Choanal atresia
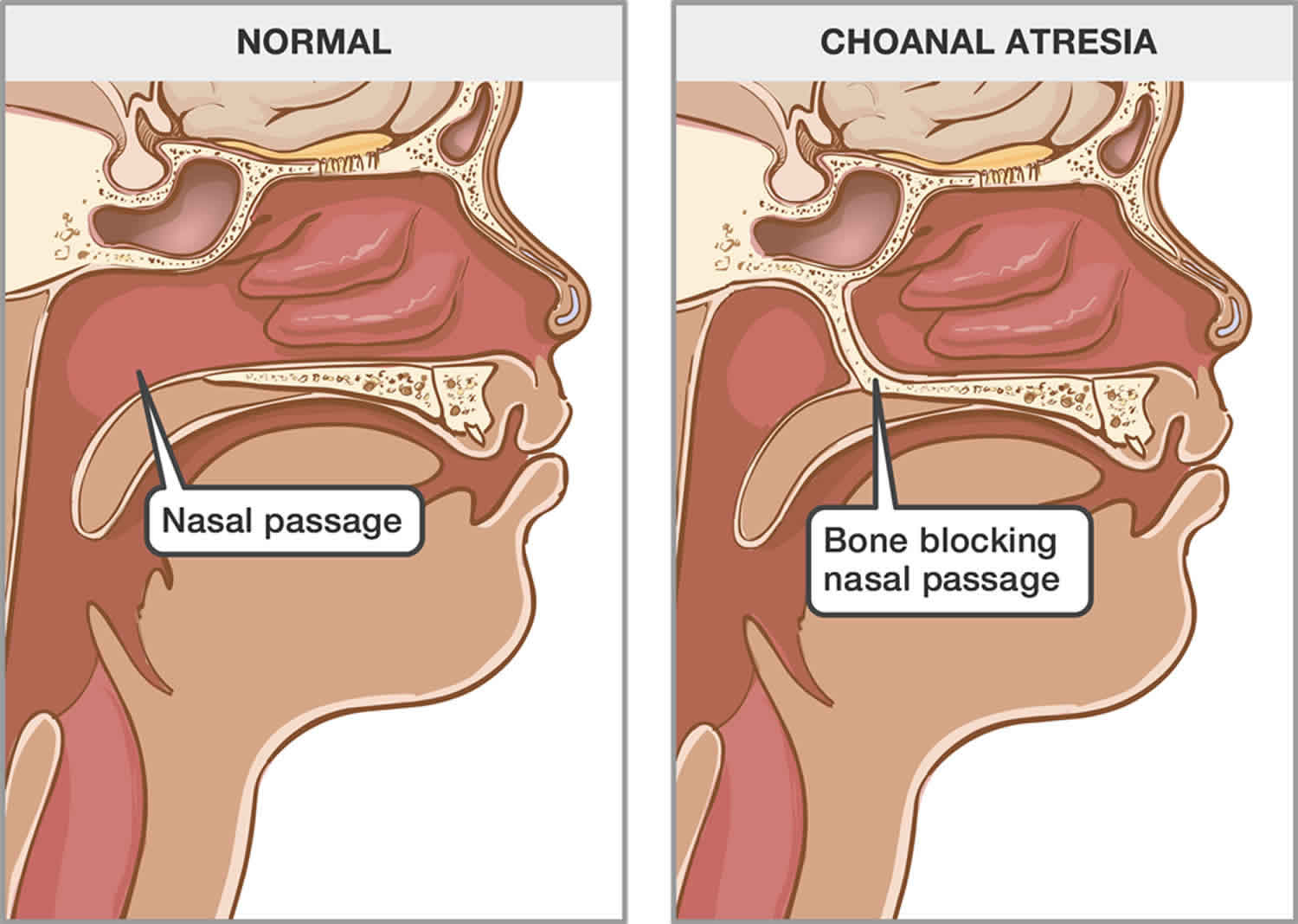
Choanal atresia is a congenital (present at birth) occlusion of the back of the nasal cavity by bone, soft tissue, or both, due to failed recanalization of the nasal fossae during fetal development that causes difficulty breathing 1. Choanal atresia is rare, occurring in approximately 1 in 7,000 live births, and is seen more often in females than in males (females to males ratio 2:1). Choanal atresia is often associated with other developmental anomalies such as CHARGE syndrome, Treacher Collins syndrome, and Tessier syndrome.
If your child is diagnosed with choanal atresia, it may take two different forms. It can can be bilateral, meaning it blocks both nasal passages, or unilateral, meaning only one nasal passage is blocked. The blockage can be either completely bony (30 percent of cases) or be composed of both bone and membranes (70 percent of cases).
- Bilateral choanal atresia is life-threatening and symptoms appear immediately after birth. Babies breathe only through their noses when they are very young, so the blocked nasal passages will cause extreme difficulty breathing. Establishing an airway is an acute otolaryngologic emergency 2.
- Unilateral choanal atresia is more common (60% of case), less serious, and sometimes appears later in childhood because the child has been able to manage while breathing through only one side of the nasal passage.
The treatment of choanal atresia is essentially surgical. The objectives are to restore choanal patency, not to interfere with the patient normal craniofacial development, to minimize invasiveness, and to avoid recurrences.
Unilateral choanal atresia does not require surgical treatment as urgently as the bilateral case and can be postponed until school age when the anatomy of the region is more similar to that in adults. However, it needs to be closely monitored for any signs of a breathing problem. Using a nasal saline spray can also help to keep the nasal route clear.
Figure 1. Choanal atresia
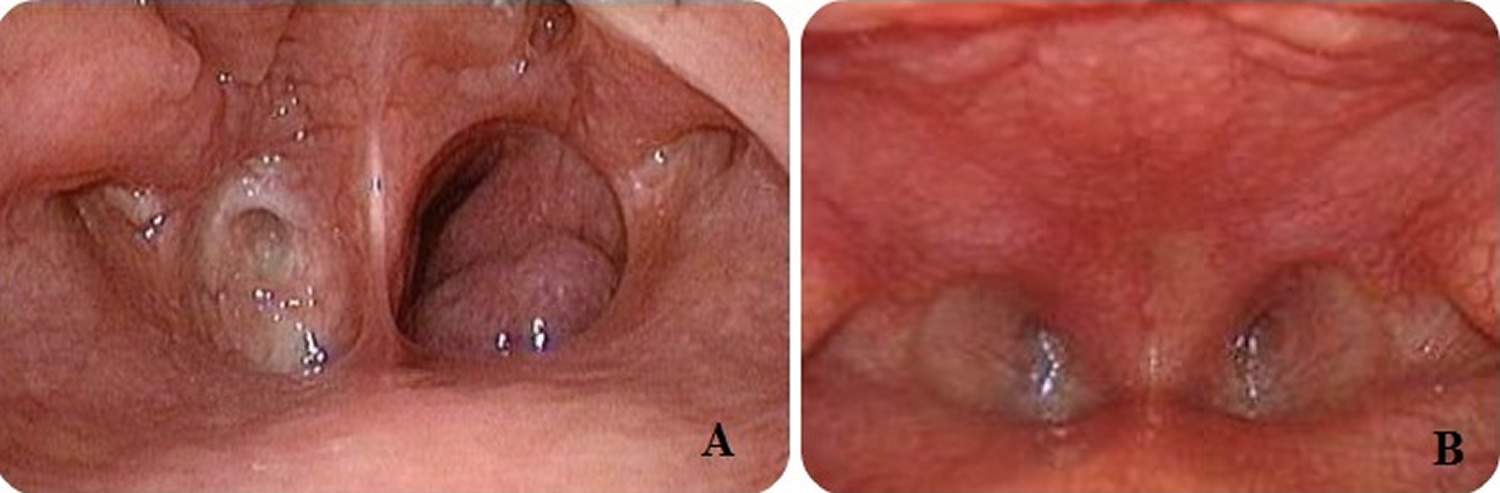
Footnote: (A) Unilateral choanal atresia; (B) Bilateral choanal atresia.
Choanal atresia causes
Choanal atresia is a developmental abnormality. Nasal choanae (paired openings that connect the nasal cavity with the nasopharynx) develop between the third and seventh embryonic weeks, following rupture of the vertical epithelial fold between the olfactory groove and the roof of the primary oral cavity (stomodeum) 1. Choanal atresia is present at birth and can be associated with other developmental abnormalities.
There is no known specific cause of choanal atresia. Most believe that choanal atresia occurs when the tissue that separates the nose and mouth area during fetal development remains after birth. The following theories have been proposed to explain the pathogenesis of choanal atresia: the persistence of the buccopharyngeal membrane, the persistence of the nasobuccal membrane of Hochstetter, the incomplete resorption of the nasopharyngeal mesoderm, and the local misdirection of neural crest cell migration. These theories are associated with molecular and genetic studies to give further insights into the pathogenesis of choanal atresia 3.
Choanal atresia symptoms
The symptoms of choanal atresia include:
- Cyclic respiratory distress relieved with crying
- Noisy breathing
- Feeding difficulties
- Inability to pass a 5/6 French suction catheter into the nasopharynx
- Nasal drainage
Babies with unilateral choanal atresia often show symptoms later during infancy and childhood with signs of unilateral nasal obstruction (discharge, mouth breathing, inability to move air on one side) and/or a history of chronic sinusitis. Since one side is open at birth, it is rare that these infants have difficulty breathing when they are first born. In some cases, the correct diagnosis is not reached until adulthood due to the non-specific symptoms of unilateral nasal obstruction.
Babies with bilateral choanal atresia often have respiratory distress with cyanosis episodes immediately after birth. These are relieved only when the baby begins to cry and with the return of cyanosis with rest (paradoxical cyanosis). Feeding difficulty can be the initial alerting event in which the infants can present with progressive airway obstruction and choke episodes during feeding because of their inability to breathe and feed at the same time. The child can not breathe during normal circumstances and can only breath when they open their airway to cry. Because of this, infants with bilateral choanal atresia often require intubation immediately after delivery. Once the airway is secured, the baby can be evaluated for other developmental abnormalities. CHARGE syndrome is the most common of these and consists of coloboma, heart disease, atresia choanae, growth and mental retardation, genital hypoplasia, and ear anomalies 4.
Choanal atresia diagnosis
The diagnosis of choanal atresia should be done immediately after birth. The initial clinical evaluation includes placing a laryngeal mirror under to nostril to check for fogging and introducing a suction catheter through each nostril and into the child’s oral cavity. The clinical suspicion of choanal atresia can be confirmed by examination with a flexible nasal endoscope in a newborn with proper preparation, such as nasal decongestion and mucous suctioning, allowing direct visualization of the possible obstruction in the nasal passage. To confirm the diagnosis of choanal atresia a CT scan should be done to further delineate characteristics of the malformation, such as the anatomy of the atretic area, including the thickness of the atretic plate and the presence and thickness of a bony plate. Besides delineating the nature and severity of choanal atresia, CT is also useful in differentiating other causes of nasal obstruction from choanal atresia. Differential diagnoses include pyriform aperture stenosis, nasolacrimal duct cysts, turbinate hypertrophy, septal dislocation and deviation, antrochoanal polyp, or nasal neoplasm.
Choanal atresia treatment
Choanal atresia treatment depends on the severity of the anomaly (unilateral or bilateral), how much it affects the child’s breathing and eating, and what other medical conditions the patient has.
In August 2019, the International Pediatric Otolaryngology Group published consensus recommendations, including the following, with regard to pediatric choanal atresia diagnosis and care 5:
- Nasal endoscopy or fiberscopy and computed tomography (CT) scanning are recommended diagnostic modalities
- Whenever possible, unilateral choanal atresia repair should wait until the patient is over age 6 months
- Treatment with transnasal endoscopic repair is preferred
- Patient follow-up for at least 1 year, via nasofiberscopy or rigid endoscopy (but without systematic imaging), is recommended
Treatment for mild choanal atresia cases
Sometimes, a child with unilateral choanal atresia has no respiratory distress or significant feeding issues. These patients may initially be managed with close observation and occasionally supplemental oxygen. Nasal saline can help to keep the nasal linings healthy and free of discharge. Parents with children diagnosed with unilateral choanal atresia may wait until the child grows older before deciding to repair the condition.
During surgery, the nasal passage is opened. A small plastic tube called a nasal stent is placed in the nostril to keep the nasal passage open while it is healing. Nasal stents are usually left in the nasal passage for about three months. When your child is ready, the stent will be removed in the hospital under a general anaesthetic.
Aero-digestive evaluation
If your infant has choanal atresia, he should be evaluated for both airway and feeding issues. Management of the airway often requires a combination of supportive, medical and surgical care. Feeding and swallowing issues are very common in children with these conditions and often need to be addressed by speech pathologists and gastroenterologists. Children born with syndromes often need other subspecialty evaluations (cardiology, ophthalmology, etc.) and benefit greatly from the coordinated care provided in the multidisciplinary setting.
Treatment for severe choanal atresia cases
If your child is diagnosed with bilateral choanal atresia the condition must be treated as soon as possible. The acute care of infants with bilateral choanal atresia in asphyxia consists of endotracheal intubation (when available, may be utilized a McGovern nipple to maintain an adequate oral airway, consisting in an intraoral nipple with a large opening by cutting its end off, secured in the mouth with ties around the infant’s occiput) followed by perforation of the atresia plate.
Surgery should be performed as soon as the patient is stable and has been evaluated for other anomalies. The major goal of the surgical repair is to open the nasal airway sufficiently, allowing the infant to breathe on his own. There are five different surgical approaches available (i.e., transpalatal, transeptal, sublabial, transantral. and transnsal) to accomplish this goal, all of which are performed in the operating room under general anesthesia.
Choanal atresia repair
The growing experience in both instrumentation and technique in endoscopic sinus surgery have led many surgeons to make more frequent use of the endoscopic endonasal technique for the repair of choanal atresia, which has provided better results and fewer surgical complications than in traditional procedures.
- Transnasal endoscopic approach: Currently, surgeons prefer to treat children with choanal atresia using the transnasal endoscopic approach. It can be done safely on infants just a few days old. The posterior nasal airway is opened using a combination of dilators, sinus instruments, ear curettes and drills. In some cases, a piece of endotracheal tube is placed inside the nasal passage as a stent to maintain the opening while the area heals. The stent will be removed a few weeks after the surgery at the bedside or during an office visit. Sometimes stenting is not required.
- The transseptal technique consists of making a window in the septum anterior to the atretic plate.
- Transpalatal approach: The transpalatal approach was the most frequently used until the advent, in the last decades, of the endoscopic endonasal approach. The increased blood loss and the possible occurrence of palatal fistula, palatal dysfunction, and maxillofacial growth disturbance are complications of this procedure. In rare circumstances where the skull base is abnormally developed (other craniofacial anomalies are present), the surgeon may need to use a transpalatal approach to reach the area of choanal atresia through the roof of the mouth.
The use of choanal stenting and mitomycin C as an adjunct therapy to prevent restenosis are a controversial topic in the management of choanal atresia as there is no clear-cut evidence on the effectiveness of using stents or mitomycin after choanal atresia repair 6.
Follow-up
Following surgical repair of choanal atresia, patients may require operative debridement or periodic dilatations. Periodic dilations can sometimes be performed as an outpatient procedure with local decongestant and topical anesthesia using urethral sounds.
Bedwell et al 7 described the use of balloon dilation to repair choanal atresia in a series of patients with membranous stenoses, postrepair granulation, and scar tissue in revision cases. They concluded that balloon dilation is an effective adjuvant tool for use in the repair of choanal atresia and stenosis.
- Andaloro C, La Mantia I. Choanal Atresia. [Updated 2019 Apr 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507724[↩][↩]
- Murray S, Luo L, Quimby A, Barrowman N, Vaccani JP, Caulley L. Immediate versus delayed surgery in congenital choanal atresia: A systematic review. Int. J. Pediatr. Otorhinolaryngol. 2019 Apr;119:47-53.[↩]
- Kurosaka H. Choanal atresia and stenosis: Development and diseases of the nasal cavity. Wiley Interdiscip Rev Dev Biol. 2019 Jan;8(1):e336.[↩]
- Smith MM, Ishman SL. Pediatric Nasal Obstruction. Otolaryngol. Clin. North Am. 2018 Oct;51(5):971-985.[↩]
- Moreddu E, Rizzi M, Adil E, et al. International Pediatric Otolaryngology Group (IPOG) consensus recommendations: Diagnosis, pre-operative, operative and post-operative pediatric choanal atresia care. Int J Pediatr Otorhinolaryngol. 2019 Aug. 123:151-5.[↩]
- Moreddu E, Rossi ME, Nicollas R, Triglia JM. Prognostic Factors and Management of Patients with Choanal Atresia. J. Pediatr. 2019 Jan;204:234-239.e1.[↩]
- Bedwell J, Shah RK, Bauman N, Zalzal GH, Preciado DA. Balloon dilation for management of choanal atresia and stenosis. Int J Pediatr Otorhinolaryngol. 2011 Dec. 75(12):1515-8.[↩]





{kind=link}