Denys Drash syndrome
Denys-Drash syndrome is a rare disorder consisting of the triad of congenital nephropathy, Wilms tumor and intersex disorders resulting from mutations in the Wilms tumor suppressor (WT1) gene 1. Nephropathy is a constant feature; in the incomplete forms of the Denys-Drash syndrome, the nephropathy is present with either Wilms tumor or intersex disorders, but the vast majority of patients with Denys-Drash syndrome are destined to develop Wilms tumor in any residual renal tissue. The risk of developing Wilms’ tumor in Denys Drash syndrome is up to 50% 2, with the mean age of 1.6 years which is earlier than isolated Wilms’ tumor 3.
Denys-Drash syndrome is characterized by kidney disease that begins within the first few months of life. Affected individuals have a condition called diffuse glomerulosclerosis, in which scar tissue forms throughout glomeruli, which are the tiny blood vessels in the kidneys that filter waste from blood. In people with Denys-Drash syndrome, this condition often leads to kidney failure in childhood. People with Denys-Drash syndrome have an estimated 90 percent chance of developing a rare form of kidney cancer known as Wilms tumor. Affected individuals may develop multiple tumors in one or both kidneys.
Although males with Denys-Drash syndrome have the typical male chromosome pattern (46,XY), they have gonadal dysgenesis, in which external genitalia do not look clearly male or clearly female (ambiguous genitalia) or the genitalia appear completely female. The testes of affected males are undescended, which means they are abnormally located in the pelvis, abdomen, or groin. As a result, males with Denys-Drash are typically unable to have biological children (infertile).
Affected females usually have normal genitalia and have only the kidney features of the condition. Because they do not have all the features of the condition, females are usually given the diagnosis of isolated nephrotic syndrome.
The prevalence of Denys-Drash syndrome is unknown; at least 150 affected individuals have been reported in the scientific literature 4.
Figure 1. Denys Drash syndrome
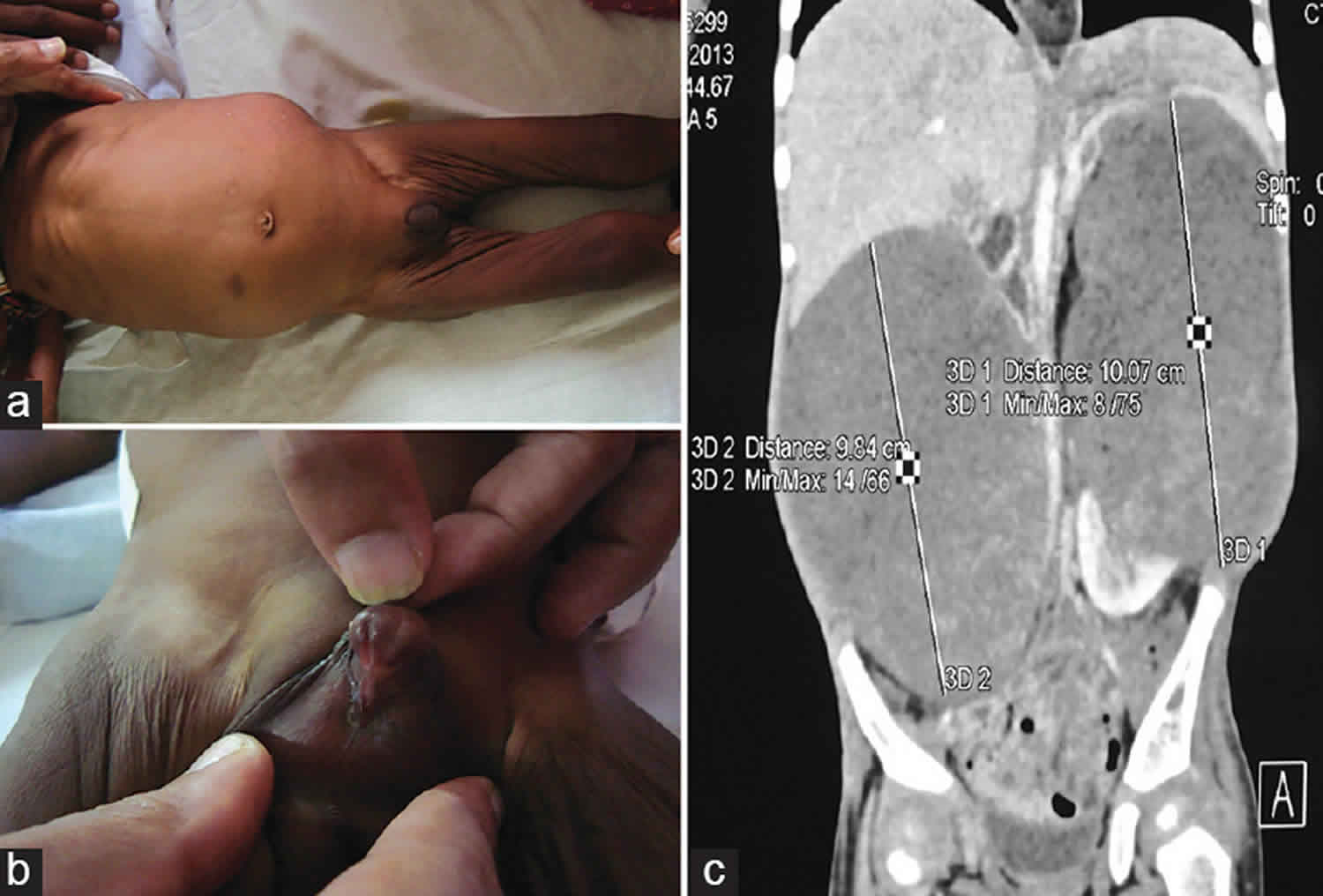
Footnote: An 8-month-old male child was brought to a hospiatl for swelling of the abdomen and failure to thrive associated with decreased activity since 1-month. (a-c) Bilateral renal lumps in an 8-month-old malnourished infant with penoscrotal type of hypospadias with empty scrotum. Image of computed tomography scan shows bilateral well defined, heterogeneously enhancing masses from both kidneys. The histopathological examination from both renal masses was showing triphasic pattern of classic Wilms’ tumor with predominant blastema component.
[Source 5 ]Denys Drash syndrome causes
Mutations in the Wilms tumor suppressor gene (WT1 gene) cause Denys-Drash syndrome. The WT1 gene (Wilms tumor suppressor gene) provides instructions for making a protein that regulates the activity of other genes by attaching (binding) to specific regions of DNA. On the basis of this action, the WT1 protein is called a transcription factor. The WT1 protein plays a role in the development of the kidneys and gonads (ovaries in females and testes in males) before birth.
WT1 gene mutations that cause Denys-Drash syndrome lead to the production of an abnormal protein that cannot bind to DNA. As a result, the activity of certain genes is unregulated, which impairs the development of the kidneys and reproductive organs. Abnormal development of these organs leads to diffuse glomerulosclerosis and gonadal dysgenesis, which are characteristic of Denys-Drash syndrome. Abnormal gene activity caused by the loss of normal WT1 protein increases the risk of developing Wilms tumor in affected individuals.
Denys-Drash syndrome has features similar to another condition called Frasier syndrome, which is also caused by mutations in the WT1 gene. Because these two conditions share a genetic cause and have overlapping features, some researchers have suggested that they are part of a spectrum and not two distinct conditions.
Denys Drash syndrome inheritance pattern
Denys-Drash syndrome is inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder. However, most cases of Denys-Drash syndrome result from new (de novo) mutations in the gene that occur during the formation of reproductive cells (eggs or sperm) or in early embryonic development. These cases occur in people with no history of the disorder in their family.
Often autosomal dominant conditions can be seen in multiple generations within the family. If one looks back through their family history they notice their mother, grandfather, aunt/uncle, etc., all had the same condition. In cases where the autosomal dominant condition does run in the family, the chance for an affected person to have a child with the same condition is 50% regardless of whether it is a boy or a girl. These possible outcomes occur randomly. The chance remains the same in every pregnancy and is the same for boys and girls.
- When one parent has the abnormal gene, they will pass on either their normal gene or their abnormal gene to their child. Each of their children therefore has a 50% (1 in 2) chance of inheriting the changed gene and being affected by the condition.
- There is also a 50% (1 in 2) chance that a child will inherit the normal copy of the gene. If this happens the child will not be affected by the disorder and cannot pass it on to any of his or her children.
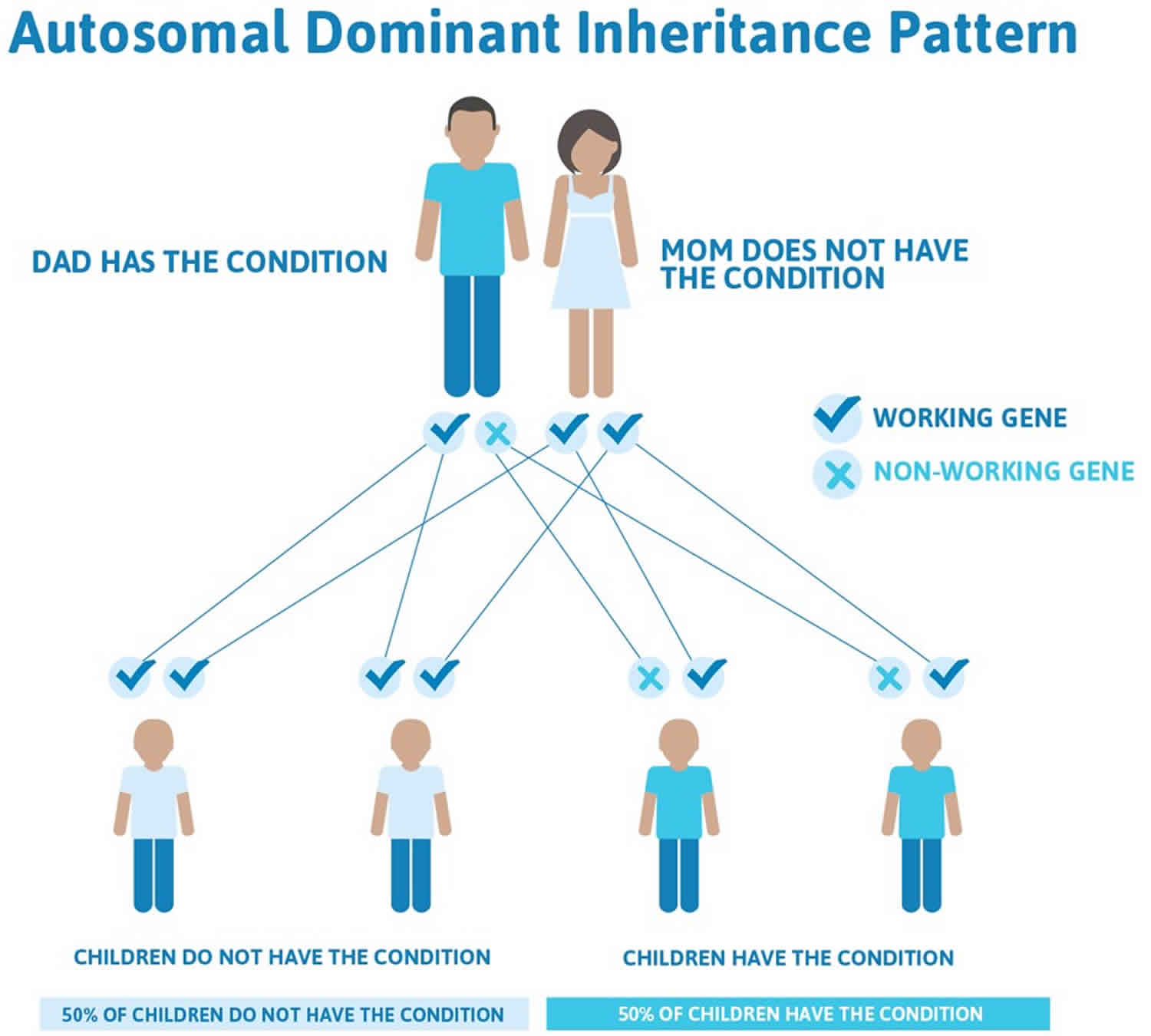
Figure 2 illustrates autosomal dominant inheritance. The example below shows what happens when dad has the condition, but the chances of having a child with the condition would be the same if mom had the condition.
Figure 2. Denys Drash syndrome autosomal dominant inheritance pattern
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
Denys Drash syndrome symptoms
The initial symptoms of Denys Drash syndrome may be similar to nephrotic syndrome and include edema, abdominal distention and recurrent infections, sometimes present at birth but more often developing between 1 and 2 years of age. Many affected children develop high blood pressure (hypertension). The kidney abnormality that results in abnormal kidney function is termed diffuse mesangial sclerosis and usually results in a progression to renal failure during the first three years of life.
Wilms tumor occurs in approximately 90% of affected individuals and is sometimes the first clinical sign of the disease. Signs of Wilms tumor can include abdominal swelling, blood in the urine, decreased urination, low-grade fever, loss of appetite, paleness, weight loss and lethargy.
Disorders of sexual development also occur in males with Denys Drash syndrome and are rare in females with this condition. These are conditions in which a boy has normal male chromosomes (46, XY), but the external genitals are incompletely formed, ambiguous, or clearly female. Testes may be normal, malformed, absent, or internal (undescended). Affected individuals of both genders are at risk for cancers of the testes or ovaries.
Denys Drash syndrome diagnosis
Denys Drash syndrome is diagnosed by physical signs and symptoms, laboratory tests, imaging studies, and kidney biopsy to document diffuse mesangial sclerosis. Molecular genetic testing for the WT1 gene is available to confirm the diagnosis.
Denys Drash syndrome treatment
The treatment of Denys Drash syndrome is supportive and requires consultation with a pediatric nephrologist, pediatric oncologist, pediatric surgeon, pediatric endocrinologist and geneticist.
- Pediatric nephrologist – For managing the nephropathy, end-stage renal disease (ESRD), hypertension, and medical aspects of transplantation
- Pediatric oncologist – For diagnosis and treatment of Wilms tumor and gonadoblastoma
- Pediatric surgeon – For managing Wilms tumor, access in renal replacement therapy and surgical aspects of renal transplantation, and evaluation and possible removal of abnormal gonads
- Pediatric endocrinologist – For evaluation and management of intersex disorders
- Geneticist – For chromosomal analysis, molecular diagnosis, and genetic counseling
Medical care involves management of fluids and electrolytes, treatment for hypertension and chemotherapy for Wilms tumor, if present. Prophylactic removal of kidneys (nephrectomy) is recommended when the diagnosis of Denys Drash syndrome is made prior to development of Wilms tumor. Renal replacement therapy, including dialysis and/or kidney transplantation, is recommended following end-stage renal failure or nephrectomy. Surgical removal of internal reproductive organs (gonadectomy) is recommended because of the high risk for gonadal malignancy.
A low-sodium diet is important to manage hypertension and edema. Patients with renal insufficiency require a low-potassium, low-phosphate diet.
Genetic counseling is recommended. Other treatment is symptomatic and supportive.
Surgical care
Surgical treatment of patients with Denys-Drash syndrome and Wilms tumor should follow the guidelines of the National Wilms Tumor Study-4 Protocols 6. Prophylactic total bilateral nephrectomy has been advocated because the risk of Wilms tumor is very high in any residual renal tissue.
For patients without Wilms tumor at the time of initial presentation with Denys-Drash syndrome, early prophylactic bilateral nephrectomy, followed by renal replacement therapy, is recommended to avoid the risk of Wilms tumor development and consequent delay of kidney transplantation. As the risk of gonadal malignancy is also high in patients with gonadal dysgenesis, performing a gonadectomy at the time of nephrectomy is best. Institute appropriate hormonal therapy in these patients at puberty.
Kidney transplantation is the treatment of choice after bilateral nephrectomy. For patients with Wilms tumor, a 2-year period free of chemotherapy and tumor is recommended prior to renal transplantation.
- Denys-Drash Syndrome. https://emedicine.medscape.com/article/943103-overview[↩]
- Eddy AA, Mauer SM. Pseudohermaphroditism, glomerulopathy, and Wilms tumor (Drash syndrome): Frequency in end-stage renal failure. J Pediatr 1985;106:584-7.[↩]
- Montgomery BT, Kelalis PP, Blute ML, Bergstralh EJ, Beckwith JB, Norkool P, et al. Extended follow-up of bilateral Wilms tumor: Results of the National Wilms Tumor Study. J Urol 1991;146:514-8.[↩]
- Denys-Drash syndrome. https://ghr.nlm.nih.gov/condition/denys-drash-syndrome[↩]
- Modi J, Modi P, Pal B, Kumar S. Bilateral Wilms’ tumors in an infant with Denys-Drash syndrome and rarely seen truncation mutation in the WT1 gene-exon 6. J Indian Assoc Pediatr Surg 2015;20:197-8[↩]
- Breslow NE, Collins AJ, Ritchey ML, et al. End stage renal disease in patients with Wilms tumor: results from the National Wilms Tumor Study Group and the United States Renal Data System. J Urol. 2005 Nov. 174(5):1972-5.[↩]





{kind=link}