Buckle fracture
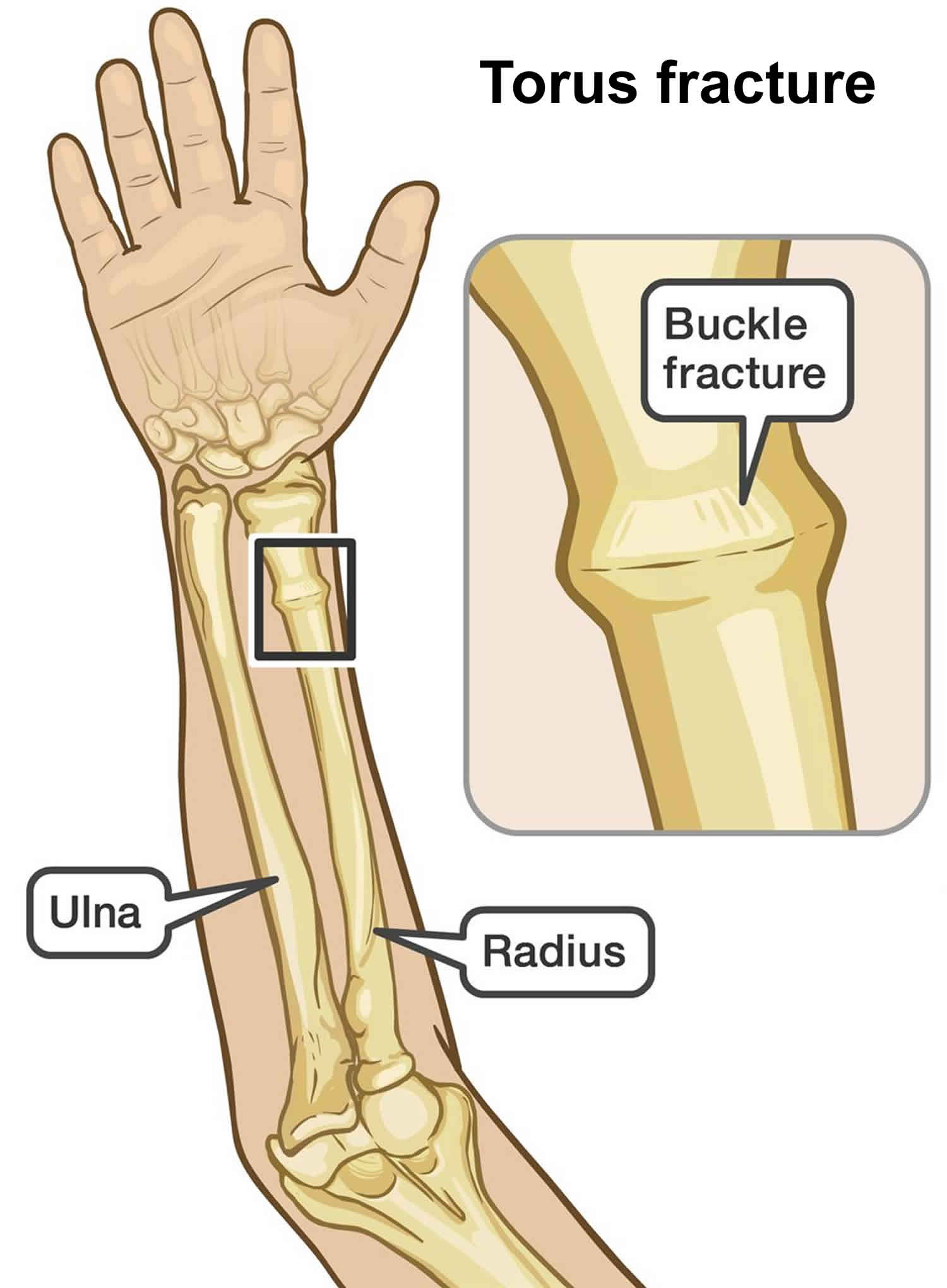
Buckle fracture also called torus fracture, is an incomplete fracture of the shaft of a long bone that occurs when a bone “buckles” or slightly crushes in on itself and is characterized by bulging of the cortex of the bone. The topmost layer of bone on one side of the bone is compressed, causing the other side to bend away from the growth plate. Torus or buckle fracture occurs in the transition zone between metaphyseal and diaphyseal bone 1. Torus (buckle) fractures of the distal forearm are common injuries in children and young adolescents, typically occurring after a fall on an outstretched arm 2.
The most common type of buckle fracture in children occurs in the forearm, near the wrist, usually after a child falls onto an outstretched arm. The injury affects the radius bone in particular. The bone will have a very small fracture, which is so minor that it may be difficult to see on X-ray (Figure 2). The wrist may be tender, slightly swollen, and painful to move. There is no deformity in the wrist, which means the wrist will not be out of its usual shape.
Buckle fracture or torus fracture is a stable fracture, meaning that the broken pieces of bone are still in position and have not separated apart (displaced). Buckle fractures or torus fractures are stable due to the thick periosteum present in this patient population and unlike other pediatric wrist and forearm fractures, the risk of future displacement is minimal 3.
Buckle fractures are treated by wearing a removable backslab (a partial cast held in place with bandages) or ready-made splint, which should be worn as much as possible but can be removed for bathing or showering. An arm sling is optional, and may help reduce any pain or discomfort.
Buckle fractures are more common in children, especially aged 5-10 years, due to the elasticity of their bones. In adults, the commonest form of buckle fracture seen is a buckle fracture of the ribs.
Buckle fracture key points to remember:
- A buckle fracture in the wrist is a small area of compressed bone.
- Your child should wear a removable backslab (partial cast) or splint for three weeks. A sling may help reduce discomfort.
- Most children will not need a follow-up appointment or X-ray, because buckle fractures usually heal quickly without any problems.
- Avoid contact sports for six weeks after the injury.
Figure 1. Buckle fracture
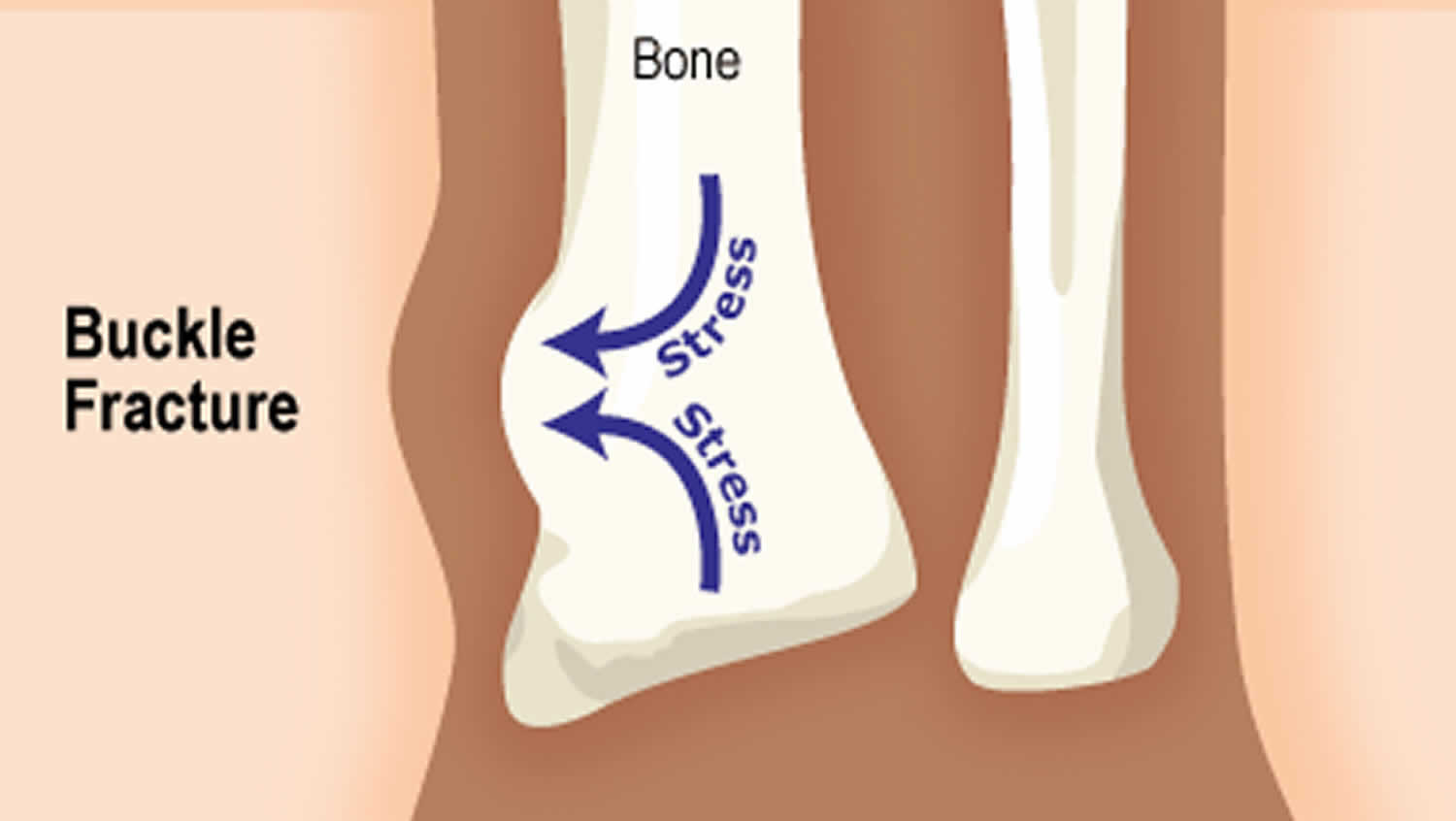
Figure 2. Buckle fracture of the distal radius

Footnote: A buckle fracture of the distal radius in a six-year-old child. Arrows point to buckling of the cortex.
[Source 4 ]Figure 3. Buckle fracture splint

Buckle fracture causes
Children love to run, hop, skip, jump and tumble, all of which are activities that could potentially result in a buckle fracture to the forearm should an unexpected fall occur. In most cases, forearm fractures in children are caused by:
- A fall onto an outstretched arm
- A fall directly on the forearm
- A direct blow to the forearm
Torus fractures or buckle fractures, are incomplete fractures of the shaft of a long bone that is characterized by bulging of the cortex. They result from trabecular compression due to an axial loading force along the long axis of the bone. They are usually seen in children, frequently involving the distal radial metaphysis.
Strictly speaking, a torus fracture refers to a circumferential buckle fracture 5. However, the terms are often used interchangeably.
Cortical buckle fractures occur when there is axial loading of a long bone. This most commonly occurs at the distal radius or tibia following a fall on an outstretched arm; the force is transmitted from carpus to the distal radius and the point of least resistance fractures, usually the dorsal cortex of the distal radius.
Buckle fracture symptoms
A forearm buckle fracture usually results in severe pain. Your child’s forearm and hand may also feel numb, a sign of potential nerve injury.
Symptoms of a broken arm may include:
- Immediate, severe pain
- Swelling and tenderness
- Numbness in the forearm, hand or elbow
- Deformity of the forearm, elbow or wrist
- Difficulty turning or rotating the forearm
Additionally, your child may feel the need to support the injured arm with their other hand.
Buckle fracture diagnosis
Diagnosing a forearm torus fracture typically begins with a physical examination of your child’s arm, wrist and elbow. The physician will look for any deformity of the arm, as well as swelling, tenderness, and an inability to rotate the affected arm.
In most cases, clinicians will recommend X-rays of your child’s forearm to confirm the diagnosis and determine the extent of your child’s injury. X-rays produce images of bones and help doctors identify the type of fracture so they can recommend the best treatment for your child.
In addition to a physical exam and X-rays, your child may also undergo:
- Range of motions tests to determine how the injury is affecting your child’s movement and dexterity
- Nerve assessment tests to determine if the injury has damaged or compressed any nerves in your child’s arm or hand
The more information we have about your child’s condition, the better we can treat their unique injury.
Buckle fracture treatment
Buckle fractures or torus fractures are usually treated with a pre-made wrist splint or a removable Plaster of Paris backslab (a partial cast held in place with bandages), which should be worn as much as possible but can be removed for bathing or showering. Both these methods, combined with simple painkillers such as acetaminophen (paracetamol) and ibuprofen, will help control your child’s pain. An arm sling is optional, and may help reduce any pain or discomfort.
Historically torus fractures or buckle fractures were managed with cast immobilization, and serial radiographic follow-up in an orthopedic outpatient setting 6.
The traditional management of pediatric torus fractures or buckle fractures of the distal forearm has mirrored that of other fractures in this region, including cast immobilization and serial radiographic and clinical follow-up to assess for displacement until fracture union 6. However, emerging literature over the last two decades has supported a ‘minimalist’ approach to managing these injuries. Van Bosse et al 7 described treatment with removable splint application at time of injury, appropriate patient and caregiver counseling, a short (three to four week) period of immobilization and either self-discontinuation of the splint at home or a single follow-up appointment with clinical examination only. Radiographs become necessary only in the setting of re-injury or continued pain after the treatment period. Numerous other studies have highlighted safe and efficacious management of these injuries in a similarly ‘minimalist’ fashion 8. The recent National Institute for Health and Care Excellence guidelines 9 advocate management of torus fractures with nonrigid casts or splints. The patient can remove both of these without the need for further radiographs or follow-up 9.
In addition to pre-fabricated and removable splints, multiple other non-casting alternatives have been found to be equally safe in the management of paediatric torus fractures of the distal forearm. Soft bandage 10 and soft cast 11, neither of which require a physician visit for removal, have both been demonstrated to be acceptable treatment options. In the appropriately selected patient, home-based removal of immobilization can further simplify management and has been demonstrated to have equivalent outcomes to clinic-based reexamination and removal 12. By eliminating the additional orthopedic clinic visits for cast removal and radiographic exams, these management approaches theoretically minimize the burden to the caregiver and patient while simultaneously reducing treatment cost 3.
Care at home
Buckle injuries may be painful. Although immobilizing the arm with the backslab or splint will help to reduce the pain, additional pain relief (e.g. paracetamol) is sometimes needed. Give the pain relief medication as required, following the directions on the packet or as directed by the doctor.
Never cut or attempt to modify the cast, and make sure you avoid getting it wet.
Buckle fracture healing time
A stable fracture, such as a buckle fracture, may require 3 to 4 weeks in a cast.
Follow-up
Because buckle injuries are stable and heal quickly without problems, most children will not need a follow-up appointment with the doctor or hospital. Further X-rays or physiotherapy are usually not required.
Three weeks after their injury, your child can just stop wearing their backslab or splint.
After the backslab or splint is removed
Wrist movement may be a little stiff and sore at first. Contact sports (or rough and tumble play) should be avoided for six weeks after the injury.
Take your child to your doctor if:
- your child’s wrist remains very painful or swollen three weeks after the injury
- your child will not use their wrist, hand or fingers within two to three days of the back slab or splint being removed.
- Witney-Iagen C, Smith C, Walsh G. Softcast versus rigid cast for treatment of distal radius buckle fractures in children. Injury. 2018;44:508–513.[↩]
- Noonan KJ, Price CT. Forearm and distal radius fractures in children. J Am Acad Orthop Surg 1998;6:146-156.[↩]
- Firmin F, Crouch R. Splinting versus casting of “torus” fractures to the distal radius in the paediatric patient presenting at the emergency department (ED): a literature review. Int Emerg Nurs 2009;17:173-178.[↩][↩]
- Buckle fractures of the distal radius in children. Maxim Ben-Yakov, Kathy Boutis. CMAJ Apr 2016, 188 (7) 527; DOI: 10.1503/cmaj.151239 https://doi.org/10.1503/cmaj.151239[↩]
- B. J. Manaster, David A. May, David G. Disler. Musculoskeletal Imaging,The Requisites (Expert Consult – Online and Print), 4th ed (2013). ISBN: 9780323081771[↩]
- Williams BA, Alvarado CA, Montoya-Williams DC, Matthias RC, Blakemore LC. Buckling down on torus fractures: has evolving evidence affected practice?. J Child Orthop. 2018;12(2):123–128. doi:10.1302/1863-2548.12.170122 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5902745[↩][↩]
- van Bosse HJP, Patel RJ, Thacker M, Sala DA. Minimalistic approach to treating wrist torus fractures. J Pediatr Orthop 2005;25:495-500.[↩]
- Neal E. Comparison of splinting and casting in the management of torus fracture. Emerg Nurse 2014;21:22-26.[↩]
- Fractures (non-complex): assessment and management. NICE guideline [NG38]. 17 February 2016 https://www.nice.org.uk/guidance/ng38[↩][↩]
- West S, Andrews J, Bebbington A, Ennis O, Alderman P. Buckle fractures of the distal radius are safely treated in a soft bandage: a randomized prospective trial of bandage versus plaster cast. J Pediatr Orthop 2005;25:322-325.[↩]
- Witney-Lagen C, Smith C, Walsh G. Soft cast versus rigid cast for treatment of distal radius buckle fractures in children. Injury 2013;44:508-513.[↩]
- Symons S, Rowsell M, Bhowal B, Dias JJ. Hospital versus home management of children with buckle fractures of the distal radius. A prospective, randomised trial. J Bone Joint Surg [Br] 2001;83-B:556-560.[↩]





{kind=link}