
Chronic granulomatous disease
Chronic granulomatous disease is an inherited immune deficiency disease that causes your immune system to malfunction, resulting in a form of immunodeficiency. Immunodeficiencies are conditions in which your immune system is not able to protect your body from foreign invaders such as bacteria and fungi. People with chronic granulomatous disease are highly susceptible to frequent and sometimes life-threatening bacterial and fungal infections. People with chronic granulomatous disease may also have areas of granulomas (clusters of white blood cells in infected areas) in various tissues that can result in damage to those tissues. The features of chronic granulomatous disease usually first appear in childhood, although some individuals do not show symptoms until later in life. Milder forms may be diagnosed during the teenage years, or even in adulthood.
Chronic granulomatous disease is also called chronic septic granulomatosis, Bridges–Good syndrome and Quie syndrome.
Chronic granulomatous disease is a genetic disorder in which phagocytes (a type of white blood cell that kills bacteria and fungi – neutrophils and macrophages) are unable to kill certain types of bacteria and fungi. Chronic granulomatous disease is caused by defects in an enzyme called nicotinamide adenine dinucleotide phosphate (NADPH) oxidase that phagocytes need to kill certain bacteria and fungi.
Chronic granulomatous disease is characterized by:
- The inability of phagocytes — cells that ingest microorganisms — to make the chemicals necessary to kill off some types of fungi and bacteria
- The presence of granulomas, or aggregations of immune cells which cluster around sites that are inflamed or infected
- Inflammation, even in absence of infection
Chronic granulomatous disease is estimated to occur in 1 in 200,000 to 250,000 people worldwide. People with chronic granulomatous disease typically have at least one serious bacterial or fungal infection every 3 to 4 years. The lungs are the most frequent area of infection; pneumonia is a common feature of this condition. Individuals with chronic granulomatous disease may develop a type of fungal pneumonia, called mulch pneumonitis, which causes fever and shortness of breath after exposure to decaying organic materials such as mulch, hay, or dead leaves. Exposure to these organic materials and the numerous fungi involved in their decomposition causes people with chronic granulomatous disease to develop fungal infections in their lungs. Other common areas of infection in people with chronic granulomatous disease include the skin, liver, and lymph nodes.
Inflammation can occur in many different areas of the body in people with chronic granulomatous disease. Most commonly, granulomas occur in the gastrointestinal tract and the genitourinary tract. In many cases the intestinal wall is inflamed, causing a form of inflammatory bowel disease that varies in severity but can lead to stomach pain, diarrhea, bloody stool, nausea, and vomiting. Other common areas of inflammation in people with chronic granulomatous disease include the stomach, colon, and rectum, as well as the mouth, throat, and skin. Additionally, granulomas within the gastrointestinal tract can lead to tissue breakdown and pus production (abscesses). Inflammation in the stomach can prevent food from passing through to the intestines (gastric outlet obstruction), leading to an inability to digest food. These digestive problems cause vomiting after eating and weight loss. In the genitourinary tract, inflammation can occur in the kidneys and bladder. Inflammation of the lymph nodes (lymphadenitis) and bone marrow (osteomyelitis), which both produce immune cells, can lead to further impairment of the immune system.
Rarely, people with chronic granulomatous disease develop autoimmune disorders, which occur when the immune system malfunctions and attacks the body’s own tissues and organs.
Repeated episodes of infection and inflammation reduce the life expectancy of individuals with chronic granulomatous disease; however, with treatment, most affected individuals live into mid- to late adulthood.
Treatment for chronic granulomatous disease is aimed at helping you avoid infections and manage your condition. Treatments may include:
- Infection management. Your doctor will work to prevent bacterial and fungal infections before they occur. Treatment may include continuous antibiotic therapy, such as trimethoprim and sulfamethoxazole (Septra) to protect against bacterial infections, and itraconazole (Omnel, Sporanox) to prevent fungal infection. Additional antibiotics or antifungal medications may be necessary should infection occur.
- Interferon-gamma. You may have interferon-gamma injections periodically, which may help boost cells in your immune system to fight infections.
- Stem cell transplantation. In some cases, a stem cell transplant can provide a cure for chronic granulomatous disease. Deciding to treat with stem cell transplantation depends on a number of factors, including prognosis, donor availability and personal preference.
Gene therapy is currently being explored for chronic granulomatous disease treatment, but further research is necessary before it’s a viable option.
Chronic granulomatous disease causes
Mutations in the CYBA, CYBB, NCF1, NCF2, or NCF4 gene can cause chronic granulomatous disease 1. There are five types of this condition that are distinguished by the gene that is involved. The proteins produced from the affected genes are parts (subunits) of an enzyme complex called NADPH oxidase, which plays an essential role in the immune system. Specifically, nicotinamide adenine dinucleotide phosphate (NADPH) oxidase is primarily active in immune system cells called phagocytes. These cells catch and destroy foreign invaders such as bacteria and fungi. Within phagocytes, NADPH oxidase is involved in the production of a toxic molecule called superoxide. Superoxide is used to generate other toxic substances, which play a role in killing foreign invaders and preventing them from reproducing in the body and causing illness. Nicotinamide adenine dinucleotide phosphate (NADPH) oxidase is also thought to regulate the activity of immune cells called neutrophils. These cells play a role in adjusting the inflammatory response to optimize healing and reduce injury to the body.
Mutations in the CYBA, CYBB, NCF1, NCF2, and NCF4 genes result in the production of proteins with little or no function or the production of no protein at all. Mutations in the genes that cause chronic granulomatous disease that prevent the production of any functional protein are designated “0”. For example, mutations in the CYBB gene that lead to no functional beta chain are designated CYBB0. Mutations that lead to a reduction of the amount of protein produced are designated “-“, for example, CYBB-.
Without any one of its subunit proteins, NADPH oxidase cannot assemble or function properly. As a result, phagocytes are unable to kill foreign invaders and neutrophil activity is not regulated. A lack of NADPH oxidase leaves affected individuals vulnerable to many types of infection and excessive inflammation.
Some people with chronic granulomatous disease do not have an identified mutation in any of these genes. The cause of the condition in these individuals is unknown.
Chronic granulomatous disease inheritance pattern
About half of chronic granulomatous disease cases are passed down through families as a sex-linked recessive trait. This means that boys are more likely to get the disorder than girls. When chronic granulomatous disease is caused by mutations in the CYBB gene, the condition is inherited in an X-linked recessive pattern (Figure 1). The CYBB gene is located on the X chromosome, which is one of the two sex chromosomes. In males (who have only one X chromosome), one altered copy of the gene in each cell is sufficient to cause the condition. In females (who have two X chromosomes), a mutation would have to occur in both copies of the gene to cause the disorder. Because it is unlikely that females will have two altered copies of this gene, males are affected by X-linked recessive disorders much more frequently than females. A characteristic of X-linked inheritance is that fathers cannot pass X-linked traits to their sons. Rarely, females with one altered copy of the CYBB gene have mild symptoms of chronic granulomatous disease, such as an increased frequency of bacterial or fungal infections.
When chronic granulomatous disease is caused by CYBA, NCF1, NCF2, or NCF4 gene mutations, the condition is inherited in an autosomal recessive pattern (see Figure 2), which means both copies of the gene in each cell have mutations. The parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition. Men and women are affected by autosomal recessive conditions equally.
Figure 1. Chronic granulomatous disease X-linked recessive inheritance pattern
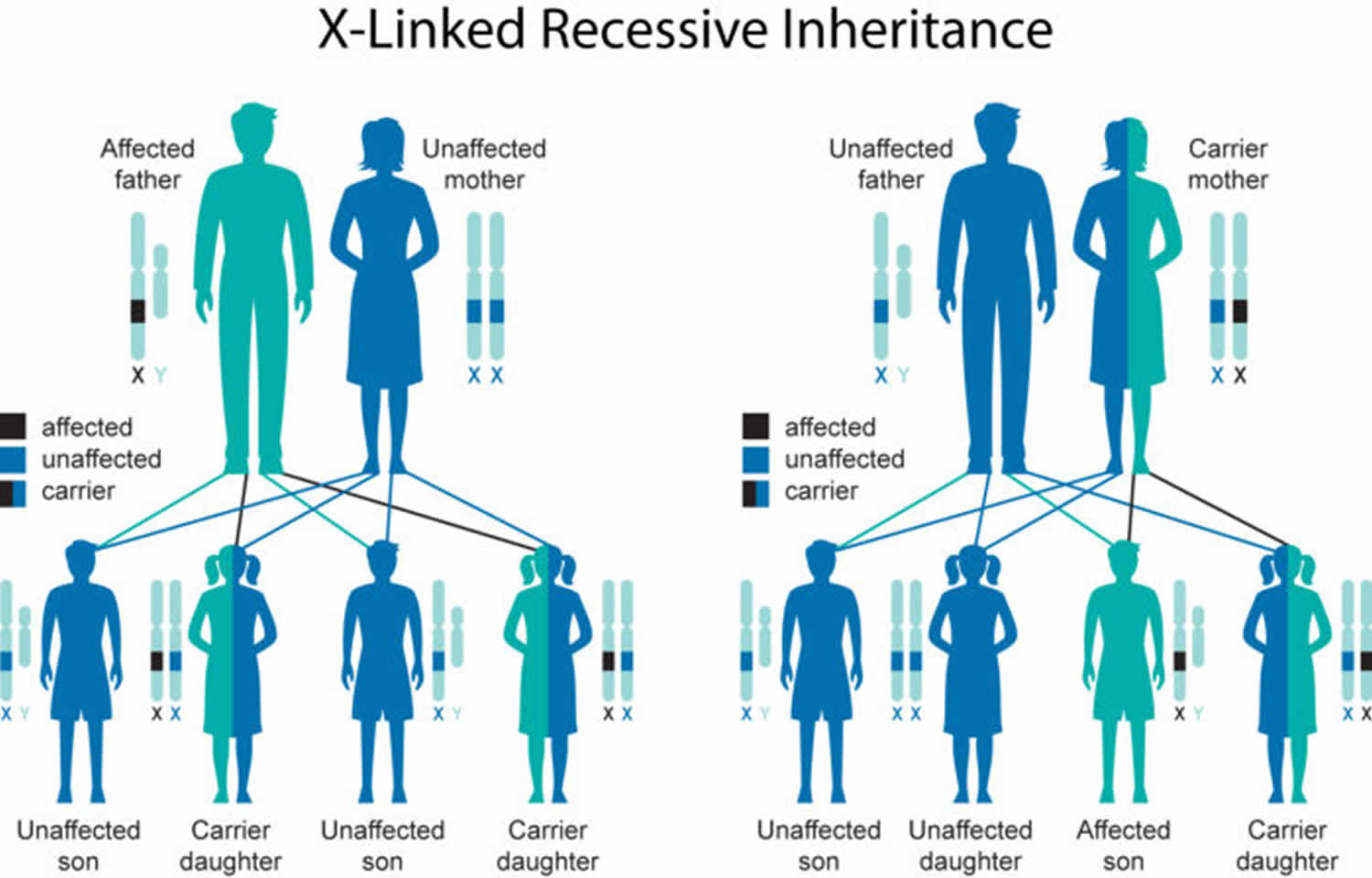
Figure 2. Chronic granulomatous disease autosomal recessive inheritance pattern

Chronic granulomatous disease prevention
Genetic counseling is recommended if you are planning to have children and you have a family history of this disease. Advances in genetic screening and increasing use of chorionic villus sampling (a test that may be done during a woman’s 10th to 12th week of pregnancy) have made early detection of chronic granulomatous disease possible. However, these practices are not yet widespread or fully accepted.
Genetic counseling
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
Chronic granulomatous disease symptoms
People with chronic granulomatous disease are highly susceptible to infections caused by certain bacteria and fungi, such as Staphylococcus aureus, Serratia marcescens, Burkholderia cepacia, Nocardia species, and Aspergillus species. They may develop abscesses (boils) in their lungs, liver, spleen, bones, or skin and masses of cells, called granulomas, that can obstruct the bowel or urinary tract. In some people, granulomas can cause an inflammatory bowel disease similar to Crohn’s Disease.
Common signs and symptoms for chronic granulomatous disease include:
- Skin or bone infections involving the bacteria Serratia marcescens. Any infant testing positive for this species should be tested for chronic granulomatous disease.
- Bacterial infections due to Staphylococcus aureus, Burkholderia cepacia complex and Nocardia.
- Fungal infections, including Aspergillus species.
- Inflammation of the intestines. This occurs in 40–50% of patients with chronic granulomatous disease, and can sometimes be mistaken for Crohn disease.
- It responds to treatments such as systemic steroids, antibiotics and immunosuppressive therapy but not to biologics that block tumour necrosis factor alpha (TNFα).
Infants with chronic granulomatous disease present with:
- Dermatitis
- Gastrointestinal obstruction
- Colitis with resulting diarrhea
- Failure to thrive
- Recurrent infections
Furthermore, heart or kidney problems, diabetes, and autoimmune disease may occur in people with chronic granulomatous disease, but this varies depending on which gene is mutated. chronic granulomatous disease is diagnosed by special blood tests that show how well phagocytes produce hydrogen peroxide, an indicator that they are functioning properly.
Chronic granulomatous disease can cause many types of skin infections that are hard to treat, including:
- Blisters or sores on the face (impetigo)
- Eczema
- Growths filled with pus (abscesses)
- Pus-filled lumps in the skin (boils)
Chronic granulomatous disease can also cause:
- Persistent diarrhea
- Swollen lymph nodes in the neck
- Lung infections, such as pneumonia or lung abscess
Chronic granulomatous disease possible complications
Chronic granulomatous disease may cause these complications:
- Bone damage and infections
- Chronic infections in the nose
- Pneumonia that keeps coming back and is hard to cure
- Lung damage
- Skin damage
- Swollen lymph nodes that stay swollen, occur often, or form abscesses that need surgery to drain them
Chronic granulomatous disease diagnosis
To diagnose chronic granulomatous disease, your doctor will review your family and medical history and conduct a physical examination.
Your health care provider will do an examination and may find:
- Liver swelling
- Spleen swelling
- Swollen lymph nodes
There may be signs of a bone infection, which may affect many bones.
Your doctor may order several tests to diagnose chronic granulomatous disease, including:
- Neutrophil function tests. Your doctor may conduct a dihydrorhodamine reduction (DHR) test or other tests to see how well a type of white blood cell (neutrophil) in your blood is functioning. Dihydrorhodamine reduction (DHR) is also known as the Neutrophil Oxidative Burst Measurement test. It assesses phagocyte production of hydrogen peroxide and other important chemicals. After diagnosis, further testing is done to establish the genetic subtype. Doctors usually use this test to diagnose chronic granulomatous disease.
- Genetic testing. Your doctor may request a genetic test to confirm the presence of a specific genetic mutation that results in chronic granulomatous disease.
- Prenatal testing. Doctors may conduct prenatal testing to diagnose chronic granulomatous disease if one of your children already has been diagnosed with chronic granulomatous disease.
- Bone scan
- Chest x-ray
- Complete blood count (CBC)
- Flow cytometry tests to help confirm the disease
- Tissue biopsy
Chronic granulomatous disease treatment
Chronic granulomatous disease is treated with:
- Aggressive antibiotic therapy, intravenously if necessary, and preferably with a specific rather than a broad-spectrum antibiotic
- Transfusion of plasma
- Antibiotic prophylaxis with a combination of trimethoprim and sulfamethoxazole
- Regular use of itraconazole, an oral antifungal drug
- Injections of gamma interferon 3 times weekly
People with chronic granulomatous disease take lifelong regimens of antibiotics and antifungals to prevent infections. Injections with interferon gamma, a protein that improves the activity of phagocytes, also may be helpful to reduce the number of severe infections. Abscesses need aggressive care, which may include surgery. Granulomas may require steroid therapy. A medicine called interferon-gamma may also help reduce the number of severe infections.
Some people with chronic granulomatous disease have been cured with bone marrow transplantation but this procedure is complex and this option is not available to all patients. In patients who have undergone hematopoietic cell transplantation, the success rate is highest in young and disease-free individuals 2. Ultimately, the decision to undergo hematopoietic cell transplantation depends on the prognosis, donor availability, access to transplantation, and patient preference.
Long-term antibiotic treatments may help reduce infections, but early death can occur from repeated lung infections.
Chronic granulomatous disease prognosis
Due to advances in medical technology/treatment, the prognosis for chronic granulomatous disease patients has improved substantially. Many patients are able to lead full and healthy lives, with some restrictions such as:
- Swimming only in chlorinated pools
- Getting prompt treatment for minor infections
- Avoiding some outdoor activities such as raking, mulching or mowing (due to risk of Aspergillus exposure)
- Avoiding of the use of marijuana or marijuana products, due to Aspergillus exposure
Chronic granulomatous disease life expectancy
Autosomal recessive forms of chronic granulomatous disease have a better prognosis compared to X-linked chronic granulomatous disease 2. On average, chronic granulomatous disease patients survive at least 40 years especially with the use of long-term prophylactic antimicrobials 2. Often a severe fungal or bacterial infection can be fatal. Aspergillus is the most common fungal respiratory infection and is the most common cause of death in chronic granulomatous disease. Mortality and morbidity will continue to decrease as advances are made in prophylactic methods, bone marrow transplantation, and other immunomodulatory therapy.
- Chronic granulomatous disease. https://ghr.nlm.nih.gov/condition/chronic-granulomatous-disease[↩]
- Lent-Schochet D, Jialal I. Chronic Granulomatous Disease. [Updated 2018 Dec 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK493171[↩][↩][↩]





{kind=link}