What is a dermatome
A dermatome is an area of skin that is mainly supplied by a single spinal nerve. There are 8 cervical nerves (C1 being an exception with no dermatome), 12 thoracic nerves, 5 lumbar nerves and 5 sacral nerves. Each of these nerves relays sensation (including pain) from a particular region of skin to the brain. The skin over your entire body is supplied by somatic sensory neurons that carry nerve impulses from the skin into the spinal cord and brain.
Understanding the nerve distribution along the dermatomes is helpful in determining how certain diseases, such as shingles and some other neurological conditions, target one area of the body.
Several anatomic landmarks help easily identify or estimate different dermatomal levels 1:
- C6 – Thumb
- C7 – Middle finger
- C8 – Little finger
- T1 – Anteromedial forearm and arm
- T2 – Medial forearm and arm to the axilla
- T4 – Nipple
- T6 – Xyphoid process
- T10 – Umbilicus
- L3 – Medial knee
- L4 – Anterior knee and medial malleolus
- L5 – Dorsal surface of the foot and first, second, and third toes
- S1 – Lateral malleolus
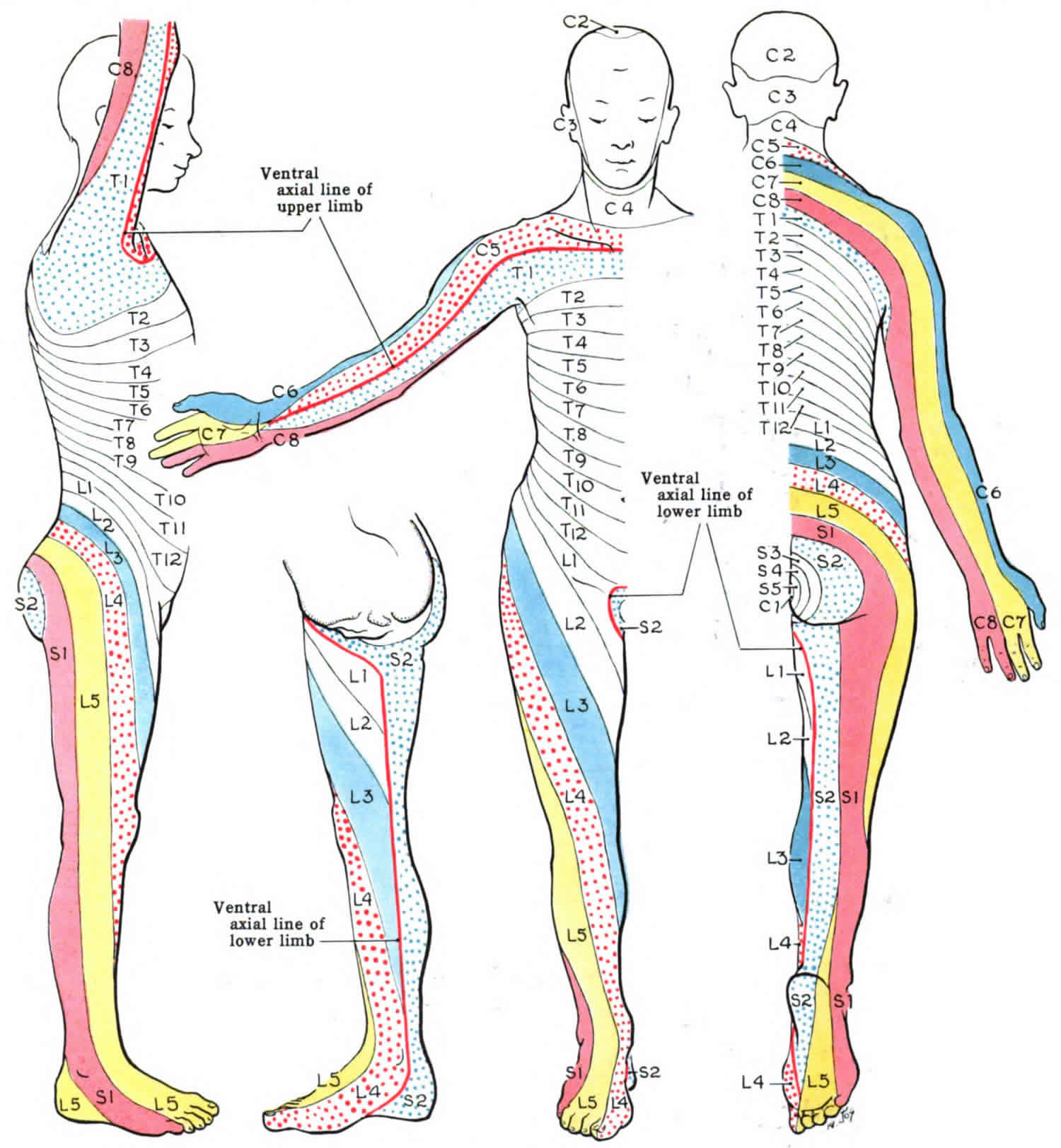
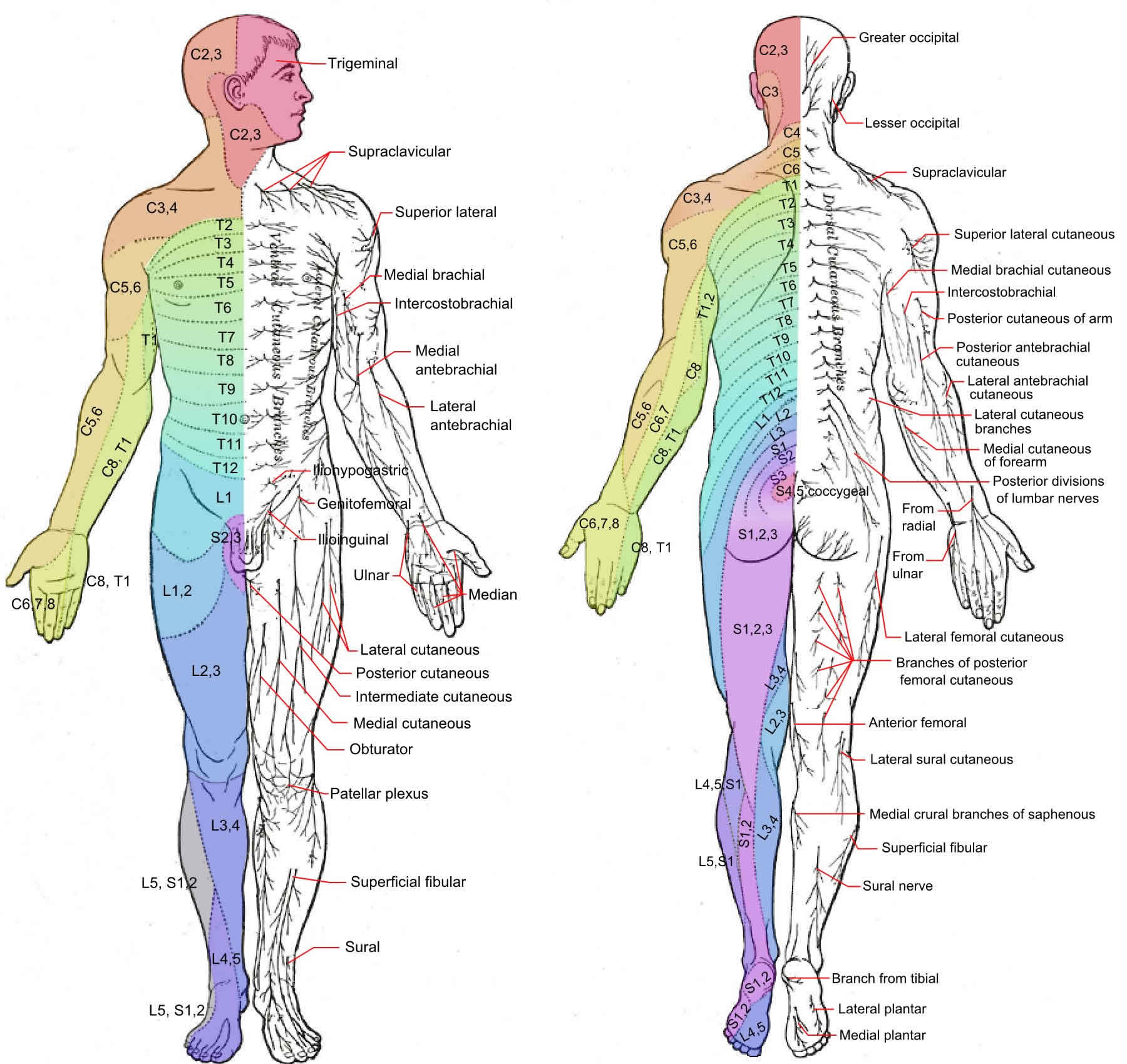
Each spinal nerve contains sensory neurons that serve a specific, predictable segment of the body called a dermatome (derma- = skin; -tome = thin segment) (Figure 1). One of the cranial nerves, the trigeminal (V) nerve, serves most of the skin of the face and scalp. The nerve supply in adjacent dermatomes overlaps somewhat. Knowing which spinal cord segments supply each dermatome makes it possible to locate damaged regions of the spinal cord. If the skin in a particular
region is stimulated but the sensation is not perceived, the nerves supplying that dermatome are probably damaged. In regions where the overlap is considerable, little loss of sensation may result if only one of the nerves supplying the dermatome is damaged.
Information about the innervation patterns of spinal nerves can also be used therapeutically. Cutting posterior roots or infusing local anesthetics can block pain either permanently or transiently. Because dermatomes overlap, deliberate production of a region of complete anesthesia may require that at least three adjacent spinal nerves be cut or blocked by an anesthetic drug.
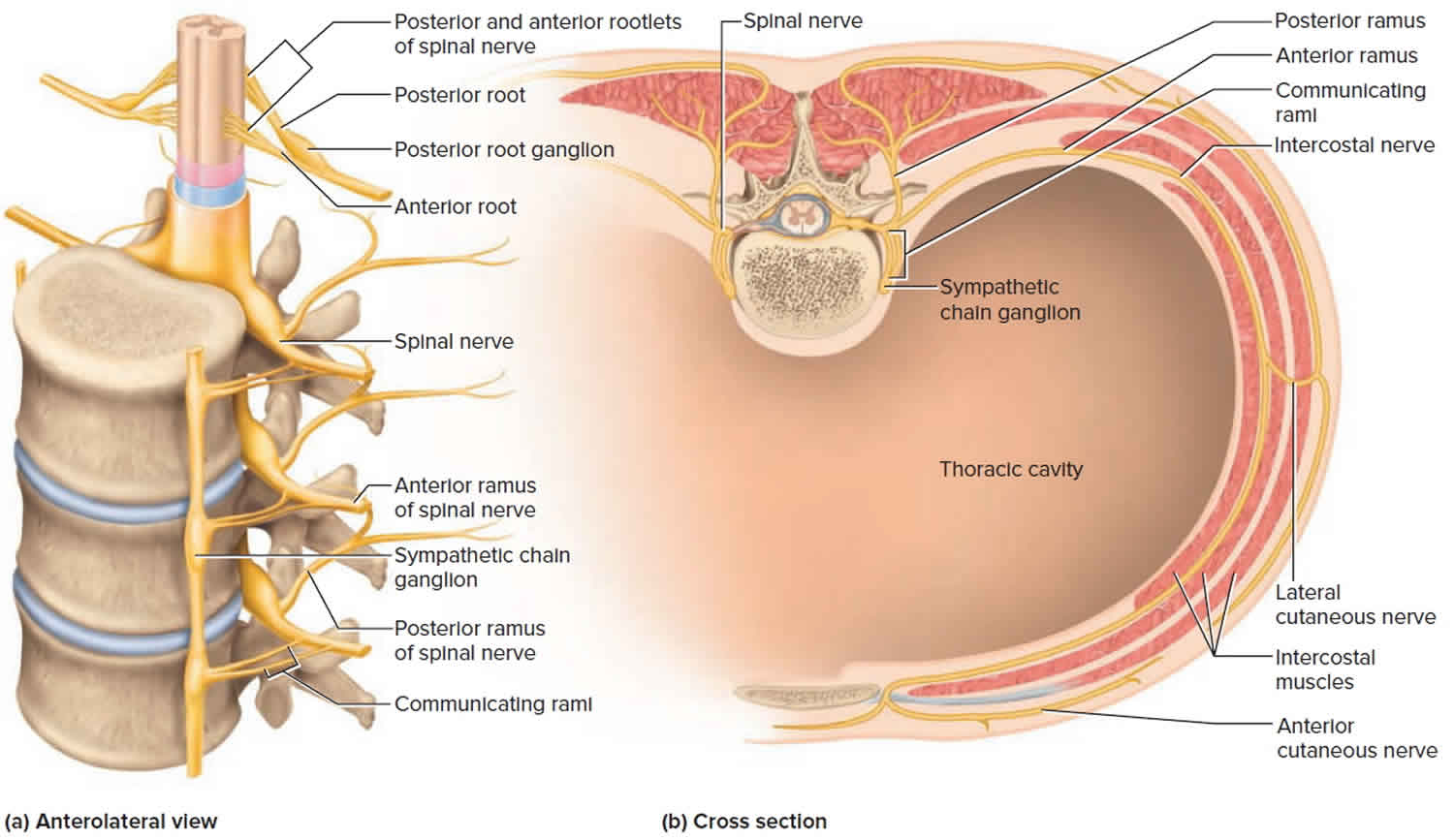
Spinal nerves form from the dorsal nerve roots and the ventral nerve roots which branch from the dorsal and ventral horn of the spinal cord, respectively. The spinal nerves exit through the intervertebral foramina or neuroforamina and travel along their respective dermatomal distributions from posterior to anterior, creating the specific, observable dermatomal patterns 2.In total, there are 31 distinct spinal segments and thus 31 distinct spinal nerves bilaterally. These 31 spinal nerves are composed of 8 pairs of cervical nerves, 12 pairs of thoracic nerves, five pairs of lumbar nerves, five pairs of sacral nerves, and one pair of coccygeal nerve 2.
The cervical nerves C1-C7 exit through the intervertebral foramina above their respective vertebrae. Cervical nerve C8 exits between the C7 vertebra and the T1 vertebra. The remaining spinal nerves all exit below their respective vertebrae 2.
The dermatomes on the trunk are layered horizontally, one on top of the other 1. This horizontal pattern contrasts with the pattern on the extremities, where it is typically more longitudinal. This pattern is fairly standard although some variations can exist from person to person because spinal nerves overlap in the areas of the body they supply.
Figure 1. Dermatome levels
Footnote: The letter-number combinations show the relationship between each area and its corresponding sensory nerve. The vertebrae are classified as C for cervical, T for thoracic, L for lumbar, and S for sacral. The trigeminal nerve is the fifth cranial nerve, represented by V.
Figure 2. Spinal nerve segments
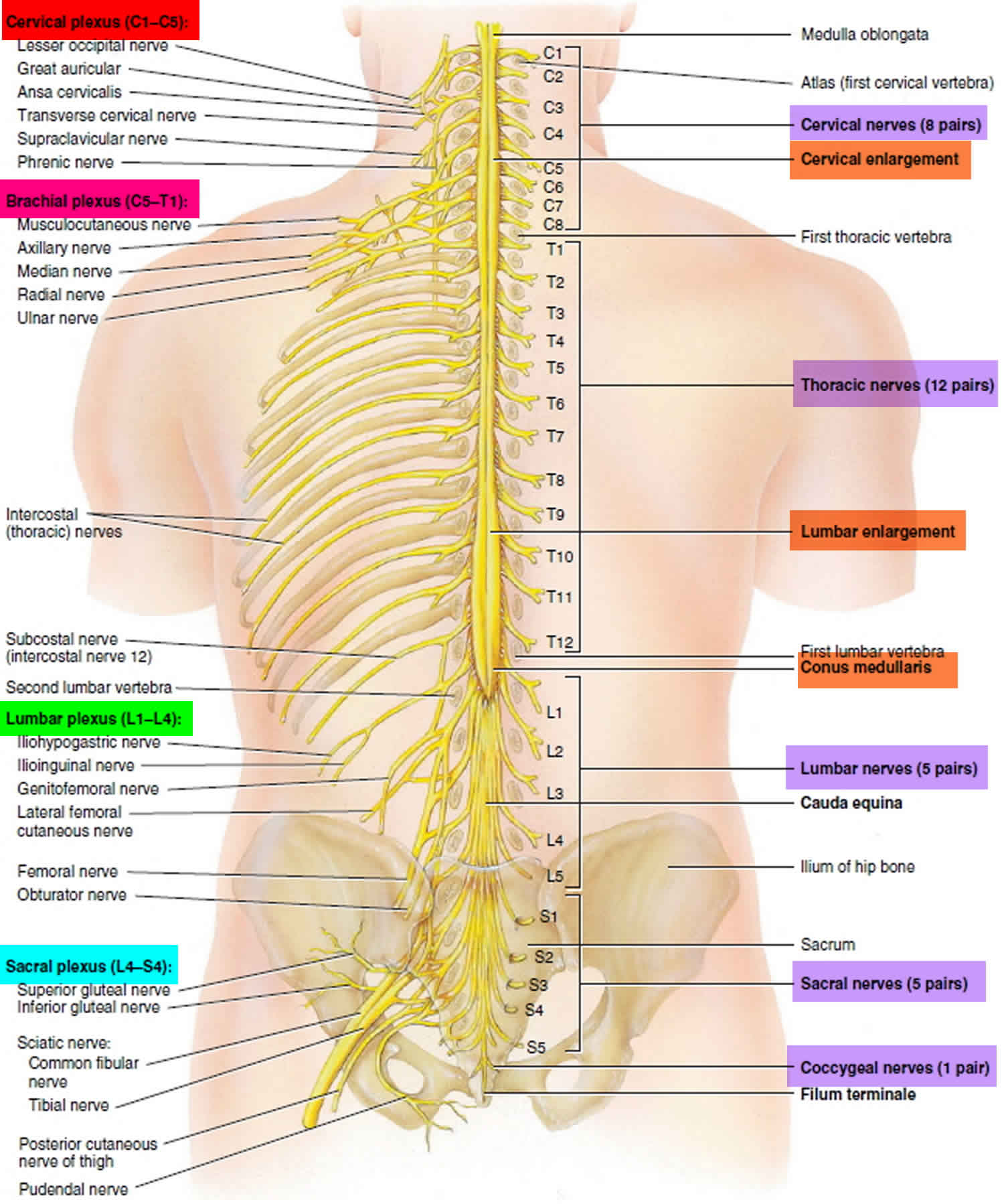
Figure 3. Spinal nerve anatomy
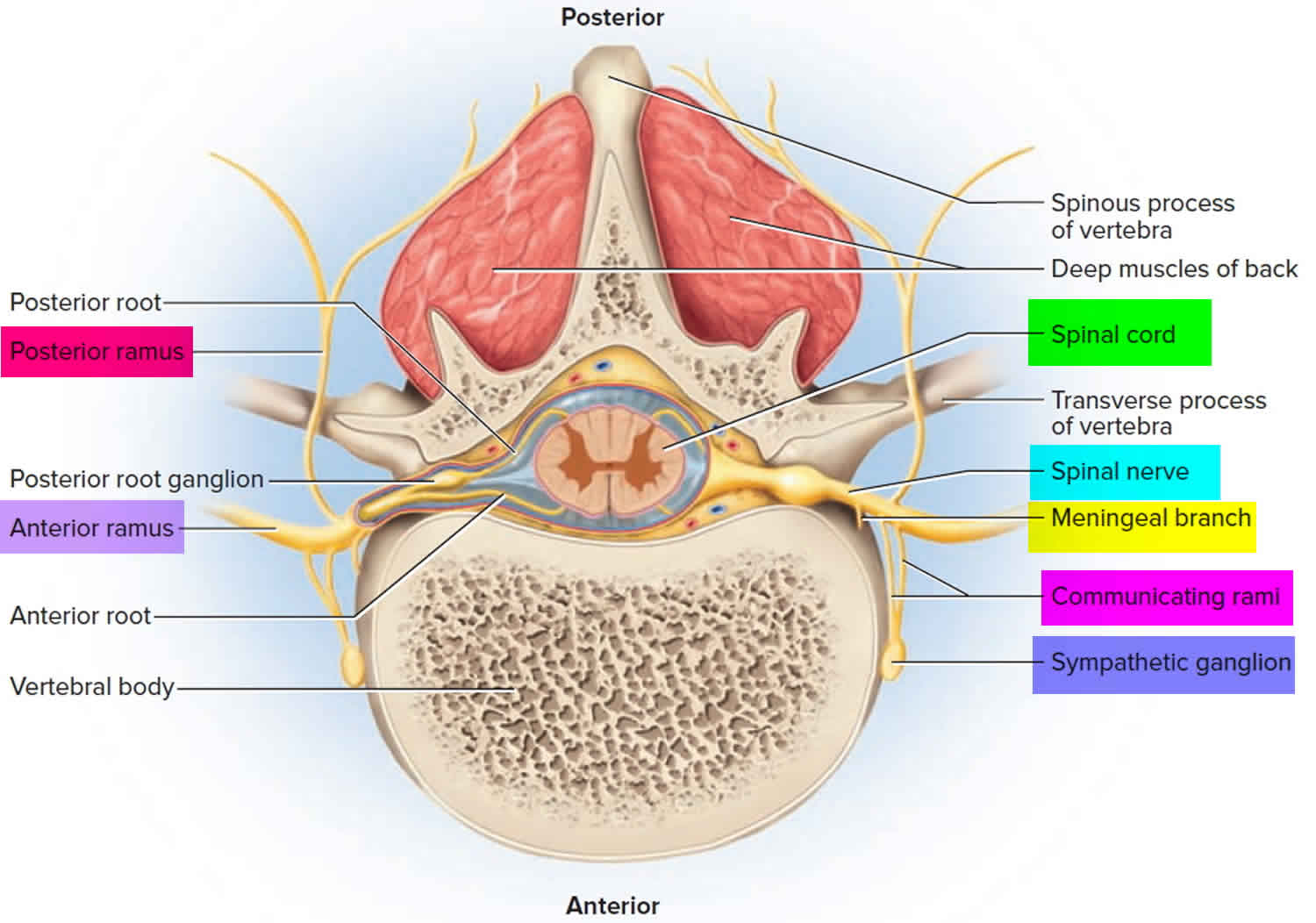
Figure 4. Spinal nerve rami
Dermatomes clinical significance
Neurological evaluation of dermatomes helps to assess radiculopathy or neurologic deficits as radicular patterns can suggest specific spinal nerve involvement. For example, sciatica, will often present along the dermatome of the involved spinal nerve 3. Sciatica-associated pain will commonly follow a path from the posterior hip down the back of the thigh to the knee involving the S1 or S2 dermatome. Neurological assessment of dermatomes helps to assess the level of spinal cord injury 4.
Herpes zoster infections, also known as chickenpox and shingles, are caused by varicella zoster virus or human herpesvirus 3 (HHV-3). In the primary varicella infection, the distribution is widespread and diffuse, progressing in a cephalocaudal manner with classic lesions often described as “dew drops on a rose petal.” With the resolution of the primary infection, the virus retreats into the dorsal root ganglia awaiting reactivation. Viral reactivation can frequently be due to a triggering event while in an immunocompromised state, but immunosuppression is not requisite for reactivation of the virus and presentation of the secondary disease 5.
Once reactivated, the viral symptoms typically present in 3 different phases. The pre-eruptive, or prodromal, phase exhibits symptoms associated with sensory phenomena presenting along the affected dermatome. These sensory symptoms may present as pain, burning, itching, or paresthesias. After the pre-eruptive phase follows the eruptive phase during which the affected dermatome erupts in a grouped vesicular rash (herpetiform) on an erythematous base. The vesicular lesions will most commonly present along a truncal dermatome, with facial onvolvement the second most prevalent. The lesions progress through a pattern of vesicles, pustules, crusting, and resolution 6.
Disseminated herpes zoster is significantly rare and almost exclusively associated with severely immunocompromised states (i.e., AIDS, malignancy, long-term immunosuppressive therapy use, etc.). Affected patients are also at risk of life-threatening conditions including encephalitis or pneumonitis.
Of particular concern for herpes zoster infections is the involvement of the cranial nerves, particularly the trigeminal nerves (cranial nerve 5). Herpes zoster ophthalmicus presents similarly to herpes zoster infections affecting the trunk, beginning with the prodromal phase of burning or itching on the skin, and can sometimes be clinically confused with trigeminal neuralgia while still in the pre-eruptive stage. The concern with herpes zoster ophthalmicus is that with the eruptive phase, lesions distribute along the face, and if involving the optic nerve, the oculomotor nerve, or the trigeminal nerve, blindness can result. Hutchinson’s sign, herpetic lesions along the lateral nose tip, indicates the involvement of the nasociliary branch of the first trigeminal nerve and is ominous of potential ocular involvement 2.
Upon resolution of the lesions, pain can remain and continue to affect patients along the affected dermatome as postherpetic neuralgia 6.
- Whitman PA, Adigun OO. Anatomy, Skin, Dermatomes. [Updated 2018 Dec 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535401[↩][↩]
- Ludwig PE, Varacallo M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Feb 4, 2019. Neuroanatomy, Central Nervous System[↩][↩][↩][↩]
- Violante FS, Mattioli S, Bonfiglioli R. Low-back pain. Handb Clin Neurol. 2015;131:397-410[↩]
- Davis D, Vasudevan A. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Oct 27, 2018. Sciatica.[↩]
- Nair PA, Patel BC. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Dec 2, 2018. Herpes Zoster [Shingles][↩]
- Kedar S, Jayagopal LN, Berger JR. Neurological and Ophthalmological Manifestations of Varicella Zoster Virus. J Neuroophthalmol. 2018 Sep 01[↩][↩]





{kind=link}