Caviar tongue
Caviar tongue also known as lingual varicosities or sublingual varices, is considered as a benign physiological change associated with advancing age, usually developing due to senile elastolytic degeneration of sublingual veins 1. Caviar lesion occurs at three sites: under surface of tongue along the sublingual vein, floor of the mouth near ostia of the sublingual glands and along the lateral portions of the under surface of the tongue 2. Caviar tongue is mostly seen at the undersurface of the tongue along the sublingual glands where the mucosal surface is thin and translucent which permits visualization of submucosal vascular structures (Figure 1) 3. Uncommon sites are lips and buccal mucosae. Caviar tongue begins as a small outpouching of the veins, and the varicosities gradually elevate the overlying thin mucosa with color varying from red to purple, resembling buckshot or caviar with iridescent surface. Histologically, caviar lesion is a dilated vein with no inflammatory changes. The endothelium is hypoplastic but the wall is thick and cellular 4.
Sublingual varices are benign vascular dilatations, usually asymptomatic and affecting 10% of the population over the age of 40 years 5. These are frequently observed by dentists and bleeding from these varices is uncommon 6. In cases of bleeding, a detailed investigation should be undertaken for underlying associations. Caviar tongue can be found in association with conditions that result in increased venous pressure such as portal hypertension or superior vena cava syndrome 7. Phleboliths or thrombophlebitis may complicate this condition. An association with angiokeratoma of scrotum has also been reported 8.
In a study by William Bean 2, caviar tongue was seen after fourth decade with increased frequency in sixth to seventh decade which is the same profile as that seen in cherry angiomas and venous stars. No evidence of any association with systemic diseases like pulmonary or vascular disease was found 2. A recent study for prevalence of oral hemangioma, vascular malformation and varix in a Brazilian population revealed 65.6% prevalence of asymptomatic multiple sublingual varices with preponderance in females and Caucasians 9.
Sublingual varices may be occasionally confused due to resemblance to tumors like hemangioma, lymphangioma, Kaposi’s sarcoma, melanoma or other conditions like Osler’s syndrome, blue rubber bleb nevus syndrome 7. However, most of these conditions can be differentiated by a detailed history and thorough clinical evaluation. Caviar tongue on histology is just a dilated vein with no inflammatory changes. Vascular tumors like hemangioma and lymphangioma show endothelial cell proliferation and dilated lymphatics respectively, while Kaposi’s sarcoma shows tumor cells composed of vascular spaces and spindle cells on histology. Sublingual varices usually need no treatment but only reassurance regarding its benign nature. Sclerotherapy or surgery has been attempted in single lesions and unusual locations like lips or buccal mucosae 9.
On dermoscopy, dark-blue lacunae (Figure 2) suggest vessel thrombosis and red lacunae suggest absence of it 10. Caviar tongue dermoscopy showed absence of pigmentation, presence of multiple loosely scattered red lacunae with bluish white (rather than white) veil present over a yellowish crimson background, surrounded and interspersed with fine arborizing vessels and scattered telangiectasias and focal white structureless areas 11. Dermoscopically, hemangiomas also show red-bluish lacunae but lack the sharp dermarcation seen in angiokeratoma of Fordyce 12. Pyogenic granuloma reveals whitish veils, but lack the red-blue lacunae 13. Cutaneous lymphangioma circumscriptum displays two distinct patterns: yellow lacunae surrounded by pale septa without inclusion of blood and yellow to pink lacunae alternating with dark-red or bluish lacunae, due to the inclusion of blood. A few lacunae contained blood, which was characteristically accumulated in the lowest part of the lacuna, resulting in an appearance similar to the so-called “hypopyon” of the eye, a new “dermatologic” metaphoric term has been used to describe this peculiar feature as half-and-half lacuna 14.
Figure 1. Caviar tongue


Footnote: Dilated tortuous purplish to black vessels seen along the lateral portions of undersurface of the tongue.
[Source 1 ]Figure 2. Caviar tongue dermoscopy
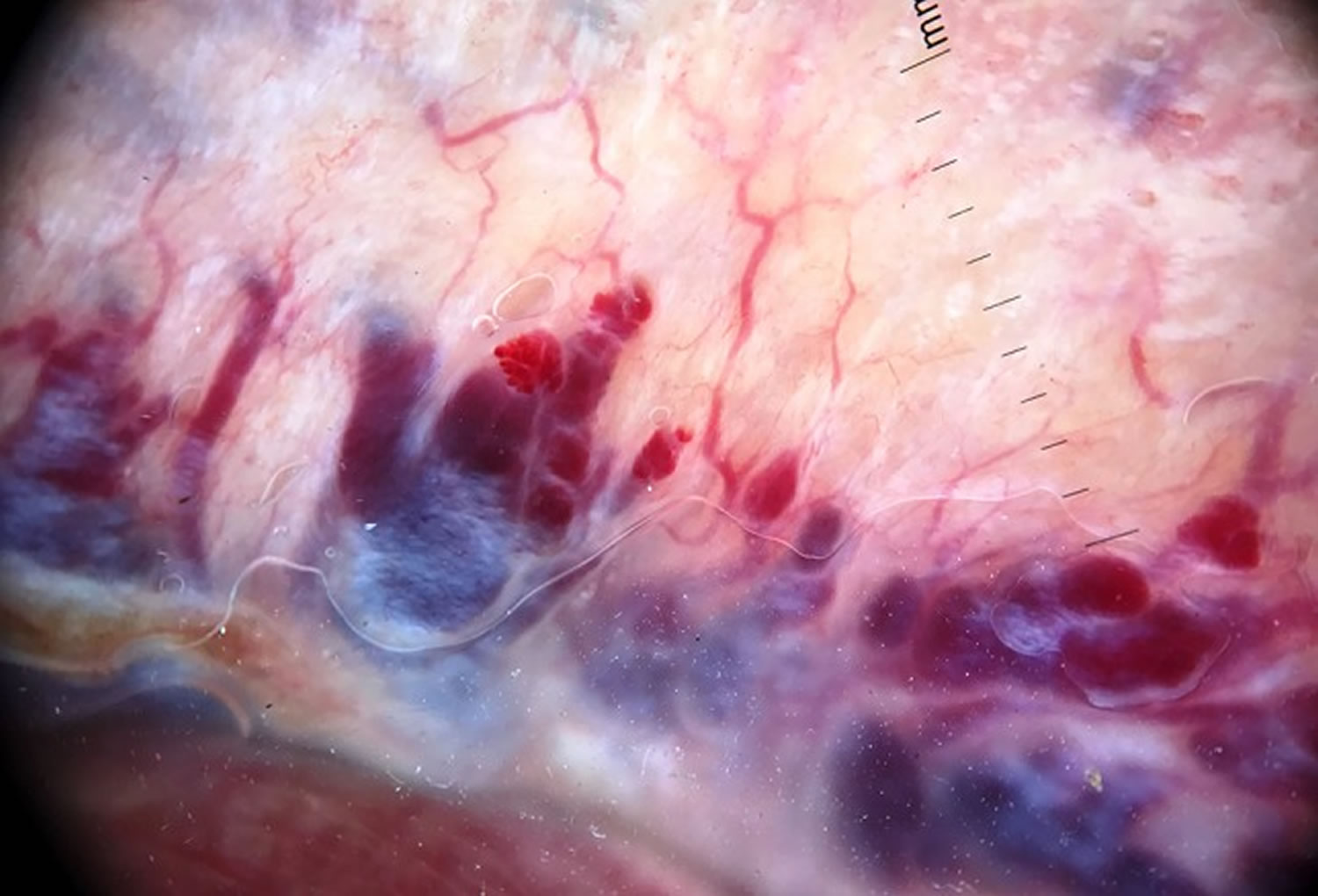
Footnote: Caviar tongue dermoscopy [polarized, 10X] showed absence of pigmentation, presence of multiple loosely scattered red lacunae with bluish white (rather than white) veil present over a yellowish crimson background, surrounded and interspersed with fine arborizing vessels and scattered telangiectasias and focal white structureless areas 11.
[Source 1 ]Caviar tongue causes
Caviar tongue also known as lingual varicosities or sublingual varices, is considered as a physiological change associated with advancing age, usually developing due to senile elastolytic degeneration of sublingual veins 1. Caviar tongue is mostly seen at the undersurface of the tongue along the sublingual glands where the mucosal surface is thin and translucent which permits visualization of submucosal vascular structures 3.
Caviar tongue symptoms
Caviar tongue is asymptomatic tortuous purplish to black swellings on the undersurface of the tongue. On mucosal examination, dilated tortuous vessels can be seen along the lateral portions of undersurface of the tongue. There is no history of bleeding from the site and there is no evidence of any associated systemic disease. Examination of the skin, hair and other mucosal surfaces were normal.
Caviar tongue diagnosis
While the diagnosis of caviar tongue is nearly always clinical, differentials including hemangioma, lymphangioma, Kaposi sarcoma, and mucosal melanoma are worth consideration 11.
Caviar tongue treatment
Caviar tongue is considered as a physiological change associated with advancing age and is benign; therefore, no treatment is needed. Sclerotherapy, surgery, or photocoagulation with high intensity diode laser or Nd:YAG (neodymium-doped yttrium aluminium garnet) laser has been tried in few lesions on unusual locations, such as the lips or buccal mucosa 1.
- Jha AK, Zeeshan MD, Jha Amar AK. Mucoscopy in lingual varicosities. Dermatol Pract Concept. 2018;8(1):54-55. Published 2018 Jan 31. doi:10.5826/dpc.0801a12 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5808374[↩][↩][↩][↩][↩]
- BEAN WB. The caviar lesion under the tongue. Trans Am Clin Climatol Assoc. 1952;64:40-51. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2248813/pdf/tacca00127-0114.pdf[↩][↩][↩]
- Lazos JP, Piemonte ED, Panico RL. Oral varix: a review. Gerodontology. 2015 Jun;32(2):82-9. doi: 10.1111/ger.12074. Epub 2013 Sep 1. https://doi.org/10.1111/ger.12074[↩][↩]
- Viswanath V, Nair S, Chavan N, Torsekar R. Caviar tongue. Indian J Dermatol Venereol Leprol 2011;77:78-9. https://www.ijdvl.com/text.asp?2011/77/1/78/75002[↩]
- Rogers RS, Bruce AJ. Tongue in clinical diagnosis. J Eur Acad Dermatol Venereol 2004;18:254-9.[↩]
- Pemberton MN. Sublingual varices are not unusual. BMJ 2006;333:202. doi: 10.1136/bmj.333.7560.202[↩]
- Roy S, Rogers II, Mehregan DA. Disorders of oral cavity. In: Moschella SL, Hurley HJ, editors. Moschella’s Dermatology. 3 rd ed. Philadelphia: WB Saunders Co; 1992. p. 2094.[↩][↩]
- James WD, Berger TG, Elston DM. Disorders of mucous membranes. In: James WD, Berger TG, Elston DM, editors. Andrews’ Diseases of the Skin; Clinical Dermatology. 10 th ed. Philadelphia: W.B. Saunders Co; 2006. p. 803.[↩]
- Corrκa PH, Nunes LC, Johann AC, Aguiar MC, Gomez RS, Mesquita RA. Prevalence of oral hemangioma, vascular malformation and varix in a Brazilian population. Braz Oral Res 2007;21:40-5.[↩][↩]
- Kocsard E, Ofner F, D’Abrera VS. The histopathology of caviar tongue. Ageing changes of the undersurface of the tongue. Dermatologica. 1970;140(5):318-22. doi: 10.1159/000252570[↩]
- Sonthalia S. Interpreting Mucoscopy in Lingual Varicosities and Beyond. Dermatol Pract Concept. 2019;9(2):146-147. Published 2019 Apr 30. doi:10.5826/dpc.0902a11 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6502301[↩][↩][↩]
- Campos-do-Carmo G, Ramos-e-Silva M. Dermoscopy: basic concepts. Int J Dermatol. 2008;47:712–719.[↩]
- Zaballos P, Llambrich A, Cuéllar F, Puig S, Malvehy J. Dermoscopic findings in pyogenic granuloma. Br J Dermatol. 2006;154:1108–1111.[↩]
- Jha AK, Lallas A, Sonthalia S. Dermoscopy of cutaneous lymphangioma circumscriptum. Dermatol Pract Concept. 2017;7(2):37-38. Published 2017 Apr 30. doi:10.5826/dpc.0702a08 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5424661[↩]





{kind=link}