
What is Coombs test
Coombs test is also called antiglobulin test, is performed to detect either red blood cell-directed IgG in plasma or IgG or complement coating on the surface of circulating red blood cells. Neither of these molecules can cause direct agglutination of red blood cells, so, to detect their presence, monoclonal antihuman globulin with specificity for IgG or various complement proteins is added to a suspension of red blood cells. The antihuman globulin reagent is sufficiently large to cause agglutination of red blood cells that are coated with IgG or complement. Figure 1 illustrates the steps of the direct antiglobulin test (direct Coombs test), which detects in vivo binding of either IgG or complement to erythrocyte antigens, and the indirect antiglobulin test (indirect Coombs test), which detects serum antibodies that bind to erythrocytes during an incubation step.
Coombs test is named for Robin Coombs, who first developed the technique of using antibodies that are targeted against other antibodies (antiglobulin test) in 1945.
Figure 1. Coombs test
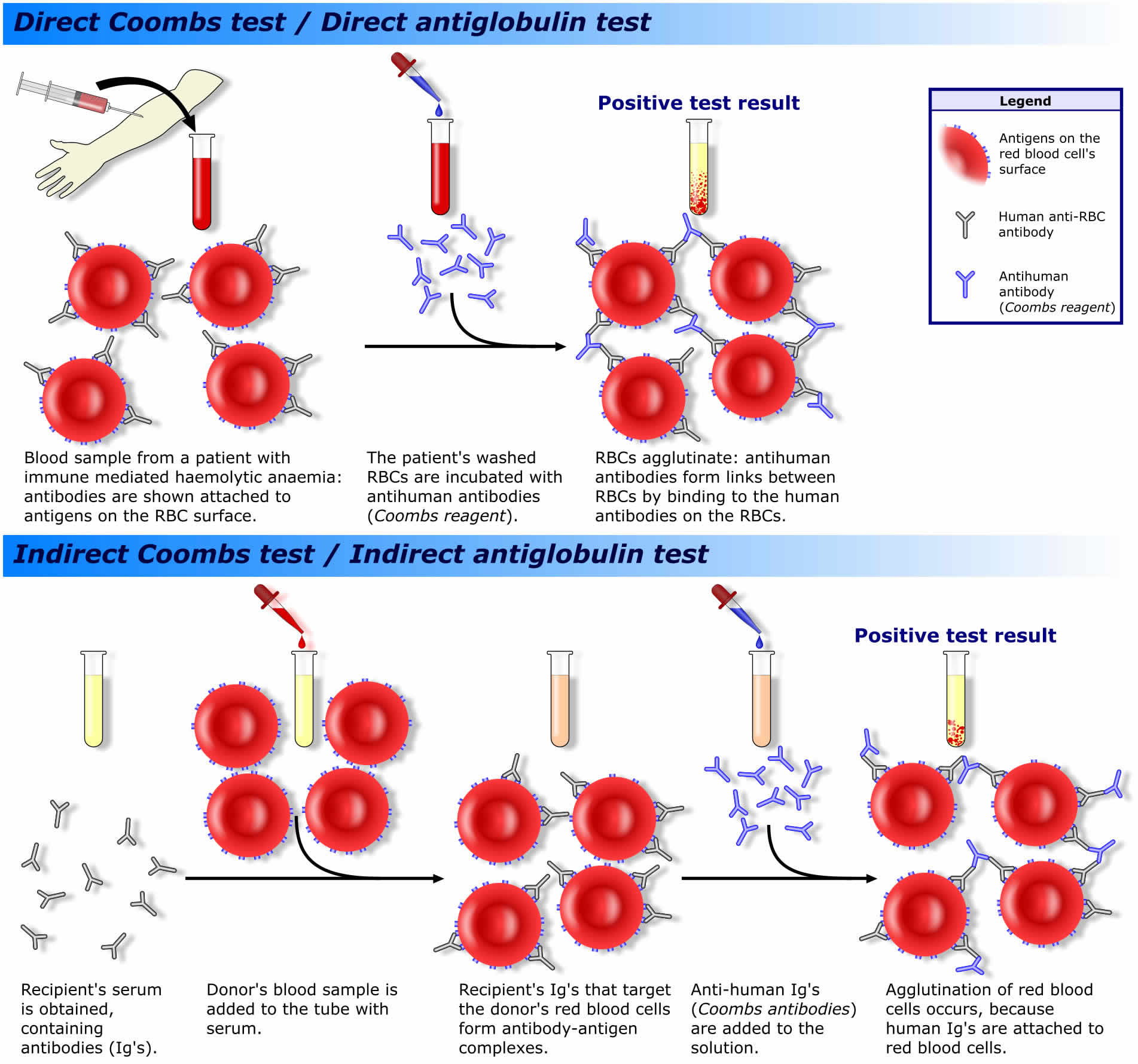
Footnote: The direct antiglobulin test (DAT) and indirect antiglobulin test (IAT). AHG = antihuman globulin. A) Direct Coombs test (direct antiglobulin test [DAT]) the red blood cells (erythrocytes) are washed to remove any unbound antibodies, and anti-IgG antihuman globulin reagent is then added. IgG antibodies cannot cause direct erythrocyte agglutination, but if the erythrocytes are coated with IgG antibodies, the antihuman globulin reagent will cause them to agglutinate. This test can also be performed using anti-complement antihuman globulin reagent. If IgG antibodies are present, they can be eluted off the erythrocytes for specificity determination. B) Indirect Coombs test (indirect antiglobulin test [IAT]) is used to detect the presence of IgG antibodies in serum (in vitro sensitization). Reagent erythrocytes are incubated in the presence of serum that potentially contains antibodies. If antibodies are present, they bind to their target antigens on the reagent erythrocytes. After the incubation period the erythrocytes are washed to remove unbound antibodies. Anti-IgG antihuman globulin reagent is added and will cause IgG-coated erythrocytes to agglutinate.
[Source 1 ]Direct Coombs test
The direct Coombs test (direct antiglobulin test [DAT]) looks for antibodies attached to red blood cells (RBCs) circulating in the bloodstream. The direct Coombs test (direct antiglobulin test [DAT]) may help to detect or identify conditions in which antibodies become attached to red blood cells (erythrocytes), causing them to break apart (hemolyze).
Red blood cells have structures on their surfaces called antigens. Each person has their own individual set of red blood cell antigens, determined by inheritance from their parents. The major antigens or surface identifiers on human red blood cells are the O, A, and B antigens, and a person’s blood is grouped into an A, B, AB, or O blood type according to the presence or absence of these antigens. Another important surface antigen is the D antigen in the Rh blood group system. If it is present on someone’s red blood cells, that person’s blood type is Rh+ (positive); if it is absent, the blood is type Rh- (negative). In addition, there are many other types of red blood cell antigens that make up lesser known but still clinically significant blood groups, such as Kell, Duffy, and Kidd.
There are a few reasons why antibodies may become attached to antigens on red blood cells:
- Autoimmune diseases and other conditions: Some people make antibodies directed against their own red blood cell antigens. These autoantibodies may be produced in autoimmune diseases and/or with some other conditions, such as lymphoma and chronic lymphocytic leukemia.
- Drug-induced anemia: Certain drugs can induce antibodies against red blood cell antigens and therefore cause hemolysis even without the presence of the drug. Sometimes, drugs may coat the surface of red blood cells, causing antibodies to react with the red blood cells. (This is relatively rare (about 1:1 million).) The drugs can induce antibodies to both the drug and the red blood cell itself, resulting in destruction of the red blood cell in the presence of drugs. This is seen with some antibiotics, such as IV penicillin, cephalosporins and pipercillin. Be sure to tell your healthcare provider about any drugs you have been taking recently. If the healthcare provider suspects drug-induced autoimmune anemia, the suspect medication will be discontinued. Symptoms typically resolve promptly after the drug is discontinued.
- Mother/baby blood type incompatibility: A baby may inherit antigens from its father that are not on its mother’s red blood cells. The mother may be exposed to the foreign antigens on her baby’s red blood cells during pregnancy or at delivery when some of the baby’s cells enter the mother’s circulation as the placenta separates. The mother may begin to produce antibodies against these foreign red blood cell antigens. This can cause hemolytic disease of the newborn, usually not affecting the first baby but affecting subsequent children when the mother’s antibodies cross the placenta, attach to the baby’s red blood cells, and hemolyze them. However, any baby may be affected by hemolytic disease of the newborn caused by antibodies to the ABO system. This generally is mild, which is fortunate, as it is the leading cause of maternal antibodies attaching to fetal red blood cells today. A mother will be screened for antibodies during pregnancy and again at delivery. A direct Coombs test (direct antiglobulin test [DAT]) performed on the blood of a baby born to an at-risk mother will determine if its mother’s antibodies have attached to the baby’s red blood cells.
- Following a blood transfusion: Before receiving a blood transfusion, a person’s ABO group and Rh type is matched with that of the donor blood to prevent a serious transfusion reaction from occurring. That is, the donor’s blood must be compatible with the ABO group and Rh type of the person receiving the blood so that the recipient’s antibodies do not react with and destroy the donor red blood cells. If someone receives a blood transfusion, their body may also recognize other red blood cell antigens that it does not have, such as those from other blood groups (such as the Kell or Kidd blood groups), as foreign. The recipient may produce antibodies and they may become attached to these foreign antigens on the donor red blood cells circulating in the bloodstream. People who have many transfusions are more likely to make antibodies to red blood cells because they are exposed to more foreign red blood cell antigens. If someone shows symptoms of a reaction after transfusion, a direct Coombs test (direct antiglobulin test [DAT]) will be performed to determine if those antibodies have attached to the transfused donor red blood cells.
The direct Coombs test (direct antiglobulin test [DAT]) is used primarily to help determine whether the cause of hemolytic anemia, a condition in which red blood cells (red blood cells) are destroyed more quickly than they can be replaced, is due to antibodies attached to red blood cells. This may occur in autoimmune-related hemolytic anemias, which are caused by a person producing antibodies against their own red blood cell antigens (autoantibodies). Examples of this include:
- Autoimmune disorders such as systemic lupus erythematosus
- Malignant diseases such as lymphoma and chronic lymphocytic leukemia
- Infections such as mycoplasma pneumonia and mononucleosis
- With the use of certain medications, such as penicillin
A direct Coombs test (direct antiglobulin test [DAT]) may also be used to help diagnose hemolytic disease of the newborn (HDN) due to an incompatibility between the blood types of a mother and baby. When a baby is born, the mother may be exposed to the foreign antigens on the baby’s red blood cells and may produce antibodies directed against the baby’s red blood cell antigens. This may occur when an Rh-positive baby is born to an Rh-negative mother. Formerly, antibodies to the Rh antigen were the most common cause of hemolytic disease of the newborn, but this condition is now rare due to preventive treatments given to the mother during and after each pregnancy. The most common cause of hemolytic disease of the newborn nowadays is an ABO incompatibility between a Group O mother and her baby. This type of fetal-maternal incompatibility is generally mild.
A direct Coombs test (direct antiglobulin test [DAT]) may also be used to investigate a suspected transfusion reaction. If a person being given blood develops a fever or other significant symptoms suggesting a potential for a hemolytic transfusion reaction, a DAT is done to determine if the person has made an antibody that has attached to the transfused red blood cells. If the antibody is found coating the red blood cells, then the red blood cells may be destroyed (hemolyzed) or be removed from circulation faster than normal.
When is direct Coombs test ordered?
The direct Coombs test may be ordered when someone has hemolytic anemia and the healthcare provider wants to determine the cause.
This test may be ordered when a newborn is born to an at-risk mother or exhibits signs of hemolytic disease of the newborn, in the absence of other causes of symptoms that may include:
- Pale appearance
- Jaundice, including elevated bilirubin
- Enlarged liver or spleen
- Swelling of the entire body
- Difficulty breathing
A direct Coombs test will be ordered when there are signs and symptoms of a blood transfusion reaction, such as:
- Fever, chills
- Back pain
- Bloody urine
Direct coombs test positive
A positive direct Coombs test means that there are antibodies attached to the red blood cells. In general, the stronger the direct Coombs test reaction (the more positive the test), the greater the amount of antibody bound to the red blood cells, but this does not always equate to the severity of symptoms, especially if the red blood cells have already been destroyed.
If a direct Coombs test is positive due to a transfusion reaction, an infection, or drug, it will remain positive for 48 hours to 3 months. If it is positive due to an autoimmune condition, it may be positive over a long period of time (chronically).
The direct Coombs test detects the presence of the antibody, but it does not tell the healthcare provider the cause or exact type of antibody or if it is causing the symptoms. A person’s medical history and a clinical examination is needed to determine if a positive direct Coombs test is due to a transfusion reaction, autoimmune reaction, an infection, a medication, or a baby-mother blood group incompatibility. A small percentage of the normal population will be direct Coombs test-positive and not experience hemolytic anemia.
Direct coombs test negative
A negative direct Coombs test means that antibodies are most likely not attached to red blood cells and the signs and symptoms are due to another cause that requires further investigation.
Indirect Coombs test
Indirect Coombs test finds anti-D antibodies in the mother’s serum. If these were to come into contact with fetal red blood cells they would hemolyze them and hence cause hemolytic disease of the newborn. By finding maternal anti-D before fetal red blood cells have been attacked, treatment can be given to prevent or limit the severity of hemolytic disease of the newborn.
For indirect Coombs test, the mother’s serum is incubated with Rh D-positive red blood cells. If any anti-D is present in the mother’s serum, they will bind to the Rh D-positive red blood cells. The Rh D-positive red blood cells are then washed to remove all free antibodies. When anti-Ig antibodies are added, they will agglutinate any red blood cells to which maternal antibodies are bound.
This is called the indirect Coombs test (indirect antiglobulin test [IAT]) because the anti-Ig finds “indirect” evidence of harmful maternal antibodies, requiring the addition of fetal red blood cells to show the capacity of maternal anti-D to bind to fetal red blood cells.
Coombs test in newborn
Direct Coombs test
Direct Coombs test is used in newborn to diagnose hemolytic disease of the newborn. Hemolytic disease of the newborn (HDN) used to be a major cause of fetal loss and death among newborn babies. It was not until the 1950s that the underlying cause of hemolytic disease of the newborn was clarified; namely, the newborn’s red blood cells (RBCs) are being attacked by antibodies (anti-D antibodies) from the mother. The attack begins while the baby is still in the womb and is caused by an incompatibility between the mother’s and baby’s blood.
A major cause of hemolytic disease of the newborn (HDN) is an incompatibility of the Rh blood group between the mother and fetus. Most commonly, hemolytic disease is triggered by the D antigen, although other Rh antigens, such as c, C, E, and e, can also cause problems 2.
Pregnancies at risk of hemolytic disease of the newborn (HDN) are those in which an Rh D-negative mother becomes pregnant with an RhD-positive child (the child having inherited the D antigen from the father). The mother’s immune response to the fetal D antigen is to form antibodies against it (anti-D). These antibodies are usually of the IgG type, the type that is transported across the placenta and hence delivered to the fetal circulation.
The direct Coombs test detects maternal anti-D antibodies that have already bound to fetal red blood cells.
First, a sample of fetal red blood cells is washed to remove any unbound antibody (Ig). When the test antibodies (anti-Ig) are added, they agglutinate any fetal red blood cells to which maternal antibodies are already bound (see Figure 1 above).
This is called the direct Coombs test (direct antiglobulin test [DAT]) because the anti-Ig binds “directly” to the maternal anti-D Ig that coats fetal red blood cells in hemolytic disease of the newborn.
Indirect coombs test in pregnancy
Indirect Coombs test is used in the prevention of hemolytic disease of the newborn. Indirect Coombs test finds anti-D antibodies in the mother’s serum. If these were to come into contact with fetal red blood cells they would hemolyze them and hence cause hemolytic disease of the newborn. By finding maternal anti-D before fetal red blood cells have been attacked, treatment can be given to prevent or limit the severity of hemolytic disease of the newborn.
For indirect Coombs test, the mother’s serum is incubated with Rh D-positive red blood cells. If any anti-D is present in the mother’s serum, they will bind to the Rh D-positive red blood cells. The Rh D-positive red blood cells are then washed to remove all free antibodies. When anti-Ig antibodies are added, they will agglutinate any red blood cells to which maternal antibodies are bound.
This is called the indirect Coombs test (indirect antiglobulin test [IAT]) because the anti-Ig finds “indirect” evidence of harmful maternal antibodies, requiring the addition of fetal red blood cells to show the capacity of maternal anti-D to bind to fetal red blood cells.
As part of routine prenatal or antenatal care, the blood type of the mother (ABO and Rh) is determined by a blood test. A test for the presence of atypical antibodies in the mother’s serum is also performed. At present, Rh D incompatibility is the only cause of hemolytic disease of the newborn for which screening is routine.
In the United States, the frequency of Rh D-negative status varies from about 17% in Caucasians to about 7% in Hispanics and Blacks. The frequency is much lower in people of Asian descent (including people from China, India, and Japan), averaging about 2% 3.
To find out whether a pregnant Rh D-negative mother has been sensitized to the Rh D antigen, an indirect Coombs test is done (see above). If anti-D is not found in the mother’s serum, it is likely that she has not been sensitized to the Rh D antigen.
The risk of future sensitization can be greatly reduced by giving all unsensitized mothers anti-D Ig, which “mops up” any fetal red blood cells that may have leaked into the maternal circulation, reducing the risk of first-time exposure to the D antigen.
Usually, Rh D-negative mothers receive on injection of anti-D Ig at about 28 weeks gestation, which is about the time when fetal red blood cells start to express the D antigen, and mothers receive another dose at about 34 weeks, a few weeks before labor begins during which the risk of fetomaternal hemorrhage is high. A final dose of anti-D Ig is given after the baby has been delivered. In addition, anti-D Ig is given to cover other events during the pregnancy that may lead to sensitization, e.g., antepartum bleeds and pre-eclampsia.
This prophylaxis regime against Rh D sensitization is effective. However, currently, there is no routine prophylaxis for hemolytic disease of the newborn caused by incompatibility of other blood group antigens.
Once the presence of maternal anti-D has been confirmed, the next step is to determine whether the fetal red blood cells are a target, i.e., confirm the Rh status of the fetus. If the father is homozygous for the D allele (D/D), the fetus will be D positive. If however the father is heterozygous (D/d), there is a 50:50 chance that the fetus is D positive, and the only way to know the blood type for sure is to test a sample of fetal cells taken from the amniotic fluid or umbilical cord.
If the fetus is Rh D-positive, the pregnancy is carefully monitored for signs of hemolytic disease of the newborn. Monitoring includes regular ultrasound scans of the fetus and monitoring of the amount of anti-D in the mother’s serum. Active hemolysis is indicated by a rise in anti-D. If a fetal blood test confirms fetal anemia, depending upon its severity, a blood transfusion can be done in utero to replace the lyzed fetal red blood cells.
Blood transfusions may also be needed to correct anemia in the newborn period. During this period there may also be a sharp rise in the level of bilirubin in the neonate, which can be lowered by phototherapy and exchange transfusions.
If a mother has an incompatibility with one child, will she have them with all of her children?
It depends on whether the baby has the corresponding antigens for the mother’s antibodies. A baby born to a blood group O mother may have hemolytic disease of the newborn in any pregnancy. When a mother is Rh-negative, she may develop antibodies against the red blood cells of her first Rh-positive child if she does not receive prophylaxis. Any subsequent Rh-positive children may then be affected by the mother’s Rh antibodies. Fortunately, this is now relatively rare as Rh-negative mothers are tested during and after their pregnancy and are given RhIg (RhImmune Globulin, Rhogam) injections to prevent the development of Rh antibodies. Other antibodies may also recur in subsequent pregnancies and need to be discussed with the mother’s healthcare provider.
Sensitization occurs during the first pregnancy
Sensitization to an antigen occurs when the immune system encounters an antigen for the first time and mounts an immune response. In the case of hemolytic disease of the newborn caused by Rh incompatibility, an Rh D-negative mother may first encounter the D antigen while being pregnant with an Rh D-positive child, or by receiving a blood transfusion of Rh D-positive blood. Once a mother has been sensitized to the D antigen, her serum will contain anti-D. The direct Coombs test (see below) confirms the presence of anti-D and hence that the mother has been sensitized.
Only a small amount of fetal blood need enter the mother’s circulation for sensitization to occur. Typically, this occurs during the delivery of the first-born Rh D-positive child. Fetal-maternal hemorrhage is common during labor and is increased during a prolonged or complicated labor, which in turn increases the risk of sensitization. Sensitization can also occur earlier in the pregnancy, for example during a prenatal bleed or a miscarriage. It may also occur during medical procedures, such as a termination of pregnancy or chorionic villus sampling.
The risk of sensitization to the Rh D antigen is decreased if the fetus is ABO incompatible. This is because any fetal cells that leak into the maternal circulation are rapidly destroyed by potent maternal anti-A and/or anti-B, reducing the likelihood of maternal exposure to the D antigen.
References- Zarandona JM, Yazer MH. The role of the Coombs test in evaluating hemolysis in adults. CMAJ. 2006;174(3):305-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1373708/
- Dean L. Blood Groups and Red Cell Antigens [Internet]. Bethesda (MD): National Center for Biotechnology Information (US); 2005. Chapter 4, Hemolytic disease of the newborn. Available from: https://www.ncbi.nlm.nih.gov/books/NBK2266
- Garratty G , Glynn SA , McEntire R . ABO and Rh(D) phenotype frequencies of different racial/ethnic groups in the United States. Transfusion. 2004;44:703–6.





{kind=link}