
What is thumb sucking
Thumb sucking is one of the most common habits of babies and young children. The thumb sucking habit starts early in life. About 90% of newborns show some form of hand sucking by 2 hours after birth. Thumb sucking is one of the earliest reflexes exhibited and is a very strong urge in young babies. Sucking behaviors are very common in babies and young children as they give a feeling of security and many parents introduce the use of pacifiers to babies to help them settle.
Although the incidence of thumb (finger) sucking habits varies considerably between different countries, these comforting habits are common in children in many populations. A Swedish study looked at 60 consecutive births and found the incidence of thumb (finger) sucking to be 82% during the first five months of life 1 and a USA‐based study reported the incidence as 73% for a group of 130 children between two and five years of age 2. The incidence of thumb (finger) sucking reduces with age. Available data has shown that around 48% of four‐year‐olds maintain a digit or pacifier sucking habit 3, 12.1% of children past the age of seven years 4, reducing to 1.9% of children by 12 years of age 5.
Thumb sucking is normal in infants and young children 6. Thumb sucking is a form of non-nutritive sucking occurring as early as the 29th week of gestation and is seen commonly in infants and peaks at 18 to 21 months of age 7. Thumb/finger sucking habits, or non-nutritive sucking are considered to be the most prevalent of oral habits, with a reported incidence ranging from 13% to almost 100% at some time during infancy 6. Thumb sucking should cause no permanent problems if it stops by age 5. It is also generally harmless for babies to use pacifiers (dummies or soothers). There are other positive effects of pacifiers in young children, which may also contribute to their widespread use. The use of pacifiers has been shown to reduce crying in children during painful experiences such as venepuncture, and has been advocated for use in pediatric emergency departments 8. Pacifier placement for babies going to sleep has also been identified as a factor in the reduction of sudden infant death syndrome (SIDS) 9, although the mechanism behind this is currently unknown. However, the incidence of SIDS (sudden infant death syndrome) is highest at two to four months and declines towards zero at one year of age and therefore is not a reason for encouraging continuation of pacifier use in children over the age of two and a half years, when primary teeth are all present in the mouth.
Most children stop thumb sucking on their own between the ages of 2 and 4 10. Thumb sucking persisting beyond 3 to 4 years of age is usually due to physical and emotional stimuli, such as boredom, hunger, stress, hyperactivity, pleasure, sadness, and various kinds of disabilities 10. Increase in the child’s level of stress or anxiety can also account for continuation of the thumb sucking habit 11.
Experts believe that pacifier may actually be better than thumb sucking for the following reasons:
- Pacifiers are softer and cause less damage to the teeth.
- The plastic rim on the pacifier eases some of the tension placed on the teeth.
- Pacifiers can be cleaned.
Talk with your child’s healthcare provider or dentist if you are concerned with your child’s thumb sucking.
There is no reason to be concerned until the adult front teeth start erupting or breaking through the surface around the age of six. At this point, some problems may occur, these adult teeth will grow into the wrong position causing them to stick out too far or not meet properly when biting 11. As a result these children often need dental treatment to fix the problems caused by their sucking habit. The intensity of the thumb sucking is a factor in determining if problems might develop. If your child is an aggressive thumb sucker and damage is being done to the baby (primary) teeth, see your child’s dentist. Other problems that may occur with thumb sucking are sore thumbs, infections, and calluses on the thumb.
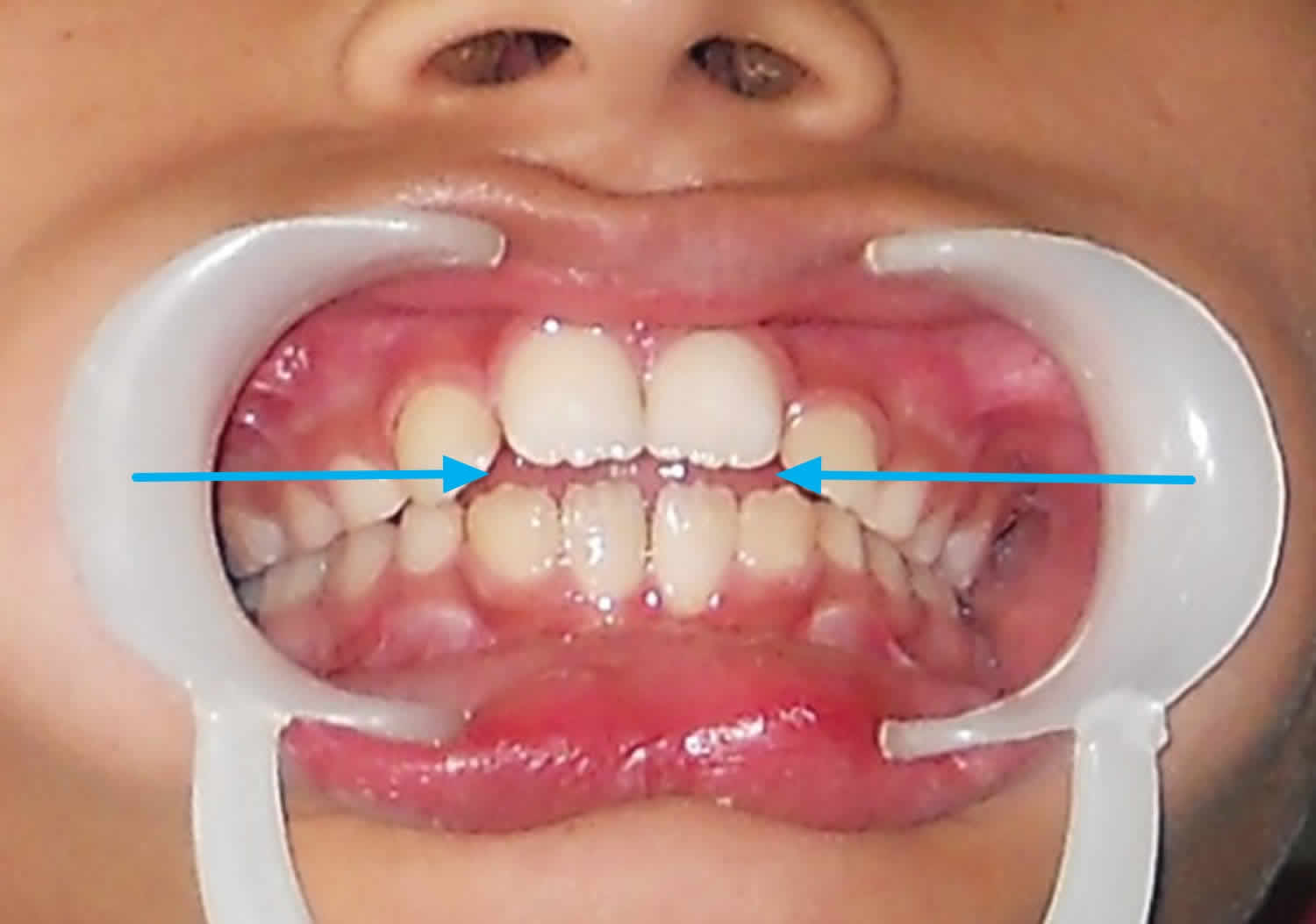
Reported maxillary changes associated with a prolonged sucking habit are proclination of the maxillary incisors, increased maxillary arch length, anterior placement of the maxillary apical base, increased sella-nasion-point A angle, and decreased palatal arch width 12, 13. Effects on the mandible include proclination of the mandibular incisors, increased intermolar distance and decreased sella-nasion-point B angle 12. Other dental alterations are increased overjet, decreased overbite and posterior crossbite 14. The response to the changes in the axial inclination of the incisors is anterior rotation of the occlusal plane. Underlying mechanisms of the mal-occlusion are direct pressure from the digit and reduced intraoral pressure produced by sucking 12.
Figure 1. Thumb sucking teeth (note the mild open bite between the front teeth)
How to stop a child from sucking thumb
Several methods have been described for the treatment of finger-sucking habits in the literature; these methods can be classified as (a) preventive therapy and (b) appliance therapy. Preventive methods include the application of adhesive tape or bitter solution and or wearing a sock, mitten, gloves, thumb guard, long-sleeve gown. Appliance therapy includes the use of fixed or removable habit breakers designed to make the sucking habit difficult or unpleasant 15. Explanations appropriate to the age of the child and positive reinforcement are other treatment options for digit suckers and are also necessary for the success of clinical management 16.
A Cochcrane review 17 found low quality evidence that orthodontic appliances (palatal arch and palatal crib) and psychological interventions (including positive and negative reinforcement) are effective at improving sucking cessation in children. There is very low quality evidence that palatal crib is more effective than palatal arch. There is insufficient evidence to determine the effect of other interventions evaluated for the cessation of digit sucking in children. Clinical experiences have shown that a bitter solution usually has a limited effect 15. Although it is not possible to draw definitive conclusions from the data, in the case of a digit sucking habit, given that the use of bitter solution requires no clinical input, is a non‐invasive, low risk procedure, is cheap and can be carried out by parents in the home setting, it is likely to continue as first line of treatment despite little evidence to support it.
Figure 2. Orthodontic deterrent appliance for thumb (finger) sucking in young children

Some of the methods discussed above have certain disadvantages. Adhesive tapes may cause infection, sweating and may also reduce the blood circulation 18, while the stuff worn on the hand can easily be removed involuntarily during sleep. Use of altered child’s pajamas to prevent the movement of hand to mouth usually increases the child’s frustration and wakefulness 19; also, the pajamas method can be used only if the habit is performed during sleep. Fixed orthodontic habit breaking appliance can cause decalcification of enamel surfaces making them more susceptible to caries and gingival inflammation may also occur; additionally removable appliances need patient cooperation. Intraoral habit breaking appliances can also cause deviation in speech and pronunciation 15. Fixed intraoral appliance may create difficulties while eating and mentally disabled children may try to remove their appliance and may frequently break it. On the other hand, removable appliances require patient compliance, making it impossible for children with mental retardation 20.
The ‘three-alarm’ system introduced by Norton and Gellin 21 by applying an appliance on the patient’s elbow is often effective in stopping the thumb sucking habit in the mature child and has some advantages over orthodontic habit breakers as it does not create difficulties during speech and chewing. Above all, general anesthesia is not required to make the impression of the elbow.
Figure 3. Modified elbow guard for thumb sucking treatment

Figure 4. Modified elbow guard for thumb sucking treatment (acrylic elbow guard with switch button on the inner surface of the acrylic elbow guard)

Figure 5. Modified elbow guard for thumb sucking treatment (acrylic elbow guard with musical chip and speaker on the outer surface of acrylic elbow guard)
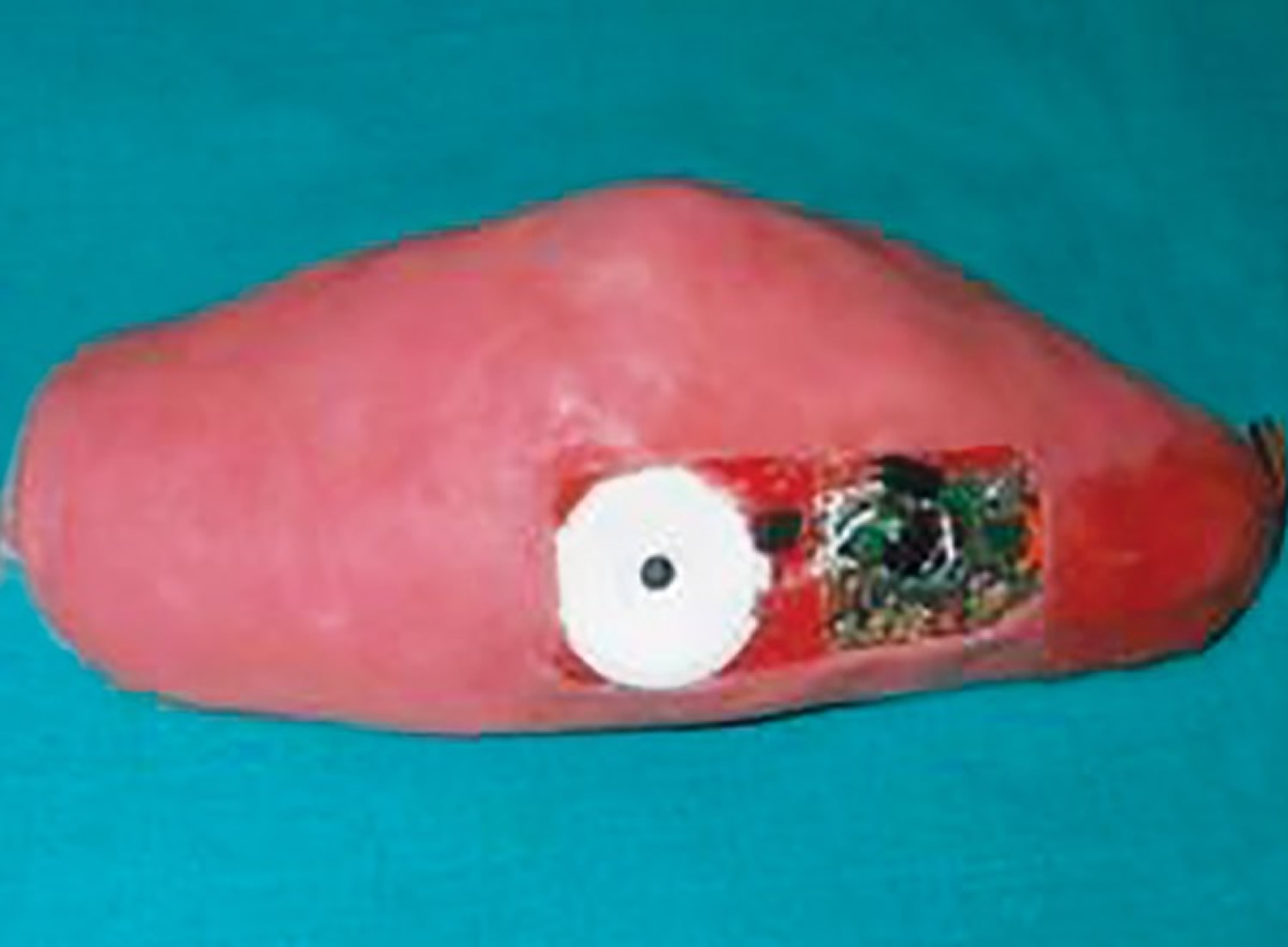
The ‘three-alarm’ system elbow guard appliance has a microchip that may be incorporated with the favorite music such that the child may indulge in hearing the music and stop the thumb/digit sucking habit. However, at school the music may be a disturbance, so the vibration chip used in mobile phones can be used so that vibrations in the elbow guard can remind the child not to suck the thumb/digit. A siren which a child is scared off also can be incorporated to remind or alarm the child to stop the habit.
Clinical observations revealed that the patient accepted the elbow guard appliance easily. They found it fashionable like a sports wear, so they did not try to remove it. The elbow guard was firm enough to prevent the child from removing the appliance and was also loose enough to allow limited movement and did not interfere with the blood flow and also the finger was protected from the harmful effects of biting. The child abandoned the habit in a short time since the appliance prevented the pleasure of sucking and, interestingly, the music reminded him to stop the habit and was distracted from sucking pleasure.
- Larsson E. Sucking, chewing, and feeding habits and the development of crossbite: a longitudinal study of girls from birth to 3 years of age. Angle Orthodontist 2001;71(2):116‐9.[↩]
- Adair SM, Milano M, Dushku JC. Evaluation of the effects of orthodontic pacifiers on the primary dentitions of 24‐ to 59‐month‐old children: preliminary study. Pediatric Dentistry 1992;14:13‐8.[↩]
- Modder T, Odenrick L, Lindner A. Sucking habits and their relation to posterior cross‐bite in 4‐year‐old children. Scandinavian Journal of Dental Research 1982;90(4):323‐8.[↩]
- Patel A. Digit sucking habits in children resident in Kettering (UK). Journal of Orthodontics 2008;35:255‐61.[↩]
- Baalack IB, Frisk AK. Finger‐sucking in children. A study of incidence and occlusal conditions. Acta Odontologica Scandinavica 1971;29(5):499‐512.[↩]
- The evaluation and treatment of pediatric oral habits. Maguire JA. Dent Clin North Am. 2000 Jul; 44(3):659-69, vii. https://www.ncbi.nlm.nih.gov/pubmed/10925776/[↩][↩]
- Thumbsucking. Rosenberg MD. Pediatr Rev. 1995 Feb; 16(2):73-4. https://www.ncbi.nlm.nih.gov/pubmed/7877915/[↩]
- Curtis SJ, Jou H, Ali S, Vandermeer B, Klassen T . A randomized controlled trial of sucrose and/or pacifier as analgesia for infants receiving venipuncture in a pediatric emergency department. BMC Pediatrics 2007;7:27.[↩]
- Hauck FR, Omojokun OO, Siadaty MS. Do pacifiers reduce the risk of sudden infant death syndrome? A meta‐analysis. Pediatrics 2005;116(5):e716‐23. http://pediatrics.aappublications.org/content/116/5/e716.long[↩]
- Shetty RM, Shetty M, Shetty NS, Deoghare A. Three-Alarm System: Revisited to treat Thumb-sucking Habit. International Journal of Clinical Pediatric Dentistry. 2015;8(1):82-86. doi:10.5005/jp-journals-10005-1289. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4472878/[↩][↩][↩][↩]
- Thumb-sucking: literature review. Johnson ED, Larson BE. ASDC J Dent Child. 1993 Nov-Dec; 60(4):385-91. https://www.ncbi.nlm.nih.gov/pubmed/8126302/[↩][↩]
- Dummy- and finger-sucking habits with special attention to their significance for facial growth and occlusion. Effect on facial growth and occlusion. Larsson E. Sven Tandlak Tidskr. 1972 Dec; 65(12):605-34.[↩][↩][↩]
- Thumb sucking habit and associated dental differences in one of monozygous twins. Willmot DR. Br J Orthod. 1984 Oct; 11(4):195-9[↩]
- Sucking habits and their relation to posterior cross-bite in 4-year-old children. Modéer T, Odenrick L, Lindner A. Scand J Dent Res. 1982 Aug; 90(4):323-8.[↩]
- Alemran SES. A new method in reminder therapy technique for ceasing digit sucking habit in children. J Clin Pediatr Dent. 2000;24(4):261–263.[↩][↩][↩]
- Van Norman R. Digit sucking: It is time for an attitude adjustment or a rationale for the early elimination of digit-sucking habits through positive behavior modification. Int J Orofacial Myology. 1985;11(2):14–21.[↩]
- Borrie FRP, Bearn DR, Innes NPT, Iheozor‐Ejiofor Z. Interventions for the cessation of non‐nutritive sucking habits in children. Cochrane Database of Systematic Reviews 2015, Issue 3. Art. No.: CD008694. DOI: 10.1002/14651858.CD008694.pub2[↩]
- Benjamin LS. The beginning of thumb sucking. Child Dev. 1967;38(4):1065–1078.[↩]
- Morley M. Management of non-nutritive or digit sucking habits in children: a practical approach. J Can Dent Assoc. 1994;60(11):969–971.[↩]
- Bengi AO, Karacy S, Guven G. A unique treatment of finger-sucking habit in children with mental retardation: report of 2 cases. Quint Int. 2007;38(3):172.e158–163.[↩]
- Norton LA, Gellin ME. Management of digital sucking and tongue thrusting in children. Dent Clin North America July. 1968:363–382. https://www.ncbi.nlm.nih.gov/pubmed/5240768[↩]





{kind=link}