Cystatin C
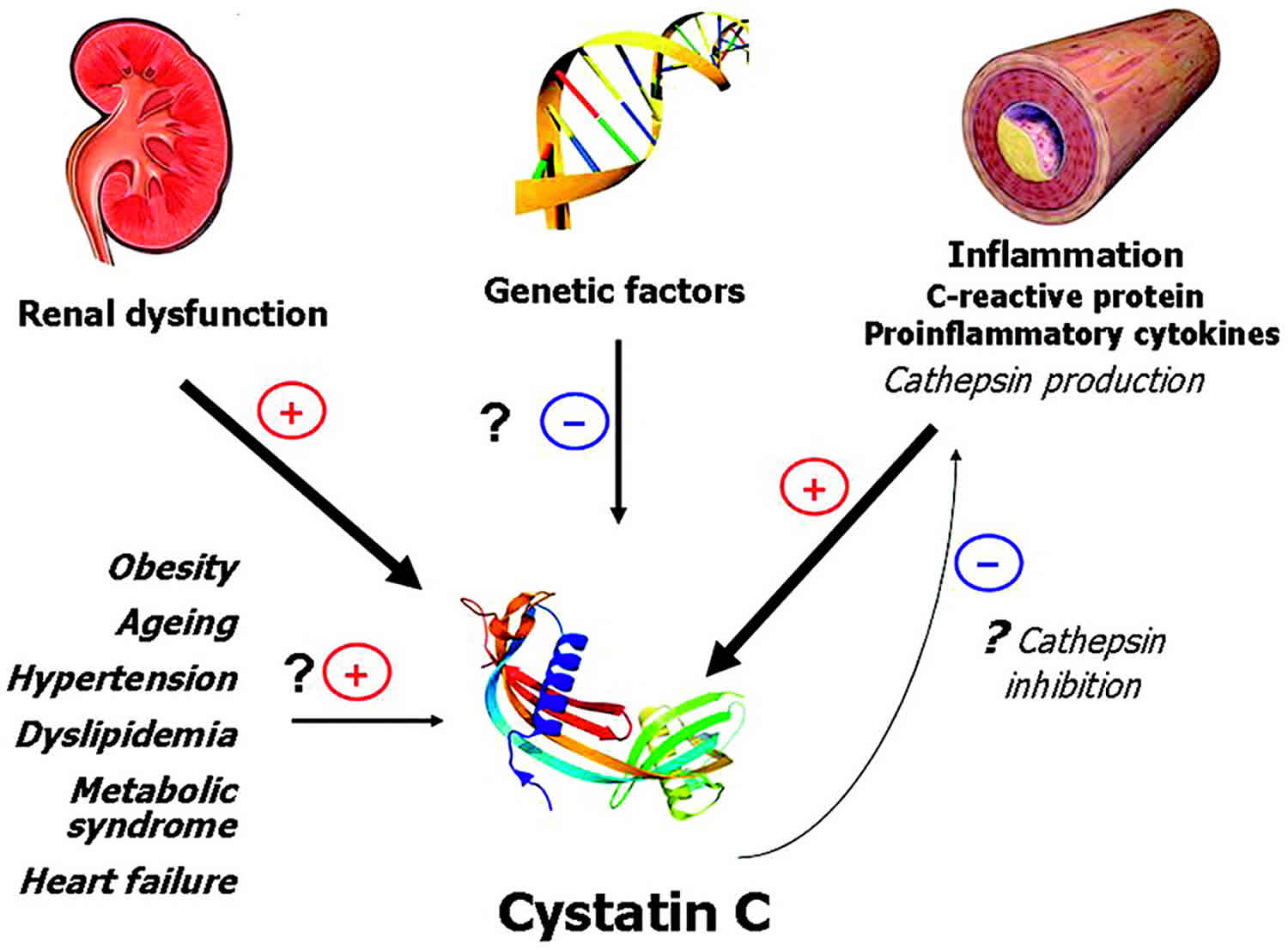
Cystatin C is a low-molecular-weight protein which functions as a protease inhibitor that is produced throughout the body by all cells that contain a nucleus and is found in a variety of body fluids, including the blood 1. Cystatin C is produced at a constant rate and freely filtered by the kidneys, and broken down at a constant rate. Cystatin C blood test is used help evaluate kidney function, because serum levels of cystatin C are inversely correlated with the glomerular filtration rate (GFR). In other words, high cystatin C values indicate low GFRs, while lower values indicate higher GFRs, similar to creatinine. The renal handling of cystatin C differs from creatinine. While both are freely filtered by glomeruli, once cystatin C is filtered, it is reabsorbed and metabolized by proximal renal tubules, unlike creatinine 1. Thus, under normal conditions, cystatin C does not enter the final excreted urine to any significant degree. Cystatin C is measured in serum and urine. The advantages of cystatin C over creatinine are that it is not affected by age, muscle bulk, or diet, and various reports have indicated that it is a more reliable marker of GFR (glomerular filtration rate) than creatinine particularly in early renal impairment 1. Cystatin C has also been incorporated into estimated glomerular filtration rate (eGFR) equations such as the combined creatinine-cystatin Kidney Disease Improving Global Outcomes Chronic Kidney Disease Epidemiology (KDIGO CKD-EPI) equation (see below). Cystatin C concentration may be affected by the presence of cancer, thyroid disease, and smoking.
Cystatin C is filtered out of the blood by the glomeruli, clusters of tiny blood vessels in the kidneys that allow water, dissolved substances, and wastes to pass through their walls while retaining blood cells and larger proteins. What passes through the walls of the glomeruli forms a filtrate fluid. From this fluid, the kidneys reabsorb cystatin C, glucose, and other substances. The remaining fluid and wastes are carried to the bladder and excreted as urine. The reabsorbed cystatin C is then broken down and is not returned to the blood.
The rate at which the fluid is filtered is called the glomerular filtration rate (GFR). A decline in kidney function leads to decreases in the GFR and to increases in cystatin C and other measures of kidney function, such as creatinine and urea in the blood. The increases in these levels occur because the kidneys are not able to properly filter the blood at a normal rate, causing their accumulation in the blood. On the other hand, improvement in kidney function is expected to lead to increases in GFR, which would cause cystatin C, creatinine, and urea to decline as a result of the kidneys being able to effectively clear them from the blood.
When the kidneys are functioning normally, concentrations of cystatin C in the blood are stable. However, as kidney function deteriorates, the concentrations begin to rise. This increase in cystatin C occurs as the GFR falls and is often detectable before there is a measurable decrease in kidney function (GFR).
Because cystatin C levels fluctuate with changes in GFR, there has been interest in the cystatin C test as one method of evaluating kidney function. Tests currently used include creatinine, a byproduct of muscle metabolism that is measured in the blood and urine, blood urea nitrogen (BUN), and eGFR (an estimate of the GFR usually calculated from the blood creatinine level). Unlike creatinine, cystatin C is not significantly affected by muscle mass (hence, sex or age), race, or diet, which has led to the idea that it could be a more reliable marker of kidney function and potentially used to generate a more precise estimate of GFR.
While there are growing data and literature supporting the use of cystatin C, there is still a degree of uncertainty about when and how it should be used. However, testing is becoming increasingly more available and steps are being taken toward standardizing the calibration of cystatin C results.
CKD-EPI Cystatin C Equation (2012) 2
- eGFR = 133 x min (standardized serum cystatin C/0.8, 1) -0.499 x max (standardized serum cystatin C/0.8, 1) -1.328 x 0.996Age x 0.932 [if female]
eGFR (estimated glomerular filtration rate) = mL/min/1.73 m²
Standardized serum cystatin C = mg/l
min = indicates the minimum of standardized serum cystatin C/0.8 or 1
max = indicates the maximum of standardized serum cystatin C/0.8 or 1
age = years
Clinical Use
- Can be used as a confirmatory test for the diagnosis of chronic kidney disease in patients with a decreased GFR as estimated from creatinine.
- Data suggests that 3.6% of U.S. adults would be classified as having chronic kidney disease (CKD) solely on the basis of a creatinine-based GFR estimate of 45 to 59 ml per minute per 1.73 m². A strategy of measuring cystatin C when the creatinine-based estimate is in this range and then reestimating GFR with the use of both these markers could correctly reclassify a substantial proportion of such patients as not having chronic kidney disease and not being at high risk.
- Can also be used to screen for chronic kidney disease (CKD) among persons who have a creatinine-based GFR estimate of 60 to 74 ml per minute per 1.73 m² without albuminuria (10.9% of U.S. adults) or to obtain a more accurate estimation of GFR in patients with muscle wasting or chronic illness.
CKD-EPI Creatinine-Cystatin Equation (2012) 3
- eGFR = 135 × min (serum creatinine/κ, 1) α × max (serum creatinine/κ, 1) -0.601 × min (serum creatinine/0.8, 1) -0.375 × max (serum creatinine/0.8, 1) -0.711 × 0.995Age × 0.969 [if female] × 1.08 [if black]
eGFR (estimated glomerular filtration rate) = mL/min/1.73 m2
SCr (serum creatinine) = mg/dL
Scys (standardized serum cystatin C) = mg/l
κ = 0.7 (females) or 0.9 (males)
α = -0.248 (females) or -0.207 (males)
min(SCr/κ or 1) = indicates the minimum of SCr/κ or 1
max(SCr/κ or 1) = indicates the maximum of SCr/κ or 1
min(Scys/0.8, 1) = indicates the minimum of Scys/0.8, 1
max(Scys/0.8, 1) = indicates the maximum of Scys/0.8, 1
age = years
Clinical Use
- Designed for use with standardized creatinine values that are calibrated to be isotope dilution mass spectrometry (IDMS) traceable and standardized cystatin C values.
May provide more accuate estimates in patients with differences in diet, extremes of muscle mass (such as body builders or patients with muscle wasting), or those outside the boundaries of where the Modification of Diet in Renal Disease (MDRD) study equation has been validated. - May also prove useful in estimating change in estimated glomerular filtration rate (eGFR) over time in people with changing muscle mass or diet.
- May have a role in identifying persons with chronic kidney disease (CKD) who have the highest risk for complications.
- Cystatin C is a basic protein produced by all nucleated cells. It is freely filtered by the glomerulus and reabsorbed and metabolized by tubular cells, with only small amounts excreted in the urine. It is reported to be generated at a relatively constant rate, irrespective of muscle mass.
- The original formula was reexpressed in 2011 for standardized cystatin C.
Cystatin C test
A cystatin C test may be used as an alternative to creatinine and creatinine clearance to screen for and monitor kidney dysfunction in those with known or suspected kidney disease. Cystatin C test is most useful in special cases where creatinine measurement could be misleading. For example, in those who have liver cirrhosis, are very obese, are malnourished, practice a vegetarian diet, have amputated limbs, or have reduced muscle mass (elderly and children), creatinine measurements may not be reliable. Since creatinine depends on muscle mass, assessment of kidney function may therefore not be accurate in these individuals with abnormally high or low body mass. Cystatin C is not affected by body mass or diet, and hence is a more reliable marker of kidney function than creatinine.
Measuring cystatin C may also be useful in the early detection of kidney disease when other test results (eGFR, creatinine or urine albumin) may still be normal or borderline and an affected person may have few, if any, symptoms. In this case, the healthcare practitioner may want to confirm if chronic kidney disease is present by measuring cystatin c.
Researchers are exploring other uses of cystatin C, such as using it alone or in combination with blood creatinine for estimating the glomerular filtration rate (GFR). A recent study found that an equation for eGFR that includes both creatinine and cystatin C was more accurate than one that uses either of these alone and could be used to confirm chronic kidney disease (CKD) in people with an eGFR near 60, the threshold for chronic kidney disease. In addition to kidney dysfunction, it has been associated with an increased risk of mortality, cardiovascular disease and heart failure in older adults. These equations are currently being validated in different patient populations prior to it being fully implemented into clinical practice.
Lastly, there is some research suggesting that cystatin C returns to a normal level more quickly than creatinine and could be used to assess kidney function and severity of illness when GFR is rapidly changing in critically ill hospitalized patients.
When is cystatin c blood test ordered?
Cystatin C is gaining acceptance as studies confirm and define its usefulness, especially as an early, sensitive marker for chronic kidney disease (CKD). It may be ordered when a person has a known or suspected disease that affects or potentially affects kidney function and reduces the rate at which the kidneys filter impurities from the blood, the glomerular filtration rate (GFR).
It may be ordered when a healthcare practitioner is not satisfied with the results of other tests, such as a creatinine or creatinine clearance, or wants to check for early kidney dysfunction, particularly in the elderly or in sick babies, and/or wants to monitor known impairment over time.
Research is ongoing to learn more about cystatin C as an indicator of risk of end stage renal disease, heart failure, and death. Studies have also found that, in diverse populations, cystatin C may improve the estimate of GFR when combined in an equation with blood creatinine.
Can cystatin C be measured in my urine?
No. Unlike creatinine, cystatin C is reabsorbed from the glomerular filtrate and then metabolized in the kidneys. Under normal conditions, cystatin C is not found at detectable levels in the urine.
How can my actual GFR be determined?
The best method for directly determining the glomerular filtration rate (GFR) is a procedure called an “inulin clearance.” It involves introducing a fluid containing the marker molecule inulin (NOT insulin) into your veins (IV – intravenous infusion) and then collecting timed urine samples over a period of hours. The urine volumes are noted and the inulin in each sample is measured to allow determination of the GFR. This test and other methods of determining GFR, such as those that use radioactive markers, are not routinely ordered and are primarily performed in research settings.
How is an eGFR calculated?
The most commonly used equation for calculating the eGFR, and the one currently recommended by the National Kidney Foundation and Kidney Disease Improving Global Outcomes guidelines for general use, is called the CKD-EPI equation. It requires a person’s serum creatinine (and/or serum cystatin c), age, and assigned values based upon sex and race. Researchers are also evaluating the usefulness of a variety of other equations to estimate GFR that combine tests such as a creatinine, BUN, and/or cystatin C.
Interpreting a cystatin C test result
A high level of cystatin C in the blood corresponds to a decreased glomerular filtration rate (GFR) and hence to kidney dysfunction.
Since cystatin C is produced throughout the body at a constant rate and removed and broken down by the kidneys, it should remain at a steady level in the blood if the kidneys are working efficiently and the GFR is normal.
Recent studies suggest that increased levels of cystatin C may also indicate an increased risk of heart disease, heart failure, and mortality.
Although cystatin C is less variable and less affected by age, body mass, and diet than creatinine in some individuals, it is not a perfect test and can be affected by a number of drugs and other medical conditions.
Some studies have reported increased cystatin C levels associated with higher levels of C-reactive protein (CRP) or body mass index (BMI), hyperthyroidism, steroid use, malignant diseases, HIV/AIDS, rheumatic diseases, and certain metabolic conditions such as hyperhomocysteinemia (increased homocysteine). In addition, other studies suggest that cystatin C can be cleared by non-kidney pathways, such as in the gut, and that its levels tend to fluctuate among patients with kidney transplants.
- Gounden V, Jialal I. Renal Function Tests. [Updated 2019 Apr 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507821[↩][↩][↩]
- CKD-EPI Cystatin C Equation (2012). https://www.kidney.org/content/ckd-epi-cystatin-c-equation-2012[↩]
- CKD-EPI Creatinine-Cystatin Equation (2012). https://www.kidney.org/content/ckd-epi-creatinine-cystatin-equation-2012[↩]





{kind=link}