What is leptomeningeal carcinomatosis
Leptomeningeal carcinomatosis also known as “leptomeningeal metastasis” or “carcinomatosis meningitis,” is a serious problem that may occur in cancer in which cancer cells spread from the original (primary) tumor to the meninges (thin layers of tissue that cover and protect the brain and spinal cord) 1. Leptomeningeal carcinomatosis is involvement by cancer of pia and arachnoid matter of the brain with the subarachnoid space in between. Studies have shown that both solid tumors, including brain tumors and hematological cancers, can metastasize to involve the leptomeninges. Leptomeningeal carcinomatosis is an uncommon and late complication seen in 5% to 8% of cases of solid tumors and 5% to 15% of cases of hematological cancers 1. Since leptomeningeal carcinomatosis is a late-stage, metastatic complication of various cancer types, it is classified as stage 4 disease. Additionally, it implies a poor prognosis and limited treatment options 2.
About 110,000 new cases of leptomeningeal carcinomatosis are diagnosed each year in the United States. The true incidence of leptomeningeal carcinomatosis is difficult to determine, as this condition is usually underdiagnosed during a gross and microscopic examination at autopsy. The incidence varies among different cancer types. Among breast cancer patients, it ranges between 5% and 8%, up to 9% to 25% in lung cancer and up to 30% in melanomas. Some authors have reported incidence rates of 6% to 18% for melanomas. The incidence of leptomeningeal carcinomatosis is increasing due to improved survival rates secondary to the improved systemic control of the disease, better imaging and diagnostic modalities, and treatment with therapies that do not cross the blood-brain barrier (BBB). The longer patients live with systemic cancer, the higher the chances of tumor spread and seeding of the leptomeninges. The median time to diagnosis of leptomeningeal carcinomatosis after diagnosis of a solid tumor ranges between 1.2 and 2 years; this time is about 11 months in hematologic cancers 3.
Leptomeningeal carcinomatosis is best managed by a multidisciplinary team that should include hospice and palliative care nurses. The prognosis for most patients is poor and thus the quality of life should be improved. Pain control and support measures should be provided. No aggressive studies or treatments are warranted for most patients as death is usually imminent 4.
The use of the newer biological agents should be used with good judgment as they only prolong the life by a few weeks or months; on the other hand, they burden the family with enormous costs of the medications.
The reported median survival is 7 months for patients with leptomeningeal carcinomatosis from breast cancers, 4 months for patients with leptomeningeal carcinomatosis from small-cell lung carcinomas, and 3.6 months for patients with leptomeningeal carcinomatosis from melanomas 5. However, with new chemotherapeutic regimens longer survival rates have been reported.
Without therapy, most patients survive 4-6 weeks, with death occurring because of progressive neurologic dysfunction.
With therapy, most patients die from the systemic complications of their cancer rather than the neurologic complications of leptomeningeal carcinomatosis.
Fixed focal neurologic deficits (eg, cranial-nerve palsies) generally do not improve, but encephalopathies can improve dramatically with treatment.
Leptomeningeal carcinomatosis key facts
- Leptomeningeal carcinomatosis continues to be a diagnostic challenge due to limited and varying sensitivities of diagnostic modalities used. Symptoms may be ignored initially in sick patients with metastatic disease, leading to a delay in diagnosis as well.
- Prognosis remains poor despite advances in therapies due to limited evidence from studies and variable/limited response to treatment which is limited by toxicity.
- Understanding the molecular mechanisms of metastasis to the brain may help find/evaluate better, focused therapies targeting tumor-specific molecular markers across different tumor types.
Leptomeningeal carcinomatosis causes
Most solid tumors are known to cause leptomeningeal carcinomatosis, but the most common solid tumors that involve the leptomeninges are breast, lung, and melanoma, gastrointestinal, and primary central nervous system tumors 1. Metastatic breast cancer is the most common etiology, followed by lung cancer (mainly small cell lung cancer), which is followed by melanoma 6.
It is postulated that cancerous cells spread to leptomeninges via several different mechanisms, including direct seeding from brain parenchyma, dura mater (not protected by BBB) and bone, endoneurial/perineural invasion, and hematogenous seeding (especially via venous plexi). Some studies also indicate a correlation between neurosurgical interventions like cerebellar metastasis resection and the opening of ventricles with leptomeningeal carcinomatosis. Another possible entry point is through fenestrated endothelium of choroid plexus which allows selective solute transport in contrast to the blood-brain barrier (BBB). One study suggests upregulation of complement component 3 by cancer cells in cerebrospinal fluid (CSF) which in turn causes interruption of blood-brain barrier (BBB) and leads to penetration of plasma growth factors into the CSF. One such plasma growth factor implicated in the process is vascular endothelial growth factor (VEGF) which promotes tumor angiogenesis and endothelial cell proliferation. It is also an important drug target. There are different patterns of involvement of the leptomeninges, but typically basal cisterns, posterior fossa, and cauda equina are affected.
Leptomeningeal carcinomatosis symptoms
Signs and symptoms may initially be nonspecific and hence may not prompt an evaluation in a sick patient with metastatic cancer. Of note, a minority of patients may be diagnosed incidentally and may be asymptomatic at diagnosis. However, some signs and symptoms may indicate the location of the involvement.
Meningeal symptoms are the first manifestations in some patients (pain and seizures are the most common presenting complaints) and can include the following:
- Headaches (usually associated with nausea, vomiting, light-headedness)
- Gait difficulties from weakness or ataxia
- Memory problems
- Incontinence
- Sensory abnormalities
A wide range of CNS signs and symptoms have been reported, including but not limited to the following:
- Cerebral: headache, confusion, cognitive impairment, psychiatric disorders, seizures.
- Posterior fossa: cranial nerve (CN) deficits especially cranial nerve 6, 7 and 8 (diplopia, facial weakness, hearing loss), ataxia.
- Vascular: ischemia and infarction.
- Spinal cord: limb weakness, dermatomal sensory loss, radicular pain, bladder, and bowel dysfunction.
- Inflammatory reactions: Tumor cells may lead to inflammatory reactions and disrupt CSF flow causing obstructive or communicating hydrocephalus and presenting as nausea, vomiting, positional headaches, and somnolence.
Leptomeningeal carcinomatosis diagnosis
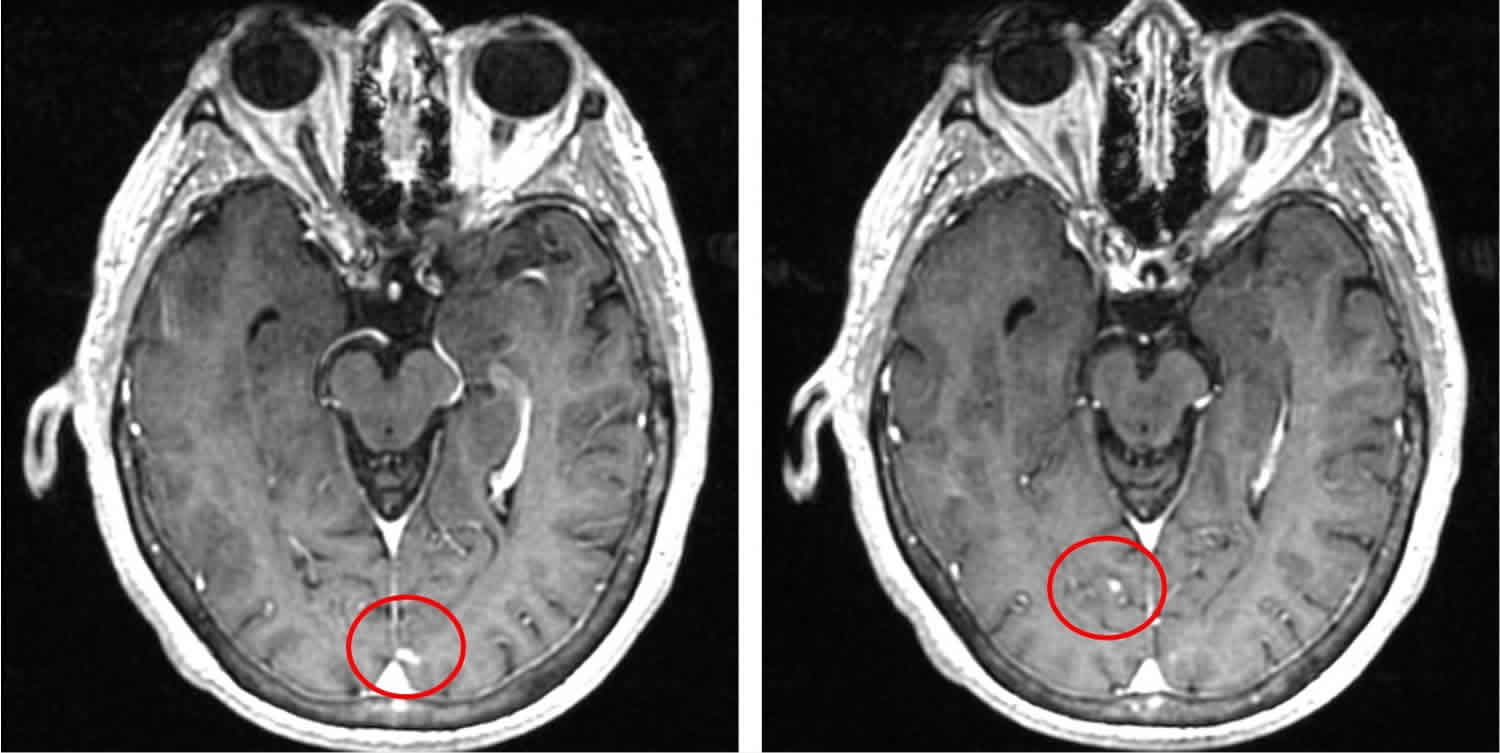
Diagnosis of leptomeningeal carcinomatosis is often challenging due to the low sensitivity of different diagnostic modalities. The initial diagnostic evaluation includes at least a high-quality MRI of brain and spine and CSF studies. MRI with gadolinium contrast has a sensitivity of 70% and specificity of 77% to 100%. It may detect leptomeningeal enhancement, hydrocephalus, subependymal nodules/deposits (which may also be seen on cerebral convexities), cisterns, and on tentorium. Spinal cord involvement may show patchy enhancement of nerve roots and extramedullary nodules.
If safe, then diagnostic evaluation should be furthered by a lumbar puncture. CSF studies in case of leptomeningeal carcinomatosis usually shows mild pleocytosis, hypoglycorrhachia (usually less than 60 mg/dL), elevated protein (greater than 45 mg/dL). If the glucose levels are very low, then infectious etiologies must be ruled out. In 50% to 70% of cases, it may show elevated opening pressure (greater than 150 mm) as well. False negative cytology results are common, and a study shows CSF cytology can have false negative results of up to 36% if samples are refrigerated for 48 hours. These false-negative results can be minimized by securing large volume (10 mL) of CSF for cytology, expediting sample processing without additional storage, and obtaining CSF from cisterns or lumbar region or a site of known leptomeningeal involvement. In most cases, positive CSF studies and suggestive radiographic findings are enough to make a diagnosis, but a negative lumbar puncture should be followed by at least one additional lumbar puncture, especially if there is high clinical suspicion. The sensitivity of cytology is 50% to 60% after the first lumbar puncture and approaches 85% to 90% with the second collection.
CSF tumor markers also have been evaluated as an aid in diagnosis, but the relative lack of sensitivity and specificity limits this modality from routine use. Nonetheless, this method may be used in certain tumors if all other workup is negative. Certain tumor markers that can be tested include CEA in adenocarcinomas, alpha-fetoprotein in hepatocellular and testicular carcinomas, and beta-human chorionic gonadotropin in choriocarcinomas and testicular carcinomas. There is also some data on determining vascular endothelial growth factor (VEGF) levels in CSF, but further research is yet to be conducted on the topic.
Recently, cell-free DNA in CSF has been evaluated to detect tumor-specific somatic mutations through next-generation sequencing which may be helpful in detecting certain tumors.
Rarely, CSF flow studies/ventriculography using Indium 111-DTPA or Technetium-99m labeled albumin may be used to identify CSF flow.
If there is no active systemic disease, then systemic restaging is advised to guide diagnosis and therapy.
Leptomeningeal carcinomatosis treatment
Leptomeningeal carcinomatosis is incurable and difficult to treat. The prognosis of leptomeningeal carcinomatosis remains poor despite advances in therapy. There is a lack of randomized clinical trials, and treatment methods are derived from lower evidence studies or clinical expert opinions. Treatment focuses on improving neurologic deficits, quality of life, and prolonging survival while minimizing toxicity. Commonly, radiation is applied to bulky or symptomatic anatomical lesions followed by intrathecal chemotherapy. CSF flow obstruction is relieved by surgical interventions; however, surgery has a very marginal role in the management of leptomeningeal carcinomatosis. Systemic therapy can be added to the regimen to treat the primary tumor and potentially prolong survival.
Palliative and supportive treatment are provided as needed with anti-depressants, anxiolytics, and opioid and non-opioid agents. Psychostimulants should always be provided in addition to pursuing treatment of the disease/cancer.
Medical therapy
Intrathecal chemotherapy
Intrathecal chemotherapy has shown a survival benefit in retrospective studies. The agent used commonly includes methotrexate (MTX), cytarabine, thiotepa, and sustained release liposomal cytarabine. Studies have shown superior efficacy of sustained-release cytarabine compared to methotrexate.
Aseptic/chemical meningitis is a common complication which can be managed with steroids. Infectious meningitis (commonly implicated organism is Staphylococcus epidermidis), seizure, myelosuppression, leukoencephalopathy are some other complications encountered.
Systemic chemotherapy
Numerous studies have shown that systemic chemotherapy has improved survival. It bypasses the administration issues of intrathecal (IT) chemotherapy, treats the primary tumor, and also is effective in treating nodular type leptomeningeal carcinomatosis. Blood-brain barrier (BBB) is disrupted in leptomeningeal carcinomatosis hence systemic chemotherapy has been demonstrated to achieve therapeutic levels in CSF. Agents used include high-dose methotrexate (MTX), high-dose cytarabine, capecitabine (particularly for breast cancer), thiotepa, and temozolomide. There seems to be some promise in using etoposide in small cell lung cancer.
Targeted therapy
Bevacizumab and Dabrafenib (BRAF inhibitors) have been reported to demonstrate a response in leptomeningeal carcinomatosis from melanoma. Intrathecal trastuzumab in leptomeningeal carcinomatosis from HER-2 positive breast cancer also has shown some promise and a favorable adverse effect profile. There are several ongoing phase II trials on the subject. EGFR-mutant non-small cell lung cancer (NSCleptomeningeal carcinomatosis) has shown a response to erlotinib and gefitinib, but at higher doses, as they do not cross the blood-brain barrier (BBB) easily. There are ongoing trials of other tyrosine kinase inhibitors (TKIs) in leptomeningeal carcinomatosis from EGFR-mutant NSCleptomeningeal carcinomatosis that have shown promising results in terms of extended survival. Anaplastic lymphoma kinase (ALK) inhibitors are another class of drugs shown to be effective in leptomeningeal carcinomatosis from non-small-cell lung carcinoma with ALK rearrangements in ongoing trials.
Novel therapeutics
Immunotherapy is another novel treatment approach to leptomeningeal carcinomatosis. Agents like nivolumab, ipilimumab, and pembrolizumab have been studied and have shown some positive results. Intrathecal Interleukin -2 (IL-2) and intrathecal tumor-infiltrating lymphocyte (TIL) therapies also have been studied, but the data on these therapies is scant so far, and further trials are needed before these regimens can be considered in routine treatment.
Radiation therapy
- Indications: Radiation important for palliation of symptoms, especially in spinal involvement as it may alleviate pain. Sometimes it may relieve hydrocephalus and associated symptoms and facilitate administration of intrathecal (IT) chemotherapy. However, a retrospective study has failed to show any survival benefit. Eradication of tumor craniospinal radiation is required which carries very high systemic and CNS toxicities and risks myelosuppression and other complications. Given poor prognosis, it is considered technically impractical.
- Dosage: Whole brain radiotherapy is usually given at a dose of 30 to 40 grays (Gy) in 2 to 3 Gy fractions. Focal radiotherapy is done for spinal lesions.
- Adverse effects: Cognitive impairment, somnolence, and late leukoencephalopathy when combined with IV or intrathecal (IT) chemotherapy.
Surgical therapy
- Indications and Techniques: Surgical procedures play a very minute role in the management of this disease. Ventriculoperitoneal (VP) shunt or intraventricular catheters can be placed for relieving symptomatic hydrocephalus and delivery of intrathecal chemotherapy respectively. In very rare instances, resection of bulky CNS disease or biopsy of leptomeninges in the previously unknown primary may be done. However, there is no known survival benefit from surgical procedures.
- Adverse Effects: Adverse effects include infection, shunt displacement, and catheter failure.
Leptomeningeal carcinomatosis prognosis
Prognosis remains grim in patients with leptomeningeal carcinomatosis. The time from diagnosis to death is about 4 to 6 weeks if left untreated. With treatment, overall survival is approximately 2 to 4 months. Patients with breast cancer have shown better prognosis and response to therapy with a median survival of 5 to 7 months compared to other solid tumors like melanoma and lung cancer with a median survival of approximately 4 months. Favorable prognostic factors include Karnofsky Performance Status (KPS) greater than 70, normal CSF flow, absence of major neurologic deficits, active treatment, chemosensitivity of primary cancer, and CSF protein less than 50 mg/dL at the time of diagnosis. According to the US National Comprehensive Cancer Network, KPS (Karnofsky Performance Status) less than 60, high CNS disease burden, extensive systemic disease with few treatment options, severe neurologic impairment, and encephalopathy are markers of poor prognosis. Karnofsky Performance Status (KPS) is a standard way of measuring the ability of cancer patients to perform ordinary tasks. The KPS scores range from 0 to 100. A higher score means the patient is better able to carry out daily activities. KPS may be used to determine a patient’s prognosis, to measure changes in a patient’s ability to function, or to decide if a patient could be included in a clinical trial.
- Batool A, Kasi A. Leptomeningeal Carcinomatosis. [Updated 2019 Jun 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499862[↩][↩][↩]
- Lasocki A, Phillips KA, Drummond K, Caspersz L. Unexpected diagnosis of spinal leptomeningeal metastatic disease on MRI myelography. J Clin Neurosci. 2019 May 16[↩]
- Franzoi MA, Hortobagyi GN. Leptomeningeal carcinomatosis in patients with breast cancer. Crit. Rev. Oncol. Hematol. 2019 Mar;135:85-94.[↩]
- Kim H, Lee EM. A Retrospective Analysis of the Clinical Outcomes of Leptomeningeal Metastasis in Patients with Solid Tumors. Brain Tumor Res Treat. 2018 Oct;6(2):54-59.[↩]
- Leptomeningeal Carcinomatosis. https://emedicine.medscape.com/article/1156338-overview[↩]
- Umezawa Y, Shirotake S, Kaneko G, Nishimoto K, Okada Y, Uchino A, Yasuda M, Oyama M. Meningeal carcinomatosis from bladder cancer: A case report and review of the literature. Mol Clin Oncol. 2019 May;10(5):506-510.[↩]





{kind=link}