What is clostridium difficile
Clostridium difficile (C. difficile) is a Gram-positive obligate anaerobic bacterium that causes antibiotic-associated diarrhea and more serious intestinal conditions such as colitis 1. Clostridium difficile infection is the most common cause of hospital-acquired and antibiotic-associated diarrhea worldwide. Clostridium difficile is responsible for 90–100% of the cases of pseudomembranous colitis, 50–75% of antibiotic-associated colitis and 10–25% of antibiotic-associated diarrhea in the USA 2. Clostridium difficile, which has been designated as an urgent threat by the Centers for Disease Control and Prevention (CDC), proliferates in the colon after the normal gut microbiota distribution and species diversity have been altered by antibiotic therapy 1. Thus, previous antibiotic therapy is the highest risk factor for clostridium difficile infection 3. When a person takes antibiotics, good germs that protect against infection are destroyed for several months. During this time, patients can get sick from clostridium difficile picked up from contaminated surfaces or spread from a health care provider’s hands. Those most at risk are people, especially older adults, who take antibiotics and also get medical care.
A conservative estimate by the US Centers for Disease Control and Prevention (CDC) in 2011 reported that about 500,000 diarrheal patients had clostridium difficile infection and approximately 83,000 of the patients who developed clostridium difficile experienced at least one recurrence and 29,000 died within 30 days of the initial diagnosis in the USA 4. Those most at risk are people, especially older adults, who take antibiotics and also get medical care. Furthermore, a point-prevalence survey performed by the European Centre for Disease Prevention and Control based on data from physician requests for clostridium difficile infection diagnostic test between 2011 and 2012 reported that about 124,000 patients develop healthcare-associated clostridium difficile infection within the European Union annually 5. The yearly cost of treatment of clostridium difficile infection in the USA is estimated to be up to USD$4.8 billion 6. The problem of clostridium difficile infection is important in the USA, Europe and in Canada while largely unstudied in the developing world.
Figure 1. Clostridium difficile bacteria

Symptoms of a clostridium difficile infection usually develop when you’re taking antibiotics, or when you’ve finished taking them within the last few weeks. Some people have loose stools during or shortly after antibiotic therapy. This may be due to clostridium difficile infection. See your doctor if you have three or more watery stools a day and symptoms lasting more than two days or if you have a new fever, severe abdominal pain or cramping, or blood in your stool.
Clostridium difficile symptoms include:
- Watery diarrhea (at least three bowel movements per day for two or more days)
- Fever
- Loss of appetite
- Nausea
- Abdominal pain or tenderness
- A high temperature (fever) of above 100.4 °F (38 °C)
- Loss of appetite and weight loss
If you are in good health, you likely will not get a clostridium difficile infection. The most common risk factor for clostridium difficile is the use of an antibiotic medicine. Antibiotics can disrupt the normal balance in your intestines. Your risk increases if you have taken antibiotics for a long period of time or if the antibiotic is broad-spectrum (treats a wide variety of bacteria). The elderly also have a higher risk of getting it. Clostridium difficile infection can spread in hospitals and nursing homes.
People who are 65 years of age or older are at greater risk of a clostridium difficile infection. Other risk factors include:
- surgery of the gastrointestinal (GI) tract
- stomach surgery that requires moving the intestines aside
- a stay in the hospital
- living in a nursing home or extended-care facility
- colon problems, such as inflammatory bowel syndrome (IBS) or colorectal cancer
- weakened immune system
- prior clostridium difficile infection.
Clostridium difficile bacteria are contagious. They can spread person to person. They also live a long time on surfaces, such as toilet seats, telephones, and doorknobs. Good hygiene can help you avoid the bacteria:
- Wash your hands often and well, using soap and water.
- Use disposable gloves when caring for someone who may have clostridium difficile
- Use chlorine bleach-based products to disinfect surfaces and items.
- Wash clothing that may be soiled with stool with soap and chlorine bleach.
- If you visit someone in a health care facility, wash your hands before, during, and after your visit.
- Do not use antibiotics unless your doctor recommends them.
If you have a clostridium difficile infection, wash your hands with soap and water before eating and after using the restroom. Use a chlorine bleach-based product to clean surfaces you may have touched to avoid spreading the infection to others.
Tests of your stool can diagnose clostridium difficile. Sometimes you might also need imaging tests, to check for complications. Certain antibiotics can treat clostridium difficile infection. Rarely, there are severe cases that need surgery.
In about 20% of patients, Clostridium difficile infection will resolve within 2-3 days of discontinuing the antibiotic to which the patient was previously exposed. Clostridium difficile infection can usually be treated with an appropriate course (about 10 days) of antibiotics, including metronidazole, vancomycin (administered orally), or recently approved fidaxomicin. You should improve after 72 hours of starting the medicine, although the diarrhea may continue. In about 15% to 35% of cases, a second round of antibiotics is needed. After treatment, repeat Clostridium difficile testing is not recommended if the patients’ symptoms have resolved, as patients may remain colonized.
Transplanting stool (fecal microbiota transplant) from a healthy person to the colon of a patient with repeat clostridium difficile infections has been shown to successfully treat clostridium difficile. These “fecal transplants” appear to be the most effective method for helping patients with repeat clostridium difficile infections. This procedure may not be widely available and its long term safety has not been established.
While you recover, drink plenty of fluids to replace what your body lost due to diarrhea. Avoid milk products and foods that contain wheat flour or are high in fiber. Your digestive tract may be sensitive to them for a few days.
What are the differences between Clostridium difficile colonization and Clostridium difficile infection?
Clostridium difficile colonization
- patient exhibits NO clinical symptoms
- patient tests positive for Clostridium difficile organism and/or its toxin
- more common than Clostridium difficile infection
Clostridium difficile infection
- patient exhibits clinical symptoms
- patient tests positive for the Clostridium difficile organism and/or its toxin
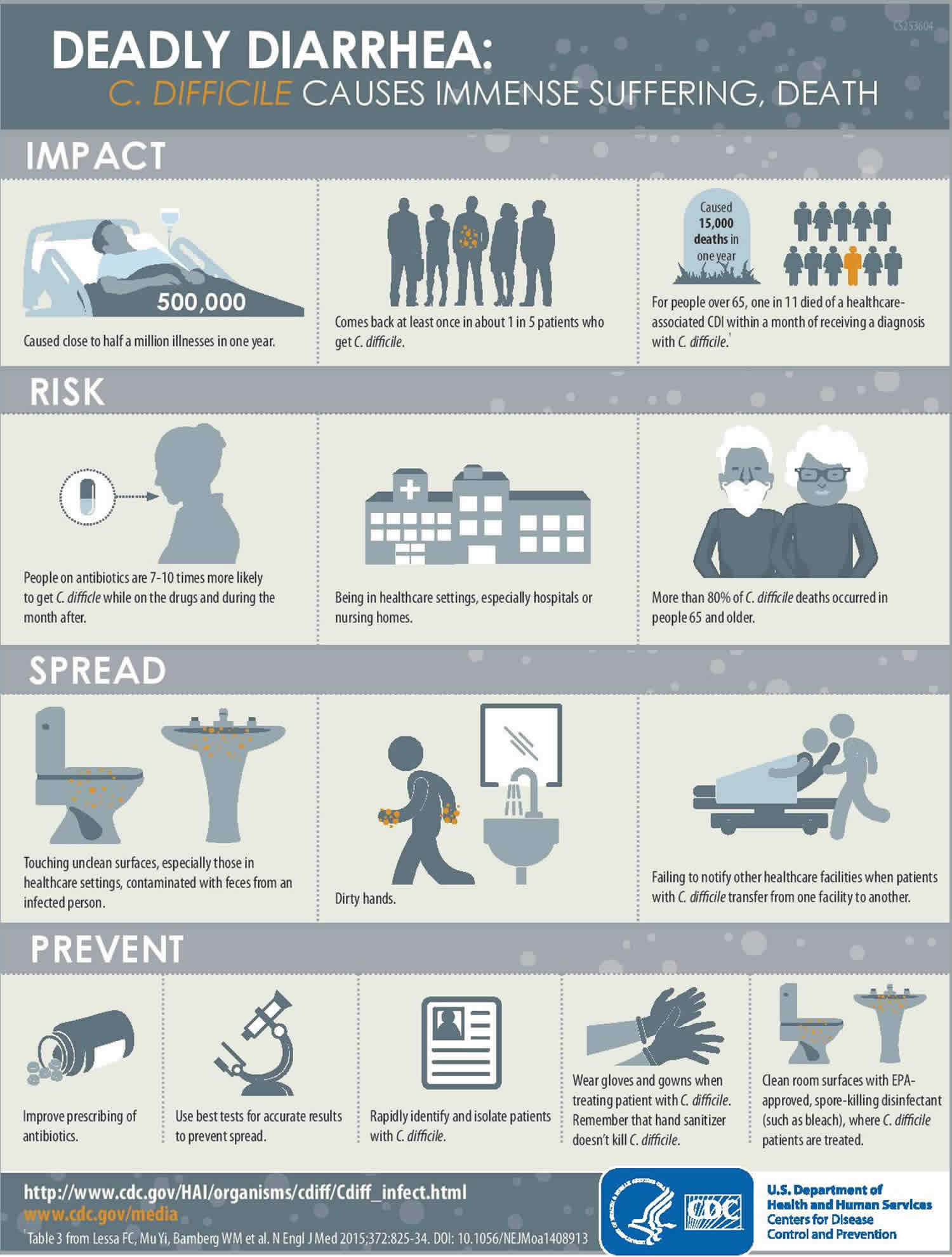
Patients with circulating antibodies to the toxins or individuals who mount a rapid and effective immunologic response during clostridium difficile infection are generally asymptomatic and do not exhibit clostridium difficile infection-associated symptoms 7. These patients often experience less severe clostridium difficile infection and a lower risk of recurrence. However, patients who fail to mount a robust immune response to the toxins develop symptoms of clostridium difficile infection such as diarrhea and colitis. Furthermore, patients who are able to restore their natural gut microbiota or mount an effective immune response to the toxins and/or the bacterium recover from the infection, whereas patients who fail to do so are susceptible to recurrent clostridium difficile infection 7. Given the importance of the immune system and the native gut microbiota in clearing clostridium difficile infection, therapies that are based on inhibiting either the clostridium difficile toxins A and B or cellular structures on the bacterium responsible for colonization, virulence, and restoration of the gut microbiota are the most important strategies to combat this multidrug-resistant pathogen 1.
Figure 2. Targets for Clostridium difficile infections
[Source 1 ]
Clostridium difficile transmission
Clostridium difficile is shed in feces. Any surface, device, or material (e.g., toilets, bathing tubs, and electronic rectal thermometers) that becomes contaminated with feces may serve as a reservoir for the Clostridium difficile spores. Clostridium difficile can live for long periods on surfaces. Clostridium difficile spores are transferred to patients mainly via the hands of healthcare personnel who have touched a contaminated surface or item.
People who have other illnesses or conditions requiring prolonged use of antibiotics, and the elderly, are at greater risk of acquiring clostridium difficile infection. Clostridium difficile bacteria are found in the feces. People can become infected if they touch items or surfaces that are contaminated with feces and then touch their mouth or mucous membranes.
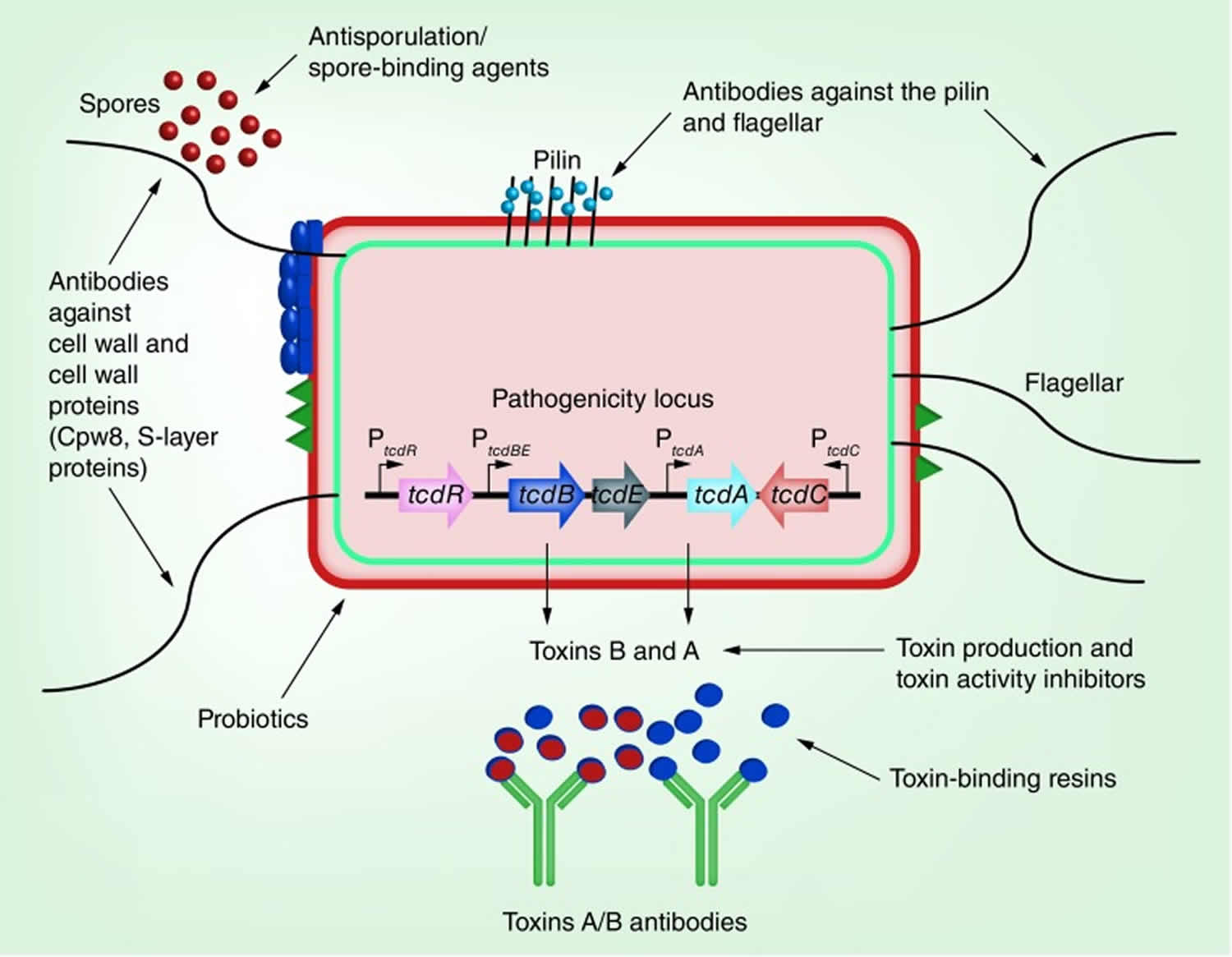
In the colon, clostridium difficile undergoes active binary division into oxygen-sensitive vegetative cells, which produce that produces two exotoxins: toxin A and toxin B and cause disease 1. To survive under aerobic conditions during dissemination from host to host, clostridium difficile forms oxygen-resistant spores (Figure 2). The vegetative cells must transform into spores in order to survive aerobic conditions and so the spores are generally acknowledged to initiate the infection process by serving as the disseminating form of this obligate anaerobic pathogen. Because only the vegetative cells can cause disease, germination of the spores into vegetative cells inside the gastrointestinal tract is critical in clostridium difficile pathogenesis.
Both toxins A and B have similar enzymatic cleavage activities 8 and are cytotoxic to cultured cells; however, toxin B is more potent than toxin A 9. During infection, the toxins are released into the colon, where they undergo internalization by the host cells through receptor-mediated endocytosis 10. The internalized toxins monoglucosylate low-molecular weight GTPases of the Rho family in the cytosol 11. This monoglucosylation interrupts the normal function of the GTPases leading to various deleterious effects including cell rounding, altered cellular signaling, actin cytoskeleton dysregulation and apoptosis 12. Intoxication of the cells by the toxins also induces the release of various immunomodulatory mediators from mast cells, epithelial cells and phagocytes resulting in inflammation and accumulation of neutrophils 13. Early detection of clostridium difficile during infection is critical to prevent further damage by the released toxins.
Figure 3. Clostridium difficile 2 life forms
Footnote: Clostridium difficile grows vegetatively by binary fission during favorable conditions and forms spores when effort to maintain vegetative growth fails. As an anaerobic pathogen, the spores serve as its disseminating agent from host to host and that germination in the gastrointestinal tract is critical for infection. Thus, drugs that inhibit sporulation and germination may help thwart the infection process.
[Source 1 ]Which patients are at increased risk for Clostridium difficile infection?
The risk for clostridium difficile infection increases in patients with:
- antibiotic exposure
- proton pump inhibitors
- gastrointestinal surgery/manipulation
- long length of stay in healthcare settings
- a serious underlying illness
- immunocompromising conditions
- advanced age
Clostridium difficile symptoms
Some people carry the bacterium clostridium difficile in their intestines but never become sick, though they may still spread the infection. Signs and symptoms usually develop within five to 10 days after starting a course of antibiotics, but may occur as soon as the first day or up to two months later.
Mild to moderate clostridium difficile infection
The most common symptoms of mild to moderate clostridium difficile infection are:
- Watery diarrhea three or more times a day for two or more days
- Mild abdominal cramping and tenderness
Severe clostridium difficile infection
In severe cases, people tend to become dehydrated and may need hospitalization. clostridium difficile causes the colon to become inflamed (colitis) and sometimes may form patches of raw tissue that can bleed or produce pus (pseudomembranous colitis). Signs and symptoms of severe infection include:
- Watery diarrhea 10 to 15 times a day
- Abdominal cramping and pain, which may be severe
- Rapid heart rate
- Fever
- Blood or pus in your stool.
- Nausea
- Dehydration
- Loss of appetite
- Weight loss
- Swollen abdomen
- Kidney failure
- Increased white blood cell count
- Low-grade fever of up to 101°F (38 °C) in children or 100°F to 102°F (37.8 to 38.9 °C) in adults
Clostridium difficile complications
Complications of clostridium difficile infections include:
- Dehydration. Severe diarrhea can lead to a significant loss of fluids and electrolytes. This makes it difficult for your body to function normally and can cause blood pressure to drop to dangerously low levels.
- Kidney failure. In some cases, dehydration can occur so quickly that kidney function rapidly deteriorates (kidney failure).
- Toxic megacolon. In this rare condition, your colon is unable to expel gas and stool, causing it to become greatly distended (megacolon). Left untreated, your colon may rupture, causing bacteria from the colon to enter your abdominal cavity. An enlarged or ruptured colon requires emergency surgery and may be fatal.
- A hole in your large intestine (bowel perforation). This is rare and results from extensive damage to the lining of your large intestine or after toxic megacolon. A perforated bowel can spill bacteria from the intestine into your abdominal cavity, leading to a life-threatening infection (peritonitis).
- Sepsis (septicemia).
- Death. Even mild to moderate clostridium difficile infections can quickly progress to a fatal disease if not treated promptly.
Clostridium difficile colitis
Clostridium difficile colitis also called pseudomembranous colitis or antibiotic-associated colitis, is inflammation of the colon associated with an overgrowth of the bacterium clostridium difficile. This overgrowth of clostridium difficile is most often related to recent antibiotic use.
Clostridium difficile colitis symptoms
Signs and symptoms of pseudomembranous colitis may include:
- Diarrhea that can be watery or even bloody
- Abdominal cramps, pain or tenderness
- Fever
- Pus or mucus in your stool
- Nausea
- Dehydration
Symptoms of clostridium difficile colitis can begin as soon as one to two days after you start taking an antibiotic, or as long as several weeks after you finish taking the antibiotic.
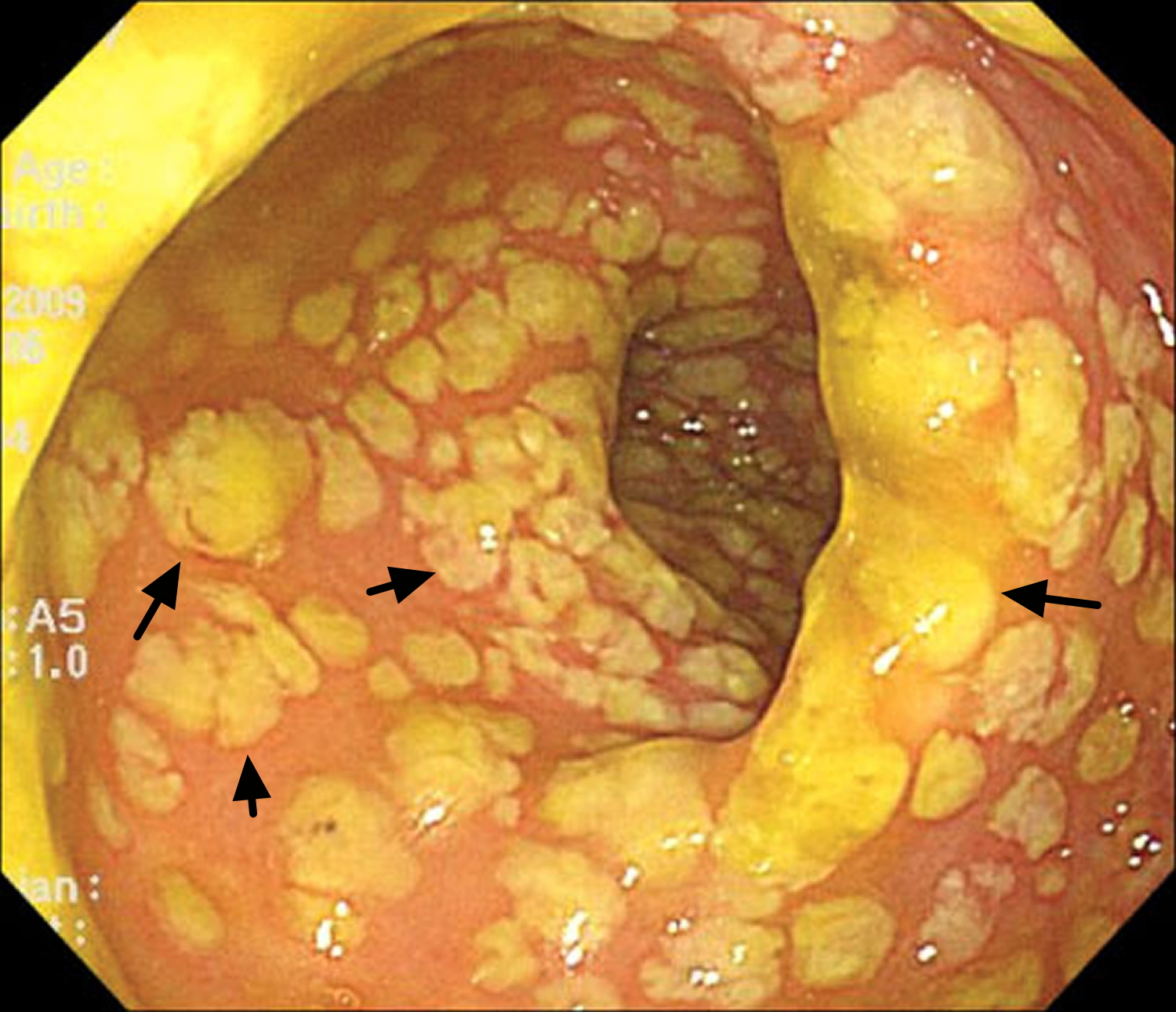
Figure 4. Pseudomembranous colitis – flexible sigmoidoscopy showing diffuse pseudomembranes covering severely edematous and friable mucosa in the rectosigmoid colon in a patient with Clostridium difficile infection.
Clostridium difficile colitis causes
Usually, your body keeps the many bacteria in your colon in a naturally healthy balance. However, antibiotics and other medications can upset this balance. Clostridium difficile colitis occurs when certain bacteria — usually clostridium difficile — rapidly outgrow other bacteria that normally keep them in check. Certain toxins produced by clostridium difficile, which are usually present in only tiny amounts, rise to levels high enough to damage the colon.
While almost any antibiotic can cause pseudomembranous colitis, some antibiotics are more likely to cause pseudomembranous colitis than others:
- Fluoroquinolones, such as ciprofloxacin (Cipro) and levofloxacin (Levaquin)
- Penicillins, such as amoxicillin and ampicillin
- Clindamycin (Cleocin)
- Cephalosporins, such as cefixime (Suprax)
Other causes
Other medications besides antibiotics can sometimes cause pseudomembranous colitis. Chemotherapy drugs that are used to treat cancer may disrupt the normal balance of bacteria in the colon.
Certain diseases that affect the colon, such as ulcerative colitis or Crohn’s disease, may also predispose people to pseudomembranous colitis.
Clostridium difficile spores are resistant to many common disinfectants and can be transmitted from the hands of health care professionals to patients. Increasingly, clostridium difficile has been reported in people with no known risk factors, including people with no recent health care contact or use of antibiotics. This is called community-acquired clostridium difficile.
Risk factors for getting clostridium difficile colitis
Factors that may increase your risk of pseudomembranous colitis include:
- Taking antibiotics
- Staying in the hospital or a nursing home
- Increasing age, especially over 65 years
- Having a weakened immune system
- Having a colon disease, such as inflammatory bowel disease or colorectal cancer
- Undergoing intestinal surgery
- Receiving chemotherapy treatment for cancer
Clostridium difficile colitis complications
Treatment of pseudomembranous colitis is usually successful. However, even with prompt diagnosis and treatment, pseudomembranous colitis can be life-threatening. Possible complications include:
- Abnormally low levels of potassium in your blood (hypokalemia), due to the loss of potassium during excessive diarrhea
- Dehydration leading to abnormally low blood pressure (hypotension), related to significant loss of fluids and electrolytes due to diarrhea
- Kidney failure, due to severe dehydration resulting from diarrhea
- A hole in your bowel (perforated colon), which can lead to an infection of your abdominal cavity
- Toxic megacolon, a rare but serious swelling of the colon, leaving it incapable of expelling gas and stool, which could cause your colon to rupture
In addition, pseudomembranous colitis may sometimes return, days or even weeks after apparently successful treatment.
Clostridium difficile colitis diagnosis
Tests and procedures used to diagnose pseudomembranous colitis and to search for complications include:
- Stool sample. There are a number of different stool sample tests used to detect clostridium difficile infection of the colon.
- Blood tests. These may reveal an abnormally high white blood cell count (leukocytosis), which may indicate pseudomembranous colitis.
- Colonoscopy or sigmoidoscopy. In both of these tests, your doctor uses a tube with a miniature camera at its tip to examine the inside of your colon for signs of pseudomembranous colitis — raised, yellow plaques (lesions), as well as swelling.
- Imaging tests. If you have severe symptoms, your doctor may obtain an abdominal X-ray or an abdominal CT scan to look for complications such as toxic megacolon or colon rupture.
Clostridium difficile colitis treatment
Treatment strategies include:
- Stopping the antibiotic or other medication that’s thought to be causing your signs and symptoms, if possible. Sometimes, this may be enough to resolve your condition or at least ease signs, such as diarrhea.
- Starting an antibiotic likely to be effective against clostridium difficile. If you still experience signs and symptoms, your doctor may use a different antibiotic to treat clostridium difficile. This allows the normal bacteria to grow back, restoring the healthy balance of bacteria in your colon. You may be given antibiotics by mouth, through a vein or through a tube inserted through the nose into the stomach (nasogastric tube). Depending on your condition, doctors will use most often use metronidazole (Flagyl), vancomycin, fidaxomicin (Dificid) or a combination.
- Having fecal microbial transplantation (FMT). If your condition is extremely severe, you may be given a transplant of stool (fecal transplant) from a healthy donor to restore the balance of bacteria in your colon. The donor stool may be delivered through a nasogastric tube, inserted into the colon or placed in a capsule you swallow. Often, doctors will use a combination of antibiotic treatment followed by fecal microbiota transplant.
Once you begin treatment for pseudomembranous colitis, signs and symptoms may begin to improve within a few days.
Researchers are exploring new treatments for pseudomembranous colitis, including alternative antibiotics and a vaccine.
Home remedies
Some research suggests that concentrated supplements of good bacteria and yeasts (probiotics) can help prevent clostridium difficile infection, but more studies are needed for their use in treating recurrences. They are safe to use and available in capsule or liquid form without a prescription.
To cope with the diarrhea and dehydration that can occur with pseudomembranous colitis, try to:
- Drink plenty of fluids. Water is best, but fluids with added sodium and potassium (electrolytes) also may be beneficial. Avoid beverages that are high in sugar or contain alcohol or caffeine, such as coffee, tea and colas, which can aggravate your symptoms.
- Choose soft, easy-to-digest foods. These include applesauce, bananas and rice. Avoid high-fiber foods, such as beans, nuts and vegetables. If you feel your symptoms are improving, slowly add high-fiber foods back to your diet.
- Eat several small meals, rather than a few large meals. Space the smaller meals throughout the day.
- Avoid irritating foods. Stay away from spicy, fatty or fried foods, and any other foods that make your symptoms worse.
Treating recurring pseudomembranous colitis
The natural occurrence of new, more-aggressive strains of clostridium difficile, which are more resistant to antibiotics, has made treating pseudomembranous colitis increasingly difficult and recurrences more common. With each recurrence, your chance of having an additional recurrence increases. Treatment options may include:
- Repeat antibiotics. You may need a second or third round of antibiotics to resolve your condition.
- Surgery. Surgery may be an option in people who have progressive organ failure, rupture of the colon and inflammation of the lining of the abdominal wall (peritonitis). Surgery has typically involved removing all or part of the colon (total or subtotal colectomy). A newer surgery that involves laparoscopically creating a loop of colon and cleaning it (diverting loop ileostomy and colonic lavage) is less invasive and has had positive results.
- Fecal microbial transplantation (FMT). Fecal microbiota transplant is used to treat recurrent pseudomembranous colitis. You’ll receive healthy, cleaned stool in a capsule, nasogastrically or inserted into your colon.
Clostridium difficile infection causes
Clostridium difficile bacteria are found throughout the environment — in soil, air, water, human and animal feces, and food products, such as processed meats. A small number of healthy people naturally carry the bacteria in their large intestine and don’t have ill effects from the infection.
Clostridium difficile infection is most commonly associated with health care and recent antibiotic use, occurring in hospitals and other health care facilities where a much higher percentage of people carry the bacteria. However, studies show increasing rates of community-associated clostridium difficile infection, which occurs among populations traditionally not considered high risk, such as children and people without a history of antibiotic use or recent hospitalization.
Spores from clostridium difficile bacteria are passed in feces and spread to food, surfaces and objects when people who are infected don’t wash their hands thoroughly. These spores can persist in a room for weeks or months. If you touch a surface contaminated with clostridium difficile spores, you may then unknowingly swallow the bacteria.
Your intestines contain about 100 trillion bacterial cells and up to 2,000 different kinds of bacteria, many of which help protect your body from infection. When you take an antibiotic to treat an infection, these drugs tend to destroy some of the normal, helpful bacteria in addition to the bacteria causing the infection. Without enough healthy bacteria to keep it in check, clostridium difficile can quickly grow out of control. The antibiotics that most often lead to clostridium difficile infections include fluoroquinolones, cephalosporins, penicillins and clindamycin.
Once established, clostridium difficile can produce toxins that attack the lining of the intestine. The toxins destroy cells and produce patches (plaques) of inflammatory cells and decaying cellular debris inside the colon and cause watery diarrhea.
Emergence of a new strain
An aggressive strain of clostridium difficile has emerged that produces far more toxins than other strains do. The new strain may be more resistant to certain medications and has shown up in people who haven’t been in the hospital or taken antibiotics. This strain of clostridium difficile has caused several outbreaks of illness since 2000. The new emergence of the current epidemic strain of clostridium difficile, known by its names assigned by various typing schemes as restriction enzyme analysis type BI, North American Pulsed Field type 1 (NAP1), or PCR ribotype 027. BI/NAP1/027 has spread widely after first being found responsible for outbreaks in Pittsburgh (2000), Atlanta (2001-2), and Montreal (2003) 14. This strain appears more virulent possibly due to its increased production of toxins A and B and its production of an additional toxin known as binary toxin, as well as other factors still under study. In addition to being more virulent, it is more resistant to a commonly-used class of antimicrobials known as the fluoroquinolones 14.
Like other strains of clostridium difficile, BI/NAP1/027 can be detected in the stool of infected patients by using laboratory tests that are commonly available in most hospitals. However, none of the FDA-approved tests differentiate between the various strains of clostridium difficile. Fortunately, because the control measures for outbreaks of any strain of clostridium difficile are similar, identification of the specific strain is not imperative for controlling outbreaks.
Risk factors for clostridium difficile infection
Although people — including children — with no known risk factors have gotten sick from clostridium difficile, certain factors increase your risk.
Taking antibiotics or other medications
Medication-associated risk factors include:
- Currently taking or having recently taken antibiotics
- Taking broad-spectrum antibiotics that target a wide range of bacteria
- Using multiple antibiotics
- Taking antibiotics for a long time
- Taking medications to reduce stomach acid, including proton pump inhibitors
Staying in a health care facility
The majority of clostridium difficile cases occur in, or after exposure to, health care settings — including hospitals, nursing homes and long-term care facilities — where germs spread easily, antibiotic use is common and people are especially vulnerable to infection. In hospitals and nursing homes, clostridium difficile spreads mainly on hands from person to person, but also on cart handles, bedrails, bedside tables, toilets, sinks, stethoscopes, thermometers — even telephones and remote controls.
Having a serious illness or medical procedure
If you have a serious illness, such as inflammatory bowel disease or colorectal cancer, or a weakened immune system as a result of a medical condition or treatment (such as chemotherapy), you’re more susceptible to a clostridium difficile infection. Your risk of clostridium difficile infection is also greater if you’ve had abdominal surgery or a gastrointestinal procedure.
Older age is also a risk factor for clostridium difficile infection. In one study, the risk of becoming infected with clostridium difficile was 10 times greater for people age 65 and older compared with younger people.
After having a previous clostridium difficile infection, your chances of having a recurring infection can be up to 20 percent, and the risk increases further with every subsequent infection.
Clostridium difficile prevention
To help prevent the spread of clostridium difficile, hospitals and other health care facilities follow strict infection-control guidelines. If you have a friend or family member in a hospital or nursing home, don’t be afraid to remind caregivers to follow the recommended precautions.
Preventive measures include:
- Hand-washing. Health care workers should practice good hand hygiene before and after treating each person in their care. In the event of a clostridium difficile outbreak, using soap and warm water is a better choice for hand hygiene, because alcohol-based hand sanitizers do not effectively destroy clostridium difficile spores. Visitors also should wash their hands with soap and warm water before and after leaving the room or using the bathroom.
- Contact precautions. People who are hospitalized with clostridium difficile have a private room or share a room with someone who has the same illness. Hospital staff and visitors wear disposable gloves and isolation gowns while in the room.
- Thorough cleaning. In any setting, all surfaces should be carefully disinfected with a product that contains chlorine bleach. clostridium difficile spores can survive routine cleaning products that don’t contain bleach.
- Avoid unnecessary use of antibiotics. Antibiotics are sometimes prescribed for viral illnesses that aren’t helped by these drugs. Take a wait-and-see attitude with simple ailments. If you do need an antibiotic, ask your doctor to prescribe one that has a narrow range and that you take for the shortest time possible.
How to stop clostridium difficile spreading
Clostridium difficile infections can be passed on very easily. You can reduce your risk of picking it up or spreading it by practising good hygiene, both at home and in healthcare settings.
The following measures can help:
- stay at home until at least 48 hours after your symptoms have cleared up
- wash your hands regularly with soap and water, particularly after going to the toilet and before eating – use liquid rather than bar soap and don’t use flannels or nail brushes
- clean contaminated surfaces – such as the toilet, flush handle, light switches and door handles – with a bleach-based cleaner after each use
- don’t share towels and flannels
- wash contaminated clothes and sheets separately from other washing at the highest possible temperature
- when visiting someone in hospital, observe any visiting guidelines, avoid taking any children under the age of 12, and wash your hands with liquid soap and
- water when entering and leaving ward areas – don’t rely on alcohol hand gels, as they’re not effective against clostridium difficile
- avoid visiting hospital if you’re feeling unwell or have recently had diarrhoea
Clostridium difficile infection prevention in hospitals and other healthcare settings
- Use antibiotics judiciously
- Use Contact Precautions: for patients with known or suspected Clostridium difficile infection:
- Place these patients in private rooms. If private rooms are not available, these patients can be placed in rooms (cohorted) with other patients with
- Clostridium difficile infection.
- Use gloves when entering patients’ rooms and during patient care.
- Perform Hand Hygiene after removing gloves.
- Because alcohol does not kill Clostridium difficile spores, use of soap and water is more efficacious than alcohol-based hand rubs. However, early experimental data suggest that, even using soap and water, the removal of C. difficile spores is more challenging than the removal or inactivation of other common pathogens.
- Preventing contamination of the hands via glove use remains the cornerstone for preventing Clostridium difficile transmission via the hands of healthcare workers; any theoretical benefit from instituting soap and water must be balanced against the potential for decreased compliance resulting from a more complex hand hygiene message.
- If your institution experiences an outbreak, consider using only soap and water for hand hygiene when caring for patients with Clostridium difficile infection.
- Use gowns when entering patients’ rooms and during patient care.
- Dedicate or perform cleaning of any shared medical equipment.
- Continue these precautions until diarrhea ceases.
- Because Clostridium difficile-infected patients continue to shed organism for a number of days following cessation of diarrhea, some institutions routinely continue isolation for either several days beyond symptom resolution or until discharge, depending upon the type of setting and average length of stay.
- Implement an environmental cleaning and disinfection strategy:
- Ensure adequate cleaning and disinfection of environmental surfaces and reusable devices, especially items likely to be contaminated with feces and surfaces that are touched frequently.
- Consider using an Environmental Protection Agency (EPA)-registered disinfectant with a sporicidal claim for environmental surface disinfection after cleaning in accordance with label instructions; generic sources of hypochlorite (e.g., household chlorine bleach) also may be appropriately diluted and used. (Note: Standard EPA-registered hospital disinfectants are not effective against Clostridium difficile spores .) Hypochlorite-based disinfectants may be most effective in preventing Clostridium difficile transmission in units with high endemic rates of Clostridium difficile infection.
- Follow the manufacturer’s instructions for disinfection of endoscopes and other devices.
- Recommended infection control practices in long term care and home health settings are similar to those practices taken in traditional health-care settings.
- Routine cleaning should be performed prior to disinfection. EPA-registered disinfectants with a sporicidal claim have been used with success for environmental surface disinfection in those patient-care areas where surveillance and epidemiology indicate ongoing transmission of Clostridium difficile.
Note: EPA-registered disinfectants are recommended for use in patient-care areas. When choosing a disinfectant, check product labels for inactivation claims, indications for use, and instructions.
Clostridium difficile test
Testing for clostridium difficile is unnecessary if you’re not having diarrhea or watery stools, and is not helpful for follow-up treatment.
Doctors often suspect clostridium difficile in anyone with diarrhea who has taken antibiotics within the past two months or when diarrhea develops a few days after hospitalization. In such cases, you’re likely to have one or more of the following tests:
- Stool culture for Clostridium difficile: While this is the most sensitive test available, it is the one most often associated with false-positive results due to presence nontoxigenic Clostridium difficile strains. However, this can be overcome by testing isolates for toxin production (i.e. so called “toxigenic culture”). Nonetheless, stool cultures for Clostridium difficile are labor intensive, require an appropriate culture environment to grow anaerobic microorganisms, and have a relatively slow turn-around time (i.e. results available in 48-96 hours) making them overall less clinically useful. Results of toxigenic cultures do serve as a gold-standard against which other test modalities are compared in clinical trials of performance.
- Molecular tests: FDA-approved PCR assays, which test for the gene encoding toxin B, are highly sensitive and specific for the presence of a toxin-producing Clostridium difficile organism.
- Antigen detection for Clostridium difficile: These are rapid tests (<1 hr) that detect the presence of Clostridium difficile antigen by latex agglutination or immunochromatographic assays. Because results of antigen testing alone are non-specific, antigen assays have been employed in combination with tests for toxin detection, PCR, or toxigenic culture in two-step testing algorithms.
- Toxin testing for Clostridium difficile:
- Tissue culture cytotoxicity assay detects toxin B only. This assay requires technical expertise to perform, is costly, and requires 24-48 hr for a final result. It does provide specific and sensitive results for Clostridium difficile infection. While it served as a historical gold standard for diagnosing clinical significant disease caused by Clostridium difficile, it is recognized as less sensitive than PCR or toxigenic culture for detecting the organism in patients with diarrhea.
- Enzyme immunoassay detects toxin A, toxin B, or both A and B. Due to concerns overtoxin A-negative, B-positive strains causing disease, most laboratories employ a toxin B-only or A and B assay. Because these are same-day assays that are relatively inexpensive and easy to perform, they are popular with clinical laboratories. However, there are increasing concerns about their relative insensitivity (less than tissue culture cytotoxicity and much less than PCR or toxigenic culture).
- Clostridium difficile toxin is very unstable. The toxin degrades at room temperature and may be undetectable within 2 hours after collection of a stool specimen. False-negative results occur when specimens are not promptly tested or kept refrigerated until testing can be done.
Colon examination
In rare instances, to help confirm a diagnosis of clostridium difficile infection and look for alternatives, your doctor may examine the inside of your colon. This test (flexible sigmoidoscopy or colonoscopy) involves inserting a flexible tube with a small camera on one end into your colon to look for areas of inflammation and pseudomembranes.
Imaging tests
If your doctor is concerned about possible complications of clostridium difficile, he or she may order an abdominal X-ray or a computerized tomography (CT) scan, which provides images of your colon. The scan can detect the presence of complications such as thickening of the colon wall, expanding of the bowel, or more rarely, a hole (perforation) in the lining of your colon.
Clostridium difficile guidelines
A panel of experts was convened by the Infectious Diseases Society of America and Society for Healthcare Epidemiology of America to update the 2010 clinical practice guideline on Clostridium difficile infection in adults. The update, which has incorporated recommendations for children (following the adult recommendations for epidemiology, diagnosis, and treatment), includes significant changes in the management of this infection and reflects the evolving controversy over best methods for diagnosis. For the updated Clostridium difficile guidelines produced by the Infectious Diseases Society of America please go here (https://www.idsociety.org/practice-guideline/clostridium-difficile/) or here https://academic.oup.com/cid/article/66/7/e1/4855916
Clostridium difficile treatment
The usual treatment for clostridium difficile infection includes, if possible, stopping antibiotics being given for other purposes and/or treatment with metronidazole or vancomycin. In order to reduce selective pressure for vancomycin resistance in enterococci, current guidelines recommend the first-line use of metronidazole over vancomycin.
For mild to moderate infection, doctors usually prescribe metronidazole (Flagyl), taken by mouth. Metronidazole is not approved by the FDA for clostridium difficile infection, but has been shown to be effective in mild to moderate infection. Side effects of metronidazole include nausea and a bitter taste in your mouth.
For more severe and recurrent cases, vancomycin (Vancocin), also taken by mouth, may be prescribed.
Another oral antibiotic, fidaxomicin (Dificid), has been approved to treat clostridium difficile. In one study, the recurrence rate of clostridium difficile in people who took fidaxomicin was lower than among those who took vancomycin. However, fidaxomicin costs considerably more than metronidazole and vancomycin. Common side effects of vancomycin and fidaxomicin include abdominal pain and nausea.
Supportive treatment for diarrhea includes:
- Drink plenty of fluids. Choose fluids containing water, salt and sugar, such as diluted fruit juice, soft drinks and broths.
- Good nutrition. If you have watery diarrhea, eat starchy foods, such as potatoes, noodles, rice, wheat and oatmeal. Other good choices are saltine crackers, bananas, soup and boiled vegetables. If you aren’t hungry, you may need a liquid diet at first. After your diarrhea clears up, you may have temporary difficulty digesting milk and milk-based products.
- Take acetaminophen (paracetamol) for tummy pain or a fever
- Don’t take anti-diarrheal medication, as this can stop the infection being cleared from your body
- Regularly wash your hands and contaminated surfaces, objects or sheets
- Stay at home until at least 48 hours after your last episode of diarrhea
Surgery
For people with severe pain, organ failure, toxic megacolon or inflammation of the lining of the abdominal wall, surgery to remove the diseased portion of the colon may be the only option.
Recent reports suggest that BI/NAP1/027 may not respond as well to treatment with metronidazole despite the absence of laboratory evidence of metronidazole resistance. Evidence suggests that more severe disease should be treated with vancomycin, over metronidazole.
How does fluoroquinolone resistance affect management of BI/NAP1/027?
Increased fluoroquinolone resistance does not affect the management of infections caused by this strain. Fluoroquinolones have never been recommended for treatment of clostridium difficile infection and susceptibility testing is performed only as a part of an epidemiological investigation. However, resistance to fluoroquinolones may provide the new strain with an advantage over susceptible strains to spread within healthcare facilities where these antibiotics are commonly used.
Recurrent clostridium difficile infection
Up to 20 percent of people with clostridium difficile get sick again, either because the initial infection never went away or because they’re reinfected with a different strain of the bacteria. But after two or more recurrences, rates of further recurrence increase up to 65 percent.
Your risk of recurrence is higher if you:
- Are older than 65
- Are taking other antibiotics for a different condition while being treated with antibiotics for clostridium difficile infection
- Have a severe underlying medical disorder, such as chronic kidney failure, inflammatory bowel disease or chronic liver disease
Treatment for recurrent clostridium difficile infection may include:
- Antibiotics. Antibiotic therapy for recurrence may involve one or more courses of a medication (typically vancomycin), a gradually tapered dose of medication or an antibiotic given once every few days, a method known as a pulsed regimen. The effectiveness of antibiotic therapy declines with each subsequent recurrence.
- Fecal microbiota transplant (FMT). Also known as a stool transplant, fecal microbiota transplant is emerging as an alternative strategy for treating recurrent clostridium difficile infections. Though not yet approved by the FDA, clinical studies of fecal microbiota transplant are currently underway. Fecal microbiota transplant restores healthy intestinal bacteria by placing another person’s (donor’s) stool in your colon, using a colonoscope or nasogastric tube. Donors are screened for medical conditions, their blood is tested for infections, and stools are carefully screened for parasites, viruses and other infectious bacteria before being used for fecal microbiota transplant. Research has shown fecal microbiota transplant has a success rate higher than 90 percent for treating clostridium difficile infections.
- Probiotics. Probiotics are organisms, such as bacteria and yeast, which help restore a healthy balance to the intestinal tract. A yeast called Saccharomyces boulardii, in conjunction with antibiotics, might help prevent further recurrent clostridium difficile infections.
- Darkoh C, Deaton M, DuPont HL. Nonantimicrobial drug targets for Clostridium difficile infections. Future Microbiol. 2017;12(11):975-985. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5618939/[↩][↩][↩][↩][↩][↩]
- Elliott B, Chang BJ, Golledge CL, Riley TV. Clostridium difficile-associated diarrhoea. Intern. Med. J. 2007;37(8):561–568.[↩]
- Bartlett JG, Perl TM. The new Clostridium difficile – what does it mean? N. Engl. J. Med. 2005;353(23):2503–2505[↩]
- Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile infection in the United States. N. Engl. J. Med. 2015;372(9):825–834. https://www.nejm.org/doi/full/10.1056/NEJMoa1408913[↩]
- Davies KA, Longshaw CM, Davis GL, et al. Underdiagnosis of Clostridium difficile across Europe: the European, multicentre, prospective, biannual, point-prevalence study of Clostridium difficile infection in hospitalised patients with diarrhoea (EUCLID) Lancet Infect. Dis. 2014;14(12):1208–1219[↩]
- Dubberke ER, Olsen MA. Burden of Clostridium difficile on the healthcare system. Clin. Infect. Dis. 2012;55(Suppl. 2):S88–S92.[↩]
- Leffler DA, Lamont JT. Clostridium difficile infection. N. Engl. J. Med. 2015;372(16):1539–1548.[↩][↩]
- Dillon ST, Rubin EJ, Yakubovich M, et al. Involvement of Ras-related Rho proteins in the mechanisms of action of Clostridium difficile toxin A and toxin B. Infect. Immun. 1995;63(4):1421–1426.[↩]
- Voth DE, Ballard JD. Clostridium difficile toxins: mechanism of action and role in disease. Clin. Microbiol. Rev. 2005;18(2):247–263[↩]
- Ho JG, Greco A, Rupnik M, Ng KK. Crystal structure of receptor-binding C-terminal repeats from Clostridium difficile toxin A. Proc. Natl Acad. Sci. USA. 2005;102(51):18373–18378.[↩]
- Just I, Gerhard R. Large clostridial cytotoxins. Rev. Physiol. Biochem. Pharmacol. 2004;152:23–47.[↩]
- Huelsenbeck SC, May M, Schmidt G, Genth H. Inhibition of cytokinesis by Clostridium difficile toxin B and cytotoxic necrotizing factors – reinforcing the critical role of RhoA in cytokinesis. Cell Motil. Cytoskeleton. 2009;66(11):967–975[↩]
- Thelestam M, Chaves-Olarte E. Cytotoxic effects of the Clostridium difficile toxins. Curr. Top. Microbiol. Immunol. 2000;250:85–96.[↩]
- Gould CV, McDonald LC. Bench-to-bedside review: Clostridium difficile colitis. Crit Care. 2008;12(1):203. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2374604/[↩][↩]





{kind=link}