
What is Marburg virus
Marburg virus causes Marburg hemorrhagic fever — an illness marked by severe bleeding (hemorrhage), organ failure and, in many cases, death. Marburg virus is native to Africa, where sporadic outbreaks have occurred for decades. The reservoir host of Marburg virus is the African fruit bat, Rousettus aegyptiacus. Fruit bats infected with Marburg virus do not to show obvious signs of illness. Primates (including humans) can become infected with Marburg virus, and may develop serious disease with high mortality. Further study is needed to determine if other species may also host the Marburg virus. Humans can contract the Marburg virus from infected animals. After the initial transmission, the Marburg virus can spread from person to person through contact with body fluids or contaminated needles.
The Rousettus bat is a sighted, cave-dwelling bat widely distributed across Africa. Given the fruit bat’s wide distribution, more areas are potentially at risk for outbreaks of Marburg hemorrhagic fever than previously suspected. Marburg virus is not known to be native to other continents, such as North America.
Marburg hemorrhagic fever typically appears in sporadic outbreaks throughout Africa; laboratory confirmed cases have been reported in Uganda, Zimbabwe, the Democratic Republic of the Congo, Kenya, Angola, and South Africa. Many of the outbreaks started with male mine workers working in bat-infested mines. The virus is then transmitted within their communities through cultural practices, under-protected family care settings, and under-protected health care staff. It is possible that sporadic, isolated cases occur as well, but go unrecognized.
Cases of Marburg hemorrhagic fever have occurred outside Africa, such as during the 1967 outbreak, but are infrequent. Marburg virus was first recognized in 1967, when outbreaks of hemorrhagic fever occurred simultaneously in laboratories in Marburg and Frankfurt, Germany and in Belgrade, Yugoslavia (now Serbia). Thirty-one people became ill, initially laboratory workers followed by several medical personnel and family members who had cared for them. Seven deaths were reported. The first people infected had been exposed to imported African green monkeys or their tissues while conducting research. One additional case was diagnosed retrospectively.
In 2008, a Dutch tourist developed Marburg hemorrhagic fever after returning to the Netherlands from Uganda, and subsequently died. Also in 2008, an American traveler developed Marburg hemorrhagic fever after returning to the US from Uganda and recovered. Both travelers had visited a well-known cave inhabited by fruit bats in a national park.
No drug has been approved to treat Marburg virus. People diagnosed with Marburg virus receive supportive care and treatment for complications. Scientists are coming closer to developing vaccines for these deadly diseases.
Table 1. Known cases and outbreaks of Marburg hemorrhagic fever in chronological order
| Year(s) | Country | Apparent or suspected origin | Reported number of human cases | Reported number (%) of deaths among cases | Situation |
|---|---|---|---|---|---|
| 1967 | Germany and Yugoslavia | Uganda | 31 | 7 (23%) | Simultaneous outbreaks occurred in laboratory workers handling African green monkeys imported from Uganda1. In addition to the 31 reported cases, an additional primary case was retrospectively serologically diagnosed 1. |
| 1975 | Johannesburg, South Africa | Zimbabwe | 3 | 1 (33%) | A man with a recent travel history to Zimbabwe was admitted to hospital in South Africa. Infection spread from the man to his traveling companion and a nurse at the hospital. The man died, but both women were given vigorous supportive treatment and eventually recovered 2. |
| 1980 | Kenya | Kenya | 2 | 1 (50%) | Recent travel history included a visit to Kitum Cave in Kenya’s Mount Elgon National Park. Despite specialized care in Nairobi, the male patient died. A doctor who attempted resuscitation developed symptoms 9 days later but recovered 3. |
| 1987 | Kenya | Kenya | 1 | 1 (100%) | A 15-year-old Danish boy was hospitalized with a 3-day history of headache, malaise, fever, and vomiting. Nine days prior to symptom onset, he had visited Kitum Cave in Mount Elgon National Park. Despite aggressive supportive therapy, the patient died on the 11th day of illness. No further cases were detected 4. |
| 1990 | Russia | Russia | 1 | 1 (100%) | Laboratory contamination 5. |
| 1998-2000 | Democratic Republic of Congo (DRC) | Durba, DRC | 154 | 128 (83%) | Most cases occurred in young male workers at a gold mine in Durba, in the north-eastern part of the country, which proved to be the epicentre of the outbreak. Cases were subsequently detected in the neighboring village of Watsa 6. |
| 2004-2005 | Angola | Uige Province, Angola | 252 | 227 (90%) | Outbreak believed to have begun in Uige Province in October 2004. Most cases detected in other provinces have been linked directly to the outbreak in Uige 7. |
| 2007 | Uganda | Lead and gold mine in Kamwenge District, Uganda | 4 | 1 (25%) | Small outbreak, with 4 cases in young males working in a mine. To date, there have been no additional cases identified 8. |
| 2008 | USA ex Uganda | Cave in Maramagambo forest in Uganda, at the southern edge of Queen Elizabeth National Park | 1 | 0 (0) | A U.S traveler returned from Uganda in January 2008. The patient developed illness 4 days after returning, was hospitalized, discharged and fully recovered. The patient was retrospectively diagnosed with Marburg virus infection 9. |
| 2008 | Netherlands ex Uganda | Cave in Maramagambo forest in Uganda, at the southern edge of Queen Elizabeth National Park | 1 | 1 (100%) | A 40-year-old Dutch woman with a recent history of travel to Uganda was admitted to hospital in the Netherlands. Three days prior to hospitalization, the first symptoms (fever, chills) occurred, followed by rapid clinical deterioration. The woman died on the 10th day of the illness 10. |
| 2012 | Uganda | Kabale | 15 | 4 (27%) | Testing at CDC/UVRI identified a Marburg virus disease outbreak in the districts of Kabale, Ibanda, Mbarara, and Kampala over a 3 week time period 11. |
| 2014 | Uganda | Kampala | 1* | 1 | Investigations are on-going 12. Testing conducted at CDC/UVRI |
Footnote: *Numbers reflect laboratory confirmed cases only.
[Source 13 ]Figure 1. Marburg virus

Figure 2. Marburg virus disease outbreak distribution map
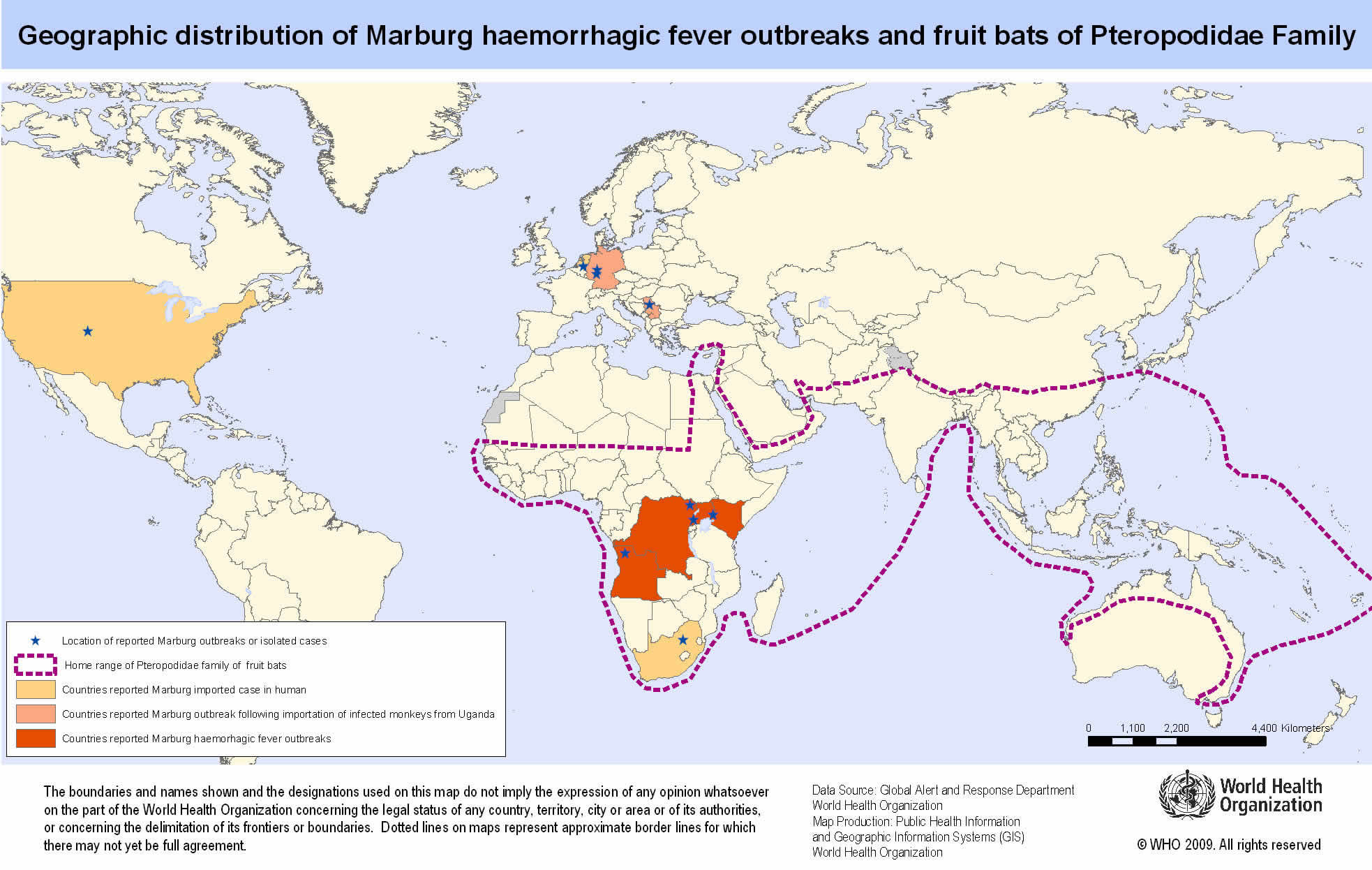
Countries reporting outbreaks of Marburg Hemorrhagic Fever
- Angola
- DR Congo
- Germany
- Kenya
- Serbia
- South Africa
- Uganda
Marburg virus transmission
Marburg virus has been found in monkeys, chimps and fruit bats in Africa. It is unknown how Marburg virus first transmits from its animal host to humans; however, for the 2 cases in tourists visiting Uganda in 2008, unprotected contact with infected bat feces or aerosols are the most likely routes of infection. After this initial crossover of Marburg virus from host animal to humans, transmission occurs through person-to-person contact. This may happen in several ways: direct contact to droplets of body fluids from infected persons, or contact with equipment and other objects contaminated with infectious blood or tissues. Marburg virus spreads through human-to-human transmission via direct contact (through broken skin or mucous membranes) with the blood, secretions, organs or other bodily fluids of infected people, and with surfaces and materials (e.g. bedding, clothing) contaminated with these fluids.
In previous outbreaks, persons who have handled infected non-human primates or have come in direct contact with their fluids or cell cultures have become infected. Spread of the Marburg virus between humans has occurred in close environments and direct contacts. A common example is through caregivers in the home or in a hospital (nosocomial transmission).
Marburg virus transmission from animals to humans
Experts suspect that both viruses are transmitted to humans through an infected animal’s bodily fluids. Examples include:
- Blood. Butchering or eating infected animals can spread the viruses. Scientists who have operated on infected animals as part of their research have also contracted the virus.
- Waste products. Tourists in certain African caves and some underground mine workers have been infected with the Marburg virus, possibly through contact with the feces or urine of infected bats.
Marburg virus transmission from person to person
Infected people typically don’t become contagious until they develop symptoms. Family members are often infected as they care for sick relatives or prepare the dead for burial.
Medical personnel can be infected if they don’t use protective gear, such as surgical masks and gloves.
There’s no evidence that Marburg virus can be spread via insect bites.
Risk of Marburg virus exposure
For most people, the risk of getting Marburg hemorrhagic fever is low. The risk increases if you:
- Travel to Africa. You’re at increased risk if you visit or work in areas where Ebola virus or Marburg virus outbreaks have occurred.
- Conduct animal research. People are more likely to contract the Ebola or Marburg virus if they conduct animal research with monkeys imported from Africa or the Philippines.
- Provide medical or personal care. Family members are often infected as they care for sick relatives. Medical personnel also can be infected if they don’t use protective gear, such as surgical masks and gloves.
- Prepare people for burial. The bodies of people who have died of Ebola or Marburg hemorrhagic fever are still contagious. Helping prepare these bodies for burial can increase your risk of developing the disease.
People who have close contact with African fruit bats, humans patients, or non-human primates infected with Marburg virus are at risk.
Historically, the people at highest risk include family members and hospital staff who care for patients infected with Marburg virus and have not used proper barrier nursing techniques. Particular occupations, such as veterinarians and laboratory or quarantine facility workers who handle non-human primates from Africa, may also be at increased risk of exposure to Marburg virus.
Exposure risk can be higher for travelers visiting endemic regions in Africa, including Uganda and other parts of central Africa, and have contact with fruit bats, or enter caves or mines inhabited by fruit bats.
Marburg virus prevention
Prevention focuses on avoiding contact with the viruses. The following precautions can help prevent infection and spread of Ebola and Marburg.
- Avoid areas of known outbreaks. Before traveling to Africa, find out about current epidemics by checking the Centers for Disease Control and Prevention website.
- Wash your hands frequently. As with other infectious diseases, one of the most important preventive measures is frequent hand-washing. Use soap and water, or use alcohol-based hand rubs containing at least 60 percent alcohol when soap and water aren’t available.
- Avoid bush meat. In developing countries, avoid buying or eating the wild animals, including nonhuman primates, sold in local markets.
- Avoid contact with infected people. In particular, caregivers should avoid contact with an infected person’s body fluids and tissues, including blood, semen, vaginal secretions and saliva. People with Ebola or Marburg are most contagious in the later stages of the disease.
- Follow infection-control procedures. If you’re a health care worker, wear protective clothing, such as gloves, masks, gowns and eye shields. Keep infected people isolated from others. Dispose of needles and sterilize other instruments.
- Don’t handle remains. The bodies of people who have died of Ebola or Marburg disease are still contagious. Specially organized and trained teams should bury the remains, using appropriate safety equipment.
Marburg virus vaccine development
Scientists are working on a variety of vaccines that would protect people from Ebola and Marburg viruses. Some of the results have been promising, but further testing is needed.
Marburg virus symptoms
After an incubation period of 5-10 days, symptom onset is sudden and marked by fever, chills, headache, and myalgia. Around the fifth day after the onset of symptoms, a maculopapular rash, most prominent on the trunk (chest, back, stomach), may occur. Nausea, vomiting, chest pain, a sore throat, abdominal pain, and diarrhea may then appear. Symptoms become increasingly severe and can include jaundice, inflammation of the pancreas, severe weight loss, delirium, shock, liver failure, massive hemorrhaging, and multi-organ dysfunction.
Because many of the signs and symptoms of Marburg hemorrhagic fever are similar to those of other infectious diseases such as malaria or typhoid fever, clinical diagnosis of the disease can be difficult, especially if only a single case is involved.
The case-fatality rate for Marburg hemorrhagic fever is between 23-90%.
Marburg virus signs and symptoms typically begin abruptly within five to 10 days of infection with Marburg virus. Early signs and symptoms include:
- Fever
- Severe headache
- Joint and muscle aches
- Chills
- Weakness
Over time, symptoms become increasingly severe and may include:
- Nausea and vomiting
- Diarrhea (may be bloody)
- Red eyes
- Raised rash
- Chest pain and cough
- Sore throat
- Stomach pain
- Severe weight loss
- Bruising
- Bleeding, usually from the eyes, and when close to death, possible bleeding from the ears, nose and rectum
- Internal bleeding
Marburg virus complications
Marburg hemorrhagic fever leads to death for a high percentage of people who are affected. As the illness progresses, it can cause:
- Multiple organ failure
- Severe bleeding
- Jaundice
- Delirium
- Seizures
- Coma
- Shock
One reason the Marburg virus is so deadly is that it interferes with the immune system’s ability to mount a defense. But scientists don’t understand why some people recover from Marburg virus and others don’t.
For people who survive, recovery is slow. It may take months to regain weight and strength, and the viruses remain in the body for weeks. People may experience:
- Hair loss
- Sensory changes
- Liver inflammation (hepatitis)
- Weakness
- Fatigue
- Headaches
- Eye inflammation
- Testicular inflammation
Marburg virus diagnosis
Many of the signs and symptoms of Marburg hemorrhagic fever are similar to those of other more frequent infectious diseases, such as malaria or typhoid fever, making diagnosis of the disease difficult. This is especially true if only a single case is involved.
However, if a person has the early symptoms of Marburg hemorrhagic fever and there is reason to believe that Marburg hemorrhagic fever should be considered, the patient should be isolated and public health professionals notified. Samples from the patient can then be collected and tested to confirm infection.
Antigen-capture enzyme-linked immunosorbent assay (ELISA) testing, polymerase chain reaction (PCR), and IgM-capture ELISA can be used to confirm a case of Marburg hemorrhagic fever within a few days of symptom onset. Virus isolation may also be performed but should only be done in a high containment laboratory with good laboratory practices. The IgG-capture ELISA is appropriate for testing persons later in the course of disease or after recovery. In deceased patients, immunohistochemistry, virus isolation, or PCR of blood or tissue specimens may be used to diagnose Marburg hemorrhagic fever retrospectively.
Marburg virus treatment
There is no specific treatment for Marburg hemorrhagic fever. No antiviral medications have proved effective in treating infection with Marburg virus. Supportive hospital therapy should be utilized, which includes balancing the patient’s fluids and electrolytes, maintaining oxygen status and blood pressure, replacing lost blood and clotting factors, and treatment for any complicating infections.
Supportive hospital care includes:
- Providing fluids
- Maintaining blood pressure
- Providing oxygen as needed
- Replacing lost blood
- Treating other infections that develop
Experimental treatments are validated in non-human primates models, but have never been tried in humans.
- Feldmann H, Slenczka W, Klenk HD. Emerging and reemerging of filoviruses. Archives of Virology. 1996;11(Suppl.):77-100[↩]
- World Health Organization. Marburg virus disease – South Africa. Weekly Epidemiological RecordCdc-pdfExternal. 1975;50(12):124-125[↩]
- Smith DH, Johnson BK, Isaacson M, et al. Marburg-virus disease in Kenya. Lancet. 1982; 1(8276):816-820.[↩]
- Johnson ED, Johnson BK, Silverstein D, et al. Characterization of a new Marburg virus isolated from a 1987 fatal case in Kenya. Archives of Virology. 1996;11(Suppl):101-114[↩]
- Nikiforov VV, Turovskii IU, Kalinin PP, et al. A case of laboratory infection with Marburg fever. Zhurnal Mikrobiologii, Epidemiologii i Immunobiologii. 1994(3):104-106[↩]
- Bausch DG, Nichol ST, Muyembe-Tamfum JJ, et al. Marburg hemorrhagic fever associated with multiple genetic lineages of virus. New England Journal of Medicine. 2006;355:909-919[↩]
- Towner JS, Khristova ML, Sealy TK, et al. Marburgvirus genomics and association with a large hemorrhagic fever outbreak in Angola. Journal of Virology. 2006;80(13):6497-6516[↩]
- Adjemian J, Farnon EC, Tschioko F, et al. Outbreak of Marburg hemorrhagic fever among miners in Kamwenge and Ibanda districts, Uganda, 2007. Journal of Infectious Diseases. 2011; 204(Suppl 3):S796-S799[↩]
- Centers for Disease Control and Prevention. Imported case of Marburg hemorrhagic fever – Colorado, 2008. Morbidity and Mortality Weekly Report. 2009; 58(49):1377-1381[↩]
- Timen A, Koopmans M, Vossen A, et al. Response to Imported Case of Marburg Hemorrhagic Fever, the Netherlands. Emerging Infectious Diseases. 2009; 15(8):1171-1175.[↩]
- Albarino CG, Shoemaker T, Khristova ML, et al. Genomic analysis of filoviruses associated with four viral hemorrhagic fever outbreaks in Uganda and the Democratic Republic of the Congo in 2012. Virology. 2013;442(2):97-100.[↩]
- Uganda Ministry of Health. Press Release, Oct. 8, 2014[↩]
- Outbreaks Chronology: Marburg Hemorrhagic Fever. https://www.cdc.gov/vhf/marburg/outbreaks/chronology.html[↩]





{kind=link}