
What is an imperforate hymen
Imperforate hymen is the most common type of blockage of the vagina. Imperforate hymen is something a girl is born with. No one knows why this happens. There is nothing that the mother did to cause it.
The hymen is a thin membrane, a layer of connective tissue that forms a transverse septum and obstructs the vaginal opening 1. The hymen is an embryological remnant of mesodermal tissue that normally perforates during the later stages of embryo development. The hymen most often covers part of the opening of the vagina. Imperforate hymen is when the hymen covers the whole opening of the vagina and there is no perforation of this membrane. Usually the central portion of this membrane perforates through the degeneration of its epithelial cells 1. Failure of the degeneration of the epithelial cells and subsequent perforation leads to a hymen that is termed imperforate 1.
The function of the hymen is not clear but is thought to include innate immunity as it provides a physical barrier to infections during the pre-pubertal period when the vaginal immunity is not fully developed 2.
Imperforate hymen is rarely associated with other female genital tract malformations 3 although some authors 4 have emphasized the need to rule out associated mullerian malformations.
The reason for non-perforation of this membrane is unknown. Imperforate hymen occurs mostly in a sporadic manner, although some familial occurrences have been reported 5. Both the recessive and dominant modes of transmission have been suggested, but no genetic markers or mutations have been proven as aetiological factors 6. An imperforate hymen in younger children (<10 years) is discovered by chance in 90% of cases, while 100% of affected adolescents first present with symptoms 7.
Girls can be diagnosed with imperforate hymen at any age. It is most often diagnosed at birth or later at puberty.
At birth or early childhood, the health care provider may see that there is no opening in the hymen during a physical exam.
At puberty, girls usually do not have any problems from an imperforate hymen until they start their period. The imperforate hymen blocks the blood from flowing out. As the blood backs up the vagina, it causes:
- Mass or fullness in the lower part of the belly (from the build up of blood that can’t come out)
- Stomach pain
- Back pain
- Problems with urinating and bowel movements
Imperforate hymen is a rare cause of abdominal pain in female adolescents 8. Imperforate hymen is seen in approximately 1 in 2000 females, although information on the true incidence is difficult to obtain 9. The lack of menstrual periods in an adolescent girl of post-menarcheal age with cyclical abdominal pain, urinary retention, constipation and/or a lower abdominal mass suggests imperforate hymen should be considered 10.
Your doctor will do a pelvic exam. Your doctor may also do a pelvic ultrasound and imaging studies of the kidneys. This is done to ensure that the problem is imperforate hymen rather than another problem. Your doctor may recommend that the girl see a specialist to make sure that the diagnosis is imperforate hymen.
Gynecological examination reveals a bluish bulging hymen and generally an abdominal mass. The diagnosis can be established with an abdominal ultrasound showing the pelvic cystic mass. Imperforate hymen should be differentiated from a low transverse vaginal septum using the Valsalva maneuver: an imperforate hymen should bulge and a transverse vaginal septum should not 11. Imperforate hymen is usually not associated with any other Müllerian abnormalities and extensive investigation for urogenital anomalies is unnecessary 11.
Early diagnosis of an imperforate hymen is important, since it can lead to serious complications such as infections, hydronephrosis (swelling of a kidney due to a build-up of urine), kidney failure, endometriosis and subfertility 12. A retrospective study showed that eight of nine patients with menstrual blood accumulates in the vagina (hematocolpos) or menstrual blood accumulates in the uterus (hematometra) due to an outflow obstruction had endometriosis at the time of intra-abdominal operation 13.
Figure 1. Female reproductive organs
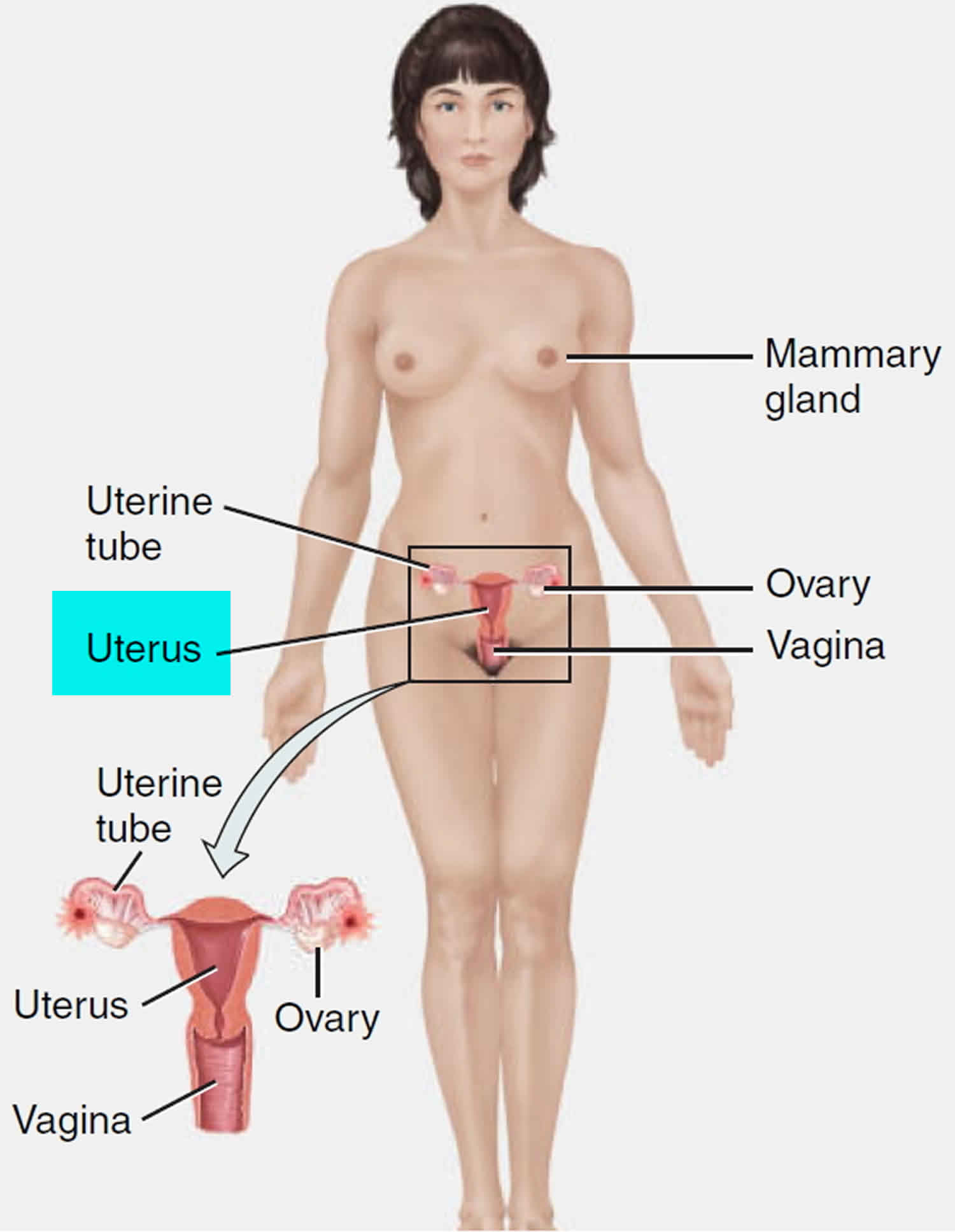
Figure 2. Side view of female reproductive organs
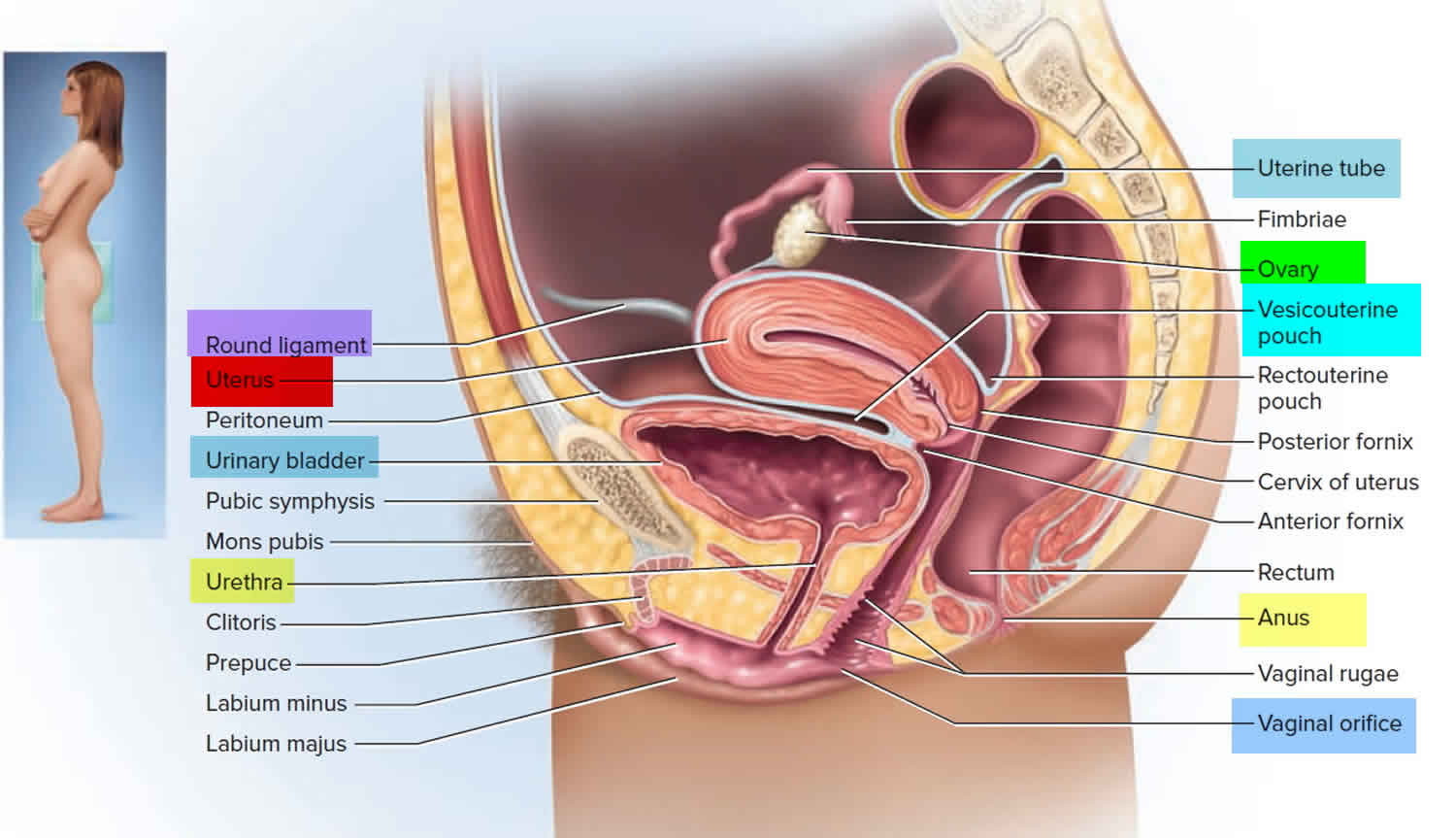
Figure 3. Front view of female reproductive organs
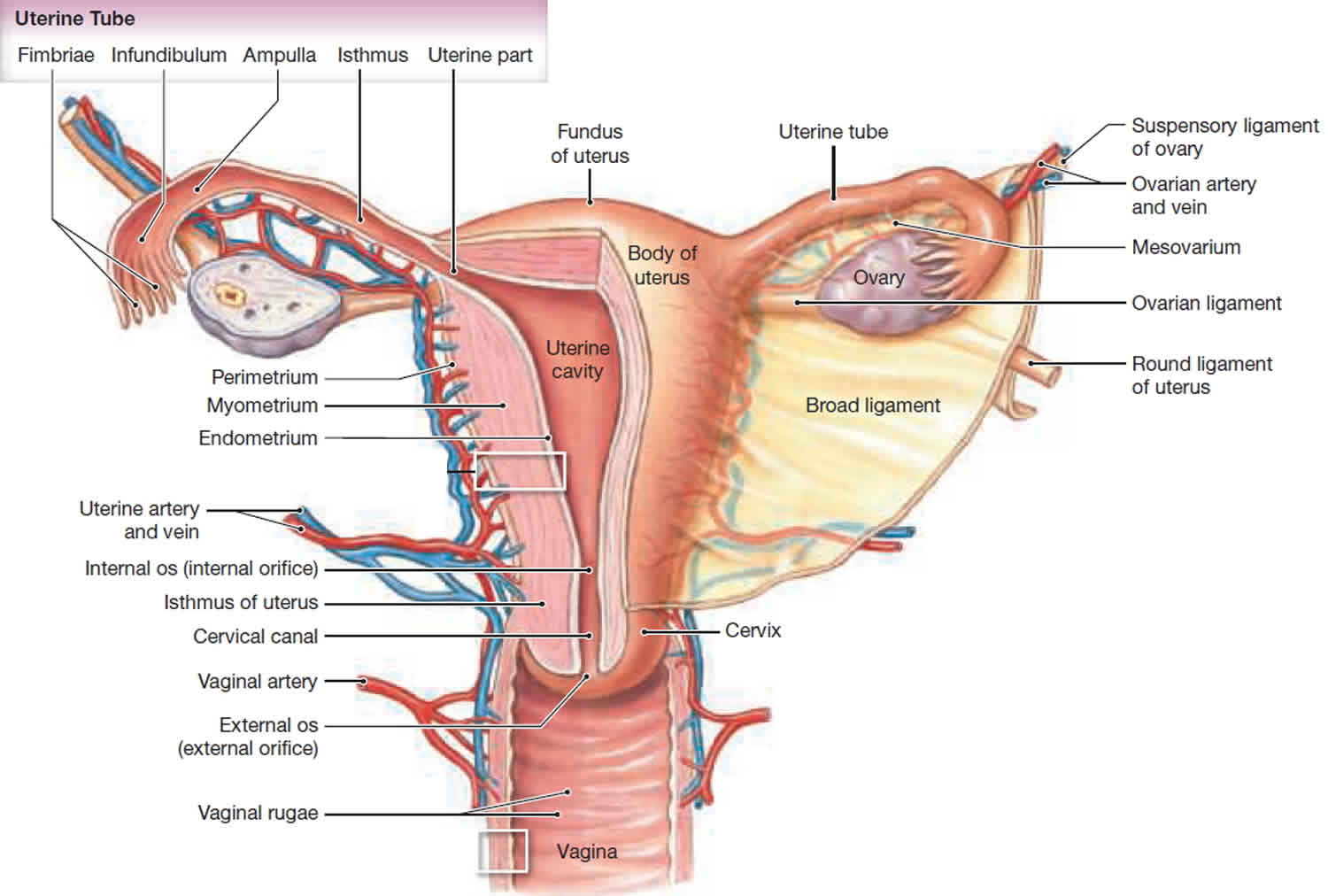
Figure 4. Imperforate hymen

Footnote: A 16-year-old girl was admitted with a history of lower abdominal pain. She was asymptomatic until a year previously. She then started developing cyclical crampy pain in the lower abdomen, which lasted for 7 days every month. The pain had become more severe during the previous 2 months and the size of her abdomen had increased over the past few months. There was no history of nausea, vomiting, fever, altered bowel habits or problems with urinating. She was 13 years old and had not yet had a menstrual period, but did have pubic hair and breast buds, confirming the onset of puberty. The patient denied any vaginal discharge and there was no history of sexual activity. No other members of her family had similar or other physical complaints. The medical history was unremarkable.
[Source 14 ]Imperforate hymen symptoms
The most common symptoms of an imperforate hymen are cyclical abdominal pain and urinary retention, usually presenting between the ages of 13 and 15 years (when menarche occurs) 15. There is primary amenorrhea (absence of menstrual periods by age 15 or 16 years, which is approximately 2.5 to 3 standard deviations from the mean) 16 but secondary sex characteristics are well developed. Because the vaginal outflow is obstructed by the non-perforated hymen, menstrual blood accumulates in the vagina (hematocolpos) and the uterus (hematometra). This may lead to mechanical effects on the urethra, bladder, intestines or pelvic blood vessels which can result in urinary retention, severe or complete constipation (obstipation) or edema of the legs 17. Irritation of the sacral plexus or nerve roots can cause lower back pain 18. Problems with intercourse are rarely mentioned, probably because most of the patients are still sexually inactive 19.
Some symptoms of appendicitis are similar to those of an imperforate hymen, and there are cases where groundless appendectomies have been performed 20. In addition, there is often an initial diagnosis of infection of the bladder, nephrolithiasis (kidney stone) or abdominal tumor, which leads to unnecessary examinations and treatment. The history and physical examination are frequently incomplete 9. One should always consider an imperforate hymen if there is a discrepancy between the Tanner stage and menarcheal status 9.
Imperforate hymen can present during three main stages in life:
- In utero: This is the rarest and occurs due to maternal estrogenic stimulation that leads to uterovaginal secretions filling up the blind vagina and presenting as hydrocolpos diagnosed through obstetric ultrasound 21. The diagnosis should be confirmed post natally.
- New-born-infanthood-childhood: In new-born period this may occur due to maternal estrogenic stimulation that leads to uterovaginal secretions filling up the blind vagina and presenting with hydrocolpos 3.
- At puberty: This is the commonest. It occurs when a girl starts menstruating and the menstrual blood accumulates in the vagina 22. The age of presentation (mean, range) is 13.2 and 11-16 years respectively according to Liang et al 1 or 12 and 10-15 years respectively according to Lui et al 23. Liang and colleagues 1 did a ten year retrospective analysis of 15 women treated for imperforate hymen through telephone based researcher administered questionnaire and a subsequent physical and sonographic examination. In their study, Lui et al 23 did a ten year retrospective analysis of the data of 15 patients treated for imperforate hymen but did not do any follow up patient interview or examination. Kurgodlu and colleagues 24 argue that the age of presentation is 2.5-4 years after thelarche (onset of secondary breast development, usually occurring at the beginning of puberty in girls).
Among the pubertal girls, imperforate hymen will present in the following ways.
Amenorrhea
- Primary amenorrhea (absence of menstruation or menstrual periods)
- This is because the girl has started menstruating but does not experience any menstrual flow as the blood accumulates in the vagina, then in the uterus and occasionally, eventually into the fallopian tubes 25.
- Secondary amenorrhea
- This can occur following spontaneous closure of previously perforate hymen 5. This can happen with a micro perforate or stenosed hymen. In such initial light periods will be experienced but continuous stenosis leads to complete obstruction and amenorrhea 5.
- It can also occur as a result of stenosis of the hymenal opening following surgical or sexual trauma 5.
- Lastly, it can occur as failure of hymenotomy 22. In the months following hymenotomy the patient experiences her menstrual flow but the margins of the hymenotomy incision adhere and eventually occlude the vaginal outflow leading to amenorrhea.
Cryptomenorrhea
Pain
Recurrent cyclical lower abdominal/pelvic pains (up to 60%) 26. This is due to continued distension of the vagina and uterus by accumulating menstrual blood.
Low back pain (38-40%) 27. Occurs as referred pain following irritation of the sacral plexus and nerve roots by the distended vagina and uterus.
Obstruction
- Urinary outflow obstruction and its complications (58%) 28
- Acute urine retention (3-60%) 28. This occurs by a number of mechanisms
- Pressure on the bladder by the distended uterus causing angulation at the bladder neck and kinking of the urethra 22
- Direct pressure on the urethra causing urethral tamponade 22
- The bulging hymen distends the vagina and may cause cephalad angulation at the urethral meatus further stretching the urethra and worsening tamponade 29.
- Complications of prolonged or recurrent urine retention /obstruction
- Acute urine retention (3-60%) 28. This occurs by a number of mechanisms
- Vaginal outflow obstruction- Cryptomenorrhea
- Intestinal obstruction
- Constipation (20-27%) 23
- Tenesmus
- Lymphovenous obstruction: Compression of the pelvic veins and lymphatics can impair lymphovenous return from the lower limbs leading to edema 3.
Mass
- Distended uterus felt as pelvic mass on abdominal examination (20%) 23
- The distended vagina is felt as a pelvic mass on digital rectal examination
- A bluish bulging hymen is observed beneath the labia (60%) 23
- A cystic retropubic mass is revealed on ultra sonography or MRI 23
Imperforate hymen treatment
Treatment of menstrual blood accumulates in the vagina (hematocolpos) or menstrual blood accumulates in the uterus (hematometra) due to an imperforate hymen is to make cruciate incision in the hymen which allows the accumulated blood to drain away 14. This has to be done aseptically as a closed vagina lacks protective Doederlein’s bacilli and the pH is alkaline or weakly acidic; there is a poor natural resistance to bacteria entering from the lower genital tract and the blood and debris provide a good culture medium 11. The complications of a hymenectomy are bleeding, scarring and stenosis of the vaginal opening 31. Less invasive treatments for an imperforate hymen include the use of CO2 lasers or a Foley catheter 32.
In a retrospective study of the long term results of surgical correction of imperforate hymen, nine of 15 patients had an irregular menstrual cycle and six of 15 patients had dysmenorrhea (painful periods) (over a follow-up of 8.5 years). Most patients had no sexual dysfunction. Pre-operative complaints of cryptomenorrhea (n=15), abdominal pain (n=11), palpable mass in the lower abdomen (n=9), urinary retention (n=6), dysuria (n=3) and problems defecating (n=4) almost all disappeared after surgery 19. Eight patients worried about their future fertility; two of them were attempting pregnancy and were successful. Another study showed that 86% of patients who attempted pregnancy succeeded after surgical correction of imperforate hymen 33.
Imperforate hymen surgery
A minor surgery can fix an imperforate hymen. The surgeon makes a small cut or incision and removes the extra hymen membrane.
- Girls who are diagnosed with imperforate hymen as babies most often have surgery when they are older and have just started puberty. The surgery is done in early puberty when breast development and pubic hair growth has begun.
- Girls who are diagnosed when they are older have the same surgery. The surgery allows retained menstrual blood to leave the body.
Imperforate hymen surgery recovery
Girls recover from this surgery in a few days. After girls recover from the surgery, they will have normal periods. They can use tampons, have normal sexual intercourse, and have children.
After surgery, the girl may have to insert dilators into the vagina for 15 minutes each day. A dilator looks like a tampon. This keeps the incision from closing on itself and keeps the vagina open.
When to see your doctor
See your doctor if:
- There are signs of infection after surgery, such as pain, pus, or fever.
- The hole in the vagina seems to be closing. The dilator will not go in or there is a lot of pain when it is inserted.
- Liang CC, et al. Long-term follow-up of women who underwent surgical correction for imperforate hymen. Arch Gynecol Obstet. 2003;269(1):5–8.[↩][↩][↩][↩][↩]
- Basaran M, et al. Hymen sparing surgery for imperforate hymen; case reports and review of the literature. J pediatr Adolesc Gynecol. 2009;22(4):e61–e64.[↩]
- Nagai N, et al. Life threatening acute renal failure due to imperforate hymen in an infant. Paediatrics International. 2012 Apr;54(2):280–2.[↩][↩][↩][↩]
- Eksioglu AS, et al. Imperforate hymen causing bilateral hydroureteronephrosis in an infant with bicornuate uterus. Urology Case Reports. 2012;2012:102683. Epub 2012 Jun 7.[↩][↩][↩]
- Khan Z.A, et al. Imperforate hymen: a rare case of secondary amenorrhea. J Obstet Gynaecol. 2011;31(1):91–92.[↩][↩][↩][↩]
- Familial occurrence of imperforate hymen. Sakalkale R, Samarakkody U. J Pediatr Adolesc Gynecol. 2005 Dec; 18(6):427-9.[↩]
- Early detection of imperforate hymen prevents morbidity from delays in diagnosis. Posner JC, Spandorfer PR. Pediatrics. 2005 Apr; 115(4):1008-12.[↩]
- Lardenoije C, Aardenburg R, Mertens H. Imperforate hymen: a cause of abdominal pain in female adolescents. BMJ Case Rep. 2009;2009:bcr08.2008.0722. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3029536/[↩]
- Posner JC, Spandorfer PR. Early detection of imperforate hymen prevents morbidity from delays in diagnosis. Pediatrics 2005; 115: 1008.[↩][↩][↩]
- Doyle JC. Imperforate hymen: with and without hematocolpos. A review of the literature and a report of twenty cases. Cal West Med 1942; 56: 242–7[↩]
- Dane C, Dane B, Erginbas M, et al. Imperforate hymen – a rare cause of abdominal pain: two cases and review of the literature. J Pediatr Adolesc Gynecol 2007; 20: 245–7[↩][↩][↩]
- Loscalzo IL, Catapano M, Loscalzo J, et al. Imperforate hymen with bilateral hydronephrosis: an unusual emergency department diagnosis. J Emerg Med 1995; 13: 337–9[↩]
- Olive DL, Henderson DY. Endometriosis and mullerian anomalies. Obstet Gynecol 1987; 69: 412–15[↩]
- Lardenoije C, Aardenburg R, Mertens H. Imperforate hymen: a cause of abdominal pain in female adolescents. BMJ Case Rep. 2009;2009:bcr08.2008.0722.[↩][↩]
- Hall DJ. An unusual case of urinary retention due to imperforate hymen. J Accid Emerg Med 1999; 16: 232–3[↩]
- McLean M, Davis AJ, Reindollar RH. Abnormalities of Female Pubertal Development. [Updated 2015 Aug 19]. In: De Groot LJ, Chrousos G, Dungan K, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK278950[↩]
- Isenhour JL, Hanley ML, Marx JA. Hematocolpometra manifesting as constipation in the young female. Acad Emerg Med 1999; 6: 752–3[↩]
- Letts M, Haasbeek J. Hematocolpos as a cause of back pain in premenarchal adolescents. J Pediatr Orthop 1990; 10: 731.[↩]
- Liang CC, Chang SD, Soong YK. Long-term follow-up of women who underwent surgical correction for imperforate hymen. Arch Gynecol Obstet 2003; 269: 5–8[↩][↩]
- Nazir Z, Rizvi RM, Qureshi RN, et al. Congenital vaginal obstructions: varied presentation and outcome. Pediatr Surg Int 2006; 22: 749–53[↩]
- Ayaz UM, et al. Ultrasonographic diagnosis of congenital hydrometrocolpos in prenatal and newborn period: a case report. Medical ultrasonography. 2011;13(3):234–236.[↩]
- Abu-Ghanem S, et al. Recurrent urinary retention due to imperforate hymen after hymenotomy failure: a rare case report and review of the literature. Urology. 2010;78(1):180–182.[↩][↩][↩][↩]
- Lui CT, et al. A retrospective study on imperforate hymen and hematocolpos in a regional hospital. Hong Kong J emerg med. 2010;17(5):435–440.[↩][↩][↩][↩][↩][↩]
- Kurgodlu Z, et al. Spontaneous rupture of the imperforate hymen in an adolescent girl with hematocoplometra. ISRN obstetrics and Gynecology. 2011;2011:520304. Epub 2010 Sep 29 [↩]
- Ercan CM, et al. Imperforate hymen causing hematocolpos and acute urinary retention in an adolescent girl. Taiwanese Journal of Obstetrics and Gynecology. 2011;50(1):118–120.[↩]
- Kurgodlu Z, et al. Spontaneous rupture of the imperforate hymen in an adolescent girl with hematocoplometra. ISRN obstetrics and Gynecology. 2011;2011:520304. Epub 2010 Sep 29[↩]
- Drakonaki EE, et al. Hematocolpometra due to an imperforate hymen presenting with low back pain. J Ultrasound Med. 2010;29(2):321–322.[↩]
- Lui CT, et al. A retrospective study on imperforate hymen and hematocolpos in a regional hospital. Hong Kong J emerg med. 2010;17(5):435–440[↩][↩]
- Anselm OO, Ezegwui UH. Imperforate hymen presenting as acute urinary retention in a 14-year old Nigerian girl. J Surg Tech case Rep. 2010;2(2):84–86.[↩]
- Shen MC, Yang LY. Imperforate hymen complicated with pyocolpos and lobar nephronia. J Chin Med Assoc. 2006;69(5):224–227.[↩]
- Chang JW, Yang LY, Wang HH, et al. Acute urinary retention as the presentation of imperforate hymen. J Chin Med Assoc 2007; 70: 559–61[↩]
- Ali A, Cetin C, Nedim C, et al. Treatment of imperforate hymen by application of Foley catheter. Eur J Obstet Gynecol Reprod Biol 2003; 106: 3–4[↩]
- Rock JA, Zacur HA, Dlugi AM, et al. Pregnancy success following surgical correction of imperforate hymen and complete transverse vaginal septum. Obstet Gynecol 1982; 59: 448–51[↩]





{kind=link}