
What is cervical disc disease
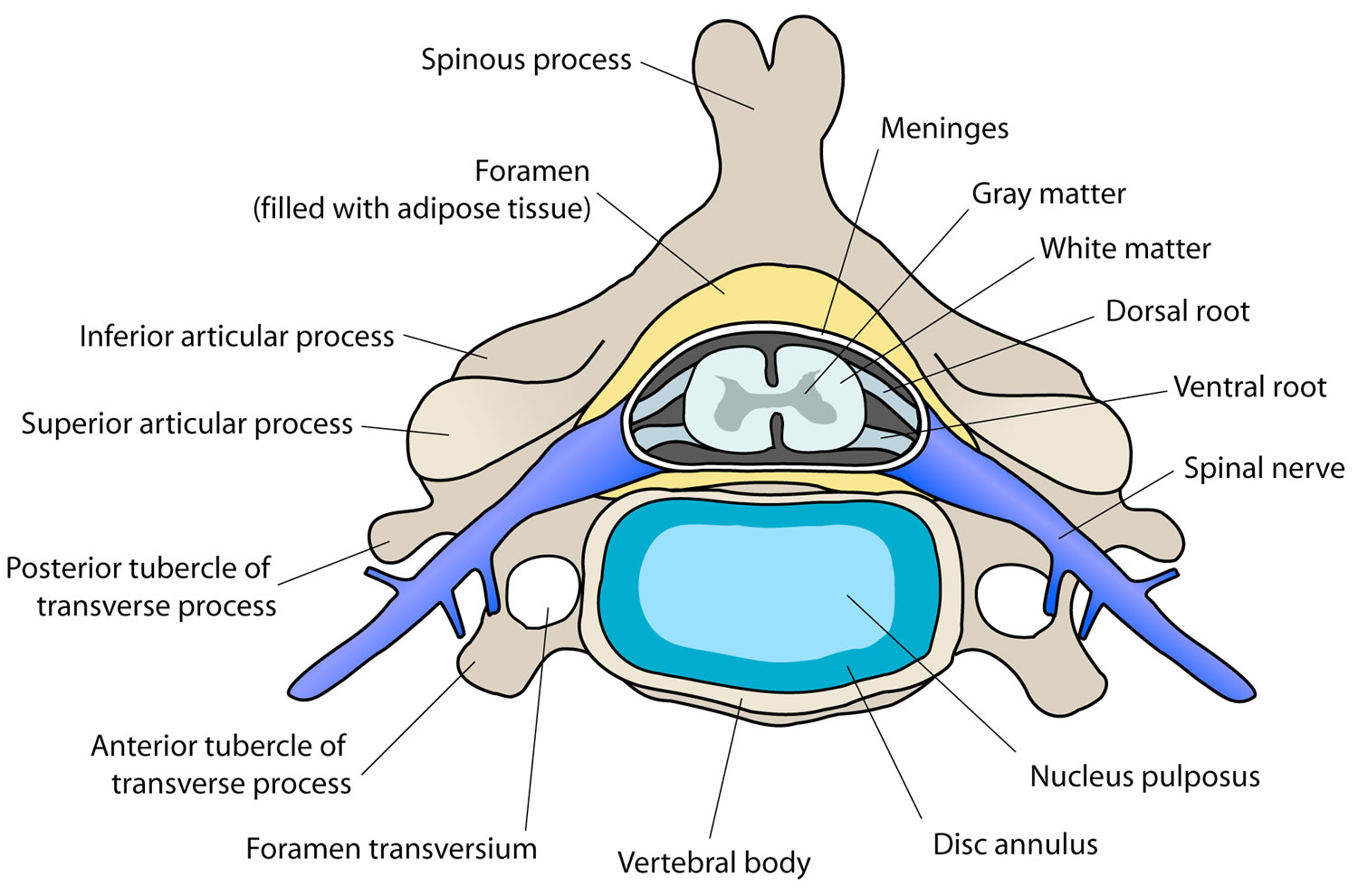
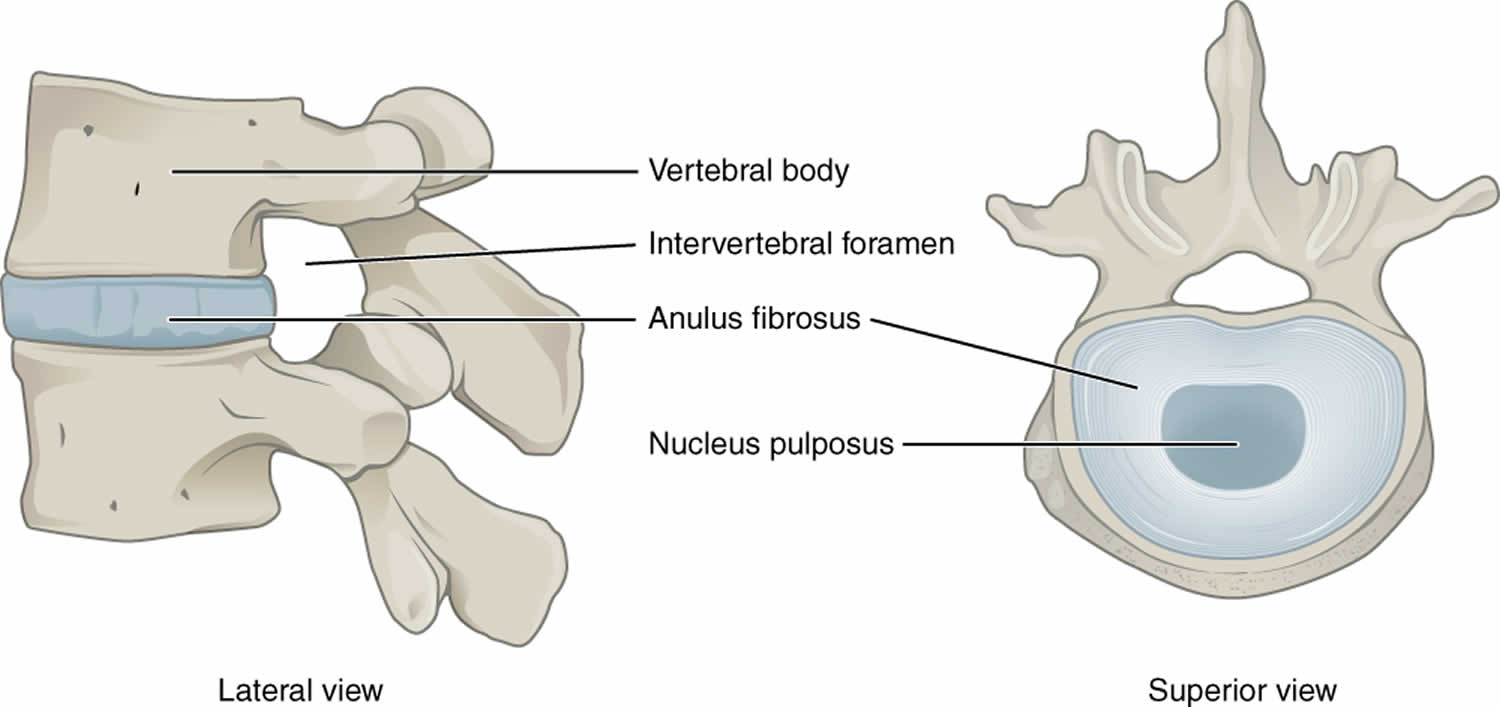
Cervical disc disease is a group of cervical disc disorders that include cervical herniated nucleus pulposus, cervical degenerative disc disease, and cervical internal disc disruption. Herniated nucleus pulposus is defined as localized displacement of nucleus, cartilage, fragmented apophyseal bone, or fragmented anular tissue beyond the intervertebral disc space 1. Most of the cervical disc herniation is made up of the annulus fibrosus. Cervical degenerative disc disease involves degenerative annular tears, loss of disc height, and nuclear degradation. Cervical internal disc disruption describes annular fissuring of the cervical disc without external disc deformation. Cervical radiculopathy or a pinched nerve can result in neck pain spreads all the way into your shoulders or arms due to a nerve root injury in the presence of disc herniation or stenosis, most commonly foraminal stenosis, leading to sensory, motor, or reflex abnormalities in the affected nerve root distribution 2.
Figure 1. Cervical disc
Cervical disc disease causes
Cervical disc disease causes include:
- Cervical herniated nucleus pulposus results from repetitive cervical stress or, rarely, from a single traumatic incident. Increased risk may accrue because of vibrational stress, heavy lifting, prolonged sedentary position, whiplash accidents, and frequent acceleration/deceleration.
- Cervical degenerative disc disease is part of natural aging, but it is also a consequence of poor nutrition, smoking, atherosclerosis, job-related activities, and genetics.
- Cervical internal disc disruption can result from cervical trauma, including whiplash, cervical flexion/rotation injury, and repetitive use.
Cervical radiculopathy results from nerve root compression secondary to herniated disc material, stenosis, or proteoglycan-mediated chemical inflammation released from discs. Smoking and certain occupational activities also predispose patients to cervical radiculopathy.
Cervical disc disease symptoms
Cervical disc disease pain without nerve root involvement is typically vague, diffuse and distributed centrally.
Pain referred from disc to upper limb usually is nondermatomal, and does not follow any predictable course
In a study using provocative discography for symptom mapping, Slipman et al 3 showed that unilateral symptoms were found just as often as bilateral symptoms. Slight variation was noted for referred somatic pain originating from each disc level to the neck, shoulder, and upper thoracic region but with a great amount of overlap.
Activities that increase intradiscal pressure (eg, lifting, Valsalva maneuver) intensify symptoms. Conversely, lying supine provides relief by decreasing intradiscal pressure.
Vibrational stress from driving can also exacerbate discogenic pain. Yates et al showed that vibration and shock loading provided sufficient mechanical injury to exacerbate preexisting herniations, whereas a flexed posture did not influence the distance of nucleus pulposus tracking 4.
Depending on whether primarily motor or sensory involvement is present, radicular (pinched nerve) pain is deep, dull, and achy or sharp, burning, and electric. Such radicular pain follows a dermatomal or myotomal pattern into the upper limb. Cervical radicular pain most commonly radiates to the interscapular region, although pain can be referred to the occiput, shoulder, or arm as well. Neck pain does not necessarily accompany radiculopathy and frequently is absent.
Patients may present with distal limb numbness and proximal weakness in addition to pain. Atrophy may be present.
A study has demonstrated cervical herniated nucleus pulposus-induced thermal changes (ie, thermatomes) in specific upper extremity distributions.
Mechanical stimulation of cervical nerve roots has shown that the distribution of referred radicular symptoms (ie, dynatome) may be different from sensory deficits outlined by traditional dermatomal maps.
Cervical disc disease diagnosis
Plain cervical spine radiographs are used to evaluate chronic cervical spine and disc degenerative changes, metastatic disease, infection, spinal deformity, and stability.
Computed tomography (CT) scans delineate cervical spine fracture and are used extensively in trauma cases.
A myelogram followed by a CT scan may be obtained prior to cervical decompressive spinal cord or nerve root surgery. This study evaluates the spinal canal, its relationship to the spinal cord, and nerve root impingement from disc, spur, or foraminal encroachment.
Magnetic resonance imaging (MRI) remains the imaging modality of choice to evaluate cervical herniated nucleus pulposus, due to its low morbidity 5. Advantages include soft-tissue definition (eg, cervical discs, spinal cord), cerebrospinal fluid visualization, noninvasiveness, and lack of patient radiation exposure.
Provocative discography is the only procedure that can determine whether a disc serves as the pain generator. Discomfort and invasiveness render this procedure less desirable than cervical MRI, which provides much of the anatomical information that provocative discography does.
Electrodiagnostic studies continue to be standard for evaluating neurologic function of the cervical spine. Advantages of these tests include limited expense and low morbidity.
Other tests may include rheumatologic workup to evaluate for possible rheumatoid arthritis, ankylosing spondylitis, Reiter syndrome, and polymyalgia rheumatica. In addition, infection workup to evaluate for possible discitis, epidural abscess, and vertebral osteomyelitis.
Cervical disc disease treatment
For most cervical disc disorders, studies support conservative treatment, such as the physical therapy and cervicothoracic stabilization programs, combined with aerobic conditioning. Painkillers like acetaminophen and ibuprofen can help ease neck pain and stiffness. You can also use ibuprofen gel on your neck. Putting heat or cold packs on your neck can also help. When sleeping use a low, firm pillow, making sure your head is the same height as the rest of your body. You try neck exercises (see below).
Physical therapy is usually the first nonsurgical treatment that your doctor will recommend. Specific exercises can help relieve pain, as well as strengthen and stretch weakened or strained muscles. In some cases, physical therapy may include posture therapy or the use of traction to gently stretch the joints and muscles of your neck. Physical therapy programs vary in length, but generally last from 6 to 8 weeks. Typically, sessions are scheduled 2 to 3 times per week.
Cervical traction may relieve radicular pain from nerve root compression. Traction does not improve soft-tissue injury pain. Hot packs, massage, and/or electrical stimulation should be applied prior to traction to relieve pain and relax muscles.
A soft cervical collar is recommended only for acute soft-tissue neck injuries and for short periods of time (ie, not to exceed 3-4 days’ continuous use).
Spinal manipulation and mobilization may restore normal range of motion (ROM) and decrease pain; however, no clear therapeutic mechanism of action is known.
Your doctor might also prescribe a muscle relaxant or other medicine if the pain has been coming and going for a long time (chronic pain).
It usually takes a few weeks for treatment to work, although the pain and stiffness can come back.
Cervical epidural, spinal nerve (or root), Z-joint, and sympathetic injections serve diagnostic and therapeutic roles. These procedures can be instrumental in determining the anatomic pain generator (eg, nerve root, facet) and providing aggressive, conservative treatment.
An anesthetic and corticosteroid mixture may be injected into the epidural space (interlaminar) or along the nerve root (transforaminal) after precise radiologic, contrast-enhanced fluoroscopic localization 6.
Studies indicate that cervical herniated nucleus pulposus with radiculopathy can be managed conservatively. Surgery is warranted when neurogenic bowel or bladder dysfunction, deteriorating neurologic function, or intractable radicular or discogenic neck pain exists. Specifically, cervical spine surgical outcomes are most favorable for radicular pain, spinal instability, progressive myelopathy, or upper extremity weakness.
Surgical outcomes for patients with myelopathy have been shown to be significantly greater with regard to motor recovery if surgical intervention is performed less than 1 year after the onset of symptoms 7.
The literature has demonstrated favorable cervical spine fusion outcomes for chronic discogenic axial neck pain when the presurgical evaluation has incorporated provocative cervical discography. However, fusion can increase intradiscal pressure and other stress at adjacent unfused levels, thereby accelerating postsurgical spinal degeneration 8.
The possibility of obtaining the goals of anterior cervical decompression and fusion while maintaining adjacent segment motion led to the advent of total disk replacement.
Cervical degenerative disc disease
Cervical degenerative disc disease also called arthritis of the neck or cervical spondylosis, arises from degenerative changes in the cervical spine (vertebrae) and intervertebral discs that occur as a result of ageing or due to injury or rheumatoid disease. These changes are normal and they occur in everyone. In fact, nearly half of all people middle-aged and older have worn cervical discs that do not cause painful symptoms.
Cervical degenerative disc disease is a common cause of chronic neck pain. Ageing causes wear and tear to muscles and bones. In advanced cervical degenerative disc disease may lead to cervical spondylosis with radiculopathy which results from compression of the spinal cord. Cervical degenerative disc disease with radiculopathy (pinched nerve) is probably the most common spinal cord disorder in people over 55 years of age in the world. More than 85 percent of people older than age 60 are affected by cervical spondylosis. As the number of elderly people increases, the incidence of cervical degenerative disc disease with radiculopathy will probably also increase.
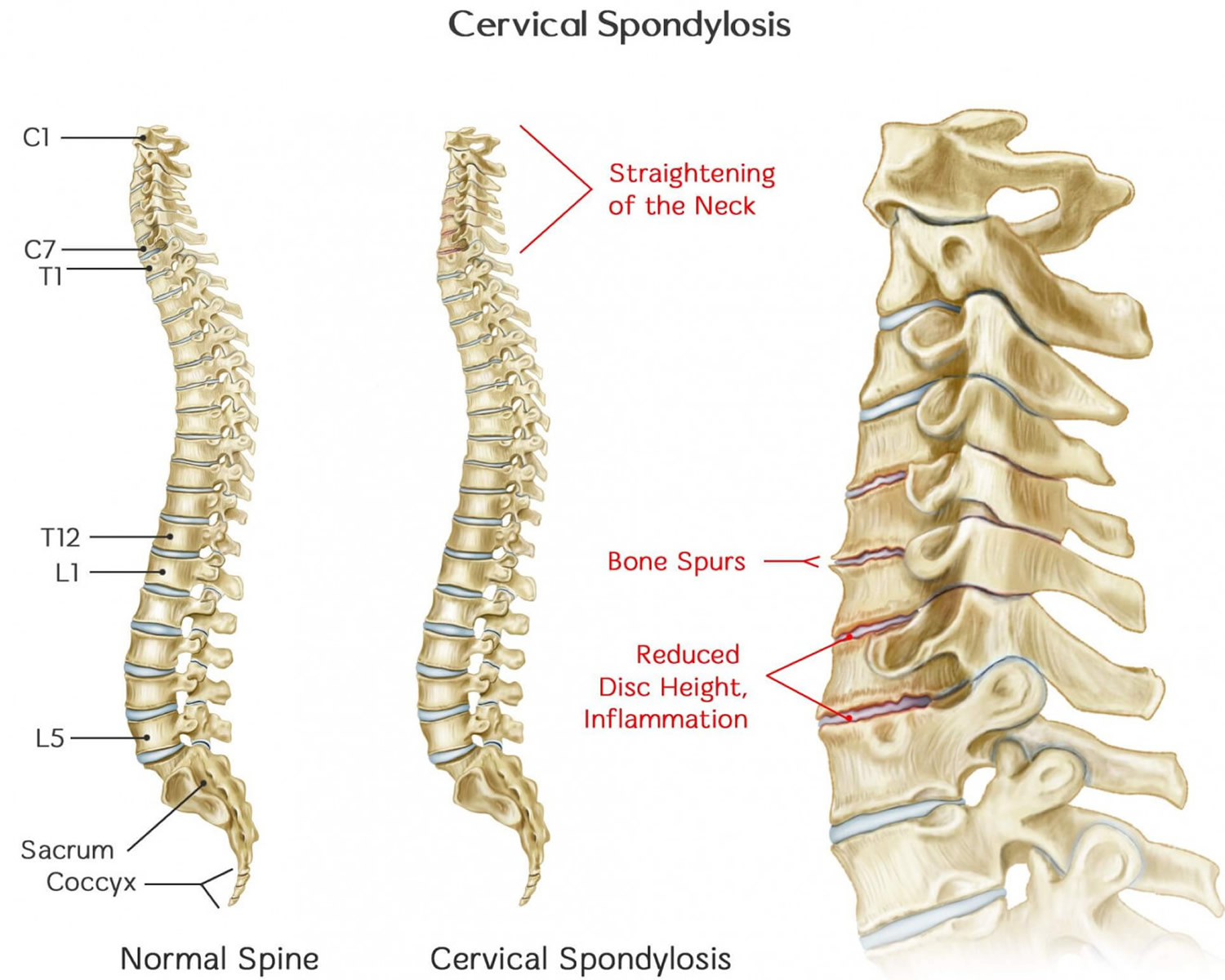
Cervical degenerative disc disease is a disorder that results from abnormal growth of the bones of the neck and degeneration and mineral deposits in the intervertebral discs between the vertebrae. As the discs dehydrate and shrink, signs of osteoarthritis develop, including bony projections along the edges of bones (bone spurs). Progressive neck pain is a key indication of cervical degenerative disc disease. It may be the only symptom in many cases. Examination often shows limited ability to bend the head toward the shoulders and limited ability to rotate the head. The goal of treatment is relief of pain and prevention of permanent spinal cord and nerve root injury.
As the discs in the spine age, they lose height and begin to bulge. They also lose water content, begin to dry out and weaken. This problem causes settling, or collapse, of the disc spaces and loss of disk space height.
As the facet joints experience increased pressure, they also begin to degenerate and develop arthritis, similar to what may occur in the hip or knee joint. The smooth, slippery articular cartilage that covers and protects the joints wears away.
If the cartilage wears away completely, it can result in bone rubbing on bone. To make up for the lost cartilage, your body may respond by growing new bone in your facet joints to help support the vertebrae. Over time, this bone overgrowth — called bone spurs — may narrow the space for the nerves and spinal cord to pass through (stenosis).
Figure 2. Cervical degenerative disc disease
A number of factors are responsible for the development of the signs and symptoms of cervical degenerative disc disease:
- Osteophytes (bony growths)
- A narrowed spinal canal present since birth
- Degeneration of the intervertebral discs
- Changes in the spinal cord and nerves due to insufficient blood supply.
See your healthcare provider if:
- The pain that’s getting much worse
- There are signs of complications like lack of co-ordination – for example trouble with tasks like buttoning a shirt
- You develop new symptoms (such as loss of movement or feeling in an area of the body) – problems walking
- Heaviness or weakness in your arms or legs
- Pins and needles in an arm as well as pain
- Dizziness
- You lose control of your bladder or bowels (see right away)
These can be signs of a more severe condition (cervical spondylosis with myelopathy) which can cause permanent damage to the spine if left untreated.
Cervical degenerative disc disease causes
Cervical degenerative disc disease is caused by aging and chronic wear on the cervical spine – many people aged over 50 have cervical degenerative disc disease. This includes the discs or cushions between the neck vertebrae and the joints between the bones of the cervical spine. There may be abnormal growths or spurs on the bones of the spine (vertebrae).
These changes can include:
- Dehydrated discs. Discs act like cushions between the vertebrae of your spine. By the age of 40, most people’s spinal disks begin drying out and shrinking, which allows more bone-on-bone contact between the vertebrae.
- Herniated discs. Age also affects the exterior of your spinal discs. Cracks often appear, leading to bulging (herniated) discs — which sometimes can press on the spinal cord and nerve roots.
- Bone spurs. Disk degeneration often results in the spine producing extra amounts of bone in a misguided effort to strengthen the spine. These bone spurs can sometimes pinch the spinal cord and nerve roots.
- Stiff ligaments. Ligaments are cords of tissue that connect bone to bone. Spinal ligaments can stiffen with age, making your neck less flexible.
Over time, these changes can press down on (compress) one or more of the nerve roots. In advanced cases, the spinal cord becomes involved – cervical degenerative disc disease with radiculopathy. This can affect not just the arms, but the legs as well.
Everyday wear and tear may start these changes. People who are very active at work or in sports may be more likely to have them.
You can get cervical degenerative disc disease at any age if you have:
- a job that involves repetitive neck movements or a lot of overhead work – like painting and decorating
- previously had a neck injury
- a family history of the condition
Some people have it without knowing, and without it being a problem.
The major risk factor is aging. By age 60, most people show signs of cervical degenerative disc disease on x-ray. Other factors that can make someone more likely to develop cervical disc disease are:
- Being overweight and not exercising
- Having a job that requires heavy lifting or a lot of bending and twisting
- Past neck injury (often several years before)
- Past spine surgery
- Ruptured or slipped disk
- Severe arthritis
Risk factors for cervical degenerative disc disease
Risk factors for cervical degenerative disc disease include:
- Age. Cervical degenerative disc disease is a normal part of aging.
- Occupation. Jobs that involve repetitive neck motions, awkward positioning or a lot of overhead work put extra stress on your neck.
- Neck injuries. Previous neck injuries appear to increase the risk of cervical spondylosis.
- Genetic factors. Some individuals in certain families will experience more of these changes over time, while others will not.
- Smoking. Smoking has been linked to increased neck pain.
- Depression or anxiety.
Cervical degenerative disc disease symptoms
For most people cervical degenerative disc disease causes no symptoms. Symptoms often develop slowly over time. But they may start or get worse suddenly. The pain may be mild, or it can be deep and so severe that you are unable to move. When symptoms do occur, they typically include pain and stiffness in the neck.
You may feel the pain over the neck and shoulder blade or stiffness – that comes and goes. It may spread to the upper arm, forearm, or fingers (in rare cases).
The pain may get worse:
- After standing or sitting
- At night
- When you sneeze, cough, or laugh
- When you bend the neck backwards or walk more than a few yards or more than a few meters
You may also have weakness in certain muscles. Sometimes, you may not notice it until your doctor examines you. In other cases, you will notice that you have a hard time lifting your arm, squeezing tightly with one of your hands, or other problems.
Other common symptoms are:
- Neck stiffness that gets worse over time
- Muscle spasms in the neck and shoulders
- Numbness or abnormal sensations in the shoulders, arms and hands and fingers
- Headaches, especially in the back of the head
- Pain on the inside of the shoulder blade and shoulder pain
- Grinding or popping noise or sensation when you turn your neck
Less common symptoms are:
- Trouble walking, loss of balance, or weakness in the hands or legs
- Pain or numbness in the legs
- Loss of control over the bladder or bowels (if there is pressure on the spinal cord)
Cervical degenerative disc disease possible complications
Cervical degenerative disc disease may lead to the following:
- Inability to hold in feces (fecal incontinence) or urine (urinary incontinence)
- Loss of muscle function or feeling
- Permanent disability (occasionally)
- Poor balance
If your spinal cord or nerve roots become severely compressed as a result of cervical degenerative disc disease, the damage can be permanent.
Cervical degenerative disc disease diagnosis
A physical exam may show that you have trouble moving your head toward your shoulder and rotating your head.
Your health care provider may ask you to bend your head forward and to each side while putting slight downward pressure on the top of your head. Increased pain or numbness during this test is usually a sign that there is pressure on a nerve in your spine.
Weakness of your shoulders and arms or loss of feeling can be signs of damage to certain nerve roots or to the spinal cord.
A spine or neck x-ray may be done to look for arthritis or other changes in your spine. Spinal x-rays may show narrowing of the disc spaces and spinal canal. Bony outgrowths (osteophytes) may be noted at the corners of the vertebrae.
MRI or CT scans of the neck are done when you have:
- Severe neck or arm pain that does not get better with treatment
- Weakness or numbness in your arms or hands
MRI is recommended to assess the extent of the cervical degenerative disc disease and to help exclude other possible causes for the symptoms. A CT may also be useful as it gives better visualization of the bony structures.
Myelograpy. This is a special type of CT scan. In this procedure, a contrast dye is injected into the spinal canal to make the spinal cord and nerve roots show up more clearly.
Your doctor might recommend tests to determine if nerve signals are traveling properly to your muscles. Nerve function tests include:
- Electromyography (EMG). This test measures the electrical activity in your nerves as they transmit messages to your muscles when the muscles are contracting and when they’re at rest.
- Nerve conduction study. Electrodes are attached to your skin above the nerve to be studied. A small shock is passed through the nerve to measure the strength and speed of nerve signals.
Other tests. In some cases, your doctor may order a blood test to determine whether a rheumatoid factor—or any other antibody indicative of inflammatory arthritis–is present.
Cervical degenerative disc disease treatment
Nonsurgical Treatment
Treatment for cervical degenerative disc disease depends on the severity of your signs and symptoms. The goal of treatment is to relieve pain, help you maintain your usual activities as much as possible, and prevent permanent injury to the spinal cord and nerves.
How you can ease neck pain yourself – painkillers like acetaminophen and ibuprofen can help ease neck pain and stiffness. You can also use ibuprofen gel on your neck. Putting heat or cold packs on your neck can also help. When sleeping use a low, firm pillow, making sure your head is the same height as the rest of your body. You try neck exercises (see below).
Physical therapy is usually the first nonsurgical treatment that your doctor will recommend. Specific exercises can help relieve pain, as well as strengthen and stretch weakened or strained muscles. In some cases, physical therapy may include posture therapy or the use of traction to gently stretch the joints and muscles of your neck. Physical therapy programs vary in length, but generally last from 6 to 8 weeks. Typically, sessions are scheduled 2 to 3 times per week.
Your doctor might also prescribe a muscle relaxant or other medicine if the pain has been coming and going for a long time (chronic pain).
It usually takes a few weeks for treatment to work, although the pain and stiffness can come back.
Your doctor and other health professionals can help you manage your pain so that you can stay active.
- Your doctor may refer you for physical therapy. The physical therapist will help you reduce your pain using stretches. The therapist will teach you exercises that make your neck muscles stronger.
- The therapist can also use neck traction to relieve some of the pressure in your neck.
- You may also see a massage therapist, someone who performs acupuncture, or someone who does spinal manipulation (a chiropractor, osteopathic doctor, or physical therapist). Sometimes, a few visits will help with neck pain.
- Cold packs and heat therapy may help your pain during flare-ups.
A type of talk therapy called cognitive behavioral therapy (CBT) may be helpful if the pain is having a serious impact on your life. This technique helps you better understand your pain and teaches you how to manage it.
Medicines can help your neck pain. Your doctor may prescribe nonsteroidal anti-inflammatory medicines (NSAIDs) for long-term pain control. Opioids may be prescribed if the pain is severe and does not respond to NSAIDs.
Medications
If over-the-counter pain relievers don’t help, your doctor might prescribe several medications to be used together to address both pain and inflammation:
- Acetaminophen. Mild pain is often relieved with acetaminophen.
- Nonsteroidal anti-inflammatory drugs (NSAIDs). Prescription-strength ibuprofen (Ibuprofen) or naproxen sodium (Anaprox, Anaprox DS) might be needed to relieve pain and inflammation.
- Corticosteroids. Oral medications, such as prednisone, might help ease pain. If your pain is severe, your doctor might suggest steroid injections.
- Steroid-based injections. Although less invasive than surgery, steroid-based injections are prescribed only after a complete evaluation by your doctor. Your doctor will talk with you about the risks and benefits of steroid-based injections for your specific condition. Many patients find short-term pain relief from steroid injections. The most common procedures for neck pain include:
- Cervical epidural block. In this procedure, steroid and anesthetic medicine is injected into the space next to the covering of the spinal cord (“epidural” space). This procedure is typically used for neck and/or arm pain that may be due to a cervical disk herniation, also known as radiculopathy or a “pinched nerve.”
- Cervical facet joint block. In this procedure, steroid and anesthetic medicine is injected into the capsule of the facet joint. The facet joints are located in the back of the neck and provide stability and movement. These joints can develop arthritic changes that may contribute to neck pain.
- Medial branch block and radiofrequency ablation. This procedure is used in some cases of chronic neck pain. It can be used to both diagnose and treat a painful joint. During the diagnosis portion of the procedure, the nerve that supplies the facet joint is blocked with a local anesthetic. If your pain is relieved, then your doctor may have pinpointed the source of your neck pain. The next step option may be to block the pain more permanently. This is done by damaging the nerves that supply the joint with a “burning” technique—a procedure called radiofrequency ablation.
- Muscle relaxants. Certain drugs, such as cyclobenzaprine (Amrix, Fexmid) and methocarbamol (Robaxin), can help relieve muscle spasms in the neck.
- Anti-seizure medications. Some types of epilepsy medications, such as gabapentin (Neurontin) and pregabalin (Lyrica), can dull the pain of damaged nerves.
- Antidepressants. Certain antidepressant medications have been found to help ease neck pain from cervical spondylosis.
- Prescription pain relievers. Your doctor might prescribe oxycodone (Percocet, Roxicet).
Acupuncture
Your doctor might recommend trying acupuncture to reduce your pain. Acupuncture is best provided by a licensed acupuncture practitioner.
If the pain does not respond to these treatments, or you have a loss of movement or feeling, surgery is considered. Surgery is done to relieve the pressure on the nerves or spinal cord.
Surgical Treatment
If conservative treatment fails or if have progressive neurologic symptoms, such as arm weakness, numbness, or falling, you might need surgery to create more room for your spinal cord and nerve roots. Surgery may also be recommended if you have severe pain that has not been relieved by nonsurgical treatment.
Surgery is only considered if:
- a nerve is being pinched by a slipped disc or bone (cervical radiculopathy)
- there’s a problem with your spinal cord (cervical myelopathy)
Surgery is not always a cure but it may stop symptoms getting worse. Some patients with severe neck pain will not be candidates for surgery. This may be due to the widespread nature of their arthritis, other medical problems, or other causes for their pain, such as fibromyalgia.
A variety of factors determine success after surgery. Factors that may be suggestive of a less satisfactory outcome include:
- severe neurological symptoms before surgery,
- evidence of spinal cord shrinkage on MRI, and
- severe cord compression seen on x-rays.
Surgical Treatment options
If after a period of time nonsurgical treatment does not relieve your symptoms, your doctor may recommend surgery. There are three surgical procedures to treat cervical radiculopathy. The procedure your doctor recommends will depend on many factors, including what symptoms you are experiencing and the location of the involved nerve root.
They are:
- Anterior Cervical Diskectomy and Fusion
- Artificial Disk Replacement
- Posterior Cervical Laminoforaminotomy
The procedure your doctor recommends will depend on a number of factors–most importantly, the type and location of your problem. Other factors include:
- Your preference for a procedure
- Your doctor’s preference and experience
- Your overall health and medical history (including whether you have had prior neck surgery)
Anterior Cervical Diskectomy and Fusion
Anterior Cervical Diskectomy and Fusion is the most commonly performed procedure to treat cervical radiculopathy. The procedure involves removing the problematic disk or bone spurs and then stabilizing the spine through spinal fusion.
The goals of anterior cervical diskectomy and fusion are to:
- Restore alignment of the spine
- Maintain the space available for the nerve roots to leave the spine
- Limit motion across the degenerated segment of the spine
Procedure. An “anterior” approach means that the doctor will approach your neck from the front. He or she will operate through a 1- to 2-inch incision along the neck crease. The exact location and length of your incision may vary depending on your specific condition.
During the procedure, your doctor will remove the problematic disk and any additional bone spurs, if necessary. The disk space is restored to the height it was prior to the disk wearing out. This makes more room for the nerves to leave the spine and aids in decompression.
Spinal fusion. After the disk space has been cleared out, your doctor will use spinal fusion to stabilize your spine. Spinal fusion is essentially a “welding” process. The basic idea is to fuse together the vertebrae so that they heal into a single, solid bone. Fusion eliminates motion between the degenerated vertebrae and takes away some spinal flexibility. The theory is that if the painful spine segments do not move, they should not hurt.
All spinal fusions use some type of bone material, called a bone graft, to help promote the fusion. The small pieces of bone are placed into the space left where the disk has been removed. Sometimes larger, solid pieces are used to provide immediate structural support to the vertebrae.
In some cases, the doctor may implant a metal, plastic, or bone spacer between the two adjoining vertebrae. This spacer, or “cage,” usually contains bone graft material to allow a spinal fusion to occur between the two vertebrae.
After the bone graft is placed or the cage is inserted, your doctor will use metal screws, plates and rods to increase the rate of fusion and further stabilize the spine.
Bone graft sources. The bone graft will come from either your own bone (autograft) or from a donor (allograft). If an autograft is used, the bone is usually taken from your hip area. Harvesting the bone graft requires an additional incision during your surgery. It lengthens surgical time and may cause increased pain after the operation. Your doctor will talk to you about the advantages and disadvantages of using an autograft versus an allograft, as well as a traditional bone graft versus a cage.
Artificial Disk Replacement
This procedure involves removing the degenerated disk and replacing it with artificial parts, as is done in hip or knee replacement. The goal of disk replacement is to allow the spinal segment to keep some flexibility and maintain more normal motion.
Similar to anterior cervical diskectomy and fusion, your doctor will use an “anterior” approach for the surgery—making a 1- to 2-inch incision along the neck crease. The exact location and length of your incision may vary depending on your specific condition.
During the surgery, your doctor will remove your problematic disk and then insert an artificial disk implant into the disk space. The implant is made of all metal or metal and plastic. It is designed to maintain the motion between the vertebrae after the degenerated disk has been removed. The implant may help restore the height between the vertebrae and widen the passageway for the nerve roots to exit the spinal canal.
Although no longer considered a new technology, the development of artificial disk replacement is more recent than that of anterior cervical diskectomy and fusion. To date, the outcomes of artificial disk replacement surgery are promising and are comparable to that of anterior cervical diskectomy and fusion surgery. The long-term outcomes are still being researched.
Artificial disk replacement may be an option for you—depending on the type and location of your problem. Your doctor will talk with you about your options.
Posterior Cervical Laminoforaminotomy
“Posterior” refers to the back part of your body. In this procedure, the doctor will make a 1- to 2-inch incision along the midline of the back of the neck. The exact location and size of your scar may vary depending on your condition.
During a posterior cervical laminoforaminotomy, the doctor uses a burr and other specialized tools to thin down the lamina—the bony arch that forms the backside of the spinal canal. Removing this allows the doctor better access to the damaged nerve.
He or she then removes the bone, bone spurs, and tissues that are compressing the nerve root. If your compression is due to a herniated disk, your doctor will remove the portion of the disk that is compressing the nerve, as well.
Unlike anterior cervical diskectomy and fusion, posterior cervical laminoforaminotomy does not require spinal fusion to stabilize the spine. Because of this, you will maintain better range of motion in your neck and your recovery will be quicker.
The procedure can be performed as open surgery, in which your doctor uses a single, larger incision to access your spine. It can also be done using a minimally invasive method, where several smaller incisions are made. Your doctor will discuss with you whether posterior cervical laminoforaminotomy is an option for you and, if so, how the surgery will be performed.
Complications
As with any surgical procedure, there are risks associated with cervical spine surgery. Possible complications can be related to the approach used, the bone graft, healing, and long-term changes. Before your surgery, your doctor will discuss each of the risks with you and will take specific measures to help avoid potential complications.
General Risks
The possible risks and complications for any cervical spine surgery include:
- Infection
- Bleeding
- Nerve injury
- Spinal cord injury
- Reaction to anesthesia
- The need for additional surgery in the future
- Failure to relieve symptoms
- Tear of the sac covering the nerves (dural tear)
- Life-threatening medical problems, such as heart attack, lung complications, or stroke
Anterior Cervical Diskectomy and Fusion and Artificial Disk Replacement Risks
There are additional potential risks and complications when an anterior approach is used in spine surgery. They include:
- Misplaced, broken, or loosened plates, screws, or implants
- Soreness or difficulty with swallowing
- Voice changes
- Breathing difficulty
- Injury to the esophagus
- Pain at the site the bone was taken from—if an autograft is used
- Nonunion of the spinal fusion (in Anterior Cervical Diskectomy and Fusion)
Recovery
After surgery, you will typically stay in the hospital for 1 or 2 days. This will vary, however, depending on the type of surgery you have had and how many disk levels were involved.
Most patients are able to walk and eat on the first day after surgery. It is normal to have difficulty swallowing solid foods for a few weeks or have some hoarseness following anterior cervical spine surgery.
You may need to wear a soft or a rigid cervical collar at first. How long you should wear it will depend on the type of surgery you have had.
After spinal fusion, it may take from 6 to 12 months for the bone to become solid. Because of this, your doctor will give you specific restrictions for some time period after your surgery. Right after your operation, your doctor may recommend only light activity, like walking. As you regain strength, you will be able to slowly increase your activity level.
Physical Therapy
Usually by 4 to 6 weeks, you can gradually begin to do range-of-motion and strengthening exercises. Your doctor may prescribe physical therapy during the recovery period to help you regain full function.
Return to Work
Most people are able to return to a desk job within a few days to a few weeks after surgery. They may be able to return to full activities by 3 to 4 months, depending on the procedure. For some people, healing may take longer.
Outcomes
Most patients experience favorable outcomes after surgery for cervical radiculopathy. In most cases, they experience relief from their pain and other symptoms and are able to successfully return to the activities of daily life after a period of recovery.
Cervical degenerative disc disease exercises
Neck pain can be helped with exercise and by improving your posture.
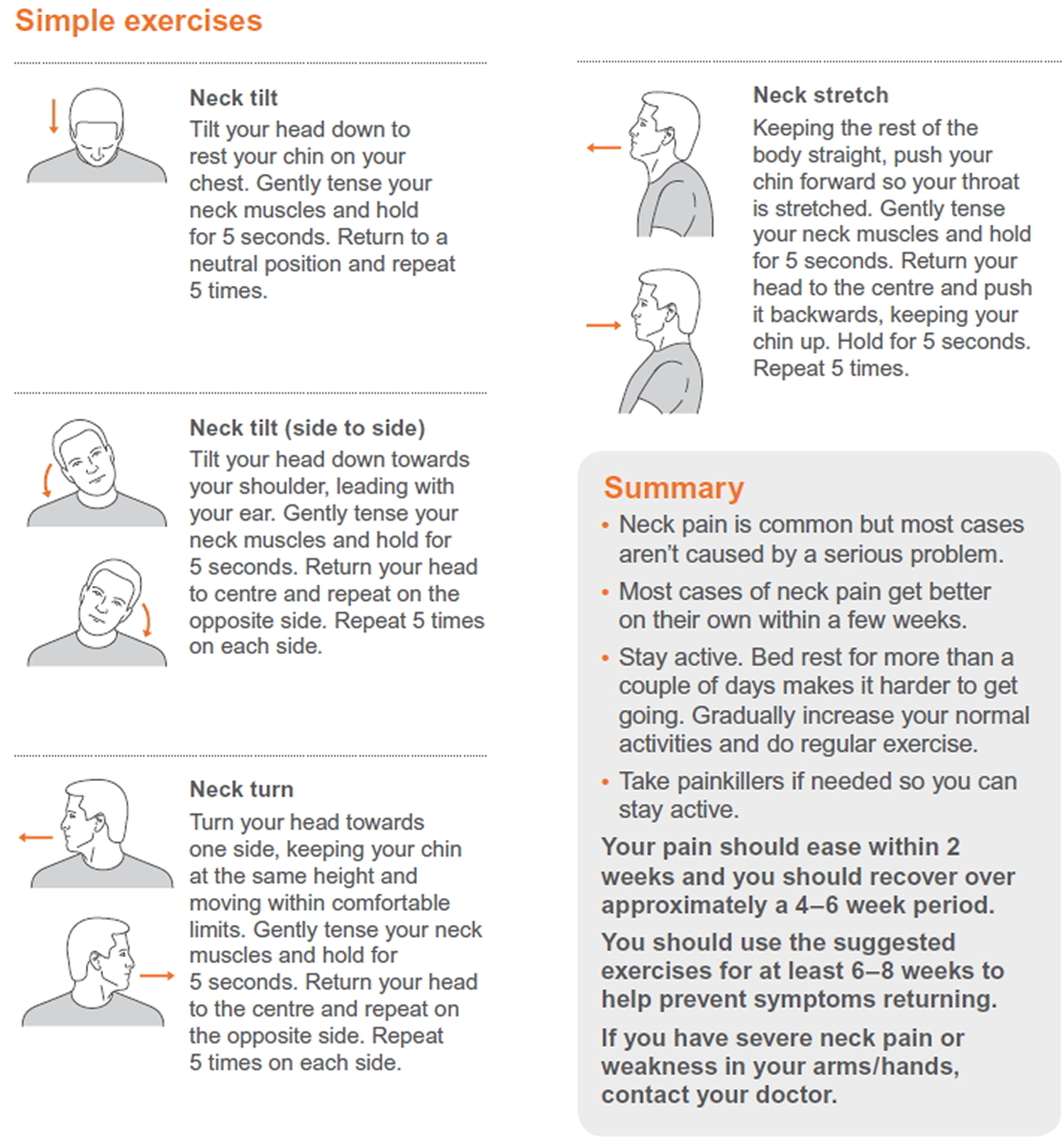
There are some simple exercises you can do to help strengthen the muscles in your neck and keep your neck mobile.
Try gently nodding 15 times. Bring your chin down to your chest as far as is comfortable, and up towards the ceiling as far as is comfortable.
Turn your head slowly from left to right 15 times. You should only turn your head as far as feels comfortable.
Tilt your head as if you are trying to touch your left shoulder with your left ear, and the same for the right 15 times. Again, only tilt your head as far as is comfortable for you. Don’t move your shoulders up to meet your ears.
Cervical flexion
Increasing neck movement by moving the head forwards in sitting.
Cervical side-flexion
Active neck movement bending side to side (side-flexion) in sitting position
Cervical rotation
Active neck movement by turning side to side (rotation) in sitting position.
Chin tucks (cervical retraction)
Strengthening of the stabilising neck muscles by drawing the chin in gently in sitting position.
Figure 3. Cervical degenerative disc disease exercises
Alternative cervical degenerative disc disease exercises
Try gently nodding 15 times. Bring your chin down to your chest as far as is comfortable, and up towards the ceiling as far as is comfortable.
Turn your head slowly from left to right 15 times. You should only turn your head as far as feels comfortable.
Tilt your head as if you are trying to touch your left shoulder with your left ear, and the same for the right 15 times. Again, only tilt your head as far as is comfortable for you. Don’t move your shoulders up to meet your ears.
And to reduce your chances of future episodes of neck pain, you can:
- Improve your posture with gentle stretching exercises, such as those popular in activities such as yoga or Pilates.
- Arrange your work space so that your desk and chair are suitable for your needs. Ask for a footrest if you find that your knees and hips are not level and your feet do not sit flat on the ground. You may also need to move items that you use regularly closer to you, so that you don’t twist or reach too far to find items you need.
- Support your neck while sleeping with a support pillow, and sleep with just one pillow.
- Make sure your neck is supported in the car by adjusting the headrest so that it is at least at eye level and as close to the back of your head as possible.
Lifestyle and home remedies
Mild cervical degenerative disc disease might respond to:
- Regular exercise. Maintaining activity will help speed recovery, even if you have to temporarily modify some of your exercises because of neck pain. People who walk daily are less likely to experience neck and low back pain.
- Over-the-counter pain relievers. Ibuprofen (Advil, Motrin IB, others), naproxen sodium (Aleve) or acetaminophen (Tylenol, others) is often enough to control the pain associated with cervical degenerative disc disease.
- Heat or ice. Applying heat or ice to your neck can ease sore neck muscles.
- Soft neck collar. This is a padded ring that wraps around the neck and is held in place with velcro. Your doctor may advise you to wear a soft cervical collar to limit neck motion and allow the muscles in your neck to rest. A soft collar should only be worn for a short period of time since long-term wear may decrease the strength of the muscles in your neck. Therefore it’s better to keep your neck moving and don’t wear a soft collar (unless a doctor tells you to).
Cervical degenerative disc disease prognosis
Most people with cervical degenerative disc disease have some long-term symptoms. These symptoms improve with non-surgical treatment and do not need surgery.
Many people with this problem are able to maintain an active life. Some people will have to live with chronic (long-term) pain.
- Fardon DF, Milette PC. Nomenclature and classification of lumbar disc pathology. Recommendations of the Combined task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. Spine (Phila Pa 1976). 2001 Mar 1. 26(5):E93-E113.[↩]
- Tanaka Y, Kokubun S, Sato T, et al. Cervical roots as origin of pain in the neck or scapular regions. Spine. 2006 Aug 1. 31(17):E568-73.[↩]
- Slipman CW, Plastaras C, Patel R, et al. Provocative cervical discography symptom mapping. Spine J. 2005 Jul-Aug. 5(4):381-8.[↩]
- Yates JP, McGill SM. The effect of vibration and posture on the progression of intervertebral disc herniation. Spine (Phila Pa 1976). 2011 Mar 1. 36(5):386-92.[↩]
- Shim JH, Park CK, Lee JH, Choi JW, Lee DC, Kim DH, et al. A comparison of angled sagittal MRI and conventional MRI in the diagnosis of herniated disc and stenosis in the cervical foramen. Eur Spine J. 2009 Mar 18.[↩]
- Derby R, Baker R, Dreyfuss P. Cervical radicular pain: transforaminal vs. interlaminar steroid injections. ISIS Scientific Newsletter: Current Concepts-SpineLine. 2005. 5(1):16-17.[↩]
- Galbraith JG, Butler JS, Dolan AM, O’Byrne JM. Operative outcomes for cervical myelopathy and radiculopathy. Adv Orthop. 2012. 2012:919153.[↩]
- Yan D, Li J, Zhu H, et al. Percutaneous cervical nucleoplasty and percutaneous cervical discectomy treatments of the contained cervical disc herniation. Arch Orthop Trauma Surg. 2010 Jan 8. [↩]





{kind=link}