Cutaneous lupus erythematosus
Cutaneous lupus erythematosus (CLE) is a form of lupus that mainly affects your skin, but cutaneous lupus can often be seen in the absence of systemic lupus erythematosus (SLE) 2, 3, 4, 5, 6, 7, 8, 9, 10, 11.
Cutaneous lupus erythematosus (CLE) is an autoimmune disease (a chronic recurrent autoimmune disease) with multiple clinical signs and symptoms ranging from an isolated skin disease to systemic disease with systemic involvement such as systemic lupus erythematosus (SLE) 6. 3. Up to 75% of patients with SLE develop cutaneous lupus, and cutaneous lupus erythematosus (CLE) may be the first indication of SLE in 25%. Cutaneous lupus erythematosus is not hereditary or contagious.
The exact cause of cutaneous lupus erythematosus is unknown, but it is believed that the cause of cutaneous lupus erythematosus is multifactorial where a combination of genetic susceptibility and environmental factors in association with innate and adaptive immune responses results in cutaneous lupus erythematosus 3, 4, 12, 13, 5, 6, 7, 8, 9, 14, 15, 16, 10, 11:
- Genetic susceptibility
- High incidence among family members
- Environmental factors
- Cigarette smoking
- Sun exposure
- Medications
- Innate and adaptive immune responses
- Autoantibodies.
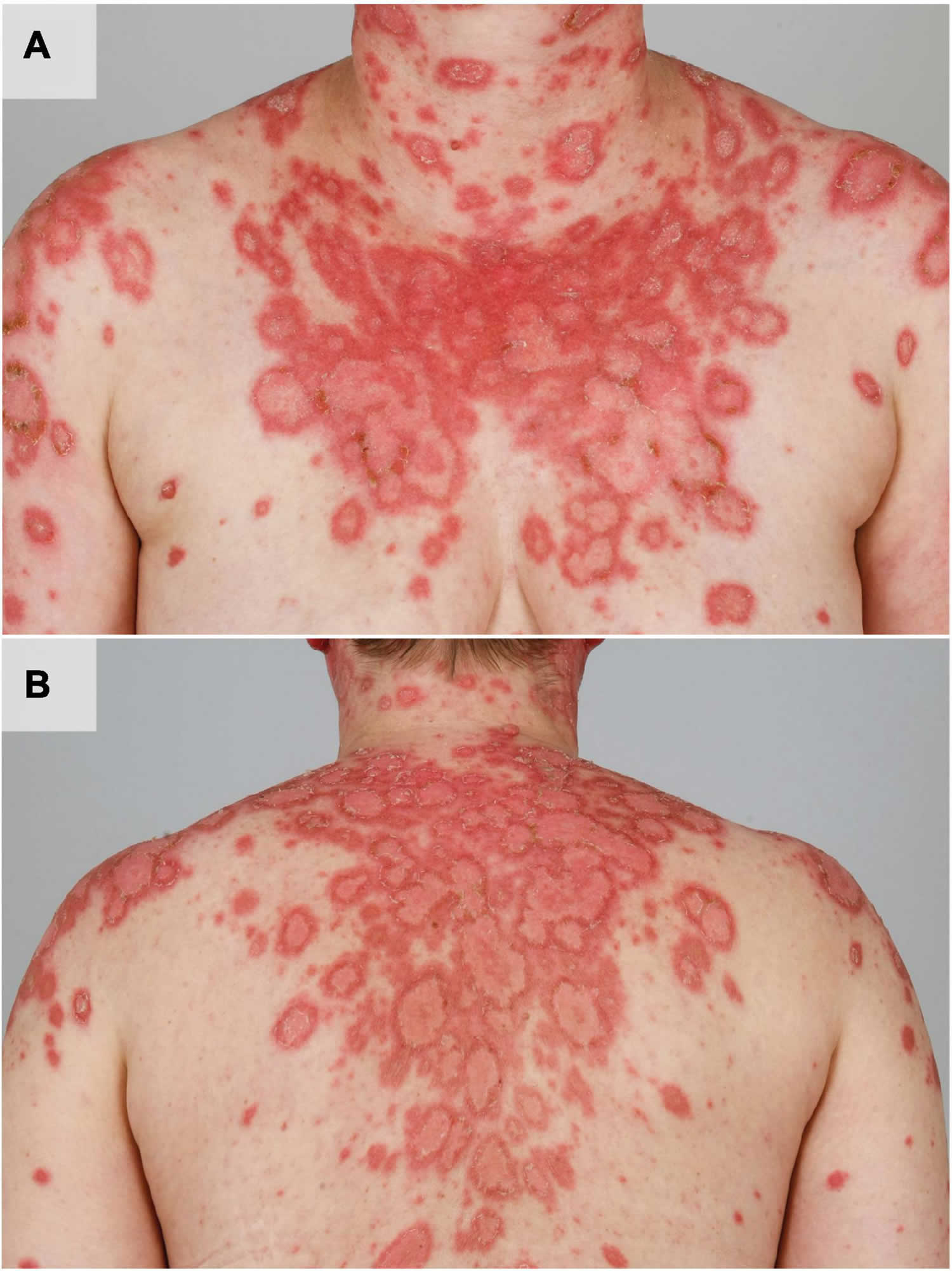
Ultraviolet (UV) light can cause a deterioration of skin lesions as well as flares of systemic lupus erythematosus (SLE) (Figures 1A,B) 17. Multiple immune cells are involved in the development of cutaneous lupus erythematosus (CLE) lesions after UV irradiation and lead to further recruitment of the adaptive immune system via release of various mediators such as type 1 interferons (IFN) 12. Recently, activation of type 1 IFNs after UV irradiation has been linked with activation of cyclic GMP-AMP-synthase (cGAS) 18. Upon T cell stimulation, B cells are recruited to the dermal compartment and produce autoantibodies. These autoantibodies are directed in particular against nucleic acids and nucleosome components, contributing to disease progression 19. UV light can also lead to increased antigen presentation and increased apoptosis in lupus erythematosus 20, 21. The cellular debris that develops after exposure to UV irradiation can accumulate and additionally lead to further immune stimulation 22.
Cigarette smoking is more common in patients with cutaneous lupus erythematosus than healthy population, with a prevalence of 60–80%. Current smokers demonstrate increased disease activity and damage, and a more pronounced effect on quality of life. Despite previous reports that smoking interferes with antimalarial efficacy in cutaneous lupus erythematosus, it is more likely that this reflects increased disease activity in this group.
Cutaneous lupus erythematosus (CLE) has an annual incidence of 4 to 4.3 cases per 100,000 people, and a prevalence of 73 cases per 100,000 23, 24, 25. As with SLE, there is a marked female predominance (female:male ratio of 9:1–10:1) with cutaneous lupus erythematosus particularly affecting women 20 to 50 years of age 23, 24, 26. However, all age groups and both sexes can be affected. Skin of color is an important predisposing factor.
There are several types of cutaneous lupus. The most common types of cutaneous lupus erythematosus are acute cutaneous lupus erythematosus (ACLE), subacute cutaneous lupus erythematosus (SCLE), intermittent cutaneous lupus (lupus erythematosus tumidus) and chronic cutaneous lupus erythematosus (CCLE) such as discoid lupus erythematosus (DLE), lupus profundus and chilblain lupus erythematosus 27, 11. The most common subtype of cutaneous lupus erythematosus is discoid lupus erythematosus (DLE), which accounts for 80% of cases 23.
A small percentage of cutaneous lupus erythematosus patients subsequently develop systemic signs and symptoms. In a previous study, 24% of cutaneous lupus erythematosus patients had already been diagnosed with SLE at the time they were diagnosed with cutaneous lupus erythematosus, and an additional 18% were diagnosed with SLE within three years of being diagnosed with cutaneous lupus erythematosus, with the probability of SLE progression being highest for the patients with subacute cutaneous lupus erythematosus (SCLE) 23. Another study showed that 12.2% of cutaneous lupus erythematosus patients underwent disease progression to SLE within four decades 25.
Currently, due to the lack of understanding the cause of cutaneous lupus erythematosus, there is no treatment specifically approved for cutaneous lupus erythematosus. Topical and systemic medications are used off label. The main goals of treatment are to reduce symptoms and the appearance of the rash as well as prevent long-term complications such as scarring and hair loss (alopecia).
General measures are important in the treatment of all forms of cutaneous lupus erythematosus. These include strict sun protection which should always include avoiding direct sunlight (e.g. by seeking out shade, wearing tightly woven longer sleeve clothing, broad brimmed hats and sunglasses) and wearing a broad spectrum SPF 50+ sunscreen. Ask your dermatologist for further advice. Avoiding soaps which can further dry and irritate the skin and using a good moisturiser regularly is important. Camouflaging the lesions with makeup may be beneficial in discoid lupus erythematosus (DLE). Stopping smoking also helps improves most cases of cutaneous lupus erythematosus.
Topical treatments for cutaneous lupus erythematosus include topical steroids and non-steroid based anti-inflammatory ointments (e.g. pimecrolimus or tacrolimus).
Oral medications may be needed to treat cutaneous lupus erythematosus. Hydroxychloroquine, an antimalarial tablet, has been used for many years to treat most forms of cutaneous lupus erythematosus. Oral medications that suppress the immune system such as azathioprine, methotrexate, cyclosporin or mycophenolate mofetil may also be used in cutaneous lupus erythematosus.
Specific treatments for discoid lupus erythematosus (DLE) include oral retinoid medications such as acitretin or isotretinoin or physical treatments such as steroid injections.
Figure 1. Cutaneous lupus erythematosus (CLE)
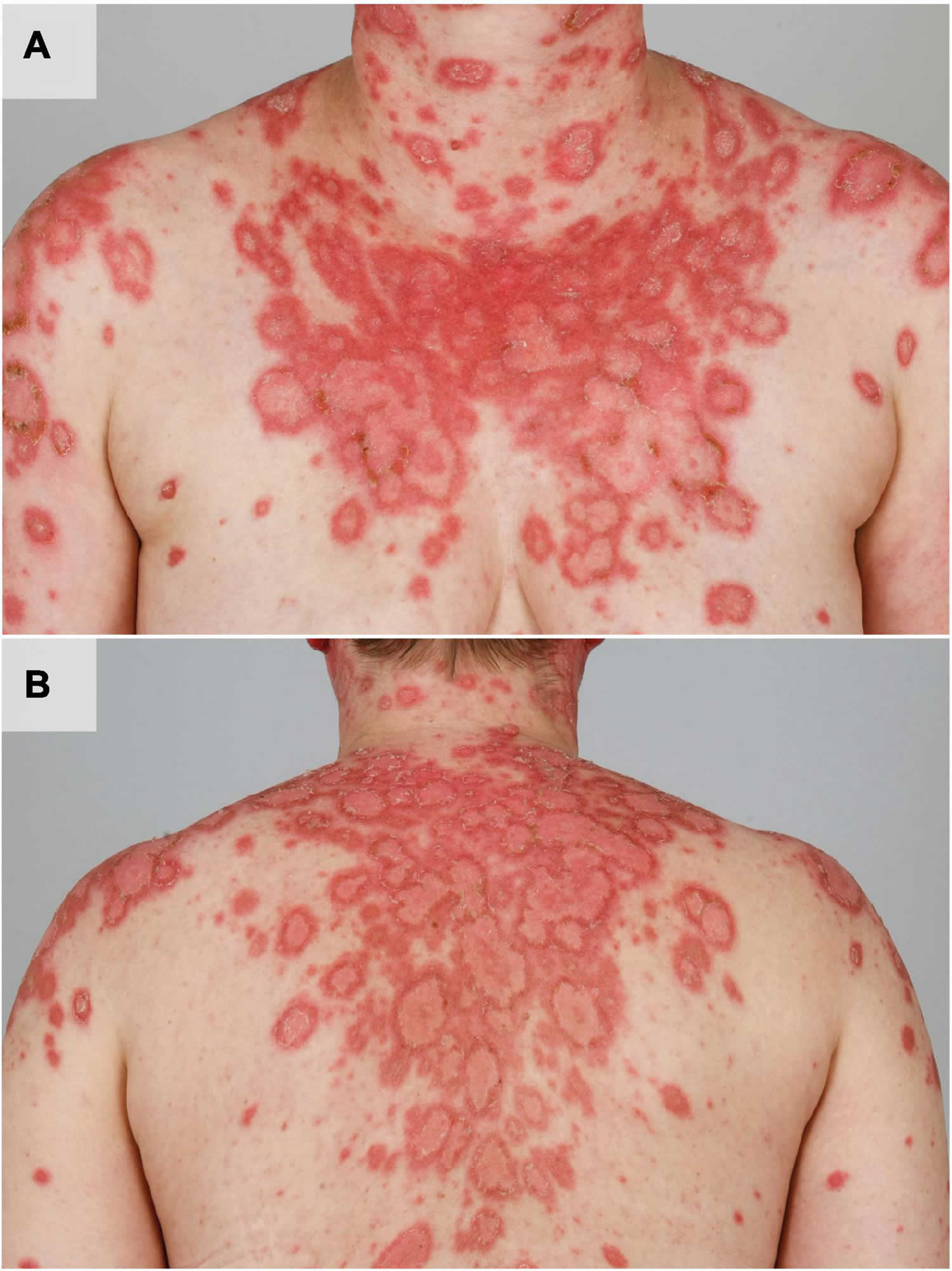
Footnotes: Ultraviolet (UV) induced acute flare of subacute cutaneous lupus erythematosus in a female patient with systemic lupus erythematosus (SLE). The patient shows multiple disseminated reddish, angular and scaly plaques in photo distributed areas such as the shoulders, upper arms, cleavage, neck (A) and the back (B).
[Source 12 ]Figure 2. Cutaneous lupus erythematosus types
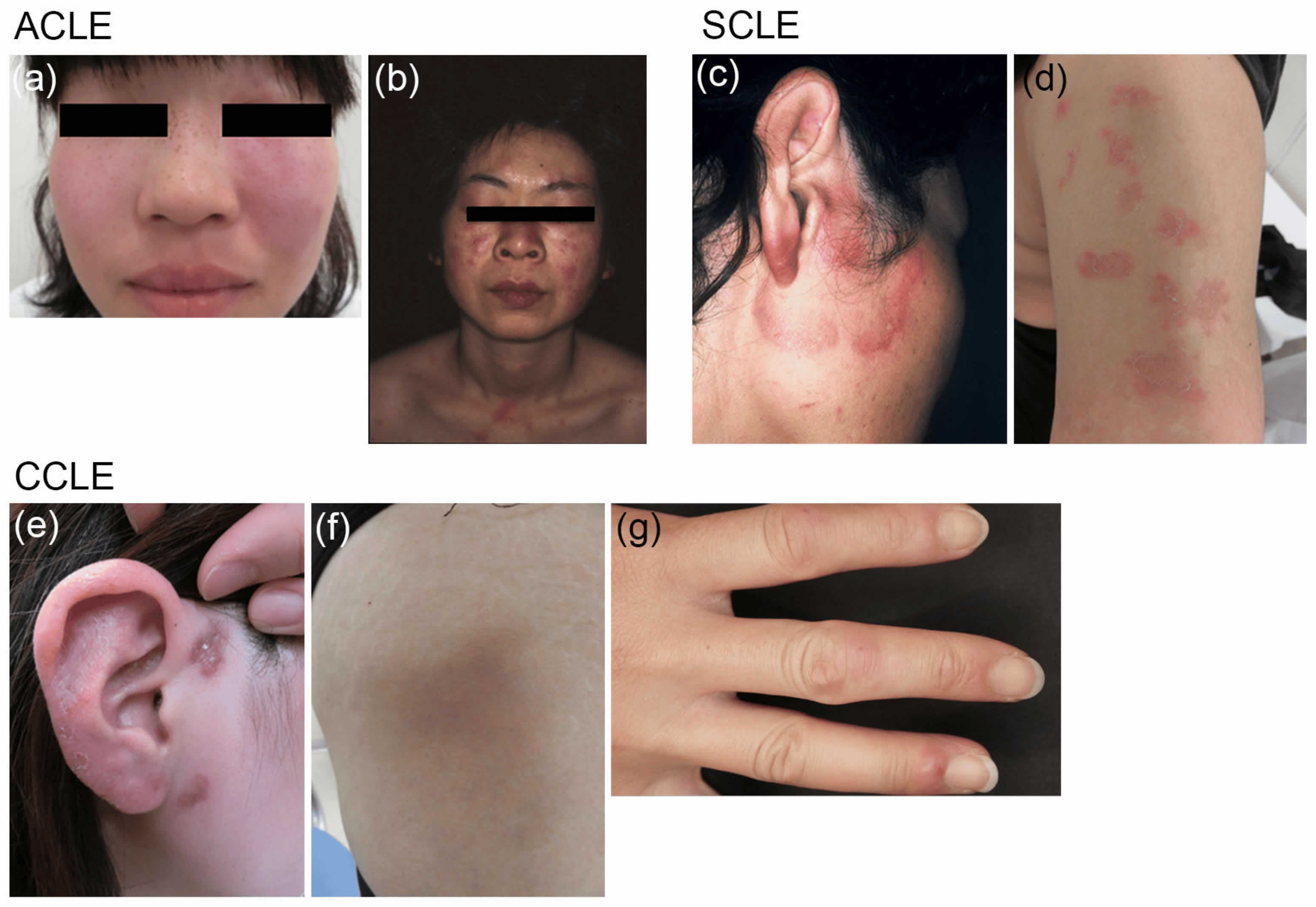
Footnotes: Typical clinical presentations of three subtypes of cutaneous lupus erythematosus (CLE). (a) Acute cutaneous lupus erythematosus (ACLE) with malar rash or butterfly rash on the face; (b) Acute cutaneous lupus erythematosus (ACLE) with widespread indurated erythema on the face, neck, upper chest, and shoulders. (c) Subacute cutaneous lupus erythematosus (SCLE) with annular-polycyclic lesions on the face; (d) Subacute cutaneous lupus erythematosus (SCLE) with papulosquamous or psoriasiform lesions on the upper arm. (e) Chronic cutaneous lupus erythematosus (CCLE) with scar-causing discoid lupus erythematosus (DLE) lesions on the face; (f) Lupus erythematosus profundus on the thigh, showing depressions; (g) Chilblain lupus erythematosus on the fingers, resembling frostbite.
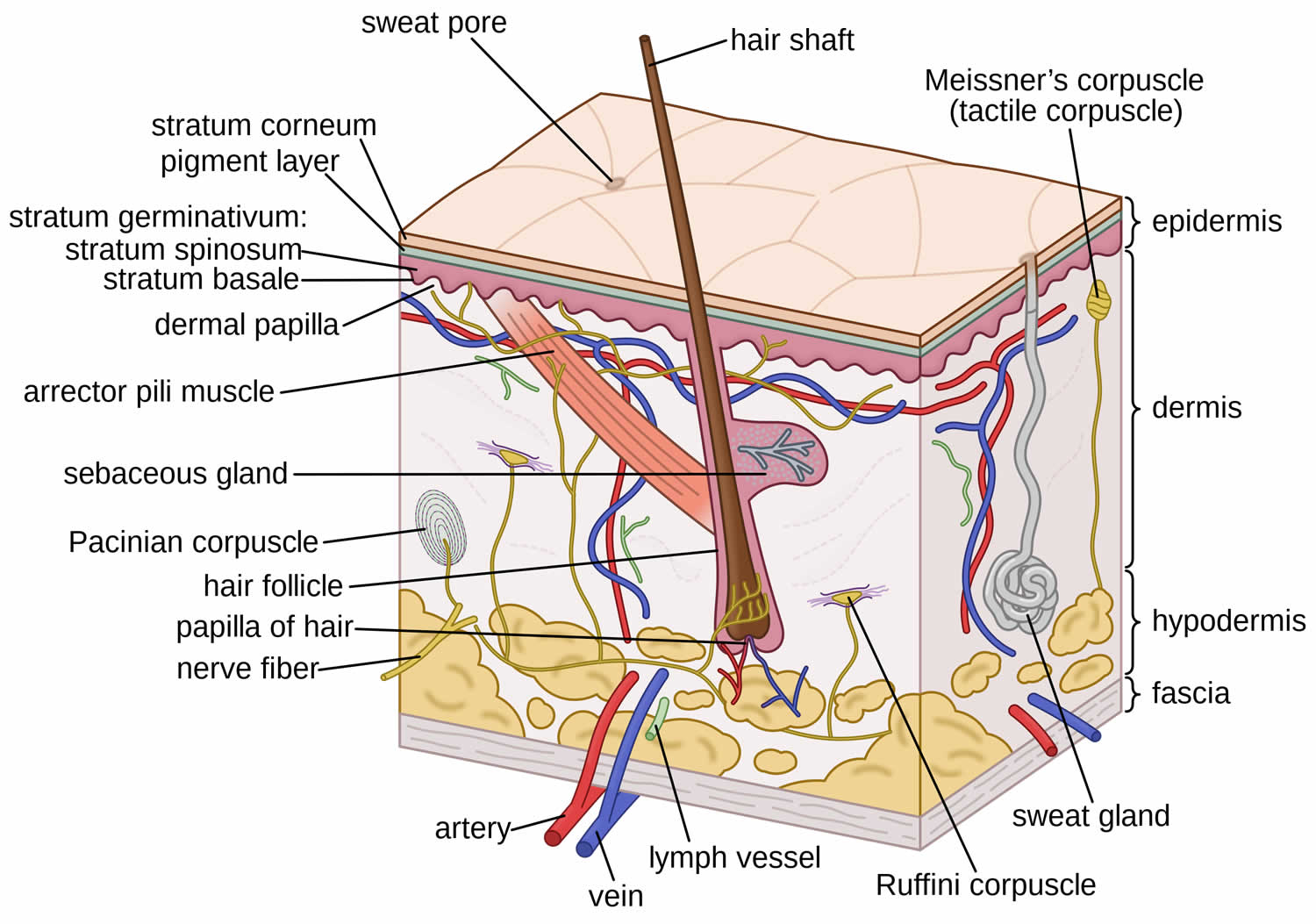
[Source 28 ]Figure 3. Skin structure and function
Cutaneous lupus erythematosus types
According to the Düsseldorf classification, cutaneous lupus erythematosus (CLE) is classified as 29, 30, 31, 32, 33, 34, 35:
- Acute cutaneous lupus erythematosus (ACLE)
- Localized (malar rash)
- Generalized
- Subacute cutaneous lupus erythematosus (SCLE)
- Annular
- Papulosquamous
- Intermittent cutaneous lupus erythematosus (ICLE) also known as lupus tumidus or lupus erythematosus tumidus (LET)
- Chronic cutaneous lupus erythematosus (CCLE)
- Discoid lupus erythematosus (DLE)
- Localized
- Generalized
- Lupus profundus also known as lupus erythematosus profundus or lupus panniculitis
- Chilblain lupus erythematosus
- Hypertrophic chronic cutaneous lupus erythematosus
- Mucocutaneous chronic cutaneous lupus erythematosus
- Discoid lupus erythematosus (DLE)
Each of of these cutaneous lupus erythematosus subtypes is subdivided on the basis of their clinical, laboratory, and histological features and how long the skin lesions last 36, 37, 34. The most common subtype of cutaneous lupus erythematosus is discoid lupus erythematosus (DLE), which accounts for 80% of cases 23.
Acute cutaneous lupus erythematosus
Acute cutaneous lupus erythematosus (ACLE) is almost always associated with systemic disease. Acute cutaneous lupus erythematosus (ACLE) typically presents as transient red patches associated with a flare of systemic lupus erythematosus (SLE) and the most typical patient is a fair-skinned female in her 30s 38.
Acute cutaneous lupus erythematosus skin changes:
- Localized acute cutaneous lupus erythematosus: malar ‘butterfly’ rash – redness and swelling over both cheeks, sparing the nasolabial folds, lasting hours to days
- Generalized acute cutaneous lupus erythematosus: diffuse or papular erythema of the face, upper limbs (sparing the knuckles), and trunk resembling a morbilliform drug eruption or viral exanthem
- Toxic epidermal necrolysis-like acute cutaneous lupus erythematosus: is associated with lupus nephritis or cerebritis, and must be distinguished from drug-induced toxic epidermal necrolysis in a patient with SLE.
Acute cutaneous lupus erythematosus lesions can be localized (concentrated above the neck) or generalized. Malar rash or butterfly reddish patch is the most typical localized lesion, a reddish patch and/or swelling over the malar eminence with a tendency to spare the nasolabial folds; it often comes after sun exposure. The lesions last for hours to days. Postinflammatory hyperpigmentation is common but scarring does not occur 38, 39.
The generalized form of acute cutaneous lupus erythematosus is more uncommon but it is also associated with a previous sun exposure and preferably located to sun-exposed areas 40, 41, 42, 43.
Figure 4. Acute cutaneous lupus erythematosus (ACLE)
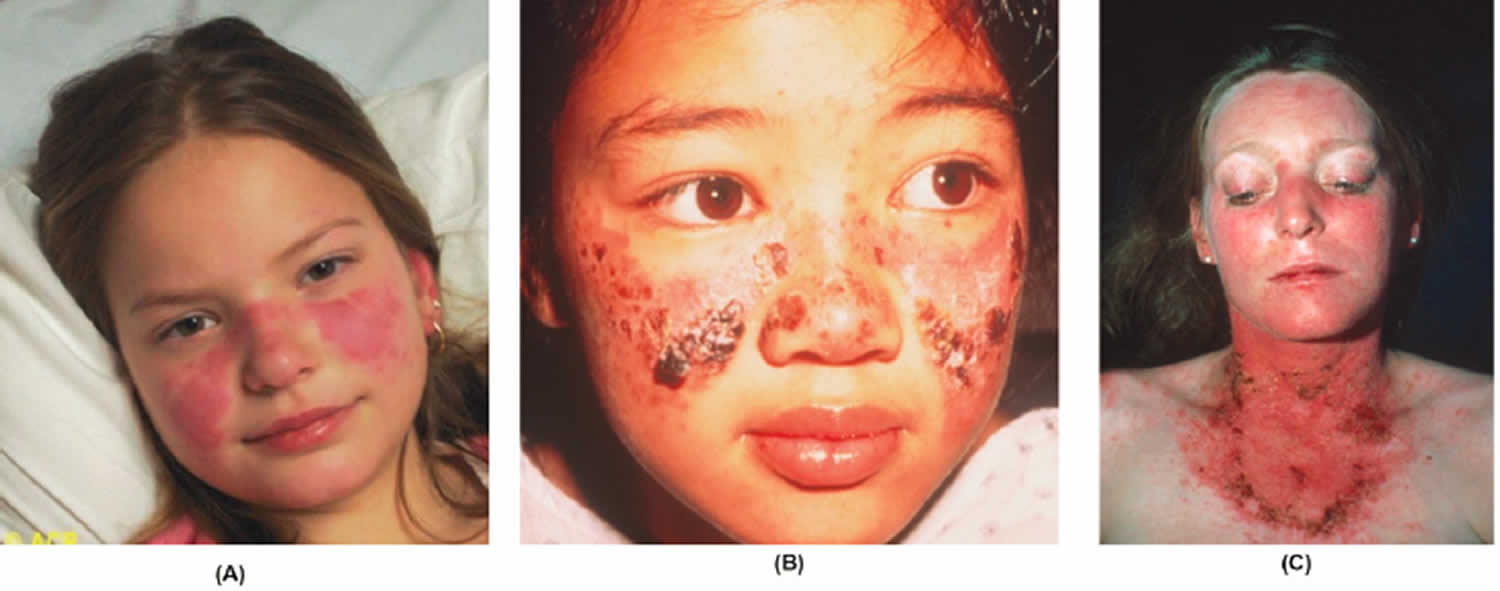
Footnotes: Acute cutaneous lupus erythematosus manifestations: (A) localized; (B) malar; and (C) generalized.
[Source 44 ]Subacute cutaneous lupus erythematosus
Subacute cutaneous lupus erythematosus (SCLE) is a subtype of cutaneous lupus erythematosus (CLE). Subacute cutaneous lupus erythematosus (SCLE) comprises 10 to 15% of cutaneous lupus erythematosus presentations. Subacute cutaneous lupus erythematosus (SCLE) presents as a widespread non-scarring photosensitive rash 45. The skin changes are more persistent than those of acute cutaneous lupus erythematosus (ACLE). Around 50% of patients with subacute cutaneous lupus erythematosus (SCLE) meet the American College of Rheumatology criteria for the diagnosis of mild systemic lupus erythematosus (SLE) 45.
Subacute cutaneous lupus erythematosus (SCLE) affects about 10% of all patients with systemic lupus erythematosus (SLE) 45:
- Patients can be of any age, sex, or ethnicity. However, SCLE is most often diagnosed in middle-aged women.
- In North America, subacute cutaneous lupus erythematosus is more common in Caucasians than other ethnicities.
- It can be associated with other diseases, including Sjögren syndrome, rheumatoid arthritis, and Crohn disease.
Subacute cutaneous lupus erythematosus (SCLE) is believed to be caused by genetic and environmental factors. Subacute cutaneous lupus erythematosus (SCLE) is associated with the human leukocyte antigen (HLA)-A1-B8-DR3-DQ2-DRw52-C4null ancestral haplotypes. Other genetic associations include:
- Deficiencies in complement proteins component (C)2 and C4
- Polymorphisms in the tumour necrosis factor (TNF)-alpha promoter gene.
Exposure to environmental triggers such as exposure to ultraviolet (UV) radiation or photosensitizing drugs causes lost of immune tolerance or autoimmune disorder. Exposure to ultraviolet (UV) radiation results in increased expression of the Ro/SSA antigen (Sjögren’s syndrome-related antigen A) on the surface of keratinocytes, binding the anti-Ro/SSA antibody and leading to the disease 46, 35. A pregnant woman who is Ro/SSA antibody-positive has a risk of delivering an infant suffering from neonatal lupus erythematosus (8–10%) and congenital heart block (1–2%) 45, 47, 48, 49, 50.
It is estimated 20 to 40% of cases of subacute cutaneous lupus erythematosus (SCLE) are drug-induced subacute cutaneous lupus erythematosus (DI-SCLE). The incubation time widely varies from a few days such as in the case of the chemotherapy agents capecitabine and paclitaxel, to years before the onset of the rash (eg, a case was reported to arise 5 years after starting a thiazide diuretic).
The drugs most commonly associated with subacute cutaneous lupus erythematosus are:
- Thiazide diuretics
- Terbinafine
- Calcium channel blockers.
Other drugs that may cause subacute cutaneous lupus erythematosus include:
- Tamoxifen
- Lansoprazole
- Statins
- Angiotensin-converting enzyme (ACE) inhibitors
- TNF-alpha inhibitors
- Leflunomide
- Carbamazepine
- Docetaxel
- Paclitaxel
- Capecitabine
- Inhaled tiotropium
- Naproxen.
There are also increasing reports of subacute cutaneous lupus erythematosus being temporally associated with underlying cancers, including carcinoma of the lung, esophagus, prostate, cholangiocarcinoma, and B-cell lymphoma.
Subacute cutaneous lupus erythematosus (SCLE) most often presents as a non-scarring papulosquamous eruption:
- Typically, there are annular plaques with raised reddish borders and central clearing.
- The plaques fuse to form polycyclic patterns.
- They may or may not have an overlying scale.
- Sometimes, there are peripheral vesicles, crusting, and bullae.
- The rash is typically symmetrically distributed on the sun-exposed sites of the neck, the upper trunk, and the outer arms, triggered or aggravated by sun exposure.
- The face is usually unaffected.
- Lesions resolve with post-inflammatory hypopigmentation and telangiectases, but no scarring; normal pigmentation recovers over time.
Other lupus-associated findings in patients with subacute cutaneous lupus erythematosus include:
- Diffuse non-scarring hair loss (50%)
- Mouth ulcers
- Livedo reticularis
- Periungual telangiectasia.
Drug-induced lupus can be indistinguishable from the non-drug-induced form of subacute cutaneous lupus erythematosus. Specific features of drug-induced subacute cutaneous lupus erythematosus (DI-SCLE) include:
- Usually presenting in older patients
- Association with a likely drug
- Malar rash
- Involvement of the legs
- Bullous, targetoid, or vasculitic variants.
Subacute cutaneous lupus erythematosus (SCLE) can be diagnosed clinically, supported by the results of blood tests and a skin biopsy.
- Around 60% of patients with subacute cutaneous lupus erythematosus (SCLE) are antinuclear antibody (ANA) positive
- More than 80% are Ro/SSA antibody positive
- La/SSB, dsDNA, anti-histone, and Sm antibodies are less common.
The histology on biopsy can resemble other forms of cutaneous lupus erythematosus.
- There is a lymphocytic interface dermatitis with basal layer degeneration.
- Epidermal atrophy and apoptotic keratinocytes are more prominent than in discoid lupus erythematosus (DLE).
- Perivascular and periadnexal lymphocytic infiltrate, follicular plugging, basement membrane thickening, and dermal mucin are less prominent than in DLE.
- Direct immunofluorescence reveals a granular deposition of immunoglobulin (Ig)G, IgM, and C3 along the dermal–epidermal junction in approximately two-thirds of patients with subacute cutaneous lupus erythematosus (SCLE) (the lupus band test).
Drug-induced subacute cutaneous lupus erythematosus (DI-SCLE) and non-drug-induced SCLE cannot be distinguished on histology.
Figure 5. Subacute cutaneous lupus erythematosus (SCLE)

Footnotes: Three patients with proton pump inhibitor (PPI) induced subacute cutaneous lupus erythematosus (SCLE). (a) Papulosquamous subacute cutaneous lupus erythematosus; (b,c) annular and polycyclic subacute cutaneous lupus erythematosus; and (d) targetoid lesions.
[Source 51 ]Subacute cutaneous lupus erythematosus treatment
Sun protection is crucial in subacute cutaneous lupus erythematosus (SCLE).
- Seek shade when outdoors.
- Wear covering, sun-protective clothing.
- Apply a broad-spectrum sunscreen to uncovered areas.
- Topical therapy may include:
- Topical steroids
- Topical calcineurin inhibitors (tacrolimus ointment and pimecrolimus cream).
The main treatment for subacute cutaneous lupus erythematosus (SCLE) is an antimalarial drug, particularly hydroxychloroquine. Antimalarial drugs are less effective in smokers.
In approximately 25% of cases, another agent is required, such as:
- An oral corticosteroid
- An oral retinoid (acitretin or isotretinoin)
- Dapsone
- Methotrexate
- Mycophenolate
- Etanercept
- Thalidomide.
Subacute cutaneous lupus erythematosus (SCLE) generally responds well to treatment, although it may flare up again each summer.
Approximately 10 to 15% of patients with subacute cutaneous lupus erythematosus (SCLE) develop SLE, including kidney and neurological involvement.
Drug-induced subacute cutaneous lupus erythematosus (DI-SCLE) can be slow to resolve on stopping the causative drug (one study found resolution took a mean of 7 weeks).
Intermittent cutaneous lupus erythematosus
Intermittent cutaneous lupus erythematosus is better known as lupus tumidus or lupus erythematosus tumidus (LET), a dermal form of lupus erythematosus. Lupus erythematosus tumidus occurs predominantly on sun exposed areas. Sometimes the skin lesions have an annular or semi-annular (“arciform”) appearance but there are no epidermal changes and therefore no scale, ulceration or crust formation. Every lesion heals without scarring or postinflammatory hyper- or hypopigmentation and therefore lupus tumidus does not result in chronic skin damage 52.
Skin lesions of lupus tumidus:
- Occur on sun-exposed areas of skin, such as the face, neck, and upper anterior chest
- Present as red, round or annular, papules and plaques with a smooth surface
- Resolve in winter without scarring.
To date, no distinct cause for lupus tumidus has been identified. However, triggering factors such as ultraviolet (UV) radiation have been implicated in worsening lesions of lupus erythematosus tumidus. Its association with autoimmune disease has been controversial; if an autoimmune disease is suspected, an autoimmune workup may be initiated 53, 54. Immunity dysregulation with suppression of T cells is hypothesized 55. Association with smoking and drugs like tumor necrosis factor antagonists, monoclonal antibodies, angiotensin-converting enzyme inhibitors, thiazide diuretics, and highly active antiretroviral therapy was reported 56, 57.
The high photosensitivity of lupus tumidus patients and the evolution of standardized photoprovocation protocols has helped to improve the scientific evaluation and identification of the disease in recent years 58, 59, 60. The development of histologic and immunohistologic evaluation procedures supported important similarities with other forms of cutaneous lupus erythematosus and has resulted in a better differentiation of lupus erythematosus tumidus from other cutaneous lupus erythematosus subtypes at the microscopic level 61, 62, 63. This has substantially increased awareness of lupus erythematosus tumidus, resulting in a higher reporting rate in the literature.
Lupus tumidus has a benign course 64. Solitary lesions are mostly self-limiting, often without any need for topical or systemic therapy. However, recurrence is noted to be high with the disease-free period in between. Long-term remission is observed in some patients 65. Lupus erythematosus tumidus lesions have a favorable prognosis than lesions of discoid lupus erythematosus or subacute cutaneous lupus erythematosus 65. Spontaneous resolution of the lesions without residual dyspigmentation or scarring may be noted within days or weeks, despite the relapses 66, 67. Sun protection alone was effective for lesion resolution in more than 50% of patients without any symptoms 68. However, avoiding sun exposure might cause vitamin D deficiency in some patients. Therefore, evaluation of the vitamin D deficiency with 25-hydroxyvitamin D level and adequate supplementation with at least 400 IU of cholecalciferol is suggested 69, 70.
Figure 6. Lupus erythematosus tumidus

Footnote: Lupus erythematosus tumidus: reddish, urticarial plaque and papules on the neck of a 43-year old male smoker.
[Source 64 ]Lupus tumidus treatment
Sun protection and topical or intralesional corticosteroids are first-line therapy for localized lupus erythematosus tumidus 71. Application of water-resistant sunscreen with a sun protection factor of 30 or higher (SPF 30+), using protective clothing, avoiding peak sun exposure, and smoking cessation are recommended. Corticosteroids are applied topically twice a day for 2-4 weeks. Clinical improvement is usually observed in about 2 weeks. Moderate to high potency corticosteroids are used for treating lesions on the trunk or extremities and low potency corticosteroids are used for the treatment of facial lesions. Cutaneous atrophy, striae, hypopigmentation, and telangiectasias are adverse effects of topical or intralesional corticosteroids. If there is no improvement in 4 weeks, other therapies should be tried. For solitary and thick lupus erythematosus tumidus lesions, intralesional triamcinolone (2.5 to 5 mg/mL) is often effective. 0.1 ml of triamcinolone acetonide can be injected into the lesion at multiple sites 1 cm apart. Intralesional injection can be repeated in 4 weeks. If there is no improvement in 8-12 weeks, intralesional corticosteroids are discontinued. Topical calcineurin inhibitors (e.g., tacrolimus, pimecrolimus) improve the lesions clinically, while decreasing the topical corticosteroid use 72. Atrophy of the skin is not caused by topical calcineurin inhibitors, making them ideal for maintenance therapy.
Patients with limited lupus erythematosus tumidus refractory to topical therapy and patients with extensive lupus tumidus should be treated with first line antimalarial therapy. Hydroxychloroquine or chloroquine can be used initially. Hydroxychloroquine is usually well tolerated than chloroquine. Between 200 and 400 mg per day of hydroxychloroquine is a reasonable dose. For chloroquine, a dose of 125 to 250 mg per day (for 5 to 7 days per week) is commonly used. Hydroxychloroquine and chloroquine may not be used in combination due to the risk of retinal toxicity. Their risk of retinal toxicity limits the maximal dose of these antimalarials. It is important to note that it may take 8 to 12 weeks to appreciate the effects of antimalarials 73. Patients should have an eye exam at baseline and then periodically while on the antimalarials. Patients need to be aware of the skin depigmentation that can occur with both hydroxychloroquine and chloroquine. This presents as a blue-gray discoloration on the shins, palate, nails, or face, and this discoloration may be permanent. Gastrointestinal side effects are the most common reason for discontinuation of antimalarial treatment. Neuromuscular and hematological side effects are also noted.
Lupus tumidus refractory to antimalarial therapy is rare. However, second-line therapy includes methotrexate (7.5 to 25 mg once weekly) or mycophenolate mofetil (1 to 3 gm per day). Folic acid 1 mg per day typically lessens the severity of the side effects associated with methotrexate. Side effects of methotrexate include gastrointestinal upset, pulmonary fibrosis, bone marrow suppression, alopecia, apart from being teratogenic. Mycophenolate mofetil’s side effects include gastrointestinal upset, reversible cytopenias, immunosuppression, gastrointestinal perforation or ulcer, hypercholesterolemia, and hypertension. Clinical improvement is usually observed with 2-3 months of therapy.
Third-line treatment options, although uncommonly used, include thalidomide and lenalidomide. Thalidomide (50 to 100 mg daily), lenalidomide (5 to 10 mg daily) are used at least for a month for clinical response. Teratogenicity, neuropathy, thromboembolism, sedation are some of the adverse effects associated with the use. Treatment regimens are usually tapered to the lowest potent dose to maintain remission.
Chronic cutaneous lupus erythematosus
Chronic cutaneous lupus erythematosus (CCLE) is the most common form of cutaneous lupus erythematosus and about 25% of SLE patients have some form of chronic cutaneous lupus erythematosus (CCLE).
Chronic cutaneous lupus erythematosus (CCLE) comprises three major clinical variants:
- Discoid lupus erythematosus (DLE)
- Lupus profundus also known as lupus erythematosus profundus or lupus panniculitis
- Chilblain lupus erythematosus (CHLE).
Discoid lupus erythematosus
Discoid lupus erythematosus (DLE) is the most common form of chronic cutaneous lupus erythematosus (CCLE) (80%) and is particularly prevalent and severe in patients with skin of color compared to the European population. Twenty-five percent of patients with SLE may develop typical discoid lupus erythematosus at some point during their illness, and only 1% to 5% of patients with discoid lupus erythematosus may develop SLE 27.
Clinical features of discoid lupus erythematosus (DLE) are discoid, livid-red plaques with deep infiltration and a tendency to scar. These plaques typically present on the face, scalp and neck (localized DLE 60-80% of cases), or lesions both above and below the neck (generalized DLE 20-40% of cases), while association with autoantibodies is rare 74, 75, 76, 46, 35, 77.
Discoid lupus erythematosus (DLE) can affect males and females of any age but occurs more frequently in women in their 20s, 30s, and 40s. Children are rarely affected. The estimated prevalence is around 20–40 people in every 100,000.
70-90% of discoid lupus erythematosus patients suffer from photosensitivity (aggravated by exposure to sunlight) and sun exposed areas such as the scalp, ears and cheeks are most commonly involved areas 78, 74, 40, 79. The lesions start as red maculae or papules with a scaly surface and then grow peripherally into larger discoid plaques that heal with atrophic scar and pigmentary changes (Figure 8). A typical clinical sign is when the keratin accumulates in the hair follicle and when peeled back a follicle-sized keratotic spike can be seen protruding from the under surface of the scale (carpet-tack sign) 78, 40. Mutilation with tissue loss can be seen when the lesions affect the ears and tip of the nose 78.
Discoid lupus erythematosus (DLE) is caused by internal and external factors.
- Internal factors include:
- Genetic predisposition with major histocompatibility complex alleles HLA-DQA1 and DRB1.
- Single nucleotide polymorphism TYK2, IRF5, CTLA4 are also associated.
- Interferon, particularly type 1, is a key cytokine in pathogenesis.
- IRF5 and TYK2 are involved in interferon regulation.
- ITGAM polymorphisms confer a greater risk for discoid lupus erythematosus than systemic lupus erythematosus (SLE).
- External factors include:
- Smoking which is more common in those with discoid lupus erythematosusand which also impairs the efficacy of antimalarials
- Ultraviolet (UV) radiation can provoke discoid lupus erythematosus as it is a photosensitive disorder. However, it can be found in non-sun exposed areas.
Skin lesions of discoid lupus erythematosus (DLE):
- Are most commonly located on the scalp, ears, cheeks, nose, and lips
- Present as destructive scaly plaques with follicular prominence (carpet tack sign) which can result in hair loss with scars (scarring alopecia)
- Heal slowly leaving post-inflammatory dyspigmentation (abnormality in the distribution of pigment in the skin) and scarring.
Discoid lupus erythematosus (DLE) may be localized (above the neck in 80%) or generalized (above and below the neck in 20%). Often the rash is asymptomatic but it can be itchy and sore. Most patients with discoid lupus erythematosus (DLE) only have skin involvement but some have or subsequently develop signs of SLE. Typically, the lesions evolve over time.
Typical signs of localized discoid lupus erythematosus (DLE) include:
- Initial dry red patches evolve to form red plaques with adherent scale. Follicular hyperkeratosis (plugs of keratin within hair follicles) is common. When this scale is removed using sticky tape the horny plugs can be seen giving rise to the “carpet-tack” sign.
- As discoid lupus erythematosus progresses atrophic scarring and scarring hair loss is common. This is associated with hyper- and or hypo- pigmentary change and is especially noticeable in those with skin of color.
- Discoid lupus erythematosus is typically located on the nose, cheeks, ear lobes, and conchal bowl (Shuster sign). It may involve lips, oral mucosa, nose, or eyelids.
Signs of generalized discoid lupus erythematosus (DLE) include:
- The morphology of the lesions is similar to that on the face and scalp but they are distributed widely including the anterior chest, upper back, dorsum of hands and less commonly on the lower limbs, palms, and soles. Rarely, there is involvement of the anogenital mucosa.
Discoid lupus erythematosus is a chronic condition which can last for many years. Discoid lupus erythematosus (DLE) commonly scars causing facial disfigurement and permanent alopecia. Pigmentary change may improve over long periods.
Discoid lupus erythematosus (DLE) can have an impact physically and psychologically affecting the patient’s quality of life. Dermatology Life Quality Index (DLQI) measures matched with Cutaneous Lupus Disease Area and Severity Index (CLASI) measures have shown that quality of life in patients with discoid lupus erythematosus (DLE) is poor.
There is a link between discoid lupus erythematosus (DLE) and systemic lupus erythematosus (SLE). Approximately 5% of patients with localised and 15% with generalized discoid lupus erythematosus develop SLE.
Discoid lupus erythematosus is diagnosed from its distribution and the clinical appearance of the plaques. A patient with discoid lupus erythematosus (DLE) should undergo a complete examination for other signs and symptoms of systemic lupus erythematosus (SLE).
- A skin biopsy usually confirms diagnosis.
- Features vary depending on the stage of the discoid lupus erythematosus (DLE) but include an interface dermatitis also involving hair follicles and a perivascular and peri-appendageal lymphocytic infiltrate in the upper and lower dermis.
- There is epidermal vacuolation and apoptotic basal cells and hyperkeratosis.
- The basement membrane may become thickened and dermal mucin may be present.
- As lesions evolve further, the inflammatory infiltrate subsides and there is dermal fibrosis.
- Blood tests include a full blood count, kidney function, and antinuclear antibodies (ANA). ANA is frequently not detected.
- Urine analysis.
Despite the multiple therapeutic options for discoid lupus erythematosus (DLE), treatment can be difficult.
Squamous cell carcinoma can rarely arise within a longstanding discoid lupus erythematosus plaque in the skin or mucous membrane.
Figure 7. Discoid lupus erythematosus (DLE)

Footnotes: Discoid lupus erythematosus with plaques on beard and scalp.
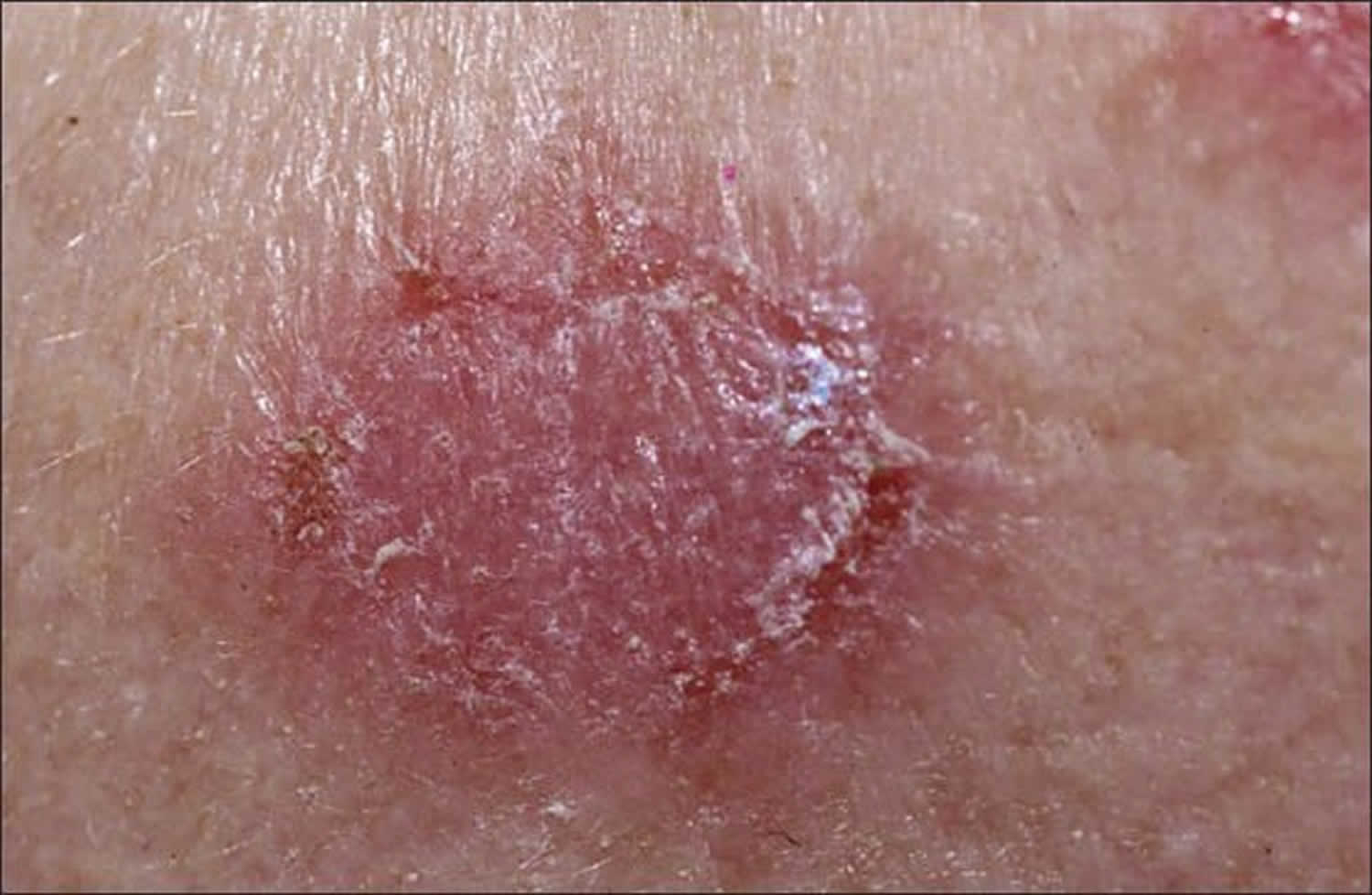
[Source 80 ]Figure 8. Discoid lupus erythematosus lesion (close up view)
Discoid lupus erythematosus treatment
General measures
- Careful year-round protection from sun exposure using clothing and generously applied SPF 50+ broad-spectrum sunscreens. Sunscreens alone are not adequate.
- While indoors, some patients may also need to stay away from glass windows, or these can be treated with UV-blocking films.
- Vitamin D supplements should be recommended for those who strictly avoid the sun.
- Smoking cessation.
Local therapy
- Intermittent courses of potent or ultrapotent topical corticosteroids applied for several weeks are the first treatment for localized discoid lupus erythematosus. Intralesional injections of corticosteroids are sometimes used.
- Calcineurin inhibitors — tacrolimus ointment and pimecrolimus cream can also be used.
- Cosmetic camouflage and wigs are useful and improves self-confidence when there is extensive scarring.
Systemic therapy
- Short term: Systemic corticosteroids such as prednisone or prednisolone can be used for short term control.
- Longer-term: The following have been used and sometimes in combinations; hydroxychloroquine, chloroquine, mepacrine, clofazimine, methotrexate, oral retinoids (isotretinoin and acitretin), mycophenolate mofetil, ciclosporin, cyclophosphamide, azathioprine, dapsone, thalidomide, intravenous immunoglobulins, and biologic agents (belimumab and rituximab).
Lupus profundus (lupus panniculitis)
Lupus profundus also known as lupus erythematosus profundus or lupus panniculitis is a mostly lobular panniculitis without vasculitis. Lupus profundus is a rare form of chronic cutaneous lupus erythematosus (CCLE) that primarily affects subcutaneous fat 82, 83, 84. Studies have described the frequency of lupus erythematosus profundus at 1% to 3% of patients with cutaneous lupus erythematosus 85, 86. Most patients are adults between 20 and 60 years old, with a female to male ratio of approximately two to one. 2% to 5% of patients with systemic lupus erythematosus (SLE) and approximately 10% of those with discoid lupus erythematosus (DLE) develop lupus panniculitis 87. In 70 percent of patients with lupus panniculitis there will be either preceding, subsequent, or concomitant lesions of discoid lupus erythematosus. A patient with lupus profundus or lupus panniculitis has approximately 50% of probability to develop systemic lupus erythematosus (SLE) 88. When lupus profundus is present in combination with SLE, the prognosis of the systemic disease is often better because the patient usually develops a mild form of SLE with infrequent neurological and renal manifestations 89, 88.
Skin lesions of lupus profundus:
- Can develop at any site
- Present as persistent, firm, deep, tender nodules
- Resolve to leave dents in the skin due to atrophy of the fat.
Lupus profundus is characterized by tender, deep, subcutaneous nodules or plaques, which are usually localized on the scalp, face, proximal extremities, and especially the lateral aspects of the arms and shoulders, breast, trunk, and buttocks 87. Skin lesions can be single or involve multiple areas of the body; however, the latter form of presentation is infrequent. The face is often affected in children with lupus profundus. Lesions may be tender and painful and frequently heal with atrophy and scars.
Lupus profundus has a chronic course that is characterized by remission and flare-ups healing with disfigurement. Redness is a common clinical feature in the overlying skin although classic discoid lupus erythematosus (DLE) can present also on the skin surface with characteristic features such as scaling, depigmentation, follicular plugging, atrophy, telangiectasias, or ulceration 87.
In addition to the classical form of lupus profundus (i.e., deep dermal or subcutaneous nodules or plaques), other clinical presentations such as linear 90, 91, 92, morphea-like lesions (hardening and discoloration of the skin) 93, sclerodermoid linear lesions 91 and annular configurations 94, 92 have been described in the literature. Other unusual manifestations include the involvement of salivary glands 95 and periorbital edema as the presenting skin symptom of lupus erythematosus panniculitis of the peribulbar fat pads 96. When the lesions have resolved, skin characteristically develops areas of lipoatrophy that present as depressions or skin retraction. This may produce great morbidity that causes destructive cosmetic results and disability that is related to painful lesions. For example, one case has been reported of lupus profundus of the scalp that was associated with Parry Romberg syndrome, which caused significant disfiguration to the patient 97.
The cause of lupus profundus is not completely understood. Sometimes, there is a history of prior trauma on the sites of skin lesions 90, 83. Clinical cases have been described in which the cutaneous lesions worsened on the sites where biopsies or injections were performed 89.
Given the association between lupus profundus and SLE 98, 99, 100, patients with lupus profundus should be regularly monitored for development of symptoms and signs that are related to SLE. Regular blood and immunologic tests have to be performed on these patients to make an early diagnosis and provide proper treatment. The biopsy with immunohistochemistry and T-cell receptor gene rearrangement studies should be repeated on those patients who are resistant to appropriate treatment to rule out subcutaneous panniculitis-like T-cell lymphoma.
The diagnosis of lupus profundus may be extremely difficult, especially in patients who lack other skin or systemic manifestations of lupus. The diagnosis of lupus profundus is based on characteristic clinical features and confirmed by histopathology. The differential diagnosis includes the inflammatory diseases of subcutaneous fat such as erythema nodosum, erythema induratum of Bazin, subcutaneous panniculitis-like T-cell lymphoma, and traumatic fat necrosis. The distinction is based on routine histology, immunofluorescence, and serology. The particularly troublesome differential diagnosis is subcutaneous panniculitis-like T-cell lymphoma 101.
The golden standard of an lupus profundus diagnosis is the histopathology examination result of a deep skin biopsy of the lesional area. Histopathology of lupus profundus shows a predominantly lymphocytic lobular or mixed panniculitis with frequent plasma cells and sometimes eosinophils. In 45% to 78% of cases, lymphoid follicles are present, sometimes with germinal centers (20% of the cases), with a perilobular distribution 89. Another characteristic feature is hyaline fat necrosis. Additional histopathology findings include pathological changes of discoid lupus erythematosus in the overlying skin, dermo-epidermal changes such as the thickening of the basement membrane, mucin deposition, calcification, and vascular changes such as lymphocytic vasculitis, fibrin thrombosis, and perivascular fibrosis. Vascular changes seem to be the cause of ulceration in some patients. The two most important histopathologic criteria for a diagnosis of lupus profundus are the presence of lymphocytic infiltrates that involve fat lobules and the hyaline necrosis of the fat lobule. Direct immunofluorescence varies among the different series from 36% 102 to 90.5% 103.
Figure 9. Lupus profundus (lupus panniculitis)
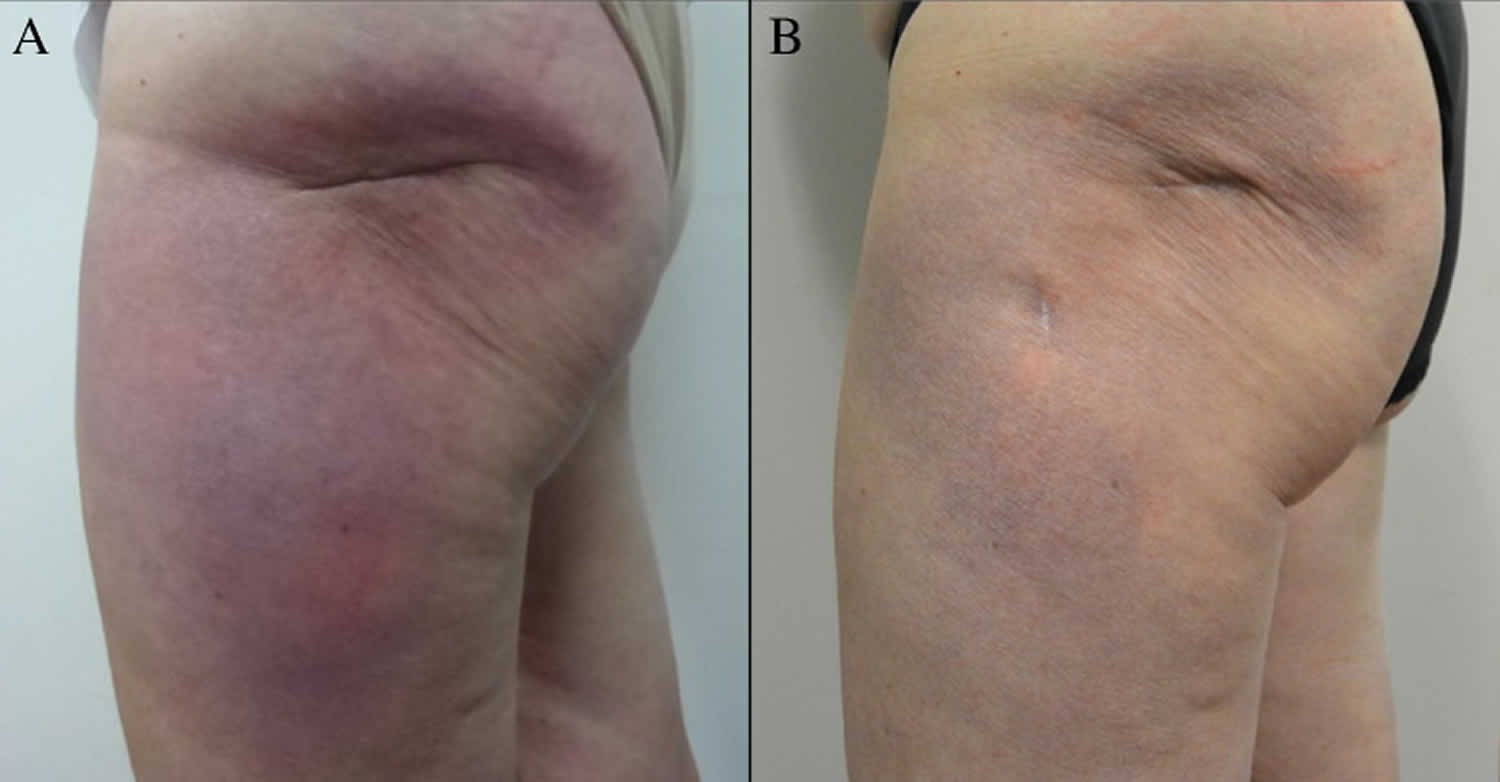
Footnotes: (A) Lupus profundus before treatment. A large, indurated, erythematous-to-violaceous, poorly demarcated plaque on the left hip and lateral aspect of the left upper thigh within a large linear skin invagination of lipoatrophy. (B) Plaque with less edema, inflammation, and induration, after 2 months of therapy, showing signs of postinflammatory hyperpigmentation.
[Source 87 ]Lupus profundus treatment
There are no randomized controlled trials of treatments for lupus profundus. Topical therapy consists of glucocorticosteroid 104 and lubricant ointments. Injections of glucocorticosteroid medications into lesional areas are generally ineffective and can exacerbate the atrophy 89. Systemic, first-line therapy for lupus profundus as well as other forms of cutaneous lupus erythematosus traditionally has been antimalarial medications such as hydroxychloroquine (dose 200-400 mg daily) or chloroquine (250-500 mg daily) 105, 106, 107. Systemic corticosteroid medications are often useful for severe cases that are accompanied by SLE 105, 106.
Other reported systemic therapies include thalidomide 107, 106, dapsone 108, methotrexate 97, cyclosporine (Espírito Santo et al., 2010, Saeki et al., 2000, Wozniacka et al., 2007), cyclophosphamide 106, 97, intravenous immunoglobulins 106, and rituximab 109, 110.
Chilblain lupus erythematosus
Chilblain lupus erythematosus (CHLE) is a rare form of chronic cutaneous lupus erythematosus involving mainly the fingers and toes of smokers triggered by exposure to a moist cold environment 111, 112, 113. Chilblain lupus erythematosus is characterised by purple plaques/nodules and edematous skin mainly around the acral regions of the body, which are most exposed to the cold. Chilblain lupus erythematosus may be familial with no association to SLE, or sporadic which can be associated with SLE.
Chilblain lupus erythematosus was first described by Jonathan Hutchinson in 1888 as cold-induced erythematous lesions. He had initially termed it ‘Lupus Pernio’ 24 years before the initial description of primary chilblains 114. Millard and Rowell classified these lesions as chilblain lupus erythematosus of Hutchinson’s; they can be a symptom of cutaneous lupus erythematosus (CLE) 115. Raynaud’s-associated discoloration can occur at the same time with chilblain lupus erythematosus lesions in some cases. Chilblain lupus erythematosus can occur in the context of SLE and is a specific subtype of chronic cutaneous lupus erythematosus in the Systemic Lupus International Ccollaborating Clinics Classification Criteria 2012 for SLE 116. In a prospective study of 33 patients affected by severe chilblains, Viguier et al. 117 proposed that persistence of lesions during hot seasons was an important feature that could delineate chilblain lupus erythematosus (CHLE) from idiopathic chilblains.
Skin lesions of chilblain lupus erythematosus:
- Are often itchy and painful
- May ulcerate or develop hyperkeratotic fissuring
- May heal leaving depigmentation and atrophic spindling of the distal phalange.
Chilblain lupus erythematosus (CHLE) is clinically characterized by symmetrically distributed circumscribed, occasionally infiltrated red to violaceous itchy or painful plaques over dorsal and lateral aspects of hands and feet, appearing during cold, damp weather conditions. Involvement of ears, nose or trunk is uncommon 118. Chilblain lupus erythematosus may be associated with lesions of discoid lupus erythematosus (DLE) or other forms of cutaneous lupus erythematosus and may progress to systemic lupus erythematosus (SLE) in up to 18% of patients 118. It can clinically simulate lupus pernio, however, it is essential to make a correct diagnosis; although clinically the two entities are similar and have in common their association with systemic disease (lupus erythematosus or sarcoidosis), the prognosis and treatment differ considerably 119. Verrucous form of chilblain lupus has also been described in literature 120. In most patients, immunological abnormalities are frequently observed in the form of polyclonal hypergammaglobulinemia, raised rheumatoid factor, antinuclear antibodies. Antibodies to Ro/SSA and antiphospholipid (APL) antibodies have also been found to be positive in a subset of chilblain lupus erythematosus patients 121. However, in patients with SLE, Bouaziz et al. 122 did not find association with anti-Ro antibodies. Full-thickness skin grafts from unaffected regions resulted in persistent improvement in two reported cases, implying that local factors might be crucial in the pathophysiology 123.
The pathogenesis of chilblain lupus erythematosus is not well understood 112. Constriction of blood vessels provoked by exposure to cold leads to the occlusion of the capillary bed and a circulation slowdown with the presence of aggregates of red blood cells visible on capillaroscopy 115, 121.
Chilblains are generally diagnosed on clinical grounds with supporting histopathology in some cases 112.
Diagnostic criteria have been proposed by the Mayo clinic (Mayo Clinic Diagnostic criteria) for both chilblain lupus erythematosus (based on five patients in 1994) 124 and idiopathic chilblains 125.
Mayo Clinic Diagnostic criteria for chilblain lupus erythematosus 124:
- 2 major criteria:
- Skin lesions of acral sites induced by exposure to cold or a drop in temperature.
- Evidence of lupus erythematosus in the skin lesions, as determined by histopathologic examination or direct immunofluorescence.
- 3 minor criteria:
- Coexistence of systemic lupus erythematosus (SLE) or other skin lesion of discoid lupus erythematosus.
- Response to anti-lupus therapy.
- Negative cryoglobulin and cold agglutinin studies.
Patients must fulfil both major criteria and at least one of the minor criteria to be diagnosed as having definite chilblain lupus erythematosus 124.
Some immunological anomalies are frequently observed (although not necessary for diagnosis) in chilblain lupus erythematosus, including hypergammaglobulinemia (>2/3 of patients), positive rheumatoid factor (∼50%), ANA, anti-Ro/SSA, and antiphospholipid (APL) antibodies 115, 126, 127. Skin biopsy can be helpful in diagnosis
Figure 10. Chilblain lupus erythematosus

Footnote: A 35-year-old Thai woman presented to her doctor with a 1-month history of an itchy and painful rash on the fingers of her right hand associated with finger swelling. Clinical features of patients with chilblain lupus erythematosus with reddish or purplish papules and plaques were observed on dorsal aspects of patient’s fingers.
[Source 111 ]Chilblain lupus erythematosus treatment
Chilblain lupus erythematosus treatment is to prevent development of new lesions and expedite the healing of current lesions to reduce discomfort and avoid scarring. Chilblain lupus erythematosus treatment includes protection from cold and damp by using insulated clothing, gloves and footwear with topical or oral antibiotics, if the lesions are infected 126. Topical corticosteroids do not appear to be particularly effective, although may be of some benefit 128, 126, 125, 129. Topical glyceryl trinitrate (GTN) 0.4% was found to be similar in efficacy to nifedipine (initially 10–20 mg daily, increased to 20–40 mg daily) in a single-blind randomized trial, although resolution was slower in the GTN arm 128. Nifedipine has inconsistent evidence in the treatment of primary chilblains. Studies suggest superiority to placebo in some studies but not others 130, 131, 132, 128, with reports of superiority to diltiazem 133 and topical 5% minoxidil solution 134.
Pentoxifylline is a xanthine derivative that non-selectively inhibits phosphodiesterase and has been shown to decrease blood viscosity and improve erythrocyte flexibility, which have been postulated to be an important factor in the pathogenesis of chilblain lesions 135. It has demonstrated superiority to placebo 136, 137, oral prednisolone and topical clobetasol 138 in studies.
Tadalafil is a selective phosphodiesterase type 5 (PDE5) inhibitor with a long half-life (17.5 hours). An open-label study demonstrated superiority over both pentoxifylline and prednisolone in terms of lesion severity after 2 weeks 137.
In difficult cases, local immunosuppressive agents such as tacrolimus, pimecrolimus or systemic agents such as systemic steroids and mycophenolate mofetil may be tried 139, 126, 140, 141.
Due to lack of good quality evidence, a number of different drugs have also been tried in single or more cases and found to be of benefit (more often in primary chilblains). These include:
- Vasodilators: etretinate, diltiazem, amlodipine, phenoxybenzamine, thymoxamine, prazosin (the last three are alpha blockers), nicotinamide and niacin derivative pyridyl carbinol.
- Others: phototherapy, full thickness skin graft 123, chemical lumbar sympathectomy 142, dapsone, vitamin D3 and vitamin K.
Antimalarial drugs (chloroquine or hydroxychloroquine) have shown to have good effects on SLE typical symptoms but not on chilblain themselves. A French meta-analysis of cutaneous manifestations of SLE suggested that anti-malarials were less effective in chilblain lupus erythematosus (response rate 31%) compared to acute cutaneous lupus erythematosus (response rate 91%) 143. In a retrospective study of five patients by Yang et al. 144, three with primary chilblains and two with SLE, hydroxychloroquine improved chilblains in four patients which included both patients with SLE. Patel and Hardo 145 and Horino et al. 146 reported successful use of hydroxychloroquine in a patient with chilblain lupus erythematosus. In a case series, Millard and Rowell 115 reported hydroxychloroquine and chloroquine were of benefit to three patients with chilblain lupus erythematosus. Discontinuation resulted in relapse of symptoms 115. In case series of 15 patients, Doutre et al. 147 reported that hydroxychloroquine at 600 mg dosage was effective after 3 months. Hydroxychloroquine was found to be effective in four out of 15 patients with chilblain lupus erythematosus in a study by Franceschini et al. 121. Su et al. reported that only one in five patients treated with chloroquine saw a complete resolution of lesions within two months 124.
Cutaneous lupus erythematosus causes
Your skin is a complex structure consisting of epidermal keratinocytes, melanocytes, dermal fibroblasts, adipose tissue and numerous immune cells (see Figure 3). All these compartments are more or less regularly exposed to ultraviolet (UV) irradiation in many areas of the body surface. In healthy skin, UV irradiation has immunological and inflammatory effects and causes a series of cellular reactions that are both metabolically stimulating, pro-inflammatory or even degenerating 148.
The exact cause of cutaneous lupus erythematosusis unknown, but it is believed that the cause of cutaneous lupus erythematosus is multifactorial where a combination of genetic susceptibility and environmental factors in association with innate and adaptive immune responses results in cutaneous lupus erythematosus 3, 4, 12, 13, 5, 6, 7, 8, 9, 14, 15, 16, 10, 11:
- Genetic susceptibility
- High incidence among family members
- Environmental factors
- Cigarette smoking
- Sun exposure
- Medications
- Innate and adaptive immune responses
- Autoantibodies.
In cutaneous lupus erythematosus it is likely that certain environmental factors such as UV light or medications may induce the increased cell death of keratinocytes in your skin 3, 7, 6, 149. In addition, clearance of keratinocytes cells is probably also impaired, leading to the accumulation of nuclear substances in the tissues. Subsequently, these factors can activate both the innate and the adaptive immune system, triggering the release of cytokines, chemokines and interferons, and thus, a self-reinforcing cycle develops 150. Keratinocytes are the main type of skin cells found in your epidermis, the outermost layer of your skin, that play critical roles in wound repair not only as structural cells but also exerting important immune functions 151, 152, 153, 154, 155.
Smoking is one of the environmental factors associated with cutaneous lupus erythematosus. A prospective cohort study showed that current smokers with cutaneous lupus erythematosus had worse disease with higher Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI) scores, had a worse quality of life, and were treated more often with a combination of hydroxychloroquine and quinacrine than non-smokers 156.
Over 100 drugs have been reported to induce cutaneous lupus erythematosus or cutaneous lupus erythematosus flares 157, 158. Unlike idiopathic cutaneous lupus erythematosus, in which discoid lupus erythematosus (DLE) is the most common subtype, subacute cutaneous lupus erythematosus (SCLE) is the most frequently described form of drug-induced cutaneous lupus erythematosus 157, 158. Numerous drugs have been implicated in the induction of drug-induced subacute cutaneous lupus erythematosus (DI-SCLE) 159, 160. The most common drugs involved used to be antihypertensives, particularly thiazide diuretics and calcium channel blockers, followed by antifungals, particularly allylamine antifungals 159. Recently, new medications, such as biologics, particularly anti-tumor necrosis factor (TNF)-α agents, proton pump inhibitors, and chemotherapeutics, have become more common causes of drug-induced subacute cutaneous lupus erythematosus 157, 161.
In rare cases, a discoid form of chronic cutaneous lupus erythematosus can be caused by medication 157, 158. Drug-induced-chronic cutaneous lupus erythematosus (DI-CCLE) has mostly been reported to be associated with 5-fluorouracil (FU), non-steroidal anti-inflammatory drugs (NSAIDs), and anti-TNF-α agents 157, 158.
Multiple cytokines such as type 1 IFN, IL-6 and TNF-α and chemokines such as CXCL10 are involved in the pathogenesis of cutaneous lupus erythematosus 19, 14, 162. Cutaneous lupus erythematosus lesions have a strong type 1 IFN signature and the level of IFN-induced genes correlates with disease activity of SLE 163, 164. Nucleic acids represent potential ligands for type 1 interferon release that can be recognized by pattern recognition receptors 165. Accumulation of nucleic acids may be caused by a deficiency of nucleases, some of which have been identified as genetic susceptibility genes in cutaneous lupus erythematosus 165. In addition to type 1 IFN, impairment in the opsonization of apoptotic cells have been detected in SLE patients 166. Furthermore, numerous immune cells such as myeloid and plasmacytoid dendritic cells, macrophages and T cells are involved in the pathogenesis of cutaneous lupus erythematosus and their functions have been studied after UV radiation 14.
Cutaneous lupus erythematosus pathophysiology
The pathogenesis of cutaneous lupus erythematosus is multifactorial, with an interplay between genetic and environmental factors 27, 3, 4, 12, 13, 5, 6, 7, 8, 9, 14, 15, 16, 10, 11. Some contributing environmental factors include ultraviolet radiation (UVR), medications, cigarette smoking, and possibly, viruses. The interaction between these multiple factors triggers an inflammatory cascade of cytokine, chemokine, and inflammatory cell responses. Genes previously associated with SLE are TYK2, IRF5, and CTLA4 and confer an increased risk of developing discoid lupus erythematosus (DLE).
An analysis of 405 patients by Bockle et al. 56 found that smoking is highly associated with discoid lupus erythematosus. Bockle et al. 56 hypothesized that smoking might play a pathogenic role in cutaneous lupus erythematosus variants (discoid lupus erythematosus, tumid lupus) by inducing apoptosis, stimulating T-cell proliferation, and increasing photosensitivity. Another explanation might be that smoking provokes DNA damage, resulting in the formation of DNA adducts and the production of ds-DNA antibodies. Keratinocytes may also participate in lupus skin damage by increasing the apoptotic rate and the production of proinflammatory cytokines such as IFN-alpha and IL-6 for SLE and IFN-lambda for discoid lupus erythematosus 167, 168.
Cutaneous lupus erythematosus signs and symptoms
Cutaneous lupus erythematosus signs and symptoms vary greatly depending on the subtypes (see Cutaneous Lupus Erythematosus Types above). Each cutaneous lupus erythematosus subtype has a diverse and unique character 169.
Skin lesions of cutaneous lupus erythematosus can be subdivided into:
- Lupus-specific changes
- Clinical signs diagnostic of or unique to lupus erythematosus
- Histology is diagnostic for lupus erythematosus; vacuolar interface dermatitis
- Lupus-nonspecific changes
- Clinical signs found not only in lupus erythematosus, but also in other connective tissue diseases
- Histology is not diagnostic for lupus erythematosus; reactive patterns seen.
Subacute cutaneous lupus erythematosus (SCLE)
- The rash usually appears as red, non-itchy patches on sun-exposed areas such as the upper chest and back and arms.
- There are two main forms of subacute cutaneous lupus erythematosus (SCLE):
- Papulosquamous subacute cutaneous lupus erythematosus occurs in approximately two thirds of cases and consists of red scaly patches.
- Annular (or polycylic) subacute cutaneous lupus erythematosus (SCLE) occurs in approximately one third of cases and causes a red ring or “arcuate shaped” rash.
- Subacute cutaneous lupus erythematosus (SCLE) heals without scarring, although the rash may fade with some colour changes.
- Rarely there may be mild symptoms such as tiredness, weakness or joint aches.
Discoid lupus erythematosus (DLE)
- Discoid lupus erythematosus (DLE) occurs most commonly on sun-exposed sites, in particular the face and scalp.
- Discoid lupus erythematosus (DLE) appears as red scaly patches and bumps which can sometimes be thickened or warty.
- If discoid lupus erythematosus (DLE) affects the hair then red scaly areas develop around the base of the hairs and result in patches of hair loss (alopecia) which may be permanent.
- Discoid lupus erythematosus (DLE) may occasionally be uncomfortable or itchy.
- Discoid lupus erythematosus (DLE) often heals with scarring and/or skin colour changes. The scarring can sometimes be disfiguring and difficult to treat.
In some cases, there may be overlap between the different forms of cutaneous lupus erythematosus present, including the presence of chilblain lupus erythematosus (perniosis).
Cutaneous lupus erythematosus complications
- Progression to SLE and the complications of SLE. A minority of cases (less than 5%) of cutaneous lupus erythematosus may become systemic lupus erythematosus (SLE). Very rarely, some lesions in discoid lupus erythematosus (DLE) may turn into skin cancer such as squamous cell carcinoma (SCC) or basal cell carcinoma (BCC).
- Dyspigmentation (an abnormality in the formation or distribution of pigmentation in the skin)
- Discoid lupus erythematosus (DLE)
- Scarring
- Permanent (cicatricial) hair loss
- Cutaneous squamous cell carcinoma
- Neonatal lupus erythematosus in baby of female patient with Ro and/or La autoantibodies
- Impact on quality of life. Cutaneous lupus erythematosus often result in depression and psychological stress. It is estimated that 20–40% of patients with cutaneous lupus erythematosus suffer from emotional problems.
- Patients report being extremely self-conscious and distressed about their appearance as well as being socially stigmatised.
- Cutaneous lupus erythematosus also interferes with leisure activities due to the need to avoid sunlight.
- Feelings of helplessness and feeling trapped by the disease are frequently reported, due to the chronicity of lupus and its lack of cure.
- Avoiding sun exposure might cause vitamin D deficiency in some patients. Therefore, evaluation of the vitamin D deficiency with 25-hydroxyvitamin D level and adequate supplementation with at least 400 IU of cholecalciferol is suggested 69, 70.
Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI)
The Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI) scores activity and damage in each of 12 anatomical locations.
- The total activity score:
- Degree of redness (0-3) and scale (0-2)
- Mucous membrane involvement (0-1)
- Recent hair loss (0-1), nonscarring alopecia (0-3)
- Total damage score:
- Degree of dyspigmentation (0-2) and scarring (0-2)
- Persistence of dyspigmentation more than 12 months doubles the dyspigmentation score
- Scalp scarring (0, 3, 4, 5, 6).
Cutaneous lupus erythematosus diagnosis
Cutaneous lupus erythematosus can be diagnosed clinically based on clinical features, supported by the results of blood tests and a skin biopsy and confirmed by histopathology (viewing under microscope).
- Skin biopsy — diagnostic histopathology and direct immunofluorescence (DIF) is seen only in specific cutaneous lupus erythematosus lesions
- The most characteristic direct immunofluorescence finding in cutaneous lupus erythematosus is antibody deposition at the dermal-epidermal junction and around hair follicles. These deposits are typically granular, and they are composed primarily of IgG and/or IgM 170, 171
- The lupus band test (LBT) is a diagnostic procedure used to detect deposits of immunoglobulins and complement components along the dermo-epidermal junction in patients with lupus erythematosus. Lupus band test (LBT) can help distinguish systemic lupus erythematosus from chronic lupus erythematosus because, in SLE patients, the lupus band test (LBT) is frequently positive in both uninvolved and involved skin, whereas in cutaneous lupus erythematosus patients, only the involved skin is positive 172, 173. The lupus band test is positive on the lesional skin in 75% of patients. Ideal lesions for lupus band test for discoid lupus erythematosus (DLE) are on the head and neck that have been present for at least a few months.
- Blood tests — full blood count, renal function test, inflammatory markers, Ro/SSA antibody, La/SSB, dsDNA, anti-histone, and Sm antibodies
- FBC and ESR are often abnormal (CRP usually normal) – anaemia is present in 75% of cases. Leucopenia, especially a lymphopenia, is said to be characteristic. Thrombocytopenia affects 20% of patients
- Rheumatoid factor is present in 40% of cases
- The lupus anticoagulant is one of a number of antiphospholipid antibodies that may be found in up to 50% of patients
- False-positive serology tests for syphilis are found in 25% of patients
- Complement levels may be reduced
- Cryoglobulins (and other cryoproteins) are found in up to 15% of cases, indeed cryoglobulinaemia may precede SLE by many years
- Serology — including ANA, ENA – are often negative in chronic cutaneous lupus erythematosus (CCLE)
Histopathology of cutaneous lupus erythematosus lesions shows a perivascular and periadnexal lymphohistiocytic infiltrate and interface dermatitis at the dermo-epidermal border often associated with vacuolization of basal keratinocytes 19.
Cutaneous lupus erythematosus treatment
Cutaneous lupus erythematosus can be managed by skin specialists (dermatologists), but so far there is no cure. The goals of skin lupus or cutaneous lupus erythematosus treatment are to control and stop the development of new lesions so as to minimize and prevent scarring and disfigurement. Avoidance of trigger factors is of utmost importance such as cessation of smoking and avoidance of sun exposure. The treatment is about the same for the different cutaneous lupus erythematosus subtypes where first-line of treatment is sun-protection and local therapy with corticosteroids or calcineurin inhibitors 174. There are very few randomized controlled trials for the treatment of cutaneous lupus erythematosus 81, 175. Antimalarial are the first choice of systemic treatment. With local therapy and antimalarial treatment about 75% of the cutaneous lupus erythematosus patients responds 176. For the refractory cases, a number of different treatments can be tried such as retinoids, metothrexate, thalidomide, mycophenolate, azathioprine and dapsone. The latest Cochrane review concluded that hydroxychloroquine and acitretin had the same clinical effect but acitretin had numerous and severe adverse effects 174. Methotrexate has been shown to be effective for recalcitrant cutaneous lupus erythematosus in a retrospective study 177.
It is important to avoid both natural and artificial UV light and use both clothes and broad-spectrum sunscreen. There is often a latency period of several weeks between UV exposure and disease symptoms so it is important for patients to know about this association.
General measures include:
- Sun protection and avoidance: SPF 50+ broad spectrum sunscreen and UPF 50+ sun-protective clothing
- Smoking cessation
- Vitamin D supplementation (in case of vitamin D deficiency following UV protection)
Topical treatment
Individual lesions of lupus are best treated by the application of topical corticosteroid medications, either in cream or ointment form. The potency of the corticosteroid used, will vary with the thickness of the lesions and their location. A potent topical steroid (e.g., Betamethasone), or, occasionally a superpotent topical steroid (e.g., Clobetasol) should be applied thinly and accurately to the plaques. Once control is gained reduce to twice weekly maintenance, increasing for flares.
An alternative are the topical calcineurin inhibitors – pimecrolimus cream appears more effective than tacrolimus ointment.
In selected cases, injection of corticosteroids directly into the lesions results in the best improvement for resistant cases, although there is a greater risk of atrophy.
Cosmetics
Cosmetics can be used to minimize the impact of established lesions. Camouflage cosmetics can efficiently minimize discoloration.
Systemic treatment
Systemic treatment is second-line treatment that used in combination with the above.
Systemic treatment include:
- Antimalarials, usually hydroxychloroquine
- Hydroxychloroquine 200–400 mg daily. The daily maintenance dose of hydroxychloroquine should not exceed 5 mg/kg/day. Hydroxychloroquine can safely be used in pregnancy.
- Mepacrine 50-100 mg once daily is indicated as follows:
- To use as an alternative if additional risk factors for retinal toxicity exist, such as concomitant tamoxifen therapy or impaired renal function (estimated glomerular filtration rate < 60 mL/min per 1.73 m²)
- If hydroxychloroquine not tolerated
- As an add in to hydroxychloroquine if response suboptimal
- Consider mepacrine up to 200 mg daily in people resistant to standard dosing, when combination antimalarials or other therapies are contraindicated.
- Chloroquine (third-line antimalarial option) less than 2.5 mg/kg/day. Take care when prescribing chloroquine as the dosing depends on the salt used and is generally expressed in reference to chloroquine base, for example chloroquine phosphate 250 mg is approximately equivalent to chloroquine sulfate 200 mg and to chloroquine base 155 mg.
- Retinal screening for antimalarials (not needed for mepacrine). Annual screening is recommended in all patients who have taken hydroxychloroquine for more than 5 years. This should include spectral domain optical coherence tomography and fundus autofluorescence imaging photography
- Annual screening may be commenced after 1 year of treatment if additional risk factors for retinal toxicity exist, such as concomitant tamoxifen therapy or impaired renal function (estimated glomerular filtration rate < 60 mL/min per 1.73 m²), or if the daily dose of hydroxychloroquine is greater than 5 mg/kg.
- Annual retinal assessment in all people with chloroquine after 1 year of therapy.
- Consider intermittent use of antimalarial therapy in people with seasonal lupus (e.g., summer flares in photosensitive lupus erythematosus and winter flares in chilblain lupus erythematosus).
- Suboptimal response to antimalarial therapy – several other treatments have been used with variable success including acitretin (25-50 mg once daily), methotrexate (up to 25 mg once a week), mycophenolate mofetil (typically 0.5 g twice daily, up to 1.5 g twice daily), clofazime, biologic therapies, intravenous immune globulin (IVIG), and thalidomide. The latter can be very effective, including in cases of chilblain lupus, although there are significant risks such as teratogenicity and polyneuropathy.
- Immune modulators such as methotrexate, mycophenolate, dapsone, ciclosporin; there is evidence of successful treatment with anifrolumab
- Consider dapsone (typically commenced at 50 mg daily and escalated to 150 mg daily, depending on response and tolerability) as a first-line systemic treatment option in people with subacute cutaneous lupus erythematosus (SCLE) and bullous SLE.
- Systemic corticosteroids. Systemic steroids – concomitant, short-term, and tapering courses can be used for flares and severe/disseminated disease
- Anifrolumab is a type 1 interferon receptor subunit blocker that has shown efficacy in systemic lupus as well as severe cutaneous lupus erythematosus
In the presence of advancing disease despite local therapy or in the presence of widespread disease, systemic therapy is considered.
First line systemic therapy consists of the use of antimalarial drugs. If the skin disease is resistant to a single antimalarial drug, a combination of antimalarial drugs is often used next.
Second line therapy consists of the use of other drugs that have been shown to modulate the immune system such as the vitamin A derivatives (isotretinoin or acitretin) or dapsone.
If these agent fail, more potent immunosuppressive drugs are used on rare occasion. These may include methotrexate, azathioprine, mofetil mycophenolate, cyclosporine, systemic corticosteroids, and thalidomide.
Cutaneous lupus erythematosus prognosis
Cutaneous lupus erythematosus can be the presenting sign of SLE, as in acute cutaneous lupus erythematosus (ACLE) or may evolve into SLE.
Subacute cutaneous lupus erythematosus (SCLE) uncomplicated by systemic disease often has a chronic course with intermittent flare-ups. It often flares up during sunnier weather. Sometimes there is spontaneous remission. The skin usually heals without scarring or permanent marks. It can be managed with treatment.
Female patients with cutaneous lupus erythematosus and Ro/La autoantibodies should be advised of the risk their baby may have neonatal lupus erythematosus including congenital heart block 47, 48, 49, 50.
Chronic cutaneous lupus erythematosus (CCLE) tends to follow a chronic relapsing course for years, with flares in spring and summer, and resolution with scarring if untreated.
In discoid lupus erythematosus (DLE) there may be permanent loss of pigmentation, scarring of the skin and/or alopecia (hair loss) leading to disfiguration and psychological distress. Early treatment may reduce the risk of scarring. Exacerbations are associated with sun exposure and often occur in spring and summer. Localized discoid lupus erythematosus involving the scalp may lead to scarring with hair loss. Generalized discoid lupus erythematosus is associated with the risk of progression to SLE in about 28 percent 178. Chronic discoid lupus erythematosus lesions in about 2 to 3 percent can progress to squamous cell carcinoma, which is usually associated with a poor prognosis 179. Early detection and treatment of discoid lupus erythematosus lesions can minimize the associated morbidity. Psychological functioning is affected by discoid lupus erythematosus (DLE) lesions 180.
Previous epidemiologic studies have shown that patients with SLE and other autoimmune diseases, such as rheumatoid arthritis have increased sickness and death due to cancer 181, 182. There are more than 100 published case reports of discoid lupus erythematosus (DLE) and squamous cell carcinoma (SCC) in lesional skin and subacute cutaneous lupus erythematosus (SCLE) has been associated with various internal cancers 78, 183, 184, 185. It has been shown that patients with cutaneous lupus erythematosus have a significantly increased cancer risk 186. The most increased risk estimates were found for buccal cancer, accompanied by an approximately four times increased risk for lymphomas, respiratory cancer and non-melanoma skin cancer 81. The increased risk estimates were not influenced by a concomitant diagnose of SLE 186. Although no causal relationship between potential risk factors and cancer development in cutaneous lupus erythematosus patients could be established in this study, smoking is probably a substantial confounder in the cutaneous lupus erythematosus patients who have been shown to smoke more than the general population 81. Other possible explanations could be that cutaneous lupus erythematosus patients are more sensitive to UV-light and certain virus infections for example HPV 81.
- Lupus. https://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Lupus[↩]
- Niebel D, de Vos L, Fetter T, Brägelmann C, Wenzel J. Cutaneous Lupus Erythematosus: An Update on Pathogenesis and Future Therapeutic Directions. Am J Clin Dermatol. 2023 Jul;24(4):521-540. doi: 10.1007/s40257-023-00774-8[↩]
- Kahlenberg JM. Rethinking the pathogenesis of cutaneous lupus. J Invest Dermatol. (2021) 141:32–5. 10.1016/j.jid.2020.05.077[↩][↩][↩][↩][↩][↩]
- Mikita N, Ikeda T, Ishiguro M, Furukawa F. Recent advances in cytokines in cutaneous and systemic lupus erythematosus. J Dermatol. 2011 Sep;38(9):839-49. doi: 10.1111/j.1346-8138.2011.01237.x[↩][↩][↩][↩]
- Jarukitsopa S, Hoganson DD, Crowson CS, Sokumbi O, Davis MD, Michet CJ Jr, Matteson EL, Maradit Kremers H, Chowdhary VR. Epidemiology of systemic lupus erythematosus and cutaneous lupus erythematosus in a predominantly white population in the United States. Arthritis Care Res (Hoboken). 2015 May;67(6):817-28. doi: 10.1002/acr.22502[↩][↩][↩][↩]
- Wenzel, J. Cutaneous lupus erythematosus: new insights into pathogenesis and therapeutic strategies. Nat Rev Rheumatol 15, 519–532 (2019). https://doi.org/10.1038/s41584-019-0272-0[↩][↩][↩][↩][↩][↩]
- Király Z, Nagy E, Bokor L, Kovács A, Marschalkó M, Hidvégi B. The Possible Clinical Significance of a Decreased Serum Level of Soluble PD-L1 in Discoid Lupus Erythematosus, but Not in Subacute Cutaneous Lupus Erythematosus-A Pilot Study. J Clin Med. 2023 Aug 30;12(17):5648. doi: 10.3390/jcm12175648[↩][↩][↩][↩][↩]
- Udompanich S, Chanprapaph K, Suchonwanit P. Hair and Scalp Changes in Cutaneous and Systemic Lupus Erythematosus. Am J Clin Dermatol. 2018 Oct;19(5):679-694. doi: 10.1007/s40257-018-0363-8[↩][↩][↩][↩]
- Dammacco R, Procaccio P, Racanelli V, Vacca A, Dammacco F. Ocular Involvement in Systemic Lupus Erythematosus: The Experience of Two Tertiary Referral Centers. Ocul Immunol Inflamm. 2018;26(8):1154-1165. doi: 10.1080/09273948.2018.1501495[↩][↩][↩][↩]
- Cutaneous Lupus Erythematosus. https://www.dermcoll.edu.au/atoz/cutaneous-lupus-erythematosus[↩][↩][↩][↩]
- Cutaneous lupus erythematosus. https://dermnetnz.org/topics/cutaneous-lupus-erythematosus[↩][↩][↩][↩][↩]
- Klein B, Kunz M. Current concepts of photosensitivity in cutaneous lupus erythematosus. Front Med (Lausanne). 2022 Aug 25;9:939594. doi: 10.3389/fmed.2022.939594[↩][↩][↩][↩][↩]
- Szczęch J, Samotij D, Werth VP, Reich A. Trigger factors of cutaneous lupus erythematosus: a review of current literature. Lupus. 2017;26(8):791-807. doi:10.1177/0961203317691369[↩][↩][↩]
- Garelli CJ, Refat MA, Nanaware PP, Ramirez-Ortiz ZG, Rashighi M, Richmond JM. Current Insights in Cutaneous Lupus Erythematosus Immunopathogenesis. Front Immunol. (2020) 11:1353. 10.3389/fimmu.2020.01353[↩][↩][↩][↩][↩]
- Kunz M, König IR, Schillert A, Kruppa J, Ziegler A, Grallert H, et al. Genome-wide association study identifies new susceptibility loci for cutaneous lupus erythematosus. Exp Dermatol. (2015) 24:510–5. 10.1111/exd.12708[↩][↩][↩]
- Hersh AO, Arkin LM, Prahalad S. Immunogenetics of cutaneous lupus erythematosus. Curr Opin Pediatr. (2016) 28:470–5. 10.1097/MOP.0000000000000383[↩][↩][↩]
- Maz MP, Michelle Kahlenberg J. Cutaneous and systemic connections in lupus. Curr Opin Rheumatol. (2020) 32:583–9. 10.1097/BOR.0000000000000739[↩]
- Skopelja-Gardner S, An J, Tai J, Tanaka L, Sun X, Hermanson P, et al. The early local and systemic type I interferon responses to ultraviolet B light exposure are cGAS dependent. Sci Rep. (2020) 10:7908. 10.1038/s41598-020-64865-w[↩]
- Wenzel J. Cutaneous lupus erythematosus: new insights into pathogenesis and therapeutic strategies. Nat Rev Rheumatol. (2019) 15:519–32. 10.1038/s41584-019-0272-0[↩][↩][↩]
- Jones SK. Ultraviolet radiation (UVR) induces cell-surface Ro/SSA antigen expression by human keratinocytes in vitro: a possible mechanism for the UVR induction of cutaneous lupus lesions. Br J Dermatol. (1992) 126:546–53. 10.1111/j.1365-2133.1992.tb00098.x[↩]
- Kuhn A, Herrmann M, Kleber S, Beckmann-Welle M, Fehsel K, Martin-Villalba A, et al. Accumulation of apoptotic cells in the epidermis of patients with cutaneous lupus erythematosus after ultraviolet irradiation. Arthritis Rheum. (2006) 54:939–50. 10.1002/art.21658[↩]
- Mahajan A, Herrmann M, Muñoz LE. Clearance deficiency and cell death pathways: a model for the pathogenesis of SLE. Front Immunol. (2016) 7:35. 10.3389/fimmu.2016.00035[↩]
- Grönhagen C., Fored C., Granath F., Nyberg F. Cutaneous lupus erythematosus and the association with systemic lupus erythematosus: A population-based cohort of 1088 patients in Sweden. Br. J. Dermatol. 2011;164:1335–1341. doi: 10.1111/j.1365-2133.2011.10272.x[↩][↩][↩][↩][↩]
- Jarukitsopa S., Hoganson D.D., Crowson C.S., Sokumbi O., Davis M.D., Michet C.J., Jr., Matteson E.L., Kremers H.M., Chowdhary V.R. Epidemiology of systemic lupus erythematosus and cutaneous lupus erythematosus in a predominantly white population in the United States. Arthritis Care Res. 2015;67:817–828. doi: 10.1002/acr.22502[↩][↩]
- Durosaro O., Davis M.D.P., Reed K.B., Rohlinger A.L. Incidence of Cutaneous Lupus Erythematosus, 1965–2005: A Population-Based Study. Arch. Dermatol. 2009;145:249–253. doi: 10.1001/archdermatol.2009.21[↩][↩]
- Petersen M.P., Möller S., Bygum A., Voss A., Bliddal M. Epidemiology of cutaneous lupus erythematosus and the associated risk of systemic lupus erythematosus: A nationwide cohort study in Denmark. Lupus. 2018;27:1424–1430. doi: 10.1177/0961203318777103[↩]
- McDaniel B, Sukumaran S, Koritala T, et al. Discoid Lupus Erythematosus. [Updated 2023 Aug 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK493145[↩][↩][↩]
- Miyagawa F. Current Knowledge of the Molecular Pathogenesis of Cutaneous Lupus Erythematosus. J Clin Med. 2023 Jan 27;12(3):987. doi: 10.3390/jcm12030987[↩]
- Kuhn A., Lehmann P., Ruzicka T. Cutaneous Lupus Erythematosus. Springer; Berlin/Heidelberg, Germany: 2004. pp. 53–58.[↩]
- Kuhn A, Landmann A. The classification and diagnosis of cutaneous lupus erythematosus. J Autoimmun. 2014 Feb-Mar;48-49:14-9. doi: 10.1016/j.jaut.2014.01.021[↩]
- Kuhn A, Kuehn E, Meuth AM, et al.. Development of a core set questionnaire by the European Society of cutaneous lupus erythematosus (EUSCLE). Autoimmun Rev 2009;8:702–12. 10.1016/j.autrev.2009.02.022[↩]
- Lu Q, Long H, Chow S, et al.. Guideline for the diagnosis, treatment and long-term management of cutaneous lupus erythematosus. J Autoimmun 2021;123:102707. 10.1016/j.jaut.2021.102707[↩]
- Worm M, Zidane M, Eisert L, Fischer-Betz R, Foeldvari I, Günther C, Iking-Konert C, Kreuter A, Müller-Ladner U, Nast A, Ochsendorf F, Schneider M, Sticherling M, Tenbrock K, Wenzel J, Kuhn A. S2k guideline: Diagnosis and management of cutaneous lupus erythematosus – Part 1: Classification, diagnosis, prevention, activity scores. J Dtsch Dermatol Ges. 2021 Aug;19(8):1236-1247. doi: 10.1111/ddg.14492[↩]
- Kunz M., Konig I.R., Schillert A., Kruppa J., Ziegler A., Grallert H., Müller-Nurasyid M., Lieb W., Franke A., Ranki A., et al. Genome-wide association study identifies new susceptibility loci for cutaneous lupus erythematosus. Exp. Dermatol. 2015;24:510–515. doi: 10.1111/exd.12708[↩][↩]
- Kuhn A., Wenzel J., Bijl M. Lupus erythematosus revisited. Semin. Immunopathol. 2016;38:97–112. doi: 10.1007/s00281-015-0550-0[↩][↩][↩]
- Gilliam J.N., Sontheimer R.D. Distinctive cutaneous subsets in the spectrum of lupus erythematosus. J. Am. Acad. Dermatol. 1981;4:471–475. doi: 10.1016/S0190-9622(81)80261-7[↩]
- Watanabe T., Tsuchida T. Classification of Lupus erythematosus Based upon Cutaneous Manifestations. Dermatological, systemic and laboratory findings in 191 patients. Dermatology. 1995;190:277–283. doi: 10.1159/000246716[↩]
- Gilliam JN, Sontheimer RD. Distinctive cutaneous subsets in the spectrum of lupus erythematosus. J Am Acad Dermatol. 1981 Apr;4(4):471-5. doi: 10.1016/s0190-9622(81)80261-7[↩][↩]
- Obermoser G, Sontheimer RD, Zelger B. Overview of common, rare and atypical manifestations of cutaneous lupus erythematosus and histopathological correlates. Lupus. 2010 Aug;19(9):1050-70. doi: 10.1177/0961203310370048[↩]
- Lee HJ, Sinha AA. Cutaneous lupus erythematosus: understanding of clinical features, genetic basis, and pathobiology of disease guides therapeutic strategies. Autoimmunity. 2006 Sep;39(6):433-44. doi: 10.1080/08916930600886851[↩][↩][↩]
- Yell JA, Mbuagbaw J, Burge SM. Cutaneous manifestations of systemic lupus erythematosus. Br J Dermatol. 1996 Sep;135(3):355-62.[↩]
- Rothfield N, Sontheimer RD, Bernstein M. Lupus erythematosus: systemic and cutaneous manifestations. Clin Dermatol. 2006 Sep-Oct;24(5):348-62. doi: 10.1016/j.clindermatol.2006.07.014[↩]
- Bielsa I, Herrero C, Font J, Mascaró JM. Lupus erythematosus and toxic epidermal necrolysis. J Am Acad Dermatol. 1987 Jun;16(6):1265-7. doi: 10.1016/s0190-9622(87)80031-2[↩]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Care Services; Committee on Selected Immune Disorders and Disability. Selected Immune Disorders and Disability. Washington (DC): National Academies Press (US); 2022 May 24. 3, Systemic Lupus Erythematosus. Available from: https://www.ncbi.nlm.nih.gov/books/NBK584485[↩]
- Subacute cutaneous lupus erythematosus. https://dermnetnz.org/topics/subacute-cutaneous-lupus-erythematosus[↩][↩][↩][↩]
- Biazar C., Sigges J., Patsinakidis N., Ruland V., Amler S., Bonsmann G., Kuhn A., Haust M., Nyberg F., Bata Z., et al. Cutaneous lupus erythematosus: First multicenter database analysis of 1002 patients from the European Society of Cutaneous Lupus Erythematosus (EUSCLE) Autoimmun. Rev. 2013;12:444–454. doi: 10.1016/j.autrev.2012.08.019[↩][↩]
- Werth VP. Cutaneous lupus: insights into pathogenesis and disease classification. Bull NYU Hosp Jt Dis. 2007;65(3):200-4.[↩][↩]
- Lin JH, Dutz JP, Sontheimer RD, Werth VP. Pathophysiology of cutaneous lupus erythematosus. Clin Rev Allergy Immunol. 2007 Oct;33(1-2):85-106. doi: 10.1007/s12016-007-0031-x[↩][↩]
- Klauninger R, Skog A, Horvath L, Winqvist O, Edner A, Bremme K, Sonesson SE, Wahren-Herlenius M. Serologic follow-up of children born to mothers with Ro/SSA autoantibodies. Lupus. 2009 Aug;18(9):792-8. doi: 10.1177/0961203309103188[↩][↩]
- Heelan K, Watson R, Collins SM. Neonatal lupus syndrome associated with ribonucleoprotein antibodies. Pediatr Dermatol. 2013 Jul-Aug;30(4):416-23. doi: 10.1111/pde.12088[↩][↩]
- Sandholdt LH, Laurinaviciene R, Bygum A. Proton pump inhibitor-induced subacute cutaneous lupus erythematosus. Br J Dermatol. 2014 Feb;170(2):342-51. doi: 10.1111/bjd.12699[↩]
- Kuhn A, Bein D, Bonsmann G. The 100th anniversary of lupus erythematosus tumidus. Autoimmun Rev. 2009;8(6):441–448. doi: 10.1016/j.autrev.2008.12.010[↩]
- Jefferson GD, Aakalu VK, Braniecki M. Tumid lupus: An unexpected diagnosis for the otolaryngologist. Am J Otolaryngol. 2017 Mar-Apr;38(2):257-259. doi: 10.1016/j.amjoto.2017.01.003[↩]
- Fogagnolo L, Soares TC, Senna CG, Souza EM, Blotta MH, Cintra ML. Cytotoxic granules in distinct subsets of cutaneous lupus erythematosus. Clin Exp Dermatol. 2014 Oct;39(7):835-9. doi: 10.1111/ced.12428[↩]
- Gambichler T, Pätzholz J, Schmitz L, Lahner N, Kreuter A. FOXP3+ and CD39+ regulatory T cells in subtypes of cutaneous lupus erythematosus. J Eur Acad Dermatol Venereol. 2015 Oct;29(10):1972-7. doi: 10.1111/jdv.13123[↩]
- Böckle BC, Sepp NT. Smoking is highly associated with discoid lupus erythematosus and lupus erythematosus tumidus: analysis of 405 patients. Lupus. 2015 Jun;24(7):669-74. doi: 10.1177/0961203314559630[↩][↩][↩]
- Schneider SW, Staender S, Schlüter B, Luger TA, Bonsmann G. Infliximab-induced lupus erythematosus tumidus in a patient with rheumatoid arthritis. Arch Dermatol. 2006 Jan;142(1):115-6. doi: 10.1001/archderm.142.1.115[↩]
- Lehmann P, Hölzle E, Kind P, Goerz G, Plewig G. Experimental reproduction of skin lesions in lupus erythematosus by UVA and UVB radiation. J Am Acad Dermatol. 1990 Feb;22(2 Pt 1):181-7. doi: 10.1016/0190-9622(90)70020-i[↩]
- Kuhn A, Sonntag M, Richter-Hintz D, Oslislo C, Megahed M, Ruzicka T, Lehmann P. Phototesting in lupus erythematosus tumidus–review of 60 patients. Photochem Photobiol. 2001 May;73(5):532-6. doi: 10.1562/0031-8655(2001)073<0532:piletr>2.0.co;2[↩]
- Kuhn A, Sonntag M, Richter-Hintz D, Oslislo C, Megahed M, Ruzicka T, Lehmann P. Phototesting in lupus erythematosus: a 15-year experience. J Am Acad Dermatol. 2001 Jul;45(1):86-95. doi: 10.1067/mjd.2001.114589[↩]
- Kuhn A, Sonntag M, Ruzicka T, Lehmann P, Megahed M. Histopathologic findings in lupus erythematosus tumidus: review of 80 patients. J Am Acad Dermatol. 2003;48(6):901–908. doi: 10.1067/mjd.2003.435[↩]
- Alexiades-Armenakas MR, Baldassano M, Bince B, et al. Tumid lupus erythematosus: criteria for classification with immunohistochemical analysis. Arthritis Rheum. 2003;49(4):494–500. doi: 10.1002/art.11206[↩]
- Rodriguez-Caruncho C, Bielsa I, Fernández-Figueras MT, Roca J, Carrascosa JM, Ferrándiz C. Lupus erythematosus tumidus: a clinical and histological study of 25 cases. Lupus. 2015;24(7):751–755. doi: 10.1177/0961203314560204[↩]
- Patsinakidis N, Kautz O, Gibbs BF, Raap U. Lupus erythematosus tumidus: clinical perspectives. Clin Cosmet Investig Dermatol. 2019 Oct 1;12:707-719. doi: 10.2147/CCID.S166723[↩][↩]
- Schmitt V, Meuth AM, Amler S, Kuehn E, Haust M, Messer G, Bekou V, Sauerland C, Metze D, Köpcke W, Bonsmann G, Kuhn A. Lupus erythematosus tumidus is a separate subtype of cutaneous lupus erythematosus. Br J Dermatol. 2010 Jan;162(1):64-73. doi: 10.1111/j.1365-2133.2009.09401.x Erratum in: Br J Dermatol. 2010 Jan;162(1):233-4.[↩][↩]
- Kuhn A, Bein D, Bonsmann G. The 100th anniversary of lupus erythematosus tumidus. Autoimmun Rev. 2009 May;8(6):441-8. doi: 10.1016/j.autrev.2008.12.010[↩]
- Choonhakarn C, Poonsriaram A, Chaivoramukul J. Lupus erythematosus tumidus. Int J Dermatol. 2004 Nov;43(11):815-8. doi: 10.1111/j.1365-4632.2004.02073.x[↩]
- Vieira V, Del Pozo J, Yebra-Pimentel MT, Martínez W, Fonseca E. Lupus erythematosus tumidus: a series of 26 cases. Int J Dermatol. 2006 May;45(5):512-7. doi: 10.1111/j.1365-4632.2004.02574.x[↩]
- Kuhn A, Aberer E, Bata-Csörgő Z, Caproni M, Dreher A, Frances C, Gläser R, Klötgen HW, Landmann A, Marinovic B, Nyberg F, Olteanu R, Ranki A, Szepietowski JC, Volc-Platzer B. S2k guideline for treatment of cutaneous lupus erythematosus – guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermatology and Venereology (EADV). J Eur Acad Dermatol Venereol. 2017 Mar;31(3):389-404. doi: 10.1111/jdv.14053[↩][↩]
- Kuhn A, Ruland V, Bonsmann G. Cutaneous lupus erythematosus: update of therapeutic options part I. J Am Acad Dermatol. 2011 Dec;65(6):e179-93. doi: 10.1016/j.jaad.2010.06.018[↩][↩]
- Saleh D, Grubbs H, Koritala T, et al. Tumid Lupus Erythematosus. [Updated 2023 Jun 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482515[↩]
- Abdullah L, Abbas O. Dermacase: Can you identify this condition? Tumid lupus erythematosus. Can Fam Physician. 2012 Jul;58(7):765, 769. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3395523[↩]
- Chang J, Werth VP. Therapeutic options for cutaneous lupus erythematosus: recent advances and future prospects. Expert Rev Clin Immunol. 2016 Oct;12(10):1109-21. doi: 10.1080/1744666X.2016.1188006[↩]
- Cardinali C, Caproni M, Bernacchi E, Amato L, Fabbri P. The spectrum of cutaneous manifestations in lupus erythematosus–the Italian experience. Lupus. 2000;9(6):417-23. doi: 10.1191/096120300678828569[↩][↩]
- Vera-Recabarren MA, García-Carrasco M, Ramos-Casals M, Herrero C. Comparative analysis of subacute cutaneous lupus erythematosus and chronic cutaneous lupus erythematosus: clinical and immunological study of 270 patients. Br J Dermatol. 2010 Jan;162(1):91-101. doi: 10.1111/j.1365-2133.2009.09472.x[↩]
- Kuhn A. Cutaneous manifestations of Lupus Erythematosus. Handbook Syst Autoimmun Dis. 2006;5:49–59.[↩]
- Elman S.A., Joyce C., Nyberg F., Furukawa F., Goodfield M., Hasegawa M., Marinovic B., Szepietowski J.C., Dutz J., Werth V.P., et al. Development of classification criteria for discoid lupus erythematosus: Results of a Delphi exercise. J. Am. Acad. Dermatol. 2017;77:261–267. doi: 10.1016/j.jaad.2017.02.030[↩]
- Kuhn A, Lehmann P, Ruzicka T, editors. Dusseldorf: Springer; 2005. Cutaneous Lupus Erythematosus.[↩][↩][↩][↩]
- Obermoser G. Lupus erythematosus and the skin: a journey at times perplexing, usually complex, often challenging, and evermore exhilarating. Lupus. 2010 Aug;19(9):1009-11. doi: 10.1177/0961203310373108[↩]
- Early Diagnosis and Treatment of Discoid Lupus Erythematosus. Suresh Panjwani. The Journal of the American Board of Family Medicine Mar 2009, 22 (2) 206-213; https://doi.org/10.3122/jabfm.2009.02.080075[↩]
- Grönhagen CM, Nyberg F. Cutaneous lupus erythematosus: An update. Indian Dermatol Online J. 2014 Jan;5(1):7-13. doi: 10.4103/2229-5178.126020[↩][↩][↩][↩][↩]
- Massone C, Kodama K, Salmhofer W, Abe R, Shimizu H, Parodi A, Kerl H, Cerroni L. Lupus erythematosus panniculitis (lupus profundus): clinical, histopathological, and molecular analysis of nine cases. J Cutan Pathol. 2005 Jul;32(6):396-404. doi: 10.1111/j.0303-6987.2005.00351.x[↩]
- Tuffanelli DL. Lupus Erythematosus Panniculitis (Profundus): Clinical and Immunologic Studies. Arch Dermatol. 1971;103(3):231–242. doi:10.1001/archderm.1971.04000150001001[↩][↩]
- Strober, B. E. (2001). Lupus panniculitis (lupus profundus). Dermatology Online Journal, 7(2). http://dx.doi.org/10.5070/D38f30c7rd[↩]
- Requena L, Sánchez Yus E. Panniculitis. Part II. Mostly lobular panniculitis. J Am Acad Dermatol. 2001 Sep;45(3):325-61; quiz 362-4. doi: 10.1067/mjd.2001.114735[↩]
- Walling HW, Sontheimer RD. Cutaneous lupus erythematosus: issues in diagnosis and treatment. Am J Clin Dermatol. 2009;10(6):365-81. doi: 10.2165/11310780-000000000-00000[↩]
- Castrillón MA, Murrell DF. Lupus profundus limited to a site of trauma: Case report and review of the literature. Int J Womens Dermatol. 2017 May 5;3(2):117-120. doi: 10.1016/j.ijwd.2017.03.002[↩][↩][↩][↩]
- Kündig TM, Trüeb RM, Krasovec M. Lupus profundus/panniculitis. Dermatology. 1997;195(1):99-101. doi: 10.1159/000245706[↩][↩]
- Fraga J, García-Díez A. Lupus erythematosus panniculitis. Dermatol Clin. 2008 Oct;26(4):453-63, vi. doi: 10.1016/j.det.2008.06.002[↩][↩][↩][↩]
- Lee HE, Ko JY, Lee CW. A case of lupus erythematosus panniculitis presenting as combined linear and lipoatrophic skin lesions. Int J Dermatol. 2011 Feb;50(2):203-5. doi: 10.1111/j.1365-4632.2010.04457.x[↩][↩]
- Marzano AV, Tanzi C, Caputo R, Alessi E. Sclerodermic linear lupus panniculitis: report of two cases. Dermatology. 2005;210(4):329-32. doi: 10.1159/000084760[↩][↩]
- Mitxelena J, Martínez-Peñuela A, Cordoba A, Yanguas I. Linear and annular lupus panniculitis of the scalp. Actas Dermosifiliogr. 2013 Dec;104(10):936-9. English, Spanish. doi: 10.1016/j.ad.2012.12.014[↩][↩]
- Stork J, Vosmík F. Lupus erythematosus panniculitis with morphea-like lesions. Clin Exp Dermatol. 1994 Jan;19(1):79-82. doi: 10.1111/j.1365-2230.1994.tb01125.x[↩]
- Bacanli A, Uzun S, Ciftcioglu MA, Alpsoy E. A case of lupus erythematosus profundus with unusual manifestations. Lupus. 2005;14(5):403-5. doi: 10.1191/0961203305lu2088cr[↩]
- White WL, Sherertz EF, Berg D, Clark RE. Periparotid lupus erythematosus panniculitis. Clinicopathologic correlation of two cases presenting as primary parotid disease. Arch Pathol Lab Med. 1993 May;117(5):535-9.[↩]
- Franke W, Kuhn A, Megahed M, Krutmann J, Ruzicka T, Lehmann P. Periorbitales Odem als Initialsymptom eines Lupus erythematodes profundus. Kasuistik und Diskussion der Literatur [Periorbital edema as the initial symptom of lupus erythematosus profundus. Case report and discussion of the literature]. Hautarzt. 1999 Dec;50(12):889-92. German. doi: 10.1007/s001050051005[↩]
- Grossberg E, Scherschun L, Fivenson DP. Lupus profundus: not a benign disease. Lupus. 2001;10(7):514-6. doi: 10.1191/096120301678416105[↩][↩][↩]
- Martens PB, Moder KG, Ahmed I. Lupus panniculitis: clinical perspectives from a case series. J Rheumatol. 1999 Jan;26(1):68-72.[↩]
- Patel RM, Marfatia YS. Lupus panniculitis as an initial manifestation of systemic lupus erythematosus. Indian J Dermatol. 2010;55(1):99-101. doi: 10.4103/0019-5154.60364[↩]
- Zhao YK, Wang F, Chen WN, Xu R, Wang Z, Jiang YW, Luo DQ, Han JD. Lupus Panniculitis as an Initial Manifestation of Systemic Lupus Erythematosus: A Case Report. Medicine (Baltimore). 2016 Apr;95(16):e3429. doi: 10.1097/MD.0000000000003429[↩]
- Arps DP, Patel RM. Lupus profundus (panniculitis): a potential mimic of subcutaneous panniculitis-like T-cell lymphoma. Arch Pathol Lab Med. 2013 Sep;137(9):1211-5. doi: 10.5858/arpa.2013-0253-CR[↩]
- Ng PP, Tan SH, Tan T. Lupus erythematosus panniculitis: a clinicopathologic study. Int J Dermatol. 2002 Aug;41(8):488-90. doi: 10.1046/j.1365-4362.2002.01510.x[↩]
- Arai S, Katsuoka K. Clinical entity of Lupus erythematosus panniculitis/lupus erythematosus profundus. Autoimmun Rev. 2009 May;8(6):449-52. doi: 10.1016/j.autrev.2008.12.011[↩]
- Yell JA, Burge SM. Lupus erythematosus profundus treated with clobetasol propionate under a hydrocolloid dressing. Br J Dermatol. 1993 Jan;128(1):103. doi: 10.1111/j.1365-2133.1993.tb00158.x[↩]
- Bednarek A, Bartoszak L, Samborski W. Case report on a patient with lupus panniculitis. Postepy Dermatol Alergol. 2015 Feb;32(1):59-62. doi: 10.5114/pdia.2014.40958[↩][↩]
- Espírito Santo J, Gomes MF, Gomes MJ, Peixoto L, C Pereira S, Acabado A, Freitas J, de Sousa GV. Intravenous immunoglobulin in lupus panniculitis. Clin Rev Allergy Immunol. 2010 Apr;38(2-3):307-18. doi: 10.1007/s12016-009-8162-x[↩][↩][↩][↩][↩]
- Housman TS, Jorizzo JL, McCarty MA, Grummer SE, Fleischer AB Jr, Sutej PG. Low-dose thalidomide therapy for refractory cutaneous lesions of lupus erythematosus. Arch Dermatol. 2003 Jan;139(1):50-4. doi: 10.1001/archderm.139.1.50[↩][↩]
- Ujiie H, Shimizu T, Ito M, Arita K, Shimizu H. Lupus erythematosus profundus successfully treated with dapsone: review of the literature. Arch Dermatol. 2006 Mar;142(3):399-401. doi: 10.1001/archderm.142.3.399[↩]
- McArdle A, Baker JF. A case of “refractory” lupus erythematosus profundus responsive to rituximab [case report]. Clin Rheumatol. 2009 Jun;28(6):745-6. doi: 10.1007/s10067-009-1158-3[↩]
- Moreno-Suárez F, Pulpillo-Ruiz A. Rituximab for the treatment of lupus erythematosus panniculitis. Dermatol Ther. 2013 Sep-Oct;26(5):415-8. doi: 10.1111/dth.12014[↩]
- Patel S, Hardo F. Chilblain lupus erythematosus. BMJ Case Rep. 2013 Nov 27;2013:bcr2013201165 https://doi.org/10.1136/bcr-2013-201165[↩][↩]
- Dubey S, Joshi N, Stevenson O, Gordon C, Reynolds JA. Chilblains in immune-mediated inflammatory diseases: a review. Rheumatology (Oxford). 2022 Nov 28;61(12):4631-4642. doi: 10.1093/rheumatology/keac231[↩][↩][↩]
- Lambertini M, Vincenzi C, Dika E, La Placa M. Chilblain Lupus with Nail Involvement: A Case Report and a Brief Overview. Skin Appendage Disord. 2018 Nov;5(1):42-45. doi: 10.1159/000488543[↩]
- Hutchinson J. Harveian Lectures on Lupus. Br Med J. 1888 Jan 14;1(1411):58-63. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2197256/pdf/brmedj04656-0002.pdf[↩]
- Millard LG, Rowell NR. Chilblain lupus erythematosus (Hutchinson). A clinical and laboratory study of 17 patients. Br J Dermatol. 1978 May;98(5):497-506. doi: 10.1111/j.1365-2133.1978.tb01935.x[↩][↩][↩][↩][↩]
- Petri M, Orbai AM, Alarcón GS, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012 Aug;64(8):2677-86. doi: 10.1002/art.34473[↩]
- Viguier M, Pinquier L, Cavelier-Balloy B, de la Salmonière P, Cordoliani F, Flageul B, Morel P, Dubertret L, Bachelez H. Clinical and histopathologic features and immunologic variables in patients with severe chilblains. A study of the relationship to lupus erythematosus. Medicine (Baltimore). 2001 May;80(3):180-8. doi: 10.1097/00005792-200105000-00004[↩]
- Bansal S, Goel A. Chilblain lupus erythematosus in an adolescent girl. Indian Dermatol Online J. 2014 Nov;5(Suppl 1):S30-2. doi: 10.4103/2229-5178.144522[↩][↩]
- Arias-Santiago SA, Girón-Prieto MS, Callejas-Rubio JL, Fernández-Pugnaire MA, Ortego-Centeno N. Lupus pernio or chilblain lupus?: two different entities. Chest. 2009 Sep;136(3):946-947. doi: 10.1378/chest.09-1005[↩]
- Pock L, Petrovská P, Becvár R, Mandys V, Hercogová J. Verrucous form of chilblain lupus erythematosus. J Eur Acad Dermatol Venereol. 2001 Sep;15(5):448-51. doi: 10.1046/j.1468-3083.2001.00346.x[↩]
- Franceschini F, Calzavara-Pinton P, Quinzanini M, Cavazzana I, Bettoni L, Zane C, Facchetti F, Airò P, McCauliffe DP, Cattaneo R. Chilblain lupus erythematosus is associated with antibodies to SSA/Ro. Lupus. 1999;8(3):215-9. doi: 10.1191/096120399678847632[↩][↩][↩]
- Bouaziz JD, Barete S, Le Pelletier F, Amoura Z, Piette JC, Francès C. Cutaneous lesions of the digits in systemic lupus erythematosus: 50 cases. Lupus. 2007;16(3):163-7. doi: 10.1177/0961203306075792[↩]
- Aoki T, Ishizawa T, Hozumi Y, Aso K, Kondo S. Chilblain lupus erythematosus of Hutchinson responding to surgical treatment: a report of two patients with anti-Ro/SS-A antibodies. Br J Dermatol. 1996 Mar;134(3):533-7.[↩][↩]
- Su WP, Perniciaro C, Rogers RS 3rd, White JW Jr. Chilblain lupus erythematosus (lupus pernio): clinical review of the Mayo Clinic experience and proposal of diagnostic criteria. Cutis. 1994 Dec;54(6):395-9.[↩][↩][↩][↩]
- Cappel JA, Wetter DA. Clinical characteristics, etiologic associations, laboratory findings, treatment, and proposal of diagnostic criteria of pernio (chilblains) in a series of 104 patients at Mayo Clinic, 2000 to 2011. Mayo Clin Proc. 2014 Feb;89(2):207-15. doi: 10.1016/j.mayocp.2013.09.020[↩][↩]
- Hedrich CM, Fiebig B, Hauck FH, Sallmann S, Hahn G, Pfeiffer C, Heubner G, Lee-Kirsch MA, Gahr M. Chilblain lupus erythematosus–a review of literature. Clin Rheumatol. 2008 Aug;27(8):949-54. doi: 10.1007/s10067-008-0942-9. Epub 2008 Jun 10. Erratum in: Clin Rheumatol. 2008 Oct;27(10):1341. Lee-Kirsch, Min Ae [added].[↩][↩][↩][↩]
- Allegue F, Alonso ML, Rocamora A, Ledo A. Chilblain lupus erythematosus and antiphospholipid antibody syndrome. J Am Acad Dermatol. 1988 Nov;19(5 Pt 1):908-10. doi: 10.1016/s0190-9622(88)80377-3[↩]
- Rustin MH, Newton JA, Smith NP, Dowd PM. The treatment of chilblains with nifedipine: the results of a pilot study, a double-blind placebo-controlled randomized study and a long-term open trial. Br J Dermatol. 1989 Feb;120(2):267-75. doi: 10.1111/j.1365-2133.1989.tb07792.x[↩][↩][↩]
- Souwer IH, Bor JH, Smits P, Lagro-Janssen AL. Assessing the effectiveness of topical betamethasone to treat chronic chilblains: a randomised clinical trial in primary care. Br J Gen Pract. 2017 Mar;67(656):e187-e193. doi: 10.3399/bjgp17X689413[↩]
- Khalid T, Maan Shehzad AM.. K. Comparison of efficacy and safety of topical glyceryl trinitrate vs. oral nifedipine in idiopathic perniosis: results of a randomized clinical trial. JPAD 2014;24:342–7.[↩]
- Kubais TA, Hasan AS, Awad KM, Tawfiq EM.. Treatment of perniosis with oral nifedipine in comparison with topical 5% minoxidil solution in Iraqi patients: single blind comparative study. Al-Anbar Med J 2010;8:40–6.[↩]
- Dowd PM, Rustin MH, Lanigan S. Nifedipine in the treatment of chilblains. Br Med J (Clin Res Ed). 1986 Oct 11;293(6552):923-4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1341713/pdf/bmjcred00256-0025b.pdf[↩]
- Souwer IH, Bor JH, Smits P, Lagro-Janssen AL. Nifedipine vs Placebo for Treatment of Chronic Chilblains: A Randomized Controlled Trial. Ann Fam Med. 2016 Sep;14(5):453-9. doi: 10.1370/afm.1966[↩]
- Jain AK, Raghavendra KR, Margaankar M.. A random comparative therapeutic trial of oral nifedipine v/s topical 5% minoxidil gel in patients of perniosis at a tertiary care center of North-western India. Indian J Clin Exp Dermatol 2018;4:62–5.[↩]
- McNamara DB, Champion HC, Kadowitz PJ. Pharmacologic management of peripheral vascular disease. Surg Clin North Am. 1998 Jun;78(3):447-64. doi: 10.1016/s0039-6109(05)70325-x[↩]
- Noaimi AA, Fadheel BM. Treatment of perniosis with oral pentoxyfylline in comparison with oral prednisolone plus topical clobetasol ointment in Iraqi patients. Saudi Med J. 2008 Dec;29(12):1762-4.[↩]
- Al-Sudany NK. Treatment of primary perniosis with oral pentoxifylline (a double-blind placebo-controlled randomized therapeutic trial). Dermatol Ther. 2016 Jul;29(4):263-8. doi: 10.1111/dth.12350[↩][↩]
- Noaimi AA, Salman HA, Sharquie KE.. Treatment of perniosis with oral tadalafil, pentoxifylline or prednisolone: a therapeutic comparative study. J Fac Med Baghdad 2015;57:210–3.[↩]
- Boehm I, Bieber T. Chilblain lupus erythematosus Hutchinson: successful treatment with mycophenolate mofetil. Arch Dermatol. 2001 Feb;137(2):235-6.[↩]
- Wenzel J, Brähler S, Bauer R, Bieber T, Tüting T. Efficacy and safety of methotrexate in recalcitrant cutaneous lupus erythematosus: results of a retrospective study in 43 patients. Br J Dermatol. 2005 Jul;153(1):157-62. doi: 10.1111/j.1365-2133.2005.06552.x[↩]
- Gouillon L, Debarbieux S, Berruyer M, Fabien N, Lega JC, Thomas L. Chilblain lupus erythematosus treated successfully with mycophenolate mofetil. Int J Dermatol. 2017 Aug;56(8):e158-e159. doi: 10.1111/ijd.13614[↩]
- Breathnach SM, Wells GC. Chilblain lupus erythematosus with response to chemical sympathectomy. Br J Dermatol. 1979 Jul;101 Suppl 17:49-51.[↩]
- Chasset F, Bouaziz JD, Costedoat-Chalumeau N, Francès C, Arnaud L. Efficacy and comparison of antimalarials in cutaneous lupus erythematosus subtypes: a systematic review and meta-analysis. Br J Dermatol. 2017 Jul;177(1):188-196. doi: 10.1111/bjd.15312[↩]
- Yang X, Perez OA, English JC 3rd. Successful treatment of perniosis with hydroxychloroquine. J Drugs Dermatol. 2010 Oct;9(10):1242-6.[↩]
- Patel S, Hardo F. Chilblain lupus erythematosus. BMJ Case Rep. 2013 Nov 27;2013:bcr2013201165. doi: 10.1136/bcr-2013-201165[↩]
- Horino T, Ichii O, Terada Y. Hydroxychloroquine-Associated Hyperpigmentation in Chilblain Lupus Erythematosus. J Clin Rheumatol. 2020 Sep;26(6):e192. doi: 10.1097/RHU.0000000000001061[↩]
- Doutre MS, Beylot C, Beylot J, Pompougnac E, Royer P. Chilblain lupus erythematosus: report of 15 cases. Dermatology. 1992;184(1):26-8. doi: 10.1159/000247494[↩]
- Clydesdale GJ, Dandie GW, Muller HK. Ultraviolet light induced injury: immunological and inflammatory effects. Immunol Cell Biol. (2001) 79:547–68. 10.1046/j.1440-1711.2001.01047.x[↩]
- Achtman JC, Werth VP. Pathophysiology of cutaneous lupus erythematosus. Arthritis Res Ther. 2015 Aug 10;17(1):182. doi: 10.1186/s13075-015-0706-2[↩]
- Wenzel J. Cutaneous lupus erythematosus: New insights into pathogenesis and therapeutic strategies. Nat. Rev. Rheumatol. 2019;15:519–532. doi: 10.1038/s41584-019-0272-0[↩]
- Piipponen M, Li D, Landén NX. The Immune Functions of Keratinocytes in Skin Wound Healing. Int J Mol Sci. 2020 Nov 20;21(22):8790. doi: 10.3390/ijms21228790[↩]
- Pastar I., Stojadinovic O., Yin N.C., Ramirez H., Nusbaum A.G., Sawaya A., Patel S.B., Khalid L., Isseroff R.R., Tomic-Canic M. Epithelialization in Wound Healing: A Comprehensive Review. Adv. Wound Care. 2014;3:445–464. doi: 10.1089/wound.2013.0473[↩]
- Souren J.M., Ponec M., van Wijk R. Contraction of collagen by human fibroblasts and keratinocytes. In Vitro Cell. Dev. Biol. 1989;25:1039–1045. doi: 10.1007/BF02624138[↩]
- Isaac C., Paggiaro A.O., Aldunate J.L.C.B., Herson M.R., Altran S.C., Mônica Beatriz M., Ferreira M.C. Role of keratinocytes in wound contraction: An impact assessment using a model of collagen matrix populated with fibroblasts. Rev. Bras. Cir. Plást. 2011;26:402–406. doi: 10.1590/S1983-51752011000300007[↩]
- Krausgruber T., Fortelny N., Fife-Gernedl V., Senekowitsch M., Schuster L.C., Lercher A., Nemc A., Schmidl C., Rendeiro A.F., Bergthaler A., et al. Structural cells are key regulators of organ-specific immune responses. Nature. 2020;583:296–302. doi: 10.1038/s41586-020-2424-4[↩]
- Piette E.W., Foering K.P., Chang A.Y., Okawa J., Ten Have T.R., Feng R., Werth V.P. The Impact of smoking in cutaneous lupus erythematosus. Arch. Dermatol. 2012;148:317–322. doi: 10.1001/archdermatol.2011.342[↩]
- Bataille P., Chasset F., Monfort J.-B., De Risi-Pugliese T., Soria A., Francès C., Barbaud A., Senet P. Cutaneous drug-induced lupus erythematosus: Clinical and immunological characteristics and update on new associated drugs. Ann. Dermatol. Vénéréologie. 2021;148:211–220. doi: 10.1016/j.annder.2021.02.006[↩][↩][↩][↩][↩]
- Vaglio A., Grayson P.C., Fenaroli P., Gianfreda D., Boccaletti V., Ghiggeri G.M., Moroni G. Drug-induced lupus: Traditional and new concepts. Autoimmun. Rev. 2018;17:912–918. doi: 10.1016/j.autrev.2018.03.016[↩][↩][↩][↩]
- Lowe G., Henderson C., Grau R., Hansen C., Sontheimer R. A systematic review of drug-induced subacute cutaneous lupus erythematosus. Br. J. Dermatol. 2011;164:465–472. doi: 10.1111/j.1365-2133.2010.10110.x[↩][↩]
- Borucki R., Werth V.P. Cutaneous lupus erythematosus induced by drugs-novel insights. Expert Rev. Clin. Pharmacol. 2020;13:35–42. doi: 10.1080/17512433.2020.1698290[↩]
- Michaelis T.C., Sontheimer R.D., Lowe G.C. An update in drug-induced subacute cutaneous lupus erythematosus. Dermatol. Online J. 2017;23 doi: 10.5070/D3233034281[↩]
- Theofilopoulos AN, Baccala R, Beutler B, Kono DH. Type I interferons (alpha/beta) in immunity and autoimmunity. Annu Rev Immunol. (2005) 23:307–36. 10.1146/annurev.immunol.23.021704.115843[↩]
- Elkon KB, Wiedeman A. Type I IFN system in the development and manifestations of SLE. Curr Opin Rheumatol. (2012) 24:499–505. 10.1097/BOR.0b013e3283562c3e[↩]
- Wenzel J, Tüting T. Identification of type I interferon-associated inflammation in the pathogenesis of cutaneous lupus erythematosus opens up options for novel therapeutic approaches. Exp Dermatol. (2007) 16:454–63. 10.1111/j.1600-0625.2007.00556.x[↩]
- Günther C. Nucleic acid immunity in the pathogenesis of cutaneous lupus erythematosus. Front Immunol. (2019) 10:1636. 10.3389/fimmu.2019.01636[↩][↩]
- Bijl M, Reefman E, Horst G, Limburg PC, Kallenberg CG. Reduced uptake of apoptotic cells by macrophages in systemic lupus erythematosus: correlates with decreased serum levels of complement. Ann Rheum Dis. (2006) 65:57–63. 10.1136/ard.2005.035733[↩]
- Kahn JS, Deverapalli SC, Rosmarin DM. JAK-STAT signaling pathway inhibition: a role for treatment of discoid lupus erythematosus and dermatomyositis. Int J Dermatol. 2018 Aug;57(8):1007-1014. doi: 10.1111/ijd.14064[↩]
- Two A, So JK, Paravar T. Discoid Lupus and Human Immunodeficiency Virus: A Retrospective Chart Review to Determine the Prevalence and Progression of Co-occurrence of these Conditions at a Single Academic Center. Indian J Dermatol. 2017 Mar-Apr;62(2):226. doi: 10.4103/0019-5154.201750[↩]
- Chanprapaph K, Tankunakorn J, Suchonwanit P, Rutnin S. Dermatologic Manifestations, Histologic Features and Disease Progression among Cutaneous Lupus Erythematosus Subtypes: A Prospective Observational Study in Asians. Dermatol Ther (Heidelb). 2021 Feb;11(1):131-147. doi: 10.1007/s13555-020-00471-y[↩]
- Mutasim DF, Adams BB. Immunofluorescence in dermatology. J Am Acad Dermatol. 2001 Dec;45(6):803-22; quiz 822-4. doi: 10.1067/mjd.2001.117518[↩]
- Dahl MV. Usefulness of Direct Immunofluorescence in Patients With Lupus Erythematosus. Arch Dermatol. 1983;119(12):1010–1017. doi:10.1001/archderm.1983.01650360056014[↩]
- Harrist TJ, Mihm MC Jr. The specificity and clinical usefulness of the lupus band test. Arthritis Rheum. 1980 Apr;23(4):479-90. doi: 10.1002/art.1780230411[↩]
- George R, Kurian S, Jacob M, Thomas K. Diagnostic evaluation of the lupus band test in discoid and systemic lupus erythematosus. Int J Dermatol. 1995 Mar;34(3):170-3. doi: 10.1111/j.1365-4362.1995.tb01560.x[↩]
- Jessop S, Whitelaw DA, Grainge MJ, Jayasekera P. Drugs for discoid lupus erythematosus. Cochrane Database of Systematic Reviews 2017, Issue 5. Art. No.: CD002954. DOI: 10.1002/14651858.CD002954.pub3[↩][↩]
- Chang AY, Werth VP. Treatment of cutaneous lupus. Curr Rheumatol Rep. 2011 Aug;13(4):300-7. doi: 10.1007/s11926-011-0180-z[↩]
- Sontheimer RD. Skin manifestations of systemic autoimmune connective tissue disease: diagnostics and therapeutics. Best Pract Res Clin Rheumatol. 2004 Jun;18(3):429-62. doi: 10.1016/j.berh.2004.03.003[↩]
- Langan SM, Groves RW, West J. The relationship between neurological disease and bullous pemphigoid: a population-based case-control study. J Invest Dermatol. 2011 Mar;131(3):631-6. doi: 10.1038/jid.2010.357[↩]
- Chong BF, Song J, Olsen NJ. Determining risk factors for developing systemic lupus erythematosus in patients with discoid lupus erythematosus. Br J Dermatol. 2012 Jan;166(1):29-35. doi: 10.1111/j.1365-2133.2011.10610.x[↩]
- Zaalberg A, Moradi Tuchayi S, Ameri AH, Ngo KH, Cunningham TJ, Eliane JP, Livneh M, Horn TD, Rosman IS, Musiek A, Anadkat MJ, Demehri S. Chronic Inflammation Promotes Skin Carcinogenesis in Cancer-Prone Discoid Lupus Erythematosus. J Invest Dermatol. 2019 Jan;139(1):62-70. doi: 10.1016/j.jid.2018.06.185[↩]
- Chen P, Broadbent E, Coomarasamy C, Jarrett P. Illness perception in association with psychological functioning in patients with discoid lupus erythematosus. Br J Dermatol. 2015 Sep;173(3):824-6. doi: 10.1111/bjd.13709[↩]
- Parikh-Patel A, White RH, Allen M, Cress R. Risk of cancer among rheumatoid arthritis patients in California. Cancer Causes Control. 2009 Aug;20(6):1001-10. doi: 10.1007/s10552-009-9298-y[↩]
- Bernatsky S, Boivin JF, Joseph L, Rajan R, Zoma A, Manzi S, Ginzler E, Urowitz M, Gladman D, Fortin PR, Petri M, Edworthy S, Barr S, Gordon C, Bae SC, Sibley J, Isenberg D, Rahman A, Aranow C, Dooley MA, Steinsson K, Nived O, Sturfelt G, Alarcón G, Senécal JL, Zummer M, Hanly J, Ensworth S, Pope J, El-Gabalawy H, McCarthy T, St Pierre Y, Ramsey-Goldman R, Clarke A. An international cohort study of cancer in systemic lupus erythematosus. Arthritis Rheum. 2005 May;52(5):1481-90. doi: 10.1002/art.21029[↩]
- Renner R, Sticherling M. Incidental cases of subacute cutaneous lupus erythematosus in association with malignancy. Eur J Dermatol. 2008 Nov-Dec;18(6):700-4. doi: 10.1684/ejd.2008.0522[↩]
- Ho C, Shumack SP, Morris D. Subacute cutaneous lupus erythematosus associated with hepatocellular carcinoma. Australas J Dermatol. 2001 May;42(2):110-3. doi: 10.1046/j.1440-0960.2001.00491.x[↩]
- Gantzer A, Regnier S, Cosnes A, Ortonne N, Wolkenstein P, Bagot M, Duong TA. Lupus cutané subaigu et cancer: deux cas et revue de la littérature [Subacute cutaneous lupus erythematosus and cancer: two cases and literature review]. Ann Dermatol Venereol. 2011 May;138(5):409-17. French. doi: 10.1016/j.annder.2011.02.015[↩]
- Grönhagen CM, Fored CM, Granath F, Nyberg F. Increased risk of cancer among 3663 patients with cutaneous lupus erythematosus: a Swedish nationwide cohort study. Br J Dermatol. 2012 May;166(5):1053-9. doi: 10.1111/j.1365-2133.2011.10773.x[↩][↩]





{kind=link}