
What is neck dissection
Neck dissection is surgery to examine and remove the lymph nodes in the neck. Cells from cancers in the mouth or throat can travel in the lymph fluid and get trapped in your lymph nodes. The lymph nodes are removed to prevent cancer from spreading to other parts of your body. Neck dissection is a common treatment option for lymph node metastasis in patients with head and neck cancer 1.
The lymph system carries white blood cells around the body to fight infection. Cancer cells in the mouth or throat can travel in the lymph fluid and get trapped in the lymph nodes. The lymph nodes are removed to prevent cancer from spreading to other parts of the body and to decide if any more treatment is needed.
Your doctor may recommend neck dissection procedure if:
- You have cancer of the mouth, tongue, thyroid gland, or other areas of the throat or neck.
- Cancer has spread to the lymph nodes.
- The cancer could spread to other parts of the body.
More than 50% of patients with squamous cell carcinoma (SCC) of the oral cavity have lymph node metastases and histological confirmation of metastatic disease is the most important prognostic factor 2. Neck metastasis is the most important prognostic factor in head and neck squamous cell carcinomas (SCC) 3. On account of this widely demonstrated fact, management of neck disease in head and neck cancer has been considered one of the most important aspects of treatment. Among patients with a clinically negative neck, the incidence of occult metastases varies with the site, size and thickness of the primary tumor. The high incidence rate of occult cervical metastases (> 20%) in tumors of the lower part of the oral cavity is the main argument in favor of elective treatment of the neck. The usual treatment of patients with clinically palpable metastatic lymph nodes has been radical neck dissection. This classical surgical procedure involves not only resection of level I to V lymph nodes of the neck but also the tail of the parotid, submandibular gland, sternocleidomastoid muscle, internal jugular vein and spinal accessory nerve. It is a safe oncological surgical procedure that significantly reduces the risk of regional recurrences, however it produces significant post-operative morbidity, mainly shoulder dysfunction.
You will be asleep during the surgery. Your doctor may make cuts under your chin and toward your ear, at the bottom of your neck, or in the middle of your neck. This depends on which lymph nodes must be removed. These cuts are called incisions. They are closed with stitches, staples, or skin clips. They will leave scars that fade with time.
Most people stay in the hospital for several days or longer after surgery. How long you stay depends on why you need surgery and how much tissue was taken out.
You may be able to go back to work or your normal routine a few weeks after the surgery. This depends on your job and the extent of your surgery.
Neck dissection levels
The classification of cervical lymph nodes is according to the system developed at Memorial Sloan-Kettering Cancer Center in the 1930s 4. This system divides the lymph nodes in the lateral aspect of the neck into five nodal levels, I through V as described below. The lymph nodes in the central compartment are in category level VI, and those in the superior anterior mediastinum are level VII. The clinical and surgical landmarks for neck node levels are (see Figure 1 below):
1. Level I (submental and submandibular triangles) borders are:
- Superior – the lower border of the body of the mandible;
- Posterior – posterior belly of digastric
- Inferior – hyoid bone
2. Level II (upper jugular lymph nodes) borders are:
- Superior – the base of the skull
- Posterior – posterior border of the sternocleidomastoid
- Anterior – lateral limit of sternohyoid
- Inferior-hyoid bone
3. Level III (middle jugular lymph nodes) borders are:
- Superior – hyoid bone
- Posterior – posterior border of the sternocleidomastoid
- Anterior – lateral limit of sternohyoid;
- Inferior – cricothyroid membrane
4. Level IV (lower jugular lymph nodes) borders are:
- Superior – cricothyroid membrane
- Posterior – posterior border of the sternocleidomastoid
- Anterior – lateral limit of sternohyoid
- Inferior – clavicle
5. Level V (posterior triangle of the neck) borders are:
- Posterior – the anterior border of the trapezius
- Anterior – the posterior border of the sternocleidomastoid
- Inferior – clavicle
6. Level VI: (central compartment of the neck) borders are:
- Superior – hyoid bone;
- Inferior – suprasternal notch
- Lateral – medial border of the carotid sheath on either side
7. Level VII: (superior mediastinal lymph nodes) borders are:
- Superior – suprasternal notch
- Inferior – innominate artery
Figure 1. Neck dissection levels
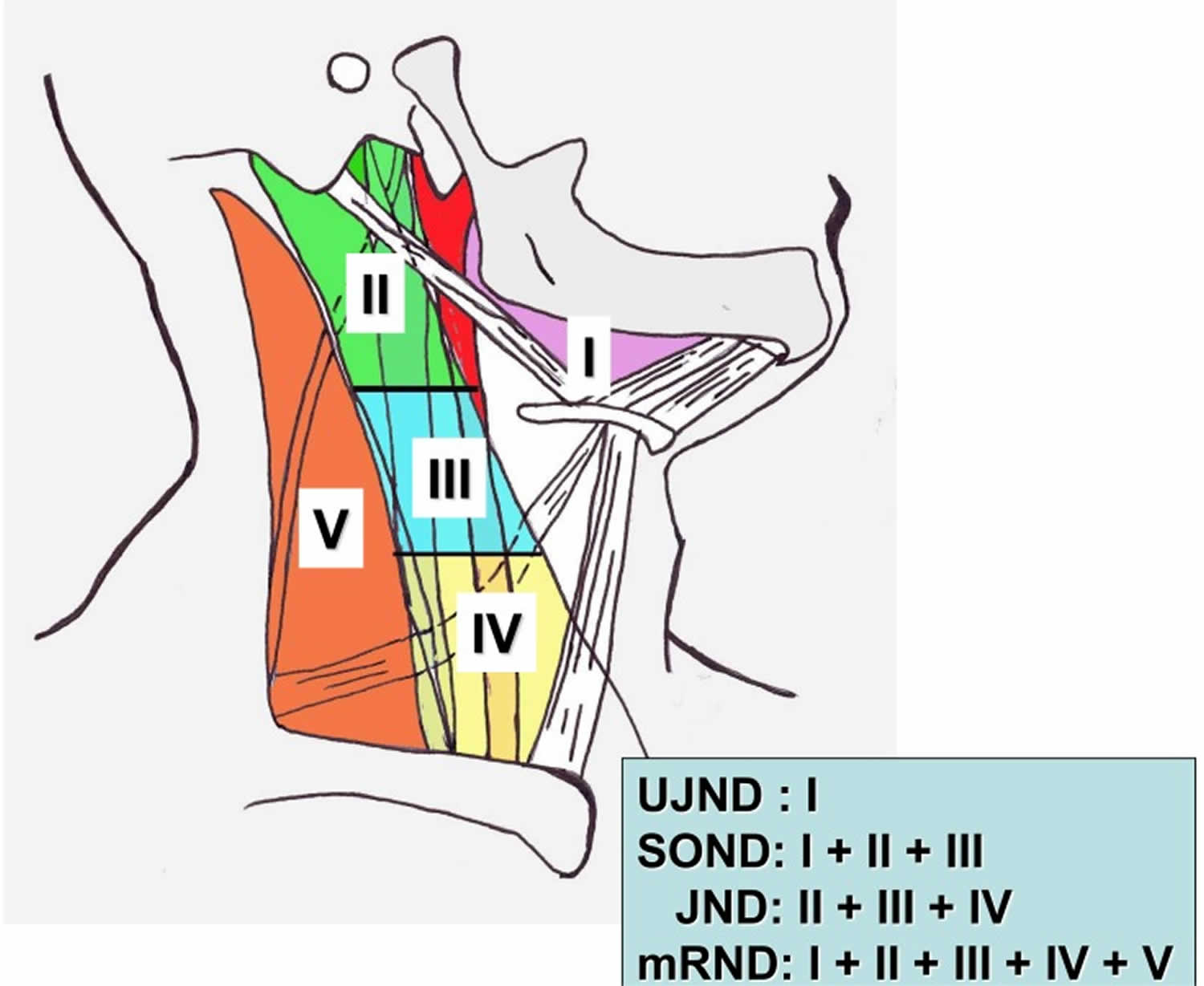
Footnote: A diagram showing levels of cervical lymph nodes. Level I: submental and submandibular; Level II: upper jugular; Level III: middle jugular; Level IV: lower jugular; Level V: posterior triangle.
Abbreviations: JND= jugular neck dissection; mRND = modified radical neck dissection; NND = no neck dissection; SOND = supraomohyoid neck dissection; UJND = upper jugular neck dissection.
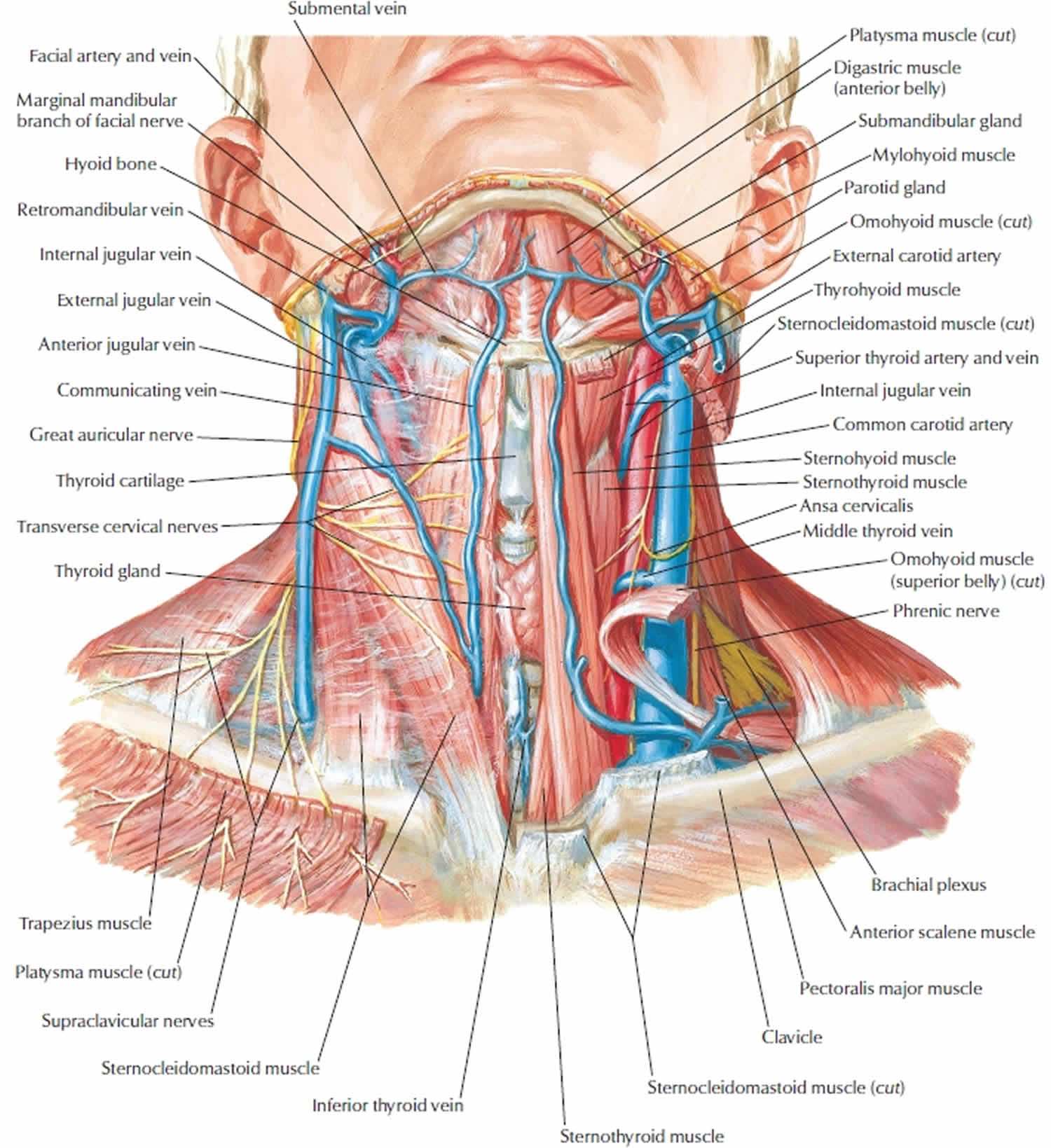
[Source 5 ]Figure 2. Radical neck dissection
Neck dissection types and indications
The credit for neck dissection as a curative procedure for cervical metastases belongs to George Washington Crile from the Cleveland Clinic 6. In 1900, he performed different types of neck dissections and subsequently described the classic operation of radical neck dissection in his seminal article of 1905 published in the Transactions of the Southern Surgical and Gynecological Association. This operation is considered being the basic neck dissection, and all other procedures are considered being its modifications. Hayes Martin from Memorial Sloan-Kettering Cancer Center, who described the stepwise procedure of radical neck dissection in his classic article in 1951 popularized this operation. However, this operative procedure is not without morbidity, as it results in a cosmetic deformity and dysfunction of shoulder movement. Argentinian Oswaldo Suarez was the first to describe functional neck dissection in 1963, now called modified radical neck dissection 7. He described the removal of all five lymph node levels in the neck while preserving the spinal accessory nerve, sternocleidomastoid muscle, and internal jugular vein to limit any functional disability in the shoulder 8.
Radical neck dissection
Lymph nodes from level I-V, ipsilateral sternocleidomastoid muscle, internal jugular vein and spinal accessory nerve undergo removal. Radical neck dissection is indicated when the neck is lymph node positive for squamous cell carcinoma (SCC) where spinal accessory nerve involved and/or extensive soft tissue disease with the invasion of sternocleidomastoid muscle and internal jugular vein 9.
Modified radical neck dissection
- Modified radical neck dissection type 1: Lymph nodes from level I-V, ipsilateral sternocleidomastoid muscle, and internal jugular vein get removed, with preservation of the spinal accessory nerve. Indications for modified radical neck dissection type I is in the neck lymph node positive for squamous cell carcinoma (SCC) where spinal accessory nerve is free of disease.
- Modified radical neck dissection type 2: Removal of lymph nodes from level I-V and ipsilateral sternocleidomastoid muscle, with preservation of internal jugular vein and spinal accessory nerve. The neck lymph node positive for squamous cell carcinoma (SCC) or thyroid cancer where internal jugular vein involved but spinal accessory nerve is free of disease.
- Modified radical neck dissection type 3: Lymph nodes from level I-V undergo removal, with preservation of sternocleidomastoid muscle, internal jugular vein and spinal accessory nerve. Modified radical neck dissection type 3 is indicated in metastatic differentiated thyroid carcinoma 10.
Selective neck dissection
If cancer has not spread far, fewer lymph nodes have to be removed. The muscle, nerve, and blood vessel in the neck may also be saved. The severe comorbidities related to the removal of sternocleidomastoid muscle, internal jugular vein and spinal accessory nerve led to the numerous modifications of the procedure with selective removal of lymph nodes. They are 7:
Supraomohyoid neck dissection
Lymph nodes removed are Levels I–III, with sparing of internal jugular vein, sternocleidomastoid muscle, and spinal accessory nerve. Supraomohyoid neck dissection is indicated in N0 neck for squamous cell carcinoma (SCC) of oral cavity and oropharynx (include level 4) and N0 neck malignant melanoma where primary site is anterior to ear (include parotidectomy for face and scalp).
Extended supraomohyoid neck dissection
Removal of lymph nodes in levels I–IV, with sparing of internal jugular vein, sternocleidomastoid muscle, and spinal accessory nerve. The procedure is indicated in N0 neck for squamous cell carcinoma (SCC) of the lateral tongue 11.
Lateral neck dissection
Removal of lymph nodes from level II-IV with sparing of internal jugular vein, sternocleidomastoid muscle, and spinal accessory nerve. Indications for this procedure are in N0 neck for squamous cell carcinoma (SCC) of larynx and hypopharynx.
Postero-lateral neck dissection
Removal of levels II–V, suboccipital, retro-auricular nodes with sparing of squamous cell carcinoma (SCC). Indications for this procedure is in N0 neck malignant melanoma where the primary site is posterior to ear.
Modified lateral neck dissection
Removal of levels II to V lymph nodes with relative sparing of sternocleidomastoid muscle, internal jugular vein, spinal accessory nerve and submaxillary gland. This procedure has an indication of therapeutic neck dissection for thyroid cancer with lateral neck nodes 12.
Neck dissection contraindications
Contraindications to neck dissection have been controversial. Some of them are listed below 13:
- Severe cardiopulmonary disease, COPD with poor functional status
- Preoperative imaging showing deep infiltration of the tumor in the prevertebral space, scalene muscles, levator scapula muscle, phrenic nerve, and brachial plexus are not suitable candidates
- The primary tumor that is uncontrollable.
- Distant metastatic disease
- Fixed neck mass in the deep cervical fascia and/or skull base involvement
Neck dissection procedure
Neck dissection is a major surgery done to remove lymph nodes that contain cancer. It is done in the hospital. Before surgery, you will receive general anesthesia. This will make you sleep and unable to feel pain.
The amount of tissue and the number of lymph nodes that are removed depend on how far the cancer has spread.
Incision
A single trifurcate neck incision was the most frequently used incision in the past. However, it is now these operations are carried out effectively with a single skin crease incision in the mid-neck of sufficient length. The named incisions that a reader should know are Latyshevsky and Freund, Mac Fee, Crile, Kocher, Schobinger, and Hockey stick incision 14.
Raising skin flaps
The skin incision is deepened through the subcutaneous tissue and then through the platysma muscle. The posterior flap is then raised in the subplatysmal plane by applying traction to the flap with skin hooks and counter-traction of the deeper soft tissues. The flap is elevated up to the anterior border of the trapezius muscle.
Identifying Marginal mandibular nerve
Careful identification of the marginal branch of the facial nerve is crucial. Posteriorly the greater auricular nerve and the external jugular vein overlying the sternocleidomastoid muscle come into view as the elevation of the flap continues. The greater auricular nerve and the external jugular vein should be identified carefully and preserved. We advise the use of the scalpel or scissors to dissect around the mandibular branch rather than electrocautery as it may cause temporary damage to the nerve. This nerve lies just anterior to the submandibular fascia and superficial to the posterior facial vein. The vein is ligated, and its upper stump retracted cephalad, protecting the marginal branch of the facial nerve. The pre-vascular facial lymph nodes are exposed and dissected out (Hayes Martin maneuver).
Superior Dissection
The fibrous fatty tissue of the submental triangle is dissected off the anterior bellies of the digastric muscles and the mylohyoid. The fascia is then dissected off the anterior belly of the digastric muscle, and the specimen is retracted posteriorly, removing the fibrous fatty tissue containing lymph nodes lateral to the mylohyoid muscle. When the dissection reaches the posterior border of the mylohyoid, this is retracted anteriorly, exposing the lingual nerve and the submandibular gland duct are divided. Finally, the facial artery is ligated as it crosses forward, under the posterior belly of the digastric muscle. The tail of the parotid gland is transected, and the sternocleidomastoid muscle is then incised close to its insertion in the mastoid process. The fibro-fatty tissue medial to the muscle is incised, exposing the splenius capitis and the levator scapulae muscles. Otherwise, incising the fascia below the digastric muscle and gentle inferior traction of the specimen allows identification of the hypoglossal nerve, the upper end of the internal jugular vein, and the spinal accessory nerve. At this point in the dissection, the internal jugular vein and the spinal accessory nerve are divided if the location and extent of the tumor permit it.
Inferior dissection
The dissection is continued posteriorly and inferiorly along the anterior border of the trapezius muscle. The spinal accessory nerve and the transverse cervical vessels are divided as they cross the anterior the border of the trapezius muscle. During this step of the operation, it is important to preserve the branches of the cervical plexus that innervate the levator scapulae muscle, unless the extent of the disease in the neck precludes it. The sternocleidomastoid muscle and the superficial layer of the deep cervical fascia are incised above the superior border of the clavicle. The external jugular vein and the omohyoid muscle are divided. The fibro-fatty tissue in this region is then gently pushed in an upward direction, exposing the brachial plexus, the scalenus anticus muscle, and the phrenic nerve. Posteriorly, the dissection is continued to join the previous dissection along the anterior border of the trapezius.
Medial dissection
The dissection is continued medially to expose the vagus nerve, the common carotid artery, and the internal jugular vein. Inferiorly, the phrenic nerve is identified and protected. The surgeon must remain very vigilant on the left side to be able to identify thoracic duct, which arches downward and forward from behind the common carotid to open into the internal jugular vein, the subclavian vein, or the angle formed by the junction of these two vessels. The duct is located anterior or superficial to the anterior scalene muscle and the phrenic nerve. To prevent a chyle leak, the surgeon must also remember that the thoracic duct may have multiple connections at its upper end and that at the base of the neck it usually receives a jugular, a subclavian, and perhaps other minor lymphatic trunks, which must be individually ligated or clipped.
The internal jugular vein can be divided either superiorly or inferiorly, depending on the location of the disease in the neck. If the tumor mass is located low in the jugulodigastric region or the mid-jugular region, the internal jugular vein is first ligated and divided superiorly. The dissection then continues in an inferior direction, separating the specimen from the vagus nerve, the carotid artery, and the superior thyroid vessels. If instead, the disease is located high in the jugulodigastric region, the internal jugular vein is dividedinferiorly, and the dissection continues in a superior direction along the common carotid artery; this is especially useful when the tumor is extensive and may require removal of the external carotid artery or the hypoglossal nerve. Mobilization of the surgical specimen from below allows easier dissection from the internal carotid artery and, if possible, the external carotid and the hypoglossal nerve.Closure: Incision closure is in two layers: the first layer approximates the platysma anteriorly and the subcutaneous tissue laterally, and the second layer approximates the skin. One or two suction drains should remain in place. The drain(s) should not rest immediately over the carotid artery or in the area of the thoracic duct.
Neck dissection complications
Risks for anesthesia and surgery in general are:
- Allergic reactions to medicines
- Breathing problems
- Bleeding
- Infection
Other risks for neck dissection surgery are:
- Numbness in the skin and ear on the side of the surgery, which may be permanent
- Damage to the nerves of the cheek, lip, and tongue
- Problems lifting the shoulder and arm
- Limited neck movement
- Drooping shoulder on the side of the surgery
- Problems talking or swallowing
- Facial droop
Neck dissection complications:
- Infection.
- Air leak.
- Postoperative bleeding.
- Chylous fistula.
Chyle leak formation is an uncommon but serious complication of head and neck surgery when the thoracic duct is inadvertently injured, particularly with the resection of malignancy low in the neck. The thoracic duct is the primary structure that returns lymph and chyle from the entire left and right lower half of the body 15. Chyle extravasation can result in delayed wound healing, dehydration, malnutrition, electrolyte disturbances, and immunosuppression. Prompt identification and treatment of a chyle leak are essential for optimal surgical outcome. The reported incidence varies between 2% and 8% of neck dissections 16. Management depends on the time of onset of the fistula, on the amount of chyle drainage in 24 hours, and the presence or absence of accumulation of chyle under the skin flaps 7. When the daily output of chyle exceeds 600 mL in a day or 200 to 300 mL per day for 3 days, especially when the chyle fistula becomes apparent immediately after surgery, conservative closed wound management is unlikely to succeed; these are indications for surgical exploration 7.
5. Synchronous bilateral radical neck dissections, in which both internal jugular veins undergo ligation, can result in the development of facial edema, cerebral edema, or both; blindness; and hypoxia 7.
6. Carotid artery rupture. The most feared and often lethal complication after neck surgery is exposure and rupture of the carotid artery. Therefore, every effort must be made to prevent it. If the skin incisions have proper design, the carotid seldom becomes exposed in the absence of a salivary fistula. If the carotid becomes exposed, it should be covered promptly with well-vascularized tissue.
7. The most notable complications observed in patients who have undergone a radical neck dissection are related to removal of the spinal accessory nerve. The resulting denervation of the trapezius muscle causes destabilization of the scapula with progressive flaring at the vertebral border, drooping, and lateral and anterior rotation. The loss of trapezius function decreases the patient’s ability to abduct the shoulder above 90 degrees at the shoulder. These physical changes result in a syndrome of pain, weakness, and deformity of the shoulder girdle commonly associated with the radical neck dissection 17.
Neck dissection recovery
A neck dissection is surgery to remove all or some of the lymph nodes and surrounding tissue from the neck. Lymph nodes are small, round or bean-shaped glands that act like filters and remove germs from your body, help fight infection, and trap cancer cells. This surgery is most often done to treat cancer of the head and neck.
You were likely to be in the hospital for 2 to 3 days. To help get ready for going home, you may have received help with:
- Drinking, eating, and perhaps talking
- Caring for your surgical wound in any drains
- Using your shoulder and neck muscles
- Breathing and handling secretions in your throat
- Managing your pain
You may leave the hospital with stitches in your cut (incision). Your doctor will tell you if you need to return to have these removed. You may still have a tube called a drain in your neck. Your doctor will probably take this out a few days after your surgery.
The area may also be swollen, and you may have a stiff neck. For most people, the swelling starts to go away 4 to 5 days after surgery. You may have numbness in your neck and ear. Your lower lip or shoulder may feel weak. For most people, these problems go away in 6 to 12 months. But sometimes these problems can be permanent. You may always feel a little numb, stiff, or weak in some areas.
If a neck muscle was removed, your neck may look flatter or thinner.
If you have cancer, you may still need other treatment after surgery, such as radiation or chemotherapy.
What to expect at home
Your health care provider will give you a prescription for pain medicines. Get it filled when you go home so you have the medicine when you need it. Take your pain medicine when you start having pain. Waiting too long to take it will allow your pain to get worse than it should.
DO NOT take aspirin, ibuprofen (Advil, Motrin), or naproxen (Aleve, Naprosyn). These medicines may increase bleeding.
You will have staples or suture in the wound. You may also have mild redness and swelling for the first couple of weeks after surgery.
You may have a drain in your neck when you leave the hospital. The provider will tell you how to care for it.
Healing time will depend on how much tissue was removed.
Incision care
You will need to learn to care for your wound.
- If your doctor told you how to care for your incision, follow your doctor’s instructions. If you did not get instructions, follow this general advice:
- After the first 24 to 48 hours, wash around the incision with clean water 2 times a day. Don’t use hydrogen peroxide or alcohol, which can slow healing.
- You may have a drain near your incision. Your doctor will tell you how to take care of it.
- You may get special antibiotic cream in the hospital to rub on your wound. Continue to do this 2 or 3 times a day after you go home.
- You can shower after you return home. Wash your wound gently with soap and water. DO NOT scrub or let the shower spray directly on your wound.
- DO NOT take a tub bath for the first few weeks after your surgery.
See your doctor if:
- You have a fever over 100.5°F (38.5°C).
- Your pain medicine is not working to relieve your pain.
- Your surgical wounds are bleeding, are red or warm to the touch, or have a thick, yellow, green, or milky drainage.
- You have problems with the drain.
- You cannot eat and lose weight because of swallowing problems.
- You are choking or coughing when you eat or swallow.
- It is hard to breathe.
Diet and Nutrition
You can eat your regular foods unless your doctor has given you a special diet.
If pain in your neck and throat is making it hard to eat:
- Take your pain medicine 30 minutes before meals.
- If it is painful to swallow, start out with cold drinks, Popsicles, and ice cream. Next, try soft foods like pudding, yogurt, canned or cooked fruit, scrambled eggs, and mashed potatoes. Avoid eating hard or scratchy foods like chips or raw vegetables. Avoid orange or tomato juice and other acidic foods that can sting the throat.
- Choose soft foods, such as ripe bananas, hot cereal, and moist chopped meat and vegetables.
- Limit foods that are hard to chew, such as fruit skins, nuts, and tough meat.
- If you cough right after drinking, try drinking thicker liquids, such as “smoothies.”
- You may notice that your bowel movements are not regular right after your surgery. This is common. Try to avoid constipation and straining with bowel movements. You may want to take a fiber supplement every day. If you have not had a bowel movement after a couple of days, ask your doctor about taking a mild laxative.
- If one side of your face or mouth is weaker, chew food on the stronger side of your mouth.
Keep an eye out for swallowing problems, such as:
- Coughing or choking, during or after eating
- Gurgling sounds from your throat during or after eating
- Throat clearing after drinking or swallowing
- Slow chewing or eating
- Coughing food back up after eating
- Hiccups after swallowing
- Chest discomfort during or after swallowing
- Unexplained weight loss
Activity
- Rest when you feel tired. Getting enough sleep will help you recover. When you lie down, put 2 or 3 pillows under your upper back and shoulders so that your neck and head are supported.
- You may move your neck gently sideways, up and down. You may be given stretching exercises to do at home. Avoid straining your neck muscles or lifting objects weighing more than 10 pounds (lbs) or 4.5 kilograms (kg) for 4 to 6 weeks.
- Try to walk every day. Start by walking a little more than you did the day before. Bit by bit, increase the amount you walk. Walking boosts blood flow and helps prevent pneumonia and constipation.
- Avoid strenuous physical activity, lifting heavy objects, and airplane travel for 3 weeks after surgery or until your doctor says it is okay.
- You can return to sports (golf, tennis, and running) after 4 to 6 weeks.
- Most people are able to go back to work in 2 to 3 weeks. Ask your provider when is it is OK for you to return to work.
- You will be able to drive when you can turn your shoulder far enough to see safely. DO NOT drive while you are taking strong (narcotic) pain medicine. Ask your doctor when you can drive again.
- Make sure your home is safe while you are recovering.
- You may be able to take showers (unless you have a drain near your incision). If you do have a drain near your incision, follow your doctor’s instructions to empty and care for it.
Exercise
- If you have trouble with shoulder and arm strength and movement, you may need physiotherapy. Your doctor or physiotherapist will help you with this.
Medicines
- Your doctor will tell you if and when you can restart your medicines. He or she will also give you instructions about taking any new medicines.
- If you take blood thinners, such as warfarin (Coumadin), clopidogrel (Plavix), or aspirin, be sure to talk to your doctor. He or she will tell you if and when to start taking those medicines again. Make sure that you understand exactly what your doctor wants you to do.
- Take pain medicines exactly as directed.
- If the doctor gave you a prescription medicine for pain, take it as prescribed.
- If you are not taking a prescription pain medicine, ask your doctor if you can take an over-the-counter medicine.
- If you think your pain medicine is making you sick to your stomach:
- Take your medicine after meals (unless your doctor has told you not to).
- Ask your doctor for a different pain medicine.
- Your doctor may have prescribed antibiotics. Take them as directed. Do not stop taking them just because you feel better. You need to take the full course of antibiotics.
Follow-up
You will need to see your provider for a follow up visit in 7 to 10 days. The sutures or staples will be removed at this time.
- Park B, Min C, Choi HG. Neck dissection does not increases the risk of stroke in thyroid cancer: A national cohort study. PLoS One. 2018;13(3):e0195074. Published 2018 Mar 29. doi:10.1371/journal.pone.0195074 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5875838[↩]
- Kowalski LP, Sanabria A. Elective neck dissection in oral carcinoma: a critical review of the evidence. Acta Otorhinolaryngol Ital. 2007;27(3):113–117. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2640044[↩]
- Ferlito A, Rinaldo A, Devaney KO, MacLennan K, Meyers JN, Petruzzelli GJ, et al. Prognostic significance of microscopic and macroscopic extracapsular spread from metastatic tumour in the cervical lymph nodes. Oral Oncol 2002;38:747-51[↩]
- Shah JP, Strong E, Spiro RH, Vikram B. Surgical grand rounds. Neck dissection: current status and future possibilities. Clin Bull. 1981;11(1):25-33[↩]
- Yagi S, Suyama Y, Fukuoka K, Takeuchi H, Kitano H. Recipient Vessel Selection in Head and Neck Reconstruction Based on the Type of Neck Dissection. Yonago Acta Med. 2016;59(2):159–162. Published 2016 Jun 29. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4973022[↩]
- Subramanian S, Chiesa F, Lyubaev V, Aidarbekova A, Brzhezovskiy V. The evolution of surgery in the management of neck metastases. Acta Otorhinolaryngol Ital. 2007 Apr;27(2):309-16[↩]
- Gogna S, Gupta N. Cancer, Neck Resection and Dissection. [Updated 2019 Jan 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536998[↩][↩][↩][↩][↩]
- Ferlito A, Rinaldo A. Osvaldo Suárez: often-forgotten father of functional neck dissection (in the non-Spanish-speaking literature). Laryngoscope. 2004 Jul;114(7):1177-8.[↩]
- MARTIN H, DEL VALLE B, EHRLICH H, CAHAN WG. Neck dissection. Cancer. 1951 May;4(3):441-99[↩]
- Pugazhendi SK, Thangaswamy V, Venkatasetty A, Thambiah L. The functional neck dissection for lymph node neck metastasis in oral carcinoma. J Pharm Bioallied Sci. 2012 Aug;4(Suppl 2):S245-7[↩]
- Brazilian Head and Neck Cancer Study Group. End results of a prospective trial on elective lateral neck dissection vs type III modified radical neck dissection in the management of supraglottic and transglottic carcinomas. Head Neck. 1999 Dec;21(8):694-702[↩]
- Results of a prospective trial on elective modified radical classical versus supraomohyoid neck dissection in the management of oral squamous carcinoma. Brazilian Head and Neck Cancer Study Group. Am. J. Surg. 1998 Nov;176(5):422-7[↩]
- Lydiatt DD, Karrer FW, Lydiatt WM, Johnson PJ. The evaluation, indications, and contraindications of selective neck dissections. Nebr Med J. 1994 May;79(5):140-4[↩]
- Shaw HJ. A modification of the MacFee incisions for neck dissection. J Laryngol Otol. 1988 Dec;102(12):1124-6[↩]
- Sean W. Delaney, Haoran Shi, Alireza Shokrani, and Uttam K. Sinha, “Management of Chyle Leak after Head and Neck Surgery: Review of Current Treatment Strategies,” International Journal of Otolaryngology, vol. 2017, Article ID 8362874, 12 pages, 2017. https://doi.org/10.1155/2017/8362874[↩]
- M. Dhiwakar, G. I. Nambi, and T. V. Ramanikanth, “Drain removal and aspiration to treat low output chylous fistula,” European Archives of Oto-Rhino-Laryngology, vol. 271, no. 3, pp. 561–565, 2014[↩]
- Dedivitis RA, Guimarães AV, Pfuetzenreiter EG, Castro MA. [Neck dissection complications]. Braz J Otorhinolaryngol. 2011 Jan-Feb;77(1):65-9[↩]





{kind=link}