
What is COPD
COPD stands for Chronic Obstructive Pulmonary Disease (COPD), a name for a chronic inflammatory lung disease that causes obstructed airflow from the lungs making breathing difficult. Although chronic obstructive pulmonary disease (COPD) makes breathing increasingly more difficult, COPD develops slowly over many years and you may not be aware you have it at first.
Symptoms include breathing difficulty, cough, mucus (sputum) production and wheezing. It’s caused by long-term exposure to irritating gases or particulate matter, most often from cigarette smoke. People with COPD are at increased risk of developing heart disease, lung cancer and a variety of other conditions.
COPD includes:
- Emphysema – damage to the air sacs in the lungs
- Chronic bronchitis – long-term inflammation of the airways
Emphysema and chronic bronchitis are the two most common conditions that contribute to COPD. Chronic bronchitis is inflammation of the lining of the bronchial tubes, which carry air to and from the air sacs (alveoli) of the lungs. It’s characterized by daily cough and mucus (sputum) production.
Emphysema is a condition in which the alveoli at the end of the smallest air passages (bronchioles) of the lungs are destroyed as a result of damaging exposure to cigarette smoke and other irritating gases and particulate matter.
COPD is a common condition that mainly affects middle-aged or older adults who smoke. Many people don’t realize they have COPD until they reach their late 40s or 50s.
The breathing problems tend to get gradually worse over time and can limit your normal activities, although treatment can help keep the condition under control.
While there’s currently no cure for COPD, COPD is treatable and the sooner treatment begins, the less chance there is of severe lung damage.
With proper management, most people with COPD can achieve good symptom control and quality of life, as well as reduced risk of other associated conditions.
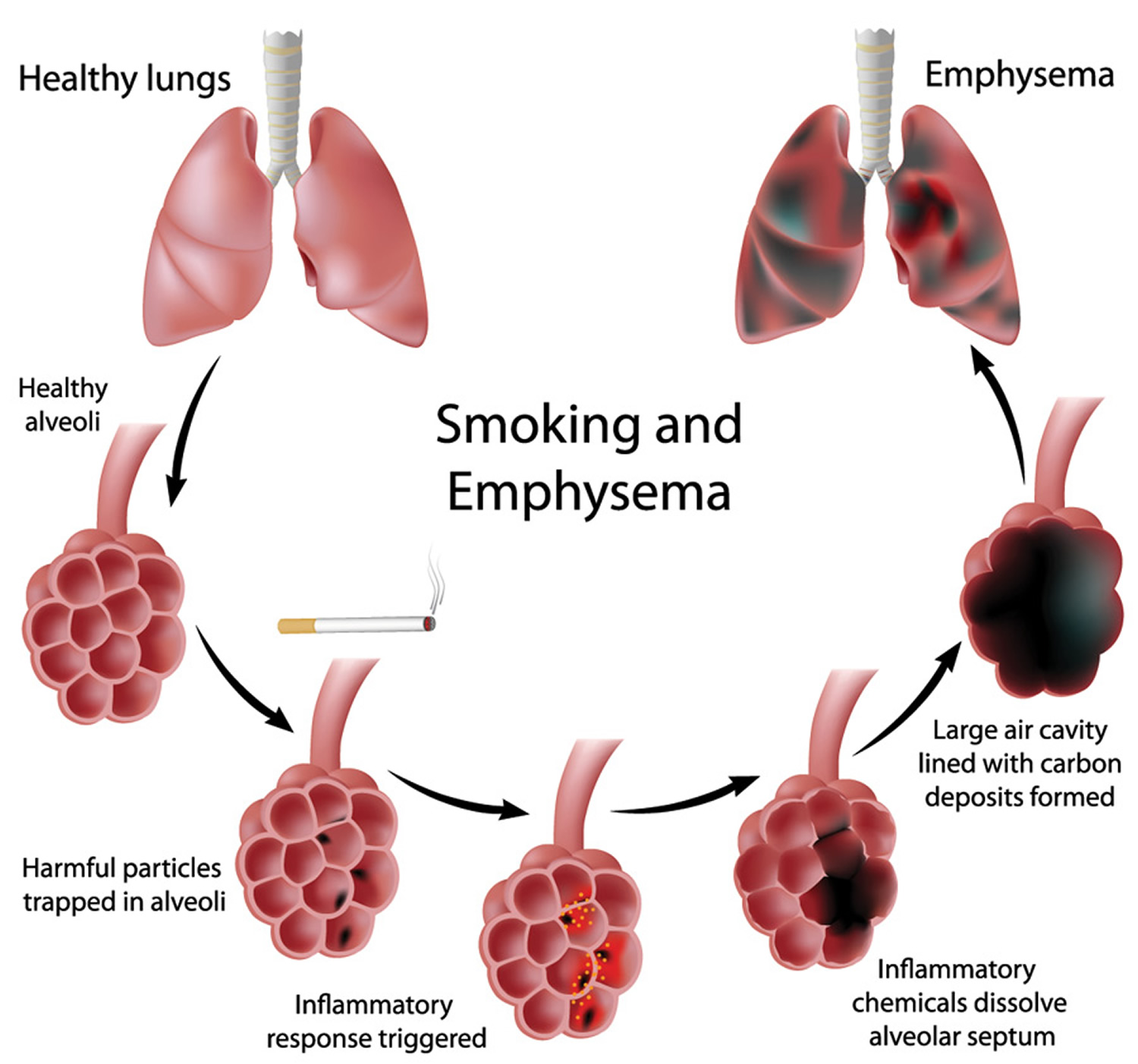
Figure 1. Normal Lungs and Lungs With Emphysema (COPD)
COPD life expectancy
Various measures have been shown to correlate with prognosis in COPD, including forced expiratory volume in 1 second (FEV1), diffusion capacity for carbon monoxide (DLCO), blood gas measurements, body mass index (BMI), exercise capacity, and clinical status. A correlation has also been established between radiographic severity of emphysema and mortality 1.
A widely used simple prognostication tool is the BODE index, which is based on:
- Body mass index (BMI),
- Obstruction (FEV1),
- Dyspnea (using Medical Research Council Dyspnea Scale), and
- Exercise capacity (ie, 6-minute walk distance).
You can make an estimated calculation for your BODE Index for COPD life expectancy with a BODE Index calculator (https://reference.medscape.com/calculator/bode-index-copd). Here’s what you’ll need before you enter information into the calculator:
- FEV1 percentage predicated after using a bronchodilator to open airways from your pulmonary function test
- Your 6-minute walk test distance
- Body mass index
- Level of dyspnea or difficulty breathing.
After you enter the information, an approximate survival prediction will show. Of course, it’s important to remember that this is a tool to help estimate life expectancy, and you need to discuss your BODE Index and COPD with your doctor.
BODE index
Body mass index (BMI) is scored as follows:
- Greater than 21 kg/m2 = 0 points
- Less than 21 kg/m2= 1 point
FEV1 (postbronchodilator percent predicted) is scored as follows:
- Greater than 65% = 0 points
- 50-64% = 1 point
- 36-49% = 2 points
- Less than 35% = 3 points
Modified Medical Research Council (MMRC) dyspnea scale is scored as follows:
- MMRC 0 = Dyspneic on strenuous exercise (0 points)
- MMRC 1 = Dyspneic on walking a slight hill (0 points)
- MMRC 2 = Dyspneic on walking level ground; must stop occasionally due to breathlessness (1 point)
- MMRC 3 = Dyspneic after walking 100 yards or a few minutes (2 points)
- MMRC 4 = Cannot leave house; dyspneic doing activities of daily living (3 points)
Six-minute walking distance is scored as follows:
- Greater than 350 meters = 0 points
- 250-349 meters = 1 point
- 150-249 meters = 2 points
- Less than 149 meters = 3 points
BODE’s approximate 4-year survival is as follows:
- 0-2 points = 80%
- 3-4 points = 67%
- 5-6 points = 57%
- 7-10 points = 18%
Mortality/morbidity
A US Centers for Disease Control and Prevention (CDC) Morbidity Mortality Weekly Report study of the National Vital Statistics System reported an age-standardized death rate from COPD in the United States for adults older than 25 years of 2.3 deaths per 100,000 population 2. This rate varied by location, with the lowest rate in Hawaii (27.1 deaths per 100,000 population) and the highest rate in Oklahoma (93.6 deaths per 100,000 population).
What causes COPD
The main cause of COPD in developed countries is tobacco smoking. In the developing world, COPD often occurs in people exposed to fumes from burning fuel for cooking and heating in poorly ventilated homes.
Only about 20 to 30 percent of chronic smokers may develop clinically apparent COPD, although many smokers with long smoking histories may develop reduced lung function. Some smokers develop less common lung conditions. They may be misdiagnosed as having COPD until a more thorough evaluation is performed.
COPD pathophysiology
Air travels down your windpipe (trachea) and into your lungs through two large tubes (bronchi). Inside your lungs, these tubes divide many times — like the branches of a tree — into many smaller tubes (bronchioles) that end in clusters of tiny air sacs (alveoli).
The air sacs have very thin walls full of tiny blood vessels (capillaries). The oxygen in the air you inhale passes into these blood vessels and enters your bloodstream. At the same time, carbon dioxide — a gas that is a waste product of metabolism — is exhaled.
Your lungs rely on the natural elasticity of the bronchial tubes and air sacs to force air out of your body. COPD causes them to lose their elasticity and overexpand, which leaves some air trapped in your lungs when you exhale.
Causes of airway obstruction
Causes of airway obstruction include:
- Emphysema. This lung disease causes destruction of the fragile walls and elastic fibers of the alveoli. Small airways collapse when you exhale, impairing airflow out of your lungs.
- Chronic bronchitis. In this condition, your bronchial tubes become inflamed and narrowed and your lungs produce more mucus, which can further block the narrowed tubes. You develop a chronic cough trying to clear your airways.
Cigarette smoke and other irritants
In the vast majority of cases, the lung damage that leads to COPD is caused by long-term cigarette smoking. But there are likely other factors at play in the development of COPD, such as a genetic susceptibility to the disease, because only about 20 to 30 percent of smokers may develop COPD.
Other irritants can cause COPD, including cigar smoke, secondhand smoke, pipe smoke, air pollution and workplace exposure to dust, smoke or fumes.
In the vast majority of cases, the lung damage that leads to COPD is caused by long-term cigarette smoking. But there are likely other factors at play in the development of COPD, such as a genetic susceptibility to the disease, because only about 20 to 30 percent of smokers may develop COPD.
Other irritants can cause COPD, including cigar smoke, secondhand smoke, pipe smoke, air pollution and workplace exposure to dust, smoke or fumes.
Alpha-1-antitrypsin deficiency
In about 1 percent of people with COPD, the disease results from a genetic disorder that causes low levels of a protein called alpha-1-antitrypsin. Alpha-1-antitrypsin (AAt) is made in the liver and secreted into the bloodstream to help protect the lungs. Alpha-1-antitrypsin deficiency can affect the liver as well as the lungs. Damage to the lung can occur in infants and children, not only adults with long smoking histories.
For adults with COPD related to AAt deficiency, treatment options include those used for people with more-common types of COPD. In addition, some people can be treated by replacing the missing AAt protein, which may prevent further damage to the lungs.
Intravenous drug user
Emphysema occurs in approximately 2% of persons who use intravenous drugs. This is attributed to pulmonary vascular damage resulting from the insoluble filler (eg, cornstarch, cotton fibers, cellulose, talc) contained in methadone or methylphenidate.
The bullous cysts found in association with intravenous use of cocaine or heroin occur predominantly in the upper lobes. In contrast, methadone and methylphenidate injections are associated with basilar and panacinar emphysema.
Immune deficiency syndromes
Human immunodeficiency virus (HIV) infection was found to be an independent risk factor for emphysema, even after controlling for confounding variables such as smoking, intravenous drug use, race, and age 3.
Apical and cortical bullous lung damage occurs in patients who have autoimmune deficiency syndrome and Pneumocystis carinii infection. Reversible pneumatoceles are observed in 10-20% of patients with this infection.
Vasculitis
Hypocomplementemic vasculitis urticaria syndrome (HVUS) may be associated with obstructive lung disease.
Other sequellae include angioedema, nondeforming arthritis, sinusitis, conjunctivitis, and pericarditis.
Connective-tissue disorders
Cutis laxa, a disorder of elastin that is characterized most prominently by the appearance of premature aging. The disease is usually congenital, with various forms of inheritance (ie, dominant, recessive). Precocious emphysema has been described in association with cutis laxa as early as the neonatal period or infancy. The pathogenesis of this disorder includes a defect in the synthesis of elastin or tropoelastin.
Marfan syndrome is an autosomal dominant inherited disease of type I collagen characterized by abnormal length of the extremities, subluxation of the lenses, and cardiovascular abnormality. Pulmonary abnormalities, including emphysema, have been described in approximately 10% of patients.
Ehlers-Danlos syndrome refers to a group of inherited connective-tissue disorders with manifestations that include hyperextensibility of the skin and joints, easy bruisability, and pseudotumors.
Salla disease
Salla disease is an autosomal recessive storage disorder described in Scandinavia; the disease is characterized by intralysosomal accumulation of sialic acid in various tissues. The most important clinical manifestations are severe mental retardation, ataxia, and nystagmus.
Risk factors for COPD
Risk factors for COPD include:
- Exposure to tobacco smoke. The most significant risk factor for COPD is long-term cigarette smoking. The more years you smoke and the more packs you smoke, the greater your risk. Pipe smokers, cigar smokers and marijuana smokers also may be at risk, as well as people exposed to large amounts of secondhand smoke.
- People with asthma who smoke. The combination of asthma, a chronic inflammatory airway disease, and smoking increases the risk of COPD even more.
- Occupational exposure to dusts and chemicals. Long-term exposure to chemical fumes, vapors and dusts in the workplace can irritate and inflame your lungs.
- Exposure to fumes from burning fuel. In the developing world, people exposed to fumes from burning fuel for cooking and heating in poorly ventilated homes are at higher risk of developing COPD.
- Age. COPD develops slowly over years, so most people are at least 40 years old when symptoms begin.
- Genetics. The uncommon genetic disorder alpha-1-antitrypsin deficiency is the cause of some cases of COPD. Other genetic factors likely make certain smokers more susceptible to the disease.
Complications of COPD
COPD can cause many complications, including:
- Respiratory infections. People with COPD are more likely to catch colds, the flu and pneumonia. Any respiratory infection can make it much more difficult to breathe and could cause further damage to lung tissue. An annual flu vaccination and regular vaccination against pneumococcal pneumonia can prevent some infections.
- Heart problems. For reasons that aren’t fully understood, COPD can increase your risk of heart disease, including heart attack. Quitting smoking may reduce this risk.
- Lung cancer. People with COPD have a higher risk of developing lung cancer. Quitting smoking may reduce this risk.
- High blood pressure in lung arteries. COPD may cause high blood pressure in the arteries that bring blood to your lungs (pulmonary hypertension).
- Depression. Difficulty breathing can keep you from doing activities that you enjoy. And dealing with serious illness can contribute to development of depression. Talk to your doctor if you feel sad or helpless or think that you may be experiencing depression.
Prevention of COPD
Unlike some diseases, COPD has a clear cause and a clear path of prevention. The majority of cases are directly related to cigarette smoking, and the best way to prevent COPD is to never smoke — or to stop smoking now.
If you’re a longtime smoker, these simple statements may not seem so simple, especially if you’ve tried quitting — once, twice or many times before. But keep trying to quit. It’s critical to find a tobacco cessation program that can help you quit for good. It’s your best chance for preventing damage to your lungs.
Occupational exposure to chemical fumes and dust is another risk factor for COPD. If you work with this type of lung irritant, talk to your supervisor about the best ways to protect yourself, such as using respiratory protective equipment.
5 Steps to Reduce Your Risk for COPD
If you are concerned about getting COPD, there are steps you can take to protect yourself.
- If you are a smoker, STOP SMOKING. Quitting smoking is the single most important thing a smoker can do to live a longer and healthier life. The American Lung Association 4 has many programs to help you quit for good.
- If you don’t smoke, don’t start. Smoking causes COPD, lung cancer, heart disease and other cancers.
- Avoid exposure to secondhand smoke. Make your home smokefree. You’ll not only protect yourself, but your family too. Learn about your rights to a smoke free environment at work and in public places.
- Be aware of other dangers. Take care to protect yourself against chemicals, dust and fumes in your home and at work.
- Help fight for clean air. Work with others in your community to help clean up the air you and your family breathe.
COPD signs and symptoms
COPD symptoms often don’t appear until significant lung damage has occurred, and they usually worsen over time, particularly if smoking exposure continues. For chronic bronchitis, the main symptom is a daily cough and mucus (sputum) production at least three months a year for two consecutive years.
The main common symptoms of COPD are:
- Increasing breathlessness, particularly when you’re active
- A persistent chesty cough with phlegm (sputum or mucus) that may be clear, white, yellow or greenish – some people may dismiss this as just a “smoker’s cough”
- Frequent chest infections
- Persistent wheezing
The symptoms will usually get gradually worse over time and make daily activities increasingly difficult, although treatment can help slow the progression.
Sometimes there may be periods when your symptoms get suddenly worse – known as flare-ups or COPD exacerbations. It’s common to have a few flare-ups a year, particularly during the winter.
Less common symptoms of COPD include:
- Unintended weight loss (in later stages)
- Tiredness
- Lack of energy
- Swollen ankles, feet or legs from a build-up of fluid (edema)
- Chest tightness
- Blueness of the lips or fingernail beds (cyanosis)
- Chest pain and coughing up blood – although these are usually signs of another condition, such as a chest infection or possibly lung cancer
These additional symptoms only tend to occur when COPD reaches a more advanced stage.
COPD diagnosis
COPD is commonly misdiagnosed — former smokers may sometimes be told they have COPD, when in reality they may have simple deconditioning or another less common lung condition. Likewise, many people who have COPD may not be diagnosed until the disease is advanced and interventions are less effective.
A diagnosis of COPD should be considered in patients over the age of 35 who have a risk factor (generally smoking) and who present with one or more of the following symptoms:
- exertional breathlessness
- chronic cough
- regular sputum production
- frequent winter ‘bronchitis’
- wheeze (less common)
To diagnose your condition, your doctor will review your signs and symptoms, discuss your family and medical history, and discuss any exposure you’ve had to lung irritants — especially cigarette smoke.
Your doctor will also:
- examine your chest and listen to your breathing with a stethoscope
- alculate your body mass index (BMI) using your weight and height
- ask if you have a family history of lung problems
Your doctor may also carry out or arrange for you to have a breathing test called spirometry and some of the other tests described below to diagnose your condition.
Tests may include:
Lung (pulmonary) function tests. Pulmonary function tests measure the amount of air you can inhale and exhale, and if your lungs are delivering enough oxygen to your blood.
Spirometry is the most common lung function test. During this test, you’ll be asked to blow into a large tube connected to a small machine called a spirometer. This machine measures how much air your lungs can hold and how fast you can blow the air out of your lungs.
Spirometry can detect COPD even before you have symptoms of the disease. It can also be used to track the progression of disease and to monitor how well treatment is working. Spirometry often includes measurement of the effect of bronchodilator administration. Other lung function tests include measurement of lung volumes, diffusing capacity and pulse oximetry.
Chest X-ray. A chest X-ray can show emphysema, one of the main causes of COPD. An X-ray can also rule out other lung problems or heart failure.
CT scan. A CT scan of your lungs can help detect emphysema and help determine if you might benefit from surgery for COPD. CT scans can also be used to screen for lung cancer.
Arterial blood gas analysis. This blood test measures how well your lungs are bringing oxygen into your blood and removing carbon dioxide.
Laboratory tests. Laboratory tests aren’t used to diagnose COPD, but they may be used to determine the cause of your symptoms or rule out other conditions. For example, laboratory tests may be used to determine if you have the genetic disorder alpha-1-antitrypsin (AAt) deficiency, which may be the cause of some cases of COPD. This test may be done if you have a family history of COPD and develop COPD at a young age, such as under age 45.
COPD stages
The FEV1 is used to stage the severity of COPD. It is normalized as a percentage of predicted for healthy controls. The following Global Initiative for Chronic Obstructive Lung Disease (GOLD) staging system is widely used (note that the postbronchodilator FEV1 is used):
- Stage I (mild) – FEV 1 of 80% or more of predicted
- Stage II (moderate) – FEV 1 of less than 80% and 50% or more of predicted
- Stage III (severe) – FEV 1 less than 50% and 30% or more of predicted
- Stage IV (very severe) – FEV 1 less than 30% of predicted or FEV 1 less than 50% and chronic respiratory failure
Respiratory failure is defined as a PaO2 less than 60 mm Hg (kPa 8.0) or a PaCO2 higher than 50 mm Hg (kPa 6.7).
Many doctors use more than one way to determine your chronic obstructive pulmonary disease (COPD) stage.
BODE Index for COPD
Other scientists came up with the BODE Index to measure the severity of COPD. BODE stands for body mass, airflow obstruction, dyspnea and exercise capacity. The BODE Index accounts for how COPD affects your life.
- Body Mass
- Airflow Obstruction
- Dyspnea
- Exercise Capacity
The body mass index (BMI) helps determine if you’re overweight, obese or underweight. Airflow obstruction refers to your FEV1, which is similar to the GOLD system. Dyspnea means trouble breathing, and exercise capacity refers to exercise tolerance. Many people with COPD take a six-minute walk test—the distance you can walk in 6 minutes—to evaluate their level of exercise tolerance. These combined measurements make up the BODE Index and can be used to put COPD into stages or approximate life expectancy with COPD.
You can make an estimated calculation for your BODE Index for COPD life expectancy with a BODE Index calculator (https://reference.medscape.com/calculator/bode-index-copd). Here’s what you’ll need before you enter information into the calculator:
- FEV1 percentage predicated after using a bronchodilator to open airways from your pulmonary function test
- Your 6-minute walk test distance
- Body mass index
- Level of dyspnea or difficulty breathing.
After you enter the information, an approximate survival prediction will show. Of course, it’s important to remember that this is a tool to help estimate life expectancy, and you need to discuss your BODE Index and COPD with your doctor.
Remember, seeing your doctor regularly to keep track of your GOLD chronic obstructive pulmonary disease (COPD) stages and other measurements, such as BODE index and pulmonary function test, is important. Being proactive in your healthcare is essential to improving and maintaining your quality of life.
COPD treatment
There’s currently no cure for chronic obstructive pulmonary disease (COPD), but treatment can help slow the progression of the condition and control the symptoms.
A diagnosis of COPD is not the end of the world. Most people have mild forms of the disease for which little therapy is needed other than smoking cessation. Even for more advanced stages of disease, effective therapy is available that can control symptoms, reduce your risk of complications and exacerbations, and improve your ability to lead an active life.
Treatments include:
- stopping smoking – if you have COPD and you smoke, this is the most important thing you can do
- inhalers and medications – to help make breathing easier
- pulmonary rehabilitation – a specialised programme of exercise and education
- surgery or a lung transplant – although this is only an option for a very small number of people
Your doctor will discuss the various treatment options with you.
The National Institute for Health and Care Excellence (NICE) has produced guidance on the diagnosis and treatment of COPD, which outlines the care you can expect to receive.
Quit Smoking
The most essential step in any treatment plan for COPD is quitting smoking and to stop all smoking. It’s the only way to keep COPD from getting worse — which can eventually reduce your ability to breathe. But quitting smoking isn’t easy. And this task may seem particularly daunting if you’ve tried to quit and have been unsuccessful.
Talk to your doctor about nicotine replacement products and medications that might help, as well as how to handle relapses. Your doctor may also recommend a support group for people who want to quit smoking. It’s also a good idea to avoid secondhand smoke exposure whenever possible.
Nicotine Replacement Therapy
Supervised use of pharmacologic agents is an important adjunct to self-help and group smoking cessation programs. Nicotine is the ingredient in cigarettes primarily responsible for the addiction of smoking. Withdrawal from nicotine may cause unpleasant adverse effects (ie, anxiety, irritability, difficulty concentrating, anger, fatigue, drowsiness, depression, and sleep disruption). These effects usually occur during the first weeks after quitting smoking. Nicotine replacement therapies after smoking cessation reduce withdrawal symptoms. A person who smokes and who requires the first cigarette within 30 minutes of waking is likely to be highly addicted and would benefit from nicotine replacement therapy. Several nicotine replacement therapies are available.
Nicotine polacrilex is a chewing gum and produces improved quit rates compared to counseling alone. Transdermal nicotine patches are readily available for replacement therapy. Long-term success rates have been 22-42%, compared with 2-25% with placebos. These agents are well tolerated, and the adverse effects are limited to localized skin reactions. The use of an antidepressant medication, bupropion at 150 mg bid has been shown to be effective for smoking cessation and may be used in combination with nicotine replacement therapy.
The most recent drug to receive approval for smoking cessation is varenicline. Varenicline is a partial agonist selective for alpha4, beta2 nicotinic acetylcholine receptors. Its mechanism of action is believed to be binding the nicotinic subtype receptor, producing agonist activity while simultaneously preventing nicotine binding. Varenicline’s agonistic activity is significantly lower than nicotine’s.
COPD medications
A variety of medicines are used to treat COPD and there is no “best” medicine for all people. Each person’s COPD is different and your doctor and healthcare team will work with you to set up the best plan to address your symptoms and needs.
Doctors use several kinds of medications to treat the symptoms and complications of COPD. You may take some medications on a regular basis and others as needed.
By taking the right medicine at the right time, you can:
- Breathe better
- Do more of the things you enjoy
- Have fewer flare-ups or exacerbations
Most people with COPD take long-acting medicine every day to help shortness of breath. In addition, short-acting medicine is used on an only-when-needed basis to decrease shortness of breath. For many, a combination of medicines is prescribed.
Oral and inhaled steroids
Decreasing inflammation leads to less swelling and mucus production in the airways and that makes it easier to breath. These medicines are known as corticosteroids or steroids. They are usually inhaled with an inhaler device. Make sure you rinse your mouth with water immediately after using a steroid inhaler to prevent thrush, a yeast infection of the throat.
Corticosteroids can also be swallowed as a pill and are usually delivered for short periods of time in special circumstances when your symptoms are getting more severe. Steroids have serious side effects, such as weight gain, diabetes, osteoporosis, cataracts and increased risk of infection so they must be monitored carefully. Your doctor will talk with you about these side effects.
For people who have a moderate or severe acute exacerbation, short courses (for example, five days) of oral corticosteroids prevent further worsening of COPD. However, long-term use of these medications can have serious side effects, such as weight gain, diabetes, osteoporosis, cataracts and an increased risk of infection.
Phosphodiesterase-4 inhibitors
A new type of medication approved for people with severe COPD and symptoms of chronic bronchitis is roflumilast (Daliresp), a phosphodiesterase-4 inhibitor. This drug decreases airway inflammation and relaxes the airways. Common side effects include diarrhea and weight loss.
Theophylline
This very inexpensive medication may help improve breathing and prevent exacerbations. Side effects may include nausea, headache, fast heartbeat and tremor. Side effects are dose related, and low doses are recommended.
Antibiotics
People with COPD do experience flare-ups with more coughing, more mucus and more shortness of breath. This is often caused by bacterial or viral infections. Your doctor may give you an antibiotic or an anti-viral prescription to keep on hand and fill for when you have an infection.
Make sure you take all of the antibiotic exactly as prescribed. You may start to feel better during the antibiotic course but make sure you take the antibiotic for the prescribed duration. Short cutting the antibiotic course may allow the infection to come back or become resistant to the antibiotic.
In patients with COPD, chronic infection or colonization of the lower airways with S pneumoniae, H influenzae, and/or Moraxella catarrhalis is common. Patients with severe disease have a higher prevalence of Gram-negative organisms such as Pseudomonas. The use of antibiotics for the treatment of acute exacerbations is well supported 5. The patients who benefited most from antibiotic therapy were those with exacerbations that were characterized by at least two of the following: increases in dyspnea, sputum production, and sputum purulence (The Winnipeg criteria).
Inpatient management of acute exacerbations of COPD includes empiric antibiotic coverage with a macrolide, a beta-lactam, or doxycycline.
The prophylactic use of antibiotics, in particular azithromycin, to prevent COPD exacerbations has been explored over the past 20 years. In 2011, Albert et al 5 reported on the use of azithromycin to prevent exacerbations of COPD; they showed that among 1,142 patients with severe COPD (defined as an FEV1 of less than 40% predicted), those randomized to take 250 mg of daily azithromycin for 1 year had fewer clinical exacerbations, longer time to first exacerbation, and higher quality of life scores when compared with placebo. Adverse effects include hearing loss and prolongation of the QT interval.
In 2013, the FDA released an announcement of sudden death associated with azithromycin, stating that patients at particular risk for developing torsades de pointes were known to have preexisting prolonged QT interval, low levels of potassium or magnesium, bradycardia, history of antiarrhythmics, or known arrhythmias. However, a recent study shows that the antibiotic azithromycin prevents exacerbations, but it isn’t clear whether this is due to its antibiotic effect or its anti-inflammatory properties.
Mucolytic agents
Viscous lung secretions in patients with COPD consist of mucus-derived glycoproteins and leukocyte-derived DNA. Mucolytic agents reduce sputum viscosity and improve secretion clearance. Although mucolytic agents have been shown to decrease cough and chest discomfort, they have not been shown to improve dyspnea or lung function 6.
However, in 2009-2010, Chinese investigators designed and implemented a prospective, randomized, double-blind placebo-controlled trial, studying the effects of long-term oral N-acetylcysteine at 600 mg twice daily in subjects with GOLD stage I COPD. They found long-term use (over a year and a half) can actually prevent exacerbations in moderate disease. Interesting enough, exacerbations of COPD were the most significant adverse effect of the trial 7. The study was published in The Lancet in March of 2014.
Alpha1-antitrypsin deficiency treatment
The treatment strategies for alpha1-antitrypsin deficiency involve reducing the neutrophil elastase burden, primarily by smoking cessation, and augmenting the levels of alpha1-antitrypsin. Available augmentation strategies include pharmacologic attempts to increase endogenous production of alpha1-antitrypsin by the liver (ie, danazol, tamoxifen) or administration of purified alpha1-antitrypsin by periodic intravenous infusion or by inhalation. Tamoxifen can increase endogenous production of alpha1-antitrypsin to a limited extent, so this may be beneficial in persons with the PIZZ phenotype.
Intravenous augmentation therapy is the only available approach that can increase serum levels to greater than 11 mmol/L, the protective threshold. Studies show that the infusions can maintain levels of more than 11 mmol/L, and replacement is administered weekly (60 mg/kg), biweekly (120 mg/kg), or monthly (250 mg/kg). The ability of intravenous alpha1-antitrypsin augmentation to alter the clinical course of patients with alpha1-antitrypsin deficiency has not been demonstrated. Uncontrolled observations of patients suggest that the FEV1 may fall at a slower rate in patients who receive alpha1-antitrypsin replacement 8.
COPD inhalers
Bronchodilators
Bronchodilators relax the muscles around the airways which helps to keep them open and makes breathing easier. Most bronchodilators are often delivered through an inhaler or can be nebulized so you breathe the medicine straight into your lungs. Inhalers operate in different ways, so make sure to ask your healthcare team to show you how your specific inhaler works. This ensures you will get a full dose of medicine with each breath. Other bronchodilators are swallowed as a pill.
Bronchodilators can be short-acting or long-acting. Short-acting bronchodilators work quickly so that you get relief from symptoms fast, but they wear off in a few hours. Long-acting bronchodilators provide relief for many hours, but the effect is slower. Short- and long-acting bronchodilators include beta2-agonists and anticholinergics.
- Beta2-Agonists are very potent at relaxing tightened muscles around your airways. This opens the airway and makes breathing easier. Short-acting beta-agonists work within minutes but last only 4-6 hours. Long-acting beta-agonists are slow to start working but can last up to 12 hours so are used to maintain open airways throughout the day or the night.
- Anticholinergics prevent the muscles around your airways from tightening so keep the airways open and help clear mucus from your lungs. This combination allows your cough to expel mucus more easily. There are short-acting and long-acting anticholinergics. Beta-agonists and anticholinergics can be delivered through an inhaler or a nebulizer.
Depending on the severity of your disease, you may need a short-acting bronchodilator before activities, a long-acting bronchodilator that you use every day or both.
Short-acting bronchodilators include albuterol (ProAir HFA, Ventolin HFA, others), levalbuterol (Xopenex HFA), and ipratropium (Atrovent). The long-acting bronchodilators include tiotropium (Spiriva), salmeterol (Serevent), formoterol (Foradil, Perforomist), arformoterol (Brovana), indacaterol (Arcapta) and aclidinium (Tudorza).
Inhaled steroids
Inhaled corticosteroid medications can reduce airway inflammation and help prevent exacerbations. Side effects may include bruising, oral infections and hoarseness. These medications are useful for people with frequent exacerbations of COPD. Fluticasone (Flovent HFA, Flonase, others) and budesonide (Pulmicort Flexhaler, Uceris, others) are examples of inhaled steroids.
Combination inhalers
A corticosteroid, an anticholinergic and a beta-agonist can be combined into one inhaler or nebulizer solution. The most common combinations contain two of these medicines as a:
- Short-acting beta-agonist and short-acting anticholinergic
- Long-acting beta-agonist and corticosteroid
- Long-acting anticholinergic and corticosteroid
Some medications combine bronchodilators and inhaled steroids. Salmeterol and fluticasone (Advair) and formoterol and budesonide (Symbicort) are examples of combination inhalers.
Lung therapies
Doctors often use these additional therapies for people with moderate or severe COPD:
- Oxygen therapy. If there isn’t enough oxygen in your blood, you may need supplemental oxygen. There are several devices to deliver oxygen to your lungs, including lightweight, portable units that you can take with you to run errands and get around town.
Some people with COPD use oxygen only during activities or while sleeping. Others use oxygen all the time. Oxygen therapy can improve quality of life and is the only COPD therapy proven to extend life. Talk to your doctor about your needs and options.
- Pulmonary rehabilitation program. These programs generally combine education, exercise training, nutrition advice and counseling. You’ll work with a variety of specialists, who can tailor your rehabilitation program to meet your needs.
Pulmonary rehabilitation may shorten hospitalizations, increase your ability to participate in everyday activities and improve your quality of life. Talk to your doctor about referral to a program.
Pulmonary Rehabilitation
Pulmonary rehabilitation is an outpatient program and may be based in a hospital or a clinic. You may also be able to receive certain forms of pulmonary rehabilitation in your own home. Pulmonary rehabilitation is a program of education and exercise to increase awareness about your lungs and your disease. You will learn to achieve exercise with less shortness of breath. The classes are offered in a group setting so you get the chance to meet others with your condition, give support to them, as well as receive support from them. The skills and knowledge learned in the program will help you to feel better and manage your chronic lung disease. You become stronger by increasing your level of fitness. Exercising your lungs and your muscles helps you be more active so you can do the things you enjoy with your loved ones. Pulmonary rehabilitation may even decrease the need for hospital visits.
Pulmonary rehabilitation is recommended for patients with COPD who experience shortness of breath frequently and are not able to do daily activities despite daily medication use. Many patients in rehabilitation programs have a diagnosis of COPD, but these programs also help people with other types of chronic lung disease that limits breathing and activity.
Pulmonary rehab programs vary in format and length. Most programs use a small group format and include:
- Education about your condition, symptoms, medications and oxygen
- Supervised exercise classes and instruction
- Breathing techniques
- Nutritional counseling
- Emotional health support
Education
In pulmonary rehab, patients learn everything they need to know about their specific chronic lung disease. Sawchuk says her clients go over anatomy, physiology, breathing techniques and medication management—which includes things like the best time of day to take medications.
Exercise
Because of breathing challenges, people with chronic lung disease tend to avoid exercise. However, the right amount and type of exercise has many benefits. It can improve your heart and muscle strength, increase energy levels and help you use oxygen more efficiently.
In pulmonary rehab, patients are monitored and taught to exercise safely by paying attention to their breathing and oxygen levels, as well as learning modifications such as using a chair for weight lifting and yoga.
Breathing and Oxygen
All pulmonary rehab patients are taught pursed lipped breathing and diaphragmatic breathing exercises, and other breathing strategies, to help increase oxygen levels and better manage symptoms—and fears.
In a pulmonary rehab program, people can learn how to keep breathing issues in check and avoid supplementary oxygen. Others learn how and when to use their oxygen correctly to maximize quality of life.
Nutritional Counseling
Achieving and maintaining a healthy weight is an important part of an overall healthy lifestyle, and it’s no different for people with chronic lung disease. Excessive body weight can increase shortness of breath, and low body weight can decrease your ability to fight infections. Plus, when short of breath it can be hard to eat. People learn to prepare nutritious food without getting stressed or too tired.
Emotional Health Support
Because many people with chronic lung disease, or any chronic illness, often experience depression, anxiety and other emotional problems, many pulmonary rehab programs offer counseling services, or partner with an organization that offers them.
Maintenance
The information acquired during pulmonary rehab needs to be used throughout life in order to avoid hospitalizations, complications and other issues. Plus, importantly, people who use those tools feel better. Many programs offer a maintenance option that allows clients to return for exercise classes and support groups after the program is over.
Managing exacerbations
Even with ongoing treatment, you may experience times when symptoms become worse for days or weeks. This is called an acute exacerbation, and it may lead to lung failure if you don’t receive prompt treatment.
Exacerbations may be caused by a respiratory infection, air pollution or other triggers of inflammation. Whatever the cause, it’s important to seek prompt medical help if you notice a sustained increase in coughing, a change in your mucus or if you have a harder time breathing.
When exacerbations occur, you may need additional medications (such as antibiotics, steroids or both), supplemental oxygen or treatment in the hospital. Once symptoms improve, your doctor will talk with you about measures to prevent future exacerbations, such as quitting smoking, taking inhaled steroids, long-acting bronchodilators or other medications, getting your annual flu vaccine, and avoiding air pollution whenever possible.
Vaccinations
COPD increases your risk for infection with influenza (flu) and pneumonia. Vaccines are available to protect you against the flu and you should get immunized every year. You need a yearly flu shot because the influenza virus changes slightly every year and you must get the latest and newest vaccine. Find where you can get vaccinated in your area. Pneumococcal pneumonia is a bacterial infection of the lung that often follows an influenza infection. There are two vaccines to protect against this infection. You only need to get vaccinated once but you need to get each one. Your doctor can provide these to you.
Sleep and COPD
Patients with COPD may develop substantial decreases in nocturnal PaO2 during all phases of sleep but particularly during rapid eye movement sleep. These episodes are associated with rises in pulmonary arterial pressures and disturbance in sleep architecture initially, but patients may develop pulmonary arterial hypertension and cor pulmonale if the hypoxemia remains untreated. Therefore, patients who have a daytime PaO2 greater than 60 mm Hg but demonstrate substantial nocturnal hypoxemia should be prescribed oxygen supplementation for use during sleep.
Supplemental Oxygen
Chronic obstructive pulmonary disease (COPD) can damage the way that our lungs work to the extent that extra oxygen is needed in order to do daily tasks.
Your body needs oxygen to do everything from digesting food, daily household chores, to going to the grocery store. Sometimes with COPD, your breathing becomes restricted so much that the body needs extra oxygen or supplemental oxygen (also called oxygen therapy).
When the lung alone is unable to provide adequate oxygen, supplemental oxygen benefits the body by:
- Improving sleep and mood
- Increasing mental alertness and physical strength
- Maintaining normal body function
- Preventing heart failure in people with severe lung disease
Providing Oxygen Therapy at Home
- Oxygen can be delivered to your home as compressed oxygen gas or as liquid oxygen. Compressed oxygen gas is stored in steel and aluminum tanks or cylinders. Larger tanks are stationary and used at home. Smaller tanks are more portable for use when you leave the house. Liquid oxygen is made by cooling oxygen gas and converting it to a liquid. Since liquids can be stored in a smaller volume, liquid oxygen is more convenient than compressed oxygen gas for active people. A disadvantage of liquid oxygen is the time of usage as it is more prone to evaporate than compressed oxygen gas.
- Oxygen concentrators also are available for home use. An oxygen concentrator is an electrical device about the size of an end table. It concentrates oxygen in the air by removing nitrogen. This method is less expensive and easier to maintain as it requires no refilling of tanks. However, oxygen concentrators may give off heat and be noisy. Usage may also increase your electricity bill. You will still need a back-up source of oxygen in case of a power failure. There are several reliable portable oxygen concentrators that allow you to leave your home to work, enjoy recreational activities and travel.
You may need oxygen therapy for all or just part of the day. A doctor’s prescription is required for supplemental oxygen.
Safety Tips
There are important safety factors to keep in mind when using oxygen. Oxygen is a safe gas and is non-flammable, however it supports combustion. Materials burn more readily in an oxygen-enriched environment. Follow these tips for safe oxygen use:
- Post “No Smoking” and “No Open Flames” signs in and outside your home to remind people not to smoke
- Avoid open flames in the presence of oxygen such as matches, cigarette lighters, candles and burning tobacco. Insist that people who wish to smoke step outside your home.
- Use caution around other sources of heat, such as electric or gas heaters and/or stoves—at least 5 feet is a recommended distance between oxygen and other heat sources.
- Avoid using lotions or creams containing petroleum, which are more likely to catch fire in the presence of oxygen. Use water-based products instead.
- Store cylinders safely in an upright position, secured in an approved cart or storage device.
- Remember that oxygen supply valves should be turned off when not in use.
- Always follow the instructions of your oxygen supply company regarding safe usage.
- Losing access to oxygen can be very dangerous if you need oxygen continually. Make sure to have backup equipment (normally a large oxygen tank) and tell your power company that you have life-sustaining equipment in your home.
Other breathing treatments or assisted breathing devices are being used more frequently for people with COPD. These treatments are known as CPAP, BiPAP or nasal positive pressure ventilation.
Lifestyle and home remedies
If you have COPD, you can take steps to feel better and slow the damage to your lungs:
- Control your breathing. Talk to your doctor or respiratory therapist about techniques for breathing more efficiently throughout the day. Also be sure to discuss breathing positions and relaxation techniques that you can use when you’re short of breath.
- Clear your airways. With COPD, mucus tends to collect in your air passages and can be difficult to clear. Controlled coughing, drinking plenty of water and using a humidifier may help.
- Exercise regularly. It may seem difficult to exercise when you have trouble breathing, but regular exercise can improve your overall strength and endurance and strengthen your respiratory muscles. Discuss with your doctor which activities are appropriate for you.
- Eat healthy foods. A healthy diet can help you maintain your strength. If you’re underweight, your doctor may recommend nutritional supplements. If you’re overweight, losing weight can significantly help your breathing, especially during times of exertion.
- Avoid smoke and air pollution. In addition to quitting smoking, it’s important to avoid places where others smoke. Secondhand smoke may contribute to further lung damage. Other types of air pollution also can irritate your lungs.
- See your doctor regularly. Stick to your appointment schedule, even if you’re feeling fine. It’s important to steadily monitor your lung function. And be sure to get your annual flu vaccine in the fall to help prevent infections that can worsen your COPD. Ask your doctor when you need the pneumococcal vaccine. Let your doctor know if you have worsening symptoms or you notice signs of infection.
Surgery
Surgery is an option for some people with some forms of severe emphysema who aren’t helped sufficiently by medications alone.
Some people with COPD will experience fewer or less severe symptoms and be more active after surgery, but others will not benefit. Some considerations for surgery candidates include:
- You must be strong enough to have the surgery.
- You must participate in a pulmonary rehabilitation program.
- You cannot be a current smoker.
Some lung surgeries require that the lung damage must be in an area that is localized (a specific area) and can be removed. The decision for surgery is based on the results of many tests. Talk to your doctor to find out if lung surgery is right for you.
Surgical options include:
- Lung volume reduction surgery. In this surgery, your surgeon removes small wedges of damaged lung tissue from the upper lungs. This creates extra space in your chest cavity so that the remaining healthier lung tissue can expand and the diaphragm can work more efficiently. In some people, this surgery can improve quality of life and prolong survival.
- Lung transplant. Lung transplantation may be an option for certain people who meet specific criteria. Transplantation can improve your ability to breathe and to be active. However, it’s a major operation that has significant risks, such as organ rejection, and it’s necessary to take lifelong immune-suppressing medications.
- Bullectomy. Large air spaces (bullae) form in the lungs when the walls of the air sacs are destroyed. These bullae can become very large and cause breathing problems. In a bullectomy, doctors remove bullae from the lungs to help improve air flow.
- Endobronchial valve placement through bronchoscopy is under investigation as an alternative to Lung Volume Reduction Surgery. These valves are unidirectional and allow exhalation but do not allow inhalation. This results in a deflated lung distal to the valve. Bronchi are chosen to isolate segments of the lung that show the greatest emphysema and hyperinflation. The benefit, similar to Lung Volume Reduction Surgery, is obtained by decreasing the volume of most diseased portions of the lung. The Endobronchial Valve for Emphysema Palliation Trial (VENT) studied the safety and efficacy of this approach in a nonblinded, prospective, randomized multicenter study. Results showed a modest but significant improvement in both the FEV 1 (relative increase, 6.8%) and 6-minute walk test (relative increase, 19.1 m) in the study group. Analysis revealed that the greatest benefit was obtained by those patients with greater heterogeneity of emphysema and intact interlobar fissures. The study group unfortunately also showed significantly higher rates of COPD exacerbations and hemoptysis 9.
Lung Transplants
Sometimes COPD can cause severe damage to the lungs, causing them not to function normally. Your doctor may recommend a lung transplant if the damage is not repairable. Lung transplants can improve your ability to breathe and be active. However, like any major operation, you should consider the risks and complications, such as organ rejection or needing to take immune suppressing medications daily. Talk to your doctor to find out more information about how and where to receive a lung transplant evaluation or the process for becoming an organ donor.
Lung transplantation provides improved quality of life and functional capacity but does not result in survival benefit. The lack of survival benefit makes the timing of transplant difficult. The patients selected to receive transplants should have a life expectancy of 2 years or less. Current guidelines by the International Society of Heart and Lung Transplantation recommends referring for transplantation when the BODE index (body mass index, obstruction [FEV1], dyspnea [ie, Medical Research Council Dyspnea Scale], and exercise capacity [ie, 6-min walking distance]) is greater than 5 10.
Palliative Care and COPD
Palliative care is a specialty in medicine focused on treating the symptoms, pain and stress that accompany serious illnesses like COPD. It is available to you from the moment you are diagnosed and through the entire course of your illness. The goal of palliative care is to help you and your family, achieve the highest quality of life. Palliative care is appropriate for all people living with COPD regardless of stage or prognosis.
If you or a loved one has COPD, palliative care can help you in several ways including:
- Therapies to relieve the discomfort of shortness of breath or anxiety
- Education about lifestyle changes during COPD
- Medication and disease management
What Are the Benefits of Palliative Care ?
Palliative care improves quality of life by relieving overwhelming physical and emotional symptoms and improving communication with your healthcare providers.
Who Administers Palliative Care ?
Palliative care specialists include a team of doctors, nurses and social workers. Your other doctors and nurses will work to alleviate your symptoms, but palliative care specialists ensure that the goals of COPD care match your specific expectations.
How Do I Get Palliative Care ?
Anytime is the best time to discuss palliative care during your journey in COPD care. Never fear that it is too late to seek out a palliative care specialist. Ask your doctor for a palliative care referral, or you can search for a palliative care team at GetPalliativeCare.org 11.
- Haruna A, Muro S, Nakano Y, Ohara T, Hoshino Y, Ogawa E, et al. CT scan findings of emphysema predict mortality in COPD. Chest. 2010 Sep. 138(3):635-40.[↩]
- Deaths from chronic obstructive pulmonary disease–United States. https://www.cdc.gov/nchs/fastats/copd.htm[↩]
- Crothers K, Butt AA, Gibert CL, Rodriguez-Barradas MC, Crystal S, Justice AC. Increased COPD among HIV-positive compared to HIV-negative veterans. Chest. 2006 Nov. 130(5):1326-33.[↩]
- Stop Smoking. http://www.lung.org/stop-smoking/[↩]
- Albert RK, Connett J, Bailey WC, Casaburi R, Cooper JA Jr, Criner GJ, et al. Azithromycin for prevention of exacerbations of COPD. N Engl J Med. 2011 Aug 25. 365(8):689-98.[↩][↩]
- Petty TL. The National Mucolytic Study. Results of a randomized, double-blind, placebo-controlled study of iodinated glycerol in chronic obstructive bronchitis. Chest. 1990 Jan. 97(1):75-83[↩]
- Zheng JP, Wen FQ, Bai CX, Wan HY, Kang J, Chen P, et al. Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON): a randomised, double-blind placebo-controlled trial. Lancet Respir Med. 2014 Mar. 2(3):187-94.[↩]
- American Thoracic Society/European Respiratory Society statement: standards for the diagnosis and management of individuals with alpha-1 antitrypsin deficiency. Am J Respir Crit Care Med. 2003 Oct 1. 168(7):818-900.[↩]
- Sciurba FC, Ernst A, Herth FJ, Strange C, Criner GJ, Marquette CH, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med. 2010 Sep 23. 363(13):1233-44.[↩]
- Sciurba FC, Ernst A, Herth FJ, Strange C, Criner GJ, Marquette CH, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med. 2010 Sep 23. 363(13):1233-44[↩]
- Center to Advance Palliative Care. https://getpalliativecare.org/[↩]





{kind=link}