Danon disease
Danon disease is a rare X-linked dominant genetic disorder that is characterized by weakening of the heart muscle (cardiomyopathy); weakening of the skeletal muscles used for movement (myopathy) and intellectual disability 1. Danon disease is caused by genetic mutations in the lysosome-associated membrane 2 (LAMP2) gene, with most mutations leading to an absence of LAMP2 protein 2. There are currently over 160 different mutations that researchers have identified in the literature through observational studies, case reports, and databases 3. The most detrimental mutations are considered to be those leading to a complete absence of the LAMP2 protein. Partial LAMP2 mutation may be an association with less severe clinical symptoms.
Danon disease is a rare condition, but the exact prevalence is unknown 4. While the prevalence of Danon disease is unknown, it is thought to affect any ethnic group 5. A pediatric study on hypertrophic cardiomyopathy identified 4% of its patients as having Danon disease 6. Another observational study diagnosed Danon disease in 17% of patients with both thickened left ventricular walls and electrocardiogram evidence of pre-excitation 7.
Males with Danon disease usually develop the condition at a younger age than females and are more severely affected. Signs and symptoms such as muscle weakness and possibly delayed motor skills begin in childhood or adolescence in most affected males and in early adulthood in most affected females. Affected males, on average, live to age 19, while affected females live to an average age of 34.
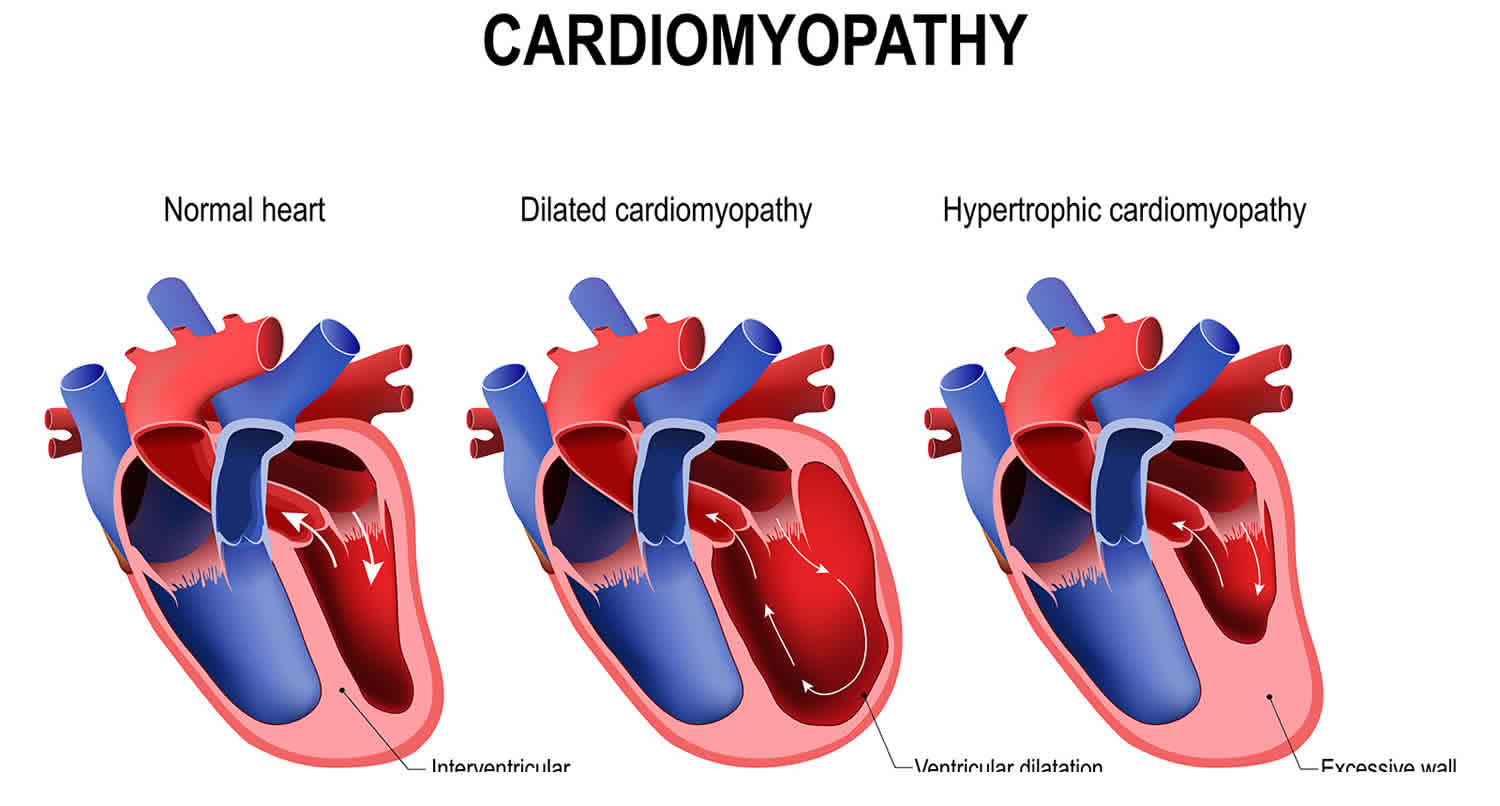
Cardiomyopathy is the most common symptom of Danon disease and occurs in all males with the condition. Most affected men (90%) have hypertrophic cardiomyopathy, which is a thickening of the heart muscle that may make it harder for the heart to pump blood. Other affected males have dilated cardiomyopathy, which is a condition that weakens and enlarges the heart, preventing it from pumping blood efficiently. Some affected men with hypertrophic cardiomyopathy later develop dilated cardiomyopathy. Either type of cardiomyopathy can lead to heart failure and premature death. Most women with Danon disease also develop cardiomyopathy; of the women who have this feature, about half have hypertrophic cardiomyopathy, and the other half have dilated cardiomyopathy. Fatigue, dyspnea, and lower extremity edema may be a manifestation of progressive cardiomyopathy. Sudden cardiac death from cardiac disease occurs more frequently in males in their second and third decades of life 8. Arrhythmias are very common, noted in 53% of patients 8. Sudden cardiac death likely from ventricular arrhythmias is a significant cause of death in Danon disease patients. In one high-profile series, sudden cardiac death occurred in 2 of 9 patients (29%) 9.
Affected individuals can have other heart-related signs and symptoms, including a sensation of fluttering or pounding in the chest (palpitations), an abnormal heartbeat (arrhythmia), or chest pain. Many affected individuals have abnormalities of the electrical signals that control the heartbeat (conduction abnormalities). People with Danon disease are often affected by a specific conduction abnormality known as cardiac preexcitation. The type of cardiac preexcitation most often seen in people with Danon disease is called the Wolff-Parkinson-White syndrome pattern.
Skeletal myopathy occurs in most men with Danon disease and about half of affected women. The weakness typically occurs in the larger muscle groups of the upper arms, shoulders, neck, back, and upper thighs 10. Danon disease may manifest as difficulty with arm raise, getting up from a chair, or walking up a flight of stairs. Many males with Danon disease have elevated levels of an enzyme called creatine kinase in their blood, which often indicates muscle disease.
Most men with Danon disease, but only a small percentage of affected women, have intellectual disability. If present, the disability is usually mild.
There can be other signs and symptoms of the condition in addition to the three characteristic features. Several affected individuals have had gastrointestinal disease, breathing problems, or visual abnormalities.
Other clinical manifestations may be harder to diagnose. Liver and lung involvement may be a component of skeletal myopathy leading to liver enzyme increase and respiratory muscle weakness. Visual problems due to the loss of retinal pigment may also affect Danon disease patients 11.
The role of cognitive issues and psychiatric disease in Danon disease is still unclear. Intellectual disability is typically mild in males as they are still usually able to read, hold jobs, and live independently 10. A recent observational study exploring cognitive deficits and psychiatric comorbidities in Danon disease revealed that 9 of 12 participants had a normal IQ score, while only one patient had an intellectual disability 12. However, this study also showed that 69% of participants met criteria for a psychiatric disorder, primarily mood and anxiety disorder, which underscores the need for psychiatric assessment.
Of note, females typically manifest with symptoms during middle adulthood with symptoms of heart disease. Skeletal myopathy and intellectual disability may not be present in females with Danon disease 10.
The most extensive observational study comprised 82 total Danon disease patients from 36 different families 8. This study revealed that 100% of males are affected with intellectual disability, 88% of males are affected by hypertrophic cardiomyopathy, and 80% of males present with skeletal myopathy. Affected males were unlikely to live until age 25 without cardiac transplantation. In affected females, the study reported cognitive deficits in 47%, skeletal myopathy in 50%, and cardiomyopathy in 61% (with an approximately equal prevalence of dilated and hypertrophic cardiomyopathy).
Danon disease cause
Danon disease is caused by mutations in the LAMP2 gene. The LAMP2 gene provides instructions for making a protein called lysosomal associated membrane protein-2 (LAMP-2), which, as its name suggests, is found in the membrane of cellular structures called lysosomes. Lysosomes are compartments in the cell that digest and recycle materials. The role the LAMP-2 protein plays in the lysosome is unclear. Some researchers think the LAMP-2 protein may help transport cellular materials or digestive enzymes into the lysosome. The transport of cellular materials into lysosomes requires the formation of cellular structures called autophagic vacuoles (or autophagosomes), which then attach (fuse) to lysosomes. The LAMP-2 protein may be involved in the fusion between autophagic vacuoles and lysosomes.
Mutations in the LAMP2 gene lead to the production of very little or no LAMP-2 protein, which may impair the process of transporting cellular material into the lysosome. Some studies have shown that in cells without the LAMP-2 protein, fusion between autophagic vacuoles and lysosomes occurs more slowly, which may lead to the accumulation of autophagic vacuoles. People with Danon disease have an abnormally large number of autophagic vacuoles in their muscle cells. It is possible that this accumulation leads to breakdown of the muscle cells, causing the muscle weakness seen in Danon disease.
Danon disease inheritance pattern
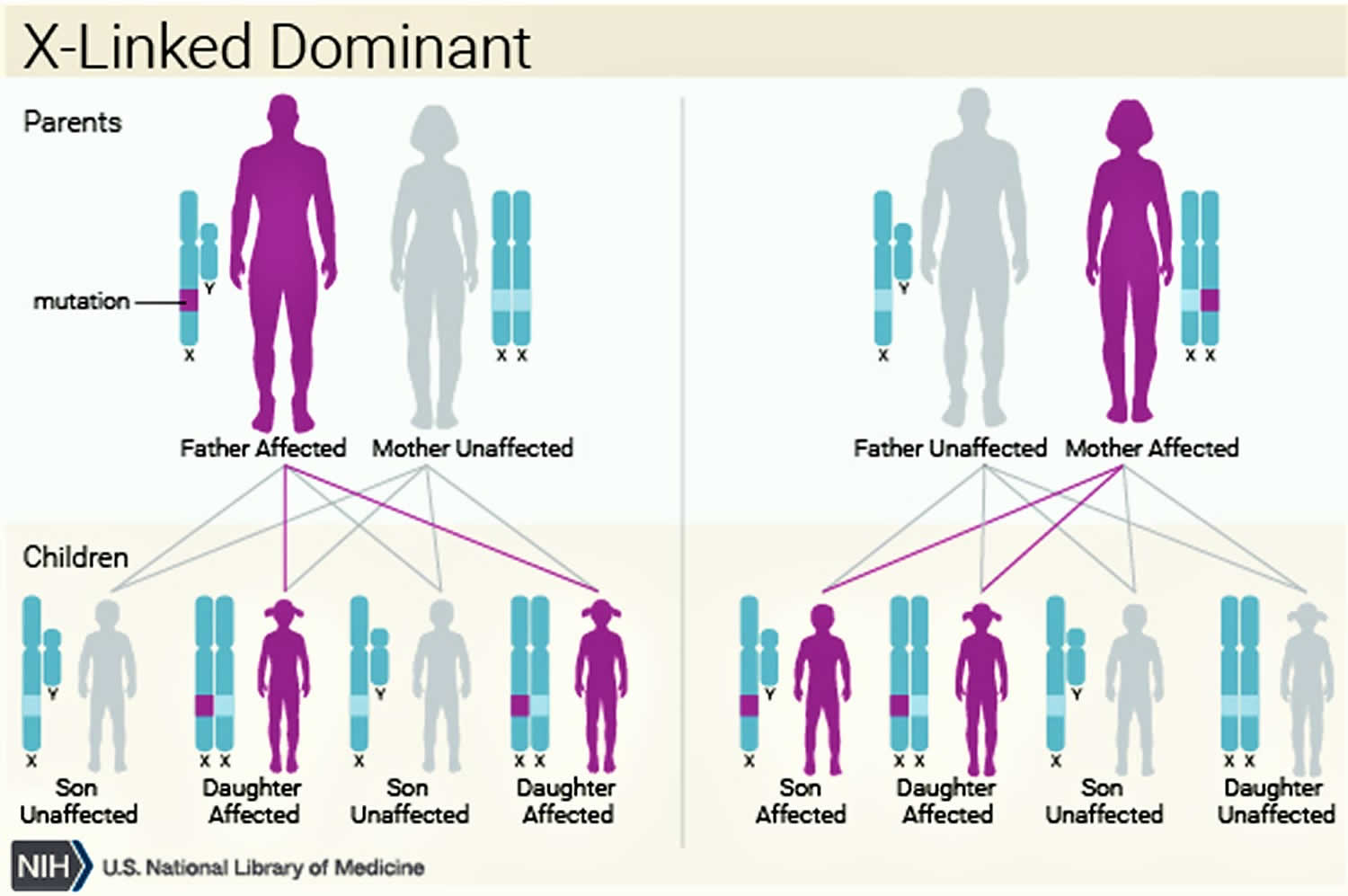
Danon disease is inherited in an X-linked dominant pattern. The gene associated with this condition is located on the X chromosome, which is one of the two sex chromosomes. In females (who have two X chromosomes), a mutation in one of the two copies of the gene in each cell is sufficient to cause the disorder. In males (who have only one X chromosome), a mutation in the only copy of the gene in each cell causes the disorder. In most cases, males experience more severe symptoms of the disorder than females. A characteristic of X-linked inheritance is that fathers cannot pass X-linked traits to their sons. A male cannot pass an X-linked gene to his sons because males always pass their Y chromosome instead of their X chromosome to male offspring. Female carriers of an X-linked disorder have a 25% chance with each pregnancy to have a carrier daughter like themselves, a 25% chance to have a non-carrier daughter, a 25% chance to have a son affected with the disease, and a 25% chance to have an unaffected son.
X-linked dominant disorders, like Danon disease, are also caused by an abnormal gene on the X chromosome, but in these rare conditions, females with an abnormal gene are affected with the disease. Males with an abnormal gene are more severely affected than females, and many of these males do not survive. In the case of Danon disease, males can survive to adulthood, however, their medical problems and the typical need for heart transplantation likely limits their ability to have children.
Figure 1. Danon disease X-linked dominant inheritance pattern
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://findageneticcounselor.nsgc.org) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://abgc.learningbuilder.com/Search/Public/MemberRole/Verification) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (https://www.acmg.net/ACMG/Directories.aspx) has a searchable database of medical genetics clinic services in the United States.
Danon disease symptoms
Symptoms of Danon disease vary from person to person and depend on gender. Boys usually show early signs of muscle problems (difficulty sitting or walking) and motor skills may be awkward or delayed. Intellectual disability is usually noticed by parents and/or teachers and can be quite mild. The development of heart disease can lead to further fatigue and shortness of breath. Visual complaints are also prevalent with serious color vision disturbances and near-complete loss of retinal pigment in some patients.
In general, young girls may have no symptoms and will report normal muscle strength and have normal intellect. As females age, symptoms of heart disease can begin to develop. Muscle symptoms are reported by some girls and women but overt findings of frank muscle weakness are usually absent. Visual complaints may also be reported in women and can be an early feature of the disease, although manifestations are less severe than in men.
Clinical researchers believe that the skeletal muscle involvement in Danon disease preferentially involves the muscles of the back, shoulder, upper legs and the neck muscles. These are the proximal muscles; that is, those closest to the center of the body. Symptoms of weakness in these muscles can include back pain and difficulty raising one’s arms over the head, getting out of a chair, or walking up steps. In a young boy, these problems may be suggested by problems meeting motor milestones (sitting, crawling, and walking, running). An experienced neurologist can recognize the extent of muscle disease by performing a physical examination. Increasingly it is apparent that for some patients the muscle disease progresses over time and some older males may require assistance devices (walkers, wheelchairs).
The diseased heart muscle (cardiomyopathy) can lead to a thickened, stiff heart (hypertrophic cardiomyopathy) or to an enlarged heart (dilated cardiomyopathy). Hypertrophic cardiomyopathy is more common in males (approximately 90% hypertrophic and 10% dilated), whereas females are more apt to show features of dilated cardiomyopathy (approximately 50% hypertrophic and 50% dilated). Sometimes the cardiomyopathy can be the first sign of disease in male children. In both instances, problems with heart function and symptoms of heart failure (shortness of breath, fatigue, fluid gain) can occur. Death from the heart disease seems to more occur frequently in males, especially as they reach the second and third decades of life. Heart transplantation has been performed successfully and can greatly improve symptoms and extend life. Implantable cardiac defibrillators are used to manage heart arrhythmias and should probably be considered at the first symptoms of arrhythmia.
The extent of intellectual disability in affected males has been described in some epidemiological studies. The majority of boys will be mildly affected cognitively, usually allowing them to achieve the ability to read, hold jobs, form relationships, and live independently. Furthermore, providing education and learning support may help some boys improve their intellectual functioning. In women, intellect appears to be normal, although very little information in the literature addresses this question.
Less prevalent symptoms also include liver and lung involvement, although these have not been studied extensively and might be secondary to muscle involvement (e.g. serum liver enzyme elevation and respiratory muscle weakness). Some speculation also exists on psychiatric disease, with some case reports detailing depression, psychosis, suicidal ideation, and attention-deficit hyperactivity disorder in Danon disease patients. However, it is unclear if psychiatric episodes are related to Danon disease.
Males with Danon disease typically have abnormalities on certain laboratory tests. The creatine kinase (CPK) level in the blood is often elevated, and is a reflection of ongoing muscle damage. The creatine kinase is usually elevated in males, but can be normal in some females who have Danon disease. Abnormalities in liver enzyme tests are common in males; in some boys, these are mistakenly interpreted as a sign of primary liver disease rather than a reflection of skeletal muscle dysfunction; frank liver dysfunction has not been well-described in Danon disease. The electrocardiogram (ECG), which measures electrical impulses made by the heart, is often abnormal. This abnormality in conduction and electrical impulse is also known as an arrhythmia. Frequently, an arrhythmia called Wolff-Parkinson-White syndrome or a pre-excitation syndrome will be seen on the ECG. An examination of the retina by an experienced eye doctor (ophthalmologist) will often detect changes in the pigment of the retina. This can be a useful sign in women, as the retinal changes appear to precede other symptoms of the disease in some females.
Danon disease diagnosis
Because Danon disease is rare and unfamiliar to most physicians, diagnosis is difficult and takes substantial time. The diagnosis is suggested on the basis of a family history compatible with X-linked dominant inheritance and symptoms in affected relatives (cardiomyopathy, skeletal myopathy, intellectual disability, Wolff-Parkinson White, etc.). Skeletal muscle biopsy is done in some males in an effort to determine the cause of muscle weakness. If, in the course of examining the biopsy materials, glycogen buildup and/or empty spaces appear in the cells of the muscle tissue (vacuolization), Danon disease must be considered. This also holds true for the analysis of a heart biopsy. A muscle biopsy that yields evidence of glycogen build-up and empty spaces in the muscle cells are key signs and indications that a diagnosis of Danon disease is a high probability.
It is important to recognize that, in early stages of Danon disease, and probably also in women, the muscle biopsy can be non-specific. Thus, a normal or non-specific muscle biopsy does not exclude Danon disease. If other features of Danon disease are present, a non-diagnostic muscle biopsy should not discourage more definitive genetic testing. Patients who appear to have Pompe disease (based on muscle biopsy for instance) but have normal acid maltase activity, should be evaluated for Danon disease. Unexplained hypertrophic cardiomyopathy in males is probably due to Danon disease in some people.
Antibodies to the LAMP-2 protein are available and tissue staining (of a muscle biopsy) for the absence of LAMP-2 protein is another potential, but not widely available, diagnostic approach. LAMP-2 antibody testing is likely to be normal in women with Danon disease and if done should be interpreted with caution due to the possibility of a false-negative result.
Genetic testing of the LAMP2 gene is currently the gold standard for diagnosis and is available in specialized genetics laboratories. Most genetic mutations causing Danon disease predict reduced levels or even absence of the LAMP2 gene product, the LAMP-2 protein. Although the sensitivity of LAMP2 genetic testing is not known at this time, it is the best that is available. The noninvasive nature of DNA-based testing and the inclusion of LAMP2 gene testing in hypertrophic cardiomyopathy genetic diagnostic panels favor this method as the most common route to diagnosis.
Danon disease treatment
The treatment of Danon disease is directed toward the specific symptoms that are apparent in each individual. It requires a team that should include a primary care physician as well as several specialists, including a cardiologist, neurologist, ophthalmologist, geneticist, genetic counselor, rehabilitation physician, educational specialist, and physical therapist. Currently there is no specific therapy that is known to slow the underlying biological problems caused by LAMP-2 protein deficiency.
The severity of cardiomyopathy is the major prognostic factor. Imaging studies including echocardiography and cardiac magnetic resonance can assess heart function, extent of hypertrophy, and degree of cardiac fibrosis (formation of scar tissue on the heart). Medications for heart disease should be given when indicated by clinical signs and symptoms. The rapid progression of the cardiomyopathy in some males necessitates prompt consideration for heart transplantation. Early involvement of electrophysiology to study the electrical conduction system of the heart is warranted in patients with arrhythmias. A device called a Holter monitor can be used to continuously record the electrical impulses of the heart. For symptomatic arrhythmias, early implantation of a cardioverter-defibrillator may be appropriate. Cardiac ablation therapy, which is a technique utilized to destroy the abnormal focus in the heart generating the irregular rhythm, can also be performed. As the disease can progress rapidly in males, consideration for early defibrillator implantation and evaluation for cardiac transplantation are appropriate in males as cardiomyopathy progresses.
Assessment of muscle strength, especially the proximal muscles of the shoulder, neck, and legs, should be performed regularly. Physical therapy can be helpful in maintaining muscle strength and flexibility. Intellectual disability should be screened for in males and appropriate educational interventions applied as needed. Regular eye examinations, to track the development and progression of retinal disease, should be considered. Biological relatives who are at risk for Danon disease should be evaluated by a physician for early signs of disease. At a minimum, evaluation of such relatives should include a medical history, physical examination (attention to cardiac, neurological, and ocular exams), creatine kinase testing, ECG, and echocardiogram.
Genetic consultation and counseling is recommended for all patients and families so that inheritance and reproductive risks are clearly communicated.
Danon disease prognosis
Danon disease prognosis primarily depends on the severity of cardiomyopathy. The need for cardiac transplantation is typically inevitable for most males by the second and third decades 8. A study by Boucek and colleagues 8 reported that the average age of first symptom, heart transplant, and death are 12.1, 17.9, and 19.0 years in male patients, and 27.9, 33.7, and 34.6 years in female patients. A recent nationwide questionnaire study was carried out in Japan on 39 total Danon disease patients from 20 different families (39 male, 22 female) 13. In this study, 20 patients died from either cardiac failure or sudden cardiac death. Wolff-Parkinson-White syndrome was evident in a high proportion of included patients (54% of males and 22% of females). Interestingly, de novo mutations were present in half of the probands.
- D’souza, R.S., Levandowski, C.B., Slavov, D., Graw, S.L., Allen, L.A., Pretorius, V., Mestroni, L., & Taylor, M.R. (2014). Danon disease: clinical features, evaluation, and management. Circulation. Heart failure, 7 5, 843-9.[↩]
- Nishino I, Fu J, Tanji K, Yamada T, Shimojo S, Koori T, Mora M, Riggs JE, Oh SJ, Koga Y, Sue CM, Yamamoto A, Murakami N, Shanske S, Byrne E, Bonilla E, Nonaka I, DiMauro S, Hirano M. Primary LAMP-2 deficiency causes X-linked vacuolar cardiomyopathy and myopathy (Danon disease). Nature. 2000 Aug 24;406(6798):906-10.[↩]
- D’Souza RS, Law L. Danon Disease. [Updated 2019 Jul 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545211[↩]
- Danon disease. https://ghr.nlm.nih.gov/condition/danon-disease[↩]
- Nishino I. Autophagic vacuolar myopathy. Semin Pediatr Neurol. 2006 Jun;13(2):90-5.[↩]
- Charron P, Villard E, Sébillon P, Laforêt P, Maisonobe T, Duboscq-Bidot L, Romero N, Drouin-Garraud V, Frébourg T, Richard P, Eymard B, Komajda M. Danon’s disease as a cause of hypertrophic cardiomyopathy: a systematic survey. Heart. 2004 Aug;90(8):842-6.[↩]
- Arad M, Maron BJ, Gorham JM, Johnson WH, Saul JP, Perez-Atayde AR, Spirito P, Wright GB, Kanter RJ, Seidman CE, Seidman JG. Glycogen storage diseases presenting as hypertrophic cardiomyopathy. N. Engl. J. Med. 2005 Jan 27;352(4):362-72.[↩]
- Boucek D, Jirikowic J, Taylor M. Natural history of Danon disease. Genet. Med. 2011 Jun;13(6):563-8.[↩][↩][↩][↩][↩]
- Maron BJ, Roberts WC, Arad M, Haas TS, Spirito P, Wright GB, Almquist AK, Baffa JM, Saul JP, Ho CY, Seidman J, Seidman CE. Clinical outcome and phenotypic expression in LAMP2 cardiomyopathy. JAMA. 2009 Mar 25;301(12):1253-9.[↩]
- D’souza RS, Levandowski C, Slavov D, Graw SL, Allen LA, Adler E, Mestroni L, Taylor MR. Danon disease: clinical features, evaluation, and management. Circ Heart Fail. 2014 Sep;7(5):843-9.[↩][↩][↩]
- Schorderet DF, Cottet S, Lobrinus JA, Borruat FX, Balmer A, Munier FL. Retinopathy in Danon disease. Arch. Ophthalmol. 2007 Feb;125(2):231-6.[↩]
- Yardeni M, Weisman O, Mandel H, Weinberger R, Quarta G, Salazar-Mendiguchía J, Garcia-Pavia P, Lobato-Rodríguez MJ, Simon LF, Dov F, Arad M, Gothelf D. Psychiatric and cognitive characteristics of individuals with Danon disease (LAMP2 gene mutation). Am. J. Med. Genet. A. 2017 Sep;173(9):2461-2466.[↩]
- Sugie K, Komaki H, Eura N, Shiota T, Onoue K, Tsukaguchi H, Minami N, Ogawa M, Kiriyama T, Kataoka H, Saito Y, Nonaka I, Nishino I. A Nationwide Survey on Danon Disease in Japan. Int J Mol Sci. 2018 Nov 08;19(11).[↩]





{kind=link}