to identify your landmarks prior to to the sterilization process, using a skin impression or marking pen at the site of insertion can maintain an accurate position during the prepping and draping of the skin.
While drawing back on the plunger to check for intra-articular blood or synovial fluid. Once the syringe is filled, a hemostat can be placed on the hub of the needle to facilitate removal of a syringe filled with synovial fluid to be sent for analysis and placement of an additional syringe (if needed) to draw of any additional fluid. This same syringe exchange technique can be used to attach a syringe filled with local anesthetic and or injectable steroid as indicated. The skin is then cleaned, and a bandage is placed.
Technique: Posterior Approach
Utilizing the same preparation technique as noted above, the posterior approach is commonly utilized for aspiration/injection to the glenohumeral joint. The entry point is two fingers’ breadth inferior and medial to the palpated posterolateral border of the acromion. The needle is directed anteromedially, with the opposite hand palpating the coracoid process. The coracoid serves as a directional reference point to help guide the clinician’s needle trajectory.
Shoulder arthrocentesis complications
The most important risk to discuss with the patient is an iatrogenic infection. While this complication is rare (approximately 1/10000), it remains a possibility.
- Pain
- Bleeding (from the site and into the joint)
- Damage to surrounding soft tissue (nerves, tendons, etc.)
- Damage to bone or cartilage
Elbow arthrocentesis
Elbow arthrocentesis is a procedure performed to aspirate the contents of a joint cavity to evaluate and treat elbow effusion 6. Arthrocentesis is considered a minor surgical procedure. However, there is always the chance, as with introducing any needle through the skin, for infection, injury to nerves, vessels, tendons, or other connective tissue. Therefore, this procedure should only be performed by health care providers trained in arthrocentesis with a strong understanding of elbow anatomy. Arthrocentesis is commonly used to evaluate the underlying etiology of joint effusion including infectious, inflammatory, and hemorrhagic causes. Aspiration of the joint space and removal of the contents reduces the fluid pressure in the joint capsule and reduces pain. In addition, access to the joint space provides the opportunity to inject therapeutic agents in the setting of pain or degenerative joint disease. Of the causes above, the most important to diagnose properly is septic arthritis, as cultures are crucial to prompt and adequate treatment.
Elbow arthrocentesis indications
Elbow arthrocentesis is performed to aspirate effusions for two reasons, both diagnosis and therapeutic relief of pain caused by fluid pressure. Diagnostically the primary etiologies of concern are septic arthritis, hemarthrosis, and inflammation. Of these, a suspected septic joint and crystalline arthropathy are the two most common indications. Additionally, arthrocentesis may be used to evaluate therapeutic response for septic arthritis or unexplained arthritis with synovial effusion. Although not the topic of this discussion access to the joint space may also be used to inject therapeutic agents and to challenge the joint with fluid for evaluation of joint capsule integrity if overlying laceration is present 10.
Elbow arthrocentesis contraindications
The only absolute contraindication to arthrocentesis is overlying cellulitis which may lead to seeding of the joint with bacteria 11. Relative contraindications include coagulopathy, joint prosthesis, acute fracture, and adjacent osteomyelitis. Prosthetic joints warrant discussion with orthopedic surgery prior to tapping as many surgeons believe a prosthetic joint should only undergo tapping in the operative theater.
Elbow arthrocentesis procedure
Position your patient with the elbow bent 90 degrees and pronated palm down. This rolls the radial head to open the joint space. Use an ultrasound if available to localize fluid collection and direct the needle. Mark the approach by identifying the insertion site inferior to the lateral humeral epicondyle, anterior to the olecranon, and superior/posterior to the radial head (anconeus triangle). Use a skin pen to mark or pressure to indent the surface of the skin. Now clean the area with a wide margin using chlorhexidine or iodine solution. Gown, glove, and then drape in a sterile fashion. Raise a bleb of 1% lidocaine using a sterile technique at the site of insertion. Once anesthetized an 18-22 gauge needle 1.5 inches long is attached to a 5-10mL syringe and advanced into the joint space while retracting to watch for blood return. Once the joint space is accessed synovial fluid, blood, or infectious material may be aspirated. With the needle held in place, multiple syringes may be used to aspirate all the contents of the joint. If inflammatory etiology is suspected a glucocorticoid may be injected before leaving the joint space to prevent relapse of effusion 12. The needle is then withdrawn, a bandage is applied, and the collected fluid sent to the lab. Studies should include fluid gram stain and culture, cell count with differential, protein, glucose, and polarized light microscopy for crystalline arthropathies 13.
Other considerations
Arthrocentesis is safe within the therapeutic range of anticoagulation with warfarin or properly dosed anticoagulant medication. Considerations for the anticoagulated patient includes using smaller needle size 14.
Ultrasonography may be used in a sterile fashion to guide the needle if dry tap occurs and septic arthritis is suspected 15.
Shaving is of no benefit.
Elbow arthrocentesis complications
Complications with arthrocentesis are rare. There are two major categories to take into consideration, infectious complications and noninfectious complications. Of the complications, the most feared is septic arthritis 16. The frequency of this complication lies somewhere between 1 in 2000 and 1 in 15000. It is best avoided by maintaining a sterile field, minimizing attempts, using single-dose vials, changing to a new needle after drawing up medication before injecting, and avoiding introduction of a needle through cellulitis. The other concerning infection is septic bursitis which arises when the needle approach travels through a bursa, the olecranon bursa in the case of the elbow, on the way to the joint and is due to direct inoculation from skin flora. Non-infectious complications which arise include tendon rupture, vascular damage, and neurologic damage. All three complications directly result from trauma secondary to the penetrating needle and are more common when injecting glucocorticoids than aspirating. These complications are mediated by carefully planning the approach and identifying the proper anatomical location for insertion and needle travel. Bleeding management is with tamponade. The patient should also be informed there may be a recurrence of joint effusion until the resolution of the underlying cause 13.
Knee arthrocentesis
Crystal analysis is usually an important result of a successful knee aspiration. Most commonly, the clinician differentiates gout (negatively birefringent urate crystals), pseudogout (weakly positive birefringent crystals), and an infectious process 17.
Knee arthrocentesis procedure
The most important step is having the patient lay in a comfortable position with the affected knee fully extended or flexed at 15 to 20 degrees with a towel roll under the knee. This position helps to facilitate procedure success by ensuring quadriceps muscle relaxation. The clinician should then locate the patella. The clinician may mark it with a marking pen.
The knee is the largest synovial cavity in the body and can easily be accessed from either the medial or lateral aspect, and superior, inferior at the midpoint of the patella.
Sterilize area and drape in typical sterile fashion.
Choose the approach, then use a small syringe and small bore needle, draw up lidocaine and anesthetize superficial skin and then deeper tissue in the projected trajectory of joint aspiration to anesthetize the track.
- For midpoint approach, insert 18 g needle with 30 cc to 60 cc syringe one cm lateral or medial to the patella, directing the needle posterior and horizontal toward the intercondylar notch of the femur.
- Make sure to pull back on the syringe while inserting and stop once you aspirate synovial fluid.
- Attempt to aspirate as much fluid as possible.
- The superior approach is performed one cm superior and one cm medial or lateral to the patella, directing towards intercondylar notch of the femur.
- The infrapatellar approach requires the patient to be sitting upright, with the knee flexed at 90 degrees. Needle insertion is five mm below the inferior border of patella while also directing posterior to the patellar tendon, making this a less desirable approach.
“Milking” or compressing the joint can help facilitate aspiration of fluid.
Transfer fluid to specimen tubes. Remove the needle from joint and place bandage over the insertion site.
Knee arthrocentesis complications
Local trauma, including damage to nearby structures, pain, infection, and reaccumulation of effusion 18.
If the needle placement is poor or if the synovium is thickened, it may result in a dry tap.
Hemarthrosis can occur if a large needle damages a blood vessel when multiple attempts are made. In most cases, the hemarthrosis presents within a few hours after the procedure. It is often associated with pain, stiffness, and swelling of the joint. The majority of hemarthrosis are self-limited and resolve within a few weeks. If the patient has a coagulopathy, it may need to be corrected, and consultation with a hematologist may be helpful.
If arthrocentesis is performed through an infected area of skin to look for a septic joint, the patient must be given antibiotics promptly. If the fluid is frankly purulent, admission is recommended.
- Seidman AJ, Limaiem F. Synovial Fluid Analysis. [Updated 2019 Jan 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537114[↩]
- Shmerling RH, Delbanco TL, Tosteson AN, Trentham DE. Synovial fluid tests. What should be ordered? JAMA. 1990 Aug 22-29;264(8):1009-14.[↩]
- Chiodo CP, Logan C, Blauwet CA. Aspiration and Injection Techniques of the Lower Extremity. J Am Acad Orthop Surg. 2018 Aug 01;26(15):e313-e320.[↩]
- Zahar A, Lausmann C, Cavalheiro C, Dhamangaonkar AC, Bonanzinga T, Gehrke T, Citak M. How Reliable Is the Cell Count Analysis in the Diagnosis of Prosthetic Joint Infection? J Arthroplasty. 2018 Oct;33(10):3257-3262[↩]
- Shmerling RH, Delbanco TL, Tosteson AN, Trentham DE. Synovial fluid tests. What should be ordered? JAMA. 1990 Aug 22-29;264(8):1009-14[↩]
- Daniel JE, Fowles SM. Elbow Arthrocentesis. [Updated 2019 Jan 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537287[↩][↩]
- Baruffi S, Varacallo M. Shoulder Arthrocentesis Technique. [Updated 2019 Jan 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK519052[↩]
- Acute monoarthritis. N Engl J Med. 1993 Sep 30;329(14):1013-20. https://www.nejm.org/doi/full/10.1056/NEJM199309303291407[↩]
- Dilisio MF, Miller LR, Warner JJ, Higgins LD. Arthroscopic tissue culture for the evaluation of periprosthetic shoulder infection. J Bone Joint Surg Am. 2014 Dec 03;96(23):1952-8.[↩]
- Bettencourt RB, Linder MM. Arthrocentesis and therapeutic joint injection: an overview for the primary care physician. Prim. Care. 2010 Dec;37(4):691-702, v.[↩]
- Smyth TT, Chirino-Trejo M, Carmalt JL. In vitro assessment of bacterial translocation during needle insertion through inoculated culture media as a model of arthrocentesis through cellulitic tissue. Am. J. Vet. Res. 2015 Oct;76(10):877-81[↩]
- [↩]
- Bettencourt RB, Linder MM. Arthrocentesis and therapeutic joint injection: an overview for the primary care physician. Prim. Care. 2010 Dec;37(4):691-702, v[↩][↩]
- Thumboo J, O’Duffy JD. A prospective study of the safety of joint and soft tissue aspirations and injections in patients taking warfarin sodium. Arthritis Rheum. 1998 Apr;41(4):736-9.[↩]
- Sibbitt WL, Peisajovich A, Michael AA, Park KS, Sibbitt RR, Band PA, Bankhurst AD. Does sonographic needle guidance affect the clinical outcome of intraarticular injections? J. Rheumatol. 2009 Sep;36(9):1892-902[↩]
- Ross JJ. Septic Arthritis of Native Joints. Infect. Dis. Clin. North Am. 2017 Jun;31(2):203-218[↩]
- Guyver PM, Arthur CH, Hand CJ. The acutely swollen knee. Part 1: Management of atraumatic pathology. J R Nav Med Serv. 2014;100(1):24-33[↩]
- Battistone MJ, Barker AM, Grotzke MP, Beck JP, Berdan JT, Butler JM, Milne CK, Huhtala T, Cannon GW. Effectiveness of an Interprofessional and Multidisciplinary Musculoskeletal Training Program. J Grad Med Educ. 2016 Jul;8(3):398-404[↩]





{kind=link}