
Cyanotic heart disease
Cyanotic heart disease also called critical congenital heart disease, is present at birth (congenital) heart defect which results in low oxygen levels in the blood and causes the child’s lips, fingers, and toes to look blue (cyanosis) 1. Cyanosis refers to a bluish color of the skin and mucous membranes.
Cyanotic heart disease can be further classified into 3 different type of lesions 2:
- Right heart obstructive lesions
- Pulmonary atresia
- Tricuspid atresia
- Tetralogy of Fallot
- Critical pulmonary stenosis
- Left heart obstructive lesions
- Hypoplastic left heart syndrome
Interrupted aortic arch or coarctation of the aorta
Critical aortic stenosis
- Hypoplastic left heart syndrome
- Mixing lesions
- Transposition of the great arteries
- Total anomalous pulmonary venous return
- Truncus arteriosus
Normally, blood returns from the body and flows through the heart and lungs.
- Blood that is low in oxygen (blue blood) returns from the body to the right side of the heart.
- The right side of the heart then pumps the blood to the lungs, where it picks up more oxygen and becomes red.
- The oxygen-rich blood returns from the lungs to the left side of the heart. From there, it is pumped to the rest of the body.
Congenital heart disease affects 8 to 9 per 1000 live births, and approximately 25% are considered cyanotic heart disease. The incidence of congenital heart disease increase to 2% to 6% for a second pregnancy after the birth of a child with congenital heart disease or if a parent is affected. Tetralogy of Fallot is the most common cyanotic heart disease (5% of all cyanotic heart disease). Transposition of the great arteries is the second most common cyanotic heart disease (approximately 2% of all cyanotic heart disease), and it is the most common cyanotic heart disease manifesting in the first week after birth. It is estimated that 35% of infant deaths due to congenital malformations are related to cardiovascular anomalies.
Some infants may need to stay in the hospital after birth so they can receive oxygen or be put on a breathing machine. They may receive medicines to:
- Get rid of extra fluids
- Help the heart pump harder
- Keep certain blood vessels open
- Treat abnormal heartbeats or rhythms
The treatment of choice for most congenital heart diseases is surgery to repair the defect. There are many types of surgery, depending on the kind of birth defect. Surgery may be needed soon after birth, or it may be delayed for months or even years. Some surgeries may be staged as the child grows.
Your child may need to take water pills (diuretics) and other heart medicines before or after surgery. Be sure to follow the correct dosage. Regular follow-up with the provider is important.
Many children who have had heart surgery must take antibiotics before, and sometimes after having any dental work or other medical procedures. Make sure you have clear instructions from your child’s heart doctor (cardiologist).
Ask your child’s provider before getting any immunizations. Most children can follow the recommended guidelines for childhood vaccinations.
Figure 1. Normal heart blood flow

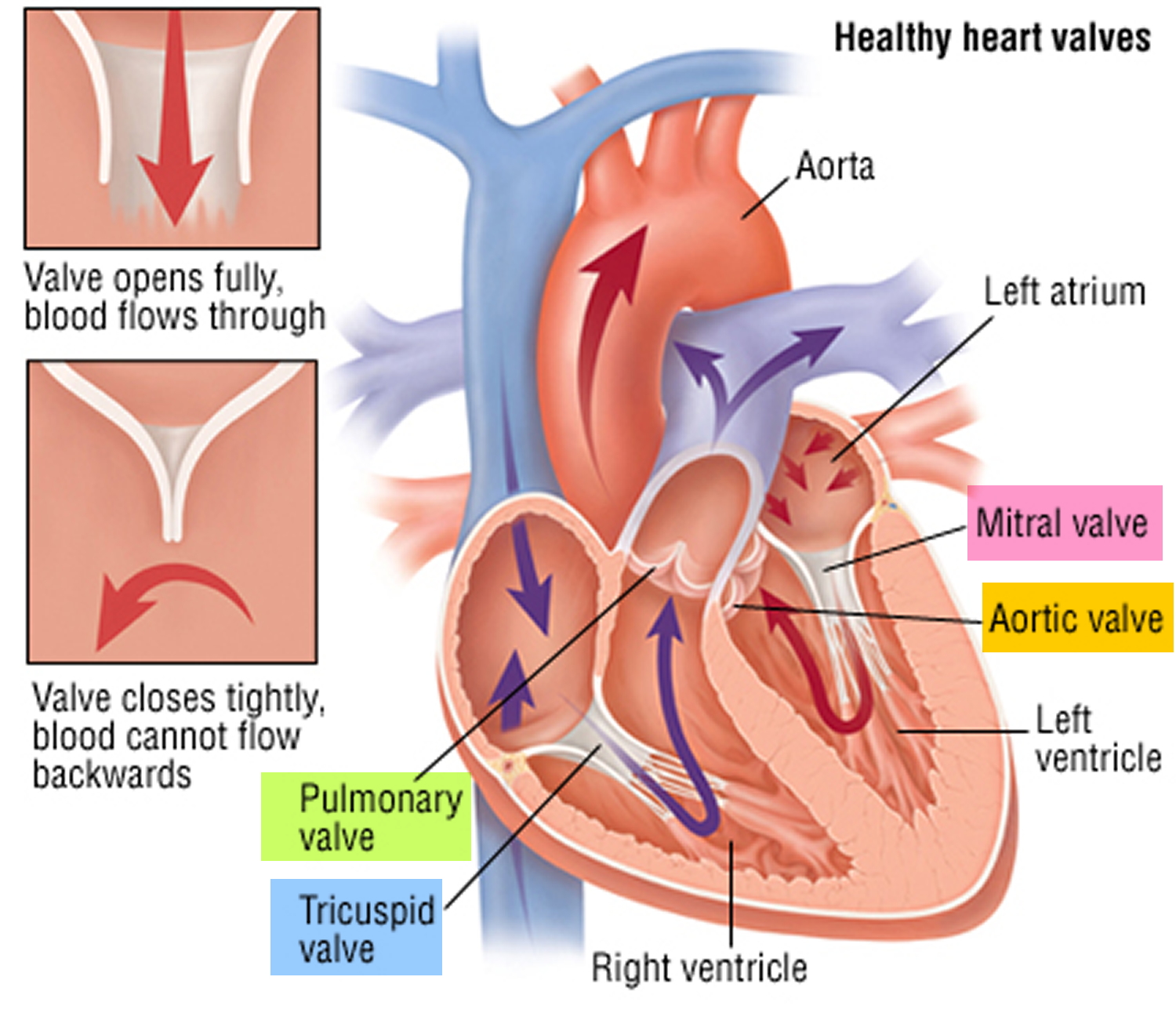
Figure 2. Heart valves function
See your child’s doctor if your baby has:
- Bluish skin (cyanosis) or grayish skin
- Breathing difficulty
- Chest pain or other pain
- Dizziness, fainting, or heart palpitations
- Feeding problems or reduced appetite
- Fever, nausea, or vomiting
- Puffy eyes or face
- Tiredness all the time
Cyanotic heart disease causes
Most forms of cyanotic heart disease have no known cause. Mothers will often wonder if something they did during the pregnancy caused the heart problem. In most cases, nothing can be attributed to the heart defect.
Many cases of cyanotic heart disease are multifactorial and result from a combination of genetic predisposition and environmental risk factors. Cyanotic heart disease is usually isolated and sporadic, but it can also be associated with genetic syndromes.
Some heart problems do occur more often in families, so there may be a genetic link to some heart conditions. Other congenital heart diseases are likely to occur if the mother had a disease while pregnant and was taking medications, such as anti-seizure medicines. However, most of the time there is no identifiable reason as to why the heart condition occurred.
Approximately 15% to 20% of infants with cyanotic heart disease are related to known chromosomal abnormalities, most of these are aneuploidies (trisomy 21, 13, and 18 and Turner syndrome). Potential environmental risk factors include maternal illnesses, including diabetes and phenylketonuria, maternal exposure to toxins or drugs and viral infections during pregnancy 1.
Heart defects that children are born with can change the way blood flows through the heart and lungs. These defects can cause less blood to flow to the lungs. They can also result in blue and red blood mixing together. This causes poorly oxygenated blood to be pumped out to the body. As a result:
- The blood that is pumped out to the body is lower in oxygen.
- Less oxygen delivered to the body can make the skin look blue (cyanosis).
Some of these heart defects involve the heart valves. These defects force blue blood to mix with red blood through abnormal heart channels. Heart valves are found between the heart and the large blood vessels that bring blood to and from the heart. These valves open up enough for blood to flow through. Then they close, keeping blood from flowing backward.
Heart valve defects that can cause cyanosis include:
- Tricuspid valve (the valve between the 2 chambers on the right side of the heart) may be absent or unable to open wide enough.
- Pulmonary valve (the valve between the heart and the lungs) may be absent or unable to open wide enough.
- Aortic valve (the valve between the heart and the blood vessel to the rest of the body) is unable to open wide enough.
Other heart defects may include abnormalities in valve development or in the location and connections between blood vessels. Some examples include:
- Coarctation or complete interruption of the aorta: In this condition, the aorta is narrowed or constricted, obstructing blood flow to the lower part of the body and increasing blood pressure above the constriction.
- Ebstein anomaly: In this condition the tricuspid valve is elongated and displaced downward towards the right ventricle. The abnormality causes the tricuspid valve to leak blood backwards into the right atrium.
- Hypoplastic left heart syndrome: A combination of several abnormalities of the heart and the great blood vessels.
- Tetralogy of Fallot: This condition is characterized by four defects, including an abnormal opening, or ventricular septal defect; a narrowing (stenosis) at or just beneath the pulmonary valve that partially blocks the flow of blood from the right side of the heart to the lungs; a right ventricle that is more muscular than normal and often enlarged; and an aorta that lies directly over the ventricular septal defect.
- Total anomalous pulmonary venous return: Total anomalous pulmonary venous return is a heart defect in which the 4 veins that take blood from the lungs to the heart do not attach normally to the left atrium (left upper chamber of the heart). Instead, they attach to another blood vessel or the wrong part of the heart. It is present at birth (congenital heart disease).
- Transposition of the great arteries: With this condition, the positions of the pulmonary artery and the aorta are switched or reversed.
- Truncus arteriosus: In this condition, the aorta and pulmonary artery start as a single blood vessel, which eventually divides and becomes two separate arteries. Truncus arteriosus occurs when the single great vessel fails to separate completely, leaving a connection between the aorta and pulmonary artery.
Certain medical conditions in the mother can increase the risk of certain cyanotic heart disease in the infant. Some examples include:
- Chemical exposure
- Genetic and chromosomal syndromes, such as Down syndrome, trisomy 13, Turner syndrome, Marfan syndrome, and Noonan syndrome
- Infections (such as rubella) during pregnancy
- Poorly controlled blood sugar level in women who have diabetes during pregnancy
- Medicines prescribed by your health care provider or bought on your own and used during pregnancy
- Street drugs used during pregnancy.
Cyanotic heart disease pathophysiology
In fetal circulation, gas exchange occurs in the placenta. From the placenta, oxygenated blood travels through the umbilical vein into the Inferior vena cava through the ductus venosus, bypassing the liver circulation. In the heart, most of the oxygenated blood is shunted from the right atrium to the left atrium through the foramen ovale. From the left atrium, blood is pumped to the left ventricle and into the aorta to reach systemic circulation. A small portion of blood is pumped from the right atrium to right ventricle and the pulmonary artery. From the pulmonary artery, blood is shunted to the aorta through the ductus arteriosus, bypassing the lungs. Deoxygenated blood return to the placenta by the umbilical arteries 3.
Cyanotic heart disease is silent in fetal life because fetus receives oxygenated blood from the placenta and either the foramen ovale or ductus arteriosus can increase systemic blood flow. After ductus arteriosus and foramen ovale closure soon after birth, most cyanotic heart disease become symptomatic. Cyanosis may be caused by persistence of fetal circulation, right-to-left shunting across the foramen ovale and ductus ductus arteriosus in the presence of pulmonary outflow tract obstruction or persistent pulmonary hypertension of the newborn.
Cyanotic heart disease prevention
Women who are pregnant should get good prenatal care.
- Avoid using alcohol and drugs during pregnancy.
- Tell your doctor that you are pregnant before taking any prescribed medicines.
- Get a blood test early in the pregnancy to see if you are immune to rubella. If you are not immune, you must avoid any exposure to rubella and should get immunized right after delivery.
- Pregnant women with diabetes should try to get good control over their blood sugar level.
Some inherited factors may play a role in congenital heart disease. Many family members may be affected. If you are planning to get pregnant, talk to your doctor about screening for genetic diseases.
Cyanotic heart disease symptoms
Some heart defects cause major problems right after birth.
The main symptom is cyanosis is a bluish color of the lips, fingers, and toes that is caused by the low oxygen content in the blood. It may occur while the child is resting or only when the child is active.
Some children have breathing problems (dyspnea). They may get into a squatting position after physical activity to relieve breathlessness.
Others have spells, in which their bodies are suddenly starved of oxygen. During these spells, symptoms may include:
- Anxiety
- Breathing too quickly (hyperventilation)
- Sudden increase in bluish color to the skin
Infants may get tired or sweat while feeding and may not gain as much weight as they should.
Fainting (syncope) and chest pain may occur.
Other symptoms depend on the type of cyanotic heart disease, and may include:
- Feeding problems or reduced appetite, leading to poor growth
- Decrease amount of formula per feed
- History of longer time per breastfeed
- Sweating (diaphoresis) and crying with feedings
- Poor weight gain
- Grayish skin
- Puffy eyes or face
- Tiredness all the time.
- Irritability or decreased level of activity
- Fast and/or irregular breathing
- Bluish or purple discoloration of the skin or mucous membranes
- Older children may present with exercise intolerance, including dyspnea, diaphoresis cyanosis or palpitations during exercise.
Physical findings associated with cyanotic heart disease include:
- Cyanosis
- Tachypnea
- Increased work of breathing
- Pulmonary edema
- Tachycardia
- Heart murmur
- Hepatomegaly (Liver edge located more than 2.5 cm below the right costal margin)
- Weak femoral pulses
- Signs of poor perfusion or shock
- Lethargy
Cyanotic heart disease possible complications
Complications of cyanotic heart disease include:
- Abnormal heart rhythms and sudden death
- Long-term (chronic) high blood pressure in the blood vessels of the lung
- Heart failure
- Infection in the heart
- Stroke
- Death
Cyanotic heart disease diagnosis
Physical examination confirms cyanosis. Older children may have clubbed fingers.
Your child’s doctor will listen to the heart and lungs with a stethoscope. Abnormal heart sounds, a heart murmur, and lung crackles may be heard.
Tests will vary depending on the cause, but may include:
- Chest x-ray
- Checking oxygen level in the blood using an arterial blood gas test or by checking it through the skin with a pulse oximeter
- Complete blood count (CBC)
- ECG (electrocardiogram)
- Looking at the heart structure and blood vessels using echocardiogram or MRI of the heart
- Passing a thin flexible tube (catheter) into the right or left side of the heart, usually from the groin (cardiac catheterization)
- Transcutaneous oxygen monitor (pulse oximeter)
- Echo-Doppler
Summary of cyanotic heart disease evaluation findings
Right Heart Obstructive Lesions:
- Pulmonary atresia
- Tricuspid atresia
- Tetralogy of Fallot
- Critical pulmonary stenosis
Right heart obstructive lesions lead to decrease pulmonary flow. Patent ductus arteriosus supplies pulmonary blood flow by shunting blood from the aorta to the pulmonary artery. There is a right-to-left intracardiac shunt. Patent foramen ovale shunts deoxygenated blood from the right atrium to the left atrium, and when ventricular septal defect is present, blood is shunted from the right ventricle to the left ventricle.
Screening findings
Positive cyanotic heart disease screening with oxygen saturation less than 90% without a difference in oxygenation between upper and lower extremities. Hyperoxia test is positive in these conditions. Chest x-ray shows decreased or normal pulmonary blood flow. ECG is an important tool to differentiate among these lesions. Left axis (0 to 90 degrees) is characteristic of pulmonary atresia; left superior axis (0 to -90 degrees) for tricuspid atresia, and right axis (90 to 180 degrees) for critical pulmonary stenosis and Tetralogy of Fallot.
Left Heart Obstructive Lesions:
- Hypoplastic left heart syndrome
- Interrupted aortic arch or coarctation of the aorta
- Critical aortic stenosis.
Left heart obstructive lesions lead to decreased systemic flow. Patent ductus arteriosus supplies systemic blood flow by shunting blood from the pulmonary artery to the aorta. There is a Left-to-right intracardiac shunt with secondary pulmonary over-circulation. Patent foramen ovale shunts oxygenated blood from the left atrium to the right atrium, and when ventricular septal defect is present, blood is shunted from the left ventricle to the right ventricle.
Screening findings
Positive cyanotic heart disease screening with oxygen saturation less than 95%; there is a greater than 3% difference between upper and lower oxygen saturation. Negative hyperoxia test. Positive BP gradient between upper and lower extremities is seen in this lesions, except for hypoplastic left heart syndrome. Chest x-ray shows increase pulmonary blood flow. ECG shows normal axis for a newborn (90 to 180 degrees), except for critical aortic stenosis which has left axis for a newborn (0 to 90 degrees).
Mixing Lesions
- Transposition of the great arteries
- Total anomalous pulmonary venous return
- Truncus arteriosus
Cyanosis presents from mixing pulmonary and systemic blood flow. These conditions are considered Ductal-independent lesions. PDA is not required, but they can present with or without PFO.
Screening findings
Positive cyanotic heart disease screening with oxygen saturation less than 95%. There is no difference between upper and lower oxygen saturation, except for d-transposition of great arteries with pulmonary hypertension or coarctation of the aorta, where O2 saturation is higher in the foot than in the right arm. Negative Hyperoxia Test. Chest x-ray shows normal to increased pulmonary blood flow. ECG shows normal axis for a newborn (90 to 180 degrees).
Fetal echocardiogram
A fetal echocardiogram should be performed in all fetuses with a suspected cardiac abnormality noted on obstetric ultrasound. Prenatal ultrasound can identify structural heart disease. However, the sensitivity of congestive heart disease detection is highly variable, depends on the operator expertise, gestational age fetal position, and type of cardiac defect 4.
Pulse oximetry screening
The pulse oximetry screening for cyanotic heart disease in newborns was added to the Recommended Uniform Screening Panel in the United States in 2011, and it was endorsed by the American Academy of Pediatrics in 2012. Screening is performed in the well-infant nursery when the baby is at least 24 hours of age, or as late as possible if the baby is to be discharged from the hospital before 24 hours of life. Earlier screening can lead to false-positive results.
Cyanotic heart disease screening will only identify cardiac lesions with the right to left shunt and cyanosis. Screening is recommended in the right hand and either foot. Positive screen result includes one of the following:
- Any Oxygen Saturation less than 90%
- Oxygen Saturation less than 95% in both extremities, on 3 measures, each separated by 1 hour
- More than 3% absolute difference in oxygen saturation between the right hand and foot on 3 measures, each separated by 1 hour
Differential cyanosis, lower oxygen saturation in the lower extremities, can be seen in persistent pulmonary hypertension of the newborn with interrupted aortic arch, and coarctation of the aorta. Reverse cyanosis, lower oxygen saturation in the right hand, is a manifestation of transposition of great arteries with concurrent coarctation of the aorta or interrupted aortic arch. Positive pulse oximetry screen will require prompt evaluation, including 4-limb blood pressure measurement, chest radiography, ECG, and echocardiography.
The seven primary cyanotic heart disease screening targets are:
- Hypoplastic left heart syndrome
- Pulmonary atresia
- Tetralogy of Fallot
- Total anomalous pulmonary venous return
- Transposition of great arteries
- Tricuspid atresia
- Truncus arteriosus.
Secondary screening targets are coarctation of the aorta, interrupted aortic arch, critical aortic stenosis, double outlet right ventricle, Ebstein anomaly and single ventricle complex. Cyanotic heart disease screening would miss about 15% of all cyanotic heart disease cases; coarctation of the aorta, interrupted aortic arch, total anomalous pulmonary venous return and Tetralogy of Fallot cases are the most common conditions missed. A failed newborn screen may also indicate other disease processes, such as pulmonary hypertension, primary pulmonary parenchymal disease, or hemoglobinopathies.
Hyperoxia test
Hyperoxia test is the initial method to distinguish cyanotic heart disease from pulmonary disease. The test consists in measuring an arterial blood gas at room air and 100% inspired oxygen after 10 minutes. Neonates with congenital heart disease are usually not able to increase PaO2 above 100 mm Hg during 100% oxygen administration. In patients with pulmonary disease, PaO2 generally increased greater than or equal to 100 mm Hg with 100% oxygen as ventilation-perfusion discrepancies are overcome. A positive result indicates the cardiac origin and further cardiac workup is indicated to rule out cyanotic heart disease.
Electrocardiogram (ECG)
ECG identifies rhythm abnormalities, auricular or ventricular hypertrophy, dextrocardias, or abnormal axis deviation.
Chest X-Ray
Chest x-ray indicates whether pulmonary blood flow is increased, normal, or decreased. Can identify specific unique findings of cyanotic heart disease – “egg-shaped” heart seen in transposition of great arteries, “snowman” in total anomalous pulmonary venous return, “boot-shaped” heart in tetralogy of Fallot, extreme cardiomegaly in Ebstein’s anomaly. May also be helpful in the differentiation of pulmonary and cardiac disease.
Two-Dimensional Echocardiography
The definitive noninvasive test to determine the presence of congenital heart disease. Echocardiography with Doppler can determine the degree and direction of the shunt and the gradient of outflow tract obstruction.
Additional imaging modalities
These include cardiac catheterization and angiography, magnetic resonance imaging (MRI) and CT scanning, to further visualize cardiac anatomy in preparation for cardiac surgery.
Cyanotic heart disease treatment
After fetal echocardiogram makes a diagnosis of cyanotic heart disease, specialized delivery room planning in a tertiary care center is required for prompt evaluation and management 5.
At birth, if a cyanotic heart disease is suspected and cardiac investigation or pediatric cardiologist is not easily available, appropriate stabilization, oxygen therapy, infusion of prostaglandin E1, and prompt transportation to a tertiary care center is necessary. Prostaglandin E1 is useful for ductal-dependent lesions as bridging therapy for further interventions or cardiac surgery. Approximately 25% of children born with a congenital heart disease will need heart surgery or other interventions to survive. Balloon atrial septostomy is performed acutely in cases of transposition of great arteries, allowing adequate blood mixing, and in cases of pulmonary hypertension, relieving right-sided pressures. The patient can undergo early corrective surgery or, in some cases, undergo palliation with a shunt prior to their corrective surgery. After the cardiac surgery is performed, it is essential that the primary source of each postoperative problem be identified and treated, for example, respiratory failure, cardiac rhythm disorders, heart failure, renal failure, seizures, thromboembolism and stroke, hemolysis, infections, postpericardiotomy syndrome, among others.
Routine immunizations should be given. Careful consideration for the timing of administration of live-virus vaccination is required in patients who are potential candidates for cardiopulmonary bypass, heart or heart-lung transplantation. Prophylaxis against the respiratory syncytial virus is recommended during respiratory syncytial virus season in infants with unrepaired congenital heart disease and significant hemodynamic abnormalities. Subacute bacterial endocarditis prophylaxis is recommended for patients undergoing dental procedures for patients with high risk of adverse outcomes according to 2007 Statement of the American Heart Association. Other management considerations include treatment of iron-deficiency anemia, close observation for excessive polycythemia, avoidance of dehydration to prevent the risk of stroke. Parents who have a child with congenital heart disease require counseling regarding the probability of a cardiac malformation occurring in subsequent children.
Cyanotic heart disease prognosis
The outlook depends on the specific disorder. One-year survival for infants with cyanotic heart diseases has improved over time; however, mortality remains high. About 75% of babies born with a cyanotic heart disease are expected to survive to 1 year of age. About 69% of babies born with cyanotic heart diseases are expected to survive to 18 years of age. Children with cyanotic heart disease are at an increased risk for developmental delay and disability, heart rhythm disorders, heart failure, sudden cardiac arrest or stroke.
- Ossa Galvis MM, Mendez MD. Cyanotic Heart Disease. [Updated 2019 Dec 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK500001[↩][↩]
- Desai K, Rabinowitz EJ, Epstein S. Physiologic diagnosis of congenital heart disease in cyanotic neonates. Curr. Opin. Pediatr. 2019 Apr;31(2):274-283.[↩]
- Chikkabyrappa S, Mahadevaiah G, Buddhe S, Alsaied T, Tretter J. Common Arterial Trunk: Physiology, Imaging, and Management. Semin Cardiothorac Vasc Anesth. 2019 Jun;23(2):225-236.[↩]
- Van De Bruaene A, Meier L, Droogne W, De Meester P, Troost E, Gewillig M, Budts W. Management of acute heart failure in adult patients with congenital heart disease. Heart Fail Rev. 2018 Jan;23(1):1-14.[↩]
- Bedair R, Iriart X. EDUCATIONAL SERIES IN CONGENITAL HEART DISEASE: Tetralogy of Fallot: diagnosis to long-term follow-up. Echo Res Pract. 2019 Mar 01;6(1):R9-R23.[↩]





{kind=link}