What is the MTHFR gene
The MTHFR gene which is short for methylenetetrahydrofolate reductase gene, provides instructions for making an enzyme called methylenetetrahydrofolate reductase. Methylenetetrahydrofolate reductase (MTHFR) enzyme plays a role in processing amino acids, the building blocks of proteins. Methylenetetrahydrofolate reductase (MTHFR) is important for a chemical reaction involving forms of the vitamin folate (also called vitamin B9). Specifically, methylenetetrahydrofolate reductase (MTHFR) enzyme converts a molecule called 5,10-methylenetetrahydrofolate to a molecule called 5-methyltetrahydrofolate. This reaction is required for the multistep process that converts the amino acid homocysteine to another amino acid, methionine. The body uses methionine to make proteins and other important compounds.
When there are mutations or variations in the MTHFR gene, it can lead to serious genetic disorders such as homocystinuria, anencephaly, spina bifida, and others. The MTHFR enzyme is critical for metabolizing one form of B vitamin, folate, into another. It is also part of the process that converts homocysteine into methionine, an important building block for many proteins. Homocysteine is a type of amino acid, a chemical your body uses to make proteins. Normally, folic acid and other B vitamins break down homocysteine and change it into other substances your body needs. There should then be very little homocysteine left in the bloodstream.
If you have an MTHFR mutation, your MTHFR gene may not work right. This may cause too much homocysteine to build up in the blood, leading to various health problems, including:
- Homocystinuria, a disorder that affects the eyes, joints, and cognitive abilities. It usually starts in early childhood.
- An increased risk of heart disease, stroke, high blood pressure, and blood clots
In addition, women with MTHFR mutations have a higher risk of having a baby with one of the following birth defects:
- Spina bifida, known as a neural tube defect. This is a condition in which the bones of the spine do not completely close around the spinal cord.
- Anencephaly, another type of neural tube defect. In this disorder, parts of the brain and/or skull may be missing or deformed.
If someone has increased levels of homocysteine, that means the body is not processing it properly. One cause of that could be a mutation in the MTHFR gene, causing homocystinuria. While at least seven unique MTHFR mutations have been found in people with homocystnuria, there are two relatively common DNA sequence variants, known as single nucleotide polymorphisms (SNPs), that are tested. The two MTHFR variants are called C677T and A1298C, and individuals can inherit one or both variants. These SNPs result in changes in the DNA (or mutations) that are associated with decreased MTHFR activity and increased homocysteine levels in the blood, which may increase the risk of premature cardiovascular disease (CVD), formation of inappropriate blood clots (thrombosis), and stroke.
Approximately 5-14% of the U.S. population is homozygous for C677T, meaning that they have two copies of it. There is some ethnic variability in the frequency, with the highest being in those of Mediterranean ancestry and the lowest in those of African ancestry.
The C677T variant results in a less active form of the MTHFR enzyme and reduced ability to process folate and homocysteine. When a person has two copies of the MTHFR C677T gene mutation (homozygous) or one copy of MTHFR C677T and one copy of A1298C (compound heterozygous), decreased MTHFR enzyme activity slows down the homocysteine-to-methionine conversion process and can lead to a buildup of homocysteine in the blood.
The increase in homocysteine is often mild to moderate but will vary from person to person depending upon the amount of MTHFR enzyme activity. Even if a person has two copies of the MTHFR mutation, that person may not develop high homocysteine levels since adequate folate intake can “cancel out” the effect of the MTHFR mutation.
Results of some studies suggest that high levels of homocysteine in the blood may contribute to risk of CVD by damaging blood vessel walls and promoting formation of plaque (atherosclerosis) and inappropriate blood clots. However, a direct link between homocysteine levels and cardiovascular disease or thrombotic risk has not been found.
You can reduce your homocysteine levels by taking folic acid or other B vitamins These can be taken as supplements or added through dietary changes. If you need to take folic acid or other B vitamins, your health care provider will recommend which option is best for you.
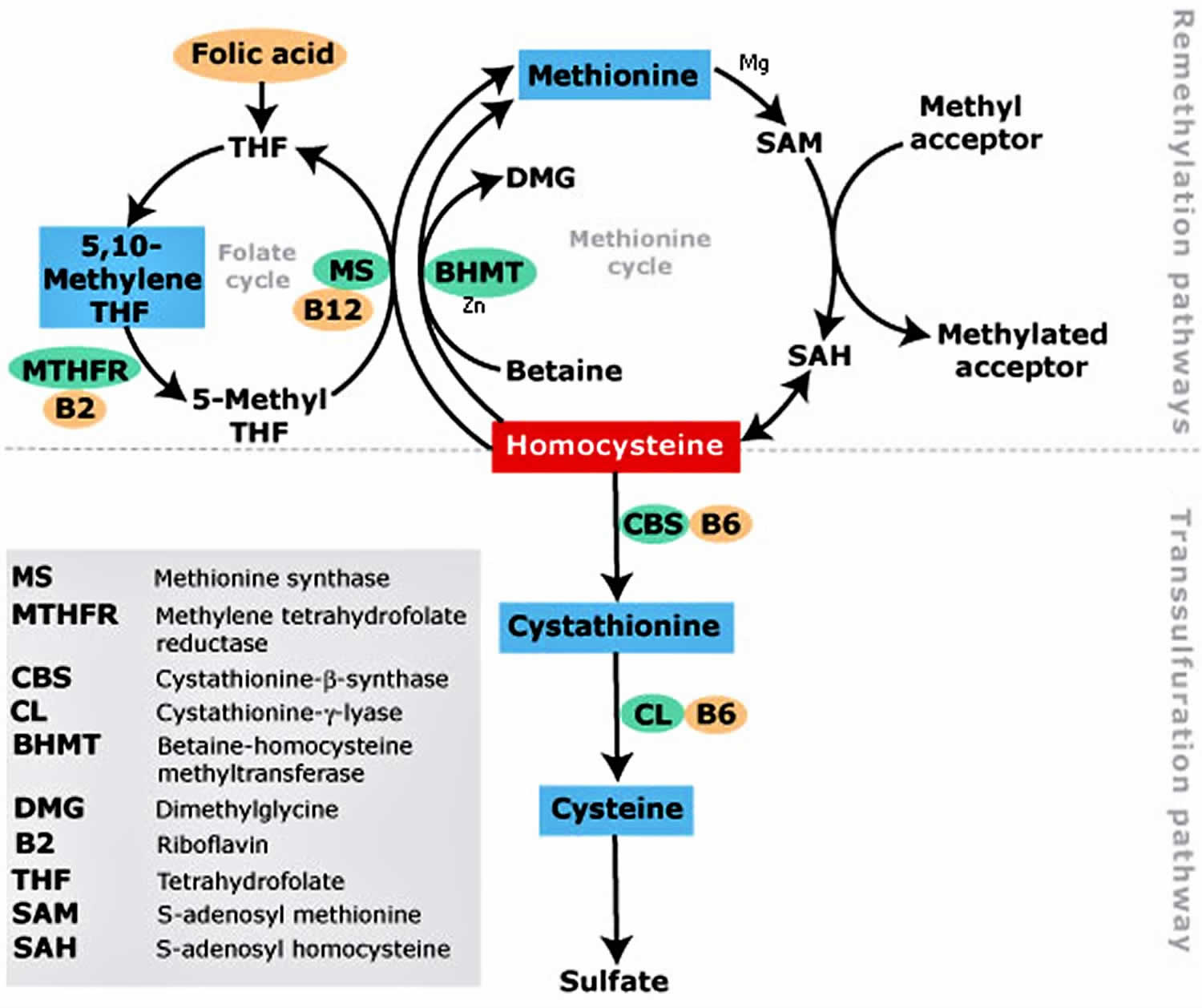
Figure 1. Homocysteine metabolism
Can my MTHFR genes change?
No, you inherit a copy of the gene from each of your parents and they will not change over time.
If I have the same MTHFR gene mutations as a relative, why is my homocysteine level significantly different?
Even when two people have the same MTHFR mutations, the results and their risks are often different. Many things can affect homocysteine levels, including MTHFR enzyme activity, folate or other B vitamin levels, and a person’s health status.
What is MTHFR gene mutation
MTHFR (methylenetetrahydrofolate reductase) is a gene. You carry two copies of MTHFR gene. MTHFR tells your body how to create an enzyme involved in breaking down the amino acid homocysteine 1. As is true for any gene, the DNA code of the MTHFR gene can vary. When doctor identify a part of the sequence that varies, they call it a “variant.” Genetic research aims to identify specific variants that cause harm or benefit to health.
Methylenetetrahydrofolate reductase (MTHFR) plays a central role in folate and homocysteine metabolism by catalyzing the conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate, the primary circulatory form of folate which is utilized in homocysteine remethylation to methionine 2. Genetic variations in the MTHFR gene can lead to impaired function or inactivation of this enzyme, which results in mildly elevated levels of homocysteine, especially in individuals who are also deficient in folate 3. In these individuals, a daily supplement of low dose folic acid may reduce and often normalize their homocysteine levels, but this has not been demonstrated to improve health outcomes 4.
There are two MTHFR gene variants, called C677T and A1298C, that have been an active area of study. These variants are common. In America, about 25% of people who are Hispanic, and 10-15% of people who are Caucasian have two copies of C677T 5. The TT genotype is least common in individuals of African descent (6%) 6. Individuals who carry two copies of this variant (“TT homozygous”) tend to have higher homocysteine levels and lower serum folate levels compared to controls 7.
Studies have found that women with two C677T gene variants have an increased risk for having a child with a neural tube defect 7. Studies have also found that men and women with two C677T gene variants and elevated homocysteine levels may be at a mild increased risk for blood clots (venous thromboembolism) 7.
Another common MTHFR variant, A1298C, does not cause increased homocysteine levels in heterozygous or homozygous individuals, but combined heterozygosity of 1298A>C and 677C>T results in an outcome similar to TT homozygous individuals 8.
Until recently, it was thought that MTHFR deficiency, by causing elevated homocysteine levels, led to an increased risk of venous thrombosis, coronary heart disease, and recurrent pregnancy loss 9. However, more recent analysis has not found an association between elevated homocysteine levels and the risk of venous thrombosis or the risk of coronary heart disease 10.
MTHFR polymorphism genotyping should not be ordered as part of the clinical evaluation for thrombophilia, recurrent pregnancy loss, or for at-risk family members 11.
Rarely, more severe variants in the MTHFR gene can be a cause of an autosomal recessive inborn error or metabolism where extremely high levels of homocysteine accumulate in the urine and plasma. This can cause developmental delay, eye disorders, thrombosis, and osteoporosis. But more commonly, homocystinuria is caused by variants in a different gene (cystathionine beta-synthase) 7.
Very high homocysteine levels rarely result from having two common variants alone. People with very high homocysteine levels should be carefully evaluated for other factors known to affect homocysteine. Doing so may bring to light dietary deficiencies, thyroid disease, diabetes, high cholesterol, or life-style factors (physical inactivity, smoking and obesity) which can impact homocystine levels. If high levels of homocysteine cannot be explained by these factors, a consultation with a genetics professional may be helpful in identifying rare genetic causes of the high homocysteine 12.
MTHFR gene mutation symptoms
People with common MTHFR variants can have normal or elevated levels of homocysteine in their blood or urine. MTHFR variants and elevated homocysteine levels have been studied as risk factors for a number of health conditions.
When thinking about risk factors it is important to not only think about if the variants put you at risk for a condition, but if so, how much risk. You will find many studies on MTHFR and health risks. For most of these, evidence is lacking regarding an association 13. Described below are conditions that are more widely recognized to be associated with the common MTHFR variants.
Studies suggest that women with two C677T gene variants are twice as likely to have a child with a neural tube defect 7. However, because neural tube defects are rare, their actual risk is still far less than 1% (0.14%) 14.
Studies have also found that men and women with two C677T gene variants and elevated homocysteine levels may be at a mildly increased risk for blood clots (venous thromboembolism) 7.
Risks associated with having one C677T and one A1298C is the same, or possibly slightly lower than, that of having two C677T gene changes 15.
For the vast majority of people the overall risk associated with the common MTHFR variants is small. So small, that having them does not change treatment. This is why testing for the variants is not recommended, unless a person has very high homocysteine levels. It is important to keep in mind that neural tube defects and blood clots have many other risk factors.
Very high homocysteine levels rarely result from having the common variants alone. People with very high homocysteine levels should be carefully evaluated for other factors known to affect homocysteine, such as 16:
- Low thyroid hormones (hypothyroidism)
- Chronic conditions (obesity, diabetes, high cholesterol, physical inactivity, high blood pressure)
- Medications (atorvastatin, fenofibrate, methotrexate, andnicotinic acid)
- Smoking
- Advanced age
High homocysteine levels can also result from dietary deficiencies of folate, vitamin B6, and vitamin B12. It is very important to diagnose vitamin B12 deficiencies, as high dose folic acid supplements can mask B12 deficiencies, and put people at risk for serious and irreversible symptoms.
If high levels of homocysteine can not be explained by factors such as those listed above, a consultation with a genetics professional may be helpful in identifying rare genetic causes of the high homocysteine 12.
MTHFR gene mutation diagnosis
Genetic testing is available for MTHFR gene variants, however testing is rarely recommended 17.
The American Congress of Obstetricians and Gynecologists (ACOG) and the American College of Medical Genetics recommends against testing for common MTHFR gene variants. Common MTHFR gene variants have not been proven to be a concerning risk factor for blood clots, pregnancy loss, or other negative pregnancy outcomes 18.
The American Heart Association recommends against testing for the common MTHFR gene variants or homocysteine as a screen for increased risk of cardiovascular conditions 15. The American Heart Association does not consider MTHFR a major risk factor for heart disease.
The College of American Pathologists, the American College of Medical Genetics, and the American Heart Association recommend against testing for C677T and A1298C in people with blood clots. This is because results have little impact on a persons medical management 7.
Any individual who suspects that a disease or disorder is related to MTHFR deficiency should talk to their doctor about testing for fasting homocysteine levels in the blood 7.
If the fasting blood homocysteine level is high, then the patient should seek medical advice from an expert doctor in this field who can address the possible medical implications. If the fasting homocysteine level in the blood is normal, then it is unlikely that the person’s symptoms are due to the MTHFR genetic variation.
MTHFR gene mutation test
Everyone has two MTHFR genes, one inherited from your mother and one from your father. Mutations can occur in one or both MTHFR genes. There are different types of MTHFR mutations. An MTHFR test looks for two of these mutations, also known as variants. The MTHFR variants are called C677T and A1298C. MTHFR gene mutation test may be used to detect two relatively common mutations in the MTHFR gene that are associated with elevated levels of homocysteine in the blood. MTHFR gene mutation test is not routinely ordered.
MTHFR gene mutation test is sometimes ordered as a follow-up to an elevated homocysteine test and may be occasionally ordered along with other cardiac risk tests if a person has a personal or family history of premature cardiovascular disease (CVD) or inappropriate blood clots (thrombosis). However, its utility for assessing risk of cardiovascular disease has not been established and some expert guidelines do not recommend it for thrombosis screening.
MTHFR gene mutation test may be ordered if a person has a close relative with known MTHFR genetic mutations, particularly if that person also has elevated homocysteine levels. MTHFR C677T and A1298C gene mutations are the most common and the ones that are typically tested. If someone has a different mutation in their family, then that specific mutation should be tested.
An MTHFR test may sometimes be ordered along with other inherited clotting risk tests, such as Factor V Leiden or prothrombin 20210 mutation tests to help evaluate a person’s overall risk of developing inappropriate blood clots.
Although the MTHFR mutation test may be used to help determine the cause of elevated homocysteine, the value of measuring homocysteine levels is not clear. While evidence from some studies suggests that elevated homocysteine levels contribute to the risk of cardiovascular disease and/or thrombosis, a direct link has not been established. Routine testing for homocysteine levels as a cardiac risk marker is not recommended by the American Heart Association. The College of American Pathologists and the American College of Medical Genetics recommend against testing for the C677T variant, citing limited utility for patients with blood clots. Furthermore, use of homocysteine levels for the purpose of determining risk of cardiovascular disease, peripheral vascular disease, and stroke is in doubt at this time given that several studies show no benefit or risk reduction in people who were treated with folic acid and vitamin B supplements that lowered their homocysteine level.
What is MTHFR gene mutation test used for?
This test is used to find out if you have one of two MTHFR mutations: C677T and A1298C. It is often used after other tests show you have higher than normal homocysteine levels in the blood. Conditions such as high cholesterol, thyroid disease, and dietary deficiencies can also raise homocysteine levels. An MTHFR test will confirm whether the raised levels are caused by a genetic mutation.
Even though an MTHFR mutation brings a higher risk of birth defects, the test is not usually recommended for pregnant women. Taking folic acid supplements during pregnancy can greatly reduce the risk of neural tube birth defects. So most pregnant women are encouraged to take folic acid, whether or not they have an MTHFR mutation.
When is MTHFR gene mutation test ordered?
The MTHFR mutation test may sometimes be ordered when a person has elevated homocysteine levels, especially when the person has a personal or family history of premature cardiovascular disease or thrombosis. It may sometimes be ordered when a close relative has MTHFR gene mutations, although it may not be useful if that relative has normal homocysteine levels, and some laboratories and organizations recommend against using it for thrombophilia screening.
If a person is suspected to have high homocysteine levels, it is recommended to test for homocysteine level rather than MTHFR mutation. In a significant number of cases of homocysteinemia (increase in blood homocysteine level), the MTHFR mutation test is unnecessary.
Why do I need an MTHFR gene mutation test?
You may need this test if:
- You had a blood test that showed higher than normal levels of homocysteine
- A close relative was diagnosed with an MTHFR mutation
- You and/or close family members have a history of premature heart disease or blood vessel disorders
Your new baby may also get an MTHFR test as part of routine newborn screening. A newborn screening is a simple blood test that checks for a variety of serious diseases.
How is a MTHFR gene mutation test performed?
A health care professional will take a blood sample from a vein in your arm, using a small needle. After the needle is inserted, a small amount of blood will be collected into a test tube or vial. You may feel a little sting when the needle goes in or out. This usually takes less than five minutes.
For a newborn screening, a health care professional will clean your baby’s heel with alcohol and poke the heel with a small needle. He or she will collect a few drops of blood and put a bandage on the site.
Testing is most often done when a baby is 1 to 2 days old, usually in the hospital where he or she was born. If your baby wasn’t born in the hospital or if you have left the hospital before the baby could be tested, talk to your health care provider about scheduling testing as soon as possible.
Will I need to do anything to prepare for the MTHFR gene mutation test?
You don’t need any special preparations for an MTHFR mutation test.
What does the MTHFR gene mutation test result mean?
Results typically are reported as negative or positive and, if positive, the report will name the mutation(s) present. Often, an interpretation of the results is also provided.
Only a small percentage of cases of elevated homocysteine are due to an inherited cause. Of these, MTHFR C677T and A1298C mutations are among the most common.
If a person has two copies (homozygous) of MTHFR C677T, or has one copy of C677T and one of A1298C, then it is likely that elevated homocysteine levels are due to these inherited mutations, or that the mutations are contributing to them.
Two copies of A1298C are not typically associated with increased homocysteine levels.
If the MTHFR mutation test is negative, then the C677T and A1298C mutations were not detected and the tested person’s elevated homocysteine level is likely due to another cause. Other, more rare MTHFR genetic mutations will not be detected with typical testing.
Those with MTHFR mutations and other clotting risk factors, such as Factor V Leiden or PT 20210 mutations, may be at an increased risk of thrombosis. Research suggests that women with two C677T variants have double the risk of having a child with a neural tube defect, but the risk is far below 1%.
People who have elevated homocysteine levels may be at an increased risk of developing premature cardiovascular disease and/or thrombosis, but many, including those with MTHFR mutations, will never develop cardiovascular disease or thrombosis. A review of data published in 2012 determined that lifelong moderately elevated homocysteine levels had little to no effect on coronary heart disease.
Besides MTHFR mutations, there are other causes of elevated homocysteine levels, including deficiency of vitamins B6, B12, and/or folate; these vitamins are required for homocysteine metabolism. The MTHFR mutation may not be present with these acquired, as opposed to inherited, causes of elevated homcysteine. Additionally, if a more rare mutation of MTHFR is causing elevated homocysteine levels, the C677T and A1298C tests will not detect those other mutations.
For MTHFR mutations, the C677T variant results in substitution of the amino acid alanine for valine. The A1298C variant results in an alanine substitution (versus a glutamine). The C677T valine substitution results in a less active form of the MTHFR enzyme.
A review of studies published in 2014 supported an association between the MTHFR C677T allele and congenital heart disease in Asian populations and the A1298C allele and CHD in the pediatric Caucasian population.
The MTHFR enzyme is involved in folate metabolism. Because of this, those who have MTHFR mutations and take drugs that affect folate metabolism, such as methotrexate, may be more likely to experience toxicity. An MTHFR mutation test may be performed for a person who is prescribed methotrexate in order to adjust dosages and reduce risk of toxicity.
What does having two copies of the A1298C mutation mean for treatment and further testing recommendations?
Having two copies of A1298C is not associated with significant health risks 18. Experts recommend that you discuss this with your doctor to determine if further testing is recommended.
Does having one C677T mutation in the MTHFR gene increase a person’s risk of developing blood clots?
Having one mutation in the MTHFR gene is typically not associated with an increased risk of blood clots, because it usually does not lead to high levels of homocysteine in the blood 19.
MTHFR gene mutation treatment
Regardless of the reason for high homocysteine levels, your health care provider may recommend taking folic acid and/or other vitamin B supplements, and/or changing your diet. B vitamins can help bring your homocysteine levels back to normal. We recommend you speak with a trusted healthcare professional before taking any supplement.
If you have questions about your results, talk to your health care provider.
Having MTHFR gene variants alone does not impact treatment. If a person has high homocysteine levels they should be carefully evaluated to identify all causes. Very high homocysteine levels rarely result from having the common variants alone. People with very high homocysteine levels should be carefully evaluated for other factors known to affect homocysteine, such as 16:
- Low thyroid hormones (hypothyroidism)
- Chronic conditions (obesity, diabetes, high cholesterol, physical inactivity, high blood pressure)
- Medications (atorvastatin, fenofibrate, methotrexate, andnicotinic acid)
- Dietary deficiencies (folate, vitamin B6, vitamin B12)
- Smoking
- Advanced age
Treatments and life-style changes are given based upon the patient’s circumstances. As mentioned above, homocysteine levels can rise in people with and without MTHFR gene variants if they lack folate, choline, or B vitamins (B12, B6, and riboflavin) 20. People with concerns about their nutrition should speak with a healthcare professional. Supplements may be recommended if the person is found to have a nutritional deficiency 20.
Current clinical guidelines do not recommend changes in prenatal care or prenatal vitamins based upon MTHFR gene variant status alone. Women of childbearing age should take the standard dose of folate supplementation to reduce the risk of neural tube defects 7. Women with a previous child with a neural tube defect or a family history of neural tube defect should talk to their doctors about requirements for extra folate supplementation 18.
- Overview of homocysteine. https://www.uptodate.com/contents/overview-of-homocysteine[↩]
- Rosenblatt DS. Inherited disorders of folate transport and metabolism. In: Scriver CR, Beaudet AL, Sly S, Valle D, eds. The Metabolic and Molecular Bases of Inherited Disease. Seventh ed. New-York: McGraw-Hill. 1995:3111–3128.[↩]
- Holmes M.V., Newcombe P., Hubacek J.A., Sofat R., et al. Effect modification by population dietary folate on the association between MTHFR genotype, homocysteine, and stroke risk: a meta-analysis of genetic studies and randomised trials. Lancet. 2011;378(9791):584–94.[↩]
- Shiran A., Remer E., Asmer I., Karkabi B., et al. Association of Vitamin B12 Deficiency with Homozygosity of the TT MTHFR C677T Genotype, Hyperhomocysteinemia, and Endothelial Cell Dysfunction. Isr Med Assoc J. 2015;17(5):288–92.[↩]
- Hickey S.E., Curry C.J., Toriello H.V. ACMG Practice Guideline: lack of evidence for MTHFR polymorphism testing. Genet Med. 2013;15(2):153–6. [↩]
- Wilcken B., Bamforth F., Li Z., Zhu H., et al. Geographical and ethnic variation of the 677C>T allele of 5,10 methylenetetrahydrofolate reductase (MTHFR): findings from over 7000 newborns from 16 areas world wide. Journal of medical genetics. 2003;40(8):619–25.[↩]
- Dean L. Methylenetetrahydrofolate Reductase Deficiency. 2012 Mar 8 [Updated 2016 Oct 27]. In: Pratt V, McLeod H, Rubinstein W, et al., editors. Medical Genetics Summaries [Internet]. Bethesda (MD): National Center for Biotechnology Information (US); 2012-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK66131[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- van der Put N.M., Gabreels F., Stevens E.M., Smeitink J.A., et al. A second common mutation in the methylenetetrahydrofolate reductase gene: an additional risk factor for neural-tube defects? American journal of human genetics. 1998;62(5):1044–51.[↩]
- Humphrey L.L., Fu R., Rogers K., Freeman M., et al. Homocysteine level and coronary heart disease incidence: a systematic review and meta-analysis. Mayo Clinic proceedings. 2008;83(11):1203–12.[↩]
- Clarke R., Bennett D.A., Parish S., Verhoef P., et al. Homocysteine and coronary heart disease: meta-analysis of MTHFR case-control studies, avoiding publication bias. PLoS Med. 2012;9(2):e1001177.[↩]
- Hickey S.E., Curry C.J., Toriello H.V. ACMG Practice Guideline: lack of evidence for MTHFR polymorphism testing. Genet Med. 2013;15(2):153–6.[↩]
- Homocystinuria due to deficiency of N(5,10)-Methylenetetrahydrofoloate reductase activity. Online Mendelian Inheritance in Man. 2007[↩][↩]
- Liew SC & Gupta ED. Methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism: epidemiology, metabolism and the associated diseases. Eur J Med Genet. January 2015; 58(1):1-10. https://www.ncbi.nlm.nih.gov/pubmed/25449138[↩]
- Williams J, Mai CT, Mulinare J, et al. Updated estimates of neural tube defects prevented by mandatory folic Acid fortification – United States, 1995-2011. MMWR Morb Mortal Wkly Rep. 2015;64(1):1-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4584791/[↩]
- Hickey SE, Curry CJ, Toriello HV.. ACMG Practice Guideline: lack of evidence for MTHFR polymorphism testing. Genet Med. February 2013; 15(2):153-156. https://www.ncbi.nlm.nih.gov/pubmed/23288205[↩][↩]
- Varga E and Moll S. Homocysteine and MTHFR Mutations. Circulation. 2015; 132:e6-e9. https://www.ahajournals.org/doi/pdf/10.1161/CIRCULATIONAHA.114.013311[↩][↩]
- MTHFR gene variant. https://rarediseases.info.nih.gov/diseases/10953/mthfr-gene-mutation[↩]
- Levin BL, Varga E. MTHFR: Addressing Genetic Counseling Dilemmas Using Evidence-Based Literature. J Genet Couns.. 2016 Oct; 25(5):901-11:https://www.ncbi.nlm.nih.gov/pubmed/27130656[↩][↩][↩]
- Varga EA, Sturm AC, Misita CP & Moll S. Homocysteine and MTHFR Mutations: Relation to Thrombosis and Coronary Artery Disease. Circulation. 2005; 111:e289-e293. http://circ.ahajournals.org/content/111/19/e289.full[↩]
- Folate. https://lpi.oregonstate.edu/mic/vitamins/folate[↩][↩]





{kind=link}