What is labrum tear shoulder
Shoulder labrum tear is an injury to the labrum of the shoulder, which is the ring of cartilage that surrounds the socket of the shoulder joint. Shoulder labrum tear is also called superior labral anterior to posterior (SLAP) lesions constitute a recognized clinical subset of complex shoulder pain pathologies. Shoulder labrum tear has a preference for young laborers, overhead athletes, and middle-aged manual laborers 1. In 1985, Andrews first described superior labral pathologies, and Snyder later coined the term “SLAP lesion” because of the location and characteristic tear extension patterns 2. Snyder developed the initial 4-subtype classification of these lesions. In the ensuing decades, other groups including Morgan et al. 3 and Maffet et al. 4 further subdivided the shoulder labrum tear (SLAP) classification schemes to ultimately delineate ten different types of shoulder labrum tear (SLAP) tear patterns, including combined shoulder labrum tear (SLAP)- and Bankart-type injuries seen in specific associative patterns 5.
Advances in contemporary diagnostic capabilities and arthroscopic management techniques have led to evolving management paradigms since the original descriptions of shoulder labrum tear (SLAP)-type lesions. These injuries are not solely limited to young throwing athletes as originally described, and shoulder labrum tear tears commonly can be seen in various patient populations with varying degrees of actual clinical relevance. There is increasing evidence that shoulder labrum tear tears are frequently present on MRI in asymptomatic overhead athletes.
The highest incidence rates of shoulder labrum tear (SLAP) lesions present in the 20- to 29-year-old and 40- to 49-year-old age groups 6. Additionally, experts now recognize that shoulder labrum tear (SLAP) lesions commonly occur in asymptomatic overhead athletes 7. Analogous to meniscal cleavage planes, many Major League Baseball (MLB) team physicians now recognize these asymptomatic “tears” as adaptive changes in high-level, experienced overhead throwers and MLB pitchers 8.
As knowledge evolved over time with improvements in magnetic resonance imaging (MRI) quality, shoulder labrum tear (SLAP) subsequently became a more frequent diagnosis. However, the ideal treatment of shoulder labrum tear (SLAP) was never fully elucidated, and thus the increasing recognition of shoulder labrum tear (SLAP) injuries brought about an increased incidence of shoulder labrum tear (SLAP) repair rates across institutions.
As our knowledge regarding the actual clinical significance of shoulder labrum tear (SLAP) presentations continued to evolve from 2010 and beyond, the initial rise in the incidence rate of shoulder labrum tear (SLAP) repairs performed reached its peak before subsequently declining over the last decade. Moreover, clinicians began reporting on the critical importance of differentiating younger, active patient populations (e.g., under 40 years old) and overhead athletes from the older patients (e.g., over 40 years old) with degenerative shoulder labrum tears (SLAP) secondary to repetitive overhead manual laborer occupations 9.
Erickson et al. 10 reported in 2016 that an institutional trend from 2004 to 2014 revealed decreasing rates of total shoulder labrum tear (SLAP) repairs performed. Further, the age of patients operated on for shoulder labrum tears was decreasing, and the majority of shoulder labrum tear (SLAP) repairs still being performed by the latter half of the study were limited to mostly type 2 shoulder labrum tears (SLAP).
A 2015 study investigated the adjusted incidence rates of shoulder labrum tears (SLAP) as reported in the Defense Medical Epidemiological Database between 2002 and 2009. The adjusted annual incidence rate for shoulder labrum tear (SLAP) lesions increased from 0.31 cases per 1000 person-years in 2002 to 1.88 cases per 1000 person-years in 2009, with an average annual increase of just over 20% during the study period 11.
Despite the aforementioned limitations, the contemporary consensus regarding shoulder labrum tears (SLAP) is that they account for 80% to 90% of labral pathology in the stable shoulder, although they are typically seen in association with other shoulder pathologies and rarely present in isolation 12. Furthermore, shoulder labrum tears (SLAP) account for approximately 1% to 3% of injuries presenting to sports medicine referral centers, and shoulder labrum tears (SLAP) are present in approximately 6% of shoulder arthroscopy procedures 13.
Shoulder anatomy
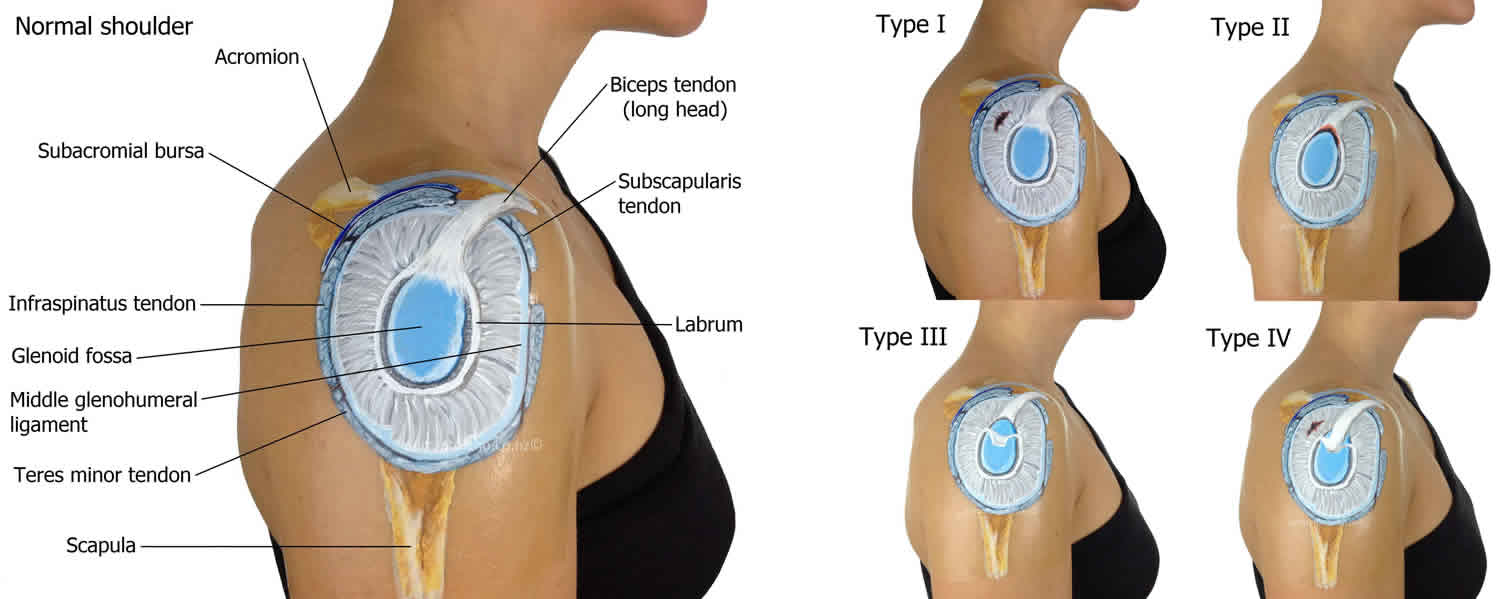
Your shoulder is a ball-and-socket joint made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
The head of your upper arm bone fits into a rounded socket in your shoulder blade. This socket is called the glenoid. Surrounding the outside edge of the glenoid is a rim of strong, fibrocartilage tissue called the labrum 14. The labrum helps to deepen the socket and stabilize the shoulder joint. It also serves as an attachment point for many of the ligaments of the shoulder, as well stabilizing the long head of biceps tendon improving glenohumeral joint stability 15.
The glenohumeral joint is stabilized by static and dynamic restraints. Static restraints include capsuloligamentous structures, labrum and negative intraarticular pressure. Dynamic restraints include rotator cuff muscles, periscapular muscles and biceps muscle 16. The vascular supply of labrum is provided by suprascapular, circumflex scapular and posterior humeral arteries 17. The anterosuperior margin of the glenoid rim has limited vascularity making it more vulnerable to injuries and having impaired healing potential 17. The relationship between superior labrum and long head of biceps tendon is a special concern because of the considerable anatomic variability between this structures 16. There are some anatomic variants for glenoid labrum and biceps tendon; the most common normal variation is a labrum attached to the glenoid rim and there is a broad middle glenohumeral ligament. One kind of anatomic variation is the sublabral recess, which represents a gap located inferior to the biceps anchor and the anterosuperior portion of the labrum. It is usually seen in 12-o’clock position of the glenoid in arthroscopic surgery 18. Another variant is the sublabral foramen, which is a groove between the normal anterosuperior labrum and the anterior cartilaginous border of the glenoid rim. Another variation is the Buford complex which is characterized by the absence of the anterosuperior labral tissue with the presence of a thick cord-like middle glenohumeral ligament 18.
Figure 1. Shoulder anatomy
Shoulder labrum tear causes
The specific cause underlying the various shoulder labrum tear (SLAP) presentations is multifactorial and remains a topic of debate and controversy 5. Regardless of the underlying cause, patients presenting with symptomatic shoulder labrum tear tears will commonly report the acute onset of deep shoulder pain accompanied by mechanical symptoms such as popping, locking, or catching with various shoulder movements.
Acute traumatic shoulder labrum tear lesions
Traumatic injuries commonly occur following acute, index events based on one of the following mechanisms 2:
- Compression-type injuries
- Classically advocated by Snyder 2 as his original case series from 1990 reported about half of the patient presentations were status post a fall onto an outstretched arm with the arm in varying degrees of shoulder abduction
- Traction-type injuries
- Occur secondary to sudden jerking movements or after lifting heavy objects
- Can occur after an unexpected pull on the arm
- Combined-type injuries
Attritional shoulder labrum tear injuries
Peel-back mechanism
Compared to the acute, traumatic shoulder labrum tear injuries, the overhead athlete is more likely to present with attritional-based etiologies. In these scenarios, shoulder labrum tears present with the insidious onset and progressive deep shoulder pain in young athletes with the arm in the abduction and external rotation position during the late-cocking phase of throwing. In this position, the force on the biceps coupled with the posterior glide of the humerus results in the peeling off of the posterosuperior quadrant of the glenoid and posterior labrum 19.
There remains debate regarding whether the so-called peel-back mechanism versus the deceleration phase of throwing is most responsible for the pathologic forces driving shoulder labrum tears in overhead athletes 20. The former implicates the late-cocking phase of throwing while the latter would theoretically implicate more traction-based mechanisms. Cadaveric studies have demonstrated shoulder labrum tears are more likely to occur with the shoulder in a forward flexed position compared to positions in extension 21.
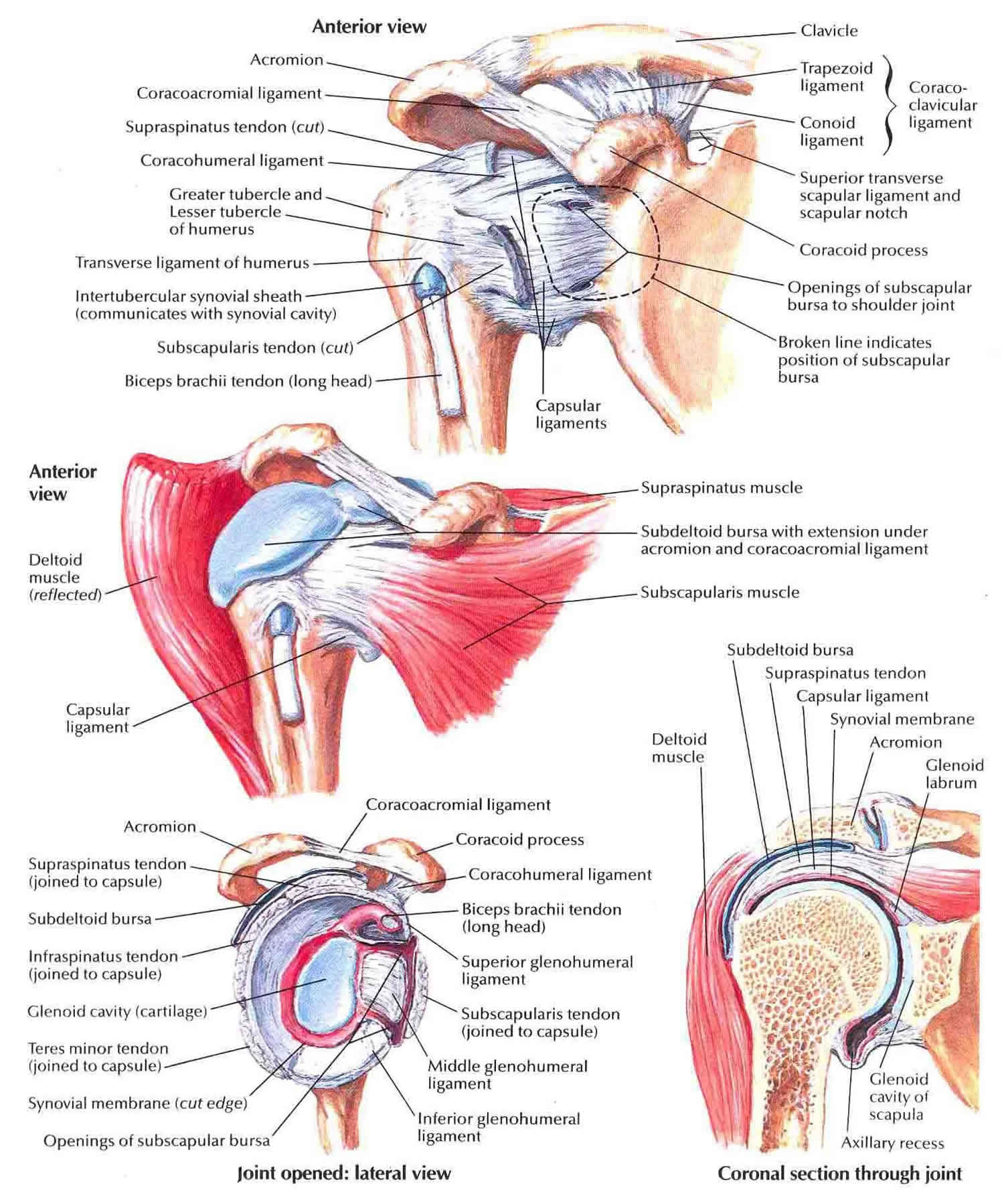
Figure 2. Shoulder labrum tear classification
Footnote: Superior labrum anterior to posterior tear classification. Type 1: Degenerative fraying of the superior labrum, biceps anchor is intact; Type 2: Superior labrum and biceps tendon detachment from glenoid rim; Type 3: Bucket-handle tear of labrum with intact biceps anchor; Type 4: Bucket-handle tear of labrum extended into the biceps tendon; Type 5: Superior labrum anterior to posterior (SLAP) with anterior inferior extension; Type 6: Anterior or posterior flap tear with the bucket handle component tear; and Type 7: SLAP with extension to the middle glenohumeral ligament.
[Source 22 ]Degenerative shoulder labrum tear lesions
Degenerative shoulder labrum tears can develop secondary to the normal “wear-and-tear” patterns seen in patients with advanced age. Degenerative shoulder labrum tears often affect overhead laborers with increasing degrees of association in patients over 40 years old 10.
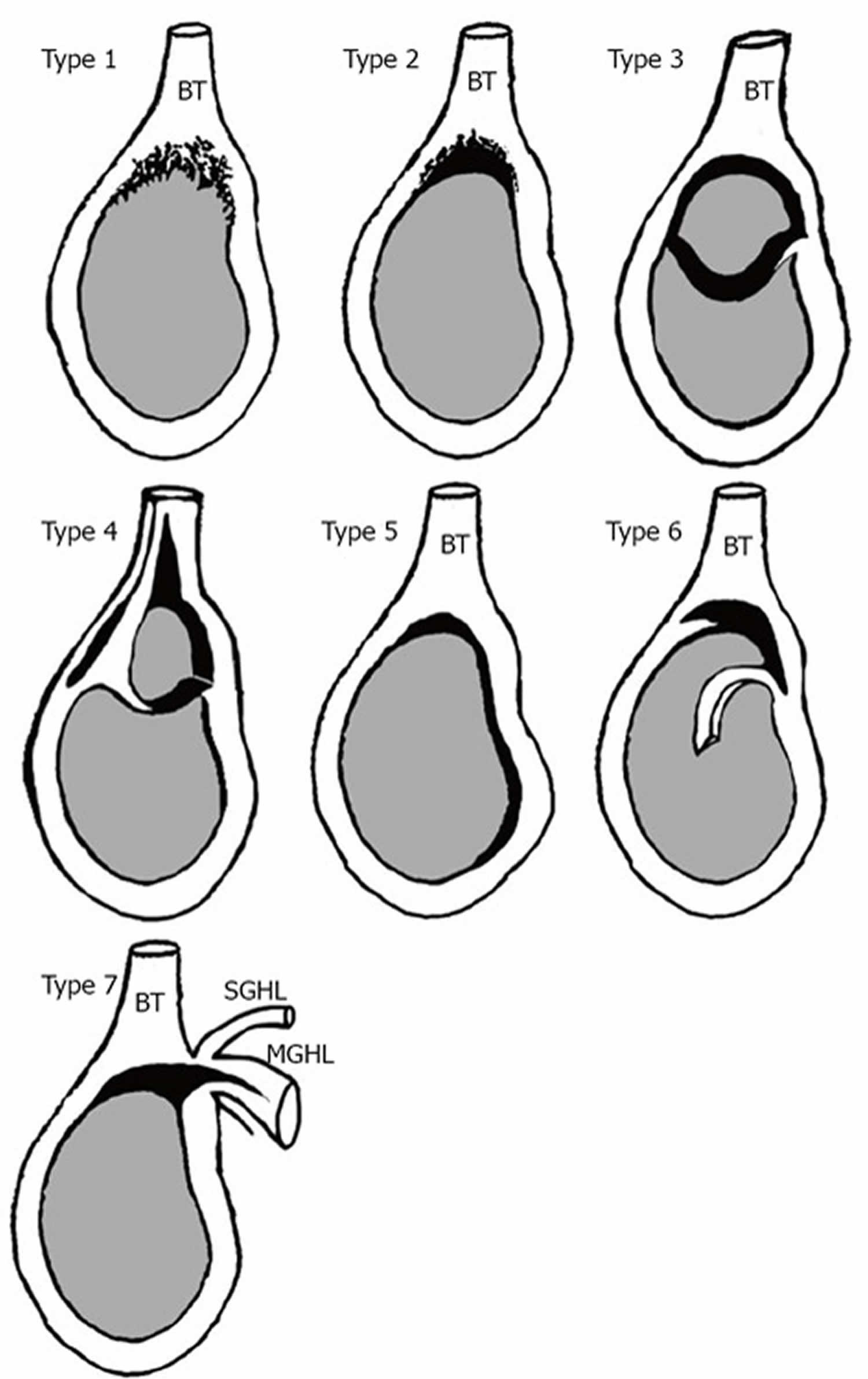
Types 1 – 8 23
Type 1 shoulder labrum tear
- Degenerative
- Fraying occurs at the free edge of the labrum
- Insertion to the superior glenoid remains intact
Type 2 shoulder labrum tear
- Acute
- The labrum and the long head of biceps tendon are torn and avulses off the glenoid cavity
- The avulsed area is now devoid of cartilage in the zone of injury
Type 3 shoulder labrum tear
- The “bucket-handle” pattern
- The labral insertion of long head of the biceps tendon is left unaffected
- Rarest form
Type 4 shoulder labrum tear
- “Type 3 plus anterior shoulder instability”
- Type 3 tear pattern plus extension into the long head of the biceps tendon
- Often seen in association with shoulder instability, and anterior labral tears
Type 5 shoulder labrum tear
- “Type 2 plus anterior shoulder instability”
Type 6 shoulder labrum tear
- Incidence rate is unknown
- Tear pattern involves larger superior labral flaps without detachment of the long head of the biceps tendon insertion
Type 7 shoulder labrum tear
- Type 2 shoulder labrum tear pattern plus middle and inferior inferior glenohumeral ligament compromise
- Tear pattern seen in the setting of complex shoulder instability presentations
Type 8 shoulder labrum tear
- Type 2 shoulder labrum tear pattern plus additional cartilage injury adjacent to the bicipital footplate
Shoulder labrum tear symptoms
The common symptoms of a shoulder labrum tear (SLAP) are similar to many other shoulder problems. They include:
- A sensation of locking, popping, catching, or grinding
- Pain with movement of the shoulder or with holding the shoulder in specific positions
- Pain with lifting objects, especially overhead
- Decrease in shoulder strength
- A feeling that the shoulder is going to “pop out of joint”
- Decreased range of motion
- Pitchers may notice a decrease in their throw velocity, or the feeling of having a “dead arm” after pitching
Pertinent elements in history taking to best elucidate the nature of a potential shoulder labrum tear (SLAP) (or other associated shoulder injuries) include 24:
- Acute onset of “deep” shoulder pain
- Mechanical symptoms: popping, locking, catching with various movements and activity
- History of any sudden, jerking force to the shoulder with an associated onset of pain
- History of or current episodes of shoulder instability
- History of or current sport-specific participation
- Including level of competition (e.g., professional, collegiate, recreational)
- Common shoulder labrum tear (SLAP)-provoking sports include but are not limited to:
- Overhead sports (volleyball, baseball pitchers, javelin, swimming)
- History or current manual/physical laborer occupations
Characteristics of long head of the biceps tendon-associated pathologies have been previously described and may include any combination of the following:
- Atraumatic, insidious onset of anterior shoulder pain
- Symptom exacerbation with overhead activities
- Pain radiating down the anterior arm from the shoulder
- Clicking or audible popping reported in the setting of proximal biceps instability
- Pain at rest, pain at night
In addition, a thorough history includes a detailed account of the patient’s occupational history and current status of employment, hand dominance, history of injury/trauma to the shoulder(s) and/or neck, and any relevant surgical history.
Shoulder labrum tear diagnosis
Your doctor will talk with you about your symptoms and when they first began. If you can remember a specific injury or activity that caused your shoulder pain, it can help your doctor diagnose your shoulder problem — although many patients may not remember a specific event. Any work activities or sports that aggravate your shoulder are also important to mention, as well as the location of the pain, and what treatment, if any, you have had.
During the physicial examination, your doctor will check the range of motion, strength, and stability of your shoulder.
He or she may perform specific tests by placing your arm in different positions to reproduce your symptoms. Your doctor may also examine your neck and head to make sure that your pain is not coming from a “pinched nerve.”
The results of these tests will help your doctor decide if additional testing or imaging of your shoulder is necessary.
Imaging Tests
X-rays. This imaging test creates clear pictures of dense structures, like bone. The labrum of the shoulder is made of soft tissue so it will not show up on an x-ray. However, your doctor may order x-rays to make sure there are no other problems in your shoulder, such as arthritis or fractures.
Magnetic resonance imaging (MRI) scan. This test can better show soft tissues like the labrum. To make a tear in the labrum show up more clearly on the MRI, a dye may be injected into your shoulder before the scan is taken.
Shoulder labrum tear test
The available evidence of level I and II studies in the recent literature suggests that a combination of specific tests such as the Speed’s test and uppercut test is recommended for the clinical detection of biceps tendon lesions 5.
Recent studies have reported on the diagnostic accuracy of specific tests concerning diagnosing shoulder labrum tears (SLAP):
Speed’s test 25:
- Sensitivity: 32%
- Specificity: 75%
- A positive test consists of pain elicited in the bicipital groove when the patient attempts to forward elevate the shoulder against examiner resistance; the elbow is slightly flexed, and the forearm is supinated
Uppercut test 26:
- Sensitivity: 73%
- Specificity: 78%
- The involved shoulder is positioned at neutral, the elbow is flexed to 90 degrees, the forearm is supinated, and the patient makes a fist. The examiner instructs the patient to perform a boxing “uppercut” punch while placing his or her hand over the patient’s fist to resist the upward motion. A positive test is a pain or a painful pop over the anterior shoulder near the bicipital groove region
Yergason’s test 27:
- Sensitivity: 43%
- Specificity: 79%
- The arm is stabilized against the patient’s trunk, and the elbow flexed to 90 degrees with the forearm pronated. The examiner manually resists supination while the patient also externally rotated the arm against resistance. A positive test is noted if the patient reports pain over the bicipital groove and/or subluxation of the long head of the biceps tendon.
Bear-Hug test 26:
- Sensitivity: 79%
- Specificity: 60%
- The patient places their hand on the contralateral (normal) shoulder in a “self-hug” position. The palm is on the anterior aspect of the contralateral shoulder with the elbow flexed to 90 degrees. The examiner applies a perpendicular external rotational force to try and lift the patient’s hand off of the shoulder. A positive test results when the patient cannot hold the hand against the shoulder as the examiner applies an external rotation force
Belly Press test 26:
- Sensitivity: 31%
- Specificity: 85%
- The examiner has the patient’s arm at 90 degrees of elbow flexion, and internal rotation testing is performed by the patient pressing the palm of his/her hand against the belly, bringing the elbow in front of the plane of the trunk. The examiner initially supports the elbow, and a positive test occurs if the elbow does not maintain this position upon the examiner removing the supportive force
O’Brien/Active Compression test 26:
- Sensitivity: 38%
- Specificity: 61%
- The patient is standing, and the arm of interest is positioned at 90 degrees of forward flexion, 10 degrees of adduction, and internally rotated so the thumb points toward the floor. The examiner places his or her hand over the patient’s elbow while instructing the patient to resist the examiner’s downward force applied to the arm. This maneuver is repeated with the patient’s arm now rotated, so the palm faces the ceiling. A positive test is denoted by pain located at the joint line during the initial maneuver (thumb down/internal rotation) in conjunction with reported improvement or elimination of the pain during the subsequent maneuver (palm up/external rotation)
Anterior slide test 28:
- Sensitivity: 10%
- Specificity: 82%
- The patient stands with his or her hand of the involved arm placed on the ipsilateral hip with the thumb pointing posteriorly. The examiner places one hand on the joint line of the shoulder and the other hand on the elbow. The examiner then applies an axial load in an anterosuperior direction from the elbow to the shoulder. A positive test includes pain or a painful click on the anterior or posterior joint line
Supine Resistance test 29:
- Sensitivity: 80%
- Specificity: 69%
- The patient lies supine on the exam table with his or her arms resting in full elevation with the forearm and hand supported by the table. The palm is facing upward. The examiner then applies a downward resistive force just distal to the elbow while asking the patient to perform a throwing motion. The test registers positive only if it elicits pain deep inside the shoulder joint or at the shoulder’s dorsal aspect along the joint line during the resisted movement. Performance of the test on the nonaffected shoulder should not elicit any pain
Mayo Shear test (also known as the Modified O’Driscoll test or the Modified dynamic labral shear test) 30:
- Sensitivity: 80%
- The patient stands with his or her involved arm flexed 90 degrees at the elbow and abducts the shoulder in the scapular plane to above 120 degrees. The examiner then applies terminal external rotation until resistance is appreciated. Next, the examiner applies a shear force through the shoulder joint by maintaining external rotation and horizontal abduction and lowering the arm from 120 to 60 degrees abduction. A positive test includes a reproduction of the pain and/or a painful click or catch in the joint line along the posterior joint line between 120 and 90 degrees of abduction
Shoulder labrum tear treatment
It is essential to understand that not all shoulder labrum tears (SLAP) are created equal. Clinicians should focus on the potential relevance of the shoulder labrum tear (SLAP) lesion as it attributes to the specific patient’s pain and dysfunction. Asymptomatic shoulder labrum tears (SLAP) should be observed. Those that are potentially contributing to patient-reported symptoms may require surgery, and depending on the particular shoulder labrum tear (SLAP) pattern and the presence (or absence) of other associated shoulder pathologies, the recommended surgical technique(s) may vary. Moreover, for the vast majority of shoulder labrum tear (SLAP) injuries, the initial management is nonoperative.
Nonoperative management
Anti-inflammatory medications, cryotherapy/cooling/ice application, rest and activity modification.
An initial period of rest following the acute (or acute-on-chronic) injury should be implemented in all patients. In the appropriate patient, the use of NSAIDs and cryotherapy device/ice pack application can be beneficial for pain control. Athletes and overhead laborers should also be placed on a restricted sport-specific timeline protocol, and manual laborers should receive appropriate occupational modifications.
Physical therapy
The goal of physical therapy should be to treat any underlying pathologic shoulder biomechanics that may have been present at baseline before the acute injury. Also, shoulder girdle proprioceptive training is beneficial to help prevent re-injury.
Scapulothoracic dyskinesia may result from any degree of imbalance of the shoulder girdle muscles and static/dynamic glenohumeral joint stabilizers. In addition, posterior shoulder joint capsular contractures should be addressed with various stretching and strengthening programs. Utilizing dedicated formal physical therapy regimens can help ensure each “SLAP tear” diagnosis is most appropriately managed to help mitigate the risks of inferior patient outcomes.
Multiple reports on high-level (i.e., professional) overhead throwers have demonstrated equivalent outcomes regarding return to play and return to play performance in athletes managed with operative versus nonoperative modalities alone. Nonoperative physical therapy regiments focused on correcting for scapular dyskinesia and glenohumeral internal rotation deficit (GIRD) 31.
If the non-operative therapy fails and symptoms persist that prevent sports activities or activities of daily living, then this would indicate the need for operative treatment.
Surgical management
Your doctor may recommend surgery if your pain does not improve with nonsurgical methods.. Surgical management is considered in tandem while keeping in mind each patient’s age, concomitant pathologies, functional requirements, occupational demands, and sport-specific goals.
Several authors have proposed surgical treatment algorithms depending on the specific type of shoulder labrum tear (SLAP) lesion identified on advanced imaging, clinical exam, and during intraoperative arthroscopy 25. It is critical to discern whether the labrum alone is responsible for the patient’s symptoms and whether restoring the labral attachment and biceps root to the glenoid will help. In addition, understanding how to treat a shoulder labrum tear (SLAP) in the setting of other concomitant injuries is imperative. For example, in older patients with or without rotator cuff repair, the repair of the shoulder labrum tear (SLAP) correlates with inferior results in comparison to intentional neglect or performing a bicep tenodesis/tenotomy regarding stiffness, persistent pain and need for revision surgery 8. However, in younger patients presenting with shoulder instability, the shoulder labrum tear (SLAP) injury may be present and contributing to symptoms, especially in the setting of an acute anterior and/or posterior labral tear. The following algorithm has been previously proposed 25.
Type 1 shoulder labrum tear
- Surgical treatment: arthroscopic debridement
Type 2 shoulder labrum tear
- Surgical treatment: SLAP repair versus biceps tenotomy/tenodesis
- The arthroscopic criterion for a type 2 SLAP lesion includes the ability to demonstrate (usually with an arthroscopic probe) the definitive separation of the superior labrum from the supraglenoid cartilage rim
- Burkhart previously described demonstrating a ‘‘peel-back’’ sign during arthroscopy 32
- The arm is released from traction and brought into an abducted/externally rotated position. The authors noted that in cases of a positive peel-back sign (i.e., not present in normal shoulders during an arthroscopic examination), the biceps anchor assumes a more vertical and posterior angle that is dynamically visible
Type 3 shoulder labrum tear
- Surgical treatment: SLAP repair versus resection
- The bucket-handle tear of the superior labrum is resected, with (rarely) additional repair of the SLAP complex (rare) if needed
Type 4 shoulder labrum tear
Surgical treatment:
- IF < 50% of the biceps tendon is affected, consider SLAP repair/resection
- IF > 50% of the biceps tendon is affected, perform tenotomy/tenodesis
Type 5 shoulder labrum tear
- Surgical treatment: Bankart repair plus SLAP repair
Type 6 shoulder labrum tear
- Surgical treatment: SLAP repair versus resection
Type 7 shoulder labrum tear
- Surgical treatment: Suture/anchor fixation of anterosuperior labrum plus SLAP repair
Type 8 shoulder labrum tear
- Surgical treatment: SLAP repair versus biceps tenotomy/tenodesis; gentle debridement of any cartilage/chondral unstable flap
SLAP repair technique
Multiple SLAP repair techniques have been previously described. Also, a wide array of implant options are available depending on surgeon preference. Previous authors have advocated for the use of simple versus mattress sutures and the option for knotless fixation devices to minimize the risk of having a bulky knot create symptoms postoperatively 33.
After probing to confirm the diagnosis of a shoulder labrum tear, a shaver can be used to resect unstable flaps of tissue that are deemed irreparable. Glenoid neck preparation is with a tissue elevator, rasp, and/or shaver instrument. The Neviaser portal is often utilized and established under direct visualization once confirming the appropriate trajectory are achieved. The determination of appropriate anchor placement depends on the predominant region of instability regarding the superior labral-biceps tendon complex.
Shoulder labrum tear rehab
Weeks 0 to 4 to 6 postop
- Sling immobilization until 4 weeks postop
- Early shoulder pendulum exercises, periscapular muscle activation exercises
- Passive and active-assist forward elevation encouraged, may progress limitations depending on surgeon preference
- Avoid extremes of abduction and external rotation
Weeks 4 to 6 postop
- Begin incorporation of active ROM (range of motion)
- Avoid extremes of abduction and external rotation
Weeks 6 to 12 postop
- Functional exercise and light strengthening can be progressively incorporated
- OK to begin biceps resistance exercises beyond 6-8 weeks postop
- Resisted elbow flexion, resisted forearm supination
Week 12 and beyond
- Advance strength and ROM, sport-specific
- Typical return to sport around 6 months
Labrum tear shoulder recovery time
At first, the repair needs to be protected while the labrum heals. To keep your arm from moving, you will most likely use a sling for 2 to 4 weeks after surgery. How long you require a sling depends upon the severity of your injury.
Once the initial pain and swelling has settled down, your doctor will start you on a physical therapy program that is tailored specifically to you and your injury.
In general, a therapy program focuses first on flexibility. Gentle stretches will improve your range of motion and prevent stiffness in your shoulder. As healing progresses, exercises to strengthen the shoulder muscles and the rotator cuff will gradually be added to your program. This typically occurs 4 to 6 weeks after surgery.
Your doctor will discuss with you when it is safe to return to sports activity. In general, throwing athletes can return to early interval throwing 3 to 4 months after surgery.
Although Level I and II studies in the literature are lacking regarding outcomes following arthroscopic type 2 shoulder labrum tear repairs, most studies report overall favorable results and good outcomes in the appropriately selected patients 34. A number of authors report good results in athletes, including those with sport-specific overhead demand requirements 35.
Inferior outcomes have been demonstrated in the literature following revision arthroscopic SLAP repairs and in high-level (i.e. professional) overhead athletes 36. Professional baseball pitchers demonstrate relatively inferior outcomes in terms of return to play and return to prior performance level. In fact, superior outcomes have been reported in this particular subset of athletic patients following non-surgical management alone 31.
Risk factors for revision surgery are critical in discussing overall patient expectations and discussing the risks of continued pain, stiffness, dysfunction, and the potential need for further surgery in the future. A 2017 level III case-control study highlighted the potential risk factors for revision surgery following SLAP repair, with the inclusion of nearly 5000 patients in the database query 37:
- Age greater than 40 years
- Female gender
- Obesity
- Smoking
- Presence of concomitant long head of the biceps tendinitis or tendinosis
- Odds ratio for revision surgery was 5.1 in the setting of long head of the biceps tendon tearing/fraying
- Odds ratio for revision surgery was 3.5 in the setting of long head of the biceps tendinitis alone.
Shoulder labrum tear prognosis
The majority of patients report improved shoulder strength and less pain after surgery for a shoulder labrum tear.
Because patients have varied health conditions, complete recovery time is different for everyone.
In cases of complicated injuries and repairs, full recovery may take several months. Although it can be a slow process, following your surgeon’s guidelines and rehabilitation plan is vital to a successful outcome.
- Andrews JR, Carson WG, McLeod WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. 1985 Sep-Oct;13(5):337-41[↩]
- Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy. 1990;6(4):274-9[↩][↩][↩]
- Morgan CD, Burkhart SS, Palmeri M, Gillespie M. Type II SLAP lesions: three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy. 1998 Sep;14(6):553-65[↩]
- Maffet MW, Gartsman GM, Moseley B. Superior labrum-biceps tendon complex lesions of the shoulder. Am J Sports Med. 1995 Jan-Feb;23(1):93-8[↩]
- Varacallo M, Mair SD. Superior Labrum Anterior Posterior (SLAP) Lesions. [Updated 2019 Feb 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538284[↩][↩][↩]
- Zhang AL, Kreulen C, Ngo SS, Hame SL, Wang JC, Gamradt SC. Demographic trends in arthroscopic SLAP repair in the United States. Am J Sports Med. 2012 May;40(5):1144-7[↩]
- Connor PM, Banks DM, Tyson AB, Coumas JS, D’Alessandro DF. Magnetic resonance imaging of the asymptomatic shoulder of overhead athletes: a 5-year follow-up study. Am J Sports Med. 2003 Sep-Oct;31(5):724-7[↩]
- Mathew CJ, Lintner DM. Superior Labral Anterior to Posterior Tear Management in Athletes. Open Orthop J. 2018;12:303-313[↩][↩]
- Johannsen AM, Costouros JG. A Treatment-Based Algorithm for the Management of Type-II SLAP Tears. Open Orthop J. 2018;12:282-287[↩]
- Erickson BJ, Jain A, Abrams GD, Nicholson GP, Cole BJ, Romeo AA, Verma NN. SLAP Lesions: Trends in Treatment. Arthroscopy. 2016 Jun;32(6):976-81[↩][↩]
- Waterman BR, Cameron KL, Hsiao M, Langston JR, Clark NJ, Owens BD. Trends in the diagnosis of SLAP lesions in the US military. Knee Surg Sports Traumatol Arthrosc. 2015 May;23(5):1453-9[↩]
- Ilahi OA, Labbe MR, Cosculluela P. Variants of the anterosuperior glenoid labrum and associated pathology. Arthroscopy. 2002 Oct;18(8):882-6[↩]
- Kim TK, Queale WS, Cosgarea AJ, McFarland EG. Clinical features of the different types of SLAP lesions: an analysis of one hundred and thirty-nine cases. J Bone Joint Surg Am. 2003 Jan;85-A(1):66-71[↩]
- Anatomy, histology, and vascularity of the glenoid labrum. An anatomical study. Cooper DE, Arnoczky SP, O’Brien SJ, Warren RF, DiCarlo E, Allen AA. J Bone Joint Surg Am. 1992 Jan; 74(1):46-52.[↩]
- Diagnosis and management of superior labral anterior posterior tears in throwing athletes. Knesek M, Skendzel JG, Dines JS, Altchek DW, Allen AA, Bedi A. Am J Sports Med. 2013 Feb; 41(2):444-60.[↩]
- Kanatli U, Ozturk BY, Bolukbasi S. Anatomical variations of the anterosuperior labrum: prevalence and association with type II superior labrum anterior-posterior (SLAP) lesions. J Shoulder Elbow Surg. 2010;19:1199–1203[↩][↩]
- Cooper DE, Arnoczky SP, O’Brien SJ, Warren RF, DiCarlo E, Allen AA. Anatomy, histology, and vascularity of the glenoid labrum. An anatomical study. J Bone Joint Surg Am. 1992;74:46–52[↩][↩]
- Knesek M, Skendzel JG, Dines JS, Altchek DW, Allen AA, Bedi A. Diagnosis and management of superior labral anterior posterior tears in throwing athletes. Am J Sports Med. 2013;41:444–460[↩][↩]
- Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part I: pathoanatomy and biomechanics. Arthroscopy. 2003 Apr;19(4):404-20[↩]
- Kuhn JE, Lindholm SR, Huston LJ, Soslowsky LJ, Blasier RB. Failure of the biceps superior labral complex: a cadaveric biomechanical investigation comparing the late cocking and early deceleration positions of throwing. Arthroscopy. 2003 Apr;19(4):373-9[↩]
- Clavert P, Bonnomet F, Kempf JF, Boutemy P, Braun M, Kahn JL. Contribution to the study of the pathogenesis of type II superior labrum anterior-posterior lesions: a cadaveric model of a fall on the outstretched hand. J Shoulder Elbow Surg. 2004 Jan-Feb;13(1):45-50[↩]
- Aydin N, Sirin E, Arya A. Superior labrum anterior to posterior lesions of the shoulder: Diagnosis and arthroscopic management. World J Orthop. 2014;5(3):344–350. Published 2014 Jul 18. doi:10.5312/wjo.v5.i3.344 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4095028[↩]
- Clavert P. Glenoid labrum pathology. Orthop Traumatol Surg Res. 2015 Feb;101(1 Suppl):S19-24[↩]
- Popp D, Schöffl V. Superior labral anterior posterior lesions of the shoulder: Current diagnostic and therapeutic standards. World J Orthop. 2015 Oct 18;6(9):660-71[↩]
- Brockmeyer M, Tompkins M, Kohn DM, Lorbach O. SLAP lesions: a treatment algorithm. Knee Surg Sports Traumatol Arthrosc. 2016 Feb;24(2):447-55[↩][↩][↩]
- Ben Kibler W, Sciascia AD, Hester P, Dome D, Jacobs C. Clinical utility of traditional and new tests in the diagnosis of biceps tendon injuries and superior labrum anterior and posterior lesions in the shoulder. Am J Sports Med. 2009 Sep;37(9):1840-7[↩][↩][↩][↩]
- Holtby R, Razmjou H. Accuracy of the Speed’s and Yergason’s tests in detecting biceps pathology and SLAP lesions: comparison with arthroscopic findings. Arthroscopy. 2004 Mar;20(3):231-6[↩]
- Meserve BB, Cleland JA, Boucher TR. A meta-analysis examining clinical test utility for assessing superior labral anterior posterior lesions. Am J Sports Med. 2009 Nov;37(11):2252-8.[↩]
- Ebinger N, Magosch P, Lichtenberg S, Habermeyer P. A new SLAP test: the supine flexion resistance test. Arthroscopy. 2008 May;24(5):500-5[↩]
- Pandya NK, Colton A, Webner D, Sennett B, Huffman GR. Physical examination and magnetic resonance imaging in the diagnosis of superior labrum anterior-posterior lesions of the shoulder: a sensitivity analysis. Arthroscopy. 2008 Mar;24(3):311-7[↩]
- Fedoriw WW, Ramkumar P, McCulloch PC, Lintner DM. Return to play after treatment of superior labral tears in professional baseball players. Am J Sports Med. 2014 May;42(5):1155-60[↩][↩]
- Burkhart SS, Morgan CD. The peel-back mechanism: its role in producing and extending posterior type II SLAP lesions and its effect on SLAP repair rehabilitation. Arthroscopy. 1998 Sep;14(6):637-40[↩]
- Tennent D, Pearse E. A Percutaneous Knotless Technique for SLAP Repair. Arthrosc Tech. 2016 Feb;5(1):e33-5[↩]
- Neri BR, Vollmer EA, Kvitne RS. Isolated type II superior labral anterior posterior lesions: age-related outcome of arthroscopic fixation. Am J Sports Med. 2009 May;37(5):937-42[↩]
- Neuman BJ, Boisvert CB, Reiter B, Lawson K, Ciccotti MG, Cohen SB. Results of arthroscopic repair of type II superior labral anterior posterior lesions in overhead athletes: assessment of return to preinjury playing level and satisfaction. Am J Sports Med. 2011 Sep;39(9):1883-8[↩]
- Gorantla K, Gill C, Wright RW. The outcome of type II SLAP repair: a systematic review. Arthroscopy. 2010 Apr;26(4):537-45[↩]
- Taylor SA, Degen RM, White AE, McCarthy MM, Gulotta LV, O’Brien SJ, Werner BC. Risk Factors for Revision Surgery After Superior Labral Anterior-Posterior Repair: A National Perspective. Am J Sports Med. 2017 Jun;45(7):1640-1644[↩]





{kind=link}